summary of benefits - medicare insurance program of benefits for empire mediblue plussm ... you may...
TRANSCRIPT

Summary of Benefitsfor Empire MediBlue PlusSM (HMO)
Available in Suffolk County in New York
This plan is an HMO plan with a Medicare contract. Services provided by Empire HealthChoice HMO,Inc. licensee of the Blue Cross and Blue Shield Association, an association of independent Blue Cross andBlue Shield plans.
Y0071_12_12913_T_031 CMS Approved 09/15/2011 23461MUSENMUB_031H3370 004 NY HMO

Section I:
Introduction to the Summary of BenefitsThank you for your interest in Empire MediBlue Plus (HMO). Our plan is offered by Empire HealthChoice HMO,Inc., a Medicare Advantage Health Maintenance Organization (HMO). This Summary of Benefits tells you somefeatures of our plan. It doesn't list every service that we cover or list every limitation or exclusion. To get a completelist of our benefits, please call Empire MediBlue Plus (HMO) and ask for the "Evidence of Coverage".
You Have Choices in Your Health CareAs a Medicare beneficiary, you can choose from differentMedicare options. One option is the Original(fee-for-service) Medicare Plan. Another option is aMedicare health plan, like Empire MediBlue Plus(HMO). You may have other options too. You make thechoice. No matter what you decide, you are still in theMedicare Program.
You may join or leave a plan only at certain times. Pleasecall Empire MediBlue Plus (HMO) at the telephonenumber listed at the end of this introduction or1-800-MEDICARE (1-800-633-4227) for moreinformation. TTY/TDD users should call1-877-486-2048. You can call this number 24 hours aday, 7 days a week.
How Can I Compare My Options?You can compare Empire MediBlue Plus (HMO) andthe Original Medicare Plan using this Summary ofBenefits. The charts in this booklet list some importanthealth benefits. For each benefit, you can see what ourplan covers and what the Original Medicare Plan covers.
Our members receive all of the benefits that the OriginalMedicare Plan offers. We also offer more benefits, whichmay change from year to year.
Where Is Empire MediBlue Plus (HMO)Available?The service area for this plan includes the followingcounties:
Suffolk county, NY.
You must live in this area to join the plan.
Who Is Eligible to Join Empire MediBluePlus (HMO)?You can join Empire MediBlue Plus (HMO) if you areentitled to Medicare Part A and enrolled in MedicarePart B and live in the service area. However, individualswith End-Stage Renal Disease are generally not eligibleto enroll in Empire MediBlue Plus (HMO) unless theyare members of our organization and have been sincetheir dialysis began.
Can I Choose My Doctors?Empire MediBlue Plus (HMO) has formed a networkof doctors, specialists, and hospitals. You can only usedoctors who are part of our network. The health providersin our network can change at any time.
You can ask for a current provider directory. For anupdated list, visit us at www.empireblue.com/medicare.Our customer service number is listed at the end of thisintroduction.
What Happens If I Go to a Doctor Who'sNot in Your Network?If you choose to go to a doctor outside of our network,you must pay for these services yourself except in limitedsituations (for example, emergency care). Neither theplan nor the Original Medicare Plan will pay for theseservices
Page 2 – Empire MediBlue Plus (HMO)

Where Can I Get My Prescriptions If IJoin this plan?Empire MediBlue Plus (HMO) has formed a networkof pharmacies. You must use a network pharmacy toreceive plan benefits. We may not pay for yourprescriptions if you use an out-of-network pharmacy,except in certain cases. The pharmacies in our networkcan change at any time. You can ask for a pharmacydirectory or visit us at www.empireblue.com/medicare.Our customer service number is listed at the end of thisintroduction.
Does My Plan Cover Medicare Part Bor Part D Drugs?Empire MediBlue Plus (HMO) does cover both MedicarePart B prescription drugs and Medicare Part Dprescription drugs.
What Is a Prescription Drug Formulary?Empire MediBlue Plus (HMO) uses a formulary. Aformulary is a list of drugs covered by your plan to meetpatient needs. We may periodically add, remove, or makechanges to coverage limitations on certain drugs or changehow much you pay for a drug. If we make any formularychange that limits our members' ability to fill theirprescriptions, we will notify the affected enrollees beforethe change is made. We will send a formulary to you andyou can see our complete formulary on our Web site atwww.empireblue.com/medicare.
If you are currently taking a drug that is not on ourformulary or subject to additional requirements or limits,you may be able to get a temporary supply of the drug.You can contact us to request an exception or switch toan alternative drug listed on our formulary with yourphysician's help. Call us to see if you can get a temporarysupply of the drug or for more details about our drugtransition policy.
How Can I Get Extra Help With MyPrescription Drug Plan Costs or GetExtra Help With Other Medicare Costs?You may be able to get extra help to pay for yourprescription drug premiums and costs as well as get helpwith other Medicare costs. To see if you qualify forgetting extra help, call:
* 1-800-MEDICARE (1-800-633-4227). TTY/TDDusers should call 1-877-486-2048, 24 hours a day/7 daysa week and see www.medicare.gov 'Programs for Peoplewith Limited Income and Resources' in the publicationMedicare & You.
* The Social Security Administration at 1-800-772-1213between 7 a.m. and 7 p.m., Monday through Friday.TTY/TDD users should call 1-800-325-0778 or
* Your State Medicaid Office.
What Are My Protections in this plan?All Medicare Advantage Plans agree to stay in theprogram for a full calendar year at a time. Plan benefitsand cost-sharing may change from calendar year tocalendar year. Each year, plans can decide whether tocontinue to participate with Medicare Advantage. A planmay continue in their entire service area (geographic areawhere the plan accepts members) or choose to continueonly in certain areas. Also, Medicare may decide to enda contract with a plan. Even if your Medicare AdvantagePlan leaves the program, you will not lose Medicarecoverage. If a plan decides not to continue for anadditional calendar year, it must send you a letter at least90 days before your coverage will end. The letter willexplain your options for Medicare coverage in your area.
