strengthening home visiting through research
TRANSCRIPT
Journal of ZERO TO THREE: National Center for Infants, Toddlers, and Families
January 2013 Volume 33 No. 3
Strengthening
Home Visiting
Through
Research
Measuring Program Quality
Positive Effects of Universal Access
Home Visiting to Promote School
Readiness
Exploring Family Risk Factors and
Program Outcomes
Also in This Issue:Federal Initiatives to Support Home Visiting
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

THIS ISSUE AND WHY IT MATTERS
T he passage in July 2010 of the Patient Protection and Affordable Care Act established a federal grant program for home visiting services. The large federal investment
underscored the need to expand the knowledge base around high-quality, evidence-based home visiting programs. Since that time, efforts are underway to advance the understanding of effective home visiting practices across the country. This issue of Zero to Three presents a collection of articles that share new findings from the Pew Home Visiting Campaign, a project of the Pew Center on the States. With funding from the Doris Duke Charitable Foundation and the Children’s Services Council of Palm Beach County (Florida), the Pew Home Visiting Campaign commissioned a variety of research projects to investigate critical questions regarding program design and implementation. The five research projects featured in this issue explore various aspects of evidence-based programming that lead to success. Two additional articles share efforts related to the Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program, part of The Patient Protection and Affordable Care Act that provides $1.5 billion over 5 years to states, territories, and tribes. A goal of the MIECHV program is the integration of home visiting services into a high-quality, comprehensive early childhood system that promotes health and well-being for pregnant women, parents, caregivers, and children from birth to 5 years old. In addition to the feature articles, this issue offers two “Perspectives” columns: one explores the relationship between home visiting staffing patterns, training, and outreach activities and maternal program involvement; the other discusses the value of reflective practice for home visitors and the families they serve.
Stefanie Powers Editor
Monica Herk and Andrea Hewitt Guest Editors
T his issue of Zero to Three also marks a milestone as we launch a new digital edition of the Journal. The digital version provides many benefits and features: you can easily search for topics of
interest; access the Journal from wherever you are; store your library of back issues; and much more. Subscribers to Zero to Three will have free access to the digital edition through your email address, so it’s important to make sure your records are up-to-date. To update the e-mail address we have on file for you, please call 1-800-899-4301 or email [email protected].
Another exciting development with the Zero to Three Journal is the opportunity to earn Continuing Education Units (CEUs) for reading Journal issues and taking an online assessment. Offered in collaboration with the University of Wisconsin–Stout, you can earn 1 CEU for each themed issue of the Journal. Each CEU is worth 10 training hours. Go to www.zerotothree.org/JournalCEU to learn more!
Visit the Zero to Three Journal on Facebook at www.facebook.com/zerotothreejournal and let us know what you think of these new innovations. And be sure to check out ZERO TO THREE’s new organizational Facebook page at www.facebook.com/ZEROTOTHREE.
Stefanie Powers, [email protected]
Patient Protection and Affordable Care Act. (2010). Pub. L. No. 111-148, §2702, 124 Stat. 119, 318-319.
The views expressed in this material represent the opinions of the respective authors and are intended for education and training to help promote a high standard of care by professionals. Publication of this material does not constitute an endorsement by ZERO TO THREE of any view expressed herein, and ZERO TO THREE expressly disclaims any liability arising from any inaccuracy or misstatement, or from use of this material in contravention of rules, regulations, or licensing requirements.
®
Fo u n d e d i n 1 9 8 0
Sally Provence, Editor 1980 –1985
Jeree Pawl, Editor 1985–1992
Emily Fenichel, Editor 1992–2006
�Editor
Stefanie Powers
Director of Production
Jennifer Moon Li
�Design Consultant
Heroun + Co.
Production
K Art and Design, Inc.
�Executive Director
Matthew E. Melmed
ZERO TO THREE Board of Directors
T. BERRY BRAZELTONSELMA FRAIBERG
STANLEY I. GREENSPANJ. RONALD LALLY
BERNARD LEVYREGINALD S. LOURIE
PETER B. NEUBAUERROBERT A. NOVERSALLY PROVENCE
JULIUS B. RICHMONDALBERT J. SOLNITLEON J. YARROW
SAMUEL J. MEISELS KYLE D. PRUETT
ARNOLD J. SAMEROFF
MARILYN M. SEGALJACK P. SHONKOFF
EDWARD ZIGLER
Founding Members
Directors Emeriti
KATHRYN E. BARNARD T. BERRY BRAZELTON
MARIA D. CHAVEZ HELEN EGGER
ROBERT N. EMDE LINDA GILKERSON WALTER GILLIAM
BRENDA JONES HARDENJ. RONALD LALLY
ALICIA F. LIEBERMAN JOHN LOVE
ANN PLESHETTE MURPHYBRIAN A. NAPACK
JOY D. OSOFSKY JEREE H. PAWL CHERYL POLKRIZWAN SHAH
REBECCA SHAHMOON SHANOK PAUL. G. SPICEREUGENE STEIN
MINDY STEINLYNN G. STRAUS
ROSS THOMPSONGINGER WARD
SERENA WIEDER HARRY H. WRIGHT
CHARLES H. ZEANAH
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
January 2013 Volume 33 No. 3ContentsStr engthening Home Visiting Through R esea rch
5 NEW RESEARCH STRENGTHENS HOME VISITING FIELD: The Pew Home Visiting Campaign
L i b b y D o g g e t t
10 ASSESSING QUALITY IN HOME VISITING PROGRAMS J o n Ko r f m ac h e r , Au d r e y L a s z e w s k i , M a r i e l S pa r r , a n d
J e n n i f e r H a m m e l
17 TOWARD POPULATION IMPACT FROM HOME VISITING K e n n e t h A . D o d g e , W. B e n j a m i n G o o d m a n , R o b e r t M u r p h y,
K a r e n J . O ’ D o n n e l l , a n d J e a n n i n e M . S at o
24 DOES HOME VISITING BENEFIT ONLY FIRST-TIME MOTHERS?: Evidence From Healthy Families Virginia
L e e H u n t i n g t o n a n d J o s e p h G a l a n o
31 EFFECTIVENESS OF HOME VISITING AS A STRATEGY FOR PROMOTING CHILDREN’S ADJUSTMENT TO SCHOOL
K r i s t e n K i r k l a n d
39 HOME VISITING PROCESSES: Relations With Family Characteristics and Outcomes
C a r l a A . P e t e r s o n , L o r i A . R o g g m a n , B e t h G r e e n ,
R ac h e l C h a z a n - C o h e n , J o n Ko r f m ac h e r , L o r r a i n e M c K e lv e y,
D o n g Z h a n g , a n d J a n e B . At wat e r
A l s o i n T h i s I s s u e :2 This Issue and Why It Matters—S t e fa n i e P ow e r s , M o n i c a
H e r k , a n d A n d r e a H e w i t t
4 Letters—W h at O u r R e a d e r s H av e t o S a y
45 NEW OPPORTUNITIES AND DIRECTIONS IN HOME VISITING RESEARCH AND EVALUATION— L au r e n H .
S u p p l e e , R o b i n L . H a r w o o d , N a n c y G e y e l i n M a r g i e , a n d
A l e t a L . M e y e r
51 FEDERAL HOME VISITING UNDER THE AFFORDABLE CARE ACT— K at h l e e n S t r a d e r , J ac q u e l i n e C o u n t s , a n d
J i l l F i l e n e
58 PERSPECTIVES—MATERNAL ENGAGEMENT IN HOME VISITING: The MOM Program—J e r i ly n n R a d c l i f f e
a n d D o n a l d F. S c h wa r z
62 PERSPECTIVES—REFLECTIVE PRACTICE: Look, Listen, Wonder, and Respond—D e b o r a h J . W e at h e r s t o n
66 Field Notes—N e w s B r i e f s a n d R e s e a r c h I n s i g h t s
67 Jargon Buster—A G l o s s a r y o f S e l e c t e d T e r m s
Cover photo: James Kegley
Zero to Three is the bimonthly journal of ZERO TO THREE: National Center For Infants, Toddlers, and
Families. All rights reserved. To obtain permission for reproduction or use in course work of Zero To Three materials by copy centers of university bookstores, contact: Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400; fax (978) 750-4470, www.copyright.com ISSN 0736-8038 © 2013 Zero To Three: National
Center For Infants, Toddlers, and Families, 1255 23rd Street, NW, Suite 350, Washington, DC 20037, (202) 638-1144; Customer Service: 1-800-899-4301
www.zerotothree.org/journal
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Letters
Understanding School ReadinessI want to congratulate you on the comprehen-sive September 2012 issue of the Zero to Three Journal, Understanding School Readiness. I have shared the information with program and development staff, community policy leaders, board members and early child-hood educators. Each article in the Journal addresses key concerns with thoughtfulness, supporting research and a common language that everyone can understand. Diverse com-munities in Wisconsin are implementing strategies to measure school readiness with-out fully understanding the complexity of preparing children and adults alike, so that we can achieve the educational outcomes we
desire. Our community is involved in several “cradle to career” initiatives, school readi-ness assessment efforts and child care quality improvement approaches that are struggling with this issue from a variety of angles. The September Journal helped to better frame and articulate the research, the practice and the policy implications that will guide us to success. Thanks to the authors and to the Zero to Three Journal editorial staff for taking a wealth of information and synthesizing it so well for those of us in the field.
Christine P. Holmes, MSW Penfield Children’s Center
Milwaukee, Wisconsin
Send your feedback to the Editor
of the Zero to Three Journal. Email
Stefanie Powers at spowers@
zerotothree.org, call 202-857-2641,
or fax 202-638-0851. Include your
name, affiliation, city, and state.
Letters may be edited for length and
clarity.
Getting Ready for School Begins at BirthHow to Help Your Child Learn in the Early YearsCLAIRE LERNER and LYNETTE CIERVO
Getting Ready for School Begins at Birth helps parents and other caregivers understand how children from birth to 3 years learn the basic skills they need to be successful in school. It also shows parents and caregivers how they can nurture the development of those crucial skills.
2004. 12 pages.
ENGLISH VERSION: SPANISH VERSION:ITEM #325 ITEM #326ISBN 0-943657-87-3 ISBN 0-943657-88-1$30.00/20 BROCHURES $30.00/20 BROCHURES
Getting Ready for School Begins at Birth
Order your copy today! Call toll-free (800) 899-4301 or visit our bookstore at www.zerotothree.org
The Nation’s Leading Resource
on the First Years of Life
Sold in packets
of 20 to make
them easy to
distribute to
parents
and caregivers!
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5
In 2008, The Pew Charitable Trusts launched a campaign to educate policymakers about the proven value of home visiting, provide solid research, and promote state investment in programs that achieve the strongest outcomes for children and families.
The federal Maternal, Infant, and Early Childhood Home Visiting Program was established in 2010 as part of the Patient Protection and Affordable Care Act (2010) to provide grants to support state home visiting programs. At least 75% of federal funding to each state must be spent on “evidence-based” models—those with a proven record of effectiveness. Up to 25% may be spent on promising programs that have not yet been subject to rigorous evaluation.
Iowa, Maryland, and Michigan all enacted laws in 2012 to ensure that their home visiting dollars produce maximum results for new parents and their babies and also a solid return on taxpayers’ investment. These reforms require that most of the states’ home
next generation of home visiting inquiry. The articles in this issue show how
home visiting research has progressed in the past few years. When a field first moves toward identifying and developing evidence-based practices, the initial question is “What works?”. As practitioners gain more experience implementing proven models, study questions become more nuanced, such as, “What works for whom and under
New Research Strengthens Home Visiting Field
The Pew Home Visiting Campaign
LIBBY DOGGETTPew Home Visiting Campaign
Washington, DC
visiting funds go to evidence-based programs. They also mandate that states set up the data and tracking systems necessary to ensure programs actually help achieve stated goals, such as reduced infant mortality or improved school readiness.
Over the coming months, the Pew Home Visiting Campaign will continue to partner with states to help them develop and implement high-quality, effective home visiting policies and practices. One key to those efforts is continued research. The Doris Duke Charitable Foundation understood that a major investment in the evidence base for this work was needed. With their leadership support, and key additional funding from the Children’s Services Council of Palm Beach County (Florida), the Campaign has been able to enhance the evidence base underpinning home visiting and identify areas in need of further investigation. This issue of Zero to Three provides an opportunity to share five new studies that represent the
Voluntary home visiting matches parents with trained professionals to provide information and support during pregnancy and throughout a child’s first few years. Properly designed and delivered home visiting programs improve short- and long-term child and family outcomes, including reducing the number of children in social welfare, mental health, and juvenile corrections
systems. Those outcomes, in turn, result in considerable cost savings for states and taxpayers.
AbstractExtensive research has shown that home visiting parental education programs improve child and family outcomes, and they save money for states and taxpayers. Now, the next generation of research is deepening understanding of those program elements that are essential to success, ways to improve existing models, and factors to consider in tailoring home visiting to local contexts and particular target populations. All new parents need good information about their child’s development to help them through the stress and uncertainty that come with having a baby. Years of research have shown that this vital support can be provided, in part, by formal parent-education programs called “home visiting.”
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
quality-rating tool moves us down this road, it will become an important self-assessment tool, allowing programs to measure how they do in the crucial areas and then tailor and target their improvement efforts. As Korfmacher et al. put it, the new rating tool will serve as a “roadmap to improvement.” Korfmacher and his colleagues (this issue, p. 10) field tested the current version of the tool with 21 home visiting programs in Wisconsin and Illinois. Their report is based on preliminary results from a small field test. The tool will require additional development, but their article gives an indication of the type of analyses it will enable. Although the tool does not take the place of outcome measures, Korfmacher et al. have moved the home visiting field forward toward being able to measure and compare the quality of program process across a variety of models.
Positive Results for a Universal Access Model
A consistent challenge for states has been that home visiting models with the strongest evidence of effective-
ness tend both to be intensive—prescribing regular home visits for 2 years or more—and to have high attrition rates (e.g., 40–50% of targeted participants never enroll or drop out before program completion; Daro, McCurdy, Falconnier, & Stojanovic, 2003; Harding, Reid, Oshana, & Holton, 2004: Olds, Henderson, & Kitzman, 1994). The intensity of these pro-grams makes them expensive, and the high attrition rates make it difficult to affect over-all negative outcome rates.
In their article, “Toward Population Impact From Home Visiting,” Kenneth Dodge and his colleagues (this issue, p. 17) describe a well-implemented, randomized, controlled impact evaluation of Durham Connects, a universally available, voluntary nurse-conducted home visiting program for newborns and their families.
Durham Connects is designed to have low costs ($700 per birth) and to reduce attrition. It begins with a staff visit to the family of every newborn while still in the hospital to schedule a nurse home visit if the family agrees. That initial home visit takes place when the baby is approximately 3 weeks old and is followed by one or two additional visits as needed. In addition to teaching about health and well-being, the nurse home visitor assesses the family’s health and other risk factors and refers them to appropriate community services if needed.
For an 18-month period from 2009 through 2010, every even-birth-date baby in Durham County, N.C., received Durham Connects services, while every odd-birth-date baby received “services-as-usual.” Durham Connects resulted in statistically significant
population beyond first-time, at-risk moth-ers. One such program is accessible to all new parents, while the other serves at-risk moth-ers who are having second or subsequent babies. The fourth article presents findings on home visiting’s positive impact on chil-dren’s school readiness. The fifth article uses data from the Early Head Start program eval-uation to examine relationships between participant and service characteristics, and ultimate outcomes for various groups of chil-dren and families.
A Tool for Assessing Program Quality
The article by Jon Korfmacher and colleagues, “Assessing Quality in Home Visiting Programs” (this issue,
p. 10) describes the development and initial field testing of a new standardized instru-ment—the Home Visiting Program Quality Rating Tool. This is the first tool that mea-sures overall program quality across home visiting models, eventually filling a gap in the field for the states, most of which use multi-ple models.
Researchers know that high-quality home visiting can yield better outcomes for families, but they know much less about which are the key “active ingredients” in different program models—the practices and activities essential to achieving improved outcomes for various populations. In order to identify these critical program elements, the home visiting field needs a shared vocabulary as well as common definitions and ways of measuring program practice. As this new
what circumstances?” Researchers and practitioners develop an understanding that even evidence-based models do not always achieve the same outcomes when expanded to new contexts or different populations than those for which they were initially tested.
States need an ongoing process to:
• Choose home visiting models on the basis of evidence of effectiveness in simi-lar contexts with similar populations.
• Adapt the model by applying its core principles to that state’s context.
• Routinely monitor and analyze the impact on desired program out-comes of each adjustment to the base model. In other words, which adapta-tions maintain fidelity to the model and which don’t? Which adaptations lead to improved results, which actually reduce effectiveness, and which make no differ-ence at all?
Good metrics are essential to this process, both to measure outcomes and to assess how programs are actually being delivered.
The articles that follow deepen the home visiting field’s understanding of those aspects of evidence-based programming that are essential to success. They also suggest approaches to further improve these models and tailor them to local contexts.
The first article describes a new instru-ment to measure and compare program quality from various home visiting models. The next two articles find evidence of effec-tiveness for programs that expand the target
All new parents need good information about their child’s development to help them through the stress and uncertainty that come with having a baby.
Ph
ot
o: J
am
es
K
eg
le
y
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 7
interesting to note, however, first-grade math and reading achievement did not show effects from the program.
HFNY targets disadvantaged expectant and new parents—those with an infant less than 3 months old—deemed at risk of maltreating their child. The program serves a poor, racially and ethnically diverse population of young, mostly first-time mothers and their children. Participating families receive a series of home visits lasting until the child enters kindergarten or Head Start. As is too often the case in home visiting programs, many families in the study did not receive the prescribed intensity of services.
Nevertheless, the program was able to cut the first-grade retention rate in half (from 7.10% to 3.54%) and to almost double the percentage of first graders demonstrating the school-readiness skills measured by the study (7.74% of the control children versus 13.15% of the HFNY children). These soft skills may be especially important because they help children to benefit from classroom environments throughout their school years.
Kirkland’s (this issue, p. 31) finding of no impact on math and reading grades of HFNY first graders is disappointing, but the author speculates that the measure used (reading and math grades on first-grade report cards) may be too inaccurate to discern an effect. In addition, challenges in obtaining school records significantly reduced the sample size for this portion of the analysis, perhaps contributing to the difficulty in finding a statistically significant effect. In any case, possession of soft school-readiness skills in first grade may be a more reliable and
However, it builds on the earlier study by comparing program outcomes for first-time and multiparous mothers participating in Virginia’s Healthy Families program from July 1999 through June 2010. Participation levels for multiparous mothers and their outcomes on measures of the home environment and child immunizations were generally similar to those for first-time mothers, after controlling for their higher levels of risk.
A limitation of Huntington and Galano’s study (this issue, p. 24) is that it is based on observational data. It cannot rule out the possibility that the programs involved were systematically selecting (either consciously or unconsciously) only those multiparous mothers most likely to benefit from services. Huntington and Galano wisely call for a randomized controlled study to further test their findings. Nevertheless, the evidence presented in their article suggests that the field’s presumption in favor of serving only first-time mothers should be reexamined.
Positive Effects of Home Visiting on School Readiness
Studies of home visiting’s impact on school readiness have been relatively few and have yielded mixed results.
In a well-implemented, randomized, controlled study, Kristen Kirkland (this issue, p. 31) found that Healthy Families New York (HFNY) reduced first grade retention rates and improved three so-called “soft” school-readiness skills 7 years after program enrollment. (These include ability to work or play cooperatively, follow instructions or rules, and complete work on time.) It is
improvements in a range of outcomes. Although the effect sizes were generally in the low to moderate range, the reduction in infant emergency medical care for Durham Connects families by the time infants were 6 months old was large enough to create a benefit of $1.59 per dollar spent on the program. In fact, Dodge and Goodman and their colleagues (this issue, p. 17) report that, because of the low cost of the program and the reduction in emergency medical costs, Durham Connects provides a positive return on investment by the time an infant reaches 3 months old. The researchers plan to follow participating families until the child is 6½ years old to assess what additional benefits, if any, accrue from the program over time.
One caveat is that Durham Connects is being implemented in a community with a large number of social service organi-zations to which families can be referred. Durham Connects spent 6 years prior to the launch of the home visiting program build-ing a Preventive System of Care that includes almost all community agencies and provid-ers in Durham County. It is not clear whether Durham Connects’ success could be repli-cated in areas lacking such a comprehensive set of services. The developers intend to rep-licate and evaluate the model in four rural North Carolina counties to test this question.
Evidence Supporting Service for Second-Time Mothers and Beyond
In their article, “Does Home Visiting Benefit Only First-Time Mothers? Evidence From Healthy Families
Virginia,” Lee Huntington and Joseph Galano (this issue, p. 24) compare outcomes of first-time (primiparous) mothers with those of mothers with second or later babies (multiparous) among Healthy Families participants in Virginia. The authors point out that because some of the most well-known findings concerning home visiting’s effectiveness come from evaluations of the Nurse-Family Partnership, which serves only first-time mothers, it is often assumed that first-time mothers benefit from home visiting more than others. Yet this assumption, which they say denies services to more than 60% of families that give birth each year, has seldom been tested empirically.
In an earlier randomized controlled eval-uation of the Hampton (Virginia) Healthy Start program, Galano and Huntington (1999) found that multiparous mothers and their children received benefits similar to first-time mothers and their children on measures of infant health, parent–child inter-action, and the home environment.
The study that Huntington and Galano describe in this issue of Zero to Three (p. 24) is not a randomized controlled experiment.
Properly designed and delivered home visiting programs improve short- and long-term child and family outcomes.
Ph
ot
o: J
am
es
K
eg
le
y
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

