supervised by - university of mosulmedicinemosul.uomosul.edu.iq/files/pages/page_9896672.pdfdescribe...
TRANSCRIPT


Supervised by
Dr.Bassam
Presented by:
Sarah Y. Al-obaidy
Sarah N. Ali
Neonatal Jaundice
Define Neonatal Jaundice
Explain the etiology of Neonatal Jaundice
Describe the pathophysiology
List the clinical manifestation
List the types of Neonatal Jaundice
Describe the investigation and diagnostic test
Describe the management of Neonatal Jaundice
Explain the treatment and complication
Objective

Jaundice is quite common
Full term infants: at least 50%
Preterm infants: over 80%
When - in the first week of life
Where - skin , mucosa and sclera
Jaundice become evident clinically blood bilirubin
when bilirubin concentrations is ≥(5 – 7) mg/dl.
Introduction
Neonatal jaundice :-
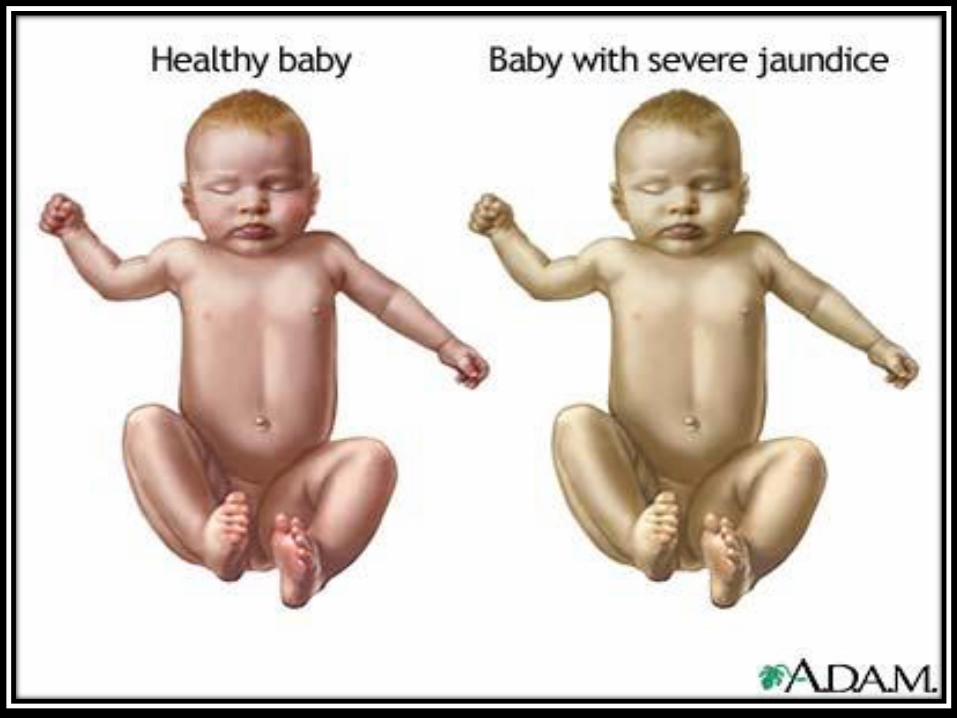
Hyperbilirubinemia: refers to an excessive level of accumulated bilirubin in the blood and is characterized by jaundice, a yellowish discoloration of the skin, sclera, mucous membranes and nails.
Unconjugated bilirubin = Indirect bilirubin.
Conjugated bilirubin = Direct bilirubin.
Definition
1) Physiological jaundice :
Characteristics
Term baby: peak of indirect bilirubin less than
12 mg/dl on day 3 of life.
Premature: Peak of indirect bilirubin less than
15 mg/dl on day 5 of life.
Maximum intensity by 4th-5th day in term baby& 7th day in preterm baby.
Types of neonatal jaundice
Increased bilirubin load : Increased bilirubin production resulting from increased
RBC mass Shortened RBC life span (70-90)days
Defective uptake from plasma. Defective conjugation. Decreased excretion. Increased entero-hepatic circulation.
