stroke care in europe l. garcia-castrillo, md, semes department of emergency medicine university...
TRANSCRIPT
Stroke Care in EuropeStroke Care in Europe
L. Garcia-Castrillo, MD, SEMES
Department of Emergency Medicine
University Hospital Marques de Valdecilla
Cantabria, Spain

L. Garcia-Castrillo
Stroke Chain of recoveryStroke Chain of recovery
Pepe PE. Ensuring the chain of recovery for stroke in your community. Acad Emerg Med 1998;5(4):352-8
EMS EMS Response & Response & TransportTransport
AlertAlert
EDED
DiagnosisDiagnosis&&
TreatmentTreatmentIdentificatioIdentificationn
DispatchDispatch

L. Garcia-Castrillo
Teaching Points to be AddressedTeaching Points to be Addressed
• Stroke care in Europe
• The role of Emergency Medicine in Stroke care

SettingSetting
L. Garcia-Castrillo

L. Garcia-Castrillo
EuropaEuropa
• 45 Languages
• 43 Countries
• 727. Mill. 400 Mill. in EU
• 15% >65 years
L. Garcia-Castrillo
Stroke in EuropeStroke in Europe
• 3rd Cause of death
• 1 million of new cases, with 400.000 casualties per year
• First cause of disability
• Accounts 3-5% of total health cost
• Great differences in cost and results

L. Garcia-Castrillo
Cerebrovascular Disease: FemalesCerebrovascular Disease: Females
per 100,000 < 41.64
< 62.64
< 83.64
< 104.6
< 125.6
125.6
AdjustedAdjusted
Death rateDeath rate
L. Garcia-Castrillo
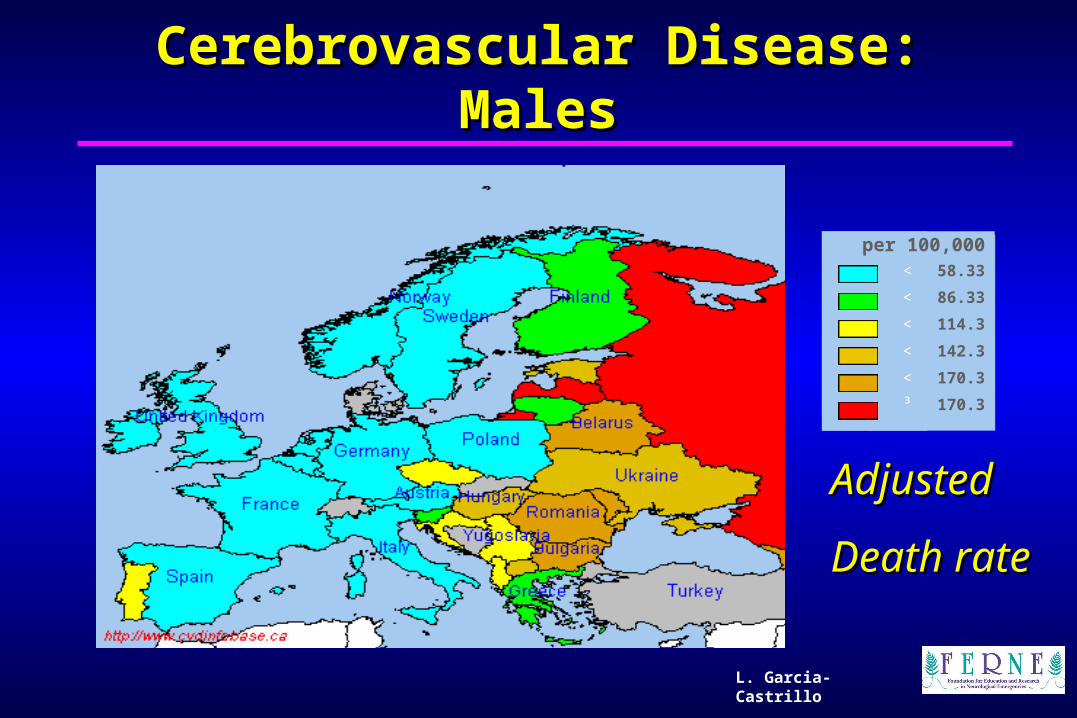
Cerebrovascular Disease: MalesCerebrovascular Disease: Males
per 100,000 < 58.33
< 86.33
< 114.3
< 142.3
< 170.3
³ 170.3
AdjustedAdjusted
Death rateDeath rate
L. Garcia-Castrillo
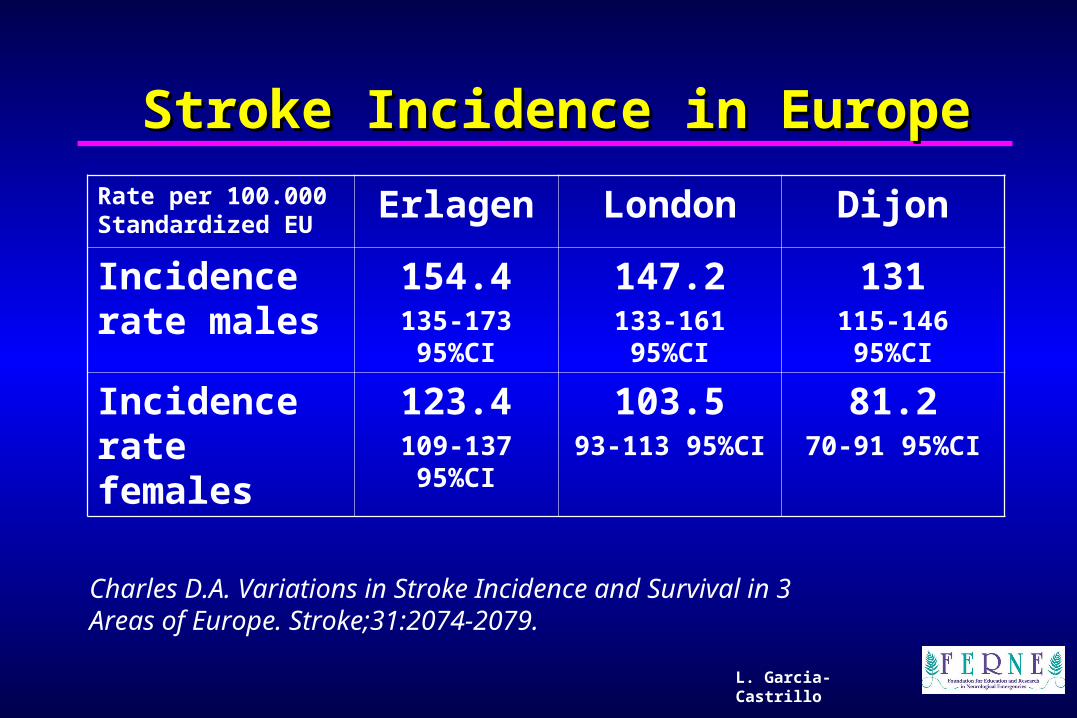
Stroke Incidence in EuropeStroke Incidence in Europe
Rate per 100.000 Standardized EU
Erlagen London Dijon
Incidence rate males
154.4135-173 95%CI
147.2133-161 95%CI
131115-146 95%CI
Incidence rate females
123.4109-137 95%CI
103.593-113 95%CI
81.270-91 95%CI
Charles D.A. Variations in Stroke Incidence and Survival in 3 Areas of Europe. Stroke;31:2074-2079.

