submitted during the course of dm...
TRANSCRIPT

SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY
TRIVANDRUM, KERALA
PROJECT REPORT
Submitted during the course of DM Cardiology
Dr. SRINIVASA PRASAD
DM Trainee
DEPARTMENT OF CARDIOLOGY
Jan 2014-Dec 2016
DECLARATION
I, Dr Srinivasa Prasad , hereby declare that the project in this book
was undertaken by me under the supervision of the faculty,
Department of Cardiology, Sree Chitra Tirunal Institute for Medical
Sciences and Technology.
Thiruvananthapuram Dr Srinivasa Prasad Date DM Trainee
Forwarded
The candidate, Dr. Srinivasa Prasad , has carried out the minimum required project.
Thiruvananthapuram Prof. Dr Ajitkumar VK
Date Head of Department of Cardiology

TITLE
Clinical Outcomes of patients with
coronary artery disease who underwent
FFR evaluation of intermediate
coronary lesionS– COFFRS Study
INVESTIGATORS
Dr. Srinivasa Prasad
Dr. Harikrishnan S, professor
Dr. Abhilash SP, Associate Professor Dr. Sanjay G, Additional Professor

ACKNOWLEDGEMENT
At the outset I would like to thank my mentor, guide - Prof
Harikrishnan S, to whom I am greatly indebted to, for his immense
support, encouragement and inspiring attitude – not only for this project,
but for many more projects, presentations and cath lab learning throughout
my DM period.
I deeply thank Dr Sanjay G, for allowing me to pursue this project
(originally his brainchild project) and for his constant guidance, valuable
inputs and motivation throughout this project.
Special thanks to my co-guide -Dr Abhilash SP for his valuable
suggestions.
My sincere thanks to technical staff of SCTIMST for their extreme
co-operation and support
Finally I express my gratitude to all my patients, and all those who
directly and indirectly helped me do this study.
Srinivasa Prasad

5
INDEX
PAGE NO
ABBREVIATIONS & ACRONYMS 6 – 8 INTRODUCTION 9 – 12
AIMS AND OBJECTIVES 13 – 14
MATERIAL AND METHODS 15 – 20
REVIEW OF LITERATURE 21 – 26
OBSERVATION AND RESULTS 27 – 32
DISCUSSION 33 – 37
CONCLUSION 38 – 39
BIBLIOGRAPHY 40 – 48 APPENDIX 49 ...

6
Abbreviations & Acronyms
7
Acronym’s & abbreviations
Abbreviations and Acronyms:
ACS: Acute Coronary Syndrome
CABG: Coronary artery bypass graft
CAD: Coronary artery disease
COURAGE Trial: Clinical Outcomes Utilizing Revascularization and
Aggressive Drug Evaluation (COURAGE) trial
DEFER Trial : Measurement of fractional flow reserve to assess the
functional severity of coronary-artery stenoses – DEFER Trial
DS: Percent diameter stenosis
ECG: Electrocardiogram
FAME 2 Trial: Fractional flow reserve versus angiography for
guidance of PCI in patients with multivessel coronary artery disease
(FAME)
FFR: Fractional Flow Reserve
LVF: Left ventricular failure
MACE: Major adverse cardiac events
MLD: Minimum luminal diameter
Non-STE-ACS: Non ST elevated acute coronary syndrome
NSTEMI: Non-ST elevated myocardial infarction
PCI: Percutaneous coronary interventions
QCA : Quantitative Coronary Angiography

8
Acronym’s & abbreviations
RD : Reference diameter,
STEMI: ST elevated myocardial infarction
TVR: Target vessel revascularization
UA : Unstable angina

Introduction
Introduction
10
Invasive coronary angiography is known for its precision in delineating
topographical anatomy of lumen of epicardial coronary arteries, but lacks the
ability to determine the functional significance of coronary stenoses. Functional
severity of coronary narrowing has been determined to be the most prominent
prognostic factor among the individuals with documented coronary artery
disease(1). Hence, combined assessment of anatomy and functional
information with high accuracy would help in guiding the treatment strategy for
patients with known or suspected coronary artery disease, particularly those
with intermediate degree of stenosis(2).
Fractional Flow Reserve (FFR) is an invasive but `easy and simple to
measure` index of the functional significance of severity of coronary stenosis
with a diagnostic precision of myocardial scintigraphy, albeit with a better
spatial resolution(2). It is derived from the ratio between coronary (distal to
stenosis) and aortic pressure measurements during maximal hyperemia(3).
Hence FFR in combination with conventional angiography is rapidly emerging
as an accurate approach of combining anatomy and physiology(4).
Role of FFR in determining the need for coronary stenting has been
studied in various trials and has been recommended to assess the significance of
intermediate coronary lesions.(2,3,5–7). FFR has been demonstrated to be an
Introduction
11
useful index in patients referred for percutaneous revascularisation with
intermediate stenosis, involving single coronary vessel (2,3,7,8) and also in
those with multi-vessel disease(5,9). Additional concerns regarding the
association between drug-eluting stents and late complications, continued
exposure to dual anti-platelet therapy, and increased costs make appropriate use
of these devices critical(10). This leaves FFR as a better choice to assess
hemodynamic significance of intermediate lesion and to guide treatment
strategy.
Clinical outcomes of the decision to intervene based on FFR has been
addressed in various trials, being conducted in controlled environment (7,11–
14). Availability of such data from routine clinical practice is limited(15). In
India, routine clinical use of FFR is more or less limited to tertiary care centres
and its utilization is probably confined to a small group of patients with CAD.
Demographic, risk profile and natural history of coronary artery disease among
Indian/ Asian patients are affected by some unique factors such as younger age
group, predominant metabolic syndrome, exposure to lipid-rich diet and
increasingly common sedentary life style(16–18) and there is data which
discuss about smaller coronary artery diameters in Indian patients undergoing
angiography(19). There is no data regarding the utility of FFR from India.
Introduction
12
In this study, we intended to assess the clinical outcome of FFR based
management strategies in Indian patients, results of which could serve to
validate and re-emphasize the utility of this investigation in our setting.
Aims and Objectives

Aims and Objectives
14
This study aims to evaluate the utility of FFR in those stable ischemic
heart disease patients with intermediate coronary disease with the following
objectives:
1. To study the clinical outcomes among the patients who underwent
FFR as part of the evaluation of their coronary stenosis
2. To compare the outcomes among patients who underwent
revascularisation versus those kept under medical follow up based
on FFR assessment.

Materials and Methods

16
Materials and Methods
Study Design
This is a retrospective study (approved by the Institutional Ethics
Committee, No: - SCT/IEC/778/ JUNE 2015) was conducted between June
2010 to June 2015 at Sree Chitra Tirunal Institute for Medical Sciences and
Technology (SCTIMST), Trivandrum, a tertiary care hospital in India.
Study Patients:
Medical records of all patients who underwent FFR during the period
between June 2010 to June 2015 were reviewed. All patients with stable
ischemic heart disease or those patients who had acute coronary event a week
or more prior to the procedure were included.
Study population were grouped into 3 groups :
Group 1 – FFR >0.8 and kept on medical followup;
Group 2 – FFR ≤0.8 and underwent revascularization by PCI or
CABG; and
Group 3 – FFR ≤0.8 and did not undergo revascularisation as per
patient preference.