As a member of Empire MediBlue Plus (HMO), youhave the right to request an organization determination,which includes the right to file an appeal if we denycoverage for an item or service, and the right to file agrievance. You have the right to request an organizationdetermination if you want us to provide or pay for anitem or service that you believe should be covered. If wedeny coverage for your requested item or service, youhave the right to appeal and ask us to review our decision.You may ask us for an expedited (fast) coveragedetermination or appeal if you believe that waiting for a
Page 3 – Empire MediBlue Plus (HMO)

decision could seriously put your life or health at risk, oraffect your ability to regain maximum function. If yourdoctor makes or supports the expedited request, we mustexpedite our decision. Finally, you have the right to filea grievance with us if you have any type of problem withus or one of our network providers that does not involvecoverage for an item or service. If your problem involvesquality of care, you also have the right to file a grievancewith the Quality Improvement Organization (QIO) foryour state. Please refer to the Evidence of Coverage(EOC) for the QIO contact information.
As a member of Empire MediBlue Plus (HMO), youhave the right to request a coverage determination, whichincludes the right to request an exception, the right tofile an appeal if we deny coverage for a prescription drug,and the right to file a grievance. You have the right torequest a coverage determination if you want us to covera Part D drug that you believe should be covered. Anexception is a type of coverage determination. You mayask us for an exception if you believe you need a drugthat is not on our list of covered drugs or believe youshould get a non-preferred drug at a lower out-of-pocketcost. You can also ask for an exception to cost utilizationrules, such as a limit on the quantity of a drug. If youthink you need an exception, you should contact usbefore you try to fill your prescription at a pharmacy.Your doctor must provide a statement to support yourexception request. If we deny coverage for yourprescription drug(s), you have the right to appeal and askus to review our decision. Finally, you have the right tofile a grievance if you have any type of problem with usor one of our network pharmacies that does not involvecoverage for a prescription drug. If your problem involvesquality of care, you also have the right to file a grievancewith the Quality Improvement Organization (QIO) foryour state. Please refer to the Evidence of Coverage(EOC) for the QIO contact information.
What Is a Medication TherapyManagement (MTM) Program?A Medication Therapy Management (MTM) Programis a free service we offer. You may be invited to participatein a program designed for your specific health andpharmacy needs. You may decide not to participate but
it is recommended that you take full advantage of thiscovered service if you are selected. Contact EmpireMediBlue Plus (HMO) for more details.
What Types of Drugs May Be CoveredUnder Medicare Part B?Some outpatient prescription drugs may be covered underMedicare Part B. These may include, but are not limitedto, the following types of drugs. Contact EmpireMediBlue Plus (HMO) for more details.
Some Antigens: If they are prepared by a doctor andadministered by a properly instructed person (whocould be the patient) under doctor supervision.Osteoporosis Drugs: Injectable drugs for osteoporosisfor certain women with Medicare.Erythropoietin (Epoetin Alfa or Epogen®): Byinjection if you have end-stage renal disease(permanent kidney failure requiring either dialysis ortransplantation) and need this drug to treat anemia.Hemophilia Clotting Factors: Self-administeredclotting factors if you have hemophilia.Injectable Drugs: Most injectable drugs administeredincident to a physician's service.Immunosuppressive Drugs: Immunosuppressive drugtherapy for transplant patients if the transplant waspaid for by Medicare, or paid by a private insurancethat paid as a primary payer to your Medicare Part Acoverage, in a Medicare-certified facility.Some Oral Cancer Drugs: If the same drug is availablein injectable form.Oral Anti-Nausea Drugs: If you are part of ananti-cancer chemotherapeutic regimen.Inhalation and Infusion Drugs administered throughDME.
Where Can I Find Information On PlanRatings?The Medicare program rates how well plans perform indifferent categories (for example, detecting and preventingillness, ratings from patients and customer service). Ifyou have access to the web, you may use the web toolson www.medicare.gov and select "Health and DrugPlans" then "Compare Drug and Health Plans" to
Page 4 – Empire MediBlue Plus (HMO)

compare the Plan Ratings for Medicare plans in yourarea. You can also call us directly to obtain a copy of the
Plan Ratings for this plan. Our customer service numberis listed below.
Please call Empire BlueCross BlueShield for more information about EmpireMediBlue Plus (HMO).
Prospective members should call locally forquestions related to the Medicare Advantageprogram or the Medicare Part D Prescription Drugprogram. 1-800-809-7328 (TTY/TDD 711)
Visit us at www.empireblue.com/medicare or, callus:
Customer Service Hours: Sunday, Monday, Tuesday,Wednesday, Thursday, Friday, Saturday, 8:00 a.m. -8:00 p.m. Eastern For more information about Medicare, please call
Medicare at 1-800-MEDICARE (1-800-633-4227).TTY users should call 1-877-486-2048. You can call24 hours a day, 7 days a week.
Current members should call toll-free for questionsrelated to the Medicare Advantage program or theMedicare Part D Prescription Drugprogram. 1-800-499-9554 (TTY/TDD 711) Or, visit www.medicare.gov on the Web.
Prospective members should call toll-free forquestions related to the Medicare Advantageprogram or the Medicare Part D Prescription Drugprogram. 1-800-809-7328 (TTY/TDD 711).
This document may be available in other formats suchas Braille, large print or other alternate formats.
