superficial bacterial infection
TRANSCRIPT

DE-SP/0411/02
BACTERIAL SKIN INFECTIONS
DE-SP/0411/02
DE-SP/0411/02
■ Bacterial skin infections (Pyodermas)Classification
Non – follicular pyodermas: Impetigo, ecthyma, erysipelas, cellulitis
Follicular pyodermas: Folliculitis, furunculosis, carbuncle
Treatment
■ Superficial Fungal skin infectionsPredisposing factors
DermatophytosisAnti-fungal drugs
Pityriasis versicolor
Cutaneous candidiasis
2 Overview
DE-SP/0411/02
BACTERIAL SKIN INFECTIONS OR PYODERMAS

DE-SP/0411/02
PYODERMA: Types
PYODERMAPYODERMA
SECONDARY (to underlying
disease)
PRIMARY
ScabiesScabies
Miliaria/Prickly heatMiliaria/Prickly heat
Eczema/DermatitisEczema/Dermatitis
Fungal infectionFungal infection
PediculosisPediculosis
4
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
DE-SP/0411/02
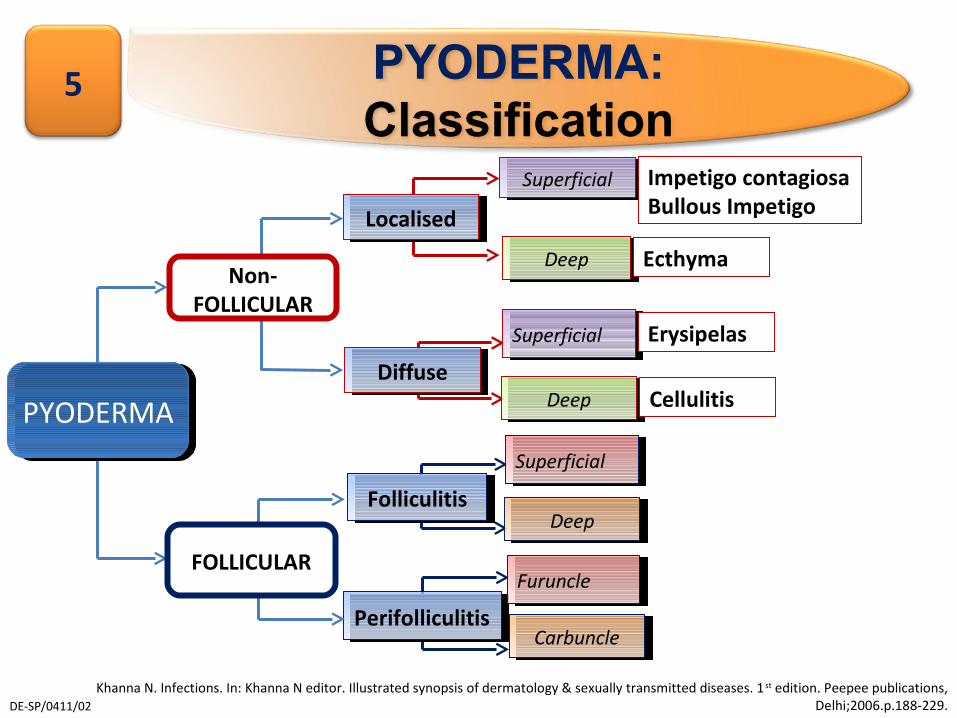
PYODERMA: Classification
5
DiffuseDiffuse
LocalisedLocalised
SuperficialSuperficial
PerifolliculitisPerifolliculitis
SuperficialSuperficial
DeepDeep
PYODERMAPYODERMA
Non-FOLLICULAR
FOLLICULAR
Impetigo contagiosa Bullous Impetigo
Ecthyma
Erysipelas
DeepDeep Cellulitis
SuperficialSuperficial
DeepDeepFolliculitisFolliculitis
FuruncleFuruncle
CarbuncleCarbuncle
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.