17
Materials and Methods
Exclusion criteria:
1) Culprit Coronary vessel responsible for acute coronary syndrome within
7 days. (However if the FFR was studied in non-culprit coronary arteries
in the same patient it was included)
2) Left Main Coronary artery lesion
3) Previous CABG
4) Contraindication to adenosine,
5) Conditions for which FFR has not been validated (tortuous coronary
arteries, left ventricular hypertrophy)
6) Life-threatening comorbidity.
7) FFR assessment of a stenosis in a coronary artery supplying collaterals
to the vascular bed subtended by a totally occluded artery.
Coronary pressure measurement and calculation of FFR:
FFR was measured in all intermediate stenoses for assessment of
hemodynamic significance. Intracoronary pressure measurements were
performed with a 0.014-inch pressure guidewire (PressureWire Aeris from St.
Jude Medical or Prime wire PRESTIGE from Volcano Inc, Rancho Cordova,
California, USA) introduced through a guide catheter. Hyperemia was induced
by intravenous adenosine (140 μg/kg/min until a steady state was obtained or
for at least 6 minutes) after a bolus dose of intracoronary nitroglycerin of

18
Materials and Methods
200micrograms. The FFR was calculated from the ratio of mean hyperemic
distal coronary pressure measured by the pressure-wire and the mean aortic
pressure obtained by the coronary guide catheter. (RADIANALYZER, St Jude
Medical OR VOLCANO, Volcano Corporation). As per the departmental
protocol, FFR value of >0.80 was considered as a criteria to defer
revascularisation at the time of procedure and the decision to revascularise was
based on the cut-off value of FFR ≤ 0.80. If there were serial stenotic lesions,
pressure gradient drop of > 10 was considered significant. All patients had
received antiplatelets, statins and beta blockers. Those who underwent
revascularization received aspirin and clopidogrel for at least 12 months after
the procedure.
Quantitative coronary arteriography:
Angiograms were reviewed by two independent investigators to
determine the severity. Quantitative assessment of lesions (QCA – Quantitative
Coronary Angiography) was done using a validated software employing
Siemens/Philips algorithm. Reference diameter (RD), minimum luminal
diameter (MLD), and percent diameter stenosis (DS) were assessed in two
orthogonal views.
19
Materials and Methods
Follow-up and clinical events:
All patients were evaluated at the outpatient intervention clinic for drug
compliance, new / persistent/ worsening symptoms, ECG changes & any
MACE events including repeat coronary angiogram and coronary
revascularisation, if done.
Primary end point
The primary endpoint during the follow-up was major adverse cardiac
events (MACE), defined as composite of cardiovascular death, non-fatal acute
coronary syndrome, and any repeat revascularization of the vessel in which
FFR was studied (target vessel revascularization – TVR). A repeat angiogram
was performed only when indicated clinically. The culprit artery responsible for
the recurrence of symptoms was based on the correlation of
electrocardiographic changes, echocardiographic data (if available), and the
diagnostic angiogram.
Secondary end point
The secondary endpoints were individual components of the MACE.
Myocardial infarction was defined as (two out of three criteria): prolonged
chest pain > 20 min; levels of serum creatine kinase (or the MB fraction) or
troponin over two-fold higher than the upper normal limit; and ST-T segment
changes or new Q waves on serial electrocardiogram indicative of myocardial
20
Materials and Methods
damage(20).
Statistical analysis:
The data was analysed with commercially available statistical software
(SPSS) to study the percentage of patients who had clinical event, MACE,
repeat angiogram and revascularization – PCI/CABG.
Continuous variables are expressed as mean with standard deviations and
discrete variables as counts and percentage. For categorical variables, chi-
square test and Fisher exact t test were used, and for continuous variables,
student t test was used. Clinical, angiographic variables and FFR values
between the deferred, revascularised and nonrevascularised groups were
compared. Survival curves were determined by Kaplan and Meier method and
compared by the log-rank test. A p value less than or equal to 0.05 was
considered statistically significant.

Review of Literature

Review of Literature
22
Several investigators have reported discrepancies between the severity of
coronary angiographic stenosis and the severity of functional coronary stenosis.
Lima RS e t a l(21), showed that 54% (77 of 143) patients with angiographic 3-
vessel disease, had either had no perfusion defect or a single vessel disease
pattern on myocardial perfusion imaging. Similarly Melikian et al (22) , found
that 26 of 67 patients with angiographic multivessel disease had no perfusion
defects and 24 had single perfusion defect by myocardial perfusion imaging
performed after coronary angiography.
Visual – functional mismatch analysis was done from the landmark trial
– FAME study(12), revealed that of 14% had significant three vessel disease on
FFR assessment, among those who were labeled as having 3 vessel disease
based on visual assessment and 46% had 2 or more coronary artery
involvement with significant FFR of ≤0.80. And a significant 9% didnot have
any physiologically significant coronary lesions. Also only 61% (816 of 1329)
target lesions (visually estimated to have >50% stenosis), had FFR ≤0.80. On
further analysis, FFR was >0.80 in 65% of the lesions assessed as 50 to 70%
stenosis severity, 20% among those estimated to have 71 to 90% stenosis and
4% among those with 91 to 99% severity.
These observations, highlighted that significant 40% of revascularization
Review of Literature
23
procedures were uncalled for, more so without a physiological assessment by
FFR. Also a considerable proportion would have benefitted by percutaneous
revascularization, rather than undergoing coronary bypass graft surgery. Hence,
it is recommended to have a physiological or functional assessment by FFR in
those coronary lesions of intermediate stenosis severity during revascularization
procedure, particularly when noninvasive tests are not available.
Several factors are implicated for the dissociation between angiographic
and FFR severity. These include length of lesion, size of the reference vessel,
and eccentricity of the lesion – all of which would affect resistance to the
coronary blood flow and thereby yield an abnormal FFR. Myocardial area or
mass being supplied by diseased coronary vessel is the major determinant of the
functional significance of the given stenotic lesion. Thus, when an intermediate
lesion of a coronary vessel that supply large myocardial territory could be
functionally significant, wherein a lesion of severe stenosis, catering to small
myocardial territory could be insignificant physiologically.
DEFER Study (“FFR to Determine Appropriateness of Angioplasty in
Moderate Coronary Stenoses”)(7), the only randomized trial till date, addressed
the issue of tailoring the management strategy comparing percutaneous
revascularization with medical therapy in those with intermediate coronary
stenosis. Study randomly assigned its 325 subjects with intermediate coronary

Review of Literature
24
lesions into 3 groups: 1. Deferral group (n = 91, FFR was ≥0.75 , all were
treated with optimal medical therapy), 2. PCI group (n = 90, FFR was ≥0.75 ,
and all these patients underwent PCI with stent implantation along with optimal
medical therapy) and 3. Reference group (n = 144, FFR was <0.75, all
underwent PCI as planned). On 5 year followup, it was noted that event-free
survival were similar among deferred and PCI groups (80% versus 73%,
P=0.52). The composite endpoints of cardiac cause of mortality and acute
myocardial infarction were 3.3% in deferred group, 7.9% in PCI group, and
15.7% in the reference group , thereby yielding <1% annual risk of cardiac
mortality or MI in those with normal FFR. Thus this study showed that
functionally non-significant coronary lesion, can be managed safely with
optimal medical therapy, deferring the PCI, regardless of angiographic stenosis,
for a period of upto 5 years.
FAME study (“The Fractional Flow Reserve versus Angiography for
Multivessel Evaluation (FAME) study ”)(12) pointed out the cost effectiveness
of FFR-based revascularization strategy over one year of followup, with
significantly low rate of composite endpoints of death, non-fatal myocardial
infarction, and repeat revascularization.
A study by Alexandre Berger,et al(23) studied the outcome of patients
with multivessel CAD (n = 102), who were grouped into those who underwent
Review of Literature
25
PCI for atleast one vessel based on FFR of < 0.75 (113 vessels), and those who
were deferred revasularisation for atleast one vessel based on FFR value of ≥
0.75. They found no significant difference in clinical cardiac events of new
onset angina, MI, or target vessel revascularisation, between the two groups
over a period of 3 years (MACE rate of 13%). Study didnot have any mortality
event. Authors conclusively showed the safety of deferring the PCI of
functionaly nonsignificant stenosis, and proceeding only with functionally
significant stenosis in patients with mutivessel disease, even if planned for
multivessel PCI based on angiographic severity.
A retrospective study(24) of real life clinical patients from Mayo clinic,
compared clinical outcomes of patients who underwent angiography guided
PCI (n = 6268), FFR guided PCI (n =369) and FFR based defer group (n = 721
). Over a follow-up period of 7 years, MACE event rates were 57% in
angiographic guided PCI group and 50 % in those with FFR guided PCI group,
(p = 0.016 between the groups); with lower rate of death or MI in FFR guided
PCI group in comparison to angiographic guided group (Hazard Ratio 0.85,
95% confidence interval : 0.71 to 1.01, p = 0.06). Also, lower rate of MI was
noted in the FFR-guided deferred-PCI group independently. (Hazard Ratio :
0.46, 95% Confidence Interval : 0.26–0.82, P = 0.008).
Study by Takafumi Yamane et al(25), compared clinical outcome

