stroke history - pdfs.semanticscholar.org · vasospasm could be observed. antunes 7 reported that...
TRANSCRIPT
e11
Celsus may have described subarachnoid hemorrhage (SAH) when he wrote in A.D. 30, “The characteristic
marks… are strong shivering, nervous relaxation, dimness of sight, delirium, vomiting together with a suppression of voice, besides these symptoms there is a violent pain chiefly about the temples or occiput”.1 Hippocrates in Aphorisms on Apoplexy probably described a case: “When persons in good health are suddenly seized with pains in the head, and straight-way are laid down speechless, and breathe with stertor, they die in seven days.” Neglecting the patient who would in those days die rapidly without articulating their history, could this be a description of “vasospasm,” or in current terminology, delayed cerebral ischemia (DCI)?
Aneurysms were well known to the ancients, but those located intracranially eluded detection by virtue of being encased in the cranium and not palpable or large and easily accessible to clinical or postmortem assessment. McDonald and Korb2 credited Biumi with describing in 1778 the first pathologically verified case of ruptured intracranial aneurysm. Weir wrote that Gull may have been the first to describe DCI in a 30-year-old female in 1859: “while walk-ing, she suddenly called out, ‘Oh, my head’ and put up her left hand. She vomited, and her friend thought, fainted. After a brief interval she partially recovered, and was able to walk back to her residence with the support of two men. When admitted to the hospital at noon the following day, only a slight impression could be made by any attempt to rouse her. The right arm was quite paralysed, the muscles flaccid; the right leg in the same condition….”3
The text goes on to describe improvement in her condition such that on day 4 she could talk and eat. However, on the fifth day she deteriorated and died and was found to have SAH in the left Sylvian fissure at autopsy. There was softening of the left hemisphere, blood in the ventricles, and 2 middle cerebral artery aneurysms, one of which was ruptured (Figure).3–22
Hunter4 was one of the earliest to state that “There are 3 states in which an artery is found, viz. first, the natural pervious state; second, the stretched; and third, the contracted state…. The contracted state of an artery arises from the action of the
muscular power….” Much of their knowledge was based on observation of trauma-induced constriction of arteries, a find-ing that led to theories that cerebral angiographic vasospasm was because of mechanical factors, that persisted even into the 1980s. Systemic arteries were observed to be innervated and much early work also focused on these nerves being important in vasospasm. Writing in 1728, Lancisi thought vasospasm caused aneurysms of peripheral arteries by increasing the pressure proximal to the spasm. Although I have not identified the basis for his conclusions, Luys23 wrote that the cerebral circulation was necessary for consciousness but also, in turn, the brain regulated its own circulation in that neuronal activity seemed to be associated with increased blood flow. By 1911, Cow24 wrote that chemicals such as carbon dioxide and amyl nitrite had been known for years, probably since the mid 19th century, to lower blood pressure by dilating arteries and that other substances constricted them.5 Cerebral vasospasm was used to explain transient ischemic attacks and other transient neurological phenomena.
Although he was not the first to study brain vasomotor responses, Florey6 observations in 1925 of constriction of cat cerebral arteries in vivo in response to electric, mechanical, and chemical stimulation—barium chloride was a powerful constrictor and nitrites were vasodilators, would later become an important basis for early experimental models of angio-graphic vasospasm.
The invention of lumbar puncture by Quinke in 1891 led to the ability to diagnose SAH antemortem. Around the same time, Symonds25 considered Froin26 thesis important in giving early description of changes in the cerebrospinal fluid after SAH, findings which remain correct to this day. The color changes from bright red to cherry red ≈5 days after SAH, the erythrocyte count declines after the third day and the super-natant fluid becomes increasingly yellow after the first day. The clinical course of untreated SAH, cerebrospinal fluid find-ings, etiologies, and key prognostic factors were startlingly well described and known even at that time, the main short-comings being lack of methods to image what was occurring
Origins of the Concept of VasospasmR. Loch Macdonald, MD, PhD
Received November 4, 2014; final revision received November 4, 2014; accepted December 30, 2014.Division of Neurosurgery, St. Michael’s Hospital, Labatt Family Centre of Excellence in Brain Injury and Trauma Research, Keenan Research Centre
for Biomedical Science, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Ontario, Canada; and Department of Surgery, University of Toronto, Ontario, Canada.
Correspondence to R. Loch Macdonald, MD, PhD, Division of Neurosurgery, St. Michael’s Hospital, Labatt Family Centre of Excellence in Brain Injury and Trauma Research, Keenan Research Centre for Biomedical Science, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Ontario, Canada. E-mail [email protected]
(Stroke. 2016;47:e11-e15. DOI: 10.1161/STROKEAHA.114.006498.)© 2015 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.006498
Section Editor: J.P. Mohr, MD, MS
Section Editor: J.P. Mohr, MD, MS
Stroke History
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
ugust 3, 2017http://stroke.ahajournals.org/
Dow
nloaded from
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
e12 Stroke January 2016
antemortem as well as limited understanding of the molecular and biochemical basis for the changes.
It was not until blood vessels could be visualized that vasospasm could be observed. Antunes7 reported that Haschek and Lindenthal27 were among the first to visualize blood ves-sels on radiographs by injecting opaque solutions into them in cadavers in 1895 and Berberich and Hirsch28 obtained extremity angiograms in 1923. Moniz, however, is credited with developing cerebral angiography. Robertson8 may have been the first to recognize the association of cerebral infarc-tions with ruptured aneurysms. In 5 pathologically examined cases, the infarctions are suggestive of DCI and of the types of infarctions or cortical damage seen under thick subarach-noid blood clots. He hypothesized the infarctions were caused by temporary arterial spasm because the arteries did not con-tain thrombi or emboli. Subsequent autopsy series by Birse and Tom29 identified focal, diffuse, patchy cortical necrosis in some cases that can now be observed radiologically. In 1964, Crompton30 associated cerebral infarctions at autopsy with the location of subarachnoid blood and with angiographic vasospasm.
There were several contemporaneous descriptions of angiographic vasospasm.9,10,31 Falconer31 thought it might be secondary to the contrast medium and does not seem to have been convinced as to its existence. The most well-known initial description was by Ecker and Riemenschneider9 who described 6 cases of reversible intradural arterial narrow-ing in patients with untreated, ruptured aneurysms. An early hint at the time course was their observation that spasm was only observed on angiograms done within 23 days of SAH. They wrote that the function of arterial smooth muscle was unknown as was whether the arteries narrowed because of the smooth muscle or elastic tissue in their walls. It was already known that mechanical stimulation, such as after gunshot wounds or other traumatic injuries, of systemic and cerebral arteries led to constriction. The arteries also were known to be innervated, leading the authors to postulate that angiographic
vasospasm was because of mechanical effects of the SAH or perhaps because of activation of perivascular nerves. They speculated that patients who did not develop vasospasm would have continued bleeding from the aneurysm and die and thus that vasospasm was life-saving. However, they also suggested it could be detrimental by restricting blood flow to the brain. Ecker32 presented the angiographic findings of vasospasm at the Cushing meeting in 1951. He later wrote that senior mem-bers were shaking their heads in disbelief during his presenta-tion. There was 1 man who smiled, as if understanding. Ecker later wrote: “I addressed the rest of my remarks to him. In discussion, after some of the older men denied the existence of cerebral arterial spasm…. I went to the unknown smiling man in the front to thank him for his encouragement. He answered, smiling, ‘I don’t speak English.’”9,32
Pool33 described the typical clinical picture of DCI in 1958. Treatment focused on topical application or intra-arte-rial injections of papaverine or procaine at the time of surgery. These treatments arose out of experiments in animals show-ing that these drugs reversed acute, mechanically induced spasm of cerebral arteries. Because papaverine was known to act directly on smooth muscle, and procaine on nerves, they interpreted this as evidence that angiographic vasospasm was because of neural mechanisms and to smooth muscle contrac-tion.33 They considered the possibility that it was something in the blood but thought this was an inadequate explanation because they sometimes observed vasospasm at craniotomy after the SAH had cleared away.