8 Z e r o t o T h r e e J a n u a r y 2 0 1 3
classifying risk subgroups for study, Peterson and her colleagues (this issue, p. 39) identified five risk factors: being a teen mother, neither being married nor living with a partner, receiving public assistance, having less than a high school education, and being neither employed nor in school or training. They also identified three degrees of risk—low, moderate, and high.
The researchers found that families at moderate risk (defined as having two to three risk factors) experienced the most positive child and family impacts from home visiting. The authors speculate that high-risk families likely face more challenges that distract parents and home visitors from focusing on the child’s development.
Overall, the findings of Peterson and her colleagues (this issue, p. 39) are complicated, interesting, and sometimes counterintuitive. For example, it was not surprising that teen mothers were less engaged in home visiting than were older mothers. However, it was surprising that greater home visiting dosage and engagement with the program were generally associated with more negative outcomes for both the children and teen mothers. The authors suggest that the association between more home visits and higher rates of negative outcomes occurred because home visitors focused greater efforts on those families they identified as needing more help. The lack of a rigorous randomized controlled trial, comparing teen mothers who are assigned different levels of home visiting services, leaves open the question of why this finding occurred. Such a study is needed to investigate the validity of the authors’ explanation and to explore the specific causes of these outcomes.
With regard to race and ethnicity, the relationship between mothers’ program participation (e.g., dosage and engagement) and ultimate child and family outcomes varied by group. For example, while greater maternal engagement led to improved cognitive outcomes among White children, higher dosage and engagement levels were associated with poor outcomes— increased aggression and lower levels of language and cognitive development—for African American children at the time researchers assessed these skills. However, increased dosage and family engagement were associated with improved parental outcomes—such as reduced maternal depression and higher income—in African American families.
As Peterson and her colleagues (this issue, p. 39) make clear, controlled experimentation with the program content and dosage offered to various subgroups will be necessary to allow researchers to determine, with high confidence, whether relationships they found
Whether this results from normal differences in developmental trajectories between boys or girls or truly a differential program impact on boys and girls is worth further exploration.
This study is an important and well-conducted piece of longitudinal research demonstrating substantive impacts on child educational outcomes 7 years after families’ enrollment. It adds to the body of research that demonstrates lasting positive impacts of home visiting on families’ life chances.
What Worked for Whom in Early Head Start Home Visiting
Carla Peterson and her colleagues, in their article “Home Visiting Processes: Relations With Family
Characteristics and Outcomes” (this issue, p. 39), explore how families’ participation in Early Head Start home visiting services—as measured by dosage (number of visits), service content, and mother’s engagement—affected key outcomes. To do so, they made good use of long-term follow-up data available from the Early Head Start Research and Evaluation Project—a large, randomized controlled evaluation of 17 Early Head Start programs that followed the subject children until they were 10 years old. These data provided an excellent opportunity to begin to examine complicated and important questions of how home visiting content and intensity affect target populations.
The study looked at various subgroups, such as teen parents, racial and ethnic minorities, and parents at high risk. In
important predictor of later academic achievement.
As with many other studies, the HFNY analysis indicated that intensity of services matters. Children who received a higher percentage of expected visits were 2.28 times more likely to excel academically in first grade than their HFNY peers who received fewer of their prescribed visits.
Finally, this study found a significant pattern of differential impact by child gender, which other research has also suggested. Compared to the control group, female HFNY first graders were more likely to excel academically (32.62% versus 17.47%) and less likely to do poorly (19.71% versus 32.17%). There were no such differences for boys.
Studies of home visiting’s impact on school readiness have been relatively few and have yielded mixed results.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/S
er
rN
ov
ik
Learn More
These articles in this issue are part of a collection of 13 new home visiting research studies. Complete reports on each study are available at the Web page of the Pew Home Visiting Campaign.pewstates.org/homevisiting
Doris Duke Charitable Foundation
www.ddcf.org
Children’s Services Council of Palm
Beach County (Florida)
www.cscpbc.org
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 9
a robust research agenda and works with advocates in target states to build political and public understanding and support for data-driven investments that align with federal guidance. She testifies before state legislatures and other government entities, and she is the author of numerous articles in outlets around the country, explaining the powerful potential of home visitation to improve the lives of children and families and yield strong returns to taxpayers.
Author’s Note:
The studies in this edition of the Zero to Three Journal were jointly funded by the Doris Duke Charitable Foundation, the Children’s Services Council of Palm Beach County (Florida), and the Pew Center on the States. The views expressed are those of the authors and do not necessarily reflect the views of the funders.
turns from relatively simple inquiries about effectiveness to more nuanced explorations of the relationships between populations served, program characteristics, and outcomes.
These articles are an important contribu-tion to the efforts by everyone in the field to improve outcomes for children and families. And these articles portend exciting advances in the quality, effectiveness, and impact of home visiting in the future.A
Libby Doggett, PhD, is director of the Pew Home Visiting Campaign at the Pew Center on the States. The campaign partners with state policymakers and other leaders to promote effective state policies and investments in quality, home-based programs for new and expectant families.
As the lead for Pew’s work to advance evidence-based home visitation, Doggett oversees
are causal versus merely correlational. The authors rightly point out that ongoing data collection and analysis are needed among practitioners and researchers to better understand and improve how program practice impacts ultimate outcomes for different groups of children and families. Their article is an important contribution to understanding what works for each group under particular circumstances, and highlights clear questions that warrant further research.
Looking Forward
Taken together, the five articles in this issue provide fresh evidence supporting the impact of high-
quality home visiting programs on important outcomes for children, families, and society. The studies demonstrate the ongoing maturation of the home visiting field as it
References
Daro, D., McCurdy, K., Falconnier, L., &
Stojanovic, D. (2003). Sustaining new parents in home visitation services: Key participant and program factors. Child Abuse and Neglect, 27, 1101–1125.
Dodge, K. A., Goodman, W. B., Murphy, R.,
O’Donnell, K. J., & Sato, J. M. (2013). Toward a population impact from home visiting. Zero to Three, 33(3), 17–23.
Galano, J., & Huntington, L. (1999). Year VI evaluation of the Hampton, Virginia Healthy Families Partnership: 1992-98. Williamsburg, VA: Center for Public Policy Research, the Thomas Jefferson Program in Public Policy, the College of William and Mary.
Harding, K., Reid, R., Oshana, D., & Holton, J.
(2004). Initial results of the HFA implementation study. Chicago, IL: National Center on Child Abuse Prevention Research, Prevent Child Abuse America.
Huntington, L., & Galano, J. (2013). Does home visiting benefit only first-time mothers? Evidence from Healthy Families Virginia. Zero to Three, 33(3), 24–30.
Kirkland, K. (2013). Effectiveness of home visiting as a strategy for promoting children’s adjustment to school. Zero to Three, 33(3), 31–37.
Korfmacher, J., Laszewski, A., Sparr, M., &
Hammel, J. (2013). Assessing quality in home visiting programs. Zero to Three, 33(3), 10–16.
Olds, D. L., Henderson, C. R., & Kitzman, H.
(1994). Does prenatal and infancy nurse home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life? Pediatrics, 94, 89–98.
Patient Protection and Affordable Care Act.
(2010). Pub. L. No. 111-148, §2702, 124 Stat. 119, 318–319.
Peterson, C. A., Roggman, L. A., Green, B.,
Chazan-Cohen, R., Korfmacher, J.,
McKelvey, L.,…Atwater, J. B. (2013). Home visiting processes: Relations with family characteristics and outcomes. Zero to Three, 33(3), 39–44.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
1 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Assessing Quality in Home Visiting Programs
JON KORFMACHERErikson Institute
AUDREY LASZEWSKIThe Early Years Home Visitation O utcomes Project of Wisconsin
Green Bay, Wisconsin
MARIEL SPARRErikson Institute
JENNIFER HAMMELChildren’s Hospital of Wisconsin
Milwaukee, Wisconsin
AbstractDefining quality and designing a quality assessment measure for home visitation programs is a complex and multifaceted undertaking. This article summarizes the process used to create the Home Visitation Program Quality Rating Tool (HVPQRT) and identifies next steps for its development. The HVPQRT measures both structural and dynamic features of program quality and provides a comprehensive look into how home visiting services are delivered. While additional research is underway for further testing and refinements, the initial research suggests that the HVPQRT is a promising instrument for home visiting stakeholders who strive to increase service quality.
Across the United States, home visiting is increasingly recognized as an important strategy for strengthening families of young children, and is even more so now that the federal government seeks to expand home visiting services through different initiatives including the Maternal, Infant, and Early Childhood Home Visiting program. Nationally recognized models have provided
evidence to varying degrees of their impact on outcomes for children and families, and the federal government has created guidelines to assess the quality of this evidence. These efforts provide guidance regarding what can be considered “evidence-based,” such as the reviews of home visiting programs on the Home Visiting Evidence of Effectiveness web site (U. S. Department of Health and Human Services, n.d.). Such guides are typically focused on program outcomes. They have less to say about how home visiting program services are actually delivered, and they do not measure best practices that might exist across different program models.
There have been attempts to identify best practices in home visitation, partly as a strategy to deal with concerns about the limited extent or the inconsistency of program results (Daro, 2006; Johnson, 2009; Weiss & Klein, 2006). As Durlak and DuPre (2008) highlighted, implementation data is an essential component of program evaluations and provides insight into program impacts, including inconsistencies in outcomes and guidance on how to increase positive impacts. Although several national models have proprietary assessment tools to measure fidelity to their model and to
activities using cross-model quality guidelines.
In this article we summarize a newly developed tool, the Home Visiting Program Quality Rating Tool (HVPQRT), designed to assess a program’s implementation of best practice elements across multiple dimensions of program operations. This effort was born from the authors’
use in credentialing sites, there is currently no tool available measuring features of program quality that is applicable across home visiting models. Furthermore, little research currently looks at common elements of practice. Many communities and states, however, support multiple home visiting programs, which creates a challenge when needing to decide how to invest limited resources. In addition to the benefits of a quality assessment tool for funders, programs themselves will also benefit from having a practical method for assessing themselves and guiding their program development
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 1 1
signify program quality. On the basis of this general consensus, we established an initial working list of features of program quality that we used in facilitated discussions with key home visiting stakeholders. We convened a small working group of program directors and consultants that met regularly over the span of a year to review our progress, help us develop descriptions and benchmarks
This multilevel framework guided the development of the HVPQRT as a measure of programs’ implementation of best practice elements as they occur within the multiple, embedded contexts of program operations. In addition, as suggested by Daro (2010), the HVPQRT measures both structural aspects of program quality (e.g., materials, resources, and education and background of staff ) as well as more dynamic program features (e.g., the content and nature of supervision sessions, the work environment, and home visitor–parent relationship quality).
We used a multistep iterative process to develop the tool. We began with a review of the literature and quickly noted gaps within the empirical research base for home visitation in regard to assessing how specific aspects of program implementation influence program effectiveness (the final report to the Pew Center on the States provides more detail on the results of the literature review; see Korfmacher, Laszewski, Sparr, & Hammel, 2012). For example, there is little research on the impact of administrative factors (e.g., leadership, work environment, supervision, and program monitoring) on home visiting program effectiveness and few measurement tools to address these issues, although this is generally recognized in the human service field as an essential element of program quality (Durlak & DuPre, 2008; Glisson, 2010).
Although the existing literature lacks robust empirical examinations of program quality dimensions, our review of it revealed a general consensus concerning best practice elements that are assumed or expected to
professional experiences in various quality initiatives. Our experiences suggested that home visiting program staff often agreed on broad categories of quality (e.g., providing intensive home visits), but they had different definitions of these concepts. This suggested value in developing a common understanding of the ingredients of quality as they apply to home visiting programs.
Our goal was the development of a prac-tical and reliable best practice assessment tool that works for any home visiting pro-gram model. This tool provides descriptive criteria and numerical scores for key qual-ity program areas. The criteria are based on best practice as identified in the litera-ture and the field, allowing for review of how a program measures up against a common standard. Although the field of home visita-tion recognizes the importance of—and is moving toward—more comprehensive eval-uations of program quality as part of funded initiatives (e.g., the Evidence-Based Home Visiting initiative; Boller et al., 2011), there are currently no cross-model tools avail-able that assess both structural and dynamic aspects of program quality as they operate in the multilayered environment of home vis-iting programs. We wanted our measure to be easily understandable, feasible to conduct in a timely manner, and capable of provid-ing a process for programs to reflect on their strengths as well as areas of challenge. The HVPQRT is not intended to replace model-specific credentialing or certification, but rather to complement any individual model’s quality improvement processes.
Framework for HVPQRT
Daro (2010) discussed the multi-layered nature of home visiting programs, whereby program
operations occur at a variety of levels ranging from the overall program down to individual participant experiences. One way to represent this is with an ecological framework (see Figure 1). Implementation of best practice elements occurs within a series of systems, beginning at the level of the individual home visitor and her interactions with the family over time during home visits. The home visitor’s ability to work effectively with a family is influenced both by her personal characteristics (an individual level factor) as well as by the level of support she receives from the program, in terms of supervision, training, other professional development opportunities, and curricula used (all support level factors). This support, in turn, is influenced by the organizational ability of the program, including its leadership and administration, fiscal management, organizational climate, and connection to the larger system of services in the community.
Figure 1: Ecological Framework of Program Quality
Home visiting is increasingly recognized as an important strategy for strengthening families of young children.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/d
am
ir
cu
di
c
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
1 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Nine home visiting programs piloted the initial version of the tool by using it to assess their own and a peer program. The experience of giving the tool in its draft form to programs and asking them to use and critique it was a humbling one, as we quickly came to real-ize that the initial draft of the tool was much too long and overwhelming to the home vis-iting program staff. Many indicators which seemed clear to us in theory were difficult to assess in practice, and program directors became frustrated with the time it took to col-lect the information and the vagueness of our guidelines regarding how to collect this infor-mation. This feedback led us to create specific data collection and scoring guidelines for each subscale. We also engaged in an intense period of scale reduction, as we collapsed some subscales and eliminated others.
We made difficult decisions about what to eliminate in order to remain true to our original plan of creating a tool that could be feasibly implemented in the field. One such area was direct assessment of home visiting practice. An attempt to include data collec-tion via observation of home visits proved logistically challenging within the context of a one-day site review and was eliminated. Instead, the current version relies on an ana-log assessment of practice by using case vignettes, where home visitors are given three brief scenarios covering common challenges in home visits (e.g., an unresponsive parent, or a parent concerned about his child’s devel-opment) and asked how they would respond.
As currently designed, the tool relies on interviews with home visitors and leadership staff, chart and record review, and completion of short online surveys by both home visitors and program administration staff. The online surveys were created to further reduce the burden of interviewing staff during the day of the site visit. The interview questions were replaced by checklists and survey questions. For example, the program’s use of reflective supervision was assessed by home visitors’ responses to 14 survey questions (e.g., “I have the opportunity to think about my actions and how it impacts the work I do with families.”). These questions were developed on the basis of facilitated discussions with home visiting program directors and staff, interviews with home visiting trainers in Wisconsin responsible for the development of reflective supervision training, and other relevant literature.
These revisions resulted in the tool being organized into 5 scales, with 23 subscales and 63 indicators using a 7-point scaling with a threshold scoring system (see Table 1). These refinements were further tested by members of the research team at three site visits prior to the formal field testing.
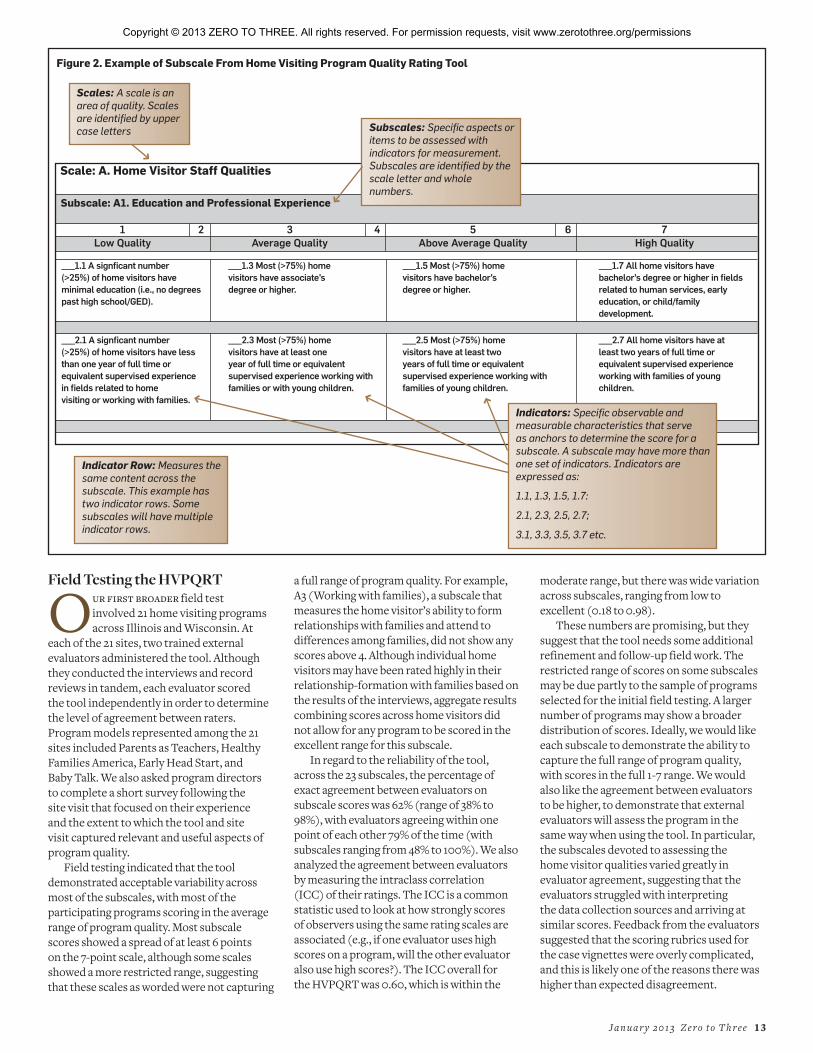
Each of these dimensions (or scales) were further divided into 7-point subscales, ranging from two to eight subscales per dimension (see Table 1). Each subscale was further delineated into two to five indicator rows. Figure 2 uses one subscale as an example of how the tool is organized.
The format of the measure is similar to other quality rating measures, such as the Early Childhood Environmental Rating Scale (Harms, Clifford, & Cryer, 2005) or the Home Observation Rating Scale (Roggman, Boyce, & Innocenti, 2008), with specific indicators aligned to odd-numbered subscale points. The final subscale score is determined by examining the pattern of raters’ scores for the indicators comprising the subscale. For example, a subscale that has a mix of indicators scored at 3 and 5 may receive a final score of 4 for that subscale.
for the initial quality indicators, and provide feedback regarding what quality looks like from the field. We also used a larger advisory committee with representatives from two of the national program models (Healthy Families America and Parents as Teachers), as well as state government staff and trainers. From these discussions, we agreed upon a final list of quality features and developed a framework for the tool consisting of scales and subscales with specific indicators.
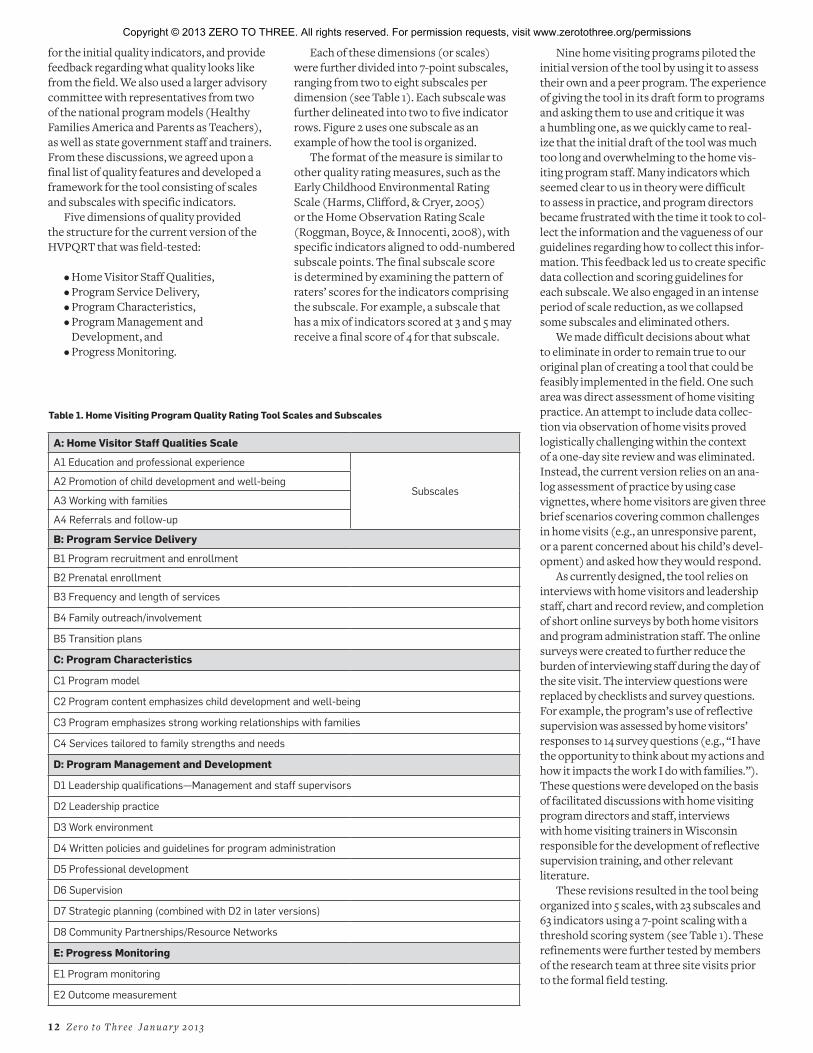
Five dimensions of quality provided the structure for the current version of the HVPQRT that was field-tested:
• Home Visitor Staff Qualities,• Program Service Delivery,• Program Characteristics,• Program Management and
Development, and• Progress Monitoring.
Table 1. Home Visiting Program Quality Rating Tool Scales and Subscales
A: Home Visitor Staff Qualities Scale
A1 Education and professional experience
SubscalesA2 Promotion of child development and well-being
A3 Working with families
A4 Referrals and follow-up
B: Program Service Delivery
B1 Program recruitment and enrollment
B2 Prenatal enrollment
B3 Frequency and length of services
B4 Family outreach/involvement
B5 Transition plans
C: Program Characteristics
C1 Program model
C2 Program content emphasizes child development and well-being
C3 Program emphasizes strong working relationships with families
C4 Services tailored to family strengths and needs
D: Program Management and Development
D1 Leadership qualifications—Management and staff supervisors
D2 Leadership practice
D3 Work environment
D4 Written policies and guidelines for program administration
D5 Professional development
D6 Supervision
D7 Strategic planning (combined with D2 in later versions)
D8 Community Partnerships/Resource Networks
E: Progress Monitoring
E1 Program monitoring
E2 Outcome measurement
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 1 3
moderate range, but there was wide variation across subscales, ranging from low to excellent (0.18 to 0.98).
These numbers are promising, but they suggest that the tool needs some additional refinement and follow-up field work. The restricted range of scores on some subscales may be due partly to the sample of programs selected for the initial field testing. A larger number of programs may show a broader distribution of scores. Ideally, we would like each subscale to demonstrate the ability to capture the full range of program quality, with scores in the full 1-7 range. We would also like the agreement between evaluators to be higher, to demonstrate that external evaluators will assess the program in the same way when using the tool. In particular, the subscales devoted to assessing the home visitor qualities varied greatly in evaluator agreement, suggesting that the evaluators struggled with interpreting the data collection sources and arriving at similar scores. Feedback from the evaluators suggested that the scoring rubrics used for the case vignettes were overly complicated, and this is likely one of the reasons there was higher than expected disagreement.
a full range of program quality. For example, A3 (Working with families), a subscale that measures the home visitor’s ability to form relationships with families and attend to differences among families, did not show any scores above 4. Although individual home visitors may have been rated highly in their relationship-formation with families based on the results of the interviews, aggregate results combining scores across home visitors did not allow for any program to be scored in the excellent range for this subscale.
In regard to the reliability of the tool, across the 23 subscales, the percentage of exact agreement between evaluators on subscale scores was 62% (range of 38% to 98%), with evaluators agreeing within one point of each other 79% of the time (with subscales ranging from 48% to 100%). We also analyzed the agreement between evaluators by measuring the intraclass correlation (ICC) of their ratings. The ICC is a common statistic used to look at how strongly scores of observers using the same rating scales are associated (e.g., if one evaluator uses high scores on a program, will the other evaluator also use high scores?). The ICC overall for the HVPQRT was 0.60, which is within the
Field Testing the HVPQRT
Our first broader field test involved 21 home visiting programs across Illinois and Wisconsin. At
each of the 21 sites, two trained external evaluators administered the tool. Although they conducted the interviews and record reviews in tandem, each evaluator scored the tool independently in order to determine the level of agreement between raters. Program models represented among the 21 sites included Parents as Teachers, Healthy Families America, Early Head Start, and Baby Talk. We also asked program directors to complete a short survey following the site visit that focused on their experience and the extent to which the tool and site visit captured relevant and useful aspects of program quality.
Field testing indicated that the tool demonstrated acceptable variability across most of the subscales, with most of the participating programs scoring in the average range of program quality. Most subscale scores showed a spread of at least 6 points on the 7-point scale, although some scales showed a more restricted range, suggesting that these scales as worded were not capturing
Figure 2. Example of Subscale From Home Visiting Program Quality Rating Tool
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

