student workbook cpr & aed - emssafetyservices.com · thrust, use the head tilt/chin lift. the...
TRANSCRIPT

CPR & AEDfor Professional Rescuers
Emergency Response for Healthcare Providers and Professional Rescuers
2010 Guidelines
Quality Training Programs:
Basic First AidAdvanced First Aid
CPR & AED for the Community & WorkplaceCPR & AED for Healthcare and Professional Rescuers
CPR & First Aid for Childcare ProvidersCPR, AED, & First Aid for the Senior Community
Oxygen AdministrationBloodborne Pathogens
Instructor Training
Available in Spanish
EMS Safety Services, Inc.1046 Calle Recodo, Suite KSan Clemente, CA 92673(800) 215-9555www.emssafety.com
Student Workbook
23
23
24
23
11
10
9
30
5
34
36
16
18
20
13
31
32
8
7
30
33
16
18
20
22
AED - Implanted Devices
AED - Medication Patches
AED Safety
AED Troubleshooting
AED Use
Bag Mask
Barriers- CPR
Bloodborne Pathogens
C-A-B
Choking- Adult or Child
Choking- Infant
CPR - Adult
CPR - Child
CPR - Infant
CPR - Team
Glove Removal
Heart Attack
Recovery Position
Rescue Breathing
Standard Precautions
Stroke
Unresponsive- Adult
Unresponsive- Child
Unresponsive- Infant
Vomiting
CPR and aEd foR PRofEssional REsCuERsEmERgEnCy REsPonsE foR HEaltHCaRE PRovidERs and
PRofEssional REsCuERs
Copyright © 2011 EMS Safety ServiceS, inc.iSBn: 978-1-937012-02-1
All rights reserved. No part of this publication may be reproduced or used in any form, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without the prior written permission of the publisher.
The emergency care procedures described in this manual are based on the most current recommendations of responsible sources at the time of publication. Meets 2010 Guidelines from the ILCOR International Consensus on CPR and ECC Science with Treatment Recommendations, as published by the American Heart Association, and the International First Aid Science Advisory Board. It is the reader’s responsibility to stay informed of changes in recommendations or information on emergency care procedures. EMS Safety Services does not guarantee or assume responsibility for the completeness, correctness or sufficiency of such information or recommendations. Other or additional safety measures may be required under particular circumstances. EMS Safety Services is not responsible for, and expressly disclaims liability for, damages of any kind arising out of use, reliance on, performance of, or reference to such information. Local or organizational treatment protocols may supersede treatment recommendations in this program.
CPR/First Aid training materials meet Federal OSHA compliance standards.CPR/First Aid material references available upon request.
PRintEd in tHE unitEd statEs of amERiCa
Emergency Index

CPR and AED for Professional Rescuers
Emergency Response for Healthcare Providers and Professional Rescuers
EMS SafEty SErvicES, inc.1046 callE rEcodo, SuitE K
San clEMEntE, ca 92673(800) 215-9555 fax (949) 388-2776
www.emssafety.com

Table of ConTenTs
introductionFirst aid is the initial care given by a responder with little or no equipment to someone who is injured or suddenly becomes ill. This course is designed to give responders the knowledge and skills needed to respond confidently and effectively in an emergency. The goal of our training is to make your community, home and work environment safer by preventing illness and injury as well as quickly recognizing and responding to emergencies to save a life or reduce disability.
You will learn by a combination of DVD, workbook, lecture and demonstration. After practicing certain skills, you will take a written exam and your Instructor will test your skills. Once you have successfully completed this course, you will receive an EMS Safety Services course completion card.
The CPR, AED and First Aid training programs by EMS Safety Services have been reviewed, approved, or meet the guidelines of numerous federal, state and local agencies, organizations and regulatory bodies, including OSHA, CECBEMS, USCG, the Joint Commission, and state Health, Human Services, and EMS departments.
EMS Safety Services’ programs are used by businesses, organizations, schools, government agencies, healthcare and public safety personnel, and independent instructors.
If you are allergic to latex, please tell your Instructor before the course begins.
Thank you for participating in this EMS Safety Services course.
Chain of Survival ...........................................3
CPR Overview ...............................................4
C-A-B .............................................................5
Recovery Position ..........................................8
CPR Barrier Devices .....................................9
Bag Mask .......................................................10
Using an AED ................................................11
Team CPR .....................................................13
Adult CPR ......................................................16
Child CPR ......................................................18
Infant CPR .....................................................20
Special Considerations-CPR .........................22
Special Considerations-AED .........................23
AED Safety ....................................................24
CPR at-a-Glance ...........................................25
How Would You REACT? ...............................26
Responding to Emergencies ..........................27
Legal Issues ..................................................29
Protection from Infection ................................30
Heart Attack ...................................................32
Stroke ............................................................33
Adult or Child Choking ...................................34
Infant Choking ...............................................36
How Would You REACT? ...............................37
Advanced Equipment.....................................38

33
Chain of survival
The pediatric chain of survival is slightly different, with an emphasis on prevention.
The percent of adults with out-of-hos-pital cardiac arrest who receive by-stander CPR.
Heart disease is the leading cause of death among adults in the United States. In many cases, heart disease leads to sud-den cardiac arrest (SCA). About 70% of heart attack-related deaths occur before the victim reaches the hospital, most of them within the first 4 hours after symptoms begin. The links in the chain of survival are the critical actions taken in saving the life of someone in sudden cardiac arrest. The first two links in the chain of survival are usually provided by a bystander. Activating EMS, early CPR and early defibrillation have the most impact on potential for survival, and the most room for improvement.
Activate Emergency Medical Services
A bystander must first recognize cardiac arrest, then quickly activate the emergency response system, usually by dialing 9-1-1. Early recognition and action saves lives!
Early CPR
Start CPR immediately after cardiac arrest, and perform high quality compressions to improve the cardiac arrest vic-tim’s chance of survival.
Early Defibrillation
Defibrillation is critical to survival of SCA. When high quality CPR is combined with rapid defibrillation, a victim has the best chance of survival.
Early Advanced Care
Advanced Life Support, such as advanced airway manage-ment and drug therapy, is handled by specially trained med-ical professionals on scene and en route to the hospital.
Post-Arrest Care
Comprehensive, organized treatment in the hospital is pro-vided by many different healthcare disciplines to improve the chance of survival with the least amount of disability.
Early advanced care
Early defibrillation
Early CPR
Activate emergency medical services
<30%Tip
4
CPr overview
Cardiopulmonary Resuscitation
What is an AED?
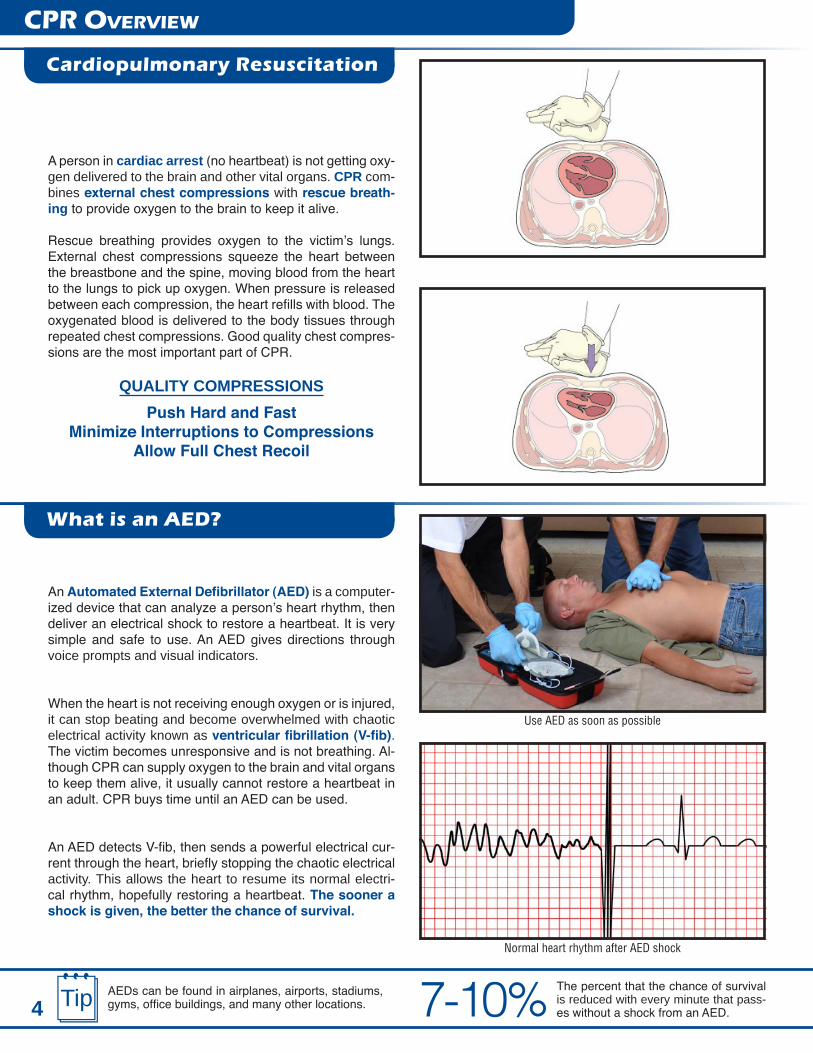
A person in cardiac arrest (no heartbeat) is not getting oxy-gen delivered to the brain and other vital organs. CPR com-bines external chest compressions with rescue breath-ing to provide oxygen to the brain to keep it alive.
Rescue breathing provides oxygen to the victim’s lungs. External chest compressions squeeze the heart between the breastbone and the spine, moving blood from the heart to the lungs to pick up oxygen. When pressure is released between each compression, the heart refills with blood. The oxygenated blood is delivered to the body tissues through repeated chest compressions. Good quality chest compres-sions are the most important part of CPR.
QUALITY COMPRESSIONSPush Hard and Fast
Minimize Interruptions to CompressionsAllow Full Chest Recoil
An Automated External Defibrillator (AED) is a computer-ized device that can analyze a person’s heart rhythm, then deliver an electrical shock to restore a heartbeat. It is very simple and safe to use. An AED gives directions through voice prompts and visual indicators.
When the heart is not receiving enough oxygen or is injured, it can stop beating and become overwhelmed with chaotic electrical activity known as ventricular fibrillation (V-fib). The victim becomes unresponsive and is not breathing. Al-though CPR can supply oxygen to the brain and vital organs to keep them alive, it usually cannot restore a heartbeat in an adult. CPR buys time until an AED can be used.
An AED detects V-fib, then sends a powerful electrical cur-rent through the heart, briefly stopping the chaotic electrical activity. This allows the heart to resume its normal electri-cal rhythm, hopefully restoring a heartbeat. The sooner a shock is given, the better the chance of survival.
Use AED as soon as possible
Normal heart rhythm after AED shock
The percent that the chance of survival is reduced with every minute that pass-es without a shock from an AED.
AEDs can be found in airplanes, airports, stadiums, gyms, office buildings, and many other locations. 7-10%Tip

51 5
C-A-B
Assessment
C-A-B stands for Compression, Airway, and Breathing. Starting CPR in this sequence gives a victim of sudden cardiac arrest the best chance of survival. The C-A-B sequence is used for unresponsive victims of all ages.
When you arrive at the victim’s side, check for response. Tap his shoulder and shout, “Are you all right?” Look for any response such as eyes opening, moaning, or talking. While checking for response, check for breathing by visu-ally scanning the victim’s chest for 5-10 seconds.
If no response and no breathing or only gasping, yell for help and have someone activate EMS and get the AED.
Check for a pulse for 5-10 seconds.
Check the carotid pulse for an adult or child. Locate the trachea (close to the Adam’s apple) and slide 2 or 3 fingers into the groove between the trachea and the muscles of the neck.
Check the brachial pulse for an infant
Check the carotid pulse for an adult or child
Check response and breathing
The number of minutes it takes for a rescuer to start to fatigue and give shallow chest compressions.
The number of minutes before a rescuer realizes that he or she is fatigued.
if aloneA professional rescuer who is responding alone should adjust his or her actions according to the most likely cause of cardiac arrest.
• Adult victim: Go activate EMS and get the AED now, then return and check pulse. If no definite pulse, begin CPR.
• Child or infant victim: Perform CPR for 2 minutes, then go activate EMS and get the AED. Return and continue CPR.
• Witnessed, sudden collapse: Go activate EMS before beginning CPR for any age victim.• Asphyxial arrest: Perform CPR for 2 minutes, then go activate EMS for any age victim. Return and continue
CPR.
Check the brachial pulse for an infant. Use 2-3 fingers to feel the inside of the upper arm between the elbow and shoulder.
If no definite pulse, begin chest compressions.