From the late 1950s until even in to the 1980s, controver-sies persisted about SAH, including about timing of surgery. Rebleeding was widely recognized as a cause of death but early surgery was particularly hazardous. Intracranial aneu-rysm surgery often was thought best performed 7 to 10 days after SAH, during what is now known to be the worst time when there is a high risk of DCI.1 Without knowing that angio-graphic vasospasm did not begin until 3 or 4 days after SAH, they misinterpreted its appearance after aneurysm surgery as
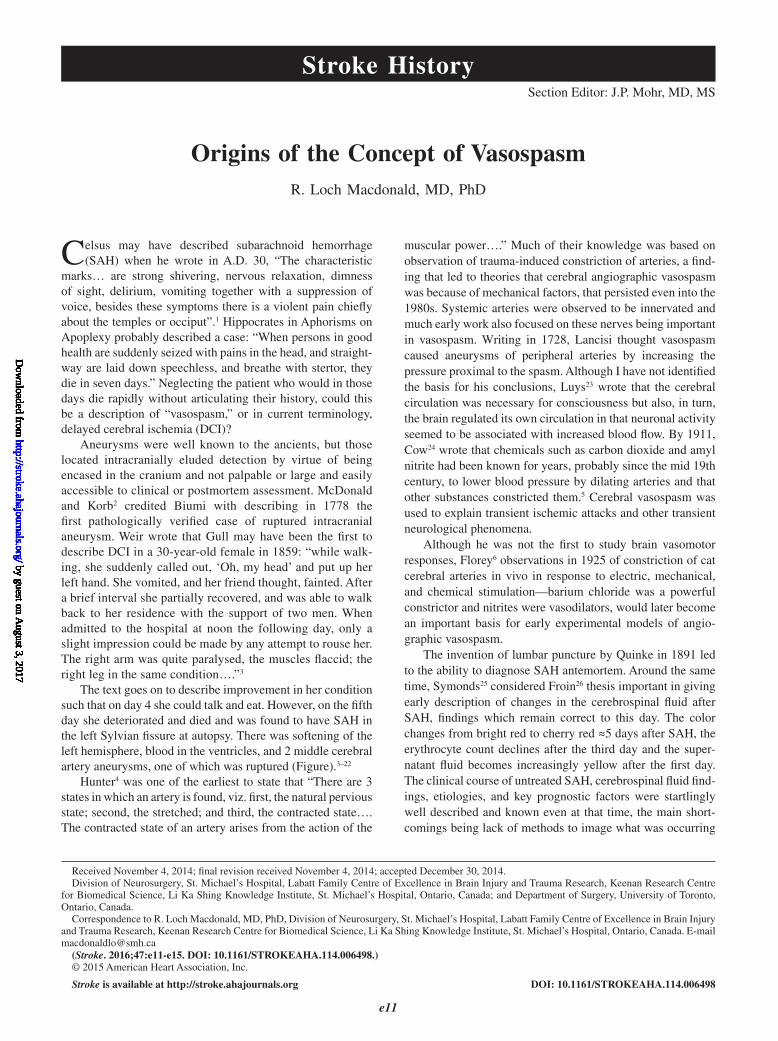
Figure. A time line with some selected events in the history of angiographic vasospasm, delayed cerebral ischemia, and subarachnoid hemorrhage, leading to current understanding of the pathophysiology shown in the lower right (reprinted from *Antunes7 with permission of the publisher. Copyright © 1974, the European Society of Cardiology; †Norlen et al10 with permission of the publisher. Copyright © 1952, the American Association of Neurological Surgeons; ‡Kosnik and Hunt13 with permission of the publisher. Copyright © 1976, the American Association of Neurological Surgeons; §Weir et al17 with permission of the publisher. Copyright © 1978, the American Associa-tion of Neurological Surgeons; ||Maroon and Nelson18 with permission of the publisher. Copyright © 1979, Wolters Kluwer Health; and Zubkov et al19 with permission of the publisher. Copyright © 1983, Springer).
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from

Macdonald Vasospasm e13
being postoperative spasm because of the surgery. In any case, by the late 1950s, it seems to have been recognized that angio-graphic vasospasm could be associated with focal neurologi-cal deficits and progress to coma and death, and that earlier reports had not usually distinguished this DCI from rebleed-ing. Walton1 wrote “Hemiparesis and other neurologic signs in the extremities cleared up completely in 14 patients dur-ing their stay in hospital; probably in these cases neurologic deficit resulted from temporary ischaemia or from compres-sion….” Surgery in the setting of unrecognized angiographic vasospasm combined with use of induced hypotension both preoperatively to prevent rebleeding, and also intraoperatively to reduce the risk of intraoperative aneurysm rupture, often indirect surgery by carotid ligation and that patients were usu-ally volume depleted led to predictably poor results.
It had been known for >20 years that chemicals, including serotonin, derived from blood, contracted cerebral arteries but it was Echlin34 who conducted extensive experiments build-ing on the previous studies of cerebral arterial constriction in response to mechanical and chemical stimulation. He noted cerebral arterial constrictions in monkeys in response to fresh blood, leading him to advocate a search for substances in blood responsible for angiographic vasospasm. Experimental mod-els of vasospasm that initially involved topical applications of drugs or blood to exposed cerebral arteries were later changed to include injections of blood into the subarachnoid space, inducing SAH by perforating cerebral arteries or by placing clotted blood into the subarachnoid space. Numerous studies showed these tended to produce more prolonged vasospasm, but the reason for this was not clarified until computed tomo-graphic scan studies in humans confirmed the role of persis-tent SAH in causing angiographic vasospasm. Nevertheless, Kennady11 was already studying methods to speed clearance of subarachnoid blood in dogs. Alksne et al35 used plasmin in experimental SAH for the same purpose in studies coinciding with efforts to remove SAH surgically and predating the tissue plasminogen activator era.
Smith and Robertson must be credited with their vision to host the first of what became known as the vasospasm meet-ings in Jackson, Mississippi, in 1972. It was attended by 18 investigators. Smith was best known for investigating struc-tural changes in the cerebral arteries in response to SAH, the role of heparin and in his disciple’s work, such as Clower et al,36 whose work on platelets and the endothelium has been recently rediscovered.37 Robertson, with White,38 also made many contributions to understanding vascular contractions after SAH. Subsequent vasospasm meetings attracted up to several hundred participants. Much of the initial experimen-tal work focused on the role of innervation of the cerebral arteries, catecholamines and their antagonists as treatments for vasospasm, none of which panned out. There also was a Princeton Conference that year, where events that played out in 1975 between Millikan39 and neurosurgeons, includ-ing Thor Sundt and Charles Drake began. First, Millikan,39 a major figure in vascular neurology and the editor of Stroke, reviewed the literature on angiographic vasospasm and SAH as well as patients treated at the Mayo clinic in Rochester. He concluded there was no clinical presentation that was consis-tently present with angiographic vasospasm, that vasospasm
had no effect on mortality because of SAH and that there was no relationship between complications of surgery and vaso-spasm. Millikan39 emphasized the role of arterial thrombosis in producing ischemia after SAH. It was implied vasospasm was sometimes used by surgeons to explain surgical compli-cations as a cause of poor outcomes. It would generally be thought now that only the first of the 3 points is correct in that not all patients with moderate-to-severe angiographic vaso-spasm have DCI. This was already known. Sundt, an equally prominent figure in neurosurgery, who may have been a direct target of Millikan39 article (D. Piepgras, personal communi-cation, October 28, 2014), had written that the correlation between angiographic vasospasm and clinical condition was incomplete.40 The Millikan39 article included data on patients managed at the Mayo clinic and at that time, such articles needed to be registered with the clinic and there would be an offer made to include as authors the other physicians whose patients were being described. This did not occur. Sundt was livid and declared to the chair of neurosurgery that “he goes or I go.” The Mayo personnel committee reviewed the situa-tion and restrictions were placed on Millikan,39 which led to his departure to the University of Utah. He admitted to some inaccuracies in the data.39 Sundt died at 62 of cancer in 1992, a disease he thought he might have contracted from radiation from cerebral blood flow studies he conducted in service to his patients. Millikan39 outlived him, dying at 1995 in 2011.
At the same time, Fisher12 wrote the definitive description of DCI, first published in short form and was among the first to use a term such as delayed ischemic deficits. He noted that it developed 3 to 13 days after SAH, was reversible in 50% of cases and that angiographic vasospasm had to be severe to produce DCI. He assumed causation based on association. Investigators in Japan published virtually identical data.41 They emphasized the potential role of subarachnoid clot in sustaining angiographic vasospasm, discovered the key role of erythrocytes in the pathogenesis of vasospasm and use of cisternal drains to remove the clot. Treatment focused on the schizophrenic administration of intravenous cocktails of vaso-dilators, including isoproterenol, phentolamine, sodium nitro-prusside, reserpine, and aminophylline with vasoconstrictors to maintain blood pressure.
Weir et al17 clarified the time course of vasospasm in man by measuring cerebral artery diameters on 627 angiograms from 293 patients with aneurysms. Vasospasm was present 3 to 12 days after SAH, and maximal around 7 to 8 days. Within 4 years of the invention of computed tomography, Japanese neurosurgeons showed that angiographic vasospasm was associated with the volume and location of subarachnoid blood.14,15 This was formalized by Fisher et al,16 in one of the most cited articles about SAH.
Two medical developments ended the decade of the 1970s. Kosnik and Hunt13 knew that Denny–Brown had reported that raising blood pressure could alleviate ischemic neurologi-cal deficits. In 1976, they specifically reported improvement in neurological deficits in patients with SAH and surgically repaired aneurysms, with intravenous fluids and induced hypertension. In those days when patients developed hypona-tremia, they were fluid restricted. They commented that these patients may be frequently volume depleted. In 1979, Maroon
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from

e14 Stroke January 2016
and Nelson18 documented this for the first time. The pendu-lum swung from induced hypotension and fluid restriction to induced hypertension and volume loading and continues to be used to varying degrees in the absence of any level 1 evidence.
Fleckenstein,42 a German pharmacologist, discovered cal-cium channel antagonists. He recounted that in 1963, German pharmaceutical companies supplied him with drugs they had synthesized and found to be coronary vasodilators. He found that in cardiac muscle they mimicked the effects of calcium withdrawal. The key event was when in 1969, Bayer provided him with the first dihydropyridine compound, nifedipine, that turned out also to be a vasodilator. Another dihydropyridine, nimodipine, was developed specifically to be a cerebral vaso-dilator that would have less effect on blood pressure and be useful for treatment of cerebral disorders.43 After multiple preclinical studies, including a number showing that it had no effect on angiographic vasospasm, as well as human clinical trials, it was eventually approved by the US Food and Drug Administration in December, 1988, after having been avail-able in Europe since 1985. The Food and Drug Administration concluded that it reduced the effect of vasospasm at causing cerebral infarctions and poor outcomes, but did not affect angi-ographic vasospasm. Its mechanism of action was unknown, and remains so today. Nothing has achieved this since, despite trials on ≈32 other drugs.44
Balloon angioplasty was first used to treat angiographic vasospasm by Zubkov et al.19 Technology improved the safety of the procedure and also spurned use of superselective infu-sions of vasodilator drugs. The efficacy of endovascular treatments has never been proven, and they are not entirely consistent with the theory that angiographic vasospasm is an epiphenomenon that does not by itself cause DCI.