DE-SP/0411/02
PYODERMAS: NON FOLLICULAR

DE-SP/0411/02
Impetigo
Risk factors3
■ Gram-positive bacterial infection of superficial epidermal layers1
■ Highly contagious - Organisms often pass from one individual to another by direct hand contact 2
■ Accounts for 10% of skin diseases treated in pediatric clinics in US2
Classification
■ Nonbullous impetigo
(Impetigo contagiosa)■ Bullous impetigo
7
hot, humid weather crowded living conditions poor hygieneimmunosuppression Nasal carriage of S. aureus: important factor in recurrent infections
1. Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3 rd ed. India:Bhalani Publishing House;1994.p.223-251.2. Available at http://emedicine.medscape.com/article/1052709-overview#a0199. Accessed on 21/04/11
3. Popovich D. Accurately Diagnosing Commonly Misdiagnosed Circular Rashes. Pediatr Nurs. 2007;33(4):315-320.

DE-SP/0411/02
Non Bullous or
Impetigo contagiosaAccounts for 70% cases of impetigo
Caused by S.aureus & S.pyogenes
Clinical presentation■ Commonly seen in children aged 2 to 5
years■ Appearance: Multiple honey colored
crusted lesions with a ring of erythema.
■ Site: Predominantly face (especially around mouth & nose)
■ Constitutional symptoms: fever, regional lymphadenopathy.
Complications■ Post streptococcal glomerulonephritis
in patients infected with nephritogenic strains
8
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.