6
C-A-B
If you can’t effectively open the airway with the jaw thrust, use the head tilt/chin lift.
The number of minutes from drop to shock when AED use is most successful.
Airway
Compressions
<3
Jaw ThrustUse the jaw thrust (without a head tilt) to open the airway when a head or neck injury is suspected. Do not move the cervical spine.
1. Determine if the jaw thrust is needed.• Suspected head or neck injury• Severe trauma
2. Kneel at the head of the victim and rest your elbows on the surface the victim is lying upon.
3. Grasp with your fingers under the angles of the jaw, near the ears. Lift the jaw forward (up) without moving the neck.
4. If the lips remain closed, use your thumbs to separate them.
After 30 compressions, quickly open the airway for rescue breaths.
Head Tilt/Chin LiftUse the head tilt/chin lift method to open the airway. Tilting the head and lifting the chin lifts the tongue off the back of the throat, so it does not block the airway.
1. Place 1 hand on the victim’s forehead and apply firm, backward pressure with your palm, tilting the head back.
2. Place 2 or 3 fingers of your other hand near the chin. Keep your fingers on the bony part of the jaw.
3. Tilt the head back while lifting the jaw upward to bring the chin forward. Head tilt/chin lift
Jaw thrust
Tip
Give compressions
Immediately provide 30 chest compressions. The victim should be face up on a firm, flat surface. Remove any cloth-ing that may interfere with compressions.To perform chest compressions:
• Place the heel of 1 hand in the center of the chest between the nipples, and the heel of the other hand on top.
• Depth: at least 2 inches on an adult• Rate: At least 100 compressions per minute• Push HARD and push FAST• Full Recoil: Allow the chest to fully expand to its start-
ing position between each compression• Minimize Interruption to Compressions

7Give just enough breath to make the chest rise. If rescue breaths are given too quickly or too forcefully, it can actually reduce the effectiveness of CPR.
Mouth-to-mask
Mouth-to-mouth
After the airway is open, provide 2 rescue breaths. Watch the chest when giving breaths. Only give enough air to cause the chest to rise, about 1 second each breath. Avoid over-ventilation (giving breaths too forcefully or too fast).
Mouth-To-Mouth Rescue BreathingIf off duty, a rescuer may choose to give mouth-to-mouth res-cue breathing. Open the airway and pinch the victim’s nose when giving rescue breaths.
Healthcare providers and professional rescuers should use a CPR barrier for rescue breathing. The mask covers the mouth and nose, so it is unnecessary to pinch the nose.
Mouth-To-Mask Rescue Breathing 1. Apply CPR mask to victim’s face2. Open the airway3. Inhale a regular-sized breath4. Breathe into the mask, approximately 1 second5. Watch for chest rise6. Lift mouth off mask7. Repeat
After 2 breaths, immediately resume compressions.
If the 1st rescue breath does not enter (no chest rise), reo-pen the airway and attempt a 2nd breath. If the 2nd breath does not enter, resume compressions.
C-A-B
Breathing
Continue CPR
TipDo not confuse occasional gasping with breathing. If a vic-tim is only gasping, begin CPR.!
Perform cycles of 30 compressions and 2 breaths. Take no more than 10 seconds to stop compressions, give 2 breaths, and resume compressions.
Continue CPR

8If more there is more than 1 trained rescuer, rotate the role of compressor every 2 minutes to help main-tain quality compressions.
Tip
C-A-B
When to use an AED
Rescue Breathing
Recovery Position
Use an AED as soon as possible.
If a second rescuer is available, the first rescuer should con-tinue CPR while the second rescuer powers on the AED and applies the pads. Switch rescuer roles every time the AED says to stop CPR. This allows the rescuer performing compressions to rest.
If the unresponsive victim is breathing normally, CPR is not required. Place the victim in the recovery position if you must leave to get help, or if fluids or vomit may block the airway. If breathing stops, immediately roll the victim onto his back and begin chest compressions.
Use the modified H.A.IN.E.S. recovery position (High Arm IN Endangered Spine) to keep the airway open and allow fluid to drain.
Use an AED when it is available
Modified H.A.IN.E.S. recovery position
The number of minutes from drop to shock when AED use is most successful.<3
Perform rescue breathing without chest compressions when a victim has a definite pulse, but no breathing or only gasping. Early and effective rescue breathing, especially in children, may prevent the onset of cardiac arrest.
Look for chest rise with each breath. Recheck the pulse about every 2 minutes. If a child or infant has a pulse less than 60 BPM, with signs of poor perfusion, perform CPR.
Age Status Rate Adult Definite pulse, no breathing 1 breath every 5-6 sec (10-12/min)
Child/Infant Definite pulse > 60 BPM, no breathing 1 breath every 3-5 sec (12-20/min)

9
CPr barriers
If you are performing CPR on a victim of poisoning, use a CPR barrier to help prevent exposure to the poison.
The risk of catching a disease while giving rescue breaths is extremely low. Despite this fact, many people are uncomfort-able giving mouth-to-mouth rescue breaths, especially on someone they don’t know.
CPR barriers may prevent or reduce exposure to a victim’s blood or body fluids by creating a barrier between the victim and rescuer. Federal OSHA requires that a professional rescuer or healthcare provider use a CPR barrier for rescue breathing. When performing CPR, it’s important that preparing a CPR barrier device does not delay starting chest compres-sions.
A CPR face mask covers both the mouth and nose so a rescuer does not have to pinch the victim’s nose during rescue breathing. A filtered valve allows air to enter, but prevents fluid backflow and directs exhaled air away from the rescuer. CPR masks are available in adult, child and infant sizes. Select the correct size mask in order to create a seal and give effective rescue breaths.
1. Apply the mask with the narrow end on the bridge of the nose, not covering the eyes. The wide bottom of the mask should not extend past the chin.
2. Press the mask firmly to the face and lift the chin to open the airway.3. Breathe into the mask and watch for chest rise. Do not over-ventilate.
A face shield contains a built-in one-way valve or filter.1. Place the shield over the face with the valve or filter over the victim’s mouth and open the airway.2. Pinch the nose (follow manufacturer’s guidelines about whether to pinch over or under the shield).3. Breathe into the one-way valve and watch for chest rise. Do not over-ventilate.
Face mask
Face shield
Using a face mask
Using a face shield
Face Mask
Face Shield
If a pediatric mask is unavailable, rotate an adult mask so that the narrow end is over the mouth.! Tip

10
bag Mask
The bag valve mask (BVM) can increase the amount of oxy-gen delivered and prevent rescuer exposure to pathogens. It is generally used by healthcare providers and profes-sional rescuers who train often and in varied conditions to ensure proper use.
The bag mask consists of a non-rebreathing mask and self-inflating bag attached to an oxygen reservoir. Tubing con-nects the bag mask to the oxygen tank. During cardiac ar-rest, the bag mask uses positive pressure ventilation when the rescuer squeezes the bag to push air into the lungs.
The bag mask is most effective when used together with emergency oxygen.
Effective ventilation can be provided more easily when 2 rescuers use the bag mask.
1. One rescuer holds the mask in place, creating a seal and maintaining a head tilt/chin lift.
2. The other rescuer squeezes the bag for 1 second and observes for chest rise.
Alternate technique: Squeeze the bag between your arm and body or arm and leg.
1. Select the appropriate size (adult, child or infant) and as-semble the bag mask.
2. If supplemental oxygen is available, connect the bag mask tubing to the oxygen regulator. Deliver oxygen at 15 LPM (minimum flow rate of 10-12 LPM).
3. Position yourself at the top of the victim’s head.4. Tilt the head back into the open airway position.5. Apply the mask to the face using the bridge of the nose
as a guide for correct position. Ensure proper fit.6. Use the thumb and index finger to create a tight seal
around the nose and mouth. Place your other fingers along the bony portion of the jaw, and lift the jaw up into the mask.
7. While maintaining the seal and head tilt with 1 hand, use the other hand to squeeze the bag and deliver the air. Ensure that no air escapes the seal around the mouth and nose.
a. Deliver each breath for 1 second.b. Watch for chest rise.c. Do not over-ventilate.
Bag valve mask
2-Rescuer Bag Mask Use
1-Rescuer Bag Mask Use
Use a bag mask to deliver about 600mL of air for an adult. Squeeze a 1-L adult bag about 2/3 of its volume, or a 2-L adult bag about 1/3 of its volume.
A bag mask is not recommended for use by a lone rescuer during CPR. TipTip
1-Rescuer Bag Mask Use
2-Rescuer Bag Mask Use

11
An AED can be used on an adult, child, or infant. Follow the AED prompts. Place the AED near the victim’s head and power on the unit. Some models require you to push a button to turn it on, while others turn on automatically when you lift the lid.
If there are two trained rescuers, one performs CPR while the other prepares the AED for use. The rescuer in charge of the AED will apply the pads around the hands of the person giving chest compressions. Do not stop CPR while the AED is being readied for use. The AED will prompt you to stop CPR when it is ready to analyze the heart rhythm.
It is critical that no one touches the victim or his clothing while the AED analyzes or delivers a shock.
When prompted by the AED to deliver a shock:• The AED user quickly looks up and down the entire
victim to ensure no one is touching him and loudly states, “Everybody clear.”
• The rescuer can now push the shock button.
Expose the chest and wipe it dry of any moisture. Apply the pads to the chest according to the pictures on the back of the pads.
• Place one pad on the right side of the chest, just below the collarbone. • Place the other pad on the lower left side of the chest.• Connect the pads to the AED. (Some pads come pre-connected to the AED.)
Place the AED near the victim’s head
Apply AED pads AED pad placement
Clear the victim
Power on the AED
The percent of out-of-hospital cardiac arrests that occur in private or residential settings.
Some AEDs will automatically deliver a shock with-out the rescuer pushing a button.Tip 80%
using an aeD
Power on the AED
Apply AED Pads
Clear the Victim & Shock