1 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
We also learned that we underestimated the amount of training evaluators needed to use the tool on site visits. In Wisconsin, we relied on a 1-day training and a follow-up phone call to discuss the scale and the scoring guides. Because of scheduling issues, the site visits occurred more than 1 month after the training session, which likely contributed to lower agreement in the field. For Illinois, training was expanded to 2 days and included scoring exercises, practice interviews, mock administration opportunities, and follow-up telephone support. Examining the data suggested that this increased training helped, as the level of agreement was higher among evaluators in Illinois than in Wisconsin.
On the basis of the results of the initial field testing, we have recently revised the scales. We created more clarity in the individual indicators, and we rewrote the data collection and scoring guides to create more specific guidance for evaluators. The revised version of the tool is currently undergoing another round of field-testing in Massachusetts through a collaboration with the Children’s Trust Fund.
Establishing Validity
Much of our initial field work focused on examining the level of agreement between raters. Deter-
mining the validity of the tool—the extent to which it measures actual dimensions of program quality—is an on-going process. Although measurement validity requires reliability, agreement between raters does not (in and of itself ) demonstrate that the agreed-upon indicators actually correspond to program quality. There are different com-ponents to demonstrating validity of the tool, all of which need to be undertaken in order to increase confidence that the tool is measur-ing what it is supposed to be measuring.
The first component is validating the data collection process. Because the tool relies greatly on interviews and surveys of home visitors and program directors, we need to ascertain whether these participants are reporting accurately about their program by verifying their statements with documentation (e.g., more in-depth chart reviews). In Massachusetts, we have added an extra half-day to the site visits to conduct validity checks of the reported information through additional document and record review. In addition, it will be necessary to collect more information on the scales embedded within the online surveys and on the scoring checklists for the case vignettes. As with the tool itself, these surveys and checklists also need to show adequate range and distribution of scores, so that we can be more confident in the cut-off values and scoring decisions we have set for them. We
can collect this information by using the surveys and vignettes with a larger number of home visitors. For example, we distributed the online home visitor survey at home visiting conferences in Wisconsin and Illinois and asked for anonymous responses from home visitors. We are currently analyzing data from more than 300 respondents to help inform our scoring cut-off values and distribution of scores. In addition, strategies such as cognitive interviewing may also be helpful in determining the extent to which respondents are interpreting the wording of the embedded surveys in the same way.
The second component to establishing validity is linking tool ratings to other established elements of program quality, including accreditation reports from the major program models, home visit observations using validated instrument (e.g., Home Observation Rating Scale; Roggman et al., 2008), or reports from families about their involvement and satisfaction with program services.
A third component is linking tool ratings to program outcomes for children and families. Specifically, outcome indicators need to be collected on a representative sample of families within a program to determine whether quality ratings of programs are positively related to families showing stronger outcomes over time. Examples would depend on the program’s logic model but would likely include such outcomes as breastfeeding rates, parent–child relationship assessments, or parent efficacy.
Finally, a fourth component is examining whether or not the tool is responsive to quality improvement efforts that a program may make. In other words, if a program makes changes in how it operates in response to feedback received from the tool’s findings, will the change be reflected in the score when the program is re-evaluated at a later time?
Feedback From Programs
A fter completion of the site visit, we asked program directors to fill out a brief online survey to provide feed-
back regarding their experience with the HVPQRT and the site visit. Six Wisconsin
programs and nine Illinois programs (15 of 21 programs) responded to the survey and pro-vided feedback.
We asked sites to rate the extent to which different aspects of the site visit were difficult or burdensome, such as scheduling, document preparation, filling out the online surveys, and participation in the interviews. One program found these elements to be difficult, but the vast majority found the demands of the evaluation to be reasonable. Two programs noted that they wanted more time to prepare for the site visit, and some program directors wrote comments that the document preparation took longer than expected. Almost all of the program directors who responded to the survey indicated that they learned things from the evaluation, they found the site visit to be a positive experience, and they believed the HVPQRT measured factors they viewed as key to quality programming. The following quotes highlight some of the feedback that we received from the program directors:
“ The evaluation process provides a better understanding of what our program should be implementing and how we should be self-evaluating.”
“ [The HVPQRT] would give guidance to state systems and larger organizations for shared language for program evaluation and would offer a simple process for agencies to use in their own self assessment.”
The program directors’ comments consistently emphasized that the HVPQRT identified areas of program strength and improvement, helped them feel connected to others in home visiting field, increased their knowledge of aspects of home visiting program quality, and gave them the opportunity to reflect and discuss their work with others. Overall, these results suggest that the tool and the process of collecting data to score it provide a meaningful learning experience for programs.
Policy and Practice
The HVPQRT was initially proposed and designed as a measurement tool with policy and practice applications.
It was designed to be a relatively practical and manageable instrument that combined in one standard rubric multiple dimensions of program quality so as to allow various parties (e.g., researchers, programs, policy stakeholders) to capture the strengths and challenges of home visiting programs no mat-ter what program model was used. Research, practice, and policy each have their particu-lar assumptions and points of view (Shonkoff,
Our goal was the
development of a practical
and reliable best practice
assessment tool that
works for any home
visiting program model.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 1 5
References
Boller, K., Daro, D. Strong, D., Barrett, K.,
Zaveri, H., Paulsell, D.,...Meagher, C. (2011). Data collection instruments for the evidence-based home visiting to prevent child maltreatment cross-site evaluation. Princeton, NJ: Mathematica Policy Research.
Daro, D. (2006). Home visitation: Assessing progress, managing expectations. Chicago, IL: Chapin Hall & Ounce of Prevention. Retrieved November 28, 2012, from www.ounceofprevention.org/
includes/tiny_mce/plugins/filemanager/files/Home%20Visitation.pdf
Daro, D. (2010, December). Replicating evidence-based home visiting models: A framework for assessing fidelity. Princeton, NJ: Mathematic Policy Research & Chapin Hall Issue Brief.
Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41(3-4), 327–350.
Glisson, C. (2010). Organizational climate and service outcomes in child welfare agencies. In M. B. Webb, K. Dowd, B. J. Harden, J. Landsverk, & M. F. Testa (Eds.), Child welfare and child well-being: New perspectives from the National Survey of Child and Adolescent Well-being (pp. 378–406). New York, NY: Oxford University Press.
Harms, T., Clifford, R., & Cryer, D. (2005). Early Childhood Environment Rating Scale (Rev. ed.) New York, NY: Teachers College Press.
Johnson, K. (2009). State-based home visiting. Strengthening programs through state leadership.
2000). This is certainly true regarding home visiting program quality, as recent discus-sions around evidence-based practice attest (Pew Center on the States, 2011).
Program staff found value in reviewing their performance across multiple domains, such as assessing the home visitors’ views of their roles in individual home visits, to supervision provided and received, fiscal management, data tracking, and the pro-gram’s connection to the larger community. This was seen both in the anecdotal feedback provided during the course of the site visits and from the program director survey. The process of preparing for an external evalua-tor site visit and participating in the site visit was an opportunity for home visiting pro-gram staff to engage in discussion on many aspects of program operations, documenta-tion, and quality. From a practice perspective, this tool can be an asset for internal pro-gram management and quality improvement initiatives. One of the contributions of the HVPQRT is that it provides measurable attri-butes of program quality with specific scale points. These indicators provide a road map for program leaders by suggesting a direction for improvement.
One aspect of the tool that requires careful consideration, however, is its potential use to allocate resources. Given the complexity of quality assessment, no one measure by itself should be the basis for high stakes decision making around program funding. Policies which promote program quality improvement efforts, however, should be considered an integral part of an infrastructure to support the field of home visitation. The HVPQRT can be part of this support. For example, the HVPQRT was used as one element of a state-wide evaluation of birth to 3 programs funded by the Illinois State Board of Education’s Prevention Initiative (ISBE PI). Thirty programs across the state participated in this evaluation. Each program received summary feedback of identified strengths and areas for improvement, which it could use as it wished. The overall results were summarized and
presented (without identifying any of the individual participating programs) to ISBE PI’s early childhood education division in order to assist their system-wide planning, including training and technical assistance activities for their birth to 3 PI programs (Korfmacher, Sparr, Chawla, Fulford, & Fleming, 2012).
The HVPQRT may also be helpful in defining the limits of program quality. If programs are regularly showing lower scores in certain areas, this may be suggestive of areas where home visiting programs are limited by the local community or system infrastructure in their ability to provide high-quality services. For example, if a major source of funding for programs provides only yearly grants or contracts with no assumption of future funding, programs will be limited in how well they can demonstrate sound fiscal planning. As another example, home visitors in programs that exist in areas with few other community resources will have a much more difficult time demonstrating their ability to link families to relevant services.
In both cases, a home visiting program will be rated on its ability to perform these functions (fiscal planning and service linkage), but it is constrained by the larger system in which it exists. Using the HVPQRT to highlight these constraints over an entire system or large set of programs is a potentially valuable mechanism for informing policy development in home visitation. For example, the subscale ratings for ISBE PI programs regarding enrolling families prenatally provoked discussion in advisory committee meetings around how to support school district-based home visiting programs in conducting outreach to hospitals and other prenatal referral sources.
In summary, we developed the HVPQRT to fill a gap in home visiting program evaluation and practice by combining both structural and dynamic aspects of program quality in a single measurement tool that can be used across a variety of program models. It is, however, a work in progress. It is our hope that as we further refine the tool and
demonstrate its validity and reliability, it will help advance the field of home visitation. The HVPQRT will also provide meaningful data for program administrators to guide quality improvement efforts and for other stakeholders in helping frame discussions around what supports are needed to further develop home visiting. A
Jon Korfmacher, PhD, is associate professor at the Erikson Institute. Dr. Korfmacher’s research focuses on evaluation of early childhood programs, with an emphasis on home visiting. Previously, he worked on analyses of program implementation of the Nurse-Family Partnership program, and was a co-investigator with a local research partner team for two programs that participated in the Early Head Start Research and Evaluation Project. He is particularly interested in issues of program quality, development of the helping relationship between providers and families, and staff development and training. He is a graduate fellow of ZERO TO THREE.
Audrey Laszewski, MS, is project director for the The Early Years Home Visitation Outcomes Project of Wisconsin and an independent consultant. Ms. Laszewski has more than 20 years of experience in project management and evaluation with a focus on outcome measurement systems for human service providers. She enjoys developing innovative ideas into successful projects and is a frequent speaker on outcome measurement for the field of home visitation.
Mariel Sparr, MS, is a doctoral student at the Erikson Institute where she has been a research assistant on both the Assessing Quality in Home Visiting Programs and the Illinois State Board of Education Birth to Three Evaluation.
Jennifer Hammel is the Child Abuse Prevention Fund director at Children’s Hospital of Wisconsin. Ms. Hammel directs grant making, technical assistance, and advocacy initiatives. She has developed the Fund into the only private sector, child abuse prevention fund in Wisconsin focusing on technical assistance. quality improvement, and outcome attainment.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

1 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
New York, NY: National Center for Children in Poverty.
Korfmacher, J., Laszewski, A., Sparr, M., &
Hammel, J. (2012). Assessing home visiting program quality. Final Report to the Pew Center on the States. www.pewstates.org/research/analysis/pew-supported-home-visiting-research-85899380942
Korfmacher, J., Sparr, M., Chawla, N.,
Fulford, J., & Fleming, J. (2012). Illinois Prevention Initiative Birth To Three evaluation: Summary report. Final report to the Illinois State Board of Education. Retrieved October 31, 2012,
from www.isbe.net/earlychi/preschool/pfa-report/pi-0-3/pi-eval-summary-rpt.pdf.
Pew Center on the States. (2011, August). States and the new federal home visiting initiative: An assessment from the starting line. Retrieved October 31, 2012, from www.pewtrusts.org/uploadedFiles/wwwpewtrustsorg/Reports/Home_Visiting/Home_Visiting_August_2011_Report.pdf
Roggman, L. A., Boyce, L. K., & Innocenti, M. S.
(2008). Developmental parenting: A guide for early childhood practitioners. Baltimore, MD: Brookes.
Shonkoff, J. P. (2000). Science, policy, and practice: Three cultures in search of a shared mission. Child Development, 71, 181–187.
U. S. Department of Health and Human
Services. (n.d.) Home Visiting Evidence of Effectiveness. Retrieved from http://homvee.acf.hhs.gov/
Weiss, H. W., & Klein, L .G. (2006). Changing the conversation about home visiting: Scaling up with quality. Cambridge, MA: Harvard Family Research Project.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 1 7
Toward Population Impact From Home Visiting
KENNETH A. DODGE
W. BENJAMIN GOODMAN
ROBERT MURPHY
KAREN J. O’DONNELL
JEANNINE M. SATOD uke University
AbstractAlthough some home visiting programs have proven effective with the families they serve, no program has yet demonstrated broader impact on an entire county or state population. This article describes the Durham Connects program, which aims to achieve broad county-level effects by coalescing community agencies to serve early-intervention goals through a Preventive System Of Care and by delivering universal, short-term, postnatal nurse home-visiting services. Evaluation of Durham Connects occurred through a randomized controlled trial of all 4,777 births in Durham, NC, over an 18-month period. The results indicated that, by 6 months old, Durham Connects infants had 18% fewer emergency room visits and 80% fewer overnight stays in the hospital than did control families. A broad effect is achievable if a program attends to the challenges of community partnership, universal reach and assessment, rigorous evaluation, and strategies for sustaining funding.
We are entering an era of home visiting to improve the healthy development of infants. and thus the use of home visiting as a service delivery strategy has become a model of how science can inform practice and policy (Haskins, Paxson, & Brooks-Gunn, 2009). Empirical support for a handful of programs (e.g., Nurse-Family
Partnership, Healthy Families America, Early Head Start Home Visiting, Family Check-Up) is strong. When tested in small randomized controlled trials with volunteer families, these programs led to positive outcomes for the families served. Buoyed by this evidence base, and authorized by the Patient Protection and Affordable Care Act of 2010, the Maternal, Infant, and Early Childhood Home Visiting program (MIECHV; Supplee, Harwood, Margie, & Meyer, this issue, p. 45) supports dissemination of these home-visiting programs to communities across the United States. This is a story of the translation of science to practice following the steps advocated in the early 1990s by the Institute of Medicine (Mrazek & Haggerty, 1994): Basic science should inspire interventions; promising interventions should be tested for efficacy in small trials; successful interventions should be brought to communities to test for effectiveness in real-world contexts; and effective programs should be broadly “scaled up” to achieve a measurable effect on public health outcomes. However, this final step, demonstration of positive effects on the population of an entire community, has never been realized for any home visiting program. Our goal in this article is to catalyze the field toward achieving broader public health effects by describing a decade-long effort in Durham, NC, to develop and evaluate a universal, short-term, nurse home visiting initiative called Durham Connects.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

1 8 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Community Partnership
Ecological models of child maltreatment implicate community characteristics, such as lack of
accessible resources to support parenting (Belsky, 1993), in leading some families to become socially isolated or disadvantaged and, thus, at risk for child maltreatment. An objective in the current federal legislation is that home visitors in federally funded programs should improve “coordination with and referrals for other community resources and supports” (Administration for Children and Families, 2010). Home visitors explicitly try to help parents navigate and take advantage of an array of community resources, such as quality child care, mental health services, and social supports. However, home visiting programs rarely attempt to improve the quality or expand the capacity of a community’s resources. Under these circumstances, if a program expands to serve an entire community, then the relatively small fixed supply of community resources and support services may reduce the program’s observed benefits compared with its performance in the initial smaller trials.
The Durham Connects program has spent a decade growing a Preventive System Of Care (PSOC; Tolan & Dodge, 2005) of community services by gaining the support of virtually all community agencies, providers, and volunteer groups in Durham County, NC. The PSOC is modeled after the System Of Care concept in child mental health treatment (Stroul & Friedman, 1996), which focuses on the needs of the child, includes all relevant members of the child’s ecology, and “wraps” services around the child. Durham Connects follows this model but implements it preventively. Durham agency leaders have met monthly since 2002 to develop this approach, and all have signed a memorandum of agreement to follow the PSOC model of family-centric care and to direct resources, including an annual allocation from county commissioners, toward prevention.
Durham Connects maintains a computer-updated network of more than 400 community agencies that serve the families of newborns.This resource benefits providers communitywide, including Durham Connects home visitors, as they assess and link families with individually needed resources. Tracking families’ needs and service use over time helps to identify gaps in resources and facilitate community efforts to fill them. Community agencies actually deliver more and higher quality services through this system because less time is spent in “case-finding” and “weeding out” inappropriate referrals.
of how the program is being implemented typically declines. Second, dissemination of a “model” program in a new community usually occurs with insufficient slots to serve all eligible families. An unanticipated result is that programs may cherry-pick the families that are easiest to serve. For example, programs may favor parents who are readily able to participate over those perceived as more difficult because of the challenges of engagement, retention, and consistent participation. In effect, the program may serve families that require fewer (or even no) resources to achieve positive outcomes. Third, if the community’s resources and support services are not increased, then the benefit for served families might be offset by a cost to nonserved families. This offset might operate if served families are tutored by a home visitor to gain a competitive advantage for fixed-sum services. If served families take up available community resources, then nonserved families actually lose resources and suffer worse outcomes. Thus, when home visiting programs expand to serve an entire community, the quality and quantity of community resources that are devoted to families of newborn infants also need to increase.
Although our analysis may seem pessi-mistic, we believe that home visiting can be scaled up and sustained in an entire com-munity, if the challenges of community partnership, universal reach and assessment, rigorous evaluation, and achieving sustain-able funding are overcome. We address each of these issues in turn.
Although we count ourselves fully in accord with the supporters, providers, and researchers of home visiting, we note three sobering facts about the field: (a) No program has yet changed an entire community’s rate of an important outcome, such as child maltreatment or infant mortality; (b) challenges in scaling up suggest that effectiveness will likely be reduced when some programs are disseminated; and (c) current funding levels and strategies for scaling up program models in the federal MIECHV law are insufficient to achieve broader population-level change. To become sustainable in this policy-making climate, we believe that the home visiting movement will need to demonstrate that a program changes a population of young children across an entire community. These are the goals of Durham Connects.
Although the total MIECHV funding is substantial, funds are allocated to single communities in relatively small amounts, so that no community is likely to achieve a discernible effect on all its families, or even a subpopulation such as all infants born in poverty. One might assume that, even when broad change is not demonstrated, home visiting programs are having a favorable effect on the individual families that they serve. We see reasons for caution. First, programs typically suffer up to a 50% reduction in quality and effect when they are disseminated more widely (Welsh, Sullivan, & Olds, 2010), a phenomenon called the scale-up penalty. When programs have passed beyond the initial evaluation stage and are being disseminated more broadly, monitoring
From left to right: Durham Connects nurse Rosalia Monaco, Lorduy’s father, Lorduy’s husband, mom Liz Lorduy, and baby Lisabeth Lorduy.
Ph
ot
o: J
ea
nn
in
e S
at
o
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 1 9
Nurses assess family risk and needs in a nondirective manner, using a high-inference approach in which the nurses gather infor-mation in multiple ways (e.g., interviews, observations, questionnaires). At the con-clusion of the interview, the nurses use these various sources of information, along with their experience and clinical judgment, to rate relative risk across each of the 12 factors. Each factor is rated on a 4-point scale: a score of 1 (low risk) in a particular area indicates that the family is functioning well with no need for intervention; a score of 2 (moderate risk) indicates some risk that can be resolved ade-quately with nurse-delivered intervention in home; a score of 3 (high risk) indicates more substantial risk that warrants a connection to one or more matched community resources to provide longer term support; a score of 4 (imminent risk), albeit rare, results in immedi-ate emergency intervention. Families assessed as low risk (scored as 1 and 2) receive short-term supportive interventions and require limited nurse time, which means more of the nurse’s time can be reserved for needier families.
During a randomized trial of the Durham Connects program with all 4,777 births in Durham over an 18-month period (described in detail later), 15 families (1%) received a score of “4” on at least one risk factor, indi-cating an emergency that received attention immediately. These emergencies included health crises and material living crises. Nurse home visitors rated 44% of families as having at least 1 risk factor of the 12 meriting a score of 3, indicating substantial risk best served by connection to a community service pro-vider. Substantial risk was most frequently identified in the health care (27%) and house-hold safety and violence (21%) domains,
is, few low-risk families are incorrectly identi-fied as being at high risk, and, conversely, few families who truly are at high risk “fall through the cracks” and fail to be identified as need-ing services.
The Durham Connects Risk Assessment Model
During the course of home visits, Durham Connects nurses use the Family Support Matrix (O’Donnell,
Goodman, Murphy, & Dodge, 2012) to assess and score health and psychosocial risk across four domains and a total of 12 factors that had been identified in empirical research to be linked with healthy child development and risk for maltreatment across multiple ecolog-ical levels:
HEALTH CARE 1. Parent health
2. Infant health and safety
3. Health care plans
PARENTING/CHILD CARE 4. Child care plans
5. Parent–child relationship
6. Management of infant crying
HOUSEHOLD SAFETY AND VIOLENCE 7. Household/material supports
8. Family and community violence
9. History of maltreatment
PARENT MENTAL HEALTH/WELL-BEING 10. Depression/anxiety
11. Substance abuse
12. Emotional support
Universal Reach and Assessment
A n ecological perspective asserts that risk for maltreatment increases from a wide variety of factors that
range from infant characteristics, which make the infant harder to parent, to parent and family characteristics, such as depression, sub-stance abuse, poverty, lack of social support, and intimate partner violence, to community characteristics, such as neighborhood vio-lence and lack of accessible resources (Belsky, 1993; Daro & Dodge, 2009). The most compel-ling lessons for prevention are that the risks for maltreatment are varied and individual. Pre-ventive interventions will be most successful if they identify and target specific risk factors and strengths for an individual family.
The most popular home visiting programs for preventing child maltreatment target fam-ilies on the basis of demographic risk, such as first time, low-income mothers, and engage them intensively for a long period of time at high per-family cost. This approach defines risk narrowly rather than accounting for risk across multiple levels of the child’s ecology. Enrolling families on the basis of demographic risk alone rather than following a system-atic assessment of individual risk means both that not all families at high risk for maltreat-ment will receive services and that some high-functioning families will receive services unnecessarily. Enrolling families solely on the basis of demographic risk may lead to dis-crepancies between families’ needs and the services provided, decreasing overall program effectiveness. Delivering expensive long-term services to families that are headed for pos-itive outcomes even without those services wastes scarce program resources, which could be better used for families with greater need.
Durham Connects was designed to address these limitations by universally engaging all families and assessing maltreatment risk across multiple levels of an infant’s ecol-ogy. Comprehensive, universal assessment offers several strategic advantages that can increase overall program uptake and effect. By offering assessments universally, fami-lies do not perceive participation in Durham Connects as stigmatizing them as “poor” or “risky,” thereby maximizing families’ partici-pation and overall community acceptance and support. A universal approach negates many criticisms of targeted programs, such as con-cerns about stereotyping families or providing costly services to specific subpopulations while ignoring others, thereby maximizing political support and acceptance. Greater compatibility between families’ needs and the services they receive maximizes broader effects on the wider community. Most impor-tant, universal assessment of families’ unique strengths and needs identifies maltreatment risk with high sensitivity and specificity. That
From left to right: Durham Connects social worker Erika Ward, Williams’ niece Jada Williams, mom Shantel Williams, baby Thomas Williams, son Deshawn Williams.
Ph
ot
o: J
ea
nn
in
e S
at
o
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

