suppl. temperature in tissues hyperthermia stationary
TRANSCRIPT

Br. J. Cancer (1982) 45, Suppl. V, 108
TEMPERATURE DISTRIBUTIONS IN TISSUES DURING LOCALHYPERTHERMIA BY STATIONARY OR STEERED BEAMS OF
UNFOCUSED OR FOCUSED ULTRASOUND
P. P. LELE AND K. J. PARKER
From the Laboratory for Medical Ultrasonics, Massachusetts Institute ofTechnology, Cambridge, MA 02139, U.S.A.
Summary.-Temperature distributions resulting from insonation with stationarvor steered beams of unfocused or focused ultrasound were measured in tissue-equivalent phantom, beef muscle in vitro, dog muscle mass, and transplanted murinetumours in vivo. Arrays of 4 to 6 thermocouples stepped through the volume ofinterest under computer control were used to measure the steady-state temperaturesat 600 to 800 locations in both in vitro and in vivo experiments. The results were con-firmed in spontaneous tumours in dog patients using fewer multi-thermocoupleprobes. Plane wave ultrasound was found to result in spatially non-uniform hyper-thermia even in superficial tumours. The region of maximum temperature rise wassmall in extent and was situated at a depth which varied in the different modelsfrom 0-5 to 1-0 cm. Neither its location nor its extent could be varied by spatialmanipulations of the transducer or by changing the insonation parameters except theultrasonic frequency. A second region of hyperthermia was produced at depth byreflective heating if an ultrasonically reflective target, such as bone or air-containingtissue, was located below the target tissue. On the other hand, using available steered,focused ultrasound techniques, tumours (whether situated superficially or at depth)could be heated to a uniform, controllable temperature without undesirable tempera-ture elevation in surrounding normal tissues. The use of steered, focused ultrasoundpermits deposition of energy to be tailored to the specific needs of each individualtumour. The small size of the focal region enables heating of tumours even whenlocated near ultrasound reflecting targets.
HYPERTHERMIA, either alone or incombination with radiation or chemo-therapy, is currently under evaluation asa modality in cancer therapy by manyinvestigators. In treatment of diseaselocalized to one or more circumscribedregions, local hyperthermia of the involvedvolume of tissue is preferable to wholebody hyperthermia, as the local tempera-tures can be raised to higher levels withoutthe toxicity and risks associated withwhole body hyperthermia. Since themargin between the temperatures fortherapeutic efficacy and damage to normaltissues surrounding the tumour is small,it is necessary that the temperatureelevation be finely and rapidly control-lable, be uniform throughout the tumourand drop off sharply outside the tumour
volume. A non-uniformity of the hyper-thermia temperature distribution maysubject some regions in the tissue volumeunder treatment to undesirably hightemperatures leading to thermal injury,while in some other regions the tempera-tures may be too low for therapeuticeffect. The possibility that such lowhyperthermia temperatures in the pro-liferating regions of the tumour mayaccelerate its growth rather than causeregression cannot be denied. Furthermore,with non-uniform intratumoral tempera-ture distribution the "heat dose" to thetumour would also be indefinable and anycorrelation with effects in tumour, at best,would be only conjectural. Thus, ideally,not only should the magnitude of tempera-ture elevation be finely controllable, but

TEMPERATURE DISTRIBUTIONS IN TISSUES
also its spatial distribution in each of thethree dimensions.
In a previous publication (Lele, 1980)it was shown that for induction of hyper-thermia, in deeply situated tumours,non-invasively, and without undesirabletemperature elevation in the overlyingskin or mucosa, it is necessary to use
focused ultrasound and to distribute theenergy within the tumour around itsperiphery. Heat transfer considerationsdiscussed later indicate that uniformdeposition of heat throughout the targetvolume of tissue will invariably lead toexcessive temperature build-up in itscentre. Thus, in addition to focusing, some
means for translocation of the focus in 3dimensions around the target volume isnecessary. Since the same considerationsalso apply to superficial tumours such a
system can also be used for hyperthermiaof superficial tumours. But, in order tocircumvent the complexity of equipmentneeded for translocation, a stationary,plane wave (unfocused) ultrasonic trans-ducer is commonly used in therapy ofsuperficial tumours. The resulting tempera-ture distributions are often measured at a
single fixed location within the tumour,since in patients it is neither feasible noradvisable to make multiple insertions ofthe thermometric device. Therefore,temperature distributions resulting fromultrasound sources, as indeed with allother sources, need to be determined inprior experiments. This paper presentsthe results of temperature distributionsmeasured in several media using bothfocused and unfocused ultrasound withstationary and steered beams and discussestheir implication to clinical use.