Review of Literature
26
between patients with intermediate coronary lesion and FFR <0.75 who
underwent PCI (n = 99) and patients with intermediate CAD and FFR between
0.75 and 0.79 who were kept on optimal medical therapy (n = 26). Kaplan
meier survival analysis revealed that over a period of 82 months, there was
poorer event-free survival of the patients with FFR between 0.75 to 0.79 and
kept on medical therapy (p=0.0148). Study concluded and proposed to consider
FFR cutoff of 0.80 among intermediate coronary lesions for deferring PCI.
Two-year clinical outcome study of patients with deferred lesions in the
FFR-guided group from the FAME study(26) demonstrated that only 0.2% (1
of 513) had MI and only 3.2% (16 of 513) needed repeat revascularization.
Other smaller studies(27–32) also have consistently shown lowerrates of
death and MI in patients with FFR guided deferred treatment of intermediate
coronary lesions.

Observations and Results

Observation and Results
Two hundred and eighty two patients with intermediate coronary lesions,
(as assessed by quantitative coronary angiography), who underwent FFR to
assess the functional severity of the lesion were included in the study. 239 of
them were males (male : female ratio 4.6 : 1). Median age was 57 years (range
= 28–78). 151 patients (53.3%) were diabetic, 117 (41.4%) were hypertensive
and 157 (55.6%) patients used tobacco (all were males). Pre-angiography stress
test result was available in 196 patients, of whom 94 (48%) tested positive for
inducible ischemia, 74 (37.6%) had inconclusive test results and 28 (14.3%)
had negative result but were advised coronary angiogram for assessment of
their symptoms. The remaining 85 patients (30.2%) underwent coronary
angiography without stress testing based on their clinical presentation.
Coronary angiogram revealed single vessel disease (SVD) in 68 (24.1%)
, double vessel disease (DVD) in 122 (43.3%) and three vessel disease (TVD)
in 92 (32.6%). 192 (68.1%) of patients had positive FFR value (FFR < 0.8) with
a mean FFR of 0.7 among these patients.
90 patients (31.9%) were in Group 1, 175 patients (62.1%) in group 2
(PCI in 141 & CABG in 29) and 17 (6%) in group 3. The baseline
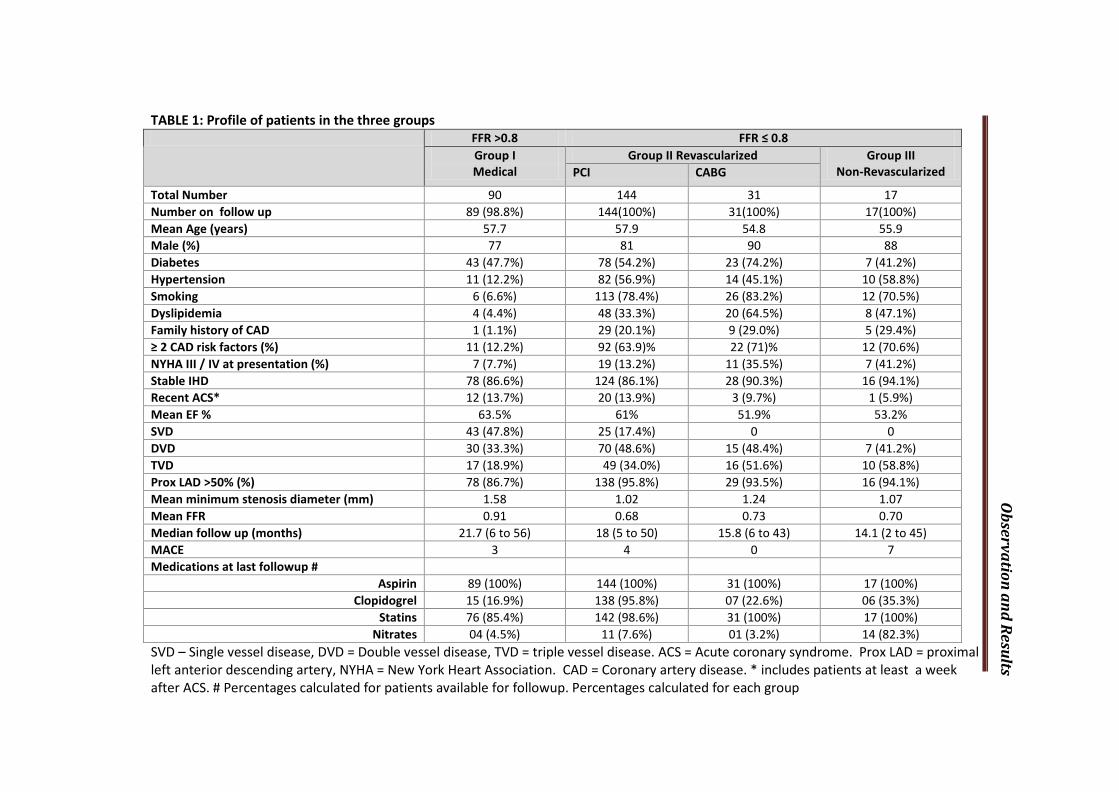
characteristics of each group are listed in table 1.
Observation and Results
TABLE 1: Profile of patients in the three groups
SVD – Single vessel disease, DVD = Double vessel disease, TVD = triple vessel disease. ACS = Acute coronary syndrome. Prox LAD = proximal left anterior descending artery, NYHA = New York Heart Association. CAD = Coronary artery disease. * includes patients at least a week after ACS. # Percentages calculated for patients available for followup. Percentages calculated for each group
FFR >0.8 FFR ≤ 0.8 Group I Medical
Group II Revascularized Group III Non-Revascularized PCI CABG
Total Number 90 144 31 17 Number on follow up 89 (98.8%) 144(100%) 31(100%) 17(100%) Mean Age (years) 57.7 57.9 54.8 55.9 Male (%) 77 81 90 88 Diabetes 43 (47.7%) 78 (54.2%) 23 (74.2%) 7 (41.2%) Hypertension 11 (12.2%) 82 (56.9%) 14 (45.1%) 10 (58.8%) Smoking 6 (6.6%) 113 (78.4%) 26 (83.2%) 12 (70.5%) Dyslipidemia 4 (4.4%) 48 (33.3%) 20 (64.5%) 8 (47.1%) Family history of CAD 1 (1.1%) 29 (20.1%) 9 (29.0%) 5 (29.4%) ≥ 2 CAD risk factors (%) 11 (12.2%) 92 (63.9)% 22 (71)% 12 (70.6%) NYHA III / IV at presentation (%) 7 (7.7%) 19 (13.2%) 11 (35.5%) 7 (41.2%) Stable IHD 78 (86.6%) 124 (86.1%) 28 (90.3%) 16 (94.1%) Recent ACS* 12 (13.7%) 20 (13.9%) 3 (9.7%) 1 (5.9%) Mean EF % 63.5% 61% 51.9% 53.2% SVD 43 (47.8%) 25 (17.4%) 0 0 DVD 30 (33.3%) 70 (48.6%) 15 (48.4%) 7 (41.2%) TVD 17 (18.9%) 49 (34.0%) 16 (51.6%) 10 (58.8%) Prox LAD >50% (%) 78 (86.7%) 138 (95.8%) 29 (93.5%) 16 (94.1%) Mean minimum stenosis diameter (mm) 1.58 1.02 1.24 1.07 Mean FFR 0.91 0.68 0.73 0.70 Median follow up (months) 21.7 (6 to 56) 18 (5 to 50) 15.8 (6 to 43) 14.1 (2 to 45) MACE 3 4 0 7 Medications at last followup #
Aspirin 89 (100%) 144 (100%) 31 (100%) 17 (100%) Clopidogrel 15 (16.9%) 138 (95.8%) 07 (22.6%) 06 (35.3%)
Statins 76 (85.4%) 142 (98.6%) 31 (100%) 17 (100%) Nitrates 04 (4.5%) 11 (7.6%) 01 (3.2%) 14 (82.3%)