2 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
of .68, which is considered a high level of reliability (Dodge et al., 2012). Across all home visits, nurses implemented an average of 14 “teachings,” or brief interventions, to each family. Of families receiving these interventions, the most common were about: (a) maternal health (55%); (b) household supports (46%); (c) infant health (40%); and (d) maternal well-being (37%). In telephone contacts 4 weeks after visits were completed, families reported that they had already connected with 61% of all community referrals that had been proposed. Almost every mother indicated that she would recommend the visit to another new mother (99%).
Effect of Durham Connects at 6 Months
Our analysis (Dodge et al., 2012) of in-home interviews and emergency room and hospital records from the smaller subsample of families indicates that Durham Connects produces multiple, statistically significant benefits for family functioning and child health at 6 months old. These benefits include the following:
Increased community connections. Durham Connects-eligible families reported accessing 14% more community resources than did control families.
Improved quality of parenting and child care. Durham Connects families reported more positive parenting behaviors than control families. No differences were found in negative parenting behaviors, knowledge of infant development, or sense of parenting competence. In-home observers rated the parenting quality of Durham Connects mothers as higher than that of control mothers. No difference was found for the likelihood of using out-of-home child care, but when infants were placed in out-of-home child care, the quality of care was higher for Durham Connects families than control families as rated by the North Carolina five-star rating system.
Enhanced mother well-being. Durham Connects mothers were less likely than control families to be rated as having possible clinical anxiety, but no differences were observed for depression or substance use.
Higher home environment quality/safety. In-home observers rated the home environment quality as higher for Durham Connects families than control families.
Fewer infant medical emergencies. Relative to control infants, Durham Connects infants had 18% fewer emergency room visits and 80% fewer overnights in the hospital than did control families.
Benefit–cost analysis. The cost of Durham Connects is about $700 per family in the community. We (Dodge et al., 2012) estimated the benefits in reduced emergency medical care using published rates that
(Kazdin, as reported by Jaffe, 2010). Consis-tent with this new perspective, the Durham Connects program used random assign-ment of every Durham County birth in an ethical way that was acceptable to the com-munity without excluding families on the basis of prior consent. For families assigned to the intervention, this design meant an “intent-to-treat” analysis that evaluated both recruitment and effect. For families assigned to the control group, it meant inclusion without informed consent but with care for confidentiality.
We achieved this solution by randomly assigning families to condition according to the child’s date of birth: For an 18-month period (July 1, 2009, through December 31, 2010), every infant born on an even date (n = 2,327; mean of 8.68 births per date) was assigned to receive intervention, and every infant born on an odd date (n = 2,450; mean of 8.75 births per date) was assigned to a control group to receive “services as usual.” Electronic discharge records provided by both hospitals in Durham County ensured that the entire population of births for the 18-month period was identified and randomized.
Because we wanted to assess family ser-vice receipt and family functioning in greater depth than administrative records could pro-vide, we selected a random, representative subsample of the 4,777 families to participate in a longitudinal study beginning when infants were 6 months old. The study examined mul-tiple outcomes related to Durham Connects program goals and implementation. Using publically available birth records, we ran-domly selected one birth for each day of the Durham Connects randomized trial period for participation in the smaller, more inten-sive study (n = 549 overall; n = 269 Durham Connects-eligible families; n = 280 control group families). To maximize experimental rigor, the study used a double-blind proto-col: Even-birthdate families were recruited without consideration of whether they had consented to receive Durham Connects services, and research assistants had no knowledge of which families received intervention.
Durham Connects Implementation
Of the 2,327 families who gave birth to an infant on an even date, 80% were successfully contacted and enrolled by trained Durham Connects staff members. Of these families, 86% successfully completed the program (69% net completion).
Independent observers rated the quality of program implementation as high. Nurse adherence to the intervention protocol averaged 84%, and nurse reliability in scoring the 12 risk factors averaged a kappa
with risk in the parent mental health/well-being (15%) and parenting/child care (8%) domains occurring less frequently. Another 48% of families received at least one score of 2 (but no scores of 3 or 4), indicating that some risk that could be addressed with short-term nurse intervention. Only 8% of families were rated as functioning well with no identified risk across all 12 factors.
Follow-up of these families until the child was 6 months old revealed that the individu-alized risk assessments of Durham Connects reduced overall error rates in predicting later emergency medical care by 39%, com-pared with the error rate if we had depended solely on traditional demographic risk assess-ment (Goodman, Murphy, O’Donnell, Sato, & Dodge, 2012). These findings suggest that comprehensive individualized assessment of risk results in more accurate identifica-tion of families at risk for maltreatment than does identification by demographic factors alone. We interpret these findings to indicate that ongoing services (including long-term home visiting programs) could be delivered more efficiently if they use individualized assessments.
Rigorous Evaluation in a Community Setting
We implemented and evaluated Durham Connects for all of Dur-ham County using a randomized
controlled trial. An assumption of traditional prevention science is that program evalua-tion designs must make tradeoffs between experimental rigor and their ability to gener-alize to a wider, real-world setting. Current thinking, however, suggests that this trad-eoff may be an unnecessary compromise
Universal screening and support through newborn home visiting is a powerful tool in enhancing public health and family well-being.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/I
va
nJ
ek
ic
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 2 1
programs have the opportunity to track community-level effects on child abuse rates, emergency care utilization, and well-baby visit compliance at lower cost than required by small trials, ironically, because of the greater availability of administrative records.
Evidence-based programs must success-fully scale up with high fidelity if they are to become relevant to other communities.
to procure sustainable funds. Programs may choose to operate as part of an exist-ing nonprofit organization, as a freestanding nonprofit, within a public health depart-ment, or as a service of a public or private health care system. If the program is oper-ating as a nonprofit, funding sources may include private foundations, philanthropists, and corporations, and public funds from fed-eral, state, and local sources. One challenge of operating as part of an existing nonprofit involves the possibility of internal fundrais-ing competition.
Credible impact findings that demon-strate value-added benefits of the program over both the short and long term are extremely important in solidifying the basis for necessary funding. In the case of Durham Connects, The Duke Endowment and the Pew Center on the States generously offered fund-ing for research and development to create and evaluate a program to reduce child mal-treatment in Durham. We are well on our way to achieving that goal. Sustaining the pro-gram in the long term, however, will require a broader variety of community investors. The program will need to meet the individual goals of these new investors as well.
Achieving recognition as an evidence-based program is crucial to obtaining this support. This step may include a randomized controlled trial with positive effect findings. We are continuing to follow the infants in our randomized controlled trial with evaluations through 5 years old. Ironically, universal
indicate a local average of $423 per emergency outpatient visit and $3,722 per hospital night. We estimate a benefit–cost ratio of 3.02, meaning that every $1 spent on the Durham Connects program saved $3.02 in costs for infant emergency medical care by age 6 months. For a community of the size of Durham, NC, with an average of 3,187 resident births per year,, an investment of $2,230,900 for the Durham Connects program would yield a communitywide emergency health care cost savings of $6,737,318 per year.
Models for Sustaining Funding
Universal screening and support through newborn home visiting is a powerful tool in enhancing public
health and family well-being. Sustaining and disseminating a universal home visiting program like Durham Connects requires strategic planning from the outset. The program must provide evidence of effectiveness, which we have provided here. Moreover, it must identify a clear, compelling rationale for why a community should invest in universal home visiting. The potential for sustainability will depend on the size and composition of a community and its newborns, its economic conditions, and the availability and interest in public and private investment in the community.
Understanding how a newborn home visiting program can complement and support a community’s goals helps position programs such as Durham Connects strategically to achieve long-term sustainability. For instance, if a community’s foremost goal is to improve infant mortality, a universal home visiting program could choose to capture this statistic and track it as an outcome. Other outcomes of interest to a community might include increased breastfeeding, improved parenting skills, proper utilization of health care providers, better pregnancy spacing and access to birth control, and other indicators related to community health and prosperity.
The costs of a universal program will vary widely according to population and birthrate, nurse salaries, and overhead costs. A small urban community, such as Durham, NC, can expect a resident birth rate of approximately 3,200 births per year and an ultimate par-ticipation rate of 70% of eligible parents. To implement the Durham Connects model with high fidelity, nurses make no more than two visits per day, with an average of six to eight visits per week. Based on a local nurse salary averaging $60,000, along with support staff and administrative expenses, the annual cost of a universal nurse home-visiting program in Durham, NC, has been about $700 per family or $2,240,000 per year.
Identifying the appropriate organizational model for the program may affect its ability
Preventive interventions will be most successful if they identify and target specific risk factors and strengths for an individual family.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/c
oo
lb
ro
th
er
sh
ar
p
Learn More
Durham Connects
www.durhamconnects.orgBackground on community approaches to home-visiting and prevention can be found at:
Daro, D., & Dodge, K. A. (2009). Creating community responsibility for child protection: Possibilities and challenges. The Future of Children, 19, 67–97.
Dodge, K. A., & Coleman, D. L. (Eds.) (2009). Preventing child maltreatment: Community approaches. New York, NY: Guilford Press.
Rosanbalm, K. D., Dodge, K. A., Murphy, R., O’Donnell, K., Christopoulos, C., Williams Gibb, S., Appleyard, K., & Daro, D. (2010). Evaluation of a collaborative community-based child maltreatment prevention initiative. Protecting Children, 25(4), 8–23.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

2 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
at Duke University and director of the Durham Connects impact evaluation. His research interests focus broadly on the influence of stress and support on the quality of parent–child relationships and child development.
Robert Murphy, PhD, is executive director of the Center for Child and Family Health, a consor-tium of Duke University, the University of North Carolina at Chapel Hill, and North Carolina Central University, dedicated to research, train-ing, and intervention related to child traumatic stress. He is an associate professor in the Duke School of Medicine Department of Psychiatry, and his research focuses on prevention, intervention, and dissemination of best practices for child mal-treatment and traumatic stress.
Karen J. O’Donnell, PhD, is the director of Global Initiatives at the Center for Child and Family Health, a consortium of Duke University, University of North Carolina, and North Carolina Central University. Her background is research and clinical work with early childhood and parent–child relationships both domestically and internationally.
Jeannine M. Sato, MA, is director of Durham Connects. She is responsible for the program’s public outreach, health provider, and community agency collaboration. She currently serves on the North Carolina Early Learning Challenge Grant leadership team for dissemination of the Durham Connects model to rural counties across North Carolina. She previously served on the local Partnership for Children allocations committee to determine early childhood spending. Sato also works with nonprofits, the North Carolina Justice Center, and North Carolina MomsRising to advocate for improved public policy related to child and family issues at the state and national level.
Acknowledgments
The authors thank The Duke Endowment and the Pew Center on the States for financial support. Those organizations approved the design of the study but had no responsibility for the conduct, collection, management, analysis, and interpretation of the data; or the preparation, review, and approval of the manuscript. The authors acknowledge the support of National Institutes of Health Grants K05DA15226, P30DA023026, and R01HD069981.
research, documentation of quality, and evidence-based practices. Until universal home visiting is widely accepted as a valuable health and social support, the quest for sustainability must, inevitably, be diverse and proactive.
Conclusion
We believe that infant home visiting programs can achieve a positive effect on the population
of children and families and high rates of return on investment when planned and implemented at the community level. Durham Connects is one empirically validated model of cost-beneficial home visiting.
However, will communities invest in home visiting?
Communitywide partnerships in a PSOC of the sort described in this article are a requirement for success. Despite a high rate of return on investment for these programs, federal funding will remain necessary, particularly because the startup cost may be prohibitive for many communities. Toward this goal, we believe that MIECHV funds should be invested more creatively to support innovation in home visiting, including strengthening the current, but discretionary, opportunity to support promising practices. This innovation can co-occur with continuing support for existing programs that have demonstrated efficacy in randomized controlled trials but have not (yet) demonstrated a communitywide effect. Finally, all federally funded programs should continue to be evaluated during dissemination to determine whether they achieve an effect on the broader populations involved. A
Kenneth A. Dodge, PhD, , is the William McDougall Professor of Public Policy at Duke University. He directs the Duke Center for Child and Family Policy, which is devoted to discovering solutions to problems facing children and families in contemporary society. His works spans from the basic science of early child development to the creation of innovative prevention programs such as Durham Connects and Fast Track, to public policy engagement.
W. Benjamin Goodman, PhD, is a research scientist at the Center for Child and Family Policy
We are now disseminating the Durham Connects model in four rural counties in North Carolina. With funding from the fed-eral Race to the Top Early Learning Challenge Grant to the state of North Carolina, the Durham Connects model is an integrated component of a “Transformation Zone” designed to develop a viable early childhood infrastructure, local capacity, and effective early childhood services, including univer-sal screening through nurse home visits with families of newborns.
When a community sustainability model includes private foundations or philanthropists, a program must align with the focus areas of those foundations. Home visiting models may fit with goals of child abuse prevention, health care integration, risk assessment and screening, community coordination of services, child and maternal health, or other goals pertaining to community health and well-being. Writing a grant proposal is often a time-consuming process that requires data collection and reporting capacity specific to the grant’s goals. Foundation grant cycles vary but are typically of time-limited duration and sometimes restricted to new projects. Because a program must continually search and apply for grants from funders with different application cycles and expectations for reporting, it is difficult for a large program to be sustained solely through private grants.
Universal newborn home visiting programs may be eligible for public funds; for example, via Medicaid reimbursement for the mother’s visit, infant’s visit, or both, depending on patient eligibility. However, Medicaid reimbursement rates are typically not substantial enough to cover the entire cost of a visit. Other opportunities for public funding may be available from state or local governments. These opportunities may include health care funds, infant mortality reduction programs, school readiness programs, maternal health and pregnancy prevention programs, depression and mental health screening, or interconception health programs.
In summary, universal newborn home visiting programs must strategically plan for long-term sustainability from the outset. Program leaders must understand the goals of potential funders and address how the program will achieve these goals through
References
Administration For Children And Families.
(2010). Linkages and referrals. Retrieved from http://homvee.acf.hhs.gov/document.aspx?rid=2&sid=28
Belsky, J. (1993). The etiology of child maltreatment: A developmental ecological analysis. Psychological Bulletin, 114, 413–434.
Daro, D., & Dodge, K. A. (2009). Creating community responsibility for child protection: Possibilities and challenges. Future of Children, 19, 67–93.
Dodge, K. A., Goodman, W. B., Murphy, R. A.,
O’Donnell, K., Sato, J., & Guptil, S. (2012). Implementation and randomized controlled trial evaluation of universal postnatal nurse home-visiting. Manuscript submitted for publication.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 2 3
Goodman, W. B., Murphy, R. A., O’Donnell, K.,
Sato, J., & Dodge, K. A. (2012). Individualized risk assessments through universal home visiting as a predictor of later child health outcomes. Manuscript submitted for publication.
Haskins, R., Paxson, C., & Brooks-Gunn, J. (2009). Social science rising: A tale of evidence shaping public policy [The Future of Children Policy Brief, Fall 2009]. Princeton, NJ: Princeton University.
Jaffe, E. (2010, September). Alan Kazdin: Reconsidering clinical psychology. APS Observer, 23(7), 27
Mrazek, P. J., & Haggerty, R. J. (Eds.). (1994).
Reducing risks for mental disorders: Frontiers for preventive intervention research. National Research Council and Institute of Medicine of the National Academies. Washington, DC: The National Academies Press
O’Donnell, K., Goodman, W. B., Murphy, R., &
Dodge, K. A. (2012). Assessment of family risk for infant maltreatment. Unpublished manual, Duke University, Durham, NC.
Stroul, B., & Friedman, R. (1996). The system of care concept and philosophy. In B. Stroul (Ed.), Children’s mental health: Creating systems of care in a changing society (pp. 3–22). Baltimore, MD: Brookes.
Supplee, L. H., Harwood, R. L., Margie, N. G.,
& Meyer, A. (2013). New opportunities and directions in home visiting research and evaluation. Zero to Three, 33(3), 45–50.
Tolan, P., & Dodge, K. A. (2005). Children’s mental health as a primary care and concern: A system for comprehensive support and service. American Psychologist, 60, 601–614.
Welsh, B. C., Sullivan, C. J., & Olds, D. L. (2010). When early crime prevention goes to scale: A new look at the evidence. Prevention Science, 11, 115–125.
Developmentally Based DiagnosisZERO TO THREE’s Diagnostic Classificationof Mental Health and DevelopmentalDisorders of Infancy and Early Childhood,Revised (DC: 0–3R) enhances your ability to assess, diagnose, and treat mental healthproblems in infants and toddlers. Mentalhealth professionals, physicians, nurses, earlyinterventionists, early childhood educators,and researchers will find DC: 0-3R to be anindispensable guide to effective evaluationand treatment planning with young childrenand their families.
Order your copy today! Call toll-free (800) 899-4301 or visit www.zerotothree.org/bookstore
Need anInterpreter?Need anInterpreter?
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

2 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Meta-Analyses on Home Visiting
Our experience combined with our review of recent studies and meta-analyses suggested that, although
it has been assumed that mothers who had previous births will both participate less fully and have poorer outcomes from early home-visitation than will first-time mothers, very little research has tested this hypothesis.
Studies of the Nurse-Family Partnership (NFP), a home visiting program that exclusively serves first-time mothers, have contributed to the assumption that these mothers benefit most from home visiting. NFP, however, has never been empirically tested with mothers with multiple children. Dr. John Holmberg, who has worked and published NFP research with David Olds, confirmed that “the NFP program has never
Does Home Visiting Benefit Only First-Time Mothers?
Evidence From Healthy Families Virginia
LEE HUNTINGTONHuntington Associates
Richmond, VA
JOSEPH GALANOCollege of William & Mary
AbstractIt is a common assumption that mothers who have had previous births would participate less fully and have poorer outcomes from early home visitation programs than would first-time mothers. The authors conducted a qualitative and quantitative study to test that assumption by measuring three aspects of participation: time in the program, the number of home visits, and the intensity of services. The study also assessed three outcomes: immunizations, the home environment, and subsequent births. Data from more than 4,000 participants at Healthy Families Virginia sites indicate that mothers who had had previous births participated and benefitted similarly to first-time mothers. These findings suggest a need for future research to better understand the conditions under which home visiting works, and they have policy implications concerning the value of universal home visitation.
been tested with multiparous women” (personal communication, November 9, 2009). Dr. Holmberg stressed that there are many reasons to focus on first-time mothers (e.g., the developmental crisis of pregnancy, ability to impact the first child’s neuropsychological health, and ability to impact the spacing between subsequent children). New mothers may also be receptive to nurses because they have medical training. He indicated that NFP had not examined working with mothers with previous children in depth because NFP was trying to improve their existing program model. Holmberg further indicated that there is a great deal to learn and understand about who benefits from home visiting and under what circumstances. Indeed, it is our goal to add to that body of knowledge by addressing both questions.
Perhaps the most authoritative meta-analysis conducted to date was the 2003 National Review of the Effectiveness of Early T
his article presents the results of a two-phase study, conducted to compare the participation and outcomes of multiparous mothers (those with previous children) in Healthy Families home visitation programs in Virginia, to those of primiparous (first-time) mothers in the same programs. The purpose of these comparisons was to examine the longstanding assumption that multiparous mothers
do not do as well as first-time mothers in home visiting programs. Targeting services on the basis of this untested hypothesis denies services to more than 60% of the American families who deliver each year, solely because they have previous children (Hamilton, Martin, & Ventura, 2011).
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 2 5
The family support worker provides parent education, child development screenings, nutrition counseling, and literacy activities. Virginia sites participate in an accreditation process that provides technical assistance and quality assurance and ensures model fidelity.
Was Number of Previous Births Related to Other Participant Characteristics?
Our initial analyses compared first-time mothers participating in HFV with multiparous mothers participating in HFV in terms of age, risk, race, education, and employment. Among mothers participating in HFV, a complex relationship exists between whether she has previous children, on the one hand, and her age, risk status, race, employment, and education on the other. Multiparous mothers were more likely to be older, have higher risk scores, be African-American, and have completed high school than were first-time mothers. Among the minority of participants who were employed, multiparous mothers were more likely to be employed full-time than part-time or intermittently. Thus, while the multiparous mothers were older, better educated, and had more job stability (for those who were employed), our assessment of their risk using the KFSC indicated that they were at slightly higher risk.
Were Multiparous Mothers at Risk in the Same Ways as First-time Mothers?
The relationship between number of previous births and risk suggested further examination of the relationship between a mother’s number of previous births and the particular risk items assessed by the KFSC.
HFV Participation and Outcomes
The study described in this article used data collected for HFV evaluations from 1999 to 2011 to
examine more thoroughly the participation and outcomes of first-time mothers compared to multiparous mothers.
What Is the Healthy Families Model?
HFV is a part of the national initiative HFA and follows the critical components established by HFA. Communities each identify a target population and referral sources to allow the HFV program to identify the families most in need of services. Each family is screened for risk factors. A Healthy Families assessment worker completes a family needs assessment using the Kempe Family Stress Checklist (KFSC; Carroll, 1978) for all those who screen positive and consent to be assessed. If a family is identified as being at risk of child maltreatment and in need of parenting support services, they are offered the opportunity to participate. Families accepting services are assigned a family support worker who provides home visiting services based on developing a trusting relationship with families and building on family strengths. Services are provided intensely (once a week initially) for the first 6 months and decrease over time using well-defined criteria. Family needs are further assessed and an Individual Family Services Plan (IFSP) is developed. This plan includes coaching in problem solving, developing effective parenting techniques and home management skills, ensuring proper immunizations for the child, and linking the family with appropriate community resources.
Childhood Home Visitation for Preventing Violence conducted by the Task Force on Community Preventive Services (Hahn et al., 2003). The Task Force identified 22 studies (representing 27 programs) that evaluated effects of early childhood home visitation on child maltreatment. Compared with control families, families that received home visiting experienced approximately 40% less child abuse and neglect. Because of this potential for prevention, the Task Force recommended implementation of early childhood visitation nationally. That review did not suggest that home visitation be provided only to first-time mothers.
In 2011 the Home Visiting Evidence of Effectiveness (HomVEE) review conducted a broad search of home visiting models and identified seven programs (Early Head-Start Home Visiting, Family Check-Up, Healthy Families America [HFA], Healthy Steps, Home Instruction of Parents of Preschool Youngsters, NFP, and Parents as Teachers) that received high or moderate ratings of effectiveness (Del Grosso, Kleinman, Esposito, Sama, Martin, & Paulsell, 2011). The HomVEE did not examine the number of previous children a mother had as a factor in program effectiveness. Thus, the HomVEE, combined with the previous reviews and meta-analyses, indicated that the commonly held assumption that multiparous mothers will not benefit from home visitation has not been supported by research.
Statewide Evaluation of Healthy Families Virginia
R esults attained by home visitation programs in Virginia during the past 20 years have also challenged
the assumption that multiparous mothers do not benefit from home visiting. A 6-year randomized-control study of the Hampton Healthy Start program (Galano & Huntington, 1999) indicated that—although there were significant differences between the intervention and control groups on measures of infant health, parent–child interaction, and the home environment—the mothers’ number of previous children was never a factor affecting these outcomes. In other words, first-time mothers and multiparous mothers, as well as their children, received similar benefits from participation in the program. In 10 years of Healthy Families Virginia (HFV) evaluations conducted since the Hampton Healthy Start study, both first-time and multiparous mothers have attained high levels of success in the program as measured by children’s immunization rates, developmentally appropriate home environments, and reductions in closely-spaced pregnancies (Galano & Huntington, 2012).
Compared with control families, families that received home visiting experienced approximately 40% less child abuse and neglect.
Ph
ot
o: H
ea
lt
hy
F
am
il
ie
s R
ap
pa
ha
nn
oc
k A
re
a
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