12
After the AED delivers a shock, or if no shock is advised, immediately resume CPR beginning with chest compressions. Every 2 minutes the AED will prompt you to stop CPR so it can analyze the heart rhythm.
CPR is hard work. The quality of compressions will deteriorate quickly, even without the rescuer being aware of it. If a sec-ond trained rescuer is present, switch roles when the AED says to stop CPR, which is every 2 minutes.
For the purpose of AED use, a child is age 1-8, or weighs less than 55 lbs. An infant is less than 1 year old. Children and infants require a lower level of energy to defibrillate the heart.
Child victim: Use an AED with pediatric pads or equip-ment. If these are not available, use an AED with adult pads and settings.
Infant victim: It’s best to use a manual defibrillator. If one is not available, use an AED with pediatric pads or equipment. If these are not available, use an AED with adult pads and settings.
Do not let AED pads touch or overlap. A child with a smaller chest may need an alternate pad placement.
AED shock
Small child pad placement - front
Child AED equipment
Resume compressions
Small child pad placement - back
Always follow your State, local, and workplace proto-cols for AED use on a child or infant.
Never use pediatric pads or equipment on an adult ( > 8 years old). The energy delivered will not be enough.!Tip
using an aeD
Resume Compressions
AED Use on Children
13
TeaM CPr
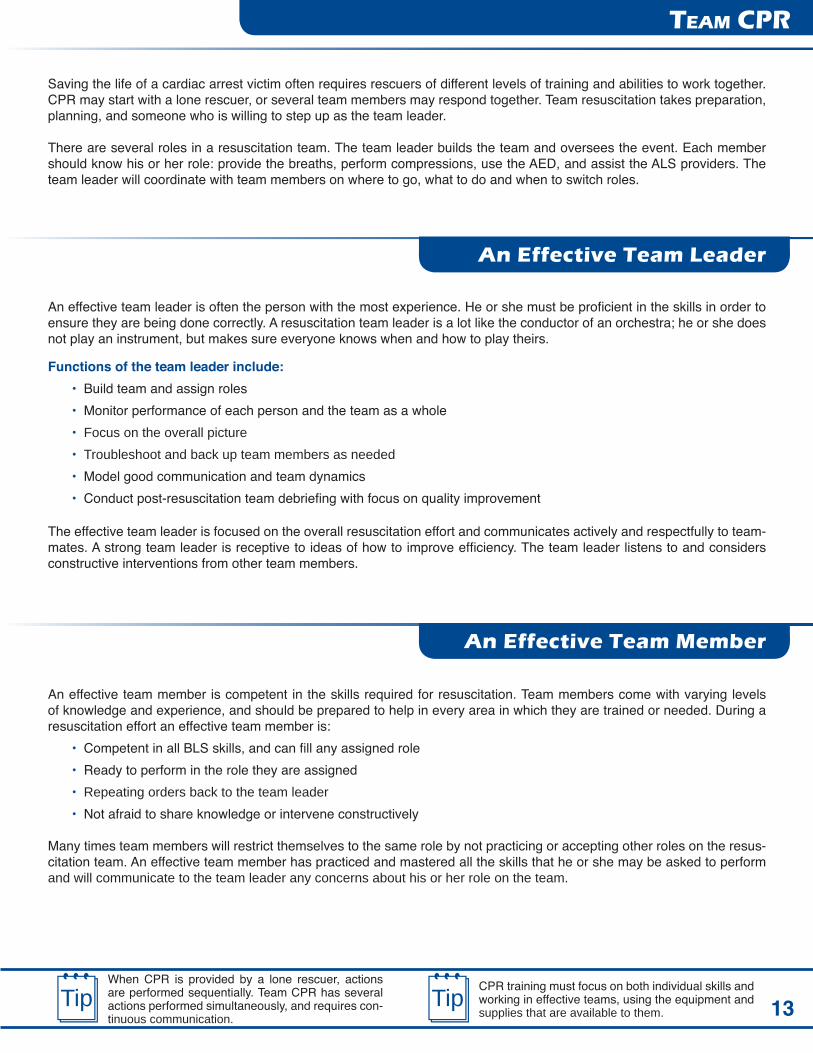
Saving the life of a cardiac arrest victim often requires rescuers of different levels of training and abilities to work together. CPR may start with a lone rescuer, or several team members may respond together. Team resuscitation takes preparation, planning, and someone who is willing to step up as the team leader.
There are several roles in a resuscitation team. The team leader builds the team and oversees the event. Each member should know his or her role: provide the breaths, perform compressions, use the AED, and assist the ALS providers. The team leader will coordinate with team members on where to go, what to do and when to switch roles.
An effective team leader is often the person with the most experience. He or she must be proficient in the skills in order to ensure they are being done correctly. A resuscitation team leader is a lot like the conductor of an orchestra; he or she does not play an instrument, but makes sure everyone knows when and how to play theirs.
The effective team leader is focused on the overall resuscitation effort and communicates actively and respectfully to team-mates. A strong team leader is receptive to ideas of how to improve efficiency. The team leader listens to and considers constructive interventions from other team members.
An effective team member is competent in the skills required for resuscitation. Team members come with varying levels of knowledge and experience, and should be prepared to help in every area in which they are trained or needed. During a resuscitation effort an effective team member is:
• Competent in all BLS skills, and can fill any assigned role• Ready to perform in the role they are assigned• Repeating orders back to the team leader• Not afraid to share knowledge or intervene constructively
Many times team members will restrict themselves to the same role by not practicing or accepting other roles on the resus-citation team. An effective team member has practiced and mastered all the skills that he or she may be asked to perform and will communicate to the team leader any concerns about his or her role on the team.
Functions of the team leader include:• Build team and assign roles• Monitor performance of each person and the team as a whole• Focus on the overall picture• Troubleshoot and back up team members as needed• Model good communication and team dynamics• Conduct post-resuscitation team debriefing with focus on quality improvement
When CPR is provided by a lone rescuer, actions are performed sequentially. Team CPR has several actions performed simultaneously, and requires con-tinuous communication.
CPR training must focus on both individual skills and working in effective teams, using the equipment and supplies that are available to them.
Tip Tip
An Effective Team Leader
An Effective Team Member

14
TeaM CPr
Team Communication
Constructive Interventions
Team leaders and members need to communicate effectively to provide the best patient care. Commonly during a resuscita-tion effort, team members do not know each other and have never worked closely together. Even when team members have worked together, effective communication is still critical. Communication and teamwork issues are often contributing factors to an unsuccessful resuscitation.
Important Aspects of Team CommunicationSend a Clear Message: Speak clearly to each other. Team members should repeat orders back to the team leader. Too many people in the room is a factor that can mix up the message. The team leader should excuse anyone without a role on the team.
Respect: Communicate in a calm and direct manner while making eye contact. Shouting over one another impairs team communication and can cause errors. The team leader should speak the most. A suggestion or constructive intervention from a team member should be acknowledged by the team leader.
Closed Loop Communication: Closing the loop (repeating back the order or request) allows the sender of the message to know it was received correctly. The team member repeating back the order is verifying that the order is correct and allowing the team leader a chance to consider the treatment or change the order. This is a primary way to avoid mistakes since it gives both the sender and receiver a chance identify and fix a potential miscommunication.
Share Knowledge: Team leaders and members must share knowledge with each other and communicate it effectively. “Okay team, we’ve been through the algorithm and we’re not seeing any changes. Is there anything we’re missing?” An ef-fective team leader and team member will ask for and offer solutions when requested. Sharing knowledge across the team can identify an intervention that was missed.
A successful resuscitation usually involves a comprehensive team effort. An adverse outcome may be the result of a poorly functioning team. During debriefings it is often identified that a team member noticed a mistake but was afraid to comment.
Constructive interventions can come from any team member who notices a mistake at any time during the resuscitation effort. A team member may notice the wrong treatment or sequence and identify that to the team leader. A team leader may intervene by assigning a different role to a team member who is performing poorly. It is every team member’s responsibility to speak out if they know something is wrong.
Give constructive interventions immediately:• Feedback on a mistake• Poorly functioning team member• Missed intervention
Every team needs a leader and team members who know their role, communicate effectively, and share knowledge. These are essential elements of team resuscitation, and can reduce mistakes and increase the chance for a successful outcome.
When mistakes occur during a resuscitation, the leading factor is poor communication and teamwork.
Be prepared to perform CPR in any setting, on duty as part of a team or off duty as a lone responder.Tip Tip

15
TeaM CPr
If a team arrives together, it will designate a team leader to delegate roles. If a team starts with a lone rescuer, it will build as each rescuer arrives.
A well-functioning team can provide more effective CPR by:
• Performing CPR while an AED is being prepared for use• Reducing fatigue during compressions• Providing feedback to each other on compressions and rescue breaths• Minimizing interruptions to compressions
The team leader and all team members should work together towards the same goals.
The 1st rescuer begins assessment and CPR. As additional rescuers arrive, they will seamlessly take over duties, such as:
• Activate EMS and get the AED• Use the AED• Set up bag mask and supplemental oxygen• Give feedback to the compressor on the quality of
chest compressions• Feel for a carotid pulse to determine effectiveness of
compressions
2-rescuer CPR:• Switch roles of compressor every 2 minutes• Take no more than 5 seconds to switch roles
More than 2 rescuers:• Rotate through the role of compressor every 2 min-
utes• Perform 2-rescuer bag mask ventilation
Count compressions out loud so that the person giv-ing rescue breaths is prepared.
Emergency scenes can be noisy and chaotic. Stay focused on the priorities, and delegate tasks accord-ingly.
Tip Tip
Building a Team
Effective CPR
Two team members provide more effective bag mask ventilation

16
aDulT CPr
C: Compressions
Perform 30 chest compressions with 2 hands.• Position the victim face up on a firm, flat surface.• Quickly remove clothing from the front of the chest if it
may interfere with compressions.• Place the heel of 1 hand in the center of the chest be-
tween the nipples, and the heel of the other hand on top.
• Compress the chest 30 times.• Rate: At least 100/minute• Depth: At least 2”• Make sure the compressions are good quality.
Push hard and fast.Allow full recoil between each compression.
Minimize interruptions to compressions.
Adult Age: Puberty and older• Male: facial or underarm hair• Female: signs of breast development
Scene Safety: Quickly survey the scene before you enter.Check Response and Breathing:
• Tap the shoulder and shout.• While checking for response, scan for breathing for
5-10 seconds.• If no response and no breathing or only gasping, yell
for help. Send someone to call 9-1-1 and get the AED.• If alone, activate EMS and get the AED yourself.
Check Pulse:• Check the carotid pulse for 5-10 seconds.• If pulse is present, perform rescue breathing.
• Give 1 breath every 5-6 seconds.• If no definite pulse, begin CPR.
Open the airway with the head tilt/chin lift maneuver. • Place 1 hand on the forehead and apply firm pressure
to tilt the head back.• Use 2 or 3 fingers of your other hand to lift the chin.
Use the jaw thrust maneuver to open the airway if you sus-pect head or neck injury.
30 chest compressions
Head tilt/chin lift
Check response and breathing
A: Airway
The maximum number of seconds in which to com-plete 30 chest compressions.
If an unresponsive victim is face down, roll him face up to check for breathing. 18Tip

17
aDulT CPr
Provide 2 rescue breaths. It should take less than 10 sec-onds to stop compressions, give 2 breaths, and resume compressions.
• Maintain an open airway.• Pinch the victim’s nose (mouth-to-mouth)• Inhale a regular-sized breath.• Give 2 rescue breaths for 1 second each breath.• Watch for chest rise.
Immediately resume compressions.
Continue cycles of 30 compressions to 2 breaths.• Continue CPR until the AED prompts you to stop.• Minimize interruptions to chest compressions.
Avoid fatigue: If an additional rescuer is present, perform 2-rescuer CPR. Switch roles every 5 cycles (about every 2 minutes).Give feedback on the quality of compressions to the res-cuer performing CPR.If the victim begins to move and breathe, leave the AED pads in place. Place in the modified H.A.IN.E.S. position if you need to keep the airway clear of fluids and vomit.
Use the AED as soon as it is ready. If there is more than one trained rescuer, have that person use the AED.
• Turn on the AED.• Follow AED prompts.
o Apply pads.o Clear the victim before shocking.
• Immediately resume compressions.
Continue CPR
Use AED if available
2 rescue breaths
B: Breathing
Continue CPR
Defibrillation
The number of minutes to perform CPR before switching to another trained rescuer to avoid fatigue.
If no chest rise with the first rescue breath, reposition the head and give a second breath.2 Tip

18
ChilD CPr
C: Compressions
Perform 30 chest compressions with 1 or 2 hands.• Position the victim face up on a firm, flat surface.• Quickly remove clothing from the front of the chest if
it may interfere with compressions.• Place the heel of 1 hand in the center of the chest
between the nipples. Place the heel of the other hand on top (optional).
• Compress the chest 30 times.• Rate: At least 100/minute• Depth: About 2”
Push hard and fast.Allow full recoil between each compression.
Minimize interruptions to compressions.
Cardiac arrest in children usually results from respiratory arrest, not from a cardiac problem. Common causes include injury, poisoning, choking, drowning, and asthma.Child Age: 1 year to pubertyScene Safety: Quickly survey the scene before you enter.Check Response and Breathing:
• Tap the shoulder and shout.• While checking for response, scan for breathing for
5-10 seconds.• If no response and no breathing or only gasping, yell
for help. Send someone to call 9-1-1 and get the AED.• If alone, stay with the child.
Check Pulse:• Check the carotid pulse for 5-10 seconds.• If pulse is > 60 BPM, perform rescue breathing.
• Give 1 breath every 5-6 seconds.• If no definite pulse or < 60 BPM, begin CPR.
30 chest compressions
Check response and breathing
Check pulse
The age when children are most at risk for drowning.
The number of children under the age of 14 who drown each day in the U.S. 21-4

19
Open the airway using the head tilt/chin lift maneuver.• Place 1 hand on the forehead and apply firm pressure
to tilt the head back.• Use 2 or 3 fingers of your other hand to lift the chin.
Head tilt/chin lift
ChilD CPr
Provide 2 rescue breaths. It should take less than 10 sec-onds to stop compressions, give 2 breaths, and resume compressions.
• Maintain an open airway position.• Pinch the victim’s nose (mouth-to-mouth).• Inhale a regular-sized breath.• Create a seal around the victim’s lips.• Exhale for about 1 second each breath.• Watch for chest rise.
If the chest won’t rise, reposition the head and try again. Retry only once before resuming chest compressions.
Continue cycles of 30:2 (1-rescuer) or 15:2 (2-rescuer).• If you are alone, activate EMS after 2 minutes (5
cycles of 30:2) if not already done. Return right away and continue CPR.
• Continue CPR if EMS has already been activated.• Minimize interruptions to compressions.
Team CPR• Perform 2-rescuer CPR with cycles of 15:2. • Switch roles every 10 cycles (about 2 minutes) to
avoid fatigue.• Give feedback to the compressor on the quality of
compressions.Continue CPR
2 rescue breaths
B: Breathing
A: Airway
Continue CPR
Provide just enough air to cause the chest to rise. Over-inflating the lungs will decrease the effectiveness of CPR.
If a victim begins to move during CPR, keep the airway open and monitor breathing closely. ! Tip

20
infanT CPr
C: Compressions
Perform 30 chest compressions with 2 fingers.• Position the victim face up on a firm, flat surface.• Quickly remove clothing from the front of the chest if
it may interfere with compressions.• Place 2 fingers in the center of the chest just below
the nipple line. • Compress the chest 30 times.• Rate: At least 100/minute• Depth: About 1 1/2”
Push hard and fast.Allow full recoil between each compression.
Minimize interruptions to compressions.
Cardiac arrest in infants usually results from respiratory ar-rest, not from a cardiac problem. Common causes include choking, injury, SIDS, and respiratory illness. With CPR, a rescuer may be able to restore normal breathing without the use of an AED. Infant Age: up to 1 year oldScene Safety: Quickly survey the scene before you enter.Check Response and Breathing:
• Tap the bottom of the foot and shout.• While checking for response, scan for breathing for
5-10 seconds.• If no response and no breathing or only gasping, yell
for help. Send someone to call 9-1-1 and get the AED.• If alone, stay with the infant.
30 chest compressions
Check response and breathing
Check pulse
The percentage of car and booster seats that are installed incorrectly.
Estimated number of lives saved each year in the U.S. by car and booster seats. 42572%
Check Pulse: • Check the brachial pulse for 5-10 seconds.• If pulse is > 60 BPM, perform rescue breathing.
o Give 1 breath every 5-6 seconds.• If no definite pulse or < 60 BPM, begin CPR.