Etiology of Physiological Jaundice
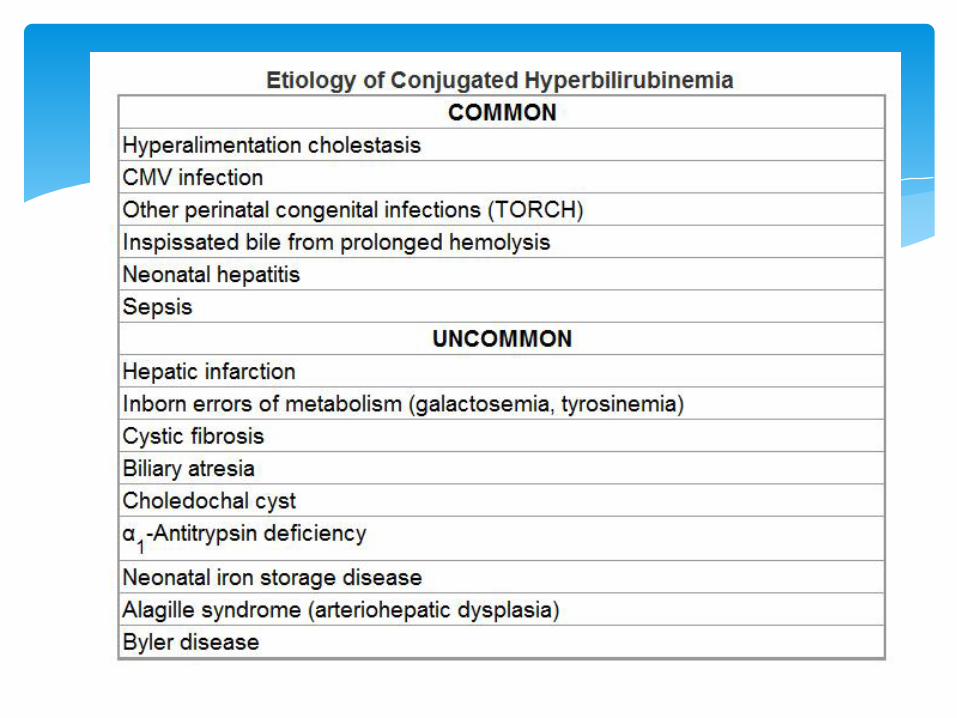
Pathological jaundice
2) Pathological jaundice
Appears within 24 hours of ageIncrease of bilirubin > 5 mg / dl / hrSerum bilirubin > 13 mg / dl in term baby and there is:
1)direct bilirubin fraction us greater than 1.5 mg/dl2) hepatospleenomegaly and anemia present
Jaundice persisting after 14 daysStool clay / white colored and urine staining clothes yellow

3) Breast feeding jaundice
Occur when the baby did not feed adequately.
When the baby did not receive enough milk, indirectly the baby did not have adequate bowel movement.
So, the bilirubin cannot be remove from the body.
Breast feeding jaundice
4) Breast milk jaundice
May be associated with unconjugated hyperbilirubinemiawithout evidence of hemolysis during the 1st to 2nd week of life.
Bilirubin levels rarely increase to more than 20 mg/dL. Interruption of breastfeeding for 1 to 2 days results in a rapid decline of bilirubin levels, which do not increase significantly after breastfeeding resumes.
Breast milk may contain an inhibitor of bilirubin conjugation or may increase enterohepatic recirculation of bilirubin because of breast milk glucuronidase.