2 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
of the Environment (HOME); Caldwell & Bradley, 1984). HOME, a standardized instrument that has been validated and is widely used, assesses six aspects of the child’s home environment that are known to foster cognitive development.
As was the case with immunizations, a regression analysis we conducted on HOME outcomes for HFV participants indicated that a mother’s number of previous births was not a significant predictor of the family’s HOME score, either at time of enrollment or when the child was at least 12 months old. Time in the program and intensity of home visits positively predicted a family’s HOME scores. All mothers, both first-time and multiparous, showed a statistically significant increase in HOME scores between initial enrollment and assessment when the child was 12 months old. Moreover, there was no significant difference between the HOME scores of first-time and multiparous mothers at either measurement point.
SUBSEQUENT BIRTHS: An important achievement of the HFV program is the low 4.5% rate of subsequent births within 24 months found in the high-risk population served. Nationally, almost 25% of adolescent mothers give birth to another child less than 24 months after the birth of their first child (Schelar, Franzetta, & Manlove, 2008). It was important for our analysis to note that first-time and multiparous mothers did not differ in their subsequent birth rates. HFV participants, both with and without previous children, have delayed subsequent births well beyond the national average.
Conclusions From Our Statistical Analysis
Overall, our statistical analysis failed to find convincing evidence in support of the assumption that multiparous mothers do not participate as well as first-time mothers in the HFV home visitation program. Although older and at higher risk than the first-time mothers, multiparous mothers in the HFV program participated similarly to their primiparous peers when risk and demographic characteristics were controlled for.
The results also indicated that the out-comes were most strongly and consistently predicted by a combination of participation and demographic variables. The strongest predictors of participant outcomes were the variables related to participation. Mothers who stayed in the program longer and those who had more intensive services had bet-ter immunization rates for their children and higher HOME scores.
The pattern of relationships of other demographics to outcomes was much weaker when participation was controlled for. White
Was Whether Mothers Had Previous Children Related to Other Participant Characteristics and Program Participation?
For home visiting programs nationwide, attracting and keeping participants is a significant concern. The recent report to Congress on Preventing Mental, Emotional, and Behavioral Disorders, by the National Research Council and the Institute of Medicine (2009), indicated that engagement and retention of high-risk families in effective programs is a major public health challenge.
Our analysis indicated that among HFV participants, whether a mother had previous children or not was not correlated with her participation (as measured by time in the program, number of home visits, or intensity of services), once the effects of the mother’s demographic and risk characteristics were controlled for. Mothers’ participation, however, was correlated with her risk score, age, race, employment, and education to varying degrees. Overall, the results of these analyses supported the conclusion that multiparous mothers participate similarly to first-time mothers in the HFV program once differences in their risk status are taken into account. Put another way, two mothers who differed only in whether they were first-time mothers or not would be equally likely to participate and engage in the HFV program.
How Do Participant Outcomes Relate to the Mother’s Previous Number of Births and Other Characteristics?
We examined three outcome indicators in this study: immunizations, the home environment, and subsequent births.
IMMUNIZATIONS: HFV tracks comple-tion of the 16 immunizations recommended by the American Academy of Pediatrics before the child is 5 years old. HFV’s objec-tive is that 80% of participating children will receive 100% of their expected immu-nizations. Among children of first-time mothers, 85.8% completed all the immu-nizations recommended by the American Academy of Pediatrics and 86.4% of children of multiparous mothers completed these immunizations, a difference that was not sta-tistically significant.
Moreover, a regression analysis we conducted indicated that a mother’s partici-pation (as measured by time in the program, number of home visits, and intensity of ser-vices) predicted her child’s completion of immunizations, but her demographic char-acteristics did not. In particular, an HFV mother’s previous number of births did not predict her child’s immunization completion.
HOME ENVIRONMENT: The second outcome we examined was the parents’ score on the Home Observation for Measurement
When they enrolled in HFV, multiparous mothers had higher risk scores for history of maltreatment, substance abuse, mental health, criminal history, child protective services involvement, coping skills, stressors and concerns, and punitive discipline. It is, however, important to note that the KFSC risk factor scores were not universally more negative for the multiparous mothers. In fact, they did not differ on 3 of the 10 scales, and the scale on which the multiparous mothers had better scores, expectations of the infant, is very important in predicting a mothers’ risk of abusing or neglecting her baby. Moreover, expectations of the infant is one area that is likely to be tempered by experience with previous children because such mothers might be more likely to have more realistic expectations of their children’s behavior and development.
These results explain why prevention programs might conclude that it would be more expedient to invest scarce resources in younger first-time mothers with fewer previously accrued risks. This conclusion probably motivated offering the program prenatally to first-time mothers, as the NFP model has done (Olds, 1980). In order to further investigate whether this is actually a useful or valid basis on which to target families, we examined the relationships between whether mothers had previous children or not, their program participation, and their outcomes.
Families accepting services are assigned a family support worker who provides home visiting services based on developing a trusting relationship with families and building on family strengths.
Ph
ot
o: C
ou
rt
es
y o
f H
ea
lt
hy
F
am
il
ie
s V
ir
gi
ni
a
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 2 7
caseload from 1 to 1.5 to take into account the challenges of working with more children (e.g., arranging child care and transportation) would also help. HFV program managers also felt that it would be useful to have curriculum resources tailored specifically to families with multiple children.
Because multi-child families tend to be socially isolated and often would bene-fit from peer interaction, the HFV program managers also recommended more opportu-nities for social interaction among parents, such as support groups and play groups. In addition, the HFV program managers felt that the capability to make more referrals to community services—especially when depression, substance abuse, or domestic violence is detected—would improve partici-pant retention and outcomes. Unfortunately, statewide funding cuts have reduced these critical community services, and linking fam-ilies to treatment is very challenging. A big wish among the HFV program managers was restoration of funding cuts. After 8 years of stable funding, HFV’s funds from the Virginia General Assembly were cut a total of 50% across the last 3 years.
Key Conclusions
Overall, our discussions with HFV pro-gram managers provided new insights into the challenges entailed in providing home visitation services for multi-child families. All the program managers concurred that serving these families posed additional chal-lenges, most of which were exacerbated in recent years by the economic downturn. They emphasized that the IFSP, which incorporates each family’s specific needs and strengths
The IFSP is the Healthy Families mecha-nism for tailoring services to the needs of the individual family (for both single child and multi-child families). Managers made the point that “multiparous mothers are not a unified block. Some are set in their ways and others are eager and open.” “Matching” was the most often cited program adaptation—making sure that characteristics of the family support worker suited the participant. In gen-eral, multiparous mothers were matched with more experienced and more organized fam-ily support workers because of the additional challenges associated with these families.
Behavioral challenges include the possi-bility that home visits could be sidetracked by older siblings (not the target child) with more serious behavioral issues. The manag-ers stated, however, that these instances also provide opportunities for experienced family support workers to model appropriate disci-plinary skills.
Finally, many managers and family support workers felt that it was their moral and professional obligation to reach out to and serve the most challenging children and families. Limiting eligibility to first-time mothers restricted their ability to do so.
Managers’ Accommodations to Better Serve Multi-Child Families
The HFV program managers we spoke with said that more flexibility around the number of home visits would be useful—especially HFV’s requirement of 3–4 visits per month for the first 6 months, which is too inflexible for multi-child families. Increasing the relative weight assigned to multi-child cases in a family support worker’s
participants did better than either African-American or Hispanic participants on the first HOME administered, but not on the follow- up. Participants with at least high school education did better on the follow-up adminis-tration of the HOME, but not on the first.
This combination of results—no predictive power for number of previous births, comparable outcomes for first-time mothers and multiparous mothers on all measures, and stronger prediction of outcomes by participation and other demographic variables—suggests that it is neither appropriate nor useful to exclude mothers from participation in Healthy Families home visitation services on the basis of whether or not they have had previous children.
Listening to Program Managers
Statistical analyses of the type we conducted are a powerful way to reveal patterns in outcomes, but they do not
explain why these results occurred. In order to begin exploring the “black box” of our sta-tistical findings, we convened a meeting with the HFV program managers. At the meet-ing we talked with the managers about their experiences and challenges in serving fami-lies with multiple children, the rationale for serving them, and the accommodations or adaptations that the programs had made to engage and retain these families.
The Challenges of Serving Multi-Child Families
By far the best insight the managers offered during the meeting was: “All the things that are challenging and stressful about parenting are made more so by having multiple children.” For example, connecting multi-child families to services such as WIC complicates transportation and logistical needs, such as for additional car seats.
Child care was especially a problem for multi-child families. There were too few child care services and too few subsidies for everyone in the population, which impacted multi-child families even more than single-child families. The families served by HFV frequently are very low-income and sometimes homeless. The presence of multiple children increases the complications faced by these families. In addition, the children in these families sometimes have separate birth fathers, which makes collection of financial support more difficult.
Program Adaptations to Serve Multi-Child Families
HFV program managers that we met with expressed strong opinions on four topics: the IFSP, matching participants with family support workers, behavioral challenges, and the moral imperative of serving all families.
For home visiting programs nationwide, attracting and keeping participants is a significant concern.
Ph
ot
o: H
ea
lt
hy
F
am
il
ie
s R
ap
pa
ha
nn
oc
k A
re
a
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

2 8 Z e r o t o T h r e e J a n u a r y 2 0 1 3
has examined intervention for depressed participants in home visiting and has shown significant improvements in depressive symptoms. HFV can contribute to this research in the future by examining differential effectiveness of the intervention for first-time compared to multiparous mothers.
With sufficient funding, HFV could enable communities to serve both multiparous and first-time mothers so that a randomized experiment could be conducted to learn more about who should be targeted for home visiting services.
Policy Implications of These Findings
W e believe that communities should consider the needs of all new families and not just first-
time mothers. Forty percent of the mothers who deliver each year (Hamilton et al., 2011) are first-time mothers, so not serving fam-ilies with multiple children means that we withhold services from 60% of America’s families with infants each year. Deborah Daro, a nationally recognized leader in the field of child abuse and neglect prevention, had a vision that HFA home visiting would be developed as a universal intervention (Daro & Dodge, 2010). Indeed that was the dream of the Hampton Healthy Families Partnership, a program that has contributed substantially to this research and a program with which we have worked for 20 years (Galano et al., 2001). The “Partnership” title was selected spe-cifically for the Hampton program to allow widely used and well-accepted institutions in the community, such as libraries and hos-pitals, to offer new services (e.g., parenting classes, Lamaze, and Welcome Baby Visits) to meet the needs of, and appeal to, a diverse cross-section of the community and to garner widespread public support for the initiative.
We further believe that Deborah Daro’s dream and the Partnership’s vision of intensive, targeted, home visitation services within the larger context of universal services should continue to motivate progress in home visiting. Such a model minimizes stigma and maximizes appeal to all citizens, much as has occurred in Europe (Kamerman & Kahn, 1993). Most European countries provide all families with voluntary service of at least one or two home visits after the birth of a child, and several countries offer more extensive services. These programs have existed since at least the end of World War II, when public health issues like high infant mortality, epidemics, and access to clean water were the driving concerns. Over time, the programs grew to include more social and health goals, focusing on the optimum development of the young child. In Europe, Kamerman and Kahn explained, “Family-focused goals have
of participants’ follow-through on refer-rals and receipt of services would be useful in determining whether differences exist between first-time and multiparous mothers.
Another point the HFV program managers emphasized was the importance of matching family service workers and participants on the basis of the family service worker’s experience. The managers felt that multi-child families were better served by the more experienced family service workers. This hypothesis could be initially explored statistically at low cost by dividing families in the existing HFV data pool into those receiving services from “low-experience” and “high-experience” family service workers and then examining the relationship between the worker’s level of experience and families’ participation and outcomes. If the initial statistical analysis supported the program managers’ belief, it would strengthen the case for testing this possibility in a more expensive randomized controlled experiment.
Another potential direction for future research would be to further examine the mental health and risk status of multiparous mothers. Multiparous mothers participating in HFV were found to be older and at higher risk, particularly on the “Mental Health, Substance Abuse, and Domestic Violence” item of the KFSC (Carroll, 1978). HFV recently began a pilot project screening participants for depression using the Edinburgh Perinatal Depression Scale (Cox, Holden, & Sagovsky, 1987) . Data from this pilot could be used to examine potential differences between the first-time and multiparous mothers, and whether these differences affect either participation or outcomes. In addition, recent research by Ammerman et al. (2009)
into a service plan, provides a unique way to approach each family. The program managers also emphasized that because of the added complexity these families exhibit in terms of needs, scheduling, and time management, only the more experienced family support workers should be matched with multi-child families. An additional benefit of this match-ing is that less experienced family support workers were able to learn about the devel-opmental progression within families by initially serving first-time mothers from birth onward before being required to work with children at multiple developmental stages. Furthermore, program managers and family support workers felt strongly that it was their moral and professional obligation to reach out to the most challenging families and all their children.
The combined results of our statistical analyses and discussions with HFV program managers indicated that, despite assumptions to the contrary, multiparous mothers are able to overcome the additional challenges they face. They can and do engage similarly to first-time mothers in home visiting. Most important, they achieve similar outcomes.
Future Research
The results of this study suggest sev-eral areas of future research. The HFV program managers that we spoke with
emphasized that serving multi-child fam-ilies required more resources and effort. It is worth examining whether family sup-port workers make more outside referrals for multi-child families compared to first-time mothers, and whether the types of referrals or services to which participants were referred differ between the two groups. Examination
An important achievement of the Healthy Families Virginia program is the low 4.5% rate of subsequent births within 24 months found in the high-risk population served.
Ph
ot
o: H
ea
lt
hy
F
am
il
ie
s R
ap
pa
ha
nn
oc
k A
re
a
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 2 9
Thomas Ashley Graves Jr. Award for Sustained Excellence in Teaching. Dr. Galano has worked at the local, state, and national levels to prevent child abuse and neglect. Since 1997, he has worked with Prevent Child Abuse Virginia to develop Virginia’s statewide child abuse prevention initiative, Healthy Families Virginia (HFV). He is HFV’s program evaluator and serves on HFV’s Advisory Council. Since 1992 he has been a member of the Healthy Families America (HFA) Research Practice Network. In 2007 he edited The Healthy Families American Initiative: Integrating Research, Theory, and Practice, published by Haworth Press. He serves on two national-level advisory councils: Healthy Families America Research Practice Policy Council (2011), and the Home Visiting Research Network (established by The Health Services Research Administration, 2012).
Acknowledgment
This research was supported by The Pew Center on the States. The views expressed are those of the authors and do not necessarily reflect the views of The Pew Center on the States or the Pew Charitable Trust. The authors are grateful for the support they received in the preparation of this report from Lee Kirkpatrick, PhD, and Robert Reid, as well as undergraduate research assistants: Brittany Hale, Victoria Haynes, Aylin Kaya, and Walker Keenan. The content of this report does not reflect the views or opinions of the College of William and Mary, but rather those of its authors. For additional information about the statewide evaluation or the Healthy Families Virginia initiative please contact Joseph Galano ([email protected]), Lee Huntington ([email protected]), or Johanna Schuchert ([email protected]).
psycho-social immunization against child abuse and neglect. Given political and economic realities in the United States today, it is unlikely that Deborah Daro’s dream for more universal home visiting will be realized. Nonetheless, it would behoove us as a nation to begin a serious conversation about the human and health costs of limiting access to services on the basis of untested assumptions about which families would benefit. A
Lee Huntington, PhD, is president of Huntington Associates in Richmond, Virginia. Dr. Huntington received his doctorate in psychology and worked in research positions at Evanston Hospital in Evanston, Illinois, and The Mailman Center for Child Development at the University of Miami. He has evaluated Healthy Families programs since 1992, has been a member of the HFA Research Network, the Research/Practice Council, and the Healthy Families America Credentialing Panel. He was one of the co-developers of the Program Information Management System (PIMS). He currently works with Healthy Families Virginia in the 14th year of developing and implementing a statewide evaluation system and providing training and technical assistance to individual sites.
Joseph Galano, PhD, is a professor emeritus of psychology at the College of William and Mary. Dr. Galano was awarded Fellow status in the Society for Community Research and Action (APA Division 27). In recognition of his career accomplishments, the American Psychological Association honored him with the 1996 Distinguished Contribution to Practice in Community Psychology award. In 2010 the College of William and Mary awarded him the
increasingly emerged as of equal importance to child health goals; this is most often reflected in more attention to parent education and referral to needed services” (p. 43).
Especially in the current environment of budget cuts and limited funding for social services, choosing which families receive services is a vexing, complex issue, one that deserves further empirical research to guide citizens, practitioners, and policymakers as they attempt to allocate these scarce resources while still serving the greater human good. A study conducted by the World Health Organization on the Family Nurse Partnership (knows as Nurse-Family Partnership in the U.S.) home visiting program in England concludes that
Targeting first-time mothers would miss 71 per cent of poor families who maltreat their children and targeting first-time mothers would miss 40 per cent of young, single moth-ers with more than one child who are suspected of maltreatment. So we are missing the target (Staines, 2009, p. 8).
The head of World Health Organization’s Collaborating Center for Child Care and Protection, Kevin Browne, suggested replac-ing the Family Nurse Partnership with “a system of universal health visitor coverage to detect and prevent child abuse” (Staines, 2009, p. 8).
Not too long ago, people accepted the inevitability of polio, smallpox, and malaria, but because researchers had a dream about universal vaccinations, these diseases no longer pose the same degree of threat to our world. Home visiting is a kind of
References
Ammerman, R. T., Putnam, F. W., Mekibib, A.,
Chen, L., Holleb, L. J., Stevens, J., Short, J. A.,
& Van Ginkel, J. B. (2009). Changes in depressive symptoms in first time mothers in home visitation. Child Abuse and Neglect, 33, 127–138.
Caldwell, B. M., & Bradley, R. H. (1984). Home Observation for Measurement of the Environment administration manual (rev. ed.). Little Rock, AK: Home Inventory.
Carroll, C. A. (1978). The social worker’s evaluation. In B. D. Schmitt (Ed.), The child protection team handbook (pp. 83–108). New York, NY: Garland STM Press.
Cox J. L., Holden J. M., & Sagovsky, R.
(1987) Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150: 782–786.
Daro, D., & Dodge, K. (2010). Strengthening home-visiting intervention policy: Expanding reach, building knowledge. In R. Haskins & W. S. Barnett. (Eds), New directions for America’s preschool policies. Washington, DC: NIERR and Brookings, 79–86.
Del Grosso, P., Kleinman, R., Esposito, A. M.,
Sama Martin, E., & Paulsell, D. (2011). Assessing the evidence of effectiveness of home visiting program models implemented in tribal communities. Office of Planning, Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services. Washington, DC.
Galano, J., Credle, W., Perry, D., Berg, S.,
Huntington, L., & Stief, E.(2001). Developing and sustaining a successful community prevention initiative: The Hampton Healthy Families Partnership. Journal of Primary Prevention, 21, 495–509.
Galano, J., & Huntington, L. (1999). Year VI evaluation of the Hampton, Virginia Healthy Families Partnership: 1992–1998. Williamsburg, VA: Center for Public Policy Research, the Thomas Jefferson Program in Public Policy, the College of William and Mary.
Galano, J., & Huntington, L. (2012). Healthy Families Virginia FY 2007–2011 statewide evaluation report. Richmond, VA: Prevent Child Abuse Virginia.
Hahn, R. A., Bilukha, O. O., Crosby, A., Fullilove,
M. T., Liberman, A., Moscicki, E. K. . . . &
Briss, P. (2003, Oct. 3,). First reports evaluating the effectiveness of strategies for preventing violence: Early childhood home visitation. Morbidity and Mortality Weekly Review, 52 (rr14), 1–9. This report is available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5214a1.htm
Hamilton, B. E., Martin, J. A., & Ventura, S. J.
(2011). Births: Preliminary data for 2010.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
3 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
National Vital Statistics Reports, 60(2). Hyattsville, MD: National Center for Health Statistics.
Kamerman, S. B., & Kahn, A. J. (1993). Home health visiting in Europe. The Future of Children, 3(3), 39–52.
National Research Council and Institute of
Medicine. (2009). Screening for prevention. In M. E. O’Connell, T. Boat, & K. E. Warner (Eds.),
Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities (221–239). Washington, DC: National Academy Press
Olds, D. L. (1980) Improving formal services for mothers and children. In J. Garbarino & S. H. Stocking (Eds.), Protecting children from abuse and neglect (173–197). San Francisco, CA: Jossey-Bass.
Schelar, E., Franzetta, K., & Manlove, J.(2008). Repeat teen childbearing: Differences across states and by race and ethnicity. Washington DC: Child Trends Research Brief. Retrieved May 12, 2008, from www.childtrends.org/Files//Child_Trends-2007_11_27_RB_RepeatCB.pdf
Staines, R. (2009). Call for replacement of Family Nurse Partnership. Pediatric Nursing, 21(10), 8.
Order your copy today! Call toll-free (800) 899-4301 or visit our bookstore at www.zerotothree.org/bookstore
Infants in the Child Welfare SystemA Developmental Framework for Policy and PracticeBRENDA JONES HARDEN
Every day, maltreated and neglected infants and toddlers are removed from theirhomes and placed into the child welfare system. Although intended to protect thechildren, the very act of separating young children from their parents and familiarcaregivers can put those children at greater risk of developmental delays.
The importance of quickly finding apermanent placement, especially for infants,cannot be overstated. In Infants in the Child Welfare System, Brenda Jones Hardenpresents a detailed examination of thedangers faced when very young children are unable to bond with a safe, dependablecaregiver. � 2007. 357 pages
Protecting Infants in Child Welfare
Protecting Infants in Child Welfare
ITEM #358 ISBN 978-0-943657-97-4 $34.95
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 3 1
Grounded in Bronfenbrenner’s (1979) ecological theory of human development, home visiting programs focus not only on the child and family, but also on the community and societal contexts in which families are nested. The main focus is on reducing risk factors and promoting protective factors at the individual level (e.g., improving knowledge and promoting skills), the dyadic
Effectiveness of Home Visiting as a Strategy for Promoting
Children’s Adjustment to SchoolKRISTEN KIRKLAND
New York State Office of Children and Family ServicesRensselaer, New York
AbstractA growing body of evidence suggests that involving families in home visiting services promotes positive experiences during the initial years of a child’s life; however less is known about whether or not the benefits continue to accrue after a child enters school. This article describes the results of a study examining the effectiveness of an evidence-based home visiting program in promoting children’s academic adjustment. The findings suggest that home visiting programs can produce positive effects on children’s academic adjustment and that changes in earlier parenting practices may play an important role in explaining how home visiting influenced these later outcomes.
level (e.g., fostering healthy parent–child interactions) and the environmental level (e.g., facilitating linkages to community services). Because home visiting programs provide services as early as possible (lasting throughout infancy and even into early childhood), they have a substantial window of time in which to influence the development and adjustment of parenting behaviors
and child development. During these early years, the home is the child’s primary developmental context, and the processes that occur within this setting are considered to be important influences on children’s subsequent development (Bronfenbrenner & Morris, 1998). T
here is a growing body of evidence suggesting that involving families in home visiting services early promotes positive experiences within the home during the initial years of life. Home visiting presents a unique opportunity to forge enduring relationships with families at a time when parents are vulnerable and the developmental path of the newborn is particularly malleable. Home visits provide a forum for
encouraging healthy prenatal behaviors and parenting attitudes, engaging infants in play, modeling a positive adult–child bond, promoting self-sufficiency skills, and facilitating linkages to supportive services. Indeed, studies have documented the ability of home-based services to effect positive changes in parenting behaviors, such as the ability to set appropriate limits (Mitchell-Herzfeld, DuMont, Lee, & Spera, 2005) and engage in responsive and cognitively engaging parenting strategies (Rodriguez, DuMont, Mitchell-Herzfeld, Walden, & Greene, 2010). Positive outcomes have also been identified for children, including lowering rates of low birthweight babies (Lee et al., 2009), producing gains in intellectual functioning during the first 2 years of life for children (Caldera et al., 2007; Landsverk et al., 2002; Olds, Robinson et al., 2004), and reducing problem behaviors through age 2 years (Caldera et al., 2007; DuMont et al., 2005; Landsverk et al., 2002).
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