Observation and Results
Figu
re: S
tudy
flow
All n
on-A
CS p
atie
nts
with
inte
rmed
iate
co
rona
ry le
sions
as
sess
ed b
y FF
R
n=28
1 FF
R ≤
0.8
n=19
2
Und
erw
ent P
CI /
CABG
n=
175
PC
I 144
; CAB
G 31
CV m
orta
lity
n= 0
Non
fata
l ACS
n=
4
Urg
ent r
evas
cula
rizat
ion
n= 0
Not
will
ing
for
reva
scul
ariza
tion
n= 1
7
CV m
orta
lity
n= 3
Non
fata
l ACS
n=
4
Urg
ent r
evas
cula
rizat
ion
n=1
FFR
> 0.
8 n=
89
OM
T n=
89
CV m
orta
lity
n= 0
Non
fata
l ACS
n=
2
Urg
ent r
evas
cula
rizat
ion
n= 1

Observation and Results
Table 2 : MACE in the three groups
Group I (n=89)
Group II PCI / CABG
(n=175)
Group III (n=17)
MACE 3 4 7 % of MACE 3.41 2.28 41.17 CV Death 3 Nonfatal ACS 2 4 4 Urgent Revascularisation 1 Group I= FFR >0.8, Group II= FFR<0.8 and underwent revascularization, Group III= FFR <0.8 and did not agree for revascularisation
281 (99.6%) patients had regular follow up in our interventional clinic at
3 weeks, 3 months, 6 months, 1 year after the procedure and thereafter yearly.
One patient was lost to followup in group 1. Mean follow up of patients was
17.9 months.
Three patients (3.4%) in Group 1 had MACE (1 STEMI who underwent
primary PCI , 2 Unstable angina – one of them underwent elective
revascularisation. 4 patients (2.3%) in Group 2 patients had admissions for
Non-STE-ACS (2 – UA, 2 NSTEMI). 7 patients (41.17%) in Group 3 had
MACE (3 death with acute LVF, 2 NSTEMI, 2 STEMI – of whom 1 needed
urgent revascularisation following an STEMI (rescue PCI involving FFR
assessed vessel), other was lysed, and later on underwent PCI electively
involving non-FFR assessed vessel. MACE rates were low and were not
significantly different in group 1 and group 2 (p=0.73).
Observation and Results
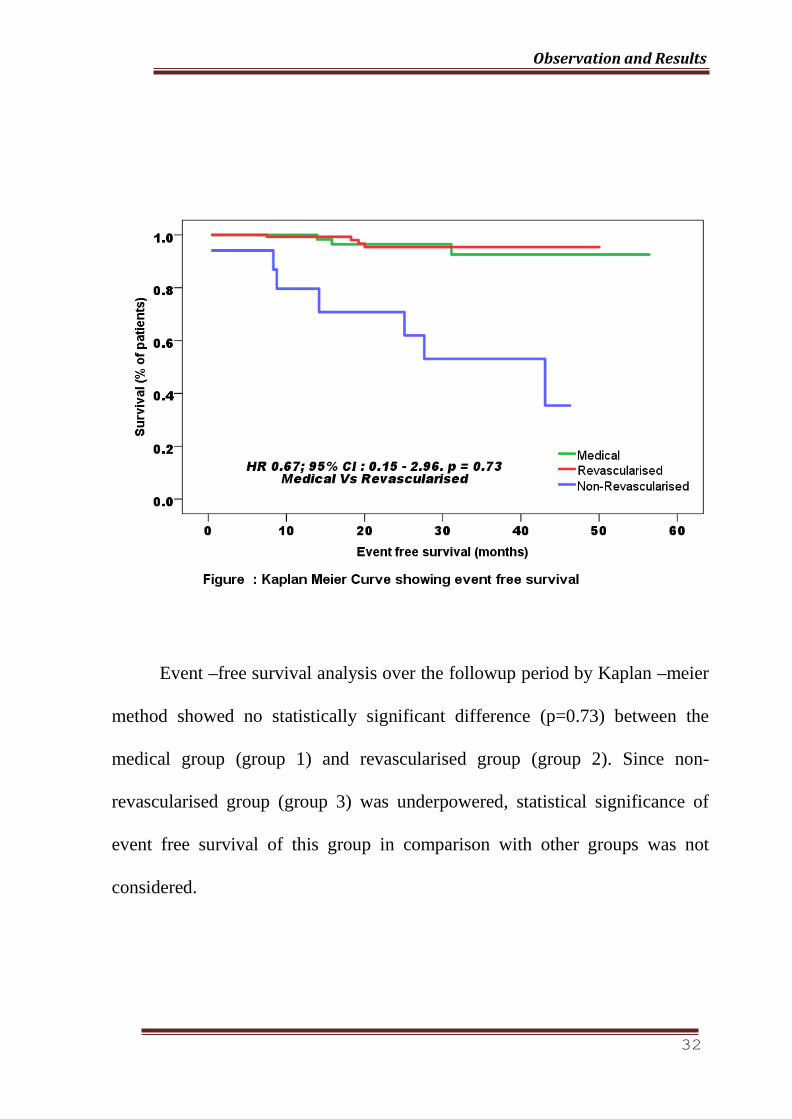
Event –free survival analysis over the followup period by Kaplan –meier
method showed no statistically significant difference (p=0.73) between the
medical group (group 1) and revascularised group (group 2). Since non-
revascularised group (group 3) was underpowered, statistical significance of
event free survival of this group in comparison with other groups was not
considered.

Discussion
Discussion
34
In this study, we compared the clinical outcomes of a FFR assessment
based coronary revascularisation. The strategy of medical management of
stenoses with FFR >0.80 and treating only stenoses that are hemodynamically
significant (<0.8) with revascularization appears safe as evidenced by the
similar MACE rates. Those patients who had coronary stenoses with FFR
<0.80 and refused to undergo revascularisation had higher MACE rates of
41.17%. Thus the results of the present study extend the usefulness of FFR in
clinical decision making in Indian patients with intermediate single or
multivessel disease.
In our observational study, we found a higher prevalence of patients with
positive FFR (68.1%). In the DEFER study, where enrollment was based
primarily on angiographic assessment of patients with negative stress test or
without a stress test, the prevalence of positive FFR was about 55%.(3)
However, in the all-comers FAME-2 study, which included consecutive
patients who underwent angiography for their symptoms and were found to
have at least 50% stenosis in coronary angiogram, 72% of the 1220 patients
who were eligible were found to have FFR < 0.8. This is similar to what was
found in our study, where the patients underwent angiogram for clinical
indications, with about 60% of the entire study population having had a positive

Discussion
35
or inconclusive stress test prior to angiography. The angiographic severity of
the lesion was assessed using quantitative coronary angiography (QCA)
algorithms, and it has been reported that QCA algorithms often yield lesser
stenotic severity when compared to visual assessment (20). This too would
have contributed to higher FFR positivity rates, unlike studies which mainly
employed visual assessment for severity estimation of lesions.
The clinical outcomes in patients who were kept on medical management
after negative FFR result were comparable to other studies. In DEFER
trial(3,7), which randomised patients with FFR ≥ 0.75 into deferred group and
PCI group showed that the 5-year event-free survival rates were statistically
comparable among both groups (80% versus 73%, P=0.52). Among the
deferred and PCI groups, composite rates of cardiac death and acute myocardial
infarction were 3.3% and 7.9% respectively. Therefore, the annual risk of
cardiac death or myocardial infarction in patients with normal FFR was <1%.
The study demonstrated that functionally nonsignificant coronary stenosis
could be safely deferred for up to 5 years, regardless of angiographic stenosis.
Among the patients who had FFR > 0.8 in the FAME-2 study (registry group),
the occurrence of MACE was 3% over one year (12,13,33,34). Many other
smaller studies(26–32) similarly have demonstrated consistently low rates of
death and myocardial infarction in patients with deferred treatment of lesions.