Thirty years after the 1972 Princeton Conference, was it planned to have a debate over whether preventing vasospasm improves outcome after SAH?45 Long-time friends Macdonald and Zhang sparred for the issue and the polls showed it was a draw. Nobody lost their jobs this time and Diringer45 con-cluded essentially the same thing as was known in 1972. Thus, the controversies over angiographic vasospasm persist to this day, but they have changed their focus. There is no disputing the existence of angiographic vasospasm but its contribution to DCI continues to be questioned. The studies of the endo-thelin antagonist, clazosentan, which reduced angiographic vasospasm but had no effect on clinical outcome, fueled the controversy.21 Sixty years after description of angiographic vasospasm, much has been learned and outcomes from SAH are better but as Diringer45 wrote: “the debate has fostered the recognition that we must broaden our field of view and consider that DCI results from a complex interaction among multiple processes.”
The initial studies of the pathology and pathogenesis of SAH focused on the brain and were followed by study of isolated blood vessels. History shows that neither compo-nent can be neglected. Current theory is that poor outcome after SAH results from an interaction of the initial vascular and brain effects of the SAH (early brain injury) followed by delayed neurological deterioration that may be because of DCI.44 DCI, in turn, is thought to be a result of interaction of multiple processes, including early brain injury, angiographic
vasospasm, cortical spreading ischemia, microthromboem-bolism, delayed neuronal apoptosis, dysautoregulation, and capillary transit time heterogeneity.44 What are the chal-lenges for the future? One will be understanding the value of continued animal experimentation and delineation of the pathophysiology of DCI in the aftermath of continued lack of translation to humans of treatments that are supposedly efficacious in animals. Possible reasons why drugs, such as clazosentan, statins, and magnesium did not improve out-come have been listed but elude precise determination.44 A lesson from history may be that of antifibrinolytics that were efficacious at their target action of reducing rebleeding, but had no effect on outcome as a result of their propensity to increase DCI and possibly thromboembolic complications. As we gain knowledge that increases the understanding, and complexity, of the disease, simple statistics suggests larger groups of patients need to be studied. Efforts to do this are underway and have identified lack of common data elements for SAH and led to a project to develop them.46 Centers less than a hundred miles apart think rescue therapy works at one and that it does not at another. This could be addressed in a randomized clinical trial. However, we are sometimes sur-prisingly unwilling to question our theories, and the current trend is toward comparative effectiveness research and col-lection of registry data. Cooperative studies and registries of SAH were conducted beginning decades ago and led to some advances in treatment of SAH. This author, however, would recommend focusing energies on more randomized clinical trials.47
DisclosuresDr Macdonald receives grant support from the Physicians Services Incorporated Foundation, Brain Aneurysm Foundation, Canadian Institutes for Health Research, and the Heart and Stroke Foundation of Canada; and is Chief Scientific Officer of Edge Therapeutics, Inc.
References 1. Walton JN. Subarachnoid Haemorrhage. Edinburgh, Scotland: E & S
Livingstone, Ltd; 1956. 2. McDonald CA, Korb M. Intracranial aneurysms. Archiv Neurol
Psychiatr. 1939;42:298–328. 3. Gull WM. Cases of aneurism of the cerebral vessels. Guys Hospital
Report 1859;5:281–304. 4. Hunter J. A Treatise on the Blood Inflammation and Gunshot Wounds.
Philadelphia, PA: J. Webster; 1813. 5. Brunton TL. The action of nitrate of amyl on the circulation. J Anat
Physiol. 1870;5(pt 1):92–101. 6. Florey H. Microscopical observations on the circulation of the blood in
the cerebral cortex. Brain 1925;48:43–64. 7. Antunes JL. Egas Moniz and cerebral angiography. J Neurosurg.
1974;40:427–432. doi: 10.3171/jns.1974.40.4.0427. 8. Robertson EG. Cerebral lesions due to intracranial aneurysms. Brain.
1949;72(pt 2):150–185. 9. Ecker A, Riemenschneider PA. Arteriographic demonstration of spasm of
the intracranial arteries, with special reference to saccular arterial aneu-rysms. J Neurosurg. 1951;8:660–667. doi: 10.3171/jns.1951.8.6.0660.
10. Norlen G, Falconer M, Jefferson G, Johnson R. The pathology, diagno-sis and treatment of intracranial saccular aneurysms. Proc R Soc Med. 1952;45:291–302.
11. Kennady JC. Investigations of the early fate and removal of subarachnoid blood. Pac Med Surg. 1967;75:163–168.
12. Fisher CM, Roberson GH, Ojemann RG. Cerebral vasospasm with ruptured saccular aneurysm–the clinical manifestations. Neurosurgery. 1977;1:245–248.
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from

Macdonald Vasospasm e15
13. Kosnik EJ, Hunt WE. Postoperative hypertension in the management of patients with intracranial arterial aneurysms. J Neurosurg. 1976;45:148–154. doi: 10.3171/jns.1976.45.2.0148.
14. Katada K, Kanno T, Sano H, Shibata T, Shah MY. Computed tomogra-phy of ruptured intracranial aneurysm in acute stage (author’s transl). No Shinkei Geka. 1977;5:955–963.
15. Takemae T, Mizukami M, Kin H, Kawase T, Araki G. Computed tomog-raphy of ruptured intracranial aneurysms in acute stage–relationship between vasospasm and high density on CT scan (author’s transl). No To Shinkei. 1978;30:861–866.
16. Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to sub-arachnoid hemorrhage visualized by computerized tomographic scan-ning. Neurosurgery. 1980;6:1–9.
17. Weir B, Grace M, Hansen J, Rothberg C. Time course of vaso-spasm in man. J Neurosurg. 1978;48:173–178. doi: 10.3171/jns.1978.48.2.0173.
18. Maroon JC, Nelson PB. Hypovolemia in patients with subarachnoid hemorrhage: therapeutic implications. Neurosurgery. 1979;4:223–226.
19. Zubkov I, Nikiforov BM, Shustin VA. 1st attempt at dilating spastic cere-bral arteries in the acute stage of rupture of arterial aneurysms. (Russian). Zhurnal Voprosy Neirokhirurgii Imeni N - N - Burdenko 1983;17–23.
20. Etminan N, Vergouwen MD, Ilodigwe D, Macdonald RL. Effect of pharmaceutical treatment on vasospasm, delayed cerebral ischemia, and clinical outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Cereb Blood Flow Metab. 2011;31:1443–1451. doi: 10.1038/jcbfm.2011.7.
21. Macdonald RL, Kassell NF, Mayer S, Ruefenacht D, Schmiedek P, Weidauer S, et al; CONSCIOUS-1 Investigators. Clazosentan to over-come neurological ischemia and infarction occurring after subarachnoid hemorrhage (CONSCIOUS-1): randomized, double-blind, placebo-controlled phase 2 dose-finding trial. Stroke. 2008;39:3015–3021. doi: 10.1161/STROKEAHA.108.519942.
22. Vergouwen MD, Vermeulen M, van Gijn J, Rinkel GJ, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneu-rysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41:2391–2395. doi: 10.1161/STROKEAHA.110.589275.
23. Luys J. Le Cerveau et ses Fonctions. Paris, France: Germer-Baillier & Cie; 1879.
24. Cow D. Some reactions of surviving arteries. J Physiol. 1911;42:125–143. 25. Symonds CP. Spontaneous sub-arachnoid hæmorrhage. Proc R Soc Med.
1924;17(Neurol Sect):39–52. 26. Froin G. Les hemorrhagies sous arachnoidiennes et le mechanism de
l’hematolyse en general These de Paris, No. 113, Paris, France; 1904. 27. Haschek E, Lindenthal OT. Ein beitrag zur praktischen verwerthung der
photographie nach rontgen. Wien Klin Wschr 1896;9:63–64. 28. Berberich J, Hirsch S. Die rontgenographische darstellung der arterien
und venun am lebenden menschen. Klin Wschr 1923;2:2226–2228. 29. Birse SH, Tom MI. Incidence of cerebral infarction associated with rup-
tured intracranial aneurysms. A study of 8 unoperated cases of anterior cerebral aneurysm. Neurology. 1960;10:101–106.
30. Crompton MR. The pathogenesis of cerebral infarction following the rupture of cerebral berry aneurysms. Brain. 1964;87:491–510.
31. Falconer MA. The surgical treatment of bleeding intracranial aneurysms. J Neurol Neurosurg Psychiatry. 1951;14:153–186.
32. Ecker A. The discovery of human cerebral arterial spasm in angiograms: an autobiographical note (Arthur Ecker). Neurosurgery. 1982;10:90.
33. Pool JL. Cerebral vasospasm. N Engl J Med. 1958;259:1259–1264. doi: 10.1056/NEJM195812252592605.
34. Echlin FA. Spasm of basilar and vertebral arteries caused by experimen-tal subarachnoid hemorrhage. J Neurosurg. 1965;23:1–11. doi: 10.3171/jns.1965.23.1.0001.
35. Alksne JF, Branson PJ, Bailey M. Modification of experimental post-subarachnoid hemorrhage vasculopathy with intracisternal plasmin. Neurosurgery. 1986;19:20–25.
36. Clower BR, Yoshioka J, Honma Y, Smith RR. Pathological changes in cerebral arteries following experimental subarachnoid hemorrhage: role of blood platelets. Anat Rec. 1988;220:161–170. doi: 10.1002/ar.1092200207.
37. Kapp JP, Neill WR, Neill CL, Hodges LR, Smith RR. The three phases of vasospasm. Surg Neurol. 1982;18:40–45.
38. White RP, Hagen AA, Robertson JT. Effect of nonsteroid anti-inflam-matory drugs on subarachnoid hemorrhage in dogs. J Neurosurg. 1979;51:164–171. doi: 10.3171/jns.1979.51.2.0164.
39. Millikan CH. Cerebral vasospasm and ruptured intracranial aneurysm. Arch Neurol. 1975;32:433–449.
40. Sundt TM Jr. Intracranial aneurysms and subarachnoid hemorrhage: a subject review for the clinician. Mayo Clin Proc. 1970;45:455–466.