3 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
nationally (e.g., those typically targeted by home visiting programs) are absent 18 or more days during a school year compared to less than 5% of children living with families having incomes at or above 3 times the level of poverty (Romero & Lee), home visiting stands to play a substantial role in facilitating children’s academic adjustment if the early positive changes it effects can be translated to this period of a child’s life. A search of the literature revealed no evaluations of home visiting’s impact on reducing rates of chronic absenteeism.
Over the past 40 years, research has generally identified grade retention as having little or no benefit—and even being harmful in the long run—to the academic and socio-emotional adjustment of children (Jimerson, 2001). However, the numerous methodological limitations inherent in the literature have made it difficult to identify the true relationship between retention and academic achievement. Studies using more advanced methodological and statistical techniques suggest that any benefits of retention are short-term and appear to diminish over time (Alexander, Entwisle, & Dauber, 2003; Wu, West, & Hughes, 2010). Few home visiting studies have had the longevity to examine the effects of home visits on children’s retention in grade. One study of a nurse home visiting program found no significant differences between the nurse-visited and control groups in the percentage of children who were ever retained in grades 1 to 3 (Olds, Kitzman et al., 2007) or through grade 6 (Kitzman et al., 2010). Thus the body of evidence regarding the ability of home visiting programs to impact children’s adjustment as they transition to school remains unclear.
This article presents the results of a 7–year randomized controlled trial of an evidence-based home visiting program to illustrate its effects on the academic adjustment of children following their transition to school. Given the important role played by the family in shaping children’s development and learning (Bronfenbrenner, 1979), the article will also describe the findings from a series of exploratory analyses that were conducted to assess the role played by early parenting practices in promoting children’s later achievement.
Healthy Families New York
Healthy Families New York (HFNY), which is based on the national Healthy Families America (HFA)
model, is a community-based prevention program that seeks to improve the health and well-being of children by providing intensive home visiting services to expectant and new parents who are considered to be at high risk
and to cooperate with peers (Alexander, Entwisle, & Dauber, 1993; Duncan et al., 2007; McClelland, Morrison, & Holmes, 2000). However, the home visiting literature pro-vides few assessments of and mixed results for these behaviors during and following the transition to school. One home visiting pro-gram reported fewer behavior problems in the borderline or clinical range by 6 years old (Olds, Kitzman et al., 2004), but other studies reported no early or lasting effects on behav-ior (DuMont et al., 2011; McCarton et al., 1997; Olds et al., 2002).
Perhaps one of the most direct influences parents can exert on children’s academic adjustment is by supporting their attendance at school. However, competing demands of work, inadequate child care, other siblings, limited financial resources, poor nutrition, illness, and nonresponsive school policies may overwhelm or undermine parent’s efforts or skills and result in unacceptable levels of absenteeism (Durham & Plank, 2010). Chronic absenteeism, which is characterized by missing 18 days or more (or about 10% of the school year; Romero & Lee, 2007) is often a symptom of neglect and has direct implications for a young child’s potential to connect with peers, learn daily routines, benefit from direct instruction, promptly hand in or receive feedback on homework, and participate in special activities. These factors in turn affect children’s subsequent rates of absenteeism, adjustment to school, and academic achievement (Romero & Lee). As approximately 15% of low income children
Although these early experiences may kindle skills that play a protective role later in the child’s life (Englund, Luckner, Whaley, & Egeland, 2004; Reynolds, Ou, & Topitzes, 2004), results from the few studies that have examined home visiting’s impacts on children’s cognitive or academic functioning during the preschool, elementary, and adolescent years suggest that the long-term benefits of these early gains tell varying stories. For example, Landsverk and colleagues (2002) and Olds and colleagues (1994; Olds, Robinson et al., 2004) found that home visiting’s effects on cognitive functioning (regardless of the model implemented) attenuated by 3 years old, while another study found that effects of nurse home visiting services on intellectual functioning emerged for the first time at 6 years old (Olds, Kitzman et al., 2004) but dissipated by 9 years old (Olds, Sandler, & Kitzman, 2007). DuMont and colleagues (2011), using maternal reports of children’s functioning at school around the time they were 7 years old, found that a significantly higher percentage of children who received home visiting services participated in gifted programs and fewer received special education services compared to children in the control group. In contrast, the researchers detected no significant differences in receipt of remedial services or receptive vocabulary.
Equally important to children’s suc-cess at school are behaviors that promote learning, such as their ability to follow rules, to listen, to organize their belongings,
During these early years, the home is the child’s primary developmental context.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/l
os
ti
nb
id
s
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 3 3
improving the parent–child relationship, helping parents understand child development and age-appropriate behaviors, encouraging optimal growth, providing assistance with access to health care, working with parents to address family challenges, and developing Individual Family Support Plans to improve self-sufficiency and family functioning. Home visitors use HFA-approved curricula, as well as standardized instruments to assess children for developmental delays. Referrals to local early intervention programs or other community services are made as needed.
The HFNY Randomized Controlled Trial and Year 7 Follow-up
In 2000, a randomized controlled trial was initiated at three HFNY sites. Eligi-ble families at each site were randomly
assigned either to an intervention group that was offered HFNY services or to a con-trol group that was given information on and referrals to other services. Baseline inter-views were conducted with 1,173 women (intervention, n=579; control, n=594). Moth-ers were again interviewed around the time of the child’s 1st, 2nd, 3rd, and 7th birthdays. At Year 7, field staff completed 942 inter-views with the original study participants, or approximately 84% of those still eligible for Year 7 assessment. Data on parenting atti-tudes, parenting practices, child behavior, access to health care, employment status, and mental health were gathered at the follow-up interviews. Child protective services reports, foster care placements, preventive services,
intensive local “wraparound” training on a variety of topics such as domestic violence, abuse and neglect, well-baby care, and communication skills. Prior to visiting families, new home visitors shadow an experienced home visitor. Once in the field, home visitors meet with their supervisors for at least 1.5 hours each week and are observed on one home visit per quarter. Additional quality assurance measures include site visits, monitoring of quarterly performance targets, field observations, and attendance at state-sponsored bi-monthly meetings for program managers.
Home Visits
Home visits are scheduled biweekly during pregnancy and increase to once a week after the mother gives birth (Level 1), usually remaining at this level until the child is at least 6 months old. As families progress through the service levels, home visits occur on a diminishing schedule, from biweekly (Level 2), to monthly (Level 3), and then quarterly (Level 4). The program continues until the target child is either 5 years old or she enrolls in kindergarten or Head Start. Home visitors typically carry a caseload of 15 when the home visitor is seeing families weekly and up to 25 cases when the families are visited less frequently. The content of the visits is intended to be individualized and culturally appropriate. During the prenatal period, home visits focus on promoting healthy behaviors, discouraging risky behaviors, coping with stress, and encouraging compliance with prenatal care. During subsequent visits, activities focus on supporting parents,
for child abuse and neglect. Specially trained home visitors provide families with support, education, and referrals to community services to: (a) promote positive parenting skills and parent–child interaction, (b) prevent child abuse and neglect, (c) ensure optimal prenatal care and child health and development, and (d) increase parents’ self-sufficiency. Participation in the program is voluntary. HFNY started in 1995 and now operates 36 programs throughout New York State.
Screening
Screening is used to target expectant parents and parents with an infant less than 3 months old who are deemed to be at risk for child abuse or neglect and live in communities that have high rates of teen pregnancy, infant mortality, welfare receipt, and late or no prenatal care. Parents who screen positive are referred to the HFNY program, and a family assessment worker (FAW) assesses parents for risk of engaging in child abuse and neglect using the Kempe Family Stress Checklist (Kempe, 1976). If parents score at or above 25 on the checklist, they are eligible for the program.
Home Visitors
After the assessment process is complete, a home visitor, also called a family support worker, is assigned to the family. Home visitors are paraprofessionals who live in the target community and share the same language and cultural backgrounds as program participants. Home visitors are selected primarily on the basis of personal attributes such as warmth, fondness for children, non-judgmental attitude, and belief in non-physical methods of disciplining children. Home visitors often are able to reach families who might not go to an office-based setting to receive services. Although home visitors are not required to have any post-secondary education, about 40% have taken courses at the post-secondary level and approximately one third of HFNY home visitors are college graduates.
Training, Quality Assurance, and Supervision
All new HFNY staff members attend a 1-week core training that is facilitated by a team of approved HFA trainers from Prevent Child Abuse New York. The goal of the core training is to teach the basic skills needed to perform home visits and assessments, including training on parent–child interaction, child development, and strength-based service delivery for home visitors; training in administering and scoring the Kempe (1976) for home visitors; and training for supervisors on their role in promoting quality services. Staff also receive
Equally important to children’s success at school are behaviors that promote learning, such as their ability to follow rules.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/M
ac
hi
ne
He
ad
z
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

3 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
class work on time). Possible scores for each subject or behavior included above grade level (3), at grade level (2), or below grade level (1). In the early grades, teachers’ ratings of these areas may be particularly informative regarding students’ receptiveness or propensity to learn, as well as predictive of their later academic success (Masten et al., 1995). The researchers also extracted data on the number of days absent and tardy, grade retention and summer school recommendations, special education, remedial and other academic intervention services receipt, and disciplinary actions.
Because of the differences between the report cards and the cumulative records, as well as differences in the information provided by districts, a number of the outcomes the researchers thought they would be able to capture were not available systematically. They were able to collect remarkably complete data for the following elements: number of days absent, whether or not the child was retained in first grade, reading or language arts achievement, math achievement, working or playing cooperatively with others, following oral directions or classroom rules, and completing home or class work on time.
Home Visiting and Children’s Adjustment to School
The researchers chose to exam-ine children’s first grade attendance and retention patterns separately
from their academic grades because these outcomes are very important indicators of academic adjustment in and of themselves. Fortunately, the school records provided remarkably complete information for these outcomes.
The researchers then created a series of variables that they thought best character-ized two groups of children on the basis of the information available from their first grade school records: those who were excel-ling academically and those who were doing poorly academically. They defined “excel-ling academically” as scoring above grade level at their best on both reading and math or scoring above grade level at their best on all three behaviors that promote learning for which the researchers had fairly complete information: working or playing coopera-tively with others, following directions or classroom rules, and completing home or class work on time. Approximately 24% of the school records sample fell into this cat-egory. Because this variable included both academic subjects and behaviors that pro-mote learning, the researchers also created a separate variable for just the academic sub-jects, called “excelling in reading and math,” which accounted for 17% of the sample, and
obtain copies of the cumulative record, which included first grade academic progress.
These efforts resulted in 577 useable first grade school records. An additional 14 records did not include academic achievement grades. Schools refused to provide records for 11 children and were unable to locate first grade records for 164 children who had moved to different schools with no records or forwarding information available. The overall school record sample was generally representative of the original baseline sample (Kirkland & Mitchell-Herzfeld, 2012).
Coding the School Records
The researchers developed a rubric and coding sheet to code each of the useable school records (Kirkland & Mitchell-Herzfeld, 2012). This task was especially challenging because most schools have their own systems for documenting students’ progress. Studies often use standardized test scores or numeric achievement grades to assess educational outcomes, but these measures are not often administered in first grade, nor are the same tests administered across schools. In the end, the researchers developed a rubric and coding sheet that considered students’ best and worst grades reported for each of several academic subject areas (e.g., reading, writing, math, physical education, music, art, science, and social studies) and for each of a number of behaviors that promote learning (e.g., working or playing cooperatively with others, following oral directions or classroom rules, listening attentively, organizing or managing personal belongings, working independently, and completing home or
and federal and state supported benefits data were obtained from administrative sources. For the first time, field staff conducted inter-views with the target children, completing interviews with 800 eligible target children. The target child interviews included mea-sures of cognitive functioning, impulsivity and self-regulation, self-reported deviance, and peer relations.
Obtaining the School Records
During the Year 7 informed consent pro-cess, field staff obtained a release form from study mothers authorizing the researchers to request the target child’s first grade school records. Field staff obtained 766 complete releases. The researchers then sent the com-plete releases, with a letter explaining the study and the purpose of the request, to more than 175 different schools in 15 states.
There were several difficulties in obtaining the first grade records from the schools. One month after sending the releases, less than one third (31%) of the initial requests to schools had resulted in a record being returned or a notification to the researchers that a record was unavailable. In general, at least two or three follow-up phone calls were required to obtain outstanding records. A substantial number of schools sent report cards for the wrong grade, often the child’s current or previous grade. These schools were contacted to clarify the request for first grade records and determine their availability. One school district, accounting for a substantial portion of the sample, did not retain copies of children’s report cards. The researchers were eventually able to
During the prenatal period, home visits focus on promoting healthy behaviors, discouraging risky behaviors, coping with stress, and encouraging compliance with prenatal care.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/S
to
ck
Li
b
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 3 5
(DuMont et al., 2008). Similarly, more HFNY mothers were found to engage in responsive and cognitively engaging parenting strategies than control mothers during observations of parent–child interactions at Year 3 (Rodriguez et al., 2010).
As the first step in this exploratory anal-ysis, the researchers examined the strength of the relationships between the signifi-cant outcomes (e.g., retention in first grade and excelling on all three behaviors that pro-mote learning) and each of the possible mechanisms (e.g., limit setting, frequency of neglect, and responsive and cognitively engaging parenting strategies). Limit set-ting and neglect at 2 years old, and responsive and cognitively engaging parenting strategies on the delay task at 3 years old were strongly related to retention in first grade. Similarly, limit setting at 2 years old, and responsive and cognitively engaging parenting strategies on the delay task at 3 years old were strongly related to excelling on all three behaviors that promote learning.
The researchers then conducted a series of analyses to assess the degree to which each of the potential mechanisms changed the effect of HFNY on retention in first grade or excelling on all three behaviors that promote learning (Kirkland & Mitchell-Herzfeld, 2012). These analyses suggested that one or more of these potential mechanisms plays a role in explaining, at least in part, how HFNY influences children’s academic adjustment. Although more sophisticated analyses will need to be conducted to better understand the actual relationships, statistical analyses of potential causal pathways (or mediating pathways) suggested that the home visiting program supported children’s learning and development by providing parents with the knowledge and skills necessary to be their child’s first teacher.
differences between the groups in the percentages of children who were excelling academically overall or for reading and math alone, although the pattern of results favored the home visited group. An examination of the children identified as doing poorly academically showed no significant differences between the control and home visited groups, either overall or within the academic subjects or behaviors that promote learning separately. As with excelling, the pattern of results generally favored the home visited group.
Understanding HFNY’s Impact
Given the potential importance of these findings, the researchers conducted a series of analyses to
examine factors that might explain how home visiting reduced the percentage of children who were retained in first grade and increased the percentage of children who were excelling on all three behaviors that promote learning (Kirkland & Mitchell-Herzfeld, 2012). After considering the literature that suggests home visiting programs have the largest and most consistent effects in the area of parenting outcomes (Gomby, 2003) and taking into account the findings from earlier examinations of HFNY, the researchers focused their attention on three possible mechanisms: appropriate limit setting, frequency of neglect, and responsive and cognitively engaging parenting strategies.
HFNY has shown an early beneficial effect on each of the candidate mechanisms. Mothers who were offered HFNY services were found to report more appropriate limit setting when their children were 2 years old than women in the control group (Mitchell-Herzfeld et al., 2005). HFNY mothers also reported a lower frequency of child neglect at Year 2 than mothers in the comparison group
one for just the behaviors that promote learn-ing, called “excelling on all behaviors that promote learning,” which accounted for 11% of the sample. These separations allowed a better understanding of where children were excelling, because it is possible for a child to excel in both academic subjects but not all three behaviors that promote learn-ing (or vice versa), in addition to excelling in all areas. Very few children excelled in every area (4%).
Use of a similar procedure created the variables that defined the group of children who were doing poorly academically except, in this case, the researchers were most interested in instances in which a child was performing poorly in any subject. Thus they defined “doing poorly academically” as at the child’s best scoring below grade level on any of the following: reading, math, working or playing cooperatively with others, following directions or classroom rules, or completing home or class work on time. Of the sample, 32% were doing poorly academically in at least one of the academic subjects or behaviors that promote learning. To be consistent with excelling, the researchers also broke this category out into a group who scored below grade level on reading or math or “doing poorly in reading or math” (24% of the sample) and a group who scored below grade level on any of the behaviors that promote learning (working or playing cooperatively with others, following directions or classroom rules, or completing home or class work on time) or “doing poorly on any behaviors that promote learning,” approximately 17% of the sample.
Next, the researchers analyzed the data to determine whether there were any differences between the HFNY and control groups on the following outcomes: retention in first grade, number of days absent, excelling academically overall, excelling in reading and math, excelling in all three behaviors that promote learning, doing poorly academically overall, doing poorly in reading or math, and doing poorly on any behaviors that promote learning (Kirkland & Mitchell-Herzfeld, 2012). As shown in Figure 1, significant differences between the two groups were identified for the percentage of children who were retained in first grade, with children in the home visited group half as likely to repeat a grade as those in the control group. In addition, there were differences between the HFNY and control groups in the percentage of children excelling on all three behaviors that promote learning, with a greater percentage of children in the home visited group excelling on all three social skills. No significant differences were identified between the HFNY and control groups on the number of days absent in first grade. Nor were there significant
Figure 1. Effect of Home Visiting on Children’s Adjustment to School
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