MATERIALS AND METHODS
Experimental mediaThese consisted of tissue-equivalent phan-
toms (t-e phantom), cuts of bovine meatin vitro and the muscle mass in the gluteal,thigh or dorso-lumbar regions of the dogin vivo. Since the acoustical properties (e.g.ultrasonic attenuation and absorption coef-
ficients and their frequency dependence,ultrasonic velocity and wavelength, acousti-cal impedance), thermophysical properties(e.g. heat capacity, heat conductivity anddiffusivity, convective heat transfer throughperfusion, etc.), as well as the anatomicaland physiological characteristics (e.g. patternof macrostructural organization with regardto homogeneity or anisotropy, degree andhomogeneity of vascularization and itsresponsivity to temperature elevation, etc.)of tumours may be significantly differentfrom those of these media, experimentswere also conducted in large specimens ofrenal adenocarcinoma transplanted subcu-taneously in the flank of the rat in vivo. Insome experiments in vivo the rat bearing thetumour was placed inside the abdomen of ananaesthetized dog to simulate deep seatedtumours.
T-e phantom.-This was a gelatin-albumin-agar mixture similar to that suggested byAstrahan (1979a, b). Its ultrasonic intensityabsorption coefficient, as compared toseveral biological tissues, is shown in Fig. 1.The molten mixture was poured into a jigcontaining 4 or more thermocouples spaced10 mm apart in both vertical and horizontalplanes. The t-e phantoms used were 15 cm indiameter and up to 15 cm in height and weremounted on a thick aluminium plate tosimulate presence of bone at that depth.Thigh of beef.-Fresh cuts of meat from
the bovine thigh, selected for uniformity ofits grain, 15 cm or more diameter and approxi-mately 15 cm in height, with and without
0.7
0.6oa
.0.5
u. 0.4w0
z 0.32
O 0.20
0.1
,,< ~~*MOUSE TUMOUR
' 1 '1 'RAT TUMOURR E
2 3 4
FREQUENCY (MHz)
FIG. 1.-Absorption coefficients of the t-ephantom and typical mammalian tissuesat different ultrasonic frequencies. Thedata shown as a cross-hatched band are
from Goss et at. (1979).
5
109
I

P. P. LELE AND K. J. PARKER
the femur, were obtained from the slaughter-house and stored in degassed normal saline,containing a mild bacteriostatic agent, attemperatures of 4 to 60C for up to one weekwhen not in use. The specimens were allowedto reach equilibrium with the ambientroom temperature of 20°C and were massaged,to dislodge any gas bubbles, before experi-ments were performed.Dog muscles.-Dogs weighing 35 to 55 kg
were tranquillized with Acepromazine andmaintained under light anaesthesia with i.v.pentobarbital sodium. Fluids were adminis-tered by a slow i.v. drip. The skin overlyingthe region under study was carefully shaved,cleaned with a detergent and massaged withultrasound coupling gel to ensure goodacoustical coupling.
Renal adenocarcinoma was transplanteds.c. in the flank of the Wistar-Lewis ratsand was used in these experiments whenapproximately 10 x 8 x 10 cm in size. Tumoursshowing any signs of necrosis were rejected.
Ultrasound sourcesX-cut quartz transducers 8 cm in diameter
at fundamental frequencies of 0.6 and 0 9MHz were driven either at the fundamentalor its odd multiple harmonic frequency,yielding frequencies of 0-6, 0 9, 1-8, 2 7, 3 0and 4-5 MHz. Central areas 1 to 6 cm indiameter were excited to change the effectivetransducer diameter for hyperthermia withplane wave ultrasonic fields. The entiretransducer diameter was excited and theenergy focused by plano-concave poly-stryrene lenses 6 cm in diameter for experi-ments with focused ultrasound. The insona-tion head was coupled to the t-e phantom orthe tissue surface by degassed water con-tained in an open plastic bag.
Ultrasound source position and motionThe insonation head containing the trans-
ducer, without or with the lens, was mountedon a computer-controlled, 3-axis positioner(Fig. 2). This enabled alignment of the axisof the insonation head with any of thethermocouple junctions, or generation ofoscillatory motions in X, Y or Z axes or ofcontinuous motion in rectilinear or curvi-linear trajectories. In the experiments des-cribed herein, oscillatory linear motions inX, Y or Z axes and circular trajectories wereused.
TRANSDUCER POSITION, MOTION 8
COMPUTER I
FIG. 2.-Insonation hdad positioning andthermocouple "stepping" system.