21
Open the airway using the head tilt/chin lift maneuver. • Place 1 hand on the forehead and apply firm pressure
to tilt the head into a neutral position. • Use 2 or 3 fingers of your other hand to lift the chin.
Do not overextend the infant’s airway. Since the infant’s air-way is not fully developed, overextending the airway can cause it to close.
Head tilt/chin lift
infanT CPr
Provide 2 rescue breaths. It should take less than 10 sec-onds to stop compressions, give 2 breaths, and resume compressions. Do not over-inflate the lungs; only provide enough air to cause the chest to rise.
• Maintain an open airway position.• Inhale a regular-sized breath.• Create a seal around the mouth and nose.• Exhale for about 1 second each breath.• Watch for chest rise.
If the chest won’t rise, reposition the head and try again. Retry only once before resuming chest compressions.
Continue cycles of 30:2 (1-rescuer) or 15:2 (2-rescuer).• If you are alone, activate EMS after 2 minutes (5 cy-
cles of 30:2) if not already done. Return right away and continue CPR.
• Continue CPR if EMS has already been activated.• Minimize interruptions to compressions.
Team CPR• Perform 2-rescuer CPR with cycles of 15:2 using the
2 thumb-encircling hands technique. • Switch roles every 10 cycles (about 2 minutes) to
avoid fatigue.• Give feedback to the compressor on the quality of
compressions.Continue CPR
2 rescue breaths
A: Airway
B: Breathing
Continue CPR
The quality of chest compressions may deteriorate quick-ly, even when performing compressions on an infant.
If you’re alone, consider carrying the infant to the phone after 2 minutes of CPR.Tip!

22
sPeCial ConsiDeraTions - CPr
Vomiting
When to Stop CPR
CPR Alternatives
Hypothermia: In a cold environment the body’s metabolism slows down, reducing the need for oxygen. This can extend the amount of time in which CPR can be successful. Do not assume it is too late to begin CPR.
Electrical shock: A victim of electrical shock may suddenly stop breathing or go into cardiac arrest. Before approaching the person, make sure the power source has been shut off and it is safe for you to approach.
Compression-only CPR is used for an adult victim if a lay rescuer is untrained in standard CPR with compressions and ventilations. It may also be used if a rescuer is unable or unwilling to give rescue breaths due to blood or injury to the victim’s mouth. Professional rescuers should carry in their response gear a CPR barrier or bag mask for protection during rescue breathing.Mouth-to-Nose rescue breathing may be used if a victim’s mouth or jaw is severely damaged. Be sure to hold the victim’s mouth closed so that air does not escape.Mask-to-Stoma rescue breathing is used if a victim has a stoma (a surgically-created opening at the base of the throat to allow for breathing). If possible, pinch the nose and close the mouth to reduce air loss.
It is common for a person in cardiac arrest to vomit while receiving CPR. If a victim vomits, quickly roll him to the side, sweep out his mouth with a gloved finger, roll him back and continue CPR.
Avoid over-ventilation when giving rescue breaths to de-crease the risk of vomiting.
Only stop CPR if:• The victim begins to move or breathe.• The AED directs you to stop.• The scene becomes unsafe.• You are physically exhausted and cannot continue.• Advanced care providers arrive and are ready to take
over.• The victim is pronounced dead by a qualified person.
Roll to the side and clear the mouth
Professional rescuers take over
A lightning strike can cause the heart to stop beating. Seek shelter in a lightning storm.
Do not perform compression-only CPR on a child or infant. Provide compressions and ventilations.
Compression-only CPR Mouth-to-nose Mask-to-stoma
Tip

23
Implanted device
Remove medication patch and wipe skin
AED maintenance
sPeCial ConsiDeraTions - aeD
Chest hair can limit the contact between the AED pads and the skin, preventing the AED from reading the heart rhythm and delivering a shock. If you have an extra set of pads, firmly apply the pads to the chest, then remove the pads with a quick movement and apply a new set of pads. You may also use a razor to shave the chest in the area of pad placement.
Some people have medical devices, such as a pacemaker, implanted into their bodies. These will appear as small, hard lumps under the skin of the chest or abdomen.
Do not place an electrode directly over an implanted device. Adjust pad placement at least 1” away from the device.
Medication can be embedded in an adhesive patch that is applied to the skin. Do not place an AED pad over a medica-tion patch. With gloved hands, remove the patch and wipe the chest clean with a towel, then attach the AED pads.
Storage: An AED should be stored ready to use, close to trained rescuers. Accessories such as extra pads, pediat-ric pads or adaptor, an extra battery, CPR mask, a towel, gloves and razor should be stored with the AED.
Inspection: Perform regular inspections according to man-ufacturer’s guidelines and local protocols. Make sure that pads and batteries have not expired, and there is no visible damage to the unit.
Troubleshooting: If the AED detects a problem, it will prompt you to troubleshoot:
• Check pads: Press down firmly on the pads, or re-place the pads; check the cable connection.
• Low battery: Replace the battery.• Movement: When the AED is analyzing the heart
rhythm, do not touch or move the victim.
Very Hairy Chest
Implanted Devices
Medication Patches
Maintenance & Troubleshooting
Most manufacturers recommend storing spare pads with the AED.
Keep the AED in an accessible area, close to a phone. Store it at room temperature, protected from the weather.
Tip Tip
24
aeD safeTy
Water
Oxygen
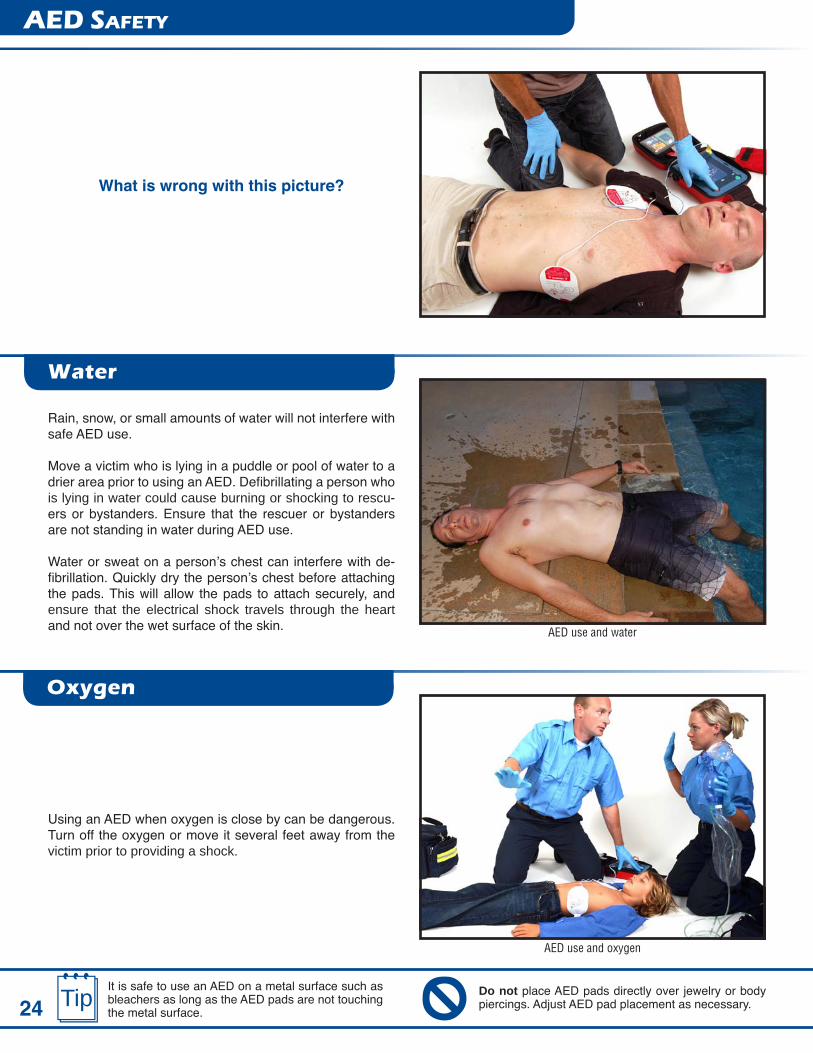
What is wrong with this picture?
Rain, snow, or small amounts of water will not interfere with safe AED use.
Move a victim who is lying in a puddle or pool of water to a drier area prior to using an AED. Defibrillating a person who is lying in water could cause burning or shocking to rescu-ers or bystanders. Ensure that the rescuer or bystanders are not standing in water during AED use.
Water or sweat on a person’s chest can interfere with de-fibrillation. Quickly dry the person’s chest before attaching the pads. This will allow the pads to attach securely, and ensure that the electrical shock travels through the heart and not over the wet surface of the skin.
Using an AED when oxygen is close by can be dangerous. Turn off the oxygen or move it several feet away from the victim prior to providing a shock.
AED use and water
AED use and oxygen
Do not place AED pads directly over jewelry or body piercings. Adjust AED pad placement as necessary.
It is safe to use an AED on a metal surface such as bleachers as long as the AED pads are not touching the metal surface.
Tip

25
CPr aT-a-glanCe
Action Adult Child InfantAge Puberty and Older 1 - Puberty < 1 Year
Assess Response & Breathing
Tap shoulder and shout Tap bottom of foot and shoutScan for 5 - 10 seconds
If no breathing or only gaspingActivate EMS Send someone to activate EMS & get AED
If Alone Activate EMS & get AED Stay with the victim
Assess CirculationCarotid pulse Brachial pulse
Check for 5 - 10 secondsIf no definite pulse If no pulse or pulse < 60 BPM with signs of poor perfusion
Compressions 30 chest compressions
Location2 hands 1 or 2 hands 2 fingers
Center of chest between nipples Just below nipple line
Depth At least 2” About 2” About 1 1/2”
Rate At least 100/minute
Open Airway Head tilt-chin lift or jaw thrust (suspected trauma)
BreathingCPR barrier or bag mask
2 breaths, 1 second each breathRatio of Compres-
sions to Ventilations30:2
1 or 2 rescuers30:2 1 rescuer15:2 2 rescuer
After 2 minutesContinue CPR/AED use Call 9-1-1 & get AED if not previously done
Switch compressor roles if > 1 rescuer
DefibrillationAED Use as soon as available
AED Age Age 8 & older or > 55 lbs. 1-8 years old < 1 year old
AED Pads Adult pads Child pads; if none, adult padsManual defibrillator; If none,
child pads; If none, adult padsPulse present, no breathing
Rescue Breathing 1 breath every 5-6 sec (10-12/minute) 1 breath every 3-5 seconds (12-20/minute)
Choking Rescue
Choking- Responsive Abdominal Thrusts 5 Back slaps 5 Chest thrusts
Choking - Unresponsive
Perform CPR & look in the mouth after compressions Remove object if seen
Adult Child Infant
26
how woulD you reaCT?
1
2
3
4
5
Law Enforcement
SCENARIOSQUESTIONS
Off Duty
Healthcare
EMS & Fire
While working on an ambulance, you are dispatched to an elementary school for an unresponsive child on the playground. As you and your partner approach, you see a child on the ground near the swings and a teacher doing CPR. How would you REACT?
You are working the triage area of the emergency de-partment when a woman runs in with an infant in a car seat carrier. She puts the infant on the desk and says, “My baby isn’t breathing!” How would you REACT?
You are off duty at a neighbor’s barbeque when one of the guests clutches his chest, stands up and falls to the ground. There is a lot of commotion and shout-ing, and the guest is not responding. How would you REACT?
You are on a daytime patrol of a residential area when a frantic woman comes out of a house and is running to a neighbor. She sees your patrol vehicle and flags you down. The woman quickly states that her father was sleeping on the sofa but she can’t wake him up and she’s not sure if he’s breathing. You have an AED and CPR mask in your vehicle. How would you REACT?
The most important part of CPR is quality:
a. Rescue breathingb. CPR barrier masksc. Chest compressionsd. Oxygen administration
The main cause of cardiac arrest in infants and children is:
a. Electrical shockb. Respiratory arrestc. Heart attackd. Stroke
The first step in using an AED is to:
a. Apply the padsb. Shock the victimc. Clear the victimd. Power on the unit
For the purpose of CPR, a victim is considered to be an adult from:
a. 10 years of ageb. 1 day to 1 year oldc. Signs of pubertyd. All of the above
It is acceptable to use child AED pads on an adult victim.
True False