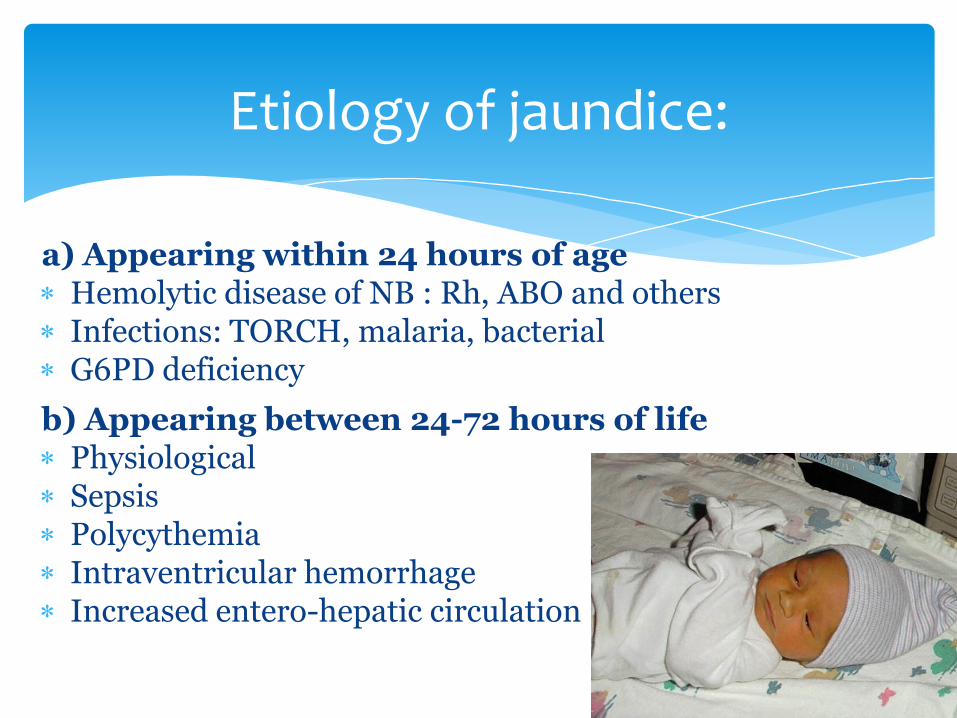
a) Appearing within 24 hours of age Hemolytic disease of NB : Rh, ABO and others Infections: TORCH, malaria, bacterial G6PD deficiency
b) Appearing between 24-72 hours of life Physiological Sepsis Polycythemia Intraventricular hemorrhage Increased entero-hepatic circulation
Etiology of jaundice:
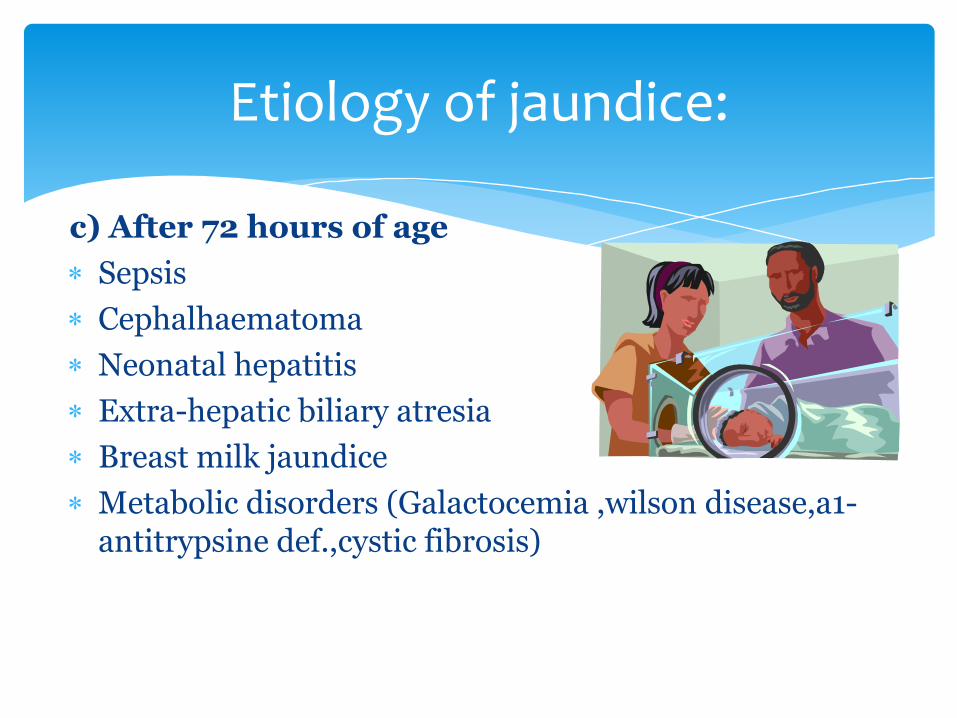
c) After 72 hours of age
Sepsis
Cephalhaematoma
Neonatal hepatitis
Extra-hepatic biliary atresia
Breast milk jaundice
Metabolic disorders (Galactocemia ,wilson disease,a1-antitrypsine def.,cystic fibrosis)
Etiology of jaundice:
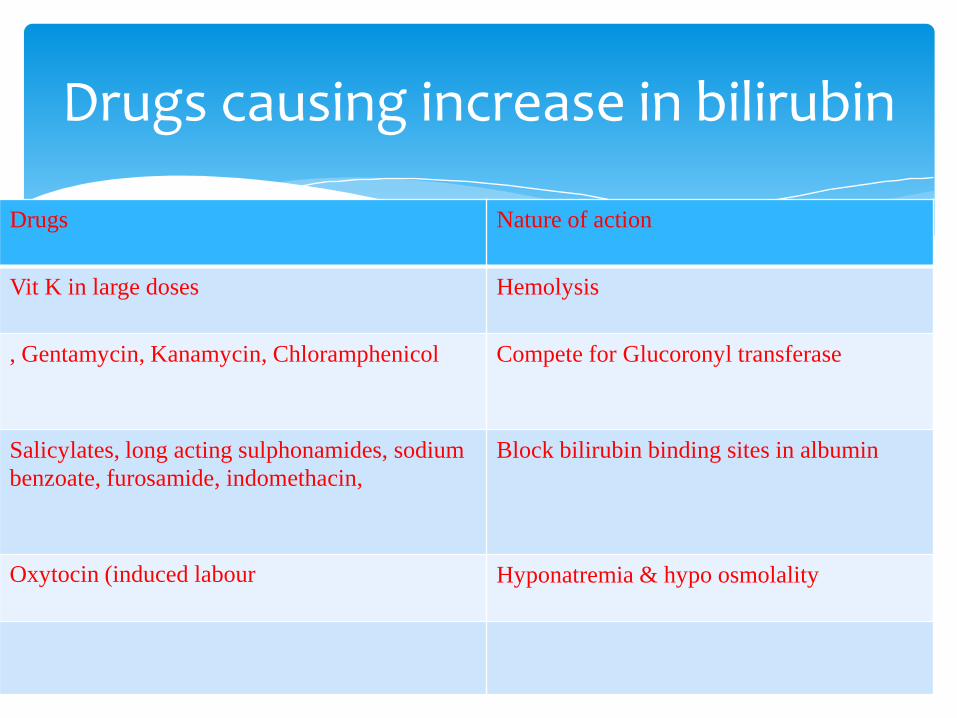
Drugs Nature of action
Vit K in large doses Hemolysis
, Gentamycin, Kanamycin, Chloramphenicol Compete for Glucoronyl transferase
Salicylates, long acting sulphonamides, sodium
benzoate, furosamide, indomethacin,
Block bilirubin binding sites in albumin
Oxytocin (induced labour Hyponatremia & hypo osmolality
Drugs causing increase in bilirubin
JAUNDICE
J - jaundice within first 24 hrs of life
A - a sibling who was jaundiced as neonate
U - unrecognized hemolysis
N – non-optimal sucking/nursing
D - deficiency of G6PD
I - infection
C – cephalhematoma /bruising
E - East Asian/North Indian
Risk factor of neonatal jaundice
Excess bilirubin In the blood
Liver immature to process bilirubin to be excrete out from body
Accumulation of bilirubin in blood
Neonatal jaundice
Pathophysiology ; neonatal jaundice
Ask 4 questions - What is the birth weight? What is the gestation? What is the postnatal age in hours? Is the jaundice physiological or pathological?
If jaundice is physiological and baby is well – only observe
If deep jaundice – Assess for bil toxicity (kernicterus) *Lethargy and poor feeding, poor or absent Moro's,
or convulsions
Approach to a jaundiced baby
Jaundice may be present at birth or at any time during the neonatal period.
Jaundice usually begins on the face and, as the serum level increases, progresses to the chest and abdomen and then the feet.
Jaundice resulting from deposition of indirect bilirubin in the skin tends to appear bright yellow or orange; jaundice of the obstructive type (direct bilirubin), a greenish or muddy yellow.