DE-SP/0411/02
Bullous Impetigo
Caused by S.aureus
Clinical presentation■ Commonly seen in infants■ Appearance: Bullae with turbid
collection of fluid without a erythematous ring rupture to form thin crusts. Heal in centre to form annular lesions.
■ Predominant site - face but any part of body including mucous membranes may be involved.
■ Constitutional symptoms & lymphadenopathy : Rare
Complications■ Rare
9
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
DE-SP/0411/02
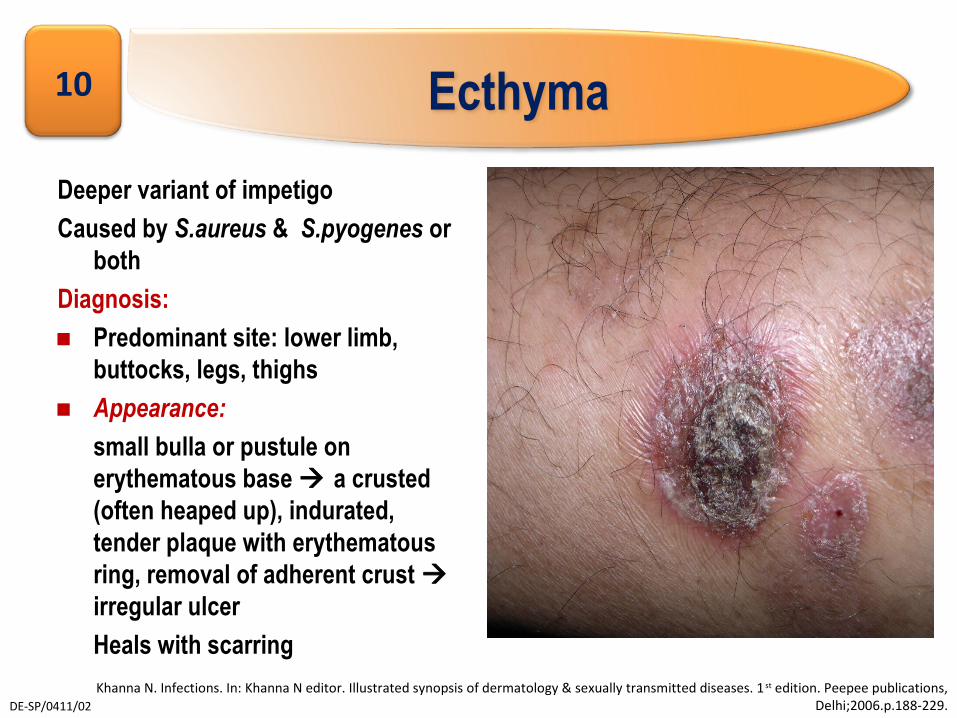
Ecthyma
Deeper variant of impetigo
Caused by S.aureus & S.pyogenes or both
Diagnosis:■ Predominant site: lower limb,
buttocks, legs, thighs■ Appearance:
small bulla or pustule on erythematous base a crusted (often heaped up), indurated, tender plaque with erythematous ring, removal of adherent crust irregular ulcer
Heals with scarring
10
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
DE-SP/0411/02
Erysipelas
Superficial streptococcal infection extending into cutaneous lymphatics
CLINICAL PRESENTATION:■ Predisposing factors: Recent streptococcal infection, HIV infection,
diabetes, alcohol abuse, nephrotic syndrome, or preexisting lymphedema
■ Appearance: small erythematous, warm patch indurated tense,shiny plaque with sharply demarcated margins, superficial vesiculation may occur. Rapidly spreads through lymphatics skin "streaking," regional lymph node swelling, tenderness
COMPLICATIONS■ Recurrent infections may cause disfiguring & disabling healing
reactions
11
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
DE-SP/0411/02
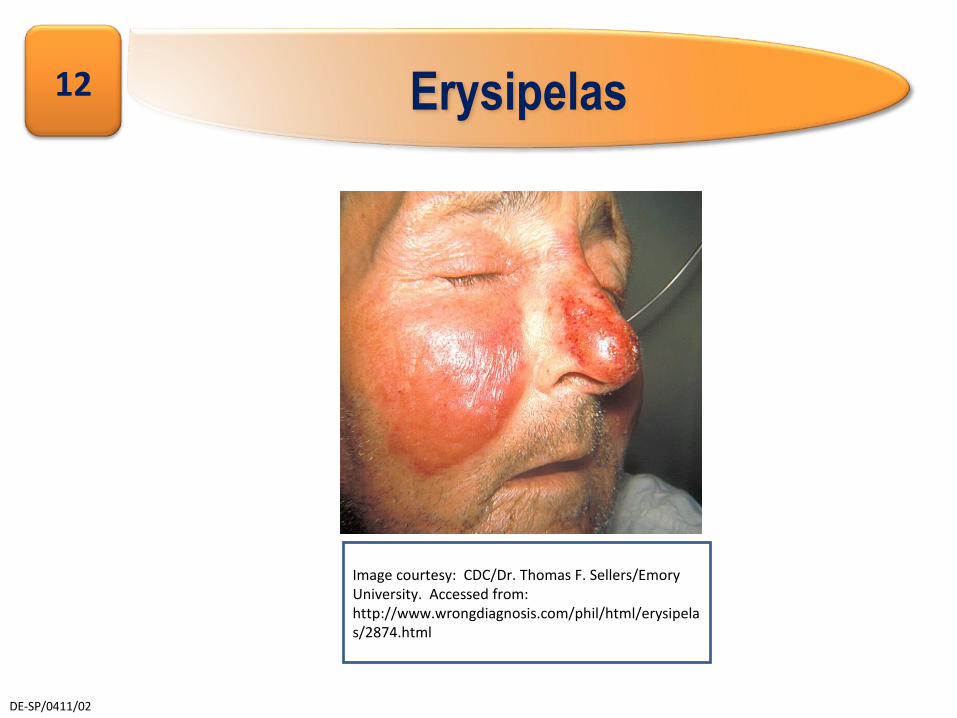
Erysipelas12
Image courtesy: CDC/Dr. Thomas F. Sellers/Emory University. Accessed from: http://www.wrongdiagnosis.com/phil/html/erysipelas/2874.html

DE-SP/0411/02
Cellulitis
■ Deeper variant of erysipelas involving the deeper subcutaneous tissue.1
■ Predisposing factor: occult diabetes2
■ Lesions: are ill-defined with indistinct borders
13
1. Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
2.Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3rd ed. India:Bhalani Publishing House;1994.p.223-251.