41. Saito I, Ueda Y, Sano K. Significance of vasospasm in the treatment of ruptured intracranial aneurysms. J Neurosurg. 1977;47:412–429. doi: 10.3171/jns.1977.47.3.0412.
42. Fleckenstein A. History of calcium antagonists. Circ Res. 1983;52(2 pt 2):I3–16.
43. Towart R, Kazda S. The cellular mechanism of action of nimodipine (BAY e 9736), a new calcium antagonist [proceedings]. Br J Pharmacol. 1979;67:409P–410P.
44. Macdonald RL. Delayed neurological deterioration after subarach-noid haemorrhage. Nat Rev Neurol. 2014;10:44–58. doi: 10.1038/nrneurol.2013.246.
45. Diringer MN. Controversy: does prevention of vasospasm in subarach-noid hemorrhage improve clinical outcome? Stroke. 2013;44(6 suppl 1):S29–S30. doi: 10.1161/STROKEAHA.111.000008.
46. Jaja BN, Attalla D, Macdonald RL, Schweizer TA, Cusimano MD, Etminan N, et al. The Subarachnoid Hemorrhage International Trialists (SAHIT) Repository: advancing clinical research in subarach-noid hemorrhage. Neurocrit Care. 2014;21:551–559. doi: 10.1007/s12028-014-9990-y.
47. Darsaut TE, Raymond J. RCTs in determining treatment indications for intracranial aneurysms: what can we learn from history? Neurochirurgie. 2012;58:76–86. doi: 10.1016/j.neuchi.2012.02.022.
KEY WORDS: angiographic vasospasm ◼ brain ischemia ◼ cerebral aneurysms ◼ delayed cerebral ischemia ◼ subarachnoid hemorrhage ◼ vasospasm
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from
R. Loch MacdonaldOrigins of the Concept of Vasospasm
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.114.006498
2016;47:e11-e15; originally published online September 3, 2015;Stroke.
http://stroke.ahajournals.org/content/47/1/e11World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2016/12/26/STROKEAHA.114.006498.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on August 3, 2017
http://stroke.ahajournals.org/D
ownloaded from

74
1(41)’2016 НЕМНОГО ИСТОРИИ
Происхождение концепции вазоспазмаИсточник: R.L. Macdonald. Origins of the concept of vasospasm. Stroke. 2016;47:1:e11–e15Division of Neurosurgery, St. Michael’s Hospital, Labatt Family Centre of Excellence in Brain Injury and Trauma Research, Keenan Research Centre for Biomedical Science, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Ontario, Canada; and Department of Surgery, University of Toronto, Ontario, Canada.
Ключевые слова: проявление вазоспазма на ангиографии (angiographic vasospasm), ишемия мозга (brain ischemia), аневризмы цереб-ральных сосудов (cerebral aneurysms), отсроченная церебральная ишемия (delayed cerebral ischemia), субарахноидальное кровоизлияние (subarachnoid hemorrhage), вазоспазм (vasospasm)
Вполне возможно, что в 30-х гг. н.э. Цельс впервые описал субарахноидальное кровоизлияние (САК), когда он написал «Характерными признаками ... являются выра-женный тремор, нервная релаксация, ослабление зрения, бред, рвота наряду с ослаблением голоса, кроме этих симп-томов беспокоит сильная боль преимущественно в височ-ной или затылочной области» [1]. Гиппократ в Афоризмах об Апоплексии, вероятно, описал один из случаев: «Когда у людей на фоне хорошего самочувствия внезапно появ-ляются головные боли, при которых они сразу падают навзничь, лишившись речи, и начинают дышать с хрипом, они умирают в течение семи дней». Если не принимать во внимание пациента, который быстро погибает в течение этих 7 дней, не предоставив возможности собрать анамнез заболевания, может ли это быть описанием «вазоспазма», или, согласно современной терминологии, отсроченной церебральной ишемии (ОЦИ)?
В древние времена аневризмы уже были хорошо извес-тны, но аневризмы, расположенные интракраниально, невозможно было обнаружить в силу их локализации в черепе, в отличие от крупных и легко пальпируемых аневризм, доступных для клинического или патологоана-томического исследования. C.A. McDonald и M. Korb [2] считали, что Biumi в 1778 г. впервые описал подтвержден-ный патологоанатомическим исследованием случай раз-рыва аневризмы внутричерепного сосуда. Weir писал, что Gull, возможно, был первым, кто описал ОЦИ у 30-летней женщины в 1859 г.: «во время прогулки, она вдруг вскрик-нула: «О, моя голова», – и подняла вверх левую руку. Ее вырвало, и ее друг подумал, что она упала в обмо-рок. Через некоторое время она частично пришла в себя и смогла вернуться в свой дом при поддержке двух муж-чин. При поступлении в больницу в полдень на следу-ющий день, при любой попытке разбудить ее удавалось добиться лишь незначительных результатов. Правая рука была достаточно парализована, мышцы вялые; правая нога в том же состоянии...» [3].
В дальнейшем в тексте описывается улучшение ее состо-яния таким образом, что на 4-й день она могла говорить и есть. Тем не менее на 5-й день развилось ухудшение, и женщина скончалась. При вскрытии было обнаружено САК в области левой латеральной борозды головного
мозга. Выявили размягчение левого полушария, кровоиз-лияние в желудочки и 2 аневризмы средней мозговой арте-рии, одна из которых разорвалась (см. рисунок) [3–22].
J. Hunter [4] был одним из первых, кто заявил: «Существуют 3 состояния, в которых может находить-ся артерия, а именно, во-первых, состояние естествен-ной проницаемости, во-вторых, состояние растяжения и, в-третьих, состояние ... сокращения. Состояние сокраще-ния артерии возникает из-за действия мышечной силы...». Бóльшая часть их знаний была основана на данных наблюдения за повреждением головного мозга в резуль-тате сужения артерий, и эти выводы привели к развитию теории, что церебральный ангиографический вазоспазм был обусловлен действием механических факторов, эта теория существовала даже в 1980-е гг. Появились резуль-таты наблюдений об иннервации системных артерий, и в ранних работах основное внимание уделяли важному влиянию этих нервов на развитие вазоспазма. В 1728 г. Lancisi написал свои размышления о том, что причиной развития вазоспазма являются аневризмы периферических артерий за счет увеличения давления проксимальнее зоны спазма. Хотя мне не удалось найти основу для этих выводов, J. Luys [23] написал, что для сохранения сознания необходимо достаточное кровоснабжение головного мозга, но в свою очередь головной мозг регулирует свое кровоснабжение таким образом, что нейронная активность ассоциирована с увеличением кровотока. В 1911 г. D. Cow [24] написал, что химические вещества, такие как двуокись углерода и амилнитрит, известные в течение многих лет, вероятно с середины 19-го века, снижают артериальное давление путем расширения артерий, а другие вещества суживают артерии [5]. Термин «церебральный вазоспазм» исполь-зовали для объяснения транзиторных ишемических атак и других транзиторных неврологических явлений.
H. Florey не был первым, кто изучал вазомоторные реак-ции головного мозга, но в 1925 г. он описал свои наблю-дения [6] о сужении церебральных артерий кошки in vivo в ответ на электрическую, механическую и химическую стимуляцию — хлорид бария был мощным вазоконс-триктором, а нитриты были вазодилататорами, и позднее результаты его наблюдений станут важной основой для ранних экспериментальных моделей ангиографического вазоспазма.
Благодаря тому, что Quinke в 1891 г. изобрел люмбаль-ную пункцию, появилась возможность диагностировать САК прижизненно. Примерно в то же время C.P. Symonds [25] рассматривал тезис G. Froin [26] как важное предо-ставление раннего описания изменений спинномозговой
© American Heart Association, Inc., 2016 Адрес для корреспонденции: R. Loch Macdonald, MD, PhD, Division of Neurosurgery, St. Michael’s Hospital, Labatt Family Centre of Excellence in Brain Injury and Trauma Research, Keenan Research Centre for Biomedical Science, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Ontario, Canada. E-mail: [email protected]
ООО "Б
ИОНИКА
МЕДИА
"
75
1(41)’2016
жидкости после САК, и это описание правомерно по сей день. Цвет цереброспинальной жидкости изменяется с ярко-красного на вишнево-красный через ≈5 дней после САК, число эритроцитов уменьшается с третьего дня, а надосадочная жидкость становится более желтой с пер-вого дня после САК. Клиническое течение САК без лече-ния, результаты исследования спинномозговой жидкости, этиология и ключевые прогностические факторы были поразительно хорошо описаны и известны даже в то время, а основными недостатками было отсутствие методов при-жизненной визуализации и ограниченное понимание молекулярных и биохимических основ наблюдаемых изменений.
Вазоспазм нельзя было наблюдать до появления возмож-ности визуализации кровеносных сосудов. J.L. Antunes [7] сообщил, что E. Haschek и O.T. Lindenthal [27] были одни-ми из первых, кто визуализировал кровеносные сосуды на рентгенограмме путем введения контрастного вещества в сосуды трупов в 1895 г., а J. Berberich и S. Hirsch [28] получили ангиограммы конечностей в 1923 г. Тем не менее развитие церебральной ангиографии приписывают Moniz. E.G. Robertson [8], вполне вероятно, одним из первых при-знал наличие связи между инфарктами головного мозга и разорвавшимися аневризмами. В 5 случаях при патолого-анатомическом изучении инфаркты указывали на наличие ОЦИ или различные типы инфарктов, или кортикальные повреждения под толстым субарахноидальным сгустком
крови. Он предположил, что инфаркты были вызваны кратковременным спазмом артерий, потому что в артери-ях не было тромбов или эмболов. В последующем патоло-гоанатомическом исследовании S.H. Birse и M.I. Tom [29] выявили очаговый, диффузный, островковый кортикаль-ный некроз, который в некоторых случаях в настоящее время можно обнаружить методами нейровизуализации. В 1964 г. M.R. Crompton [30] обнаружил связь между наличием очагов церебральных инфарктов на аутопсии, локализацией крови в субарахноидальном пространстве и ангиографическим вазоспазмом.