Clinical manifestation
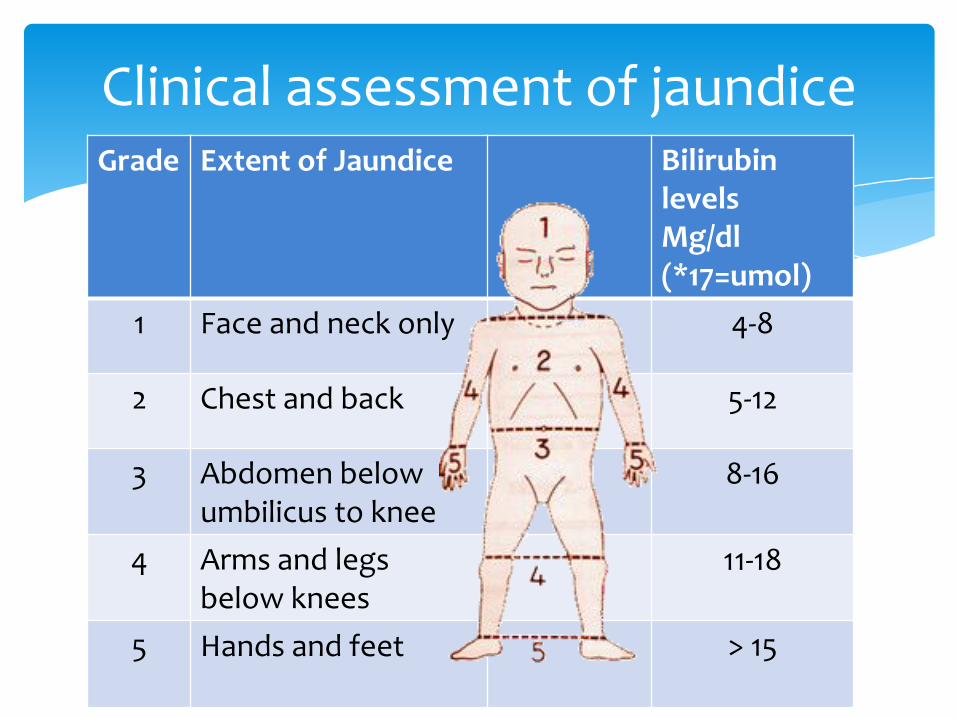
Clinical assessment of jaundiceBilirubin levelsMg/dl(*17=umol)
Extent of JaundiceGrade
4-8Face and neck only1
5-12Chest and back2
8-16Abdomen below umbilicus to knee
3
11-18Arms and legs below knees
4
> 15Hands and feet5
H/O Jaundice, Exchange Blood transfusion / Kernicterus in previous sibling
Mother – O group or Rh –ve
Jaundice – Within 24 hrs or after 72 hrs
Trunk distinctly yellow stained
Sick jaundiced baby
Jaundice persisting > 2 weeks
Yellow colored urine or clay colored stools
Indication for lab investigations (In high risk infants)
1. Total serum bilirubin (Direct&Indirect)
2. Complete blood count (Hb, shape of RBC)
3. Reticulocyte count
4. Blood group of baby and mother
5. Coombs’ test
Investigation & diagnosis
Prevention of Rh isoimmunization
Withhold drugs that aggravate jaundice or block bilirubin binding sites in albumin
Avoid phenolic detergents in nursery(Increase RBCs destruction and decrease liver enzymes activity)
Adequate feeding and hydration
Treatment of sepsis
Preventive and supportive measures

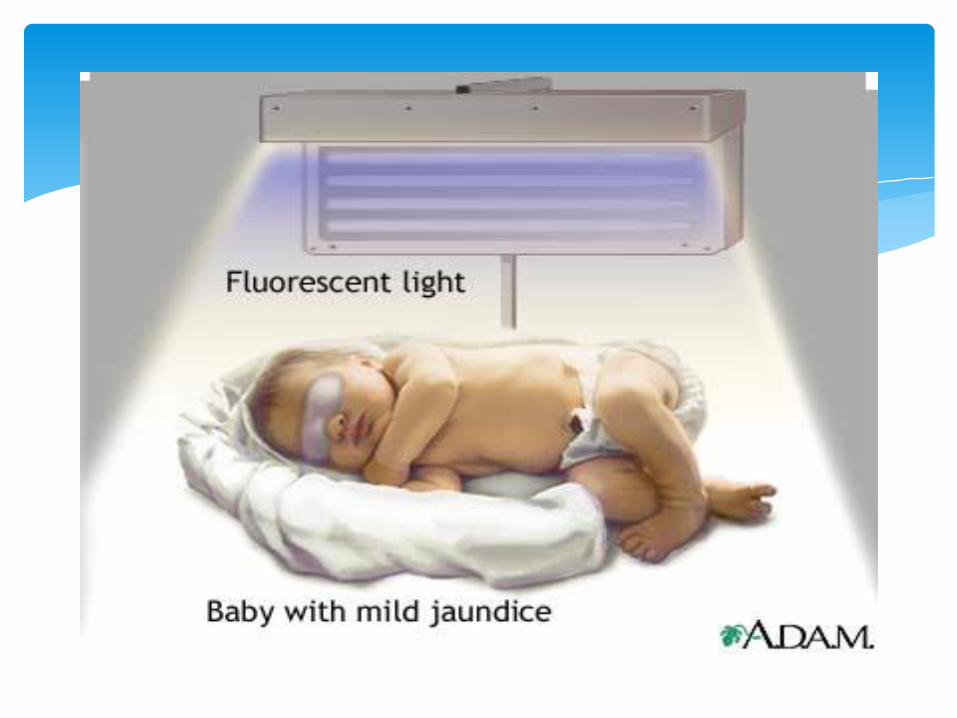
Phototherapy
Exchange transfusion
IV Immunoglobulin (for ABO &Rhincompatability in adose of 0.5_1 gm/Kg/ dose repeated every 12 hr.)