27
R – Recognize the emergencyPay attention to unusual sights, sounds, smells and situa-tions.
• A person who is unresponsive or appears seriously ill or injured
• Screams or panicked facial expressions• A collision or vehicle stopped in an unusual location• A suspicious environment: overturned furniture, dis-
turbed plants, opened chemical or medication con-tainers, broken glass, blood, etc.
• Environmental hazards: fire, flooding, damaged elec-trical wires, etc.
E – Environment safetySize-up the scene for danger before you enter. Common hazards include:
• Traffic• Fire or smoke• Wet, icy or unstable surface or structure• Downed electrical wires• Hazardous materials, chemicals, gasses• Open water, strong currents• Confined spaces• Possible crime scene, unsafe crowd
If the scene does not look safe, do not enter. Secure the area, keep others out, and call for additional help. Size-up the victim from a safe distance.
• How many victims? • What is their general condition? • Can you identify the cause of the illness or injury?
A – Assess the victimWhen you get to the victim’s side, assess responsiveness and breathing, and look for serious or life-threatening inju-ries or illness.
C – Call for helpCall your emergency response number if there is danger or if the victim is unresponsive or seriously ill or injured. Send someone else to call for help if available. If you’re not sure it’s an emergency, it’s better to call for help.
T – Treat the victimPrioritize treating problems related to breathing and circula-tion first.
An emergency is an unexpected occurrence that demands serious attention. Emergencies can happen anywhere and usually when you least expect them. The most important actions are to remain calm, stay aware of your own safety, and call 9-1-1.
Treat the victim
Call for help (activate EMS)
Recognize the emergency
Continually reassess the scene for danger. An emergency scene can quickly change from safe to unsafe.
Post the emergency response number next to every phone, first aid kit and AED.
resPonDing To eMergenCies
REACT to an Emergency
Tip !At every emergency you will assess the scene for safety, get the first aid kit and AED, put on personal protective equipment, and assess the victim.
28
Physical Response• Rapid breathing or heart rate• Trembling• Sweating• Nausea, diarrhea• Headache, muscle ache• Fatigue• Difficulty sleeping• Increased or decreased appetite
Mental Response• Cannot stop thinking about the event• Confusion, difficulty concentrating• Nightmares
Emotional Response• Anxiety, worry, guilt, fear, anger• Depression, crying• Restlessness• Change in behavior or interactions with people
It’s normal to feel stress after an incident. The response usually lasts just a few days, but sometimes may last for weeks or even months. It can affect a person’s health, fam-ily life, and work performance.
Giving care in an emergency can have a physical, mental, and emotional impact on the rescuer. The amount of stress will vary depending on the seriousness of the incident and each rescuer’s unique response to it. Consider a critical incident stress debriefing (CISD) for a very serious incident.
When EMS responders arrive, keep providing care until they say they are ready to take over.
If you are not sure what to do, call 9-1-1 (activate EMS). The 9-1-1 dispatcher will guide you.
Don’T Delay Calling 9-1-1A person has a better chance of surviving an emergency when 9-1-1 is called early. Do not delay calling 9-1-1, or assume someone else will call. Medical treatment is often more effective the sooner it is delivered.
When you call 9-1-1 or your local emergency response number:• You are connected to an emergency dispatcher.• Provide your name, location, and a description of the event.• EMS responders are on the way while the dispatcher is still getting information from you.• Always hang up last.
If your workplace has an internal emergency response system, activate that system instead of calling 9-1-1.
My workplace emergency response number:________________________________________
resPonDing To eMergenCies
Rescuer Stress
Talk about your feelings
Tip Tip
Tips for Stress Management:• Talk about your feelings• Eat properly• Avoid alcohol, drugs and caffeine• Exercise and get enough rest• Don’t judge yourself for your actions• Obtain professional help if needed
29Do not insist on treating a victim who has refused care. This could meet the legal definition of assault and battery. Transport-ing someone to a hospital without consent can meet the legal definition of kidnapping and false imprisonment .
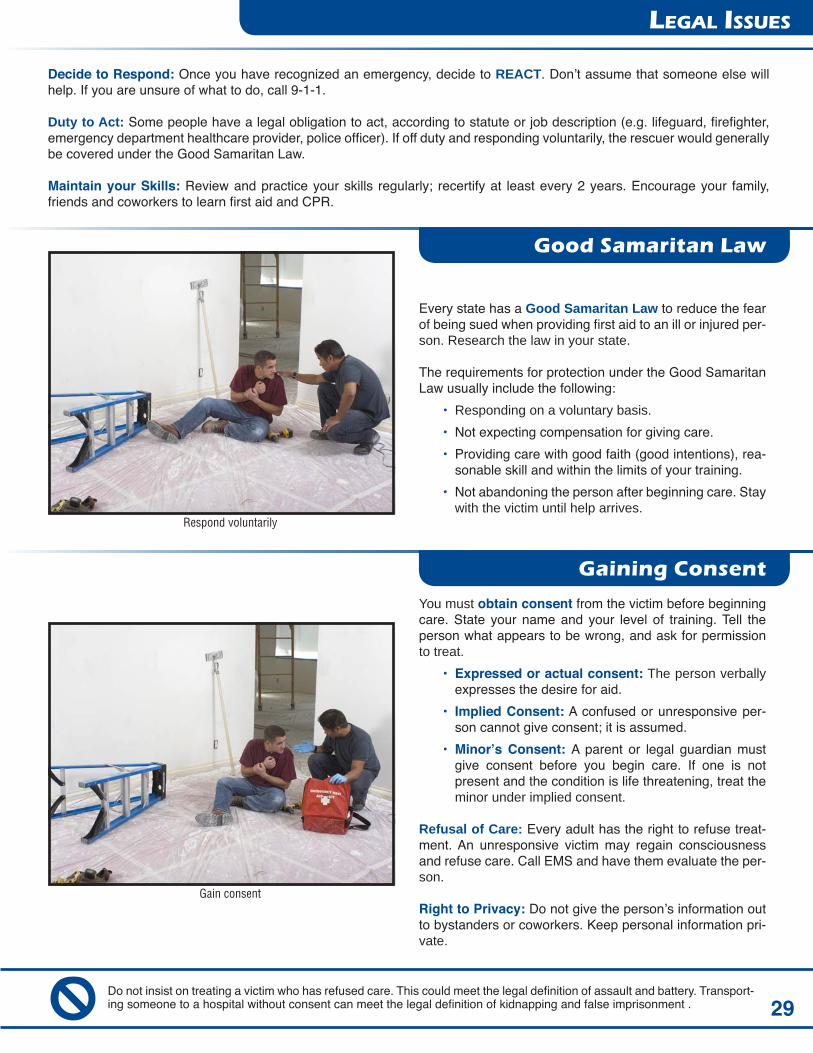
Every state has a Good Samaritan Law to reduce the fear of being sued when providing first aid to an ill or injured per-son. Research the law in your state.
The requirements for protection under the Good Samaritan Law usually include the following:
• Responding on a voluntary basis.• Not expecting compensation for giving care.• Providing care with good faith (good intentions), rea-
sonable skill and within the limits of your training.• Not abandoning the person after beginning care. Stay
with the victim until help arrives.
You must obtain consent from the victim before beginning care. State your name and your level of training. Tell the person what appears to be wrong, and ask for permission to treat.
• Expressed or actual consent: The person verbally expresses the desire for aid.
• Implied Consent: A confused or unresponsive per-son cannot give consent; it is assumed.
• Minor’s Consent: A parent or legal guardian must give consent before you begin care. If one is not present and the condition is life threatening, treat the minor under implied consent.
Refusal of Care: Every adult has the right to refuse treat-ment. An unresponsive victim may regain consciousness and refuse care. Call EMS and have them evaluate the per-son.
Right to Privacy: Do not give the person’s information out to bystanders or coworkers. Keep personal information pri-vate.
Decide to Respond: Once you have recognized an emergency, decide to REACT. Don’t assume that someone else will help. If you are unsure of what to do, call 9-1-1.
Duty to Act: Some people have a legal obligation to act, according to statute or job description (e.g. lifeguard, firefighter, emergency department healthcare provider, police officer). If off duty and responding voluntarily, the rescuer would generally be covered under the Good Samaritan Law.
Maintain your Skills: Review and practice your skills regularly; recertify at least every 2 years. Encourage your family, friends and coworkers to learn first aid and CPR.
Gain consent
Respond voluntarily
legal issues
Good Samaritan Law
Gaining Consent