This document may be available in a non-Englishlanguage. For additional information, call customerservice at the phone number listed above.Current members should call locally for questions
related to the Medicare Advantage program or theMedicare Part D Prescription Drug program.1-800-499-9554 (TTY/TDD 711)
Esta información está disponible en otros idiomas demanera gratuita. Comuníquese con el número denuestro Servicio de Atención al Cliente al1-800-499-9554 (o a la línea TTY/TDD al 711) de8 a. m. a 8 p. m., los 7 días de la semana, hasta el 14de febrero de 2012, para obtener informaciónadicional.*
* A partir del 15 de febrero de 2012, puede llamar alServicio de Atención al Cliente al 1-800-499-9554 (o ala línea TTY/TDD al 711) de 8 a. m. a 8 p. m., de lunesa viernes, excepto feriados.
Page 5 – Empire MediBlue Plus (HMO)
If you have any questions about this plan's benefits or costs, please contact Empire BlueCross BlueShield fordetails
Section II:
Summary of BenefitsEmpire MediBlue Plus (HMO)Original MedicareBenefit
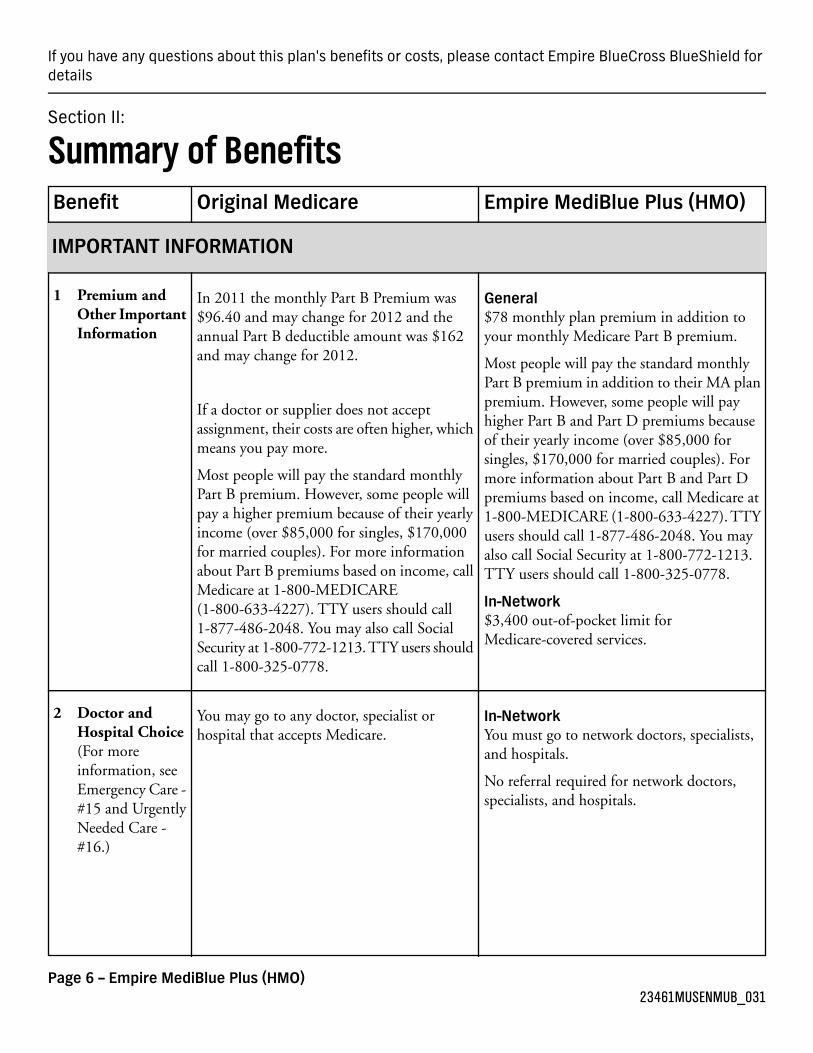
IMPORTANT INFORMATION
General$78 monthly plan premium in addition toyour monthly Medicare Part B premium.
In 2011 the monthly Part B Premium was$96.40 and may change for 2012 and theannual Part B deductible amount was $162and may change for 2012.
1 Premium andOther ImportantInformation
Most people will pay the standard monthlyPart B premium in addition to their MA planpremium. However, some people will payIf a doctor or supplier does not accept
assignment, their costs are often higher, whichmeans you pay more.
higher Part B and Part D premiums becauseof their yearly income (over $85,000 forsingles, $170,000 for married couples). For
Most people will pay the standard monthlyPart B premium. However, some people will
more information about Part B and Part Dpremiums based on income, call Medicare at
pay a higher premium because of their yearly 1-800-MEDICARE (1-800-633-4227). TTYincome (over $85,000 for singles, $170,000 users should call 1-877-486-2048. You mayfor married couples). For more information also call Social Security at 1-800-772-1213.
TTY users should call 1-800-325-0778.about Part B premiums based on income, callMedicare at 1-800-MEDICARE
In-Network$3,400 out-of-pocket limit forMedicare-covered services.
(1-800-633-4227). TTY users should call1-877-486-2048. You may also call SocialSecurity at 1-800-772-1213. TTY users shouldcall 1-800-325-0778.
In-NetworkYou must go to network doctors, specialists,and hospitals.
You may go to any doctor, specialist orhospital that accepts Medicare.
2 Doctor andHospital Choice(For moreinformation, seeEmergency Care -#15 and UrgentlyNeeded Care -#16.)
No referral required for network doctors,specialists, and hospitals.
Page 6 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
SUMMARY OF BENEFITS
Inpatient Care
In-NetworkNo limit to the number of days covered bythe plan each hospital stay.
In 2011 the amounts for each benefit periodwere:
3 InpatientHospital Care(includesSubstance AbuseandRehabilitationServices)
Days 1 - 60: $1132 deductibleFor Medicare-covered hospital stays:Days 61 - 90: $283 per day
Days 91 - 150: $566 per lifetime reserveday
Days 1 - 7: $175 copay per dayDays 8 - 90: $0 copay per day
These amounts may change for 2012. $0 copay for additional hospital daysCall 1-800-MEDICARE (1-800-633-4227)for information about lifetime reserve days.