Measures to reduce Serum Bilirubin
Safe and effective Bilirubin absorbs light maximally at 420 – 460 nm Causes photo-oxidation & photo-isomerization of
bilirubin Enhances hepatic exertion of unconjugated
bilirubin into the intestinal lumen Single & double surface system 6 - 8 daylight tubes or 4 blue/ white tubes mounted
on a stand with grounded electrical outlets. Change tubes every 1000 hours or after 3 months
of use Nurse in cradle or incubator
Phototherapy
1. Perform hand wash2. Place baby naked 45 cm away from the tube lights in
a crib or incubator 3. Fix eye shades - to prevent damage to the retina. 4. Start phototherapy5. Frequent extra breast feeding every 2 hourly6. Turn baby every two hours or after each feed (in
single surface)
8. Monitor – Temp - 2 to 4 hourly, wt -daily, urine frequency, bilirubin - 12 hrly
9. More frequent breastfeeding or 10-20% extra fluid is provided.
10. Measure rebound bilirubin 6-8 hours after stopping phototherapy.
Remember - Baby appears bleached when under phototherapy. Hence clinical assessment of jaundice not reliable. Monitor S bilirubin.
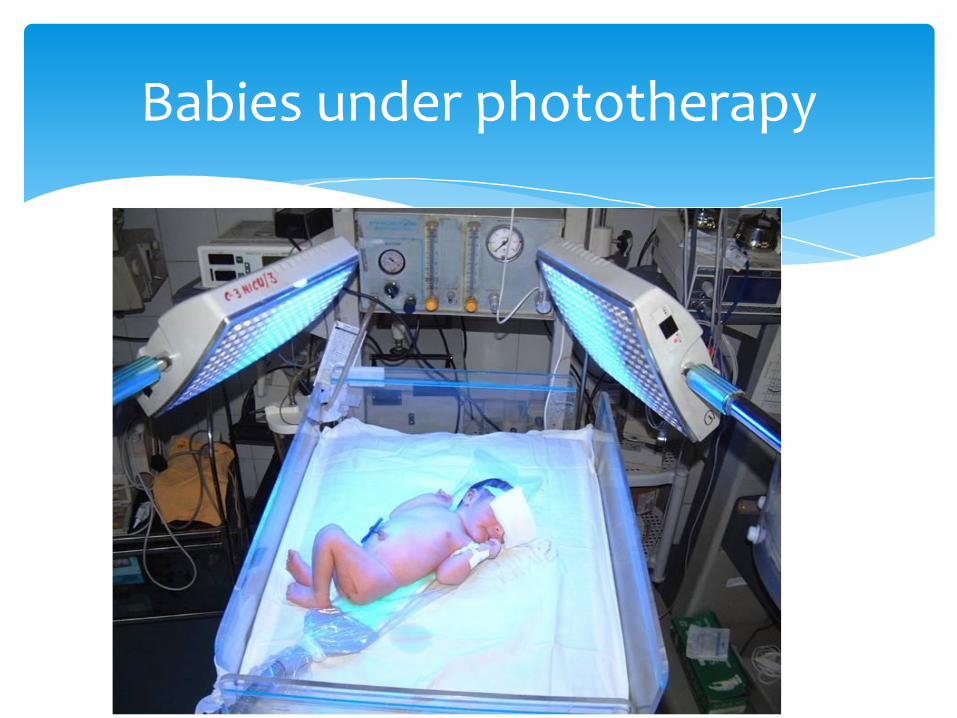
Babies under phototherapy
Increased insensible water loss
Loose stools
Skin rash
Bronze baby syndrome
Hyperthermia
Upsets maternal baby interaction
Side effects of phototherapy


Most effective and reliable method to reduce serum bilirubin.