Discussion
36
Those patients who were advised revascularization based on the FFR
values and underwent the procedure in our study (group 2) had MACE rate of
2.3 % over 18 months. In the FAME-2 trial, the MACE rate was 4.3% at one
year in patients who underwent PCI. Our patients were younger (mean age of
56.3 years vs 63.5 years in FAME 2) and had fewer acute coronary events
before angiography (12% vs 37%). The definition of MACE in our study
(cardiovascular death, non fatal ACS, target vessel revascularization) and in
FAME 2 (any death, non fatal MI, any repeat revascularization ) was also
different. While the mode of revascularization was only PCI in FAME 2, our
patients underwent either PCI or CABG. These factors along with the shorter
duration of follow up might have contributed to the apparent difference in the
primary end point rates between the two studies.
There was remarkable difference in the MACE rates between patients
who underwent revascularization and those who refused it initially (2.3% vs
41.17%) in our study than what was reported in the FAME 2 trial (4.3 % in the
PCI group vs 12.7 % in the group with FFR <0.8 randomized to medical
management). This appears to be driven by a high rate of events in the group of
patients who refused revascularization initially in our study. The higher event
rates could be explained by higher risk profile (Diabetes 41.2% – vs 25%) ,
more patients with extensive coronary involvement (Multivessel disease 100%

Discussion
37
vs 22.3%), more symptomatic patients (NYHA FC III/ IV symptoms 41.2% vs
22.5%) in our study compared to FAME 2 trial.
To the best of our knowledge, this is the first Indian study of its nature.
Despite the differences in clinical profile of patients when compared with those
in randomised clinical trials, the data from this study which reflects real-world
practice, helps in reassuring the utility of FFR-based clinical decisions in
patients with CAD in this part of the world.
Limitations:
The study, being a retrospective and non-randomised one, limits
comparison of competing strategies.The smaller sample size in the third group
might have inflated the event rates.
.
Conclusion

Conclusion
39
Among patients with intermediate coronary artery disease having at
least one stenosis with a FFR of <0.80, FFR-guided PCI with drug eluting
stents or CABG plus medical therapy, as compared with the patients with
FFR of > 0.8 on medical therapy alone, had a similar rates of mortality, MI
and need for urgent revascularization.
This study also highlights the importance of timely revascularisation
in patients with ischemic FFR, as emphasized by higher MACE rate of 41%
among the patients with FFR of 0.80 or less but did not undergo
revascularisation.
Thus, we conclude that FFR based clinical decisions in the
management of patients with coronary artery disease is safe.
Bibliography
Bibilography
41
1. De Bruyne B, Sarma J. Fractional flow reserve: a review. Heart.
2008;94(7):949–59.
2. Wijns W, De Bruyne B, Vanhoenacker PK. What does the clinical
cardiologist need from noninvasive cardiac imaging: is it time to adjust
practices to meet evolving demands? J Nucl Cardiol. Jan;14(3):366–
70.
3. Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ,
Bartunek J Koolen JJ, et al. Measurement of fractional flow reserve to
assess the functional severity of coronary-artery stenoses. N Engl J
Med. 1996 Jun 27; 334(26):1703–8.
4. Pijls NH, van Son JA, Kirkeeide RL, De Bruyne B, Gould KL.
Experimental basis of determining maximum coronary, myocardial,
and collateral blood flow by pressure measurements for assessing
functional stenosis severity before and after percutaneous transluminal
coronary angioplasty. Circulation. 1993 Apr ;87(4):1354–67.
5. Botman K-J, Pijls NHJ, Bech JW, Aarnoudse W, Peels K, van Straten
B, et al. Percutaneous coronary intervention or bypass surgery in
multivessel disease? A tailored approach based on coronary pressure
measurement. Catheter Cardiovasc Interv. 2004 Oct;63(2):184–91.

Bibilography
42
6. Pijls NHJ, Klauss V, Siebert U, Powers E, Takazawa K, Fearon WF, et
al. Coronary pressure measurement after stenting predicts adverse
events at follow-up: a multicenter registry. Circulation [Internet]. 2002
Jun 25;105(25):2950–4.
7. Pijls NHJ, van Schaardenburgh P, Manoharan G, Boersma E, Bech J-
W, van’t Veer M, et al. Percutaneous coronary intervention of
functionally nonsignificant stenosis: 5-year follow-up of the DEFER
Study. J Am Coll Cardiol. 2007 May 29;49(21):2105–11.
8. Bech GJ, De Bruyne B, Pijls NH, de Muinck ED, Hoorntje JC,
Escaned J, et al. Fractional flow reserve to determine the
appropriateness of angioplasty in moderate coronary stenosis: a
randomized trial. Circulation. 2001 Jun 19;103(24):2928–34.
9. Ragosta M, Bishop AH, Lipson LC, Watson DD, Gimple LW,
Sarembock IJ, et al. Comparison between angiography and fractional
flow reserve versus single-photon emission computed tomographic
myocardial perfusion imaging for determining lesion significance in
patients with multivessel coronary disease. Am J Cardiol. 2007 Apr
1;99(7):896–902.
10. Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P,
Hunziker P, Mueller C, et al. Late clinical events after clopidogrel

Bibilography
43
discontinuation may limit the benefit of drug-eluting stents: an
observational study of drug-eluting versus bare-metal stents. J Am Coll
Cardiol. 2006 Dec 19;48(12):2584–91.
11. Shaw LJ, Berman DS, Maron DJ, Mancini GBJ, Hayes SW, Hartigan
PM, et al. Optimal medical therapy with or without percutaneous
coronary intervention to reduce ischemic burden: results from the
Clinical Outcomes Utilizing Revascularization and Aggressive Drug
Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008 Mar
11;117(10):1283–91.
12. Tonino PAL, Fearon WF, De Bruyne B, Oldroyd KG, Leesar MA, Ver
Lee PN, et al. Angiographic versus functional severity of coronary
artery stenoses in the FAME study fractional flow reserve versus
angiography in multivessel evaluation. J Am Coll Cardiol. 2010 Jun 22
Apr 15];55(25):2816–21.
13. Tonino PAL, De Bruyne B, Pijls NHJ, Siebert U, Ikeno F, van `t Veer
M, et al. Fractional Flow Reserve versus Angiography for Guiding
Percutaneous Coronary Intervention. N Engl J Med. 2009 Jan
15;360(3):213–24.
14. Berger A, Botman KJ, MacCarthy PA. Long-Term Clinical Outcome
After Fractional Flow Reserve-Guided Percutaneous Coronary

Bibilography
44
Intervention in Patients With Multivessel Disease. ACC Curr J Rev.
2005;14(11):48–9.
15. Li J, Elrashidi MY, Flammer AJ, Lennon RJ, Bell MR, Holmes DR, et
al. Long-term outcomes of fractional flow reserve-guided vs.
angiography-guided percutaneous coronary intervention in
contemporary practice. Eur Heart J. 2013;34(18):1375–83.
16. Pais P, Pogue J, Gerstein H, Zachariah E, Savitha D, Jayprakash S, et
al. Risk factors for acute myocardial infarction in Indians: a case-
control study. Lancet (London, England). 1996 Aug
10;348(9024):358–63.
17. Gupta SR, Gupta SK, Reddy KN, Moorthy JS, Abraham KA. Coronary
artery disease in young Indian subjects. Indian Heart J. Jan;39(4):284–
7.
18. Kuppuswamy V, Gupta S. Coronary heart disease in South Asians.
Practitioner. 2003 Mar;247(1644):181–2, 186–8, 190 .
19. Lip GY, Rathore VS, Katira R, Watson RD, Singh SP. Do Indo-Asians
have smaller coronary arteries? Postgrad Med J. 1999;75(886):463–6.
20. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Alpert JS, White HD,
et al. Third universal definition of myocardial infarction. Eur Heart J.