Except in an emergency, your doctor must tellthe plan that you are going to be admitted tothe hospital.Lifetime reserve days can only be used once.
A "benefit period" starts the day you go intoa hospital or skilled nursing facility. It endswhen you go for 60 days in a row withouthospital or skilled nursing care. If you go intothe hospital after one benefit period has ended,a new benefit period begins. You must pay theinpatient hospital deductible for each benefitperiod. There is no limit to the number ofbenefit periods you can have.
In-NetworkYou get up to 190 days of inpatient psychiatrichospital care in a lifetime. Inpatient psychiatric
In 2011 the amounts for each benefit periodwere:
4 Inpatient MentalHealth Care
Days 1 - 60: $1132 deductiblehospital services count toward the 190-dayDays 61 - 90: $283 per daylifetime limitation only if certain conditions
Days 91 - 150: $566 per lifetime reserveday
are met. This limitation does not apply toinpatient psychiatric services furnished in ageneral hospital.These amounts may change for 2012.
You get up to 190 days of inpatient psychiatrichospital care in a lifetime. Inpatient psychiatric
For Medicare-covered hospital stays:
Days 1 - 7: $175 copay per dayhospital services count toward the 190-daylifetime limitation only if certain conditions Days 8 - 90: $0 copay per dayare met. This limitation does not apply to Except in an emergency, your doctor must tell
the plan that you are going to be admitted tothe hospital.
inpatient psychiatric services furnished in ageneral hospital.
Page 7 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
GeneralAuthorization rules may apply.
In 2011 the amounts for each benefit periodafter at least a 3-day covered hospital stay were:
5 Skilled NursingFacility (SNF)(in aMedicare-certifiedskilled nursingfacility)
In-NetworkPlan covers up to 100 days each benefit period
No prior hospital stay is required.
For SNF stays:
Days 1 - 20: $0 per dayDays 21 - 100: $141.50 per day
These amounts may change for 2012.
100 days for each benefit period.
A "benefit period" starts the day you go intoa hospital or SNF. It ends when you go for 60
Days 1 - 100: $60 copay per day
days in a row without hospital or skillednursing care. If you go into the hospital afterone benefit period has ended, a new benefitperiod begins. You must pay the inpatienthospital deductible for each benefit period.There is no limit to the number of benefitperiods you can have.
GeneralAuthorization rules may apply.
$0 copay.6 Home HealthCare(includesmedicallynecessaryintermittentskilled nursingcare, home healthaide services, andrehabilitationservices, etc.)
In-Network$0 copay for each Medicare-covered homehealth visit
GeneralYou must get care from a Medicare-certifiedhospice. Your plan will pay for a consultativevisit before you select hospice.
You pay part of the cost for outpatient drugsand inpatient respite care.
You must get care from a Medicare-certifiedhospice.
7 Hospice
OUTPATIENT CARE
In-Network$15 copay for each primary care doctor visitfor Medicare-covered benefits.
20% coinsurance8 Doctor OfficeVisits
$25 copay for each in-area, network urgentcare Medicare-covered visit
Page 8 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
$25 copay for each specialist visit forMedicare-covered benefits.
GeneralAuthorization rules may apply.
Supplemental routine care not covered
20% coinsurance for manual manipulation ofthe spine to correct subluxation (a
9 ChiropracticServices
In-Network$20 copay for each Medicare-covered visitdisplacement or misalignment of a joint or
body part) if you get it from a chiropractor orother qualified providers.
Medicare-covered chiropractic visits are formanual manipulation of the spine to correctsubluxation (a displacement or misalignmentof a joint or body part) if you get it from achiropractor or other qualified providers.
In-Network$25 copay for each Medicare-covered visit
Supplemental routine care not covered.
20% coinsurance for medically necessary footcare, including care for medical conditionsaffecting the lower limbs.
10 Podiatry Services
$25 copay for up to 1 supplemental routinevisit(s) every three months
Medicare-covered podiatry benefits are formedically-necessary foot care.
GeneralAuthorization rules may apply.
40% coinsurance for most outpatient mentalhealth services
11 OutpatientMental HealthCare
In-Network$40 copay for each Medicare-coveredindividual therapy visit
Specified copayment for outpatient partialhospitalization program services furnished bya hospital or community mental health center(CMHC). Copay cannot exceed the Part Ainpatient hospital deductible.
$40 copay for each Medicare-covered grouptherapy visit
"Partial hospitalization program" is astructured program of active outpatient
$40 copay for each Medicare-coveredindividual therapy visit with a psychiatrist
psychiatric treatment that is more intense than$40 copay for each Medicare-covered grouptherapy visit with a psychiatrist
the care received in your doctor's or therapist'soffice and is an alternative to inpatienthospitalization. $40 copay for Medicare-covered partial
hospitalization program services
GeneralAuthorization rules may apply.
20% coinsurance12 OutpatientSubstance AbuseCare
Page 9 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
In-Network$40 copay for Medicare-covered individualvisits
$40 copay for Medicare-covered group visits
GeneralAuthorization rules may apply.
20% coinsurance for the doctor's services
Specified copayment for outpatient hospitalfacility services Copay cannot exceed the PartA inpatient hospital deductible.
13 OutpatientServices/Surgery
In-Network$200 copay for each Medicare-coveredambulatory surgical center visit20% coinsurance for ambulatory surgical
center facility services $0 to $200 copay for each Medicare-coveredoutpatient hospital facility visit
GeneralAuthorization rules may apply.
20% coinsurance14 AmbulanceServices(medicallynecessaryambulanceservices)
In-Network$200 copay for Medicare-covered ambulancebenefits.