30
ProTeCTion froM infeCTion
Bloodborne Pathogens
Standard Precautions
Bloodborne pathogens are disease-causing microorgan-isms that are present in human blood and certain body flu-ids. The human immunodeficiency virus (HIV), hepatitis B and C are viruses that are carried in the blood and body fluids of infected persons. They can be transmitted when the blood or body fluids from an infected person or on a contaminated object enter another person’s body. Exposure to bloodborne pathogens can happen through:
• A direct splash on the rescuer’s eyes, mouth or nose• An opening in the rescuer’s skin, such as a cut, scab,
or rash
OSHA requires professional rescuers and healthcare pro-viders to use standard precautions These combine univer-sal precautions, which minimize exposures to BBP, and body substance isolation (BSI), which assumes that all moist body substances are infectious.
• Treat all victims as potential carriers of infectious dis-ease.
• Use personal protective equipment: moisture-proof gloves, mask, gown, eye protection.
• Use a CPR barrier or bag mask for rescue breathing.• Wash hands thoroughly before and after giving care,
and after cleaning an accident scene. • Dispose of sharps in appropriate puncture-resistant
containers.• Use labeled biohazard bags when appropriate.
Infectious diseases are spread when one person transmits germs to another. At an emergency scene, a rescuer may be exposed to a disease which could cause illness. Although the risk of actual disease transmission is very low, it is still impor-tant to protect yourself.
What to do if you’re ExposedIf you are exposed to blood or other body fluids, immediately remove your gloves and wash your hands and the exposed area thoroughly with soap and water. Follow your workplace Exposure Control Plan.
Exposure to blood
Personal protective equipment
If your hands are not visibly soiled and you don’t have soap and water, use hand sanitizer, then wash as soon as possible.
The number of seconds you should spend washing your hands.
Hand WashingWash your hands thoroughly immediately after glove removal. Use soap and running water, and spend at least 20 seconds scrubbing your hands. Rinse well.
!>20
31
ProTeCTion froM infeCTion
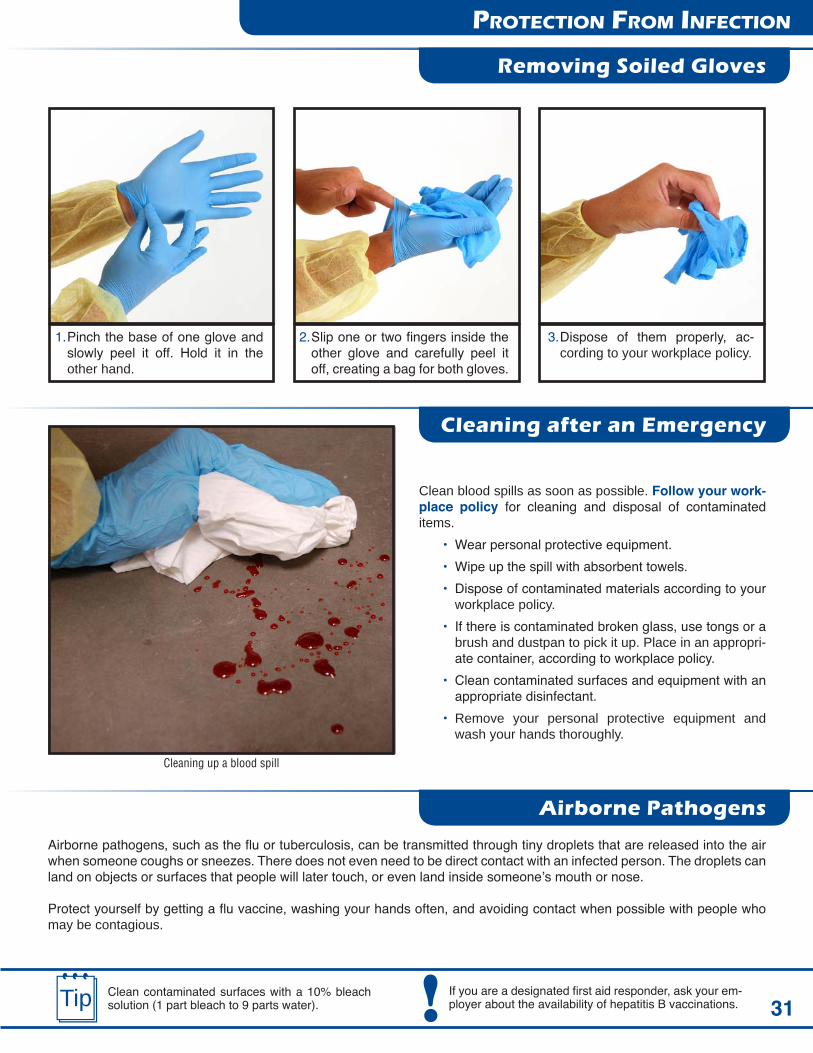
Clean blood spills as soon as possible. Follow your work-place policy for cleaning and disposal of contaminated items.
• Wear personal protective equipment.• Wipe up the spill with absorbent towels. • Dispose of contaminated materials according to your
workplace policy.• If there is contaminated broken glass, use tongs or a
brush and dustpan to pick it up. Place in an appropri-ate container, according to workplace policy.
• Clean contaminated surfaces and equipment with an appropriate disinfectant.
• Remove your personal protective equipment and wash your hands thoroughly.
Airborne pathogens, such as the flu or tuberculosis, can be transmitted through tiny droplets that are released into the air when someone coughs or sneezes. There does not even need to be direct contact with an infected person. The droplets can land on objects or surfaces that people will later touch, or even land inside someone’s mouth or nose.
Protect yourself by getting a flu vaccine, washing your hands often, and avoiding contact when possible with people who may be contagious.
Cleaning up a blood spill
Removing Soiled Gloves
Cleaning after an Emergency
Airborne Pathogens
Clean contaminated surfaces with a 10% bleach solution (1 part bleach to 9 parts water).
If you are a designated first aid responder, ask your em-ployer about the availability of hepatitis B vaccinations.
1. Pinch the base of one glove and slowly peel it off. Hold it in the other hand.
2. Slip one or two fingers inside the other glove and carefully peel it off, creating a bag for both gloves.
3. Dispose of them properly, ac-cording to your workplace policy.
!Tip

32
hearT aTTaCk
Coronary artery disease develops when fat and cholesterol attach to the walls of the coronary arteries, causing them to narrow (atherosclerosis). A heart attack occurs when a clot blocks a narrowed coronary artery, depriving the heart muscle of oxygen. The heart attack victim feels discomfort because the heart muscle is dying.
The signs of a heart attack are usually sudden. They may come and go and appear in any combination.
Unusual SymptomsWomen, diabetics and older persons may not experience the typical symptoms of chest discomfort and shortness of breath. They are more likely to have other symptoms such as jaw pain, nausea or vomiting, or unexplained fatigue.
AspirinA person with a suspected heart attack should chew either 1 adult or 2 low-dose uncoated aspirin to improve the chance of survival while waiting for EMS responders. Do not give aspirin if allergy, signs of stroke, recent bleeding problems, or not alert.
Heart attack symptoms
Offer aspirinUnusual symptoms
Follow local and workplace protocols for the administration of nitroglycerin.
The number of new or recurrent heart attacks in the U.S. each year.
Treatment
1. Call 9-1-1 (activate EMS). Send a bystander if avail-able. Do not transport the person to the hospital yourself.
2. Place in a comfortable position, usually sitting up.3. Calm and reassure.4. Offer aspirin if no allergy to aspirin, signs of stroke,
or recent stomach or intestinal bleeding problems. The victim must be alert and able to chew and swal-low the aspirin.
Signs and Symptoms
• Chest discomfort: pain, crushing, pressure, tightness, squeezing, fullness
• Radiating discomfort to arms, neck, back, jaw, or ab-domen
• Shortness of breath• Pale, cool, sweaty skin• Dizziness or fainting• Nausea or vomiting
aCTivaTe eMsHeart attack is the leading cause of sudden cardiac arrest. Fast recognition and response to early signs of heart attack is critical. Clot-busting medication is most effective in the early hours of a heart attack. The sooner a heart attack victim receives medical care, the less damage to the heart and the better the chance of survival.
1.25M!

33
sTroke
STRoke Assessment
A stroke is an injury to the brain caused by a disruption of blood flow to the brain cells. When a blood vessel becomes blocked or bursts, oxygen-rich blood is unable to reach a portion of the brain and brain cells begin to die. A stroke is a life-threatening condition that requires you to recognize the signals and act fast.
A transient ischemic attack, or mini-stroke, is a temporary lack of oxygen with total recovery of function. It may last a few seconds or several hours. Call 9-1-1.
Use the first three letters of stroke, S-T-R, to quickly look for common signs of a stroke:
Smile - Ask the person to smile. Look for uneven facial movement.
Talk – Ask the person to repeat a common phrase. Listen for slurred or incorrect words.
Reach – Ask the person to close his eyes and raise both arms. Look for arm drift or weakness on one side.
Prevent a stroke by controlling your blood pres-sure, diet, and diabetes. Stop smoking and start exercising.
The number of strokes in the U.S. each year.
Smile Talk Reach
Treatment
1. Call 9-1-1 (activate EMS). 2. If unresponsive and no breathing or only gasping,
begin CPR.3. Protect the airway. If secretions, place in recovery
position.4. Calm and reassure.5. Note the time that symptoms began.
Don’T Delay Calling 9-1-1Call 9-1-1 immediately when there is a sudden onset of any of the signs of stroke. Don’t delay and hope the signs will go away, or drive a victim to the hospital. Early recognition and rapid treatment with clot-busting medi-cations are critical to improved outcome and survival of stroke.
Signs and Symptoms (sudden onset)
• Weakness or numbness of the face, arm or leg, usu-ally on one side of the body
• Difficulty speaking or swallowing• Loss of balance or coordination, difficulty walking• Decreased mental status• Severe headache, dizziness• Change in vision
800KTip

34
Choking is a common emergency, even though it is preventable. The technique to manage choking is the same for adults and children age 1 and older. Recognize a choking emergency and act quickly. A serious airway obstruction is life-threaten-ing if it is not relieved immediately.
It’s important to tell the difference between choking and other emergencies, such as a heart attack, asthma, or seizure. Look for the universal sign of choking - one or both hands at the throat. Suspect choking when a responsive person suddenly stops talking.
With a mild airway obstruction, the person is able to cough forcefully or even speak. Do not interfere. If the person can speak, he can breathe.
A person with a severe obstruction cannot breathe, cough effectively, or speak. He may make a high-pitched sound when inhaling or turn blue around the lips and face. Act quickly to remove the obstruction, or the person will soon become unre-sponsive and die.
Consider a person’s activities to help you recognize a choking emergency. Most incidents occur while an adult is eating or a child is eating or playing.
A person who has received abdominal thrusts should be evaluated by a physician.
Mild obstruction - encourage cough
Severe obstruction - continuous abdominal thrusts
Treatment
Treatment
1. Ask the person, “Are you choking?”2. If the person can cough forcefully or speak, do not
interfere.3. Encourage coughing until the obstruction is relieved.4. Monitor for progression to a severe obstruction.
1. Ask the person, “Are you choking?”2. If he nods ‘yes’ or is unable to speak, tell him you are
going to help. Do not leave the person.3. Stand behind him and reach under his arms.4. Make a fist with one hand and place it just above the
navel, thumb side in. Grasp the fist with your other hand.
5. Perform quick, forceful inward and upward abdomi-nal thrusts until the object is expelled or he becomes unresponsive.
aCTivaTe eMs• Mild obstruction is prolonged• You are unable to help with a severe obstruction
aDulT or ChilD Choking
Mild Obstruction
Severe Obstruction
Tip !

35
aDulT or ChilD Choking
If you are at home, unlock the front door so emer-gency responders can enter.
Minimize complications from abdominal thrusts by ensur-ing that your closed fist is placed above the navel but be-low the tip of the breastbone.
Unresponsive Choking Person
Chest Thrusts
Choking Prevention Tips
Chest Thrusts- Large or Pregnant Person
If a rescuer cannot reach around the waist of a large per-son, or the victim is obviously pregnant, use chest thrusts to relieve the obstruction.
1. Place one fist in the middle of the chest on the lower half of the breastbone, with your thumb against the chest.
2. Grasp the fist with your other hand.3. Pull straight back on the chest quickly and forcefully.4. Continue until the object is expelled or the victim be-
comes unresponsive.
• Cut food into small pieces. Cut round food in half or quar-ters.
• Chew food completely and eat slowly.• Do not talk or laugh with food in your mouth.• Protect young children from objects small enough to fit
through a toilet paper roll.
When a choking person becomes unresponsive, carefully lower the person to the ground. Use CPR to relieve the ob-struction.
1. Send someone to activate EMS. If alone, activate EMS after 2 minutes of CPR.
2. Perform CPR with the added step of looking in the mouth after each set of compressions. If you see the obstruction, remove it and continue CPR.
3. Continue CPR until the person begins to breathe nor-mally.
Large or pregnant: use chest thrusts
Unresponsive adult or child
Tip !
• Supervise mealtime for children. Keep them at the table when eating.
• Don’t drink too much alcohol during a meal.• Make sure dentures fit well.

36Foods that commonly cause choking in children: meat, grapes, popcorn, peanuts, peanut butter, round carrot slices, hot dogs, and hard candy.
If you are alone and choking, perform abdominal thrusts on yourself using your fist or a firm surface such as a table or the back of a chair.
infanT Choking (less Than 1 year)
Mild Obstruction
Severe Obstruction
Unresponsive Infant
Most incidents of choking in infants and young children occur when parents or caregivers are close by, usually during eating or play. Liquids such as juice or formula are the most common cause of choking in infants.
An infant will not give the universal sign of choking. Be alert and recognize a sudden onset of the following:
• Unable to cry or cough effectively• Difficulty or no breathing• Wheezing or high-pitched sound
When a choking infant becomes unresponsive, place the infant on a hard, flat surface. Use CPR to relieve the ob-struction.
1. Send someone to activate EMS. If alone, activate EMS after 2 minutes of CPR.
2. Perform CPR with the added step of looking in the mouth after each set of compressions. If you see the obstruction, remove it and continue CPR.
3. Continue CPR until the infant begins to breathe nor-mally.
Observe for signs of choking. If the infant can cough or cry, do not interfere. Monitor for progression to a severe obstruction. Do not leave the infant.
1. Observe for signs of choking.2. If there is a severe obstruction, send someone to acti-
vate EMS. Do not leave the infant.3. Sit or kneel down, then hold the infant face down on your
forearm with the head slightly lower than the chest.4. Give 5 back slaps forcefully between the shoulder
blades. 5. Support the infant between your arms and turn face up,
with the head lower than the body.6. Give 5 quick downward chest thrusts on the lower half
of the breastbone (same location as CPR), about 1 per second.
7. Repeat the sequence of 5 back slaps and 5 chest thrusts until the object is expelled, the infant cries or becomes unresponsive. 5 back slaps 5 chest thrusts
Unresponsive infant
Tip Tip
• Bluish color skin• Bulging or tearing eyes• Panic or distressed facial expression