ThermometryElectrically insulated chromel-constantan
thermocouples, 25 to 125 microns in dia-meter, either unsheathed or sheathed in 25to 23 gauge insulated stainless steel hypo-dermic tubing (for insertion into dog musclesin vivo), were used for temperature measure-ment. Because of their small size comparedto the ultrasonic wave length in the tissues(2-5 to 0 5 mm), they were essentially non-perturbing. Heat conduction along the ther-mocouples was also found to be negligible forthe thermocouple diameters used. The barethermocouples were threaded through thespecimen and both their ends secured to ayoke. The sheathed thermocouples calibratedin mm were also inserted all the way throughthe specimen to ascertain their position andthen retracted into the tissue. The yoke or thehypodermic tubing was attached to a micro-positioner driven by a stepping motor(Fig. 2). In both instances, the thermo-junctions could be retracted through thtwregion of interest in steps of 0 01 mm orlarger under computer or manual control.The thermocouple calibration was periodi-cally checked at 3 or more temperaturesagainst a thermometer, the calibration ofwhich was traceable to N.B.S. The influenceof heat conduction along the sheath on theaccuracy of temperature measurement understeady-state conditions was determined inpreliminary experiments and suitable correc-
110

TEMPERATURE DISTRIBUTIONS IN TISSUES
tions were applied to the experimental data.For measurement of temperature distribu-tions in the specimen, 4 to 6 thermo-couples were placed in various planesthrough the volume of interest. After induc-tion of hyperthermia, when the temperaturehad stabilized, these were retracted in 0 5or 0 mm steps at intervals of 5 or moresec to allow for thermal equilibration ateach new location. Usually one additionalthermocouple was placed in the centre of
the region and held stationary to monitorchanges in the local temperature with time.For every thermocouple the temperatureand the location of the thermojunction ateach step was recorded on a multichannelstrip-chart recorder and simultaneously digi-tized and stored in the computer. Thesedata, from 600 to 800 locations within thesample, were utilized for construction ofisothermal plots. The distribution of tempera-ture was normally measured at a hyper-
B
DEPTH, cn0
2 -
3 -
4 -
5 -
6 -
7 -
8
_4 3 2 0 1 2 3 4
DIAMETER, cm DIAMETER, cm
10 I1_1_1_ 104 24 3 2 0 4 2 3 4
DIAMETER, cm DIAMETER, cm
FiG. 3.-Temperature distributions in t-e phantom, plane wave ultrasound. A, 09MHz, B, 1-8 MHz.Focused ultrasound 1-8 MHz, focused at a depth of C, 4 cm, D, 6 cm.
III

P. P. LELE AND K. J. PARKER
thermia level of approximately 6°C abovethe initial temperature.
RESULTS
The results are presented in the sequenceof increasing complexity of the mediumand are typical of those obtained in thecourse of experiments over 3 years. Therewas little variability in the distributionof temperature from specimen to specimenunder any specific experimental condi-tion. The temperature distributions pre-sented below represent the steady-statedistributions, i.e. after a steadily sustainedhyperthermia was established in thetarget medium.
(A) T-e Phantoms(i) Plane wave ultrasound.-The tem-
perature distributions obtained by insona-tion with plane-wave transducers 4 cm indiameter at frequencies of 09 and 1 8MHz, placed 1 cm from the surface ofthe phantom, are shown as plots ofisotherms in Fig. 3A and B respectively.In addition to the regularity and sym-metry of the isotherms, it should benoted that in each case the peak tempera-ture is attained over a very small volume(hot spot) and that the axial location ofthe hot spot shifts towards the surfaceat the higher frequency of ultrasound.At any of the frequencies used it was notpossible to shift the location of the hotzone higher or lower within the t-ephantom by raising or lowering thetransducer. Transducer diameter also hadno effect on the size of the hot spot.
(ii) Focused ultrasound.-The results ob-tained with focused ultrasound (Fig. 3C,D) are characterized by an absence of hotspots. Note that the temperature withinthe region of maximal insonation, whichwas 6 cm in diameter, is uniform. Further-more, the depth or the axial location ofthe hot zone can be shifted up or down bychanging the focal plane of insonation.
(B) Beef muscle in vitro(i) Plane wave ultrasound.-The tempera-
ture distributions were similar to thoseobtained in the t-e phantom as regardsthe regularity and symmetry of theisotherms and the restricted volume ofthe tissue over which peak tempera-tures could be attained (Fig. 4A, B). Theaxial location of the hottest region,however, was relatively independent ofthe distance between the transducer andthe specimen and remained at a depthof about 2 cm below the surface of themeat. Its depth was also less dependenton the ultrasonic frequency than was thecase in t-e phantom. The isothermstended to extend deeper into the tissuein the central region of insonation at thelower ultrasonic frequencies; but thetemperature gradient in the tissue betweenthe surface and the hottest region wasalways very steep, as evident from theclose spacing of the isotherms (cf, Fig. 3A, B in t-e phantom). Oscillatory motionsof the transducer along X and Y planes, oralong the Z axis, or in a circular trajec-tory, did not influence the pattern oftemperature distribution.
In an attempt to avoid the build up ofheat in the superficial regions of thetissue, two insonation strategies wereevaluated. In one, insonation was per-formed using two, cross-fired, plane wavetransducers, each angled 300 off normalso that their fields overlapped at a certaindepth within the tissue. One of the trans-ducers was driven at 2-7 MHz and theother at 1 2 MHz to provide increased"penetration depth". The resultant pat-tern of temperature distribution (Fig. 4C)is similar to those with single, perpen-dicularly placed transducers (Fig. 4A, B)except for a distortion in the symmetryof isothermal lines. The size of theregion of maximum temperature rise wasstill very small and its location could notbe shifted by varying the angles ofincidence of the two ultrasound beams.Use of focused transducers, focused atthe same region (isocentric insonation) ortwo adjacent regions within the tissuedid not significantly alter the pattern oftemperature distribution (4D). Occur-
112

TEMPERATUJRE DISTRIBUTIONS IN TISSUES
I
WE
4 i 2 i 6 i iDIAMETER,.'.