General$50 copay for Medicare-covered emergencyroom visits
20% coinsurance for the doctor's services
Specified copayment for outpatient hospitalfacility emergency services.
15 Emergency Care(You may go toany emergencyroom if youreasonably believeyou needemergency care.)
Worldwide coverage.
If you are admitted to the hospital within72-hour(s) for the same condition, you pay$0 for the emergency room visit.
Emergency services copay cannot exceed PartA inpatient hospital deductible for each serviceprovided by the hospital.
You don't have to pay the emergency roomcopay if you are admitted to the hospital as aninpatient for the same condition within 3 daysof the emergency room visit.
Not covered outside the U.S. except underlimited circumstances.
Page 10 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
General$25 copay for Medicare-coveredurgently-needed-care visits
20% coinsurance, or a set copay
NOT covered outside the U.S. except underlimited circumstances.
16 Urgently NeededCare(This is NOTemergency care,and in most cases,is out of theservice area.)
GeneralAuthorization rules may apply.
20% coinsurance17 OutpatientRehabilitationServices(OccupationalTherapy, PhysicalTherapy, Speechand LanguageTherapy)
In-Network$35 copay for Medicare-covered OccupationalTherapy visits
$35 copay for Medicare-covered Physical and/or Speech and Language Therapy visits
Outpatient Medical Services and Supplies
GeneralAuthorization rules may apply.
20% coinsurance18 Durable MedicalEquipment(includeswheelchairs,oxygen, etc.)
In-Network20% of the cost for Medicare-covered items
GeneralAuthorization rules may apply.
20% coinsurance19 ProstheticDevices(includes braces,artificial limbsand eyes, etc.)
In-Network20% of the cost for Medicare-covered items
In-Network$0 copay for Diabetes self-managementtraining
20% coinsurance for diabetes self-managementtraining
20% coinsurance for diabetes supplies
20 DiabetesPrograms andSupplies
10% of the cost for Diabetes monitoringsupplies
20% coinsurance for diabetic therapeutic shoesor inserts
10% of the cost for Therapeutic shoes orinserts
Page 11 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
GeneralAuthorization rules may apply.
20% coinsurance for diagnostic tests andx-rays
21 Diagnostic Tests,X-Rays, LabServices, andRadiologyServices
In-Network$0 copay for Medicare-covered lab services
$0 copay for Medicare-covered diagnosticprocedures and tests
$0 copay for Medicare-covered lab services
Lab Services: Medicare covers medicallynecessary diagnostic lab services that areordered by your treating doctor when they areprovided by a Clinical Laboratory $30 to $75 copay for Medicare-covered X-raysImprovement Amendments (CLIA) certified
$30 to $75 copay for Medicare-covereddiagnostic radiology services (not includingX-rays)
laboratory that participates in Medicare.Diagnostic lab services are done to help yourdoctor diagnose or rule out a suspected illnessor condition. Medicare does not cover most 20% of the cost for Medicare-covered
therapeutic radiology servicessupplemental routine screening tests, likechecking your cholesterol.
If the doctor provides you services in additionto Outpatient Diagnostic Procedures, Testsand Lab Services, separate cost sharing of $15to $25 may apply
If the doctor provides you services in additionto Outpatient Diagnostic and TherapeuticRadiology Services, separate cost sharing of$15 to $25 may apply
In-Network$0 copay for Medicare-covered CardiacRehabilitation Services
20% coinsurance Cardiac Rehabilitationservices
20% coinsurance for PulmonaryRehabilitation services
22 Cardiac andPulmonaryRehabilitationServices
$0 copay for Medicare-covered IntensiveCardiac Rehabilitation Services20% coinsurance for Intensive Cardiac
Rehabilitation services $0 copay for Medicare-covered PulmonaryRehabilitation ServicesThis applies to program services provided in
a doctor's office. Specified cost sharing forprogram services provided by hospitaloutpatient departments.
Page 12 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
PREVENTIVE SERVICES
General$0 copay for all preventive services coveredunder Original Medicare at zero cost sharing:
No coinsurance, copayment or deductible forthe following:
23 PreventiveServices andWellness/EducationPrograms
Abdominal Aortic Aneurysm ScreeningAbdominal Aortic Aneurysm screeningBone Mass Measurement. Covered once
every 24 months (more often if medicallynecessary) if you meet certain medicalconditions.
Bone Mass MeasurementCardiovascular ScreeningCervical and Vaginal Cancer Screening(Pap Test and Pelvic Exam)Cardiovascular Screening
Cervical and Vaginal Cancer Screening.Covered once every 2 years. Covered oncea year for women with Medicare at highrisk.
Colorectal Cancer ScreeningDiabetes ScreeningInfluenza VaccineHepatitis B Vaccine
Colorectal Cancer Screening HIV ScreeningDiabetes Screening Breast Cancer Screening (Mammogram)Influenza Vaccine Medical Nutrition Therapy ServicesHepatitis B Vaccine for people withMedicare who are at risk
Personalized Prevention Plan Services(Annual Wellness Visits)
HIV Screening. $0 copay for the HIVscreening, but you generally pay 20% ofthe Medicare-approved amount for thedoctor's visit. HIV screening is covered forpeople with Medicare who are pregnantand people at increased risk for theinfection, including anyone who asks forthe test. Medicare covers this test onceevery 12 months or up to three timesduring a pregnancy.
Pneumococcal VaccineProstate Cancer Screening (ProstateSpecific Antigen (PSA) test only)Smoking Cessation (Counseling to stopsmoking)Welcome to Medicare Physical Exam(Initial Preventive Physical Exam)
HIV screening is covered for people withMedicare who are pregnant and people atincreased risk for the infection, including
Breast Cancer Screening (Mammogram).Medicare covers screening mammogramsonce every 12 months for all women withMedicare age 40 and older. Medicarecovers one baseline mammogram forwomen between ages 35-39.
anyone who asks for the test. Medicare coversthis test once every 12 months or up to threetimes during a pregnancy. Please contact planfor details.