37
how woulD you reaCT?
1
2
3
4
5
Law Enforcement
SCENARIOSQUESTIONS
Off Duty
Healthcare
EMS & Fire
While working your lifeguard tower at the beach, you notice an adult male struggling to reach the shore. After you perform a rescue, you assess the victim and notice that he has difficulty speaking and using his right side, and appears to be confused. How would you REACT?
You are working at a walk-in clinic, talking with an adult female who is complaining of pain in her jaw, short-ness of breath, nausea and fatigue that began about 2 hours ago. She appears sweaty and pale. How would you REACT?
You are out for dinner when you notice an adult patron stand up and clutch his throat. He looks panicked. A person next to him asks if he is all right, but the adult patron cannot speak. How would you REACT?
You are a correctional officer supervising inmates in a recreational area, when you find an adult male inmate down on the ground. He appears unresponsive; the stomach area of his shirt appears to be soaked with blood. There are other inmates nearby. How would you REACT?
Possible hazards at an emergency scene may include:
a. Fire or smokeb. Blood or body fluidsc. Trafficd. Unstable structurese. All of the above
Implied consent allows you to treat an unrespon-sive person.
True False
You do not need to wear gloves when giving care to a bleeding child because he or she will not car-ry bloodborne pathogens.
True False
Women may experience different heart attack signs and symptoms from men. True False
If a victim has difficulty speaking or weakness on one side of the body, he or she should:
a. Wait to see if it will passb. Call a doctorc. Drive to the emergency departmentd. Call 9-1-1

38
aDvanCeD equiPMenT
When performing CPR, a team may be composed of rescuers with different levels of training. EMTs, paramedics, nurses and physicians may use equipment that is not part of a standard BLS course. Rescuers should become familiar with this equipment and understand how it is used.
Suction devices are designed to remove blood, secretions, or vomit from the victim’s airway. EMS personnel use both manual and battery-operated units. Either a rigid suction tip or a flexible suction catheter will be used with the device.
Prior to performing suctioning, measure the distance from the corner of the victim’s mouth to the ear lobe. This is the maximum distance the rigid or flexible catheter is inserted into the mouth. Inserting too deeply may stimulate the gag reflex, compromising the airway.
While a patient is being suctioned, remove the CPR mask from the victim’s face. Turn his or her head to the side and wipe out any large debris with a gloved hand. Insert the catheter, and observe for fluid traveling up the tube.
Suction Devices
Battery-operated suction device
Rigid suction tip
Flexible suction tip
If a rescuer must clear the mouth of large debris and cervical spine injury is suspected, carefully roll the victim to the side as a unit, sweep out the mouth, and roll back.
Use sterile water to cleanse the suction catheter if it becomes obstructed.Tip Tip

39
aDvanCeD equiPMenT
The terms simple airway and advanced airway describes devices used by EMS and healthcare personnel to establish or control the airway of a patient in distress. Simple airways (oral and nasal) may be inserted only by responders trained in their use. While rescuers trained at the BLS level will not use advanced airways, they may interact with and assist advanced medical providers who are using them. The course does not provide training in the placement of simple and ad-vanced airways.
Oral AirwaysThe oropharyngeal airway (OPA) is the most commonly used airway adjunct. It is placed along the roof of the mouth and rotated into position so that it rests at the back of the throat. The end of the airway rests on the lips and will be visible to the rescuer. The backbone of the OPA keeps the tongue off the back of the airway, allowing air exchange.
OPAs are used with unresponsive patients who do not have a gag reflex. They are available in adult, child, and infant sizes. Choose the correct size, because an airway that is too large may trigger a gag reflex and cause vomiting. If the OPA is too long or inserted incorrectly, the airway may become blocked.
Choose the correct size by measuring from the level of the front teeth to the angle of the jaw or the earlobe.
Nasopharyngeal airway
Oropharyngeal airway
Airway Adjuncts
When a simple airway is in place, continue cycles of compressions and ventilations during CPR.Tip
Nasal AirwaysNasopharyngeal (NPA) airways are inserted into the nose of victims who are semiconscious and have a gag reflex. They are made of soft rubber or latex and are very pliable, but sturdy enough to remain patent. These are tolerated more easily than OPAs, but do not control the airway as completely.
The correct size is determined by measuring the distance from the base of the nose to the base of the ear. The tip is lubricated with lubricant or sterile water and is inserted into the nostril. When inserted correctly, the ring at the end of the device is visible at the nose, and the sound of air move-ment is heard when the lungs expand and contract.
Do not use an NPA when there is a suspected fracture to the base of the skull or severe facial trauma.!

40
aDvanCeD equiPMenT
Supplemental Oxygen
Advanced Airways
Supplemental oxygen has been used for years by healthcare providers and professional rescuers when responding to a medical emergency. By increasing the oxygen concentration in the lungs, more oxygen can potentially reach the brain and vital organs. The goal is to prevent damage to the brain and other vital organs, and to stabilize the heart.
Oxygen can be delivered through a ventilation device such as a face mask or bag mask, a nasal cannula, or a non-re-breather mask. Follow state, local, and workplace regulations and protocols on the use of supplemental oxygen during an emergency.
Emergency Oxygen Administration is a separate course that can be renewed when your CPR certification is renewed.
Move oxygen several feet away before AED shock
Positive pressure ventilation with an endotracheal tube
Supplemental oxygen
Although supplemental oxygen normally requires a prescription, the use of emergency oxygen does not. Do not delay starting CPR in order to set up oxygen.Tip !
Advanced airways are used by professionals trained in ACLS. Examples of advanced airways include the follow-ing: an endotracheal (ET) tube, laryngeal mask airway (LMA), Combitube, or supraglottic airway. When an advanced airway is in place, rescuers no longer need to pause compressions while providing ventilations.
For victims of all ages provide:• 1 breath every 6 – 8 seconds (8 – 10 breaths/minute)• At least 100 compressions/minute without pauses for
breaths.

41
Bag mask with oxygen
eMergenCy oxygen (oPTional CerTifiCaTion)
Oxygen is a basic need for survival. The air we breathe contains about 21% oxygen. Certain medical conditions may cause the body to breathe in less oxygen, or deliver less oxygen to the organs and tissues. During an emergency, providing sup-plemental oxygen at a higher concentration than room air may allow more oxygen to be absorbed into the bloodstream and delay damage to vital organs.
Emergency oxygen is used primarily to correct mild to moderate hypoxia (insufficient oxygen delivered to the organs and tissues) and reduce the work of the heart. Guidelines for the treatment of hypoxia may differ between first aid provid-ers and professional rescuers. Follow your local EMS authority or Medical Director’s guidelines if they differ from this training. Always use standard or universal precautions, according to your workplace and OSHA guidelines, to protect your-self from exposure to infectious diseases when giving care to a patient.
Only use emergency oxygen:• After EMS has been activated.• When additional trained rescuers are available who
are not assigned other critical tasks (e.g. performing CPR, controlling severe bleeding).
Never delay critical patient care in order to prepare and administer emergency oxygen.
What is Emergency Oxygen?
Never Delay Critical Care
The use of supplemental oxygen may delay damage to vital organs, stabilize the heart, and even save a life!
An Organization’s Medical Director should review and approve emergency oxygen use and training. TipTip
Emergency oxygen
Oxygen is considered a drug, and is regulated by the FDA. Rescuers must be trained in its use and storage. 100% pure oxygen is stored in cylinders as a highly compressed gas. When supplemental oxygen is given to a patient, it is con-sidered either medical oxygen or emergency oxygen, de-pending on how it is used. Oxygen flow is measured in liters per minute (LPM).
Medical oxygen requires a prescription for use. The deliv-ery rate is less than 6 LPM or the duration is less than 15 minutes.
Emergency Oxygen:• Does not require a prescription• Has a delivery rate of at least 6 LPM for 15 min. or
longer• Must be clearly labeled as Emergency Oxygen
Emergency oxygen is delivered from a cylinder, through a pressure regulator and oxygen tubing, and into a delivery device such as a mask, cannula or bag mask.

42
guiDelines for eMergenCy oxygen use
Use emergency oxygen to treat breathing difficulty based on the patient’s condition, work of breathing and respiratory rate. Consider using emergency oxygen for:
• Respiratory rates that are too fast or too slow ◦ Adult < 12 or > 20 breaths per minute ◦ Child < 15 or > 30 breaths per minute ◦ Infant < 25 or > 50 breaths per minute
• No breathing• Cyanosis (bluish color in skin, lips and fingernail beds)• Diving decompression injuries
The emergency oxygen cylinder, also known as a ‘tank’ or a ‘bottle,’ is typically green or has green markings. It should be labeled “U.S.P.” and marked with a yellow diamond and the statement, “For emergency use only.” Cylinders are made of metal and have a built-in valve at the top. An oxy-gen wrench, which should be stored with the cylinder, is used to open the valve. An o-ring (gasket used to create a seal) usually accompanies a newly-filled cylinder.
Oxygen cylinders come in different sizes, and hold differ-ent amounts of oxygen (measured in liters). Emergency oxygen that is brought to the scene is usually stored in a D (425L), Jumbo D (640L), or E (680L) cylinder. It must be small enough to be carried by one person and secured on a cot, stretcher or gurney with the patient during transport.
Patient Assessment
Oxygen Equipment
Oxygen cylinders
Guidelines for the use of emergency oxygen may differ at the State and local levels. Contact your local medical control or EMS agency to identify any local practices or guidelines that may differ from this training.Tip
Oxygen Cylinders
Professional rescuers and healthcare providers may provide emergency oxygen based on additional signs and symptoms or if certain conditions are suspected. In addition to the guidelines previously stated, consider using emer-gency oxygen for:
• Heart attack/suspected ACS• Stroke• Severe asthma• Pulmonary embolism• Shock• Drowning• Pregnancy-related emergency• Exacerbated COPD• Hypothermia (use warmed oxygen)
Always follow state and local protocols.
Before deciding to use emergency oxygen to treat difficulty breathing, assess the patient’s effort to breathe.Signs of difficulty breathing can include:
• Labored breathing: using accessory muscles in the neck and back, heaving chest, speaking in broken sentences
• Noisy breathing: coughing, wheezing• Tripod position: sitting up position supported on arms• Cyanosis
To calculate the RPM (respirations per minute):• Use a stopwatch, second hand or other timer.• Watch the patient’s chest for 15 seconds.• Multiply the number of breaths in 15 seconds x 4.• e.g. 5 breaths in 15 seconds = 20 RPM, an accept-
able rate for adults.

43
oxygen equiPMenT
Once the pressure regulator is fitted to the cylinder, oxygen tubing connects the regulator to the oxygen delivery device.
1. Remove the protective seal over the cylinder valve, and ensure the valve is dry and clean. Slowly open and close the valve to expel particles.
2. Inspect the o-ring in the pressure regulator, and replace it if missing or worn.3. Line up the pins on the regulator with the holes on the cylinder valve, and slip the regulator over the valve. Secure in
place by turning the thumbscrew until hand tight.4. Turn the pressure gauge away from rescuers and bystanders and open the valve (counterclockwise) one full turn.5. Read the pressure gauge to determine the pressure in the cylinder.6. Listen for leaking air to ensure a tight seal between the regulator and the valve.
The pressure regulator, which connects the cylinder valve to the oxygen tubing, controls the rate of oxygen flow (LPM). There are two common types of regulators used for emer-gency oxygen:
• Dual Flow Regulator: Has only 2 settings- HIGH and LOW.
• Full Control Regulator: Can dial in the desired flow of oxygen from 2 – 25 LPM. Used primarily by profes-sional rescuers.
The pressure regulator has a gauge that displays the amount of pressure (psi) inside the cylinder. The pressure indicates the amount of oxygen in the cylinder.
• 2,000 psi = Full• 1,000 psi = Half Full• 500 psi = Time to refill
If the pressure is < 200 psi, do not use it.Pressure regulator
Connecting a Pressure Regulator
Replace the o-ring each time you refill and prepare a cylinder to maintain the best seal between the cylin-der valve and the pressure regulator.
TipOnly an authorized oxygen vendor or worksite with spe-cialized equipment and training should refill an oxygen cylinder.!
Pressure Regulator