Bibilography
45
2012;33:2551–67.
21. Lima RSL, Watson DD, Goode AR, Siadaty MS, Ragosta M, Beller
GA, et al. Incremental value of combined perfusion and function over
perfusion alone by gated SPECT myocardial perfusion imaging for
detection of severe three-vessel coronary artery disease. J Am Coll
Cardiol. 2003 Jul 2 ;42(1):64–70.
22. Melikian N, De Bondt P, Tonino P, De Winter O, Wyffels E, Bartunek
J, et al. Fractional flow reserve and myocardial perfusion imaging in
patients with angiographic multivessel coronary artery disease. JACC
Cardiovasc Interv. 2010 Mar;3(3):307–14.
23. Berger A, Botman K-J, MacCarthy PA, Wijns W, Bartunek J,
Heyndrickx GR, et al. Long-term clinical outcome after fractional flow
reserve-guided percutaneous coronary intervention in patients with
multivessel disease. J Am Coll Cardiol]. 2005 Aug 2];46(3):438–42.
24. Li J, Elrashidi MY, Flammer AJ, Lennon RJ, Bell MR, Holmes DR, et
al. Long-term outcomes of fractional flow reserve-guided vs.
angiography-guided percutaneous coronary intervention in
contemporary practice. Eur Heart J . 2013 May;34(18):1375–83.
25. Yamane T. Long-Term Follow-Up After Deferral of Percutaneous
Bibilography
46
Coronary Intervention (PCI) in Patients With Moderate Coronary
Lesions and Borderline Fractional Flow Reserve Measurements.
Circulation; 2008. p. 118: 895.
26. Pijls NHJ, Fearon WF, Tonino PAL, Siebert U, Ikeno F, Bornschein B,
et al. Fractional flow reserve versus angiography for guiding
percutaneous coronary intervention in patients with multivessel
coronary artery disease: 2-year follow-up of the FAME (Fractional
Flow Reserve Versus Angiography for Multivessel Evaluation) study. J
Am Coll Cardiol. 2010 Jul 13];56(3):177–84.
27. Oud N, Marques KM, Bronzwaer JGF, Brinckman S, Allaart CP, de
Cock CC, et al. Patients with coronary stenosis and a fractional flow
reserve of ≥0.75 measured in daily practice at the VU University
Medical Center. Neth Heart J]. 2010 Sep];18(9):402–7.
28. Legalery P, Schiele F, Seronde M-F, Meneveau N, Wei H, Didier K, et
al. One-year outcome of patients submitted to routine fractional flow
reserve assessment to determine the need for angioplasty. Eur Heart J.
2005 Dec;26(24):2623–9.
29. Mates M, Hrabos V, Hajek P, Rataj O, Vojacek J. Long-term follow-
up after deferral of coronary intervention based on myocardial
fractional flow reserve measurement. Coron Artery Dis. 2005 May

Bibilography
47
;16(3):169–74.
30. Meuwissen M, Chamuleau SAJ, Siebes M, de Winter RJ, Koch KT,
Dijksman LM, et al. The prognostic value of combined intracoronary
pressure and blood flow velocity measurements after deferral of
percutaneous coronary intervention. Catheter Cardiovasc Interv. 2008
Feb 15;71(3):291–7.
31. Reczuch K, Jankowska E, Porada A, Telichowski A, Derkacz A,
Banasiak W, et al. Long-term outcome of conservatively treated
patients with borderline coronary lesions--role of the fractional flow
reserve measurement. Kardiol Pol. 2005 Jan;62(1):6-11-3.
32. Bech GJ, De Bruyne B, Bonnier HJ, Bartunek J, Wijns W, Peels K, et
al. Long-term follow-up after deferral of percutaneous transluminal
coronary angioplasty of intermediate stenosis on the basis of coronary
pressure measurement. J Am Coll Cardiol. 1998 Mar 15 ;31(4):841–7.
33. De Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, et
al. Fractional flow reserve-guided PCI versus medical therapy in stable
coronary disease. Vol. 367, New England Journal of Medicine. 2012.
991-1001. p.
34. Van Nunen LX, Zimmermann FM, Tonino PAL, Barbato E, Baumbach
Bibilography
48
A, Engstrøm T, et al. Fractional flow reserve versus angiography for
guidance of PCI in patients with multivessel coronary artery disease
(FAME): 5-year follow-up of a randomised controlled trial. Lancet
(London, England). 2015 Dec 7;386(10006):1853–60.
49
Appendix

9%SIMILARITY INDEX
1
2
3
4
5
6
Srinivasa_Thesis.docx ORIGINALITY REPORT
PRIMARY SOURCES
Berger, A.. "Long-Term Clinical Outcome AfterFractional Flow Reserve-Guided PercutaneousCoronary Intervention in Patients With Multivessel Disease",Journal of the American College of Cardiology, 20050802CrossCheck
Li, J., M. Y. Elrashidi, A. J. Flammer, R. J. Lennon, M.R. Bell, D. R. Holmes, J. F. Bresnahan, C. S. Rihal, L.O. Lerman, and A. Lerman. "Long-term outcomes of fractionalflow reserve-guided vs. angiography-guided percutaneouscoronary intervention in contemporary practice", European HeartJournal, 2013.CrossCheck
De Bruyne, Bernard, Nico H.J. Pijls, Bindu Kalesan,Emanuele Barbato, Pim A.L. Tonino, Zsolt Piroth,Nikola Jagic, Sven Mobius-Winckler, Gilles Rioufol, Nils Witt, PetrKala, Philip MacCarthy, Thomas Engström, Keith G. Oldroyd,Kreton Mavromatis, Ganesh Manoharan, Peter Verlee, OleFrobert, Nick Curzen, Jane B. Johnson, Peter Jüni, and William F.Fearon. "Fractional Flow Reserve–Guided PCI versus MedicalTherapy in Stable Coronary Disease", New England Journal ofMedicine, 2012.CrossCheck
www.cvrf.orgInternet
171.67.121.207Internet
www.cardiovascmed.chInternet
126 words — 3%
69 words — 2%
30 words — 1%
21 words — 1%
19 words — 1%
17 words — < 1%

7
8
EXCLUDE QUOTES ON
EXCLUDE BIBLIOGRAPHY ON
EXCLUDE MATCHES OFF
content.onlinejacc.orgInternet
doria.f iInternet
16 words — < 1%
15 words — < 1%
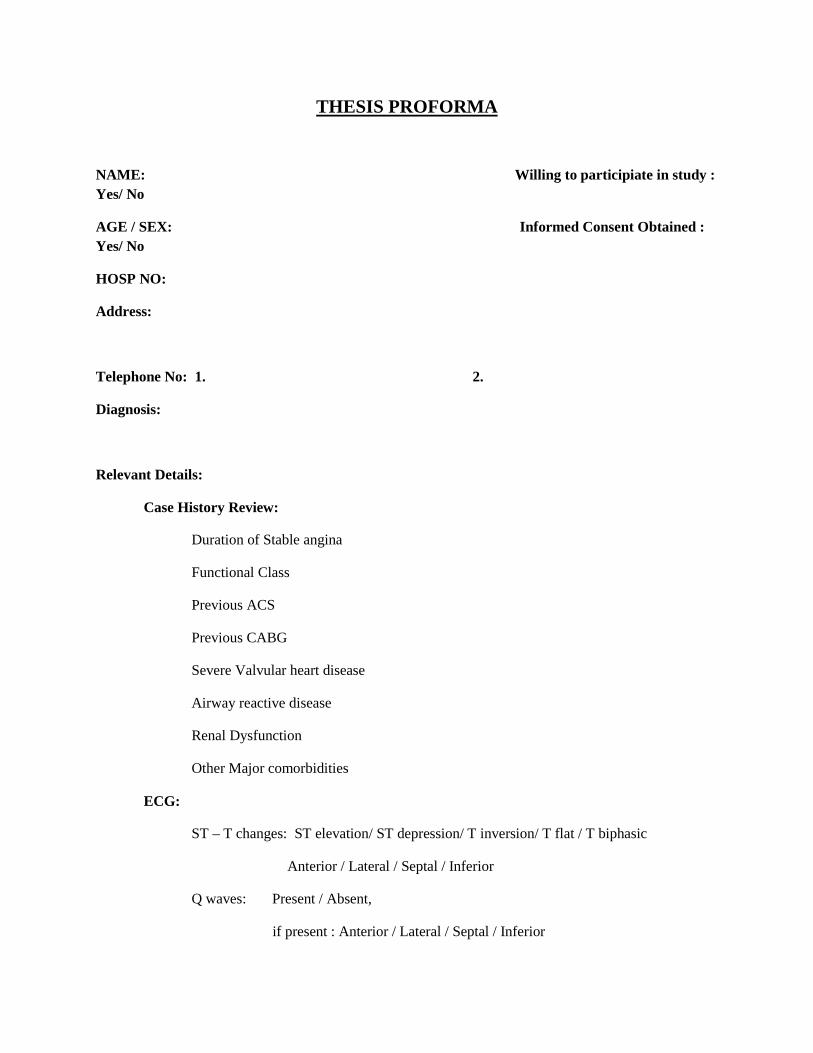
THESIS PROFORMA
NAME: Willing to participiate in study : Yes/ No
AGE / SEX: Informed Consent Obtained : Yes/ No
HOSP NO:
Address:
Telephone No: 1. 2.
Diagnosis:
Relevant Details:
Case History Review:
Duration of Stable angina
Functional Class
Previous ACS
Previous CABG
Severe Valvular heart disease
Airway reactive disease
Renal Dysfunction
Other Major comorbidities
ECG:
ST – T changes: ST elevation/ ST depression/ T inversion/ T flat / T biphasic
Anterior / Lateral / Septal / Inferior
Q waves: Present / Absent,
if present : Anterior / Lateral / Septal / Inferior