Появилось несколько одновременных описаний ангио-графического вазоспазма [9, 10, 31]. M.A. Falconer [31] думал, что это явление развивается в результате введе-ния контрастного вещества и, кажется, не был убежден в существовании этого феномена. Наиболее хорошо известно первоначальное описание, сделанное A. Ecker и P.A. Riemenschneider [9], которые изучили 6 случаев обратимого интрадурального сужения артерий у пациентов с нелеченными разорвавшимимся аневризмами. Ранним указанием на динамику процесса было наблюдение, что спазм был заметен только на ангиограммах, выполненных в течение 23 дней после развития САК. Они писали, что сужение артерий происходит из-за гладких мышц или эластичной ткани стенки артерий. Уже было известно, что механическое раздражение внемозговых и церебральных артерий, например после огнестрельных ран или других
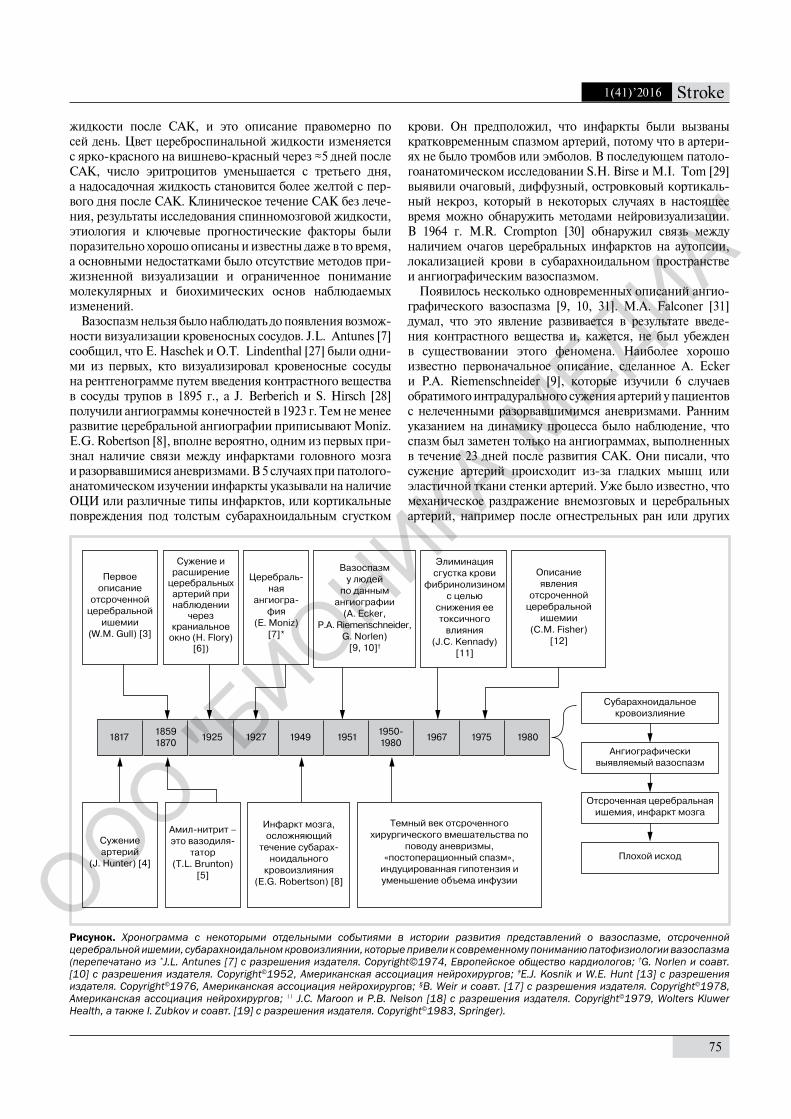
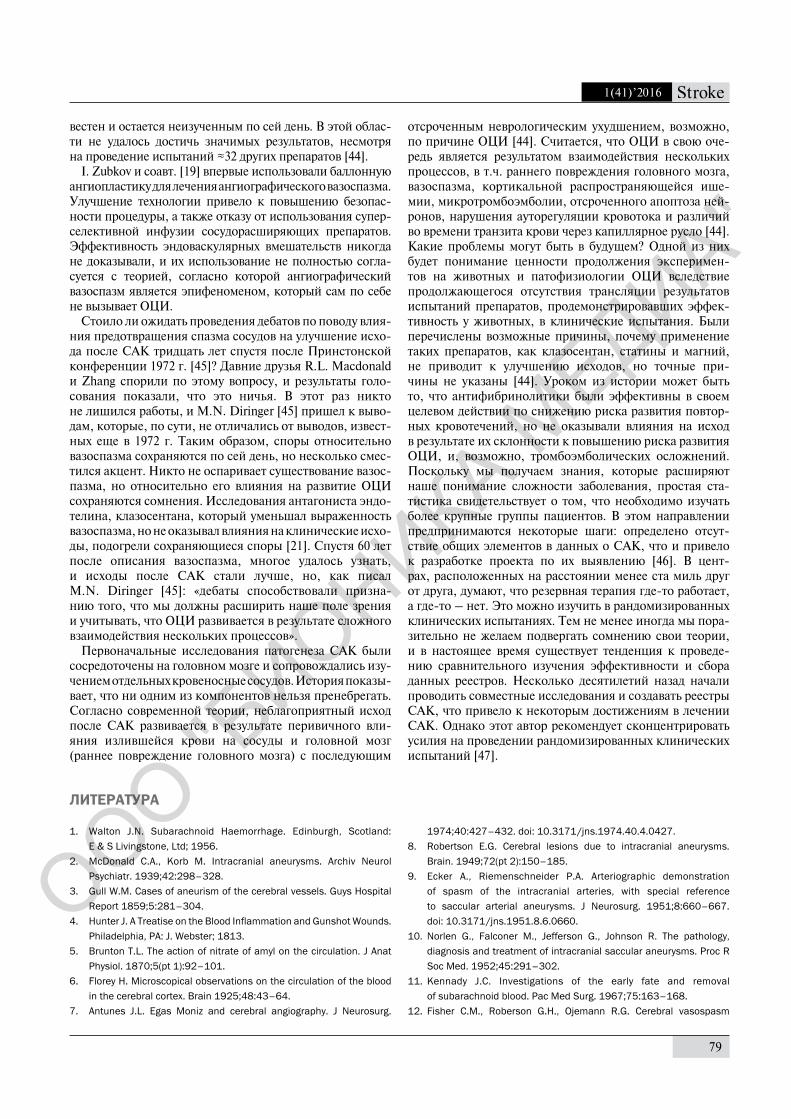
Рисунок. Хронограмма с некоторыми отдельными событиями в истории развития представлений о вазоспазме, отсроченной церебральной ишемии, субарахноидальном кровоизлиянии, которые привели к современному пониманию патофизиологии вазоспазма (перепечатано из *J.L. Antunes [7] с разрешения издателя. Copyright©1974, Европейское общество кардиологов; †G. Norlen и соавт. [10] с разрешения издателя. Copyright©1952, Американская ассоциация нейрохирургов; ‡E.J. Kosnik и W.E. Hunt [13] с разрешения издателя. Copyright©1976, Американская ассоциация нейрохирургов; §B. Weir и соавт. [17] с разрешения издателя. Copyright©1978, Американская ассоциация нейрохирургов; || J.C. Maroon и P.B. Nelson [18] с разрешения издателя. Copyright©1979, Wolters Kluwer Health, а также I. Zubkov и соавт. [19] с разрешения издателя. Copyright©1983, Springer).
1817 18591870 1925 1927 1949 1951 1950-
1980 1967 1975 1980
Первое описание
отсроченной церебральной
ишемии(W.M. Gull) [3]
Сужение артерий
(J. Hunter) [4]
Амил-нитрит – это вазодиля-
татор(T.L. Brunton)
[5]
Инфаркт мозга, осложняющий
течение субарах-ноидального
кровоизлияния(E.G. Robertson) [8]
Темный век отсроченного хирургического вмешательства по
поводу аневризмы,«постоперационный спазм»,
индуцированная гипотензия и уменьшение объема инфузии
Субарахноидальное кровоизлияние
Ангиографически выявляемый вазоспазм
Отсроченная церебральная ишемия, инфаркт мозга
Плохой исход
Церебраль-ная
ангиогра-фия
(E. Moniz) [7]*
Вазоспазм у людей
по даннымангиографии
(A. Ecker,P.A. Riemenschneider,
G. Norlen)[9, 10]†
Элиминация сгустка крови
фибринолизином с целью
снижения ее токсичного
влияния(J.C. Kennady)
[11]
Описание явления
отсроченной церебральной
ишемии(C.M. Fisher)
[12]
Сужение и расширение
церебральных артерий при наблюдении
через краниальное
окно (H. Flory) [6])
ООО "Б
ИОНИКА
МЕДИА
"

76
1(41)’2016 НЕМНОГО ИСТОРИИ
1976
1977
-19
8019
7919
8319
8819
90-
2000
2008
2010
2012
2014
Кров
ь в
суба
рахн
оида
ль-
ном
про
стра
н-ст
ве н
а КТ
ас
соци
иров
ана
с ра
звит
ием
ан
гиог
раф
иче-
ског
о ва
зосп
азм
а(K
. Kat
ada,
T. T
akem
ae,
C.M
. Fis
her)
[1
4–16
]
Гем
один
ами-
ческ
ая
тера
пия
(E.J
. Kos
nik,
W
.E. H
unt)
‡ [1
3]
Вре
мен
нáя
дина
мик
а ра
звит
ия
вазо
спаз
ма
у лю
дей
(B. W
eir)
§
[17]
Опи
сани
е м
етод
ики
балл
онно
й ан
гиоп
ласт
и-ки
(I. Z
ubko
v)¶
[19]
Клаз
озен
тан
умен
ьшае
т вы
раж
енно
сть
анги
огра
фич
ески
вы
явля
емог
о ва
зосп
азм
абе
з вл
ияни
яна
кли
ниче
ский
ис
ход
(R.L
. Mac
dona
ld)
[21]
Мул
ьтид
исци
плин
арны
й ко
нсен
сус
по т
ерм
инол
о-ги
и дл
я оп
исан
ия
анги
огра
фич
ески
вы
явля
емог
о ва
зосп
азм
а и
отср
очен
ной
цере
брал
ь-но
й иш
емии
(M.D
. Ver
gouw
en) [
22]
Умен
ьшен
ие
объе
ма
инф
узии
у па
циен
тов
с С
АК(J
.C. M
aroo
n,
P.B
. Nel
son)
II
[18]
Ним
одип
ин
одоб
рен
к пр
имен
ению
в С
ША
>16
неза
виси
мы
х ра
ндом
изир
ован
ных
испы
тани
й те
рапи
и,
напр
авле
нной
на у
мен
ьшен
ие
выра
жен
ност
и ва
зосп
азм
аи
улуч
шен
ия и
сход
ов
посл
е С
АК [2
0]
При
нтст
онск
ие
деба
ты –
улу
чшае
т ли
про
фил
акти
ка
вазо
спаз
ма
исхо
д С
АК?