Anticipation and early referral to a higher centre is important
Indications –
Cord Hb 10 gm% or less
Cord bilirubin 5 mg% or more
Unconjugated S. bil 10 mg% within 24 hrs or 15 mg% within 48 hrs or rate of rise of 0.5 mg% per hr
Exchange transfusion

When ever you suspect symptoms&signs of early or late kernikterus, we will go for exchange transfusion
Indications for Exchange Transfusion


ABO incompatibility
Use O cells of same Rh type, ideal - O cells suspended in AB plasma.
Rh isoimmunization
Other situations
Baby's blood group
Choice of blood for exchangeblood transfusion
- . Double volume exchange for jaundice:
(Approximatly 2 x 85 ml/kg)• Term infant – 200 -250 mls/kg or
80 – 85 mls/kg x 2/3• Preterm infant – 300 mls/kg or
100 – 120 mls/kg x 2/3
Single blood volume exchange for anaemia: Term infant – 80 -100mls /kg Preterm infant – 100mls/kg Volume exchanged (ml) = Wt (kg) x Blood Volume
x (Hb desired – Hb initial)
The volume of blood required
'PUSH-PULL METHOD’ via the umbilical vein.- Serial withdrawal and injection of aliquots (5-20 mls) – 1 minute for each cycle. Takes 60 – 120 minutes.- Used when arterial arterial access is a problem.
‘ISOVOLUMETRIC METHOD’ - slow removal of aliquots (10mls usually) from an artery (central or peripheral) and simultaneous infusion into a vein (central or peripheral). - preferred method- Does not cause wide fluctuations of blood volume and pressure. - Takes 60 – 90 minutes
Procedure
Exchange transfusion

Infection
Thrombocytopenia
Volume over load
GVHD
NEC
Portal vein thrombosis
Electrolytes disturbance
Cardic arrhythmias
Sudden death
Complication of exchange transfusion
Early recognition and treatment of hyperbilirubinemia prevents severe brain damage.
Complication ;
-Chronic bilirubin encephalopathy (Kernicterus)
Prognosis ??
Lipid-soluble, unconjugated, indirect bilirubin fraction is toxic to the developing central nervous system, especially when indirect bilirubin concentrations are high and exceed the binding capacity of albumin.
Kernicterus results when indirect bilirubin is deposited in brain cells and disrupts neuronal metabolism and function, especially in the basal ganglia. Indirect bilirubin may cross the blood-brain barrier because of its lipid solubility.
What is Kernicterus …?
Kernicterus usually is noted when the bilirubinlevel is excessively high for gestational age. It develop in term infants when bilirubin levels exceed 25 mg/dL
. Kernicterus may be noted at bilirubin levels less than 20 mg/dL in the presence of sepsis, meningitis, hemolysis, asphyxia, hypoxia, hypothermia, hypoglycemia, bilirubin-displacing drugs (sulfa drugs), and prematurity
Other risks for kernicterus in term infants are hemolysis, jaundice noted within 24 hours of birth, and delayed diagnosis of hyperbilirubinemia.