DE-SP/0411/02
PYODERMAS - FOLLICULAR
DE-SP/0411/02
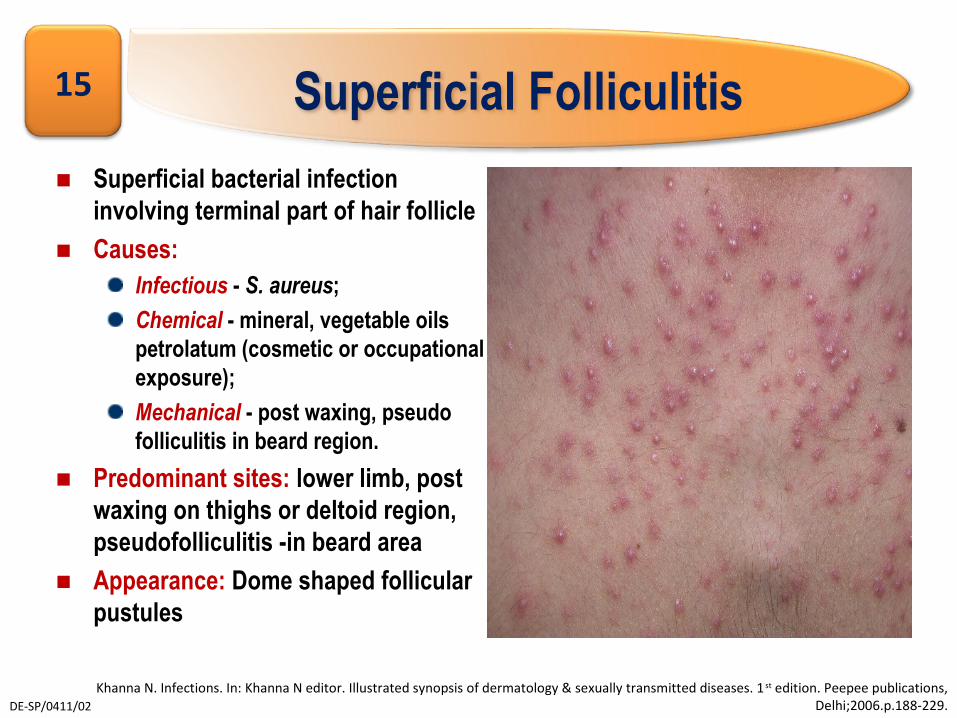
Superficial Folliculitis
■ Superficial bacterial infection involving terminal part of hair follicle
■ Causes: Infectious - S. aureus;
Chemical - mineral, vegetable oils petrolatum (cosmetic or occupational exposure);
Mechanical - post waxing, pseudo folliculitis in beard region.
■ Predominant sites: lower limb, post waxing on thighs or deltoid region, pseudofolliculitis -in beard area
■ Appearance: Dome shaped follicular pustules
15
Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.