Суб
арах
ноид
альн
ое к
рово
изли
яние
Оте
к м
озга
Вос
пале
ние
Апоп
тоз
Разр
ушен
ие
гем
атоэ
нцеф
а-ли
ческ
ого
барь
ера
Расп
рост
ране
ние
зоны
иш
емич
еско
го
повр
ежде
ния
коры
Мик
роци
ркул
яция
(дис
ауто
регу
ляци
я,
гете
роге
ннос
ть
врем
ени
тран
зита
кр
ови
по
капи
лляр
ам)
Анги
огра
фич
ески
вы
явля
емы
й ва
зосп
азм
Отс
роче
нная
це
ребр
альн
ая
ишем
ия, и
нфар
кт
моз
гаМ
икро
эмбо
лия
Пло
хой
исхо
д
Глоб
альн
ая
ишем
ияО
стра
яги
перт
ензи
яКр
овь
в су
бара
хнои
даль
ном
пр
остр
анст
веПродолжение рисунка
ООО "Б
ИОНИКА
МЕДИА
"

77
1(41)’2016
травматических повреждений, приводило к их сужению. Также было известно о наличии иннервации артерий, в связи с чем ведущие авторы предположили, что ангио-графический вазоспазм обусловлен механическим воз-действием САК или, возможно, активацией периваскуляр-ных нервов. Они предположили, что у пациентов, у кото-рых не развивается вазоспазм, кровотечение из аневризмы продолжается, и они умирают, таким образом, вазоспазм является жизнеспасающим феноменом. Тем не менее они также предложили, что этот феномен является вредным, поскольку ограничивает приток крови к мозгу. A. Ecker [32] представил ангиографические данные обнаружения вазоспазма на конференции в Кушинге в 1951 г. Позже он написал, что старшие члены организации качали головами в недоумении во время его выступления. Был 1 человек, который улыбался, как будто понимал, о чем идет речь. A. Ecker позже писал: «При ответе на реплики я обращался к нему. Во время обсуждения, после того, как некоторые пожилые мужчины отрицали существование церебрально-го вазоспазма...я подошел к этому неизвестному улыбаю-щемуся человеку, чтобы поблагодарить его за поддержку. Он ответил, улыбаясь, «Я не говорю по-английски» [9, 32].
J.L. Pool [33] описал типичную клиническую картину ОЦИ в 1958 г. Лечение ее заключалось в локальном вве-дении или внутриартериальной инъекции папаверина или прокаина во время проведения хирургического вмеша-тельства. Эти методы лечения внедрили в клиническую практику после экспериментов на животных, которые показали, что эти препараты способствуют разрешению острого механически-индуцированного спазма цереб-ральных артерий. Поскольку было известно о непосредст-венном воздействии папаверина на гладкие мышцы и про-каина на нервы, этот эффект расценили как свидетельство того, что ангиографический вазоспазм был обусловлен нейронными механизмами и сокращением гладких мышц [33]. Рассматривали возможность того, что в крови цирку-лирует некая субстанция, но считали это недостаточным объяснением, потому что иногда наблюдали вазоспазм при трепанации черепа после разрешения САК.
С конца 1950-х до 1980-х гг. сохранялись споры относи-тельно САК, в т.ч. о сроках оперативного лечения. Было хорошо известно, что повторное кровоизлияние является причиной смерти, но особенно опасным было проведение раннего вмешательства. Часто считали, что операцию по поводу аневризм внутричерепных сосудов лучше всего проводить в период с 7-го по 10-й день после развития САК, хотя сейчас известно, что это самые опасные сроки с наиболее высоким риском развития ОЦИ [1]. Поскольку тогда было неизвестно, что ангиографический вазоспазм не развивается до 3-го или 4-го дня после САК, появление вазоспазма после операции по поводу аневризмы ошибоч-но интерпретировали как послеоперационный спазм по причине вмешательства. В любом случае, к концу 1950-х гг. стало очевидно, что ангиографический вазоспазм может быть связан с очаговым неврологическим дефицитом и прогрессировать до развития комы и летального исхо-да, и что в ранее проведенных работах, как правило, не дифференцировали ОЦИ и повторные кровоизлияния. J.N. Walton [1] написал: «гемипарез и другие неврологичес-кие симптомы со стороны конечностей полностью разре-
шились у 14 пациентов во время их пребывания в клинике; вероятно, в этих случаях неврологический дефицит был обусловлен транзиторной ишемией или компрессией ... ». Хирургическое лечение в случае нераспознанного ангио графического вазоспазма сочетали с использованием инду-цированной гипотензии как до операции, с целью предо-твращения повторного кровоизлияния, так и во время оперативного вмешательства для снижения риска интра-операционного разрыва аневризмы, часто при непря-мом вмешательстве путем лигирования сонной артерии, в связи с чем у пациентов, как правило, происходило уменьшение объема перфузирующей крови, что приводи-ло к предсказуемо неблагоприятным исходам.
Уже на протяжении более 20 лет было известно, что химические вещества, циркулирующие в крови, включая серотонин, вызывают сокращение церебральных артерий, но только F.A. Echlin [34] провел обширные эксперимен-ты, основываясь на результатах предыдущих исследова-ний констрикции церебральных артерий в ответ на меха-ническую и химическую стимуляцию. Он отметил раз-витие вазоконстрикции церебральных артерий у обезьян в ответ на воздействие свежей крови, что повлекло за собой поиск в крови веществ, ответственных за ангиографичес-ки идентифицируемый вазоспазм. В экспериментальных моделях вазоспазма, в которых первоначально использо-вали локальное воздействие различными препаратами или кровью на препарированные церебральные артерии, позд-нее стали использовать инъекции крови в субарахноидаль-ное пространство, индуцировали САК путем перфорации церебральных артерий или путем введения свернувшей-ся крови в субарахноидальное пространство. В много-численных исследованиях показали, что это приводило к развитию более продолжительного спазма сосудов, одна-ко причину это феномена не удавалось уточнить до тех пор, пока в исследованиях с использованием компьютерной томографии у людей не подтвердили роль стойкого САК в развитии ангиографического вазоспазма. Тем не менее J.C. Kennady [11] уже изучал методы ускоренного очище-ния субарахноидальной крови у собак. J.F. Alksne и соавт. [35] в своих исследованиях использовали плазмин при экспериментальном САК с той же целью, наряду с усили-ями по удалению САК хирургическим путем, предшествуя эре тканевого активатора плазминогена.
R.R. Smith и E.G. Robertson впервые организова-ли т.н. конференции по вазоспазму в Джексоне, штат Миссисипи в 1972 г. В них приняли участие 18 исследова-телей. R.R. Smith был известен по работам о структурных изменениях церебральных артерий в ответ на САК, роли гепарина, а также работам его последователей, например B.R. Clower и соавт. [36], чья работа о тромбоцитах и эндо-телии недавно была открыта заново [37]. J.T. Robertson и R.P. White [38] также внесли огромный вклад в разъясне-ние механизмов сокращения сосудов после развития САК. В последующих конференциях по вазоспазму приня-ли участие несколько сотен человек. Основная часть первоначальных экспериментальных исследований была сосредоточена на изучении роли иннервации церебраль-ных артерий, влияния катехоламинов и их антагонис-тов в качестве методов лечения вазоспазма, и ни одно из исследований не дало ожидаемых результатов. В том
ООО "Б
ИОНИКА
МЕДИА
"

78
1(41)’2016 НЕМНОГО ИСТОРИИ
же году состоялась Принстонская Конференция, где отношения между C.H. Millikan [39] и нейрохирургами, в т.ч. Т.М. Sundt и C. Drake, возобновились. Во-первых, C.H. Millikan [39], крупный авторитет в области сосудис-той неврологии и редактор журнала «Stroke», изучал лите-ратуру по ангиографическому вазоспазму и САК, а также обследовал пациентов, проходивших лечение в клинике Мейо в Рочестере. Он пришел к выводу, что у пациентов отсутствовали клинические проявления, соответствую-щие наличию ангиографического вазоспазма, и что спазм сосудов не оказывал влияния на смертность по причине развития САК, а также что связи между осложнениями после оперативного лечения и вазоспазмом не было. C.H. Millikan [39] подчеркнул роль тромбоза артерий в развитии ишемии после САК. Подразумевалось, что хирурги использовали вазоспазм для объяснения раз-вития хирургических осложнений в качестве причины неблагоприятных исходов. Как правило, теперь дума-ли, что только первое из трех замечаний правильно, т.е. не у всех пациентов с умеренным и тяжелым ангиогра-фическим вазоспазмом развивается ОЦИ. Это уже было известно. T.M. Sundt, такой же видный деятель в области нейрохирургии, которому, возможно, была напрямую адресована статья C.H. Millikan [39] (D. Piepgras, личное общение, 28 октября 2014 г.), написал, что корреляция между ангиографическим вазоспазмом и клиническим состоянием была неполной [40]. C.H. Millikan [39] вклю-чил в статью данные пациентов, проходивших лечение в клинике Мейо, а в то время такие статьи нужно было регистрировать в клинике и в качестве авторов вклю-чать других врачей, которые проводили лечение описан-ных пациентов. Этого не было сделано. T.M. Sundt был в ярости и заявил на кафедре нейрохирургии «или он или я». Отдел кадров клиники Мейо изучил ситуацию и ввел ограничения на деятельность C.H. Millikan, [39], что привело к его отъезду в университет штата Юта. Он при-знался, что в опубликованных данных были некоторые неточности [39]. T.M. Sundt умер в 1992 г. в возрасте 62 лет от рака, и он считал что эта болезнь, возможно, развилась у него по причине повышенного облучения при прове-дении исследований церебрального кровотока у своих больных. C.H. Millikan [39] пережил его и умер в 2011 г.