ECHO:
RWMA: Anterior / Lateral / Septal / Inferior
Severe Valvular Heart disease
CAG Findings:
Date of procedure:
SVD/ DVD/ TVD
Left Main involvement : Yes/ No
Coronary lesions assessed:
Visual assessment of Severity*
FFR IVUS/ OCT# (Findings)
Decision ( PCI/ OMT)
Comments
1
2
3
* Visual assessment of severity would be reviewed by 2 cardiologists # if used for same vessel/ lesion

FOLLOW UP REVIEW
Date of Review: Telephonic / Hospital review
Procedure to review duration: months
Death : Yes / No
If Yes , Date and time:
Cause : cardiac / Noncardiac
Details of cause of death
Myocardial Infarction: Yes/ No Date and Time:
ECG : STEMI / NSTEMI
Details:
Cardiac Biomarker: Elevated/ Not elevated
Details:
Serial Levels:
Date & Time Biomaker Value
Repeat coronary angiogram/ revascularisation of study vessel
Date of procedure:
Revascularization: Done / Not needed
CAG Details:

CONSENT
Study on clinical outcomes in patients who underwent FFR study in borderline coronary lesions among stable angina patients is a observational study to assess the predictive role of FFR on subsequent clinical outcome in patients with chronic stable angina. This study aims to study the natural history of chronic stable angina patients who undergo FFR study for decision of revascularisation and correlate it to long term outcomes in patients with structural heart disease. The doctor performing the study has explained to me in detail about the scientific basis of this study. He has also explained to me about my role as a subject in the study. The doctor also explained that there is no risk involved as this is an observational study. I realize that I am participating in a scientific study which I agree to after realizing the issues involved. I realize that there will be no differences in my treatment and it will not increase the cost of management of my disease if I participate in this study. I am voluntarily participating in this study and i am aware of the right to refuse the consent for participating in this study at any juncture. The doctor has assured me that my personal identity will be protected during the study. I realize that I may not have any direct benefits from participating in this study. However the information collected during this study may be useful for other patients in future who will require management of arrythmias in future. Being aware of the above mentioned facts, I agree to participate in this study. Signature of patient/relative: Name of patient: Date: Signature of doctor: Name of doctor: Date: Contact address: Dr Srinivasa Prasad SR, Dept of Cardiology SCTIMST, Trivandrum

k½-X-]{Xw
tÌ_nÄ B³Pn\ tcmKnIÄ¡nSbnepÅ t\cnb lrZb XSn¸pIfpÅ, F^v. F^v.
BÀ ]T\¯n\v hnt[bcmb tcmKnIfpsS NnInÂkm^e§fpsS ]T\w KpcpXcamb
tÌ_nÄ B³Pn\ tcmKnIfnse NnInÂkm]camb ^e§fpsS Hcp ap³kqNIsa¶
\nebnepÅ F^v. F^v. Bdnsâ ]¦ns\ hnebncp¯m\pÅ Hcp \nco£W
]T\amWv. dnhmkv¡pessdtkj³ Xocpam\n¡m³ thn F^v. F^v. BÀ
]T\¯n\v hnt[bcmb KpcpXcamb tÌ_nÄ B³Pn\ tcmKnIfpsS kzm`mhnI
Ncn{Xhpw lrZb¯nsâ LS\m]camb AkpJ§fpÅ tcmKnIfpsS ZoÀLImes¯
^e§fpw X½nepÅ ]ckv]c_Ôw I¯m\mWv Cu ]T\w. Cu ]T\¯nsâ
imkv{XobmSnØm\s¯¸än ]T\w \S¯p¶ tUmIvSÀ F\n¡v hniZambn hnhcn¨p
X¶p. Cu ]T\¯nse ]¦mfnsb¶ \nebn Fsâ ]¦ns\¸änbpw hniZoIcn¨p.
CsXmcp \nco£W ]T\w am{XamIbm Zojy`e§fpmhnsöpw tUmIvSÀ
hniZoIcn¨p.
DÄs¡mÅp¶ {]iv\§Ä AndªpsImv Rm³ k½Xw \ÂIn ]s¦Sp¡p¶Xv
Hcp imkv{Xob ]T\amsW¶v Rm³ a\Ênem¡p¶p. Cu ]T\¯n Rm³
]s¦Sp¡p¶XpsImv Fsâ NnInÂkbn amä§fpmInsöpw
FsâcmKwssIImcyw sN¿p¶Xn A[nI¨nehpmInsöpw Rm³
a\Ênem¡p¶p.Rm³ kzbtah Cu]T\¯n ]s¦Sp¡pIbmWv. GXp L«¯nepw
Cu ]T\¯n ]s¦Sp¡p¶Xn hnk½Xw Adnbn¡msa¶pw F\n¡dnbmw.
]T\Ime¯v Fsâ hyànhnhc§Ä kwc£n¡psa¶v tUmIvSÀ F\n¡v Dd¸v
X¶n«pv.
F\n¡v Cu ]T\¯n \n¶pw t\cn«v KpWapmhnsödnbmw. F¶ncp¶mepwCu
]T\¯neqsS tiJcn¡p¶ hnhc§Ä `mhnbn Acßnbmkv ssIImcyw
sN¿s¸tS tcmKnIÄ ¡v {]tbmP\{]Zamtb¡mw. apIfn ]dª hkvXpXIÄ
a\Ênem¡ns¡mv Cu ]T\¯n ]s¦Sp¡phm³ Rm³ k½Xn¡p¶p.
tcmKnbpsS / _Ôphnsâ H¸v :
tcmKnbpsS t]cv :
XobXn :
tUmIvSdpsS H¸v
tUmIvSdpsS t]cv :
XobXn :
_Ôs¸Sm\pÅ taÂhnemkw
tUm. {io\nhmk {]kmZv
FkvBÀ, ImÀUntbmfPn Un¸mÀ«vsaâv
Fkv. kn. än. sF. Fw Fkv. än, Xncph\´]pcw.