3 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
respond to their children’s needs, all factors that promote behaviors similar to those that are required for success in school settings. These parenting behaviors are similar to those of authoritative parents, who display high warmth and high limit setting in their interactions with their children (Baumrind, 1967). In fact, children whose parents use authoritative parenting strategies have been shown to have more positive outcomes in a variety of domains, including academic achievement (Maccoby & Martin, 1983; Steinberg, Elmen, & Mounts, 1989).
As the field moves forward in gaining a better understanding of the impact that home visiting has on the lives of children and families, it is important to remember that understanding how these programs achieve their outcomes is just as essential. By identifying and integrating activities into practice that are known to produce results, programs become more effective, which in turn promotes better outcomes for the families being served. A
Kristen Kirkland, PhD, MSW, is a research scientist at the New York State Office of Children and Family Services, Bureau of Evaluation and Research. Her work focuses on evaluating the effectiveness of the Healthy Families New York home visiting program for families at risk for child abuse and neglect using data from a longitudinal, randomized controlled trial.
Over the long term, studies have shown that children who are rejected by peers are at increased risk for lower academic achieve-ment, grade retention, dropping out of school, and engaging in delinquent and criminal activ-ities (Raver, 2002). Additional studies have shown that behaviors that promote learn-ing, such as attentiveness, organization, and task persistence, are significant predictors of children’s early academic achievement, even taking into account early math and reading achievement (Alexander et al., 1993; Duncan et al., 2007).
Given the previous findings from HFA-based programs that showed home visiting’s ability to improve parenting outcomes (DuMont et al., 2008; Mitchell-Herzfeld et al., 2005; Rodriguez et al., 2010) and even reduce early problem behaviors in children (Caldera et al., 2007, DuMont et al., 2005; Landsverk et al., 2002), it is likely that this early intervention produced some lasting change on children’s adjustment. This hypothesis is partially supported by the findings from the exploratory analyses that suggest that engagement in positive and appropriate parenting strategies may explain, at least in part, how home visiting influences children’s later academic adjustment.
More practically speaking, the transition to school is likely easier for children of mothers who were offered HFNY services, because these mothers were more likely to set appropriate limits and proactively
Conclusion
The results of this study suggest that home visiting programs do have the capacity to produce positive effects
on children’s academic skills when they enter school. Furthermore, data from the HFNY longitudinal study suggest that the changes in parenting practices initiated early by the home visiting program are likely to have played an important role in influencing these later outcomes. The finding related to reten-tion in first grade is especially important because negative outcomes in this domain can contribute to poor outcomes later in life. Children who are retained in grade are at risk for a variety of poor outcomes includ-ing lower academic achievement (Jimerson, 2001), increased symptoms of depression and anxiety (Wu et al., 2010), and dropping out of school (Alexander et al., 2003). These negative outcomes may in turn influence children’s later employment and earnings, receipt of welfare, and incarceration rates (Bowman, 2005).
The fact that a greater percentage of home visited children were excelling on all three behaviors that promote learning not only has the potential to reduce a host of negative experiences, but may even promote posi-tive outcomes. In addition to affecting levels of classroom participation and early liter-acy skills, children’s aggressive and disruptive classroom behaviors also influence their like-lihood of acceptance by teachers and peers.
References
Alexander, K., Entwisle, D., & Dauber, S. (1993). First-grade classroom behavior: Its short- and long-term consequences for school performance. Child Development, 64, 801–814.
Alexander, K., Entwisle, D., & Dauber, S. (2003). On the success of failure: A reassessment of the effects of retention in the primary grades. Cambridge, UK: Cambridge University Press.
Baumrind, D. (1967). Child care practices anteceding three patterns of preschool behavior. Genetic Psychology Monographs, 75(1), 43–88.
Bowman, L. (2005). Grade retention: Is it a help or hindrance to student academic success? Preventing School Failure, 49(3), 42–46.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U., & Morris, P. (1998).The ecology of developmental processes. In W. Damon (Series Ed.) & R. M. Lerner (Vol. Ed.), Handbook of child psychology: Vol. 1: Theoretical models of human development (pp. 993–1028). New York, NY: Wiley.
Caldera, D., Burrell, L., Rodriguez, K., Crowne,
S. S., Rohde, C., & Duggan, A. (2007). Impact of
a statewide home visiting program on parenting and on child development. Child Abuse & Neglect, 31, 829–852.
DuMont, K., Kirkland, K., Mitchell-Herzfeld, S.,
Ehrhard-Dietzel, S., Rodriguez, M. L., Lee, E.,
et al. (2011). A randomized trial of Healthy Families New York (HFNY): Does home visiting prevent child maltreatment? Final Report to the National Institute of Justice. Available www.ncjrs.gov/pdffiles1/nij/grants/232945.pdf
DuMont, K., Mitchell-Herzfeld, S., Greene, R.,
Lee, E., Lowenfels, A., Rodriguez, M., &
Dorabawila, V. (2008). Healthy Families New York (HFNY) randomized trial: Effects on early child abuse and neglect. Child Abuse & Neglect, 32, 295–315.
DuMont, K., Spera, C., Mitchell-Herzfeld, S.,
Lee, E., Greene, R., Lowenfels, A., et al. (2005). Findings from a randomized control trial of the Healthy Families New York Program. Presented at the Society for Prevention Research, Washington, D.C.
Duncan, G., Dowsett, C., Claessens, A.,
Magnuson, K., Huston, A., Klebanov, P., et al. (2007). School readiness and later achievement. Developmental Psychology, 43(6), 1428–1446.
Durham, R., & Plank, S. (2010). Maintaining high
achievement in Baltimore: An examination of the elementary grade trajectories of four recent city schools first grade cohorts [Full Technical Report]. Available at www.baltimore-berc.org/pdfs/1A_Final%20Report_FINAL_WITH%20TABLES_06-14-10.pdf
Englund, M., Luckner, A., Whaley, G., &
Egeland, B. (2004). Children’s achievement in early elementary school: Longitudinal effects of parental involvement, expectations, and quality of assistance. Journal of Educational Psychology, 96(40), 723–730.
Gomby, D. (2003). Appendix A. Building school readiness through home visitation: Detailed research findings. Available at www.ccfc.ca.gov/pdf/help/AppendixAfinal.pdf
Jimerson, S. R. (2001). Meta-analysis of grade retention research: Implications for practice in the 21st century. School Psychology Review, 30(3), 420–437.
Kempe, H. (1976). Child abuse and neglect: The family and the community. Cambridge, MA: Ballinger Publishing Company.
Kirkland, K., & Mitchell-Herzfeld, S. (2012). Evaluating the effectiveness of home visiting services in promoting children’s adjustment in school: Final report to the Pew Center on the States. Rensselaer,
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 3 7
New York: New York State Office of Children and Family Services.
Kitzman, H., Olds, D., Cole, R., Hanks, C.,
Anson, E., Arcoleo, K., et al. (2010). Enduring effects of prenatal and infancy home visiting by nurses on children. Archives of Pediatric and Adolescent Medicine, 164(5), 412–418.
Landsverk, J., Carrilio, T., Connelly, C.,
Ganger, W., Slymen, D., Newton, R., et al. (2002). Healthy Families San Diego clinical trial: Technical report. San Diego, CA: Child and Adolescent Services Research Center and San Diego Children’s Hospital and Health Center.
Lee, E., Mitchell-Herzfeld, S., Lowenfels, A.,
Greene, R., Dorabawila, V., & DuMont, K.
(2009). Reducing low birth weight through home visitation: A randomized controlled trial. American Journal of Preventive Medicine, 36, 154–160.
Maccoby, E., & Martin, J. (1983). Socialization in the context of the family: Parent-child interaction. In E. M. Hetherington (Ed.), P. H. Mussen (Series Ed.), Handbook of child psychology: Vol. 4. Socialization, personality, and social development (pp. 1–101). New York, NY: Wiley.
Masten, A., Coatsworth, J., Neemann, J.,
Gest, S., Tellegen, A., & Garmezy, N. (1995). The structure and coherence of competence from childhood through adolescence. Child Development, 66, 1635–1659.
McCarton, C., Brooks-Gunn, J., Wallace, I.,
Bauer, C., Bennett, F., Bernbaum, J., et al. (1997). Results at age 8 years of early intervention for low-birth-weight premature
infants. Journal of the American Medical Association, 277(2), 126–132.
McClelland, M., Morrison, F., & Holmes, D. (2000). Children at risk for early academic problems: The role of learning-related social skills. Early Childhood Research Quarterly, 15(3), 307–329.
Mitchell-Herzfeld, S., DuMont, K., Lee, E., &
Spera, C. (2005). New York Healthy Families Program randomized trial: Findings from the 2 year follow-up. Presented at the Prevent Child Abuse New York Conference, Albany, NY.
Olds, D., Henderson, C. R., & Kitzman, H. (1994). Does prenatal and infancy nurse home visitation have enduring effects on qualities of parental caregiving and child health at 25 to 50 months of life? Pediatrics, 93, 89–98.
Olds, D., Kitzman, H., Cole, R., Robinson, J.,
Sidora, K., Luckey, D.W., et al. (2004). Effects of nurse home-visiting on maternal life course and child development: Age 6 follow-up results of a randomized trial. Pediatrics, 114, 550–559.
Olds, D., Kitzman, H., Hanks, C., Cole, R.,
Anson, E., Sidora-Arcoleo, K., et al. (2007). Effects of nurse home visiting on maternal and child functioning: Age 9 follow-up of a randomized trial. Pediatrics, 120, e832–e845.
Olds, D., Robinson, J., O’Brien, R., Luckey, D.,
Pettit, L., Henderson, C., et al. (2002). Home visiting by paraprofessionals and nurses: A randomized, controlled trial. Pediatrics, 110, 486–496.
Olds, D., Robinson, J., Pettit, L., Luckey, D.,
Holmberg, J., Ng, R., et al. (2004). Effects of home visits by paraprofessionals and by nurses:
Age 4 follow-up results of a randomized trial. Pediatrics, 114, 1560–1568.
Olds, D., Sandler, L., & Kitzman, H. (2007). Programs for parents of infants and toddlers: Recent evidence from randomized trials. Journal of Child Psychology and Psychiatry, 48, 355–391.
Raver, C. (2002). Emotions matter: Making the case for the role of young children’s development for early school readiness. Social Policy Report, 16(3). Society for Research in Child Development: Ann Arbor, MI.
Reynolds, A. J., Ou, S., & Topitzes, J. W. (2004). Paths of effects of early childhood intervention on education attainment and delinquency: A confirmatory analysis of the Chicago child-parent centers. Child Development, 75, 1299–1328.
Rodriguez, M., DuMont, K., Mitchell-Herzfeld, S.,
Walden, N., Greene, R. (2010). Effects of Healthy Families New York on the promotion of maternal parenting competencies and the prevention of harsh parenting. Child Abuse & Neglect, 34, 711–723.
Romero, M., & Lee, Y. (2007). A national portrait of chronic absenteeism in the early grades. New York, NY: National Center for Children in Poverty. Available at www.nccp.org/publications/pdf/text_771.pdf
Steinberg, L., Elmen, J. D., & Mounts, N. S. (1989). Authoritative parenting, psychosocial maturity, and academic success among adolescents. Child Development, 60, 1424–1436.
Wu, W., West, S., & Hughes, J. (2010). Effect of grade retention in first grade on psychosocial outcomes. Journal of Educational Psychology, 102(1), 135–152.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

Reflective Supervision and Leadership in Infant and Early Childhood ProgramsMARY CLAIRE HEFFRON AND TRUDI MURCHITEM 422-OLB • ISBN: 9781934019900 200 PAGES, $39.95
Reflective supervision is hard—and it’s an even greater challenge when the same supervi-sor must provide both reflective and admin-
istrative supervision. The authors include a unique focus on this blended model of supervision. The book illustrates the foundations and frameworks of reflective practice and outlines ways to sup-port reflective supervision in a wide variety of work settings. Other highlights of the book are:
A discussion of the roles of the reflective supervisorKnowledge and skills needed for reflective supervisionTips for providing group reflective supervisionVignettes outlining common supervisory dilemmas
Resources on Reflective SupervisionA Practical Guide to Reflective SupervisionEDITED BY SHERRYL SCOTT HELLER AND LINDA GILKERSONITEM 414-OLB • ISBN: 9781934019368 200 PAGES, $34.95
This book outlines the key steps in creating a system of reflective supervision within an early childhood program to improve services, support
staff, and better meet the needs of children and families. With chapters written by leading experts, this book provides strategies for
Conducting a reflective supervision meeting,Repairing ruptures in the supervisory relationship, and Combining reflective supervision with administrative supervision.
It also lists activities that can be used to build the reflective capacity within a staff. No program should be without this valuable resource.
Reflective SupervisionWhat Is It and Why Do It?EDITED BY STEFANIE POWERSITEM: 390-OLB • NOV. 2007 48 PAGES, $15.00
Individuals share their views and insights about the process of reflective supervision and show how the practice raises consciousness about cultural, ethnic, and racial differences.
Putting Reflective Supervision Into PracticeEDITED BY STEFANIE POWERSITEM: 419-OLB • NOV. 2010 APPROX. 56 PAGES, $15.00
This issue of the Zero to Three Journal (guest editor, Rebecca Shahmoon Shanok) builds on the accumulated knowledge base by exploring current trends and issues in reflective supervision
such as the role of neurobiology, developing an evidence base for re-flective supervision, exploring diversity in work with young children and their families, and efforts to implement reflective supervision across disciplines and professions.
Reflective Supervision in PracticeStories From the FieldREBECCA PARLAKIANITEM: 267-OLB • ISBN: 9780943657592 27 PAGES, $18.00
This powerful training resource follows four infant–family programs as they implement reflective supervision. Challenges and benefits of reflective supervision are explored. This resource is especially beneficial for trainers involved in program improvement and leaders considering implementing reflective supervision in their programs.
SPECIAL PRICE! BUY ALL THREE AND SAVE 20%!
Reflective Supervision 3-PackITEM: 007-OLB • ISBN: 943670303 • $30.00
to order:Call 1-800-499-4301
www.zerotothree.org/bookstore
Being in ChargeReflective Leadership in Infant–Family ProgramsREBECCA PARLAKIAN AND NANCY SEIBELITEM: 259-OLB • ISBN: 9780943657035 23 PAGES, $12.50
This booklet explores the experience of being a new leader in an infant–fam-ily program and describes how to use
self-awareness, observation, and flexible responses as tools to increase on-the-job effectiveness and manage stress. Issues dis-cussed include relationships with staff members and learning from conflict. Includes interactive group exercises.
Look, Listen, and LearnReflective Supervision and Relationship-Based WorkREBECCA PARLAKIANITEM: 257-OLB • ISBN: 9780943657110 19 PAGES, $12.50
Written for program supervisors, this resource explores the link between supportive supervisory practices and effective staff–parent relationships. The tools and techniques presented will help program leaders promote high-quality services to young children and their families.
The Power of QuestionsBuilding Quality Relationship-Based Work REBECCA PARLAKIANITEM: 258-OLB • ISBN: 9780943657493 11 PAGES, $12.50
This booklet address the complex decisions staff face every day in their work with parents and children. Learn how lead-ers and staff alike can use reflective approaches to establish quality relationships with families.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 3 9
Home Visiting ProcessesRelations With Family Characteristics and Outcomes
CARLA A. PETERSONIowa State University
LORI A. ROGGMANUtah State University
BETH GREENPortland State University
RACHEL CHAZAN- COHENGeorge Mason University
JON KORFMACHERErikson Institute
LORRAINE MCKELVEYUniversity of Arkansas for Medical Sciences
DONG ZHANGIowa State University
JANE B. ATWATERUniversity of Kansas
AbstractVariations in dosage, content, and family engagement with Early Head Start (EHS) home visiting services were examined for families participating in the EHS Research and Evaluation Project. Families were grouped by characteristics of maternal age, maternal ethnicity, and level of family risk. All home visiting variables were related differentially to both family characteristics and outcomes but in different ways for different groups. Results highlight the importance of documenting home visiting processes across and within families as well as using this information to guide programming and support home visitors in order to maximize the effectiveness of home visiting programs.
Home visiting has long been a favored strategy for providing support services to families of very young children because it increases opportunities to adapt services to meet each family’s specific needs in the context of their everyday environment. In the US, most home visiting programs are targeted to families whose children are deemed to be “at risk” for poor
developmental outcomes because of disabilities, living in poverty, or having parents who are very young, have low intellectual functioning, or have mental health concerns. Home visiting programs for these families have been expanding in many communities. The Patient Protection and Affordable Care Act (2010) included $1.5 billion over 5 years for the Maternal, Infant, and Early Childhood Home Visiting Program to help states establish, expand, and strengthen home visiting programs for at-risk pregnant women and children up to 5 years old (Pew Center on the States, 2010). In a rare requirement, Congress insisted that this new program be informed by scientific evidence. The legislation stipulated that states must use 75% of the federal funds for home visiting programs with evidence of effectiveness, based on rigorous evaluation research.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

4 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
delved further into the longitudinal home vis-iting program data in order to understand how home visiting services may be delivered differently for families with different charac-teristics, and how these variations in services may relate to outcomes differently for dif-ferent families. This information not only helps us understand the experiences of fami-lies participating in EHS but may also provide valuable clues regarding how to maximize the effectiveness of services for a variety of home visiting programs.
We examined data from 11 of the 17 EHSREP programs, including the 7 programs that provided only home-based services, as well as an additional 4 programs that provided mostly home-based services mixed with some center-based care (we looked at the families enrolled in these 4 programs only if they actu-ally received home visiting services). The 11 programs were located in both rural and urban areas in western, midwestern, and eastern states. Primary caregivers (mostly mothers) were White (42%), African American (30%), Hispanic (24%), and from other racial or eth-nic groups (5%). Of the children, 62% were first born and were evenly split between girls and boys, and 35% of the mothers were teens (<19 years old) at the time of the child’s birth. Almost half (47%) of the mothers had not completed high school when the study began.
Measures of Home Visiting Services
A variety of measures to describe home vis-iting services were collected. These included measures of home visiting dosage each fam-ily received (the total number of home visits received; the total minutes of home visita-tion); measures of home visiting content that each family experienced (i.e., the aver-age percentage of each visit that was spent on child-focused, family-focused, or relation-ship-building activities); and measures of individual family engagement with the pro-gram, as rated by staff at the time of program exit. Percentages of time spent on the three home visit content areas summed to 100%. Only the time spent on child development and relationship building were used in these anal-yses because time focused on family issues was highly and negatively correlated with time focused on child development.
In addition, an extensive set of measures was used to assess family characteristics, child developmental status and academic achievement, parent–child interaction, parent outcomes, and parent involvement (detailed descriptions and references to the sources of these measures can be found in Administration for Children and Families, 2002; Love, Chazan-Cohen, Raikes, & Brooks-Gunn, in press; Vogel, Xue, Moiduddin, Kisker, & Carlson, 2010). Data collectors went to family’s homes at five different
parenting practices. Furthermore, impacts of the program were strengthened when pro-grams fully implemented the comprehensive Head Start Program Performance Standards, which outline the specifications for program content, intensity, and quality of services required of all Head Start and EHS programs (Harden, Chazan-Cohen, Raikes, & Vogel, 2012). Nevertheless, within the programs participating in the EHSREP, individual fam-ilies varied widely in the amount or dosage of home visiting they received, in the con-tent covered during the home visits, and in families’ overall engagement with the home visiting program.
We were interested in how dosage, content, or engagement with EHS home visiting services differed for specific subgroups of EHS families, such as teen parents, parents from different ethnic groups, or parents facing different levels of demographic risk (e.g., single, unemployed, low education). We were also interested in what ways, if any, variations in home visiting services were related to key EHS outcomes within these subgroups of families. To address these questions, we used the EHSREP dataset of extensive program services data and child, parent, and family outcome data collected for the original evaluation and for the longitudinal follow-ups.
Examining Variations in Home Visiting Services
A s part of the Pew Home Visit-ing Research Initiative, the current authors (all of whom have been
involved across multiple stages of EHSREP)
The federally funded Home Visiting Evidence of Effectiveness (HomVEE) review of the scientific evidence for specific home vis-iting models was undertaken to determine which home visiting programs have evi-dence of effectiveness (Paulsell, Avellar, Sama Martin, & Del Grosso, 2011). The HomVEE team identified 12 home visiting program mod-els that are, at this point in time, adequately supported by robust empirical evidence that meets pre-specified stringent criteria for doc-umenting their effectiveness in promoting positive outcomes for participating families and children (Health Resources and Services Administration, n.d.). These 12 programs have been tested using experimental or quasi-experimental designs and have demonstrated statistically significant favorable outcomes for children and families in at least two domains or in at least two study samples. In this article we present an in-depth examination of home visiting processes for 1 of the 12 evidence-based home visiting programs identified by HomVEE: Early Head Start (EHS).
The findings that support inclusion of EHS as an evidence-based home visiting pro-gram model come from the Early Head Start Research and Evaluation Project (EHSREP), a rigorous random assignment evaluation of 17 of the first EHS programs funded in 1995–1996. Although EHS programs can provide services through home visiting or through center-based care (or both), the EHSREP found both immediate and long-term positive impacts specifically for families in home-based EHS programs, mainly in the domains of child development and school readiness, family economic self-sufficiency, and positive
The Early Head Start Research and Evaluation Project found both immediate and long-term positive impacts specifically for families in home-based EHS programs.
Ph
ot
o: K
iw
i S
tr
ee
t S
tu
di
os
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 4 1
ethnic groups represented in the EHSREP study sample are likely not only to experience different cultural influences on the values and goals they hold for themselves and their children but also to have needs for different kinds of services to help them support their children’s early development.
Differences in home visiting services for families of different ethnicities. Hispanic families received more home visiting dosage than White or African American families and were more engaged in their home visiting programs compared with families from either of the other two groups. White families received more home visiting dosage and were more engaged in home visiting than African American families, but the content of home visits to African American families, compared with White families, was more focused on child development.
Relations among home visiting services and outcomes for families of different ethnicities. Generally, for African American families, dosage and engagement were related to more positive parent well-being, including having fewer maternal depressive symptoms and higher family incomes. However, the opposite pattern was found for child outcomes—more home visiting dosage with African American families was related to more child aggression and to poorer language and cognitive development. For White families, home visiting dosage was not consistently related to outcomes, but family engagement was related to better child cognitive outcomes when children were 3 and 5 years old.
especially with Hispanic teens, focused less on child development compared with visits to older mothers. Finally, while White and Hispanic teens received fewer home visits than older mothers of the same ethnicity, African American teens received more home visits than older African American mothers.
Relations among home visiting services and outcomes for teenaged mothers. Although teen mothers generally experienced home visits with less focus on child development, those teens who did receive more child-development focused home visits reported less parenting stress when their children were older. Unexpectedly, for teens, both home visit dosage and maternal engagement with the home visiting program were associated with some negative outcomes. More home visits were associated with less parent involvement in their children’s preschools, poorer child academic outcomes, and higher rates of child aggression. Teen mothers who were more engaged with the home visiting programs tended to be less involved with their children’s preschools and had lower incomes. But, they also reported some positive outcomes, specifically fewer symptoms of depression and lower levels of parenting stress.
Understanding these counterintuitive and mixed findings is important. It is possible, even likely, that the vulnerability of these families led program staff to provide more intensive services in the hope that their outcomes might improve. This is an area in need of additional exploration. These findings have also led us to think about the context of being an African American teen mother. At the time of program enrollment, African American teen mothers participating in the EHSREP were twice as likely to be living alone as their White and Hispanic peers. Future analyses will continue to explore the differences in social context of being a teen mother and how differences among various ethnic groups may influence home visiting services and outcomes.
FAMILIES OF DIFFERENT ETHNICITIESFamilies of different ethnicities may
respond differently to home visiting services in ways that change the configuration of services they receive as well as the ways those services are associated with child and family outcomes. For example, cultural expectations may lead some parents to be more engaged in the child development aspects of home visiting, and thus encourage more home visiting content related to child development, compared with parents from other ethno-cultural backgrounds, who may be more engaged in the social support aspects and thus encourage more of those aspects of home visiting content. Parents in the major
points in the children’s development: when children were 14, 24, and 36 months old, 5 years old (kindergarten entry), and 10 years old (fifth grade). Child outcomes assessed directly included cognitive skills when the children were 36 months and 5 years old, sustained attention when they were 5 years old, reading and math when they were 10 years old, and vocabulary when they were 3, 5, and 10 years old. Parents reported on their children’s aggressive behaviors at 3, 5, and 10 years and their children’s approaches to learning at 5 years. The quality of the home environment for supporting children’s development was assessed at all these ages, as were maternal depressive symptoms and parenting stress. In addition, parents reported family income when their children were 5 and 10 years old. We compared home visiting service variables—dosage, content, and engagement—among subgroups divided by characteristics of maternal age, maternal ethnicity, and level of family risk. We then examined how variations in these home visiting service variables were related to child and family outcomes within key subgroups: teen mothers, families of different ethnicities, with a special focus on African American mothers, and families facing higher levels of risk. All of these analyses took into account the program site, the child’s 14-month cognitive test score, the child’s gender, earlier measures of maternal depression, ethnicity (except when comparing ethnic subgroups), and the number of family risks (except when comparing risk subgroups).
Results
A full report of the findings is not feasible in this brief article. Instead, we highlight key findings focused on groups of families for whom there are noteworthy policy and practice implications. Teen parents, for example, are a group of parents about whom there is considerable interest. Similarly, families of color and those facing multiple risks are frequently targeted for intensive services.
TEEN MOTHERSTeen parents, as well as their children, are
almost by definition at great risk. They may show less optimal outcomes for themselves and their children compared with older mothers (Jutte et al., 2010) but may also show limited involvement in home visiting programs (Honig & Morin, 2001).
Home visiting services for teenaged mothers. Home visiting experiences of teens differed from those of older mothers in three key ways. First, teen mothers were less engaged in home visiting than older mothers. Second, home visits with teen mothers,
Teen parents, as well as their children, are almost by definition at great risk, and may show less optimal outcomes for themselves and their children compared with older mothers.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/R
ic
hH
ob
so
n
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