В то же время, C.M. Fisher [12] предоставил окончатель-ное описание ОЦИ, впервые опубликовал его в краткой форме и был одним из первых, кто использовал термин «отсроченный ишемический неврологический дефицит». Он отметил, что этот дефицит развивался с 3-й по 13-й день после САК, был обратимым в 50% случаев, и что для развития ОЦИ ангиографический вазоспазм должен быть очень выраженным. Он предположил наличие причин-но-следственной связи на основе ассоциаций. Японские исследователи опубликовали практически идентичные данные [41]. Они подчеркнули потенциальную роль тромба в субарахноидальном пространстве в сохранении ангио-графического вазоспазма, выявили ключевую роль эри-троцитов в патогенезе вазоспазма и для удаления тромба использовали дренирование цистерн головного мозга. Лечение включало массивное внутривенное введение кок-тейлей вазодилататоров, в т.ч. изопротеренола, фентола-мина, нитропруссида натрия, резерпина и аминофиллина
с вазоконстрикторами для поддержания уровня артери-ального давления.
B. Weir и соавт. [17] уточнили динамику вазоспазма у людей путем измерения диаметров церебральных арте-рий на 627 ангиограммах у 293 пациентов с аневризмами. Вазоспазм развивался на 3–12-й день после САК, и был максимальным на 7–8-й день. В течение 4 лет после изобретения компьютерной томографии японские нейро-хирурги показали, что ангиографический вазоспазм был ассоциирован с объемом и локализацией крови в субарах-ноидальном пространстве [14, 15]. Эти данные были фор-мализованы C.M. Fisher и соавт. [16] в одной из наиболее цитируемых статей о САК.
Конец 1970-х гг. ознаменовался двумя достижения-ми в области медицины. E.J. Kosnik и W.E. Hunt [13] знали, что Denny–Brown сообщили о влиянии повыше-ния артериального давления на улучшение ишемического неврологического дефицита. В 1976 г. они отметили улуч-шение неврологического дефицита у пациентов с САК и аневризмами, пролеченными хирургическим путем, при проведении внутривенных инфузий и индуцированной гипертензии. В то время, когда у пациентов развива-лась гипонатриемия, им ограничивали водную нагрузку. Они отметили, что у этих пациентов часто развивалась гиповолемия. В 1979 г. J.C. Maroon и P.B. Nelson [18] впервые документально подтвердили развитие этого феномена. Маятник качнулся от индуцированной гипо-тензии и ограничения жидкости в сторону индуцирован-ной гипертензии и водной нагрузки, и последний метод лечения продолжают использовать в различной степени в отсутствие каких-либо доказательств 1-го уровня.
A. Fleckenstein [42], немецкий фармаколог, являет-ся первооткрывателем блокаторов кальциевых каналов. Он подробно изложил, что в 1963 г. немецкие фармацевти-ческие компании снабдили его новыми синтезированными препаратами, которые имели свойства коронарных вазо-дилататоров. Он обнаружил, что в сердечной мышце они имитировали эффект прекращения поступления кальция. Ключевым событием был случай, который произошел в 1969 г., когда компания Bayer предоставила ему первое соединение дигидропиридина, нифедипин, который, как оказалось, также обладал сосудорасширяющими свойст-вами. Еще один препарат дигидропиридина, нимодипин, был разработан специально в качестве церебрального вазодилататора с минимальным влиянием на системное артериальное давление для эффективного использования в лечении патологии церебральных сосудов [43]. После мно-гократных доклинических испытаний, включая большое количество испытаний, свидетельствующих об отсутст - вии влияния нимодипина на ангиографический вазоспазм, а также клинических испытаний с участием людей, этот препарат в конечном итоге был одобрен Управлением по контролю за продуктами питания и лекарственными средствами США лишь в декабре 1988 г., несмотря на его использование в Европе с 1985 г. Управление по контролю за продуктами питания и лекарственными средствами США пришло к выводу, что нимодипин уменьшает вли-яние вазоспазма на развитие церебральных инфарктов и неблагоприятных исходов, но не влияет на ангиогра-фический вазоспазм. Механизм этого действия был неиз-
ООО "Б
ИОНИКА
МЕДИА
"
79
1(41)’2016
вестен и остается неизученным по сей день. В этой облас-ти не удалось достичь значимых результатов, несмотря на проведение испытаний ≈32 других препаратов [44].
I. Zubkov и соавт. [19] впервые использовали баллонную ангиопластику для лечения ангиографического вазоспазма. Улучшение технологии привело к повышению безопас-ности процедуры, а также отказу от использования супер-селективной инфузии сосудорасширяющих препаратов. Эффективность эндоваскулярных вмешательств никогда не доказывали, и их использование не полностью согла-суется с теорией, согласно которой ангиографический вазоспазм является эпифеноменом, который сам по себе не вызывает ОЦИ.
Стоило ли ожидать проведения дебатов по поводу влия-ния предотвращения спазма сосудов на улучшение исхо-да после САК тридцать лет спустя после Принстонской конференции 1972 г. [45]? Давние друзья R.L. Macdonald и Zhang спорили по этому вопросу, и результаты голо-сования показали, что это ничья. В этот раз никто не лишился работы, и M.N. Diringer [45] пришел к выво-дам, которые, по сути, не отличались от выводов, извест-ных еще в 1972 г. Таким образом, споры относительно вазоспазма сохраняются по сей день, но несколько смес-тился акцент. Никто не оспаривает существование вазос-пазма, но относительно его влияния на развитие ОЦИ сохраняются сомнения. Исследования антагониста эндо-телина, клазосентана, который уменьшал выраженность вазоспазма, но не оказывал влияния на клинические исхо-ды, подогрели сохраняющиеся споры [21]. Спустя 60 лет после описания вазоспазма, многое удалось узнать, и исходы после САК стали лучше, но, как писал M.N. Diringer [45]: «дебаты способствовали призна-нию того, что мы должны расширить наше поле зрения и учитывать, что ОЦИ развивается в результате сложного взаимодействия нескольких процессов».
Первоначальные исследования патогенеза САК были сосредоточены на головном мозге и сопровождались изу-чением отдельных кровеносные сосудов. История показы-вает, что ни одним из компонентов нельзя пренебрегать. Согласно современной теории, неблагоприятный исход после САК развивается в результате перивичного вли-яния излившейся крови на сосуды и головной мозг (раннее повреждение головного мозга) с последующим
отсроченным неврологическим ухудшением, возможно, по причине ОЦИ [44]. Считается, что ОЦИ в свою оче-редь является результатом взаимодействия нескольких процессов, в т.ч. раннего повреждения головного мозга, вазоспазма, кортикальной распространяющейся ише-мии, микротромбоэмболии, отсроченного апоптоза ней-ронов, нарушения ауторегуляции кровотока и различий во времени транзита крови через капиллярное русло [44]. Какие проблемы могут быть в будущем? Одной из них будет понимание ценности продолжения эксперимен-тов на животных и патофизиологии ОЦИ вследствие продолжающегося отсутствия трансляции результатов испытаний препаратов, продемонстрировавших эффек-тивность у животных, в клинические испытания. Были перечислены возможные причины, почему применение таких препаратов, как клазосентан, статины и магний, не приводит к улучшению исходов, но точные при-чины не указаны [44]. Уроком из истории может быть то, что антифибринолитики были эффективны в своем целевом действии по снижению риска развития повтор-ных кровотечений, но не оказывали влияния на исход в результате их склонности к повышению риска развития ОЦИ, и, возможно, тромбоэмболических осложнений. Поскольку мы получаем знания, которые расширяют наше понимание сложности заболевания, простая ста-тистика свидетельствует о том, что необходимо изучать более крупные группы пациентов. В этом направлении предпринимаются некоторые шаги: определено отсут-ствие общих элементов в данных о САК, что и привело к разработке проекта по их выявлению [46]. В цент-рах, расположенных на расстоянии менее ста миль друг от друга, думают, что резервная терапия где-то работает, а где-то – нет. Это можно изучить в рандомизированных клинических испытаниях. Тем не менее иногда мы пора-зительно не желаем подвергать сомнению свои теории, и в настоящее время существует тенденция к проведе-нию сравнительного изучения эффективности и сбора данных реестров. Несколько десятилетий назад начали проводить совместные исследования и создавать реестры САК, что привело к некоторым достижениям в лечении САК. Однако этот автор рекомендует сконцентрировать усилия на проведении рандомизированных клинических испытаний [47].