L. Garcia-Castrillo
Relevant ContributionsRelevant Contributions
• WHO Task Force on Stroke and other Cerebrovascular Disorders, 1989;
• European Federation of Neurological Societies Task Force, 1997;
• European Ad Hoc Consensus Group, 1996;• Pan European Consensus Meeting on Stroke
Management, 1995;• EUSI European Federation of Neurological
Societies (EFNS), European Neurological Society (ENS) and European Stroke Council (ESC). 2000;
L. Garcia-Castrillo
Recommendations Recommendations Emergency AreaEmergency Area
• Education • Stroke symptoms• EMS use
• Identify Stroke as an emergency medical problem• Use protocols to identify stroke symptoms in the Dispatch
Center• Reduce delays in the prehospital phase • Transport to a Hospital with an adequate Stroke Unit
• ED • Rapid evaluation• Treat Medical Problems

ResultsResults
L. Garcia-Castrillo

Variations in OutcomesVariations in OutcomesCases Coma % CT % Barthel=20 % Mortality 3 m %
UK1 214 12 73 30 29
UK2 160 20 81 20 36
UK3 220 19 71 15 38
UK4 172 20 80 45 40
UK5 256 28 30 31 56
France 213 16 97 63 17
Portugal 6657 24 87 48 31
Hungary 160 18 64 56 22
Spain 393 16 74 34 32
Germany 1 1152 7 92 59 18
Germany 2 302 15 89 43 25
Italy 635 19 88 44 27
Chales DA Wolfe. BIOMED Study of Stroke Care Group. Stroke 1999;30:350-356. L. Garcia-Castrillo