3i 4
6-
|~~~~~~~g Vi
41
2 -61o 1 2 3 4DIAMEErER. e
4 3 I 0 1 2 3 4DIAMETER..o
FG. .4.FIG[. t-..T raur d ibut bef
in vi o. A, 04Ek9 B, 27
wave.:U W 1'! dR,
foouadgb"4b1m zMIAm__eAwtraje iie.
113
i i i4 3 2 1 0 1
DIAMETER, cm2 3 4
-
O' , , , *, a ,, a

P. P. LELE AND K. J. PARKER
A
DEPTH.c
6-
- -5 1- { | t4 3 2 0 1 2 3 4
DIAMETER, cm
FIG. 5.-Temperature distribution in beefin vitro, steered focused ultrasound.A, two beams 2-7 MHz, angled 20° off-nor-mal, focused 3 cm below surface; B, twobeams, vertical, 0 9 MHz, focused 6 cmbelow surface.
rence of hot-spots and inhomogeneity oftemperature distribution could not beavoided by varying the distance betweenthe two ultrasonic foci.The second strategy utilized a plane
wave transducer, angled at 20° to thevertical axis and rotated in a circulartrajectory with its centre 3 cm below thesurface (Fig. 4E). Note that the regionof heat build up in the superficial regionsof the meat has shifted from the central
to the annular region in path of insona-tion and that the maximum tempera-ture rise is now at a depth of 3 cm.However, the hottest region is still verysmall in volume and the temperaturefalls off sharply in all directions awayfrom it.
(ii) Focused ultrcasound.-In beef invitro, as in t-e phantoms, focused ultra-sound yields a uniform temperature distri-bution across the entire diameter ofmaximum hyperthermia (Fig. 5A, B).Note also that the axial extent and loca-tion of the hyperthermic zone can beprecisely controlled.
(C) Dog muscle in vivo(i) Plane wave ultrasound.-The tem-
perature distributions obtained in thegluteal muscle mass of the dog withplane wave ultrasound are characterizedby an asymmetric pattern (Fig. 6A, B)totally unexpected on the basis of theexperiments on the t-e phantom or on
the selected cuts of beef in vitro, in thatthe location of the hottest spot bore no
definite spatial relationship to the centreof the transducer. The size and the loca-tion of the region of highest temperature,however, was relatively independent ofthe ultrasonic frequency as was found tobe the case in beef in vitro. This was
located 1 cm from the skin surface regard-less of the distance between it and thetransducer. Also note that although thetemperatures become progressively lowerwith increasing depth below the hottestregion there exists a second hot region inthe tissue at depths of 2-5 to 5 cm. Inthis experiment the distal skin-air inter-face was at 5 cm. The occurrence of thesecond or deeper hot region must beattributed to the reflection of the trans-mitted energy back into the tissues atthe distal skin-air interface. Similar re-
flection and tissue heating would alsooccur from the presence of a bone in thepath of ultrasound.
Repetition of the experiments, withprecise localization of the thermojunctionsby scanning with focused ultrasound under6 5 4 3 2 0 12 3 4 5 6
DIAMETER, cm
114

TEMPERATURE DISTRIBUTIONS IN TISS1UES
1.8 MHz FOCUSEDINSONATION
IN CIRCULAR TRAJECTORY.1
DISTANCE, cm
DOG LEG IN VIVODEPTH cm
* \
B
DISTANCE, cm
46
* 44
_ 424
> 40
38
DOG LEG IN VIVO- DEPTH cm
14 z 2 3 4 4 3 2 0 2 3 4DISTANCE, cm DISTANCE,
FiG. 6. Temperature distributions in gluteal muscle mass of dog in vivo. Plane wave ultrasound,1-8 MHz. A, isotherm plot; B, temperature distribution at 1 cm depth. Steered, focused ultrasound,1-8 MHz at cm depth, C, isotherm plot; D, temperature (listribution at 1 cm deptl.