In-NetworkThe plan covers the following supplementaleducation/wellness programs:
Page 13 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
Medical Nutrition Therapy ServicesNutrition therapy is for people who havediabetes or kidney disease (but aren't ondialysis or haven't had a kidney transplant)when referred by a doctor. These servicescan be given by a registered dietitian andmay include a nutritional assessment andcounseling to help you manage yourdiabetes or kidney disease
Health Club Membership/Fitness ClassesNursing Hotline
Personalized Prevention Plan Services(Annual Wellness Visits)Pneumococcal Vaccine. You may only needthe Pneumonia vaccine once in yourlifetime. Call your doctor for moreinformation.Prostate Cancer Screening - ProstateSpecific Antigen (PSA) test only. Coveredonce a year for all men with Medicare overage 50.Smoking Cessation (counseling to stopsmoking). Covered if ordered by yourdoctor. Includes two counseling attemptswithin a 12-month period. Each counselingattempt includes up to four face-to-facevisits.Welcome to Medicare Physical Exam(initial preventive physical exam) Whenyou join Medicare Part B, then you areeligible as follows. During the first 12months of your new Part B coverage, youcan get either a Welcome to MedicarePhysical Exam or an Annual WellnessVisit. After your first 12 months, you canget one Annual Wellness Visit every 12months.
In-Network10% of the cost for renal dialysis
20% coinsurance for renal dialysis
20% coinsurance for kidney disease educationservices
24 Kidney Diseaseand Conditions
$0 copay for kidney disease education services
Page 14 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
Drugs Covered Under Medicare Part BGeneral20% of the cost for Part B-coveredchemotherapy drugs and other Part B-covereddrugs.
Most drugs are not covered under OriginalMedicare. You can add prescription drugcoverage to Original Medicare by joining aMedicare Prescription Drug Plan, or you canget all your Medicare coverage, including
25 OutpatientPrescriptionDrugs
prescription drug coverage, by joining a Drugs Covered Under Medicare Part DGeneralThis plan uses a formulary. The plan will sendyou the formulary. You can also see the
Medicare Advantage Plan or a Medicare CostPlan that offers prescription drug coverage.
formulary at www.empireblue.com on theweb.
Different out-of-pocket costs may apply forpeople who
have limited incomes,live in long term care facilities, orhave access to Indian/Tribal/Urban (IndianHealth Service) providers.
The plan offers national in-networkprescription coverage (i.e., this would include50 states and the District of Columbia). Thismeans that you will pay the same cost-sharingamount for your prescription drugs if you getthem at an in-network pharmacy outside ofthe plan's service area (for instance when youtravel).
Total yearly drug costs are the total drug costspaid by both you and a Part D plan.
The plan may require you to first try one drugto treat your condition before it will coveranother drug for that condition.
Some drugs have quantity limits.
Your provider must get prior authorizationfrom Empire MediBlue Plus (HMO) forcertain drugs.
You must go to certain pharmacies for a verylimited number of drugs, due to specialhandling, provider coordination, or patienteducation requirements that cannot be metby most pharmacies in your network. Thesedrugs are listed on the plan's website,
Page 15 – Empire MediBlue Plus (HMO)23461MUSENMUB_031
Empire MediBlue Plus (HMO)Original MedicareBenefit
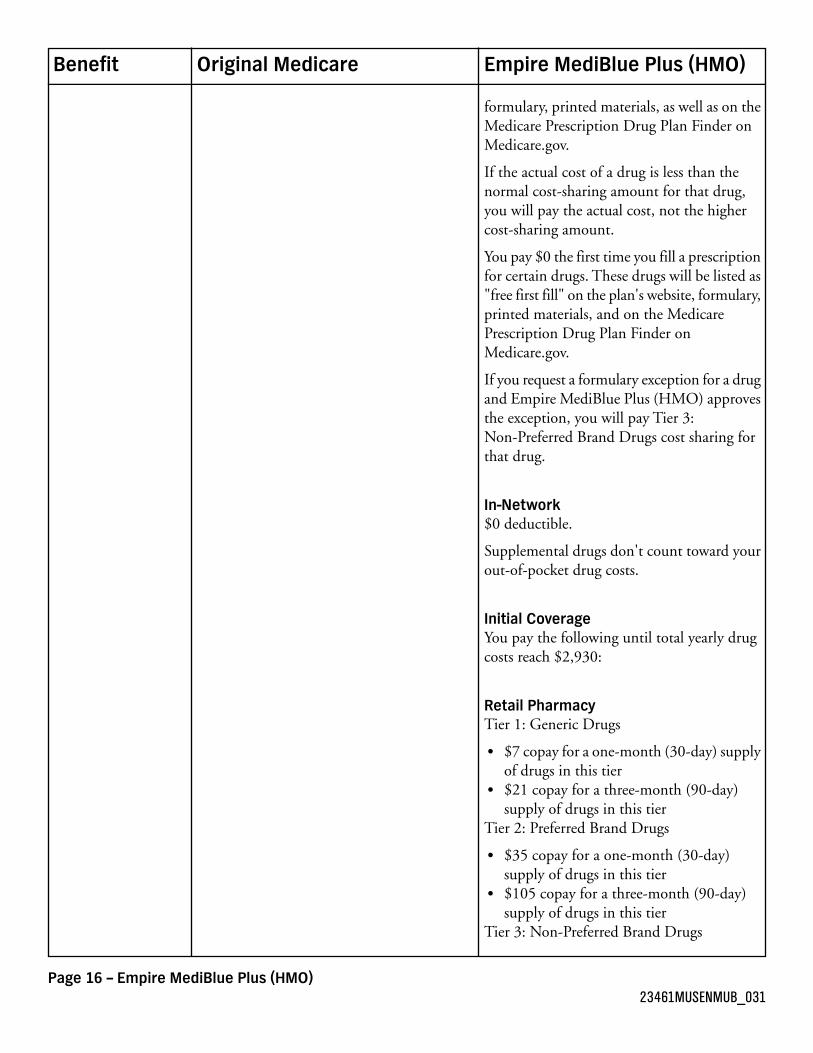
formulary, printed materials, as well as on theMedicare Prescription Drug Plan Finder onMedicare.gov.