ЛИТЕРАТУРА
1. Walton J.N. Subarachnoid Haemorrhage. Edinburgh, Scotland:
E & S Livingstone, Ltd; 1956.
2. McDonald C.A., Korb M. Intracranial aneurysms. Archiv Neurol
Psychiatr. 1939;42:298–328.
3. Gull W.M. Cases of aneurism of the cerebral vessels. Guys Hospital
Report 1859;5:281–304.
4. Hunter J. A Treatise on the Blood Inflammation and Gunshot Wounds.
Philadelphia, PA: J. Webster; 1813.
5. Brunton T.L. The action of nitrate of amyl on the circulation. J Anat
Physiol. 1870;5(pt 1):92–101.
6. Florey H. Microscopical observations on the circulation of the blood
in the cerebral cortex. Brain 1925;48:43–64.
7. Antunes J.L. Egas Moniz and cerebral angiography. J Neurosurg.
1974;40:427–432. doi: 10.3171/jns.1974.40.4.0427.
8. Robertson E.G. Cerebral lesions due to intracranial aneurysms.
Brain. 1949;72(pt 2):150–185.
9. Ecker A., Riemenschneider P.A. Arteriographic demonstration
of spasm of the intracranial arteries, with special reference
to saccular arterial aneurysms. J Neurosurg. 1951;8:660–667.
doi: 10.3171/jns.1951.8.6.0660.
10. Norlen G., Falconer M., Jefferson G., Johnson R. The pathology,
diagnosis and treatment of intracranial saccular aneurysms. Proc R
Soc Med. 1952;45:291–302.
11. Kennady J.C. Investigations of the early fate and removal
of subarachnoid blood. Pac Med Surg. 1967;75:163–168.
12. Fisher C.M., Roberson G.H., Ojemann R.G. Cerebral vasospasm
ООО "Б
ИОНИКА
МЕДИА
"

80
1(41)’2016 НЕМНОГО ИСТОРИИ
with ruptured saccular aneurysm–the clinical manifestations.
Neurosurgery. 1977;1:245–248.
13. Kosnik E.J., Hunt W.E. Postoperative hypertension in the management
of patients with intracranial arterial aneurysms. J Neurosurg.
1976;45:148–154. doi: 10.3171/jns.1976.45.2.0148.
14. Katada K., Kanno T., Sano H., Shibata T., Shah M.Y. Computed
tomography of ruptured intracranial aneurysm in acute stage
(author’s transl). No Shinkei Geka. 1977;5:955–963.
15. Takemae T., Mizukami M., Kin H., Kawase T., Araki G. Computed
tomography of ruptured intracranial aneurysms in acute stage–
relationship between vasospasm and high density on CT scan
(author’s transl). No To Shinkei. 1978;30:861–866.
16. Fisher C.M., Kistler J.P., Davis J.M. Relation of cerebral vasospasm
to subarachnoid hemorrhage visualized by computerized tomographic
scanning. Neurosurgery. 1980;6:1–9.
17. Weir B., Grace M., Hansen J., Rothberg C. Time course
of vasospasm in man. J Neurosurg. 1978;48:173–178.
doi: 10.3171/jns.1978.48.2.0173.
18. Maroon J.C., Nelson P.B. Hypovolemia in patients with subarachnoid
hemorrhage: therapeutic implications. Neurosurgery. 1979;4:223–
226.
19. Zubkov I., Nikiforov B.M., Shustin V.A. 1st attempt at dilating spastic
cerebral arteries in the acute stage of rupture of arterial aneurysms.
(Russian). Zhurnal Voprosy Neirokhirurgii Imeni N - N - Burdenko
1983;17–23.
20. Etminan N., Vergouwen M.D., Ilodigwe D., Macdonald R.L. Effect of
pharmaceutical treatment on vasospasm, delayed cerebral ischemia,
and clinical outcome in patients with aneurysmal subarachnoid
hemorrhage: a systematic review and meta-analysis. J Cereb Blood
Flow Metab. 2011;31:1443–1451. doi: 10.1038/jcbfm.2011.7.
21. Macdonald R.L., Kassell N.F., Mayer S., Ruefenacht D., Schmiedek P.,
Weidauer S., et al; CONSCIOUS-1 Investigators. Clazosentan
to overcome neurological ischemia and infarction occurring after
subarachnoid hemorrhage (CONSCIOUS-1): randomized, double-
blind, placebocontrolled phase 2 dose-finding trial. Stroke.
2008;39:3015–3021. doi:10.1161/STROKEAHA.108.519942.
22. Vergouwen M.D., Vermeulen M., van Gijn J., Rinkel G.J.,
Wijdicks E.F., Muizelaar J.P., et al. Definition of delayed cerebral
ischemia after aneurysmal subarachnoid hemorrhage as an
outcome event in clinical trials and observational studies: proposal
of a multidisciplinary research group. Stroke. 2010;41:2391–2395.
doi: 10.1161/STROKEAHA.110.589275.
23. Luys J. Le Cerveau et ses Fonctions. Paris, France: Germer-Baillier
& Cie; 1879.
24. Cow D. Some reactions of surviving arteries. J Physiol. 1911;42:
125–143.
25. Symonds C.P. Spontaneous sub-arachnoid hжmorrhage. Proc R Soc
Med. 1924;17(Neurol Sect):39–52.
26. Froin G. Les hemorrhagies sous arachnoidiennes et le mechanism
del’hematolyse en general These de Paris, No. 113, Paris, France;
1904.
27. Haschek E., Lindenthal O.T. Ein beitrag zur praktischen verwerthung
der photographie nach rontgen. Wien Klin Wschr 1896;9:63–64.
28. Berberich J., Hirsch S. Die rontgenographische darstellung der
arterien und venun am lebenden menschen. Klin Wschr
1923;2:2226–2228.
29. Birse S.H., Tom M.I. Incidence of cerebral infarction associated
with ruptured intracranial aneurysms. A study of 8 unoperated
cases of anterior cerebral aneurysm. Neurology. 1960;10:
101–106.
30. Crompton M.R. The pathogenesis of cerebral infarction following
the rupture of cerebral berry aneurysms. Brain. 1964;87:491–510.
31. Falconer M.A. The surgical treatment of bleeding intracranial
aneurysms. J Neurol Neurosurg Psychiatry. 1951;14:153–186.
32. Ecker A. The discovery of human cerebral arterial spasm
in angiograms: an autobiographical note (Arthur Ecker). Neurosurgery.
1982;10:90.
33. Pool J.L. Cerebral vasospasm. N Engl J Med. 1958;259:1259–1264.
doi:10.1056/NEJM195812252592605.
34. Echlin F.A. Spasm of basilar and vertebral arteries caused
by experimental subarachnoid hemorrhage. J Neurosurg.
1965;23:1–11. doi: 10.3171/jns.1965.23.1.0001.
35. Alksne J.F., Branson P.J., Bailey M. Modification of experimental
postsubarachnoid hemorrhage vasculopathy with intracisternal
plasmin. Neurosurgery. 1986;19:20–25.
36. Clower B.R., Yoshioka J., Honma Y., Smith R.R. Pathological
changes in cerebral arteries following experimental subarachnoid
hemorrhage: role of blood platelets. Anat Rec. 1988;220:161–170.
doi: 10.1002/ar.1092200207.
37. Kapp J.P., Neill W.R., Neill C.L., Hodges L.R., Smith R.R. The three
phases of vasospasm. Surg Neurol. 1982;18:40–45.
38. White R.P., Hagen A.A., Robertson J.T. Effect of nonsteroid anti-
inflammatory drugs on subarachnoid hemorrhage in dogs.
J Neurosurg. 1979;51:164–171. doi: 10.3171/jns.1979.51.2.0164.
39. Millikan C.H. Cerebral vasospasm and ruptured intracranial
aneurysm. Arch Neurol. 1975;32:433–449.
40. Sundt T.M. Jr. Intracranial aneurysms and subarachnoid hemorrhage:
a subject review for the clinician. Mayo Clin Proc. 1970;45:
455–466.
41. Saito I., Ueda Y., Sano K. Significance of vasospasm in the treatment
of ruptured intracranial aneurysms. J Neurosurg. 1977;47:412–
429. doi:10.3171/jns.1977.47.3.0412.
42. Fleckenstein A. History of calcium antagonists. Circ Res. 1983;52(2
pt. 2):I3–16.
43. Towart R., Kazda S. The cellular mechanism of action of nimodipine
(BAY e 9736), a new calcium antagonist [proceedings]. Br J
Pharmacol. 1979;67:409P–410P.
44. Macdonald R.L. Delayed neurological deterioration after
subarachnoid haemorrhage. Nat Rev Neurol. 2014;10:44–58.
doi: 10.1038/nrneurol.2013.246.45. Diringer M.N. Controversy: does prevention of vasospasm in
subarachnoid hemorrhage improve clinical outcome? Stroke. 2013;44(6
Suppl. 1):S29–S30. doi: 10.1161/STROKEAHA.111.000008.
46. Jaja B.N., Attalla D., Macdonald R.L., Schweizer T.A., Cusimano M.D.,
Etminan N., et al. The Subarachnoid Hemorrhage International
Trialists (SAHIT) Repository: advancing clinical research
in subarachnoid hemorrhage. Neurocrit Care. 2014;21:551–559.
doi: 10.1007/s12028-014-9990-y.
47. Darsaut T.E., Raymond J. RCTs in determining treatment
indications for intracranial aneurysms: what can we learn from
history? Neurochirurgie. 2012;58:76–86. doi: 10.1016/j.
neuchi.2012.02.022.
ООО "Б
ИОНИКА
МЕДИА
"