computer control, confirmed the asym-metry of the isotherms relative to theposition of the insonating transducer(Fig. 6B). The degree and the directionof the asymmetry varied, to some extent,with the region in which hyperthermiawas induced. In order to determine thereason for the asymmetry, the thermo-couple tracks were examined by slicingthrough the tissue post-mortem. It was
found that the thermocouples traversed a
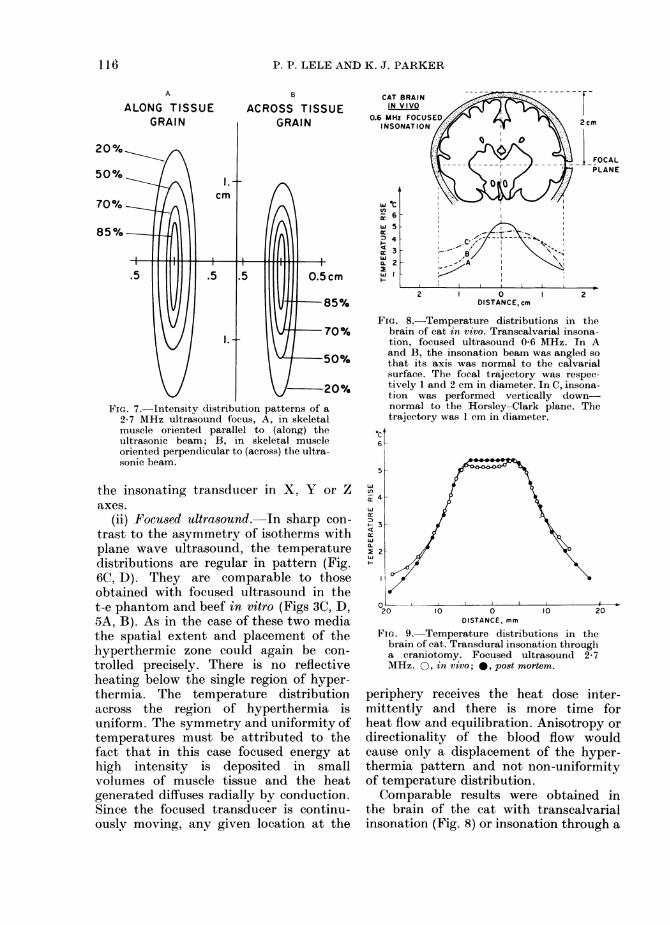
number of different muscle groups andintervening connective tissue and musclesheaths. In contrast to the selected cutsof beef in vitro, the fascicles and fibres ofdog muscles were oriented in differentdirections. Tissues such as the muscles,the nerves or the white matter of thecentral nervous system, with a conspicuousdirectionality in their pattern of organiza-tion, display anisotropy with respect topropagation of ultrasound (Lele, 1975).Fig. 7 shows the intensity distribution
patterns of the focal region of a 2-7 MHzfocused transducer in water and in musclealong and across the direction of itsfibres. The difference in the shape of thefocus along and across the muscle atteststo differences in ultrasonic propagationvelocities, which could lead to beam diffrac-tion. Similarly differences were found toexist in absorption coefficients measuredalong and across the muscles. Thesedifferences in ultrasonic absorption, to-gether with the highly directional natureof the blood flow confined to each indi-vidual muscle and the absence of bloodflow across the fascial sheaths, mayaccount for the asymmetric patterns oftemperature distributions in these experi-ments.
Neither the pattern of temperaturedistribution, including reflective tissueheating, nor the size and location of thehottest region could be significantlyaltered by linear or circular motions of
44
r 42
X 40
- 38
115
F---l'
A 'kDL ,-
P. P. LELE AND K. J. PARKER
ACROSS TISSUEr-DAIlKI
FIG. 7. Intensity distribution patterns of a2-7 MHz ultrasound focus, A, in skeletalmuscle oriented parallel to (along) theultrasonic beam; B, in skeletal muscleoriented perpendicular to (across) the ultra-sonic beam.
the insonating transducer in X, Y or Zaxes.
(ii) Focu8ed ultrasound. In sharp con-
trast to the asymmetry of isotherms withplane wave ultrasound, the temperaturedistributions are regular in pattern (Fig.6C, D). They are comparable to thoseobtained with focused ultrasound in thet-e phantom and beef in vitro (Figs 3C, D,5A, B). As in the case of these two mediathe spatial extent and placement of thehyperthermic zone could again be con-
trolled precisely. There is no reflectiveheating below the single region of hyper-thermia. The temperature distributionacross the region of hyperthermia isuniform. The symmetry and uniformity oftemperatures must be attributed to thefact that in this case focused energy athigh intensity is deposited in smallvolumes of muscle tissue and the heatgenerated diffuses radially by conduction.Since the focused transducer is continu-ously moving, any given location at the
2cm
FOCALPLANE
2 0 2DISTANCE, cm
FIG. 8.-Temperature distributions in thebrain of cat in vivo. Transcalvarial insona-tion, focused ultrasound 0-6 MHz. In Aand B, the insonation beam was angled so
that its axis was normal to the calvarialsurface. The focal trajectory was respec-
tively 1 and 2 cm in diameter. In C, insona-tion was performed vertically down-normal to the Horsley-Clark plane. Thetrajectory was 1 cm in diameter.
6c
cc
x 4
a:
3
M 2
O L j 1.
20 10 0 10 20DISTANCE, mm
FIG. 9. Temperature distributions in thebrain of cat. Transdural insonation througha craniotomy. Focused ultrasound 2- 7MHz. 0, in vivo; 0, post mortem.
periphery receives the heat dose inter-mittently and there is more time forheat flow and equilibration. Anisotropy ordirectionality of the blood flow wouldcause only a displacement of the hyper-thermia pattern and not non-uniformityof temperature distribution.Comparable results were obtained in
the brain of the cat with transcalvarialinsonation (Fig. 8) or insonation through a
A
ALONG TISSUEA. 0 ,A M
II I~~~~
I16.