DE-SP/0411/02
Deep Folliculitis1,2
■ Deeper variant of folliculitis involving whole depth of hair follicle■ Causative organism: S.aureus
Clinical presentation■ Occurs commonly in males 20-40 years of age
■ Predominant sites: beard area (sycosis barbae) especially on upper lip & below angles of mouth, scalp & nape of neck (sycosis nuchae)
■ Appearance: Deep seated erythematous perifollicular papules & pustules. Lesion heals with scarring
16
1. Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
2.Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3rd ed. India:Bhalani Publishing House;1994.p.223-251.
DE-SP/0411/02
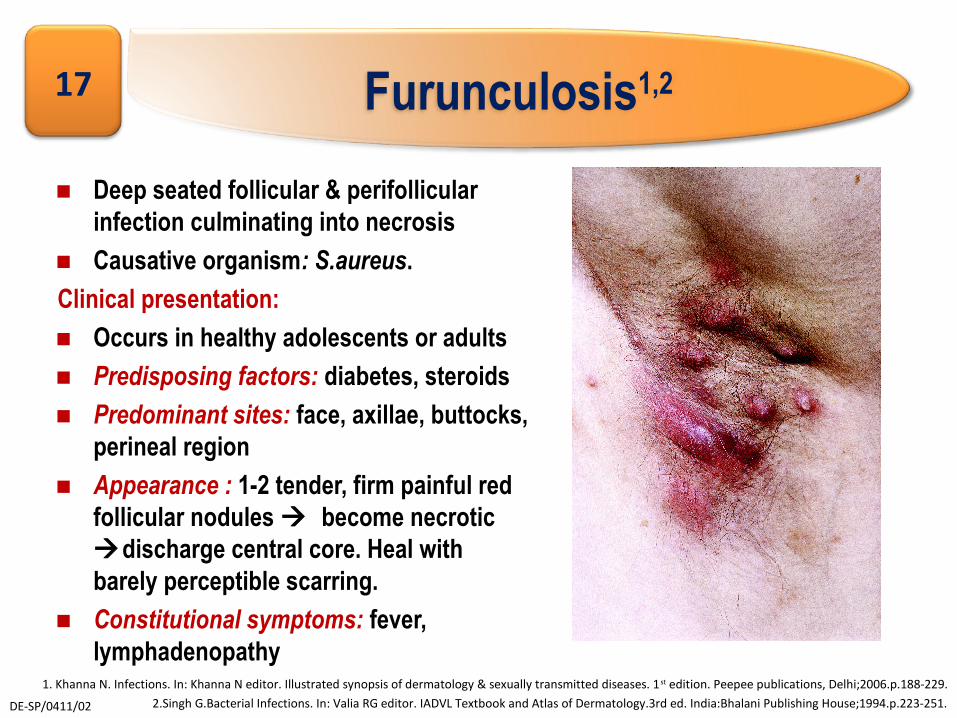
Furunculosis1,2
■ Deep seated follicular & perifollicular infection culminating into necrosis
■ Causative organism: S.aureus.
Clinical presentation:■ Occurs in healthy adolescents or adults■ Predisposing factors: diabetes, steroids ■ Predominant sites: face, axillae, buttocks,
perineal region■ Appearance : 1-2 tender, firm painful red
follicular nodules become necrotic discharge central core. Heal with barely perceptible scarring.
■ Constitutional symptoms: fever, lymphadenopathy
17
1. Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
2.Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3rd ed. India:Bhalani Publishing House;1994.p.223-251.

DE-SP/0411/02
Carbuncle1,2
■ Deep infection of contiguous hair follicles
■ Causative organism: S.aureus.Clinical presentation:■ Occurs mostly in adults with
diabetes or on steroid therapy ■ Predominant site: back■ Appearance : Tender, indurated,
lobulated, intensely erythematous plaque discharging pus from many openings.
■ Constitutional symptoms: fever, invariable.
■ Diagnosis: pus culture sensitivity
18
1. Khanna N. Infections. In: Khanna N editor. Illustrated synopsis of dermatology & sexually transmitted diseases. 1 st edition. Peepee publications, Delhi;2006.p.188-229.
2.Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3rd ed. India:Bhalani Publishing House;1994.p.223-251.

DE-SP/0411/02
TREATMENT OF BACTERIAL SKIN INFECTIONS

DE-SP/0411/02
Bacterial skin infections: Treatment1
■ Identification & elimination of predisposing factors like immunosuppresion, malnutrition, diabetes
■ Local hygiene is important & should be maintained
Encourage hand washing2
■ Supportive measures
Removal of crusts
Hot fomentation
Incision & drainage
Rest & limb elevation
Concomitant use of oral or topical anti inflammatory creams to relieve pain & inflammation
20
1. Singh G.Bacterial Infections. In: Valia RG editor. IADVL Textbook and Atlas of Dermatology.3rd ed. India:Bhalani Publishing House;1994.p.223-251.
2. . Popovich D. Accurately Diagnosing Commonly Misdiagnosed Circular Rashes. Pediatr Nurs. 2007;33(4):315-320.