L. Garcia-Castrillo
European Stroke Care InventoryEuropean Stroke Care Inventory
• 30 EFNS member countries collect information on acute stroke care
• 22 countries were represented
• Information represents national data
M. Brainin. Acute neurological stroke care in Europe: Results of the European Stroke Care Inventory Eu J Neurol 2000;7:5-10

L. Garcia-Castrillo
Stroke Management in Europe IStroke Management in Europe I
WE(10) 238 M EE(12) 300 M
Incidence 2-2.5/1000/y 3-5/1000/y
Stroke non in Hospital
20% 25-60%
CT acute 50-95% 5-50%
Hemorrhagic S. 15-18% 19-35%

L. Garcia-Castrillo
Stroke Management in Europe IIStroke Management in Europe II
WE(10) 238 M EE(12) 300 M
In hospital <3h 5-40% 20-49%
Stroke Units 0.37/1 mill 1.1/ 1 mill
Mortality 30 days
12-20% 25-35%

L. Garcia-Castrillo
Time to CareTime to Care
40%
18%
29%
13%
0-3 h
3-6 h
6-26 h
>24 h
L. Serrano Latency time and thrombolitic treatment of ischemic ictus. Emergencias 1998; 10:236-238
L. Garcia-Castrillo
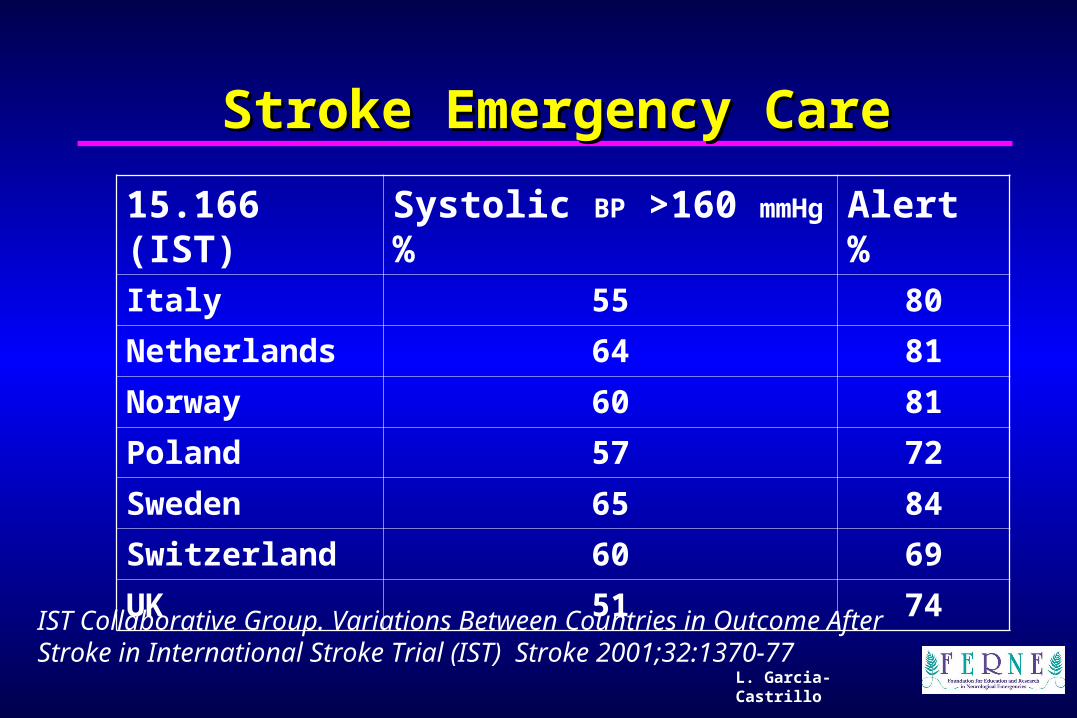
Stroke Emergency CareStroke Emergency Care
15.166 (IST) Systolic BP >160 mmHg % Alert %Italy 55 80
Netherlands 64 81
Norway 60 81
Poland 57 72
Sweden 65 84
Switzerland 60 69
UK 51 74
IST Collaborative Group. Variations Between Countries in Outcome After Stroke in International Stroke Trial (IST) Stroke 2001;32:1370-77
L. Garcia-Castrillo
Pre-hospital Stroke CarePre-hospital Stroke Care
• European European Emergency Emergency Data ProjectData Project
T.Krafft EED Group Comparing European EMS Systems GEOMED [email protected]