TEMPERATURE DISTRIBUTIONS IN TISSUES
body; e.g. those of abdominal viscera. Acomputer plot of the temperature profilesmeasured by one stepped thermocouple,representative of the results obtained inother experiments with multiple thermo-couples, is reproduced in Fig. 12. Thetemperature in the abdominal wall muscle
2 3 4
FIG. 10. Temperature distributions in aflank implanted tumour in rat in vivo.Plane wave ultrasound, 1-8 MHz.
craniotomy (Fig. 9), in vivo as well aspost mortem. Note that the uniformityof the hyperthermia is not affectedby the presence or absence of blood flow,although more power was required toattain and sustain the desired temperaturein vivo with blood flow than post mortem.
(D) Rat tumour in vivo(i) Plane wave ultrasound.-The tem-
perature distributions (Fig. 10) closelyresemble those in beef in vitro (Fig. 4)rather than those in the muscle-mass ofthe dog in vivo (Fig. 6). As in these twomedia, the size of the hottest region isvery small and its location in depth wasfixed and could not be changed bychanging the distance between the trans-ducer and the skin or by change in theultrasonic frequency.
(ii) Focused ultrasound.-Uniform andcontrollable levels of hyperthermia couldbe produced in volumes of tumour 6 to 8cm in diameter and up to 8 cm below thesurface, with the equipment available.Fig. 11 shows data from 2 such experi-ments. Note the sharp fall-off of tempera-ture away from the region of hyperthermiaat the rate of approximately 0.3°/mm.
Rat tumour in vivo placed in the abdominalcavity of dog in vivo
These experiments were conducted tosimulate tumours located deep in the
9
2 0 2 3
DISTANCE, cm
FIG. 11.-Temperature distributions in aflank-implanted tumour in rat in vivo.Steered focused ultrasound, 3 cm depth.x, 2 cm diameter; 0, 5 cm diameter.
SCHEMATIC DRAWING OF THE EXPERIMENT
45
*cv=
40
35O 2 3 4 5 6 cm
FIG. 12.-Temperature distribution in a flank-implanted tumour in rat in vivo placed inthe abdominal cavity of dog in vivo.Tumour tenperature was measured with a
stepped thermocouple. Temperature inoverlying dog tissues was continuouslymeasured with a stationary thermocouple.
t40o
ei 3811w1r-ID
-
< 36L-
32
4 3 2 0DISTANCE, cm
117
5

P. P. LELE AND K. J. PARKER
TEMPERATURE
A
LOSS
B
FiG. 13.-Schema of temperature distribu-tions in a tissue volume subjected to A,spatially uniform heat deposition; B, heatdeposition at the perimeter.
overlying the tumour in the insonationpath was measured by a stationarythermocouple. Note that, though thetemperature in the tumour was raised by11 °C, the temperature rise in the overlyingmuscle was only 2°C.
Spontaneous tumours in dog in vivo
Temperature distributions were mea-sured by withdrawing a multithermo-couple probe through the region of interestduring treatment of spontaneous tumours(Odontoma, fibrosarcomas, tonsillar car-
cinoma, melanomas etc.) in dog patients.Results were similar in all respects to thoseobtained in transplanted tumours in therat (Figs 11, 12).
DISCUSSION
The temperature distributions resultingfrom insonation of tumours and normaltissues in vivo as well as in vitro, withplane wave and moving focused ultra-sound fields, clearly demonstrate the
inefficacy of the former to raise to auniform level the temperature of anysignificant volume of even superficialtissue.
In all of the experiments with planewave fields at different ultrasonic fre-quencies, transducer dimensions, distancesfrom the surface of the medium, pre-sence or absence of transducer motionetc., whether in biological tissues or in thet-e phantom, the characteristic patternof resultant temperature distributions wasconsistently found to be a small, almostpunctate, volume of maximum tempera-ture elevation surrounded by volumes ofprogressively lower temperatures. Thedepth of the spot of maximum tempera-ture elevation from the surface of themedium was fixed for any particularmedium and could not be varied bychanging the distance of the transducer.This depth, although it could not becontrolled, varied from one medium toanother and thus must be related pre-dominantly to the ultrasonic attenua-tion and heat diffusion characteristics ofthe medium itself. With plane waveinsonation, the occurrence of a smallregion of high temperature located ap-proximately in the centre of the insonatedvolume is not surprising and is predictableon the basis of rather simple heat transferanalysis. Mathematical analysis is beyondthe scope of this article and it maysuffice here to state that since the heatfrom a hyperthermic volume of tissue mustleave the region through its periphery-whether by conduction alone or withperfusion-the peripheral regions will al-ways be cooler than the centre (Fig. 1 3A).For this reason the energy needs to bedeposited preferentially at the surface ofa tumour to achieve uniform hyper-thermia therein (Fig. 13B). This, ofcourse, is possible by moving the smallfocal region of a focused beam of ultra-sound but not with plane wave sources.Any detailed analysis of the energydeposition from plane wave sources isfurther complicated by the fact that inalmost all instances the tissues lie in their
118
i-

TEMPERATURE DISTRIBUTIONS IN TISSUES
near field in which the intensity distri-bution is very inhornogeneous.