DE-SP/0411/02
Bacterial skin infections: Treatment
■ Topical or oral antibiotic therapy is the treatment of choice ■ Localized areas are treated with antibacterial applications having a gram
positive spectrum such as:
2% Mupirocin cream or ointment, applied 2-3 times a day
2% Sodium fusidate or fusidic acid cream /ointment, 3-4 times a day
1% Nadifloxacin cream
■ Role of oral antibiotics
When widespread or deep infection is present or
If localized lesions do not improve with topical medication
Penicillinase-stable penicillins like cloxacillin, dicloxacillin are effective including erythromycin, azithromycin, cephalosporins
21
Popovich D. Accurately Diagnosing Commonly Misdiagnosed Circular Rashes. Pediatr Nurs. 2007;33(4):315-320.
DE-SP/0411/02
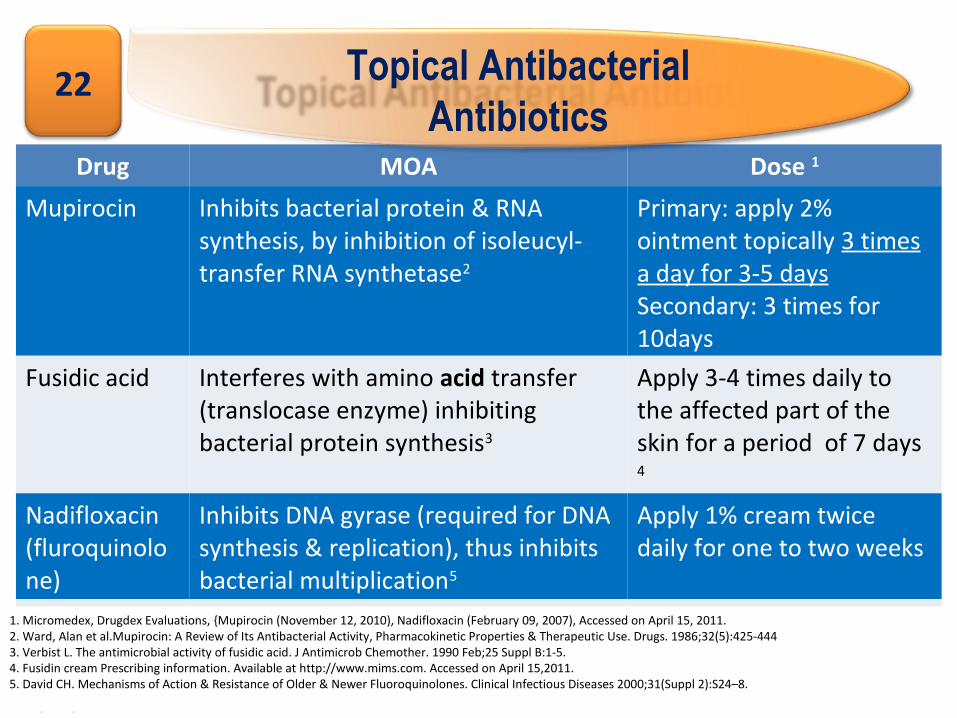
Drug MOA Dose 1
Mupirocin Inhibits bacterial protein & RNA synthesis, by inhibition of isoleucyl-transfer RNA synthetase2
Primary: apply 2% ointment topically 3 times a day for 3-5 daysSecondary: 3 times for 10days
Fusidic acid Interferes with amino acid transfer (translocase enzyme) inhibiting bacterial protein synthesis3
Apply 3-4 times daily to the affected part of the skin for a period of 7 days 4
Nadifloxacin(fluroquinolone)
Inhibits DNA gyrase (required for DNA synthesis & replication), thus inhibits bacterial multiplication5
Apply 1% cream twice daily for one to two weeks
Topical Antibacterial Antibiotics
22
1. Micromedex, Drugdex Evaluations, {Mupirocin (November 12, 2010), Nadifloxacin (February 09, 2007), Accessed on April 15, 2011.2. Ward, Alan et al.Mupirocin: A Review of Its Antibacterial Activity, Pharmacokinetic Properties & Therapeutic Use. Drugs. 1986;32(5):425-4443. Verbist L. The antimicrobial activity of fusidic acid. J Antimicrob Chemother. 1990 Feb;25 Suppl B:1-5.4. Fusidin cream Prescribing information. Available at http://www.mims.com. Accessed on April 15,2011. 5. David CH. Mechanisms of Action & Resistance of Older & Newer Fluoroquinolones. Clinical Infectious Diseases 2000;31(Suppl 2):S24–8.
DE-SP/0411/02
Summary
■ Bacterial infections of the skin could occur de novo or may secondarily infect pre-existing dermatoses
■ Commonly seen in pediatric population and adolescents but can affect all age groups
■ Common pathogens implicated are gram positive cocci (staphylococcus aureus & streptococci)
■ Clinical presentation varies with the site & depth of involvement
■ Treatment is with topical antibacterial agents; systemic antibiotics added for extensive infections, deep seated infections & for infections not improving with topical antibacterial agents
23
DE-SP/0411/02
“Disclaimer This educational initiative supported by GlaxoSmithKline Pharmaceuticals