L. Garcia-CastrilloL. Garcia-Castrillo
L. Garcia-Castrillo
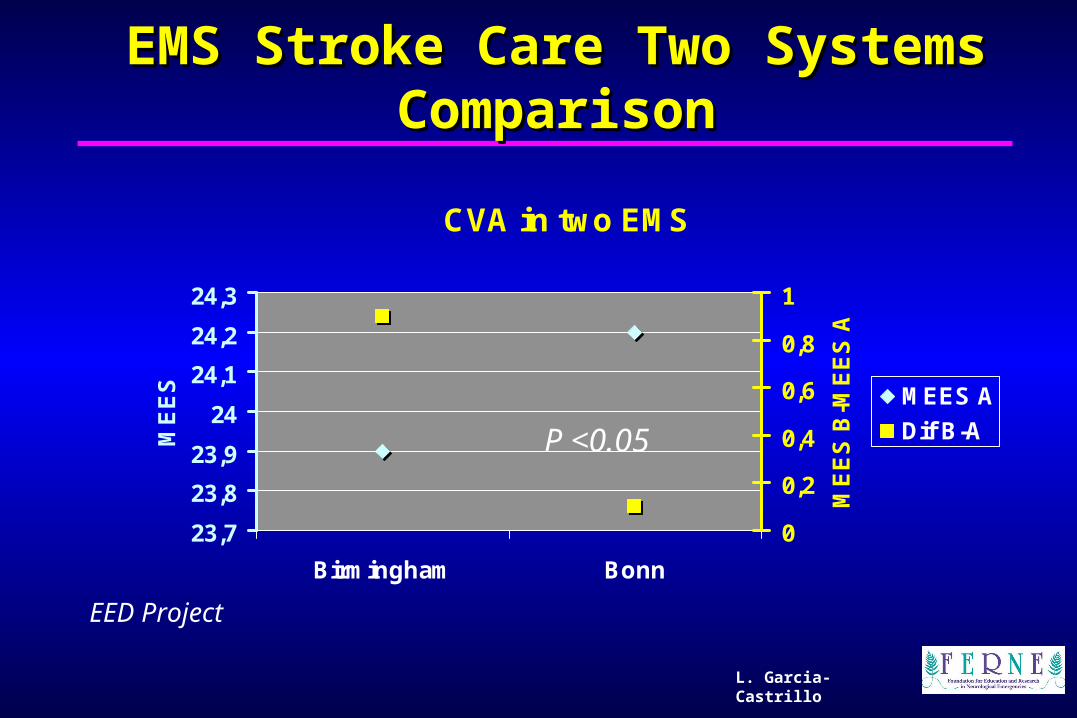
EMS Stroke Care Two SystemEMS Stroke Care Two Systemss ComparisonComparison
CVA in two EMS
23,7
23,8
23,9
24
24,1
24,2
24,3
Birmingham Bonn
ME
ES
0
0,2
0,4
0,6
0,8
1
ME
ES
B-M
EE
S A
MEES A
Dif B-AP <0.05
EED Project

L. Garcia-Castrillo
Integrated Network Stroke CareIntegrated Network Stroke Care
• Period 1998-2000• Cases 2313• Arrive with ALS unit
doctor 27%• At hospital < 3h 57%• CT < 30 min 54%• Thrombolysis 4.1%• 3 months mortality 12.9%
Steiner MM. The quality of acute stroke units on nation-wide level: the Austrian Stroke Registry for acute stroke units. Eur J Neurol 2003;4:353-60
AustrianAustrian

L. Garcia-Castrillo
Teaching Points to be AddressedTeaching Points to be Addressed
• Stroke care in Europe
• There are important geographical differences between areas; in incidence, process of care and outcomes
• Different outcomes can be explained, in part, due to the level of resources available

L. Garcia-Castrillo
Teaching Points to be AddressedTeaching Points to be Addressed
• The role of Emergency Medicine in Stroke care• EMS is a fundamental part of Stroke care
facilitating; access, high level pre-hospital care and integration with in hospital systems
• EMS-ED must be part of the concept of Integral Stroke care

L. Garcia-Castrillo
SummarySummary
• The role of Emergency Medicine in the pre-hospital and in the ED is clearly defined in guidelines and consensus documents
• More high quality research is needed to clarify the best model of care
Questions?Questions?