k½X]{Xw
BapJw
DcÊnse sshIey§Ä¡pw acW¯n\panSbm¡p¶
{][m\ImcW§fnsem¶mWv lrZbcà¡pgense tcmKw.
lrZbip²cà¡pgense kwibn¡s¸Sp¶tXm ØncoIcn¡s¸«tXm
BbtcmK¯n\v A\ptbmPyamb NnInÕ¡v, hfsc IrXyXbmÀ¶
imcocnI hnebncp¯ensâbpw IrXyamb {]hÀ¯\ hnhc§fpsSbpw
kamlrXamb hnhcw A\nhmcyamWv.cà¡pgen kvsäâv Ahiytam
F¶v Xocpam\n¡p¶Xn F^v F^v Bdnsâ ]¦ns\¸än ]e ]T\§fpw
\S¯pIbpw cà¡pgense XSn¸pIfpsS {]kàn hnebncp¯p¶Xn\v
\nÀt±in¡s¸«n«pv.
{^m£WÂ ^vtfm dnkÀhv (F^v F^v BÀ) Ìnt\mknkv KpcpXcm
hØbpsS càNw{IaW¯nse {]kàamb kqNI§fnsem¶pw
tcmK\nÀ®b¯nsâ IrXyXbn atbmImÀUnb s]À^yqj\p
kam\hpw ]s£ IpSpX hyàXIbmÀ¶XpamWv. Cu kqNIw
IXoässdtkj³ ]co£Wimebn Ipd¨p\nanj§Ä¡Iw Ffp¸¯nÂ
Af¡mhp¶Xn\m icoc¯n IS¡msXbpÅ ]cntim[\IÄ¡v
]Icam¡mhp¶XpamWv.
F^v F^v Bdns\ ASnØm\am¡nbpÅ Xocpam\§fpsS NnInÕm^ew
hyXyØ ]co£W§fn hnebncp¯nbn«pv, IqSpXepw \nb{´nXamb
kmlNcy§fnse NnInÕm]co£W§fnemWv. \nc´camb NnInÕm
cwK¯v A¯c¯nepÅ hnhc§Ä e`n¡p¶Xn\v ]cnanXnbpv.
C´ybnÂ, F^v F^v BÀ \nc´camb NnInÕm cwK¯v
D]tbmKn¡n¡p¶Xv D¶X NnInÕmtI{´§fnembn ]cnanXs¸«ncn¡p¶p.
C´y/Gjy¡mcmb lrZb ip²cà¡pg tcmKnIfnÂ,
`qanimkv{Xhpw, A]ISkm[yXbpsS hnhchpw, Øm`mhnI Ncn{Xhpw Nne
A\p]aambLSI§fmb sNdp¸amb {]mb¡mcpsSIq«w, {][m\ambpw
]N\kw_Ônbmb e£W§Ä, sImfkvt{SmÄ k¼¶amb Blmchpw
IqSnhcp¶ Ccp¶pÅ PohnX ssienbpw _m[n¡p¶p. ]mÝmXysc
At]£n¨v sNdnb cà¡pgepIfpÅ C´y³ tcmKnIfpsS F^v F^v BÀ
{]ImcapÅ NnInÕmhnhc§Ä ipivdqjbpsS KpWta· IqSpXÂ
i¡ns¸Sp¯p¶Xn\v AhiyamWv.
Cu ]T\¯nsâ Dt±isa´v
2005 apXÂ F^v F^v Bdn\v hnt[bcmb apgph³ tcmKnIfpsSbpw
sshZyimkv{X hnhc§Ä tiJcn¡phm³ Cu ]T\w Dt±in¡p¶p.
BtcmKnIfpsS NnInÕm^e§ÄImImbn Cu hnhc§Ä imkv{Xobambn
hniIe\w sN¿pw.
Cu ]T\sa´n\v
F^v F^v BÀ ASnØm\am¡nb dnhmkvIpessdtkj³ NnInÕm^e§Â
sa¨s¸Sp¯psa¦n tcmKnIfpsS NnInÕ^e§Ä sa¨s¸Sp¯phm³
Øncambn NnInÕm cwK¯v D]tbmKs¸Spsa¶v R§Ä hnizkn¡p¶p.
A\phmZwXcp¶ tcmKnsb¶\nebn Xm¦fpsS ]s¦´v.
Cu ]T\w Xm¦fpsS NnInÕbntem, ]cntim[\Ifntem `mhnNnInÕm
coXnIfntem HcpXc¯nepapÅ hyXymkapm¡p¶nÃ. Bip]{Xnbnse
Xm¦fpsS NnInÕm hnhc§Ä tiJcn¡pIbpw imkvXobamb hniIe\w
sN¿pIbpw am{XamWv. AXv Xm¦Ä¡v A[nI Nnehv Dm¡pIbnÃ.
Xm¦fpsS hyànhnhc§Ä Hcn¡epw {]kn²s¸Sp¯IbnÃ. Xm¦fpsS
kzImcyX kwc£n¡s¸Spw, Xm¦fpsS NnInÕm hniZmwi§fpÄs¸sS
hniZmwi§tfm hyànXztam {]kn²s¸Sp¯pIbnÃ.
Xm¦Ä¡v CXn ]s¦Spt¡¦ntem ]T\¯n\nSbn ]n³hm§W
sa¦ntem F´mIpw.
Cu ]T\¯n ]s¦Sp¡m\pÅ £Ww \nckn¡pItbm ]T\¯n\nSbnÂ
]n³hm§pItbm sN¿p¶Xv HcpXc¯nepw Cu Øm]\¯n \n¶pÅ
Xm¦fpsS NnInÕsb _m[n¡nÃ. Cu ]T\¯n ]s¦Sp¡m\pÅ
Xm¦fpsS k½Xw ]qÀ®ambpw kztbhbpÅXpw ]n¶oSv Xm¦Â¡v
Ft¸mÄ thWsa¦nepw XpScmXncn¡mhp¶XpamWv.
k½X]{Xw
eJphmb cà¡pg XSn¸n\pÅ F^v F^v BÀ ASnØm\am¡nb
dnhmkvIpessdtkj\v hnt[bcmb KpcpXchpw Ønchpamb B³ssP\
tcmKnIfpsS NnInÕm^e§sf¸dndn Hcp ]T\w Fkv. kn. än. sF. Fw.
Fkv. än \S¯p¶Xmbn F\n¡dnbmw.
Fs¶ Cu ]T\¯n ]¦mfnbmhm³ £Wn¨n«pv. GItZiw 400 F^v
F^v Bdn\v hnt[bcmb tcmKnIsf CXnepÄs¸Sp¯nbn«ps¶v
F\n¡dnbmw.Bip]{Xn {]thi\kab¯pw AXn\ptijapÅ XpSÀ
]cntim[\bpsSbpw NnInÕmtcJIÄ tiJcn¡pIbpw hniIe\w
\S¯pIbpw sN¿psa¶v Ft¶mSv ]dªp. Fkv. kn. än. sF. Fw. Fkv.
än ImÀUntbmfPn Un¸mÀ«vsaânepÅ Hcp tUmIvSÀ Fsâ
NnInÕmhnhc§Ä hniZambn Bip]{Xn tcJIfn \n¶v tiJcn¡psa¶v
Rm³ a\Ênem¡p¶p. XncsªSp¸nsâ BZyL«¯n am{Xta Fsâ
hyànhnhc§Ä D]tbmKn¡pIbpÅp F¶pw tijapÅ
hniIe\L«¯n Fsâ FÃm hyànhnhc§fpw FSp¯pamäpsa¶pw
Fs¶ Adnbn¨n«pv. F\n¡v GXpL«¯nepw ]T\¯nÂ\n¶pw ImcWw
ImWn¡msX ]n³hm§m³ ]qÀ® kzmX{´aps¶pw A§s\
FbvXpsImv Fsâ tcmKXn\mhiyamb NnInÕXpScmsa¶pw Ft¶mSv
]dªp. F\n¡v Cu ]T\hpambn _Ôs¸«v IqSpX hnhc§Ä¡mbn
{][m\ KthjIs\tbm (]\¯nse F¯nIvkv I½nän) tbtbm F\n¡v
_Ôs¸Smw.
Ft¶mSv Fsâ amXr`mjbn apIfn kqNn¸n¨ hnhc§Ä
hniZoIcn¡pIbpw F\v\sd kwib§Ä ]cnlcn¡m³ Ahkcw
e`n¡pIbpwsNbvXp. Rm³ Cu ]T\¯n DÂs¸Sp¯m³ ]qÀ®amb
k½Xw \ÂIp¶p.
H¸v
tcmKnbpsS t]cv
hnemkw
XobXn
km£n