Limited & prepared by Rayz Healthcare Consultancy (lead consultant - Dr. Gulrez Tyebkhan) is meant strictly & solely for presentations amongst Registered Medical Practitioners in India.
Although great care has been taken in compiling & checking the information, the sponsor GlaxoSmithKline Pharmaceuticals Limited shall not be held responsible or liable for errors, omissions or inaccuracies in this Slide Deck, whether arising from negligence or otherwise, nor for consequences arising therefrom.”
24
DE-SP/0411/02
Abbreviated prescribing information – T Bact ointment
■ T-bact Ointment (Mupirocin)
Composition: Mupirocin 2% w/w in a white, translucent water soluble polyethylene glycol base. Indications: For the topical treatment of primary skin infections such as impetigo, folliculitis, furunculosis and ecthyma and secondary bacterial skin infections such as infected dermatosis (e.g., infected eczema), infected traumatic lesions (e.g., abrasions, insect bites, minor wounds and minor burns). For prophylaxis: May be used to avoid bacterial contamination of small wounds, incisions and other clean lesions, and to prevent infection of abrasions and small cuts and wounds. Dosage and administration: Adults, children, elderly and hepatic impairment: 2-3 times a day for up to 10 days, depending on the response. Contraindications: Known hypersensitivity to any of its constituents. Warnings and precautions: Avoid contact with eyes, or use in conjunction with cannulae. If contaminated, the eyes should be thoroughly irrigated with water until the ointment residues have been removed. Do not use intranasally. Do not use in conditions where absorption of large quantities of polyethylene glycol is possible, especially if there is evidence of moderate or severe renal impairment. Interactions: No drug interactions have been reported. Pregnancy and lactation: Adequate human data on use during pregnancy and lactation are not available. However, animal studies have not identified any risk to pregnancy or embryo-foetal development. If a cracked nipple is to be treated, it should be thoroughly washed prior to breast feeding. Use in pregnancy or nursing mothers only when potential benefits outweigh potential risks. Undesirable effects: Burning, itching, erythema, stinging and dryness localised to the area of application, cutaneous sensitisation reactions and very rarely systemic allergic reactions. Version: TBTO/API/IN/2004/006AOC v01 dated 26-Nov-08. Adapted from Indian Prescribing Information Version 006 / IND 04.
25

DE-SP/0411/02
GlaxoSmithKline Pharmaceuticals Ltd Dr Annie Besant Road, Worli, Mumbai-30
For the use only of a Registered Medical Practitioner
DE-
SP/0
411/
02