If the actual cost of a drug is less than thenormal cost-sharing amount for that drug,you will pay the actual cost, not the highercost-sharing amount.
You pay $0 the first time you fill a prescriptionfor certain drugs. These drugs will be listed as"free first fill" on the plan's website, formulary,printed materials, and on the MedicarePrescription Drug Plan Finder onMedicare.gov.
If you request a formulary exception for a drugand Empire MediBlue Plus (HMO) approvesthe exception, you will pay Tier 3:Non-Preferred Brand Drugs cost sharing forthat drug.
In-Network$0 deductible.
Supplemental drugs don't count toward yourout-of-pocket drug costs.
Initial CoverageYou pay the following until total yearly drugcosts reach $2,930:
Retail PharmacyTier 1: Generic Drugs
$7 copay for a one-month (30-day) supplyof drugs in this tier$21 copay for a three-month (90-day)supply of drugs in this tier
Tier 2: Preferred Brand Drugs
$35 copay for a one-month (30-day)supply of drugs in this tier$105 copay for a three-month (90-day)supply of drugs in this tier
Tier 3: Non-Preferred Brand Drugs
Page 16 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
$80 copay for a one-month (30-day)supply of drugs in this tier$240 copay for a three-month (90-day)supply of drugs in this tier
Tier 4: Injectable Drugs
33% coinsurance for a one-month (30-day)supply of drugs in this tier33% coinsurance for a three-month(90-day) supply of drugs in this tier
Tier 5: Specialty Tier Drugs
33% coinsurance for a one-month (30-day)supply of drugs in this tier
Tier 6: Supplemental Drugs
$7 copay for a one-month (30-day) supplyof drugs in this tier$21 copay for a three-month (90-day)supply of drugs in this tier
Long-Term Care PharmacyTier 1: Generic Drugs
$7 copay for a one-month (34-day) supplyof drugs in this tier
Tier 2: Preferred Brand Drugs
$35 copay for a one-month (34-day)supply of drugs in this tier
Tier 3: Non-Preferred Brand Drugs
$80 copay for a one-month (34-day)supply of drugs in this tier
Tier 4: Injectable Drugs
33% coinsurance for a one-month (34-day)supply of drugs in this tier
Tier 5: Specialty Tier Drugs
33% coinsurance for a one-month (34-day)supply of drugs in this tier
Tier 6: Supplemental Drugs
$7 copay for a one-month (34-day) supplyof drugs in this tier
Mail OrderTier 1: Generic Drugs
Page 17 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
$14 copay for a three-month (90-day)supply of drugs in this tier
Tier 2: Preferred Brand Drugs
$70 copay for a three-month (90-day)supply of drugs in this tier
Tier 3: Non-Preferred Brand Drugs
$160 copay for a three-month (90-day)supply of drugs in this tier
Tier 4: Injectable Drugs
33% coinsurance for a three-month(90-day) supply of drugs in this tier
Tier 5: Specialty Tier Drugs
33% coinsurance for a one-month (30-day)supply of drugs in this tier
Tier 6: Supplemental Drugs
$14 copay for a three-month (90-day)supply of drugs in this tier
Coverage GapAfter your total yearly drug costs reach $2,930,you receive a discount on brand name drugsand pay 86% of the plan's costs for all genericdrugs until your yearly out-of-pocket drugcosts reach $4,700.
Catastrophic CoverageAfter your yearly out-of-pocket drug costsreach $4,700, you pay the greater of:
5% coinsurance, or$2.60 copay for generic (including branddrugs treated as generic) and a $6.50 copayfor all other drugs.
Tier 6: Supplemental Drugs
$7 copay for drugs in this tier
Out-of-NetworkPlan drugs may be covered in specialcircumstances, for instance, illness whiletraveling outside of the plan's service areawhere there is no network pharmacy. You may
Page 18 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
have to pay more than your normalcost-sharing amount if you get your drugs atan out-of-network pharmacy. In addition, youwill likely have to pay the pharmacy's fullcharge for the drug and submit documentationto receive reimbursement from EmpireMediBlue Plus (HMO).
Out-of-Network Initial CoverageYou will be reimbursed up to the plan's costof the drug minus the following for drugspurchased out-of-network until total yearlydrug costs reach $2,930:
Tier 1: Generic Drugs
$7 copay for a one-month (30-day) supplyof drugs in this tier
Tier 2: Preferred Brand Drugs
$35 copay for a one-month (30-day)supply of drugs in this tier
Tier 3: Non-Preferred Brand Drugs
$80 copay for a one-month (30-day)supply of drugs in this tier
Tier 4: Injectable Drugs
33% coinsurance for a one-month (30-day)supply of drugs in this tier
Tier 5: Specialty Tier Drugs
33% coinsurance for a one-month (30-day)supply of drugs in this tier
Tier 6: Supplemental Drugs
$7 copay for a one-month (30-day) supplyof drugs in this tier
You will not be reimbursed for the differencebetween the Out-of-Network Pharmacy chargeand the plan's In-Network allowable amount.
Additional Out-of-Network Coverage GapYou will be reimbursed up to 14% of the planallowable cost for generic drugs purchasedout-of-network until total yearly out-of-pocketdrug costs reach $4,700.