Kernicterus has developed in extremely immature infants weighing less than 1000 g when bilirubinlevels are less than 10 mg/dL because of a more permeable blood-brain barrier associated with prematurity
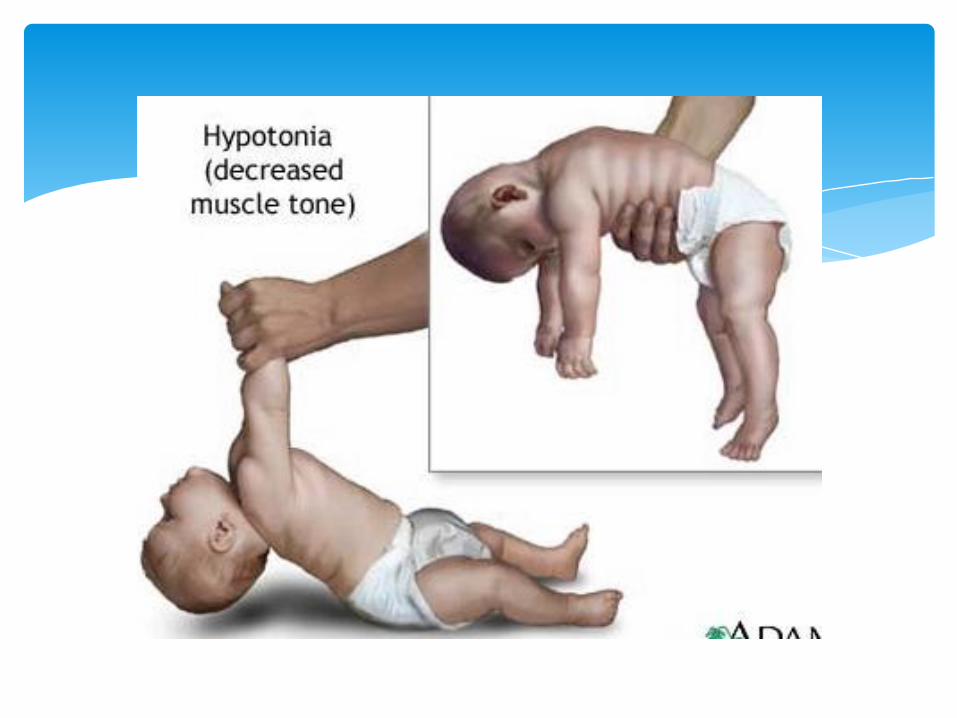
The earliest clinical manifestations of kernicterus are lethargy, hypotonia, irritability, poor Moro response, poor feeding and high-pitched cry.
Early signs are noted after day 4 of life.
Later signs include bulging fontanelle, opisthotonic posturing, pulmonary hemorrhage, fever, hypertonicity, paralysis of upward gaze, and seizures.Infants with severe cases of kernicterus die in the neonatal period. Spasticity resolves in surviving infants, who may manifest later nerve deafness, choreoathetoid cerebral palsy, mental retardation, enamel dysplasia, and discoloration of teeth as permanent sequelae
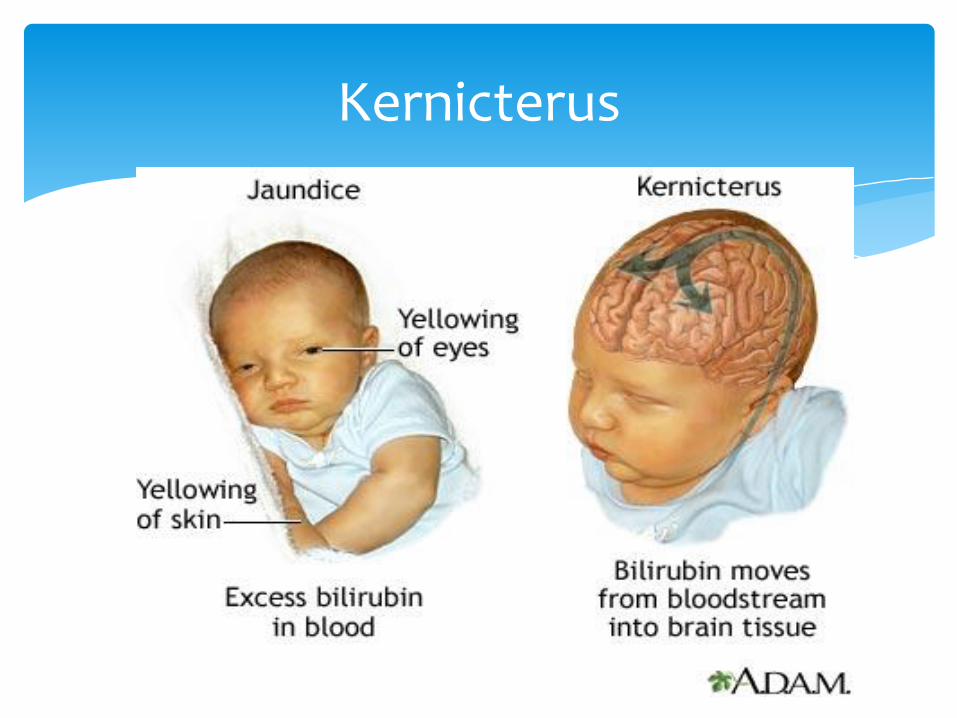
Kernicterus