Focusing of the energy also enablescontrol of the depth at which hyper-thermia is produced, which is not possiblewith plane wave sources as discussed in aprevious paper (Lele, 1980) and seen inthe results of the experiments describedherein. The ability to deliver the energyprecisely, at the surface of the targetvolume of tissue, permits generation oflocalized hyperthermia even in irregularlyshaped tumours, without subjecting anysignificant volumes of surrounding normaltissues to unnecessary heat stress. This isspecially important if the tumour islocated close to a bone or an air-con-taining organ, e.g. the lungs or intestines.The intensity reaching such an organ afterpassage through the tumour would havedecayed only by attenuation in thetumour when plane wave energy isused for insonation since, in practice, theinsonated tissues almost always are locatedin the near field of the transducer wherethe beam is collimated. With a focusedbeam it will additionally be attenuated bybeam divergence. Furthermore, with afocused beam, the angle of incidence andthe amplitude of excitation of the trans-ducer can be controlled at every point inits trajectory and thus the safety ofcritical target areas and surroundingtissues can be ensured. This is not -pos-sible with plane wave insonation systems.In superficial tumours this would be ofspecial concern, since many of thesetumours lie directly over the bone or air,as in the case of metastatic breast canceror cancer in the head and neck region.In these cases the possibility of excessiveheating of deeper tissues by energyreflected from underlying bone (Fig. 6A)must also be borne in mind. It is interest-ing to note that Marmor et al. (1979b)found that the temperature near thebone in one of their patients was signifi-cantly higher than that in the tumouritself.The measurement and specification of
temperature in the non-uniform spatial
distribution of the hyperthermia fromplane wave sources present special practi-cal and conceptual problems not en-countered in the spatially uniform hyper-thermia produced by focused ultrasound.In the absence of a non-invasive techniquewith sufficient resolution, the region ofmaximum temperature, generally restric-ted to a few millimeters in each of threedimensions, can be located only bycareful and thorough scanning of thevolume of tissue in small steps in eachof the three planes with an implantedthermometric device. Such scanning mightprove inadvisable or impracticable inmany patients because of the locationof the tumour and patient movement.Temperature measured at an arbitratilylocated point is likely to be lower thanthe peak temperature reached in thetumour. This could lead to local thermalpain or damage in the region of highertemperatures, as reported by Marmoret al. (1978; 1979a, b) in their animal andhuman patients. The occurrence of thisinjury is predictable on the basis oftemperature - duration relationships forthermal damage (Lele, 1977). Even iftemperatures at a number of points with-in the tumour were determined, becauseof the non-uniformity of temperaturedistribution it would be impossible tocorrelate them with effects on tumourgrowth or regression. This lack of uni-formity may contribute, to a large extent,to the lack of close agreement betweenthe results obtained in cell cultures andthose that have been obtained in tumourson the effects of hyperthermia on neo-plastic cells. The fact that the use ofplane wave sources results in hyper-thermia which is maximum near thecentre and falls off towards the peripheryshould be of considerable concern. Athreshold tumoricidal temperature (orheat dose) in the centre of a tumour wouldsubject the proliferating tumour tissue atthe periphery to a lower temperature (orheat dose) which at best would be ineffec-tive, and at worst may stimulate tumourgrowth. On the other hand. with steered
119

P. P. LELE AND K. J. PARKER
focused ultrasound, even under sub-optimal conditions, the temperature wouldalways be higher at the proliferatingmargins of the tumour than at thecentre, which is often necrotic in tumoursof clinically relevant sizes.
Thus, detailed and accurate measure-ment of temperature distributions, in-duced in tissues by a given mode forproduction of hyperthermia, cannot beoveremphasized. Since these measure-ments cannot be conducted in patientsdue to unavailability of non-invasivetemperature measuring devices with ade-quate spatial resolution and sensitivity,the studies must necessarily be conductedin experimental tumours or animals,excised tissues or t-e phantoms. Thebest experimental substitute for a spon-taneous tumour in man would appear tobe a spontaneous tumour in animal and,possibly, the second best a transplantedtumour both in vivo. However, thecomparison of the results obtained invivo with those obtained post mortem inthe brain and in tumours in this studyindicate that the distribution of tempera-ture in a zone of hyperthermia itselfdoes not change when perfusion ceases-only the spatial rate of the fall-off oftemperature to normothermic values isslightly lowered. The effects of perfusioncan be computed mathematically andadded to the temperature distributionsmeasured in vitro. Thus preliminarystudies, conducted in large cuts of meatcarefully selected for uniformity of grain,can yield useful data on temperaturedistributions resulting from any deviceto induce hyperthermia. In the presenceof blood flow, the power requirements forinduction and maintenance of the levelof hyperthermia are higher and thepattern of temperature distribution mayshow slight displacements. These too canbe estimated from comparison of theresults obtained in vivo and post mortem.The use of a t-e phantom can yield mis-leading results unless the phantom istruely tissue-equivalent both in its acou-stic and heat transfer characteristics.