Page 19 – Empire MediBlue Plus (HMO)23461MUSENMUB_031
Empire MediBlue Plus (HMO)Original MedicareBenefit
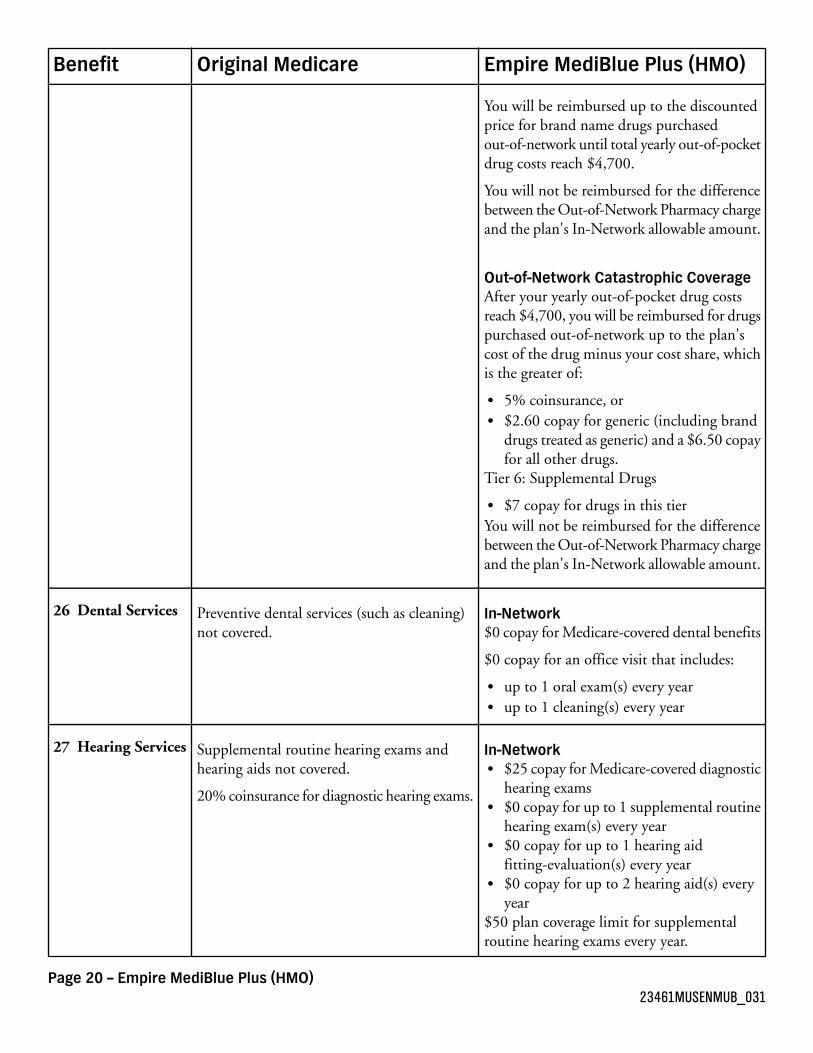
You will be reimbursed up to the discountedprice for brand name drugs purchasedout-of-network until total yearly out-of-pocketdrug costs reach $4,700.
You will not be reimbursed for the differencebetween the Out-of-Network Pharmacy chargeand the plan's In-Network allowable amount.
Out-of-Network Catastrophic CoverageAfter your yearly out-of-pocket drug costsreach $4,700, you will be reimbursed for drugspurchased out-of-network up to the plan'scost of the drug minus your cost share, whichis the greater of:
5% coinsurance, or$2.60 copay for generic (including branddrugs treated as generic) and a $6.50 copayfor all other drugs.
Tier 6: Supplemental Drugs
$7 copay for drugs in this tierYou will not be reimbursed for the differencebetween the Out-of-Network Pharmacy chargeand the plan's In-Network allowable amount.
In-Network$0 copay for Medicare-covered dental benefits
Preventive dental services (such as cleaning)not covered.
26 Dental Services
$0 copay for an office visit that includes:
up to 1 oral exam(s) every yearup to 1 cleaning(s) every year
In-NetworkSupplemental routine hearing exams andhearing aids not covered.
27 Hearing Services$25 copay for Medicare-covered diagnostichearing exams20% coinsurance for diagnostic hearing exams.$0 copay for up to 1 supplemental routinehearing exam(s) every year$0 copay for up to 1 hearing aidfitting-evaluation(s) every year$0 copay for up to 2 hearing aid(s) everyyear
$50 plan coverage limit for supplementalroutine hearing exams every year.
Page 20 – Empire MediBlue Plus (HMO)23461MUSENMUB_031

Empire MediBlue Plus (HMO)Original MedicareBenefit
$1,000 plan coverage limit for hearing aidsevery year.
In-Network20% coinsurance for diagnosis and treatmentof diseases and conditions of the eye.
28 Vision Services$0 copay for one pair of eyeglasses orcontact lenses after cataract surgery.Supplemental routine eye exams and glasses
not covered. $0 to $25 copay for exams to diagnose andtreat diseases and conditions of the eye.
Medicare pays for one pair of eyeglasses orcontact lenses after cataract surgery.
$0 copay for up to 1 supplemental routineeye exam(s) every year
Annual glaucoma screenings covered forpeople at risk.
$0 copay for up to 1 pair(s) of glasses everytwo years$0 copay for up to 1 pair(s) of contactsevery two years
$130 plan coverage limit for eye glasses (lensesand frames) every two years.
$80 plan coverage limit for contact lensesevery two years.
GeneralThe plan does not cover Over-the-Counteritems.
Not covered.Over-the-CounterItems
In-NetworkThis plan does not cover supplemental routinetransportation.
Not covered.Transportation(Routine)
In-NetworkThis plan does not cover Acupuncture.
Not covered.Acupuncture
Page 21 – Empire MediBlue Plus (HMO)23461MUSENMUB_031