44
oxygen Delivery DeviCes
Use a non-rebreather mask or a nasal cannula to delivery emergency oxygen to a patient who is breathing.
The non-rebreather mask is the preferred device. It de-livers a high concentration of oxygen to a patient who is breathing. It consists of a clear mask, one-way valve, oxy-gen reservoir, and oxygen tubing. The non-rebreather mask is most effective with a flow rate of 15 LPM, and can deliver O2 concentration as high as 90%.
The nasal cannula is a low-flow oxygen device, provid-ing between 2 – 6 LPM, and a maximum O2 concentration of about 44%. It consists of a loop of oxygen tubing with 2 prongs that are inserted into a patient’s nostrils. Use the nasal cannula when a patient is non-critical or cannot toler-ate a non-rebreather mask. Set the liter flow for 6 LPM for emergency oxygen administration.
Using a nasal cannula:1. Confirm that rescue breathing is not required.2. Inform the patient that you are going to provide some
oxygen.3. Select the right size (adult, child, or infant).4. Connect the oxygen tubing to the emergency oxygen
source. Ensure the valve is open and adjust the flow to 6 LPM.
5. Listen for the sound of oxygen flowing from the prongs.
6. Slide the adjusting band away from the prongs to fully open the cannula loop. Hold the loop with your thumb and forefingers on either side of the prongs.
7. Explain the procedure to the patient. Explain that the prongs won’t hurt.
8. Carefully insert the prongs into the patient’s nostrils. While holding the prongs in position, slide your fin-gers along the loop and wrap each side around the patient’s ears.
9. Slide the adjusting band up towards the chin. Do not overtighten or pinch the skin.
10. Instruct the patient to breathe in through his or her nose.
Using a non-rebreather mask:1. Confirm that rescue breathing is not required.2. Inform the patient that you are going to provide some
oxygen.3. Select the right size mask (adult, child, or infant).4. Connect the oxygen tubing to the emergency oxygen
source. Ensure the valve is open and adjust the flow to 15 LPM.
5. Listen for the sound of oxygen flowing through the mask.
6. Place your thumb or finger over the one-way valve in-side the mask to speed up filling the oxygen reservoir.
7. Place the mask over the patient’s face, covering the mouth and nose. Secure in place with the elastic band.
8. Instruct the patient to breathe as normally as possi-ble.
Non-Rebreather Mask
Nasal Cannula
Non-rebreather mask
Nasal cannula
Some people cannot tolerate a non-rebreather mask, and may need reassurance that they are get-ting more oxygen than normal.
Tip Monitor the O2 reservoir in the non-rebreather mask to en-sure it does not completely deflate and has enough time to refill between breaths. Increase the liter flow if needed.!

45
oxygen Delivery DeviCes
The bag mask and CPR face mask with oxygen inlet can be used to deliver emergency oxygen to a patient who is not breathing. During resuscitation, the bag mask and face mask may increase the amount of oxygen delivered with rescue breaths.
The bag mask consists of a rigid face mask and self-inflat-ing bag attached to an oxygen reservoir. Tubing connects the bag mask to the oxygen source. The bag mask requires training to be used effectively, and is generally used only by healthcare providers and professional rescuers.
The CPR face mask with oxygen inlet is used for rescue breathing.
Using a CPR face mask:1. Confirm the victim is not breathing. Follow the guide-
lines for CPR, AED use, and activating EMS.2. Select the appropriate size (adult, child or infant).3. Connect the oxygen tubing to the oxygen inlet on the
CPR face mask. Connect the other end of the tubing to the emergency oxygen source. Ensure the valve is open and adjust the flow to 15 LPM.
4. Use the face mask to give rescue breaths. Ensure there is a complete seal between the patient’s face and the mask. Watch for chest rise with each breath. Do not over-ventilate.
Using a bag mask:1. Confirm the victim is not breathing. Follow the guide-
lines for CPR, AED use, and activating EMS.2. Select the appropriate size (adult, child or infant) and
assemble the bag mask. 3. Connect the oxygen tubing to the emergency oxygen
source. Ensure the valve is open and adjust the flow to 15 LPM.
4. Use the bag mask to give rescue breaths. Ensure there is a complete seal between the patient’s face and the mask. Watch for chest rise with each breath. Do not over-ventilate.
Bag mask components
Using a bag mask
CPR face mask
A bag mask and CPR face mask with oxygen inlet can also be used for patients who are conscious and breathing. Instruct the patient to hold the device to his or her face. Use a flow rate of 15 LPM for a bag mask, and between 6-15 LPM for a CPR face mask.
Bag Mask
CPR Face Mask
Tip

46
MoniToring oxygen Delivery
Risks of Oxygen Delivery
Monitor Oxygen Delivery
In general, the benefits of emergency oxygen administration outweigh the risks. Provide emergency oxygen when indicated by a patient’s signs and symptoms, and according to local and workplace guidelines. Some risks include the following:Oxygen Toxicity: Prolonged exposure to high concentrations of oxygen can result in too much oxygen in the blood. COPD: There is some concern that if a person with COPD is given oxygen, it will decrease the stimulus to breathe. In an emergency, the cause of difficulty breathing may be related to a condition other than COPD. Do not withhold emergency oxygen administration to a patient with a history of COPD if he or she has signs or symptoms that may benefit from it.
A pulse oximeter is a small, portable electronic device that monitors the blood-oxygen level, or oxygen saturation.Emergency oxygen administration should be based on target oxygen saturation levels, not fixed flow rates, to decrease the risks associated with oxygen delivery. A trained responder with a pulse oximeter should titrate the inspired oxygen to the lowest effective level, usually 94% to 99%, in a patient with circulation. If a patient’s O2 saturation level reaches 100%, follow local protocols regarding decreasing the flow rate or changing to a low-flow device.
To use a pulse oximeter:• Turn it on and connect the monitoring probe.• Attach the probe to the finger, earlobe, or foot per
manufacturer’s instructions.• Allow the pulse oximeter to register the O2 saturation
level and pulse rate.• Verify the pulse rate with the patient’s actual pulse
rate.• Monitor and record the O2 saturation levels while pro-
viding emergency oxygen.
Most non-medical settings do not have a pulse oximeter available when responding to an emergency. A first aid provider should give emergency oxygen when indicated. The monitoring of oxygen delivery and titration of inspired oxygen may need to wait until professional rescuers arrive or the patient is transported to the emergency department.
If an Organization has emergency oxygen onsite, at least one staff member certified in its use should be present at all times during business hours.
Monitor oxygen deliveryPulse oximeter
Using oxygen to treat ‘breathlessness’ rather than low oxygen saturation levels has not been shown to help the feeling of breathlessness.
If spontaneous circulation is restored in a patient af-ter cardiac arrest, titrate emergency oxygen to limit the risk of oxygen toxicity.
Tip Tip
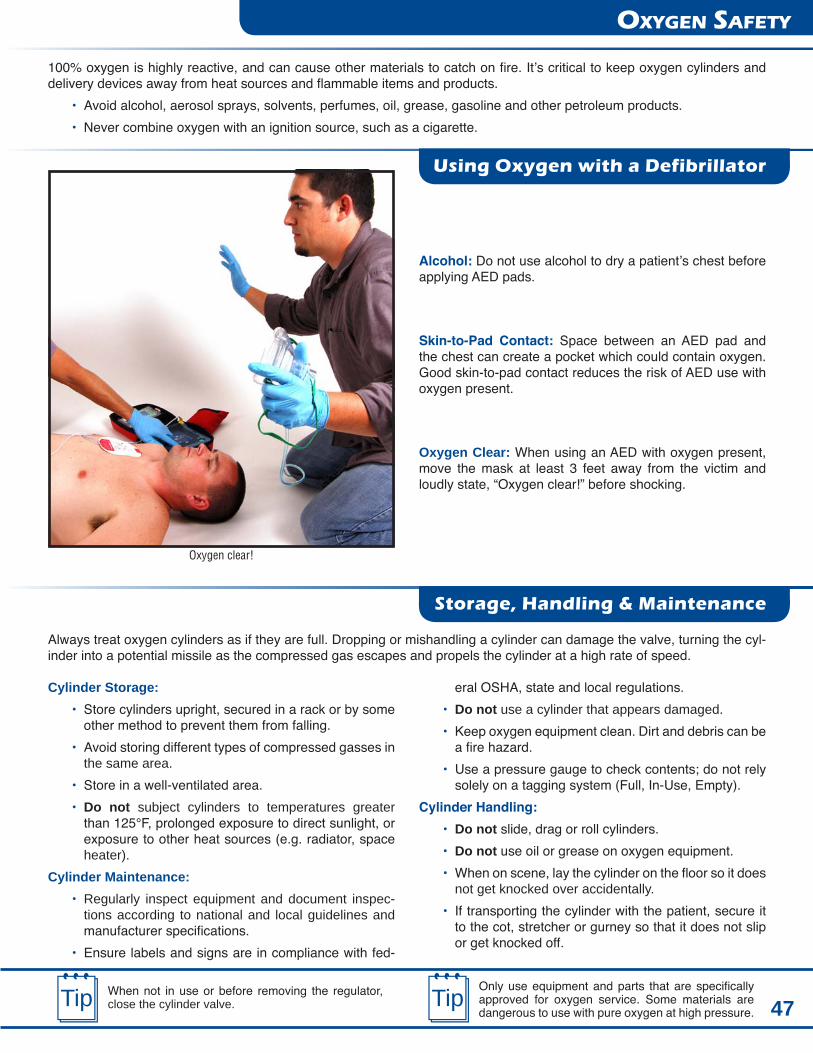
47
oxygen safeTy
100% oxygen is highly reactive, and can cause other materials to catch on fire. It’s critical to keep oxygen cylinders and delivery devices away from heat sources and flammable items and products.
• Avoid alcohol, aerosol sprays, solvents, perfumes, oil, grease, gasoline and other petroleum products.• Never combine oxygen with an ignition source, such as a cigarette.
Alcohol: Do not use alcohol to dry a patient’s chest before applying AED pads.
Skin-to-Pad Contact: Space between an AED pad and the chest can create a pocket which could contain oxygen. Good skin-to-pad contact reduces the risk of AED use with oxygen present.
Oxygen Clear: When using an AED with oxygen present, move the mask at least 3 feet away from the victim and loudly state, “Oxygen clear!” before shocking.
Always treat oxygen cylinders as if they are full. Dropping or mishandling a cylinder can damage the valve, turning the cyl-inder into a potential missile as the compressed gas escapes and propels the cylinder at a high rate of speed.
Cylinder Storage:• Store cylinders upright, secured in a rack or by some
other method to prevent them from falling.• Avoid storing different types of compressed gasses in
the same area.• Store in a well-ventilated area.• Do not subject cylinders to temperatures greater
than 125°F, prolonged exposure to direct sunlight, or exposure to other heat sources (e.g. radiator, space heater).
Cylinder Maintenance:• Regularly inspect equipment and document inspec-
tions according to national and local guidelines and manufacturer specifications.
• Ensure labels and signs are in compliance with fed-
Oxygen clear!
When not in use or before removing the regulator, close the cylinder valve.
Only use equipment and parts that are specifically approved for oxygen service. Some materials are dangerous to use with pure oxygen at high pressure.
Tip Tip
Using Oxygen with a Defibrillator
Storage, Handling & Maintenance
eral OSHA, state and local regulations.• Do not use a cylinder that appears damaged.• Keep oxygen equipment clean. Dirt and debris can be
a fire hazard.• Use a pressure gauge to check contents; do not rely
solely on a tagging system (Full, In-Use, Empty). Cylinder Handling:
• Do not slide, drag or roll cylinders.• Do not use oil or grease on oxygen equipment.• When on scene, lay the cylinder on the floor so it does
not get knocked over accidentally.• If transporting the cylinder with the patient, secure it
to the cot, stretcher or gurney so that it does not slip or get knocked off.

48
ProDuCTs
AED and CPR
First Aid Kits
Prepare Before the Next Emergency or Disaster Strikes!
Order your first aid and disaster readiness products today.Contact your Instructor or visit www.emssafety.com
Disaster and Safety
AED Units and Supplies
For the workplace, home, or personal use
Disaster Readiness Food and Supplies Pet Safety
CPR Barriers

CPR & AEDfor Professional Rescuers
Emergency Response for Healthcare Providers and Professional Rescuers
2010 Guidelines
Quality Training Programs:
Basic First AidAdvanced First Aid
CPR & AED for the Community & WorkplaceCPR & AED for Healthcare and Professional Rescuers
CPR & First Aid for Childcare ProvidersCPR, AED, & First Aid for the Senior Community
Oxygen AdministrationBloodborne Pathogens
Instructor Training
Available in Spanish
EMS Safety Services, Inc.1046 Calle Recodo, Suite KSan Clemente, CA 92673(800) 215-9555www.emssafety.com
Student Workbook