CONCLUSIONSInsonation with plane wave ultra-
sound results in spatially non-uniformhyperthermia which is characterized bythe existence of a small, almost punctate,region of maximum temperature rise thedepth of which appears to be dependenton the acoustic and heat transfer proper-ties of the medium and cannot be alteredby spatial manipulation of the planewave ultrasonic source. The existence ofan ultrasound reflecting structure belowthe target may lead to the generation of asecond region of hyperthermia at depth.The region of maximum temperatureelevation cannot be easily located, exceptby thorough scanning of the region in all3 orthogonal planes, because of thesmallness of its size and is likely to bemissed by temperature measuring pro-cedures practicable under clinical con-ditions. This may explain the occurrenceof burns observed by various investi-gators in animal and human tumourtreatments using plane wave ultrasound.Furthermore, the resultant non-uniformityof temperature distributions within thetumour renders impossible any precisecorrelation of the temperature and dura-tion of hyperthermia (either alone or incombination with radiation or chemo-therapy) with resultant effects on tumours.Thus, plane wave ultrasound is notoptimal even for therapy of superficiallesions.
All these problems and difficulties areobviated by use of focused ultrasoundwhich enables precise tailoring of the heatdose to individual tumours. Spatiallyuniform levels of hyperthermia, restrictedto the tumour, located superficially or atdepth, can be achieved with equipmentpresently available.The best model for evaluation of
devices for production of local hyper-thermia appears to be a large, non-necrotic transplanted tumour in the flankof the rat in vivo. This can be overlaidby muscles of dog in vivo to simulatedeeply situated tumours when necessary.Selected cuts of meat in vitro, appear to
120

TEMPERATURE DISTRIBUTIONS IN TISSUES 121
be satisfactory for preliminary studies.A phantom which is truly tissue-equivalent for evaluation of ultrasonichyperthermia is not yet available.
This research was supported in part by USPHSGrants CA 16111 and CA 26232. It is a pleasure toacknowledge the assistance of Mr K. E. Greene inprocurement of tissue samples, Mr R. C. Green-wald, III in the taming of the computer and MrEric Buckman in many of the scans. The considerategenerosity of Dr Ralph de Vere White, UrologyService, Boston University School of Medicine, insupplying specimens of the renal adenocarcinomatransplanted in the flank of the rat is gratefullyacknowledged.
REFERENCES
ASTRAHAN, M. A. (1979a) Letter on hyperthermiaphantom. Med. Phys., 6, 72.
ASTRAHAN, M. A. (1979b) Concerning hyperthermiaphantom. Med. Phys., 6, 235.
Goss, S. A., FRIZZELL, L. A. & DUNN, F. (1979)Ultrasonic absorption and attenuation in mam-malian tissues Ultrasound Med. Biol., 5, 181.
LELE, P. P. (1975) Hyperthermia by ultrasound.In Proceedings of the International Symposium onCancer Therapy by Hyperthermia and Radiation.
Washington, D.C., 28-30 April 1975. AmericanCollege of Radiology. p. 168.
LELE, P. P. (1977) Thresholds and mechanisms ofultrasonic damage to "organized" animal tissues.Symposium of Biological Effects and Characteriza-tions of Ultrasound Sources. (Eds DeWitt, G.,Hazzard & Litz). Proc. of a Conference held inRockville, Md., 2-3 June 1977, HEW Publication(FDA) 78-8048. p. 224.
LELE, P. P. (1980) Induction of deep, local hyper-thermia by ultrasound and electromagneticfields: problems and choices. Radiat. Environ.Biophys. 17, 205.
LELE, P. P., PARKER, K. J. & CASTRO, E. P. (1978)Deep local hyperthermia by focused ultrasound.Int. J. Radiat. Oncol. Biol. Phys., 4, Suppl. 2, 118.
LELE, P. P. (1979) A strategy for localized chemo-therapy of tumours using ultrasonic hyper-thermia. Ultrasound Med. Biol., 5, 95.
MARMOR, J. B., POUNDS, D., HAHN, N. & HAHN,G. M. (1978) Treating spontaneous tumours indogs and cats by ultrasound-induced hyper-thermia. Int. J. Radiat. Oncol. Biol. Phys., 4,967.
MARMOR, J. B., HILERIO, F. J. & HAHN, G. M.(1979a) Tumour eradication and cell survivalafter localized hyperthermia induced by ultra-sound. Cancer Res., 39, 2166.
MARMOR, J. B., POUNDS, D., POSTIC, T. B. & HAHN,G. M. (1979b) Treatment of superficial humanneoplasms by local hyperthermia induced byultrasound. Cancer, 43, 188.