4 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
families to keep them enrolled and engaged with the program. Perhaps that worked for keeping moderate and high-risk families enrolled because they received as many home visits as the families in the low risk group. Unfortunately, relationship building was not associated with home visiting program engagement in these higher risk families. For families at higher risk, it seems that focusing home visit content on child development is the more effective strategy.
Reflections and Implications
It is a challenging task to understand how home visiting processes work. Our research shows that home visiting dos-
age, the content of home visits, and the level of family engagement with the program were all associated with important outcomes, at least for some groups of families, but not in the same ways for all groups. Although many associations among home visiting services and program outcomes generally followed expected patterns, some counterintuitive results warrant careful consideration and may suggest important implications for both practice and research. Differences between subgroups are often complex. For example, White families received more home visits than African American families, and older mothers received more home visits than teen mothers, but African American teens received more visits than their older counterparts.
One especially interesting finding is that more is not necessarily better when considering overall dosage of home visits. For only one group, White families, was there a consistent pattern of greater dosage of home visits being associated with more positive outcomes. In addition, while African American parents received the lowest number of home visits, those who did receive more home visits showed more positive adult well-being outcomes, although somewhat more negative child outcomes. Teen parents also showed a pattern of more dosage predicting more negative outcomes; the findings regarding the counterintuitive associations among more home visits and poorer outcomes for African American teens (discussed above) is an especially salient example of puzzling results. Of course, it is possible, even likely, that program staff provided more intensive services to these families in the hope that their outcomes might improve. But our data do not support this hope because the increased home visitation was not associated with any differences in program outcomes, especially in the child domain. This is an area in need of additional exploration by both researchers and practitioners.
The content of home visits, specifically the percentage of visit time spent on child-focused vs. relationship-focused activities,
many of five different risk factors each experi-enced: being a teen mother, not being married or living with a partner, receiving public assistance, having less than a high school edu-cation, and being neither employed nor in school or training. Families were classified as being at low risk (0–1 risk factor), moder-ate risk (2–3 risk factors), or high risk (4–5 risk factors). Differences among families facing different levels of risk is particularly interest-ing because positive program impacts shown in the EHSREP study were greatest for fami-lies at moderate levels of risk (Administration for Children and Families, 2002).
Differences in home visiting services for families facing different levels of risk. Overall, families at moderate or high risk were less engaged in home visiting and received visits that were less focused on child development, as compared with families at low risk. Level of risk was not associated with home visiting dosage nor with home visiting content focused on building relationships between the home visitor and the family members.
Relations between home visiting services and outcomes for families facing different levels of risk. Although moderate and high risk families received visits that were less focused on child development overall, when home visits to these families were more child-focused, there were more positive outcomes. However, the outcomes differed in an important way:
• For families at highest risk, more child-development focused home visiting content predicted better parent and family outcomes: higher family incomes, less parenting stress, fewer depressive symptoms, and fewer family moves. In contrast, a stronger focus on relationship-building activities during home visits was associated with worse outcomes, including more child behavior problems and more depressive symptoms and higher levels of stress among the mothers.
• For families at moderate risk, however, more child-development focused home visiting content predicted better child outcomes: better academic outcomes and fewer externalizing behaviors at grade 5.
These patterns suggest that the focus of home visiting content on child development is particularly important for child outcomes among families facing moderate risk and for parent outcomes among families at the highest risk level. It seems that home visitors struggled to provide services to the moderate and high-risk families and spent extra time trying to build relationships with these
Although our analyses controlled for program site, the representation of different ethnic groups varied widely between program sites and may explain these mixed findings. Different associations of home visiting services with child and family outcomes may reflect the distinctiveness of communities and programs serving these families. Dosage of home visiting services is as much or more under the control of families as it is under the control of programs. Perhaps African American mothers were more likely to accept frequent home visits when those visits were helping them to reduce depressive symptoms and make steps toward self-sufficiency, or when they recognized they needed help to support the development of their child with aggressive behavior, poor cognitive development, or delayed language development. African American mothers may show their engagement in home visiting by staying enrolled in the program more than by exhibiting behaviors that program staff tend to rate as high engagement; thus, dosage may actually be a better indicator of their engagement and interest in the home visiting program. Nevertheless, the mixed results of home visiting dosage predicting better parent outcomes but worse child outcomes for African American families suggests the importance of research examining home visitation processes specifically with this group of families.
RISK SUBGROUPSThe level of cumulative risk was deter-
mined for each family by identifying how
Families of different ethnicities may respond differently to home visiting services in ways that change the configuration of services they receive.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/t
ra
ck
5
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 4 3
guide observation of home visits, focus training and technical assistance activities, or help generate ideas for enhancing family engagement and producing better outcomes.
The differences we have found among subgroups of families offer valuable insights for home visiting programs and practitioners. Information similar to what was gathered by these EHS programs could alert other programs to potential patterns that may facil-itate or hinder home visiting effectiveness. Understanding how home visiting may vary for different groups of families can be useful for improving program effectiveness overall.
The more important and elusive goal, however, is to individualize services for each family that will support positive outcomes for the parents and their children. Helping home visitors use sensitive measures of home visiting processes would enhance their ability to recognize which processes are associated with greater levels of engagement with the program overall as well as how home visit activities might be adjusted to facilitate greater focus on child development content. This information, together with ongoing monitoring of child and family outcomes, could allow home visitors to individualize activities and services to maximize their effectiveness for each family. A
Carla A. Peterson, PhD, is professor of human development and family studies and associate dean for research and graduate education of College of Human Sciences, Iowa State University. Dr. Peterson’s research focuses on the active ingredients of interventions, delivered via a variety of programs including home visiting, child care settings, and preschool classrooms. Through Project HOME, a local project with the Early Head Start Research and Evaluation Project, she and a colleague developed an observation scale to facilitate examination of the content and process of home visiting interventions.
Lori A. Roggman, PhD, is professor of human development, Utah State University. Dr. Roggman’s research focuses on parenting and children’s early development. She has extensive experience in home visiting research, integrating theory-based inquiry with program evaluation. She is a strong methodologist with expertise in observational data collection and longitudinal analysis and has authored several observation instruments used extensively by researchers and practitioners. She was principal investigator of a local research team for the Early Head Start Research and Evaluation Project.
Beth Green, PhD, is research professor and director of early childhood and family support research, Graduate School of Social Work, Portland State University (Portland, OR).
American and teen families were more likely to be “late” or “never” fully implemented. Future research that measures program implementation quality and community char-acteristics with larger samples may help us to better understand how variations in home visiting service delivery lead to different out-comes for different groups of families.
The real challenge for home visitors, how-ever, is using results such as these to guide programming. Home visiting programs pro-vide a unique opportunity to work closely with a family in their own home and over a long period of time. By using that time to learn about each family’s unique circum-stances, a home visitor can better engage the family effectively and adapt activities to meet the individual needs of each family or even each family member. This is a tall order though, and to do it effectively home visitors must understand how the active ingredients of home visiting services work, across fam-ilies as a group and within each individual family. To increase home visiting effective-ness, programs must measure these process variables accurately, use measures sensitive enough to detect subtle differences between families and within a family over time, and adapt services to maximize each family’s par-ticipation, engagement, and outcomes. Home visitors, themselves, may need a way to doc-ument and track the actual interventions provided during their visits.
The EHS programs and home visitors participating in the EHSREP were all charged with implementing the EHS home-based program within parameters delineated by the Head Start Program Performance Standards (Administration on Children and Families, 2012). As highlighted here, however, actual home visiting experiences varied both between and within different subgroups of families. Likely, similar variations are found in other home visiting models. Parameters that guide program models provide important guidelines but are seldom specific enough to require that home visitors collect and learn to use the types of information that we used in this study. Rarely, however, would program model requirements dictate against using this information to inform programming. For example, home visitors participating in the EHSREP were asked to record, at the end of each visit, the percentages of time they spent on each of three different content areas—child development, family issues, and staff–family relationship building. This was a relatively simple reporting task, and, given what we know now about the importance of focusing on child development, home visitors could likely use this information immediately to refocus a current visit or plan strategies for upcoming visits. In addition, home visiting supervisors could use this information to
in contrast to overall dosage, was related differentially to family demographics and to outcomes. Home visits to families facing more risks and to teen mothers tended to have a smaller proportion of time focused on child-related activities; however, visits with African American parents tended to be more child-focused. Spending more home visit time focused on child development was associated with more positive outcomes in several areas, especially among those subgroups who received less child-development focused content overall. For example, as a group, teen mothers experienced home visits less focused on child development—however, those teens who did receive more child-development focused home visits reported less parenting stress when their children were older. Further, among the families in the moderate and high-risk groups, those whose visits were more focused on child development had more positive outcomes across a variety of child and parent domains. Conversely, a focus on building staff–family relationships was associated with more negative outcomes for families at highest risk.
Among these specific subgroups of families, our findings are consistent with those of prior researchers who, using a larger sample of EHSREP participants, suggested that a home visiting focus on child development is associated with better outcomes (Raikes et al., 2006). It is easy to understand how home visitors can be distracted from focusing on child development when working with families facing multiple risks. These family members are likely to be facing an imminent crisis, feeling torn among competing priorities, having trouble focusing on any topic for an extended period of time, and thinking that the developmental needs of a young child are “the least of our worries.” Evidence is accumulating, however, maintaining a focus on child development during home visits, even among higher risk families, is important for promoting more positive outcomes for both children and their parents as well as for facilitating continued enrollment (Raikes et al., 2006; Roggman, Cook, Peterson, & Raikes, 2008).
Our research findings should be consid-ered carefully but not seen as conclusive. Small sample sizes in some subgroups no doubt limit our ability to detect consistent patterns and many of the subgroups are over-represented in specific sites. Although our analyses controlled for site, this is likely insufficient to account for program variations in implementation quality or other factors that may have a potentially greater impact on outcomes for these families than our mea-sured home visiting variables. For example, we found that programs serving more African
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

4 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Evaluation Project taking a leadership role in examinations of parenting behaviors and father involvement in their children’s lives.
Dong Zhang, MS, is graduate research assis-tant, Department of Human Development and Family Studies, Iowa State University. Mr. Zhang has been involved in a variety of studies to examine intervention processes in home visiting interven-tions and is currently involved in evaluations of family support programs.
Jane B. Atwater, PhD, is assistant research professor, University of Kansas. Dr. Atwater has been involved in multiple examinations of the relations among specific intervention ingredients, program quality, and child outcomes. Dr. Atwater has been involved in numerous multiple-site projects including the Early Head Start Research and Evaluation Project.
Jon Korfmacher, PhD, is associate professor, Erikson Institute (Chicago, IL). Dr. Korfmacher’s research focuses on evaluation of early childhood programs, with an emphasis on home visiting. Previously, he worked on analyses of program implementation of the Nurse-Family Partnership program, and was a co-investigator with a local research partner team for two programs that par-ticipated in the Early Head Start Research and Evaluation Project . He is particularly interested in issues of program quality, development of the helping relationship between providers and fam-ilies, and staff development and training. He is a graduate fellow of ZERO TO THREE.
Lorraine McKelvey, PhD, is assistant research professor, University of Arkansas for Medical Sciences. Dr. McKelvey’s research focuses on evaluating the efficacy of a variety of early childhood programs and services. She has been involved with research teams at multiple sites involved in the Early Head Start Research and
Dr. Green has extensive experience leading cross-site research investigations of early childhood programs. She was involved in the local research project, conducted in conjunction with the Early Head Start Research and Evaluation Project, that examined parent involvement in Early Head Start home visiting programs in Pittsburgh. In addition, Dr. Green has directed projects to evaluate state and federal policies related to child welfare.
Rachel Chazan-Cohen, PhD, is associate pro-fessor of psychology, George Mason University. Dr. Chazan-Cohen has worked with the Early Head Start Research and Evaluation Project and with Early Head Start programs across the coun-try as a project officer with the Office of Planning, Research, and Evaluation in the U.S. Department of Health and Human Services. Dr. Chazan-Cohen has conducted multiple studies involving Early Head Start and other family support pro-grams and has co-authored a book on infant mental health.
References
Administration for Children and Families. (2002). Making a difference in the lives of infants and toddlers and their families: The impacts of Early Head Start Volume II: Final technical report appendixes. Washington, DC: U.S. Department of Health and Human Services.
Administration for Children and Families.
(2012) Head Start Program performance standards. Washington, DC: US Department of Health and Human Services. Retrieved December 11, 2012, from http://eclkc.ohs.acf.hhs.gov/hslc/tta-system/operations/Fiscal/Legislation%20and%20Regulations/Head%20Start%20Program%20Performance%20Standards
Harden, B. J., Chazan-Cohen, R., Raikes, H. H.,
& Vogel, C. (2012). Early Head Start home visitation: Role of implementation in bolstering program benefits. Journal of Community Psychology, 40(4), 438–455.
Health Resources and Services Administration.
(n.d.) Home visiting models. Retrieved from http://mchb.hrsa.gov/programs/homevisiting/models.html
Honig, A. S., & Morin, C. (2001). When should programs for teen parents and babies begin? Longitudinal evaluation of a teen parents and babies program, The Journal of Primary Prevention, 21(4), 447–454.
Jutte, D. P., Roos, N. P., Brownell, M. D.,
Briggs, G., MacWilliam, L., & Roos, L. L. (2010). The ripples of adolescent motherhood: Social, educational, and medical outcomes for children of teen and prior teen mothers. Academic Pediatrics, 10(5), 293–301.
Love, J., Chazan-Cohen, R., Raikes, H., &
Brooks-Gunn, J. (in press). What makes a difference: Early Head Start evaluation findings in a developmental context. Monographs of the Society for Research in Child Development.
Patient Protection and Affordable Care Act. (2010). Pub. L. No. 111-148, §2702, 124 Stat. 119, 318–319.
Paulsell, D., Avellar, S., Sama Martin, E., &
Del Grosso, P. (2011). Home Visiting Evidence of Effectiveness review: Executive summary. Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services.
Pew Center on the States. (2010). Pew inventory of state home visiting programs. Retrieved November 30, 2010, from www.pewcenteronthestates.org/initiatives_detail.aspx? initiativeID=61051
Raikes, H., Green, B. L., Atwater, J., Kisker, E.,
Constantine, J., & Chazan-Cohen, R. (2006). Involvement in Early Head Start home visiting services: Demographic predictors and relations to child and parent outcomes. Early Childhood Research Quarterly, 21, 2–24.
Roggman, L. A., Cook, G. A., Peterson, C. A., &
Raikes, H. H. (2008). Who drops out of Early Head Start home visiting programs? Early Education and Development, 19, 1–26.
Vogel, C. A., Xue, Y., Moiduddin, E. M.,
Kisker, E. E., & Carlson, B. L. (2010). Early Head Start Children in grade 5: Long-term follow-up of the Early Head Start Research and Evaluation study sample. OPRE Report # 2011-8. Washington, DC: Office of Planning, Research, and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 4 5
New Opportunities and Directions in Home Visiting
Research and Evaluation LAUREN H. SUPPLEE
Administration for Children and Families Washington, DC
ROBIN L. HARWOODHealth Resources and Services Administration
Rockville, Maryland
NANCY GEYELIN MARGIEBusiness Strategy Consultants
Largo, Maryland
ALETA L. MEYERAdministration for Children and Families
Washington, DC
For more than a century, home visiting has been used in the U.S. as a service delivery strategy to reach high-risk families ( Weiss, 1993). A body of research has found that home visiting has the potential to affect a broad range of outcomes and be cost beneficial (Lee et al., 2012). Prior to 2010, there were estimates that states spent between $500 million and $750 million
annually on home visiting programs (Stoltzfus & Lynch, 2009). Through a provision of the Patient Protection and Affordable Care Act (2010), home visiting has been greatly expanded, with $1.5 billion over 5 years provided to states, territories, and tribes to establish evidence-based home visiting programs for at-risk pregnant women and children from birth to 5 years old. This provision created the Maternal, Infant and Early Childhood Home Visiting Program (MIECHV ) to respond to the needs of children and families in communities at risk. The Health Resources and Services Administration (HRSA) and the Administration for Children and Families (ACF) collaborate to implement MIECHV. Home visiting is one of several service strategies embedded in a comprehensive, high-quality early childhood system that promotes (a) maternal, infant, and early childhood health, safety, and development; (b) strong parent–child relationships; and (c) responsible parenting among mothers and fathers.
AbstractThe authors describe the research and evaluation activities connected to the new Maternal, Infant and Early Childhood Home Visiting program. The goal of these activities is to provide information on federal, state, and local efforts to strengthen programs by providing much needed knowledge on the best ways to support the implementation of home visiting programs at multiple levels—with families, home visitors, supervisors, organizations, and others. The collection of research and evaluation activities has a strong emphasis on capacity building, both for grantees and for the research community as a whole. This article aims to support the dissemination of research to the practice community by highlighting the resources currently available and to come.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

4 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
The review includes a broad literature search, an assessment of the quality of the study design to produce unbiased impact estimates, and a determination of whether the model meets the Department of Health and Human Services (DHHS) criteria for evidence of effectiveness. The HomVEE Web site summarizes the models that were found to have evidence of effectiveness, detailed information about the samples of families who participated in the research, the outcomes measured in each study, and the implementation guidelines for each model (see Learn More).
To date, 32 models have been reviewed and 13 meet the DHHS criteria for evidence of effectiveness: Child FIRST, Early Head Start-Home Visiting, Early Intervention Program for Adolescent Mothers, Early Start (New Zealand), Family Check-Up, Healthy Families America, Healthy Steps, Home Instruction for Parents of Preschool Youngsters (HIPPY), Nurse-Family Partnership, Oklahoma Community-Based Family Resources and Support, Parents as Teachers, Play and Learning Strategies-Infant, and SafeCare Augmented. Based on rigorous research available for primary measures (e.g., direct observation, direct assessment, administrative records, or self-report on a normed, standardized measure), HomVEE determined that most of the 13 evidence-based models had favorable impacts on child development or on school readiness and positive parenting. In addition, 3 of the 13 models had impacts on maternal health, 6 of the 13 models had impacts on child health, and 5 of the 13 had impacts on child maltreatment. The review also highlighted areas where more research is needed. For example, few of the reviewed models had impacts, using primary measures, on crime or family violence, family economic self-sufficiency, or coordination of resources and referrals (see Learn More).
HomVEE also conducted a systematic review specifically to assess evidence of effectiveness of home visiting for American Indian and Alaskan Native (AIAN) populations. None of the home visiting program models included in this review met DHHS criteria for an evidence-based early childhood home visiting service delivery model for the AIAN populations. Of the models with high or moderate quality impact studies that included AIAN populations, the studies of Healthy Families Alaska, SafeCare+, and Oklahoma Community-Based Family Resources and Support did not report findings for AIAN populations. Although the study of Early Start (New Zealand) received a moderate rating and reported findings by ethnicity, Early Start (New Zealand) does not meet the DHHS criteria
high-school drop-outs, substance abuse, unemployment, or child maltreatment. In addition, the legislation specifies priority for serving specific high-risk populations includ-ing: families living in a community at-risk, low-income families, pregnant women less than 21 years old, families with a history of child abuse or neglect, families with a his-tory of substance abuse, families with tobacco users, families with children with low student achievement or developmental delays, and military families.
The MIECHV program is unique as one of the first among several recent initiatives that explicitly linked funding and evidence together. The program reserves the majority of funding (75%) for the implementation of one or more evidence-based home visiting models. In addition, the legislation supports continued innovation by allowing for up to 25% of funding to be used for promising approaches and rigorous evaluation of those approaches. To inform the execution of the MIECHV program and to contribute knowledge to the field of home visiting broadly, the Home Visiting Evidence of Effectiveness (HomVEE) project was launched to conduct a thorough, transparent systematic review of the home visiting research literature.
HomVEE Systematic Review
HomVEE provides an assessment of the evidence of effectiveness for home visiting program models
that serve families with pregnant women and children from birth to 5 years old.
HRSA and ACF have issued guidance reflecting a vision for high-quality, evidence-based home visiting programs as part of an early childhood system. MIECHV provides an unprecedented opportunity for collaboration and partnership at the federal, state, and community levels to improve health and development outcomes for at-risk children through evidence-based home visiting programs. Through collaborative efforts with partners, this program has the opportunity to effect changes that will improve the health and well-being of vulnerable populations by addressing child development within the framework of life course development and using a socio-ecological perspective.
Program Structure
For the purposes of MIECHV, home visiting includes programs that use home visiting as a primary ser-
vice delivery strategy and in which services are offered on a voluntary basis to preg-nant women, expectant fathers, and parents and caregivers of children birth to kinder-garten entry to address relevant participant outcomes. The legislation specifies that MIECHV must target these home visiting services to communities at-risk. The legis-lation defines communities at-risk as those with high concentrations of premature birth, low-birth weight infants, and infant mortal-ity, including infant death due to neglect, or other indicators of at-risk prenatal, mater-nal, newborn, or child health; poverty; crime; domestic violence; and with high rates of
Home visiting is one of several service strategies embedded in a comprehensive, high-quality early childhood system.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/L
ig
ht
ha
un
te
r
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 4 7
for an “evidence-based early childhood home visiting service delivery model,” for the AIAN populations because the effects are on a subgroup and the findings have not been replicated in another sample. However, some important lessons about implementing home visiting in tribal communities were learned. One lesson was how to develop or adapt culturally relevant models for tribal communities. The literature suggests model developers should: engage tribal leaders in planning, development and implementation; build on cultural strengths and customs; and employ culturally competent staff or staff from within the community. The tribal review also provided implications for future research including: supporting the development and implementation of culturally relevant models; examining how home visiting models work for AIAN children and families; and maximizing the use of utilization-focused, participatory evaluation methods (see Learn More).
In addition to assessing the state of evidence on home visiting, HomVEE provides additional resources such as lessons learned around implementation of home visiting programs. Paulsell, DelGrosso, and Supplee (2012) reviewed the implementation experiences reported in the literature. This review revealed some threats to high-quality implementation of home visiting around specification of the model, necessary infrastructure supports for home visiting programs, and service delivery.
First, concerning model specification, it was learned that: (a) some models have a mismatch between goals and content; (b) complex models are difficult for home visitors to implement; (c) hiring home visitors with the qualifications specified by some models is challenging; and (d) few models have evidence on the effects of adaptations for specific populations.
Second, lessons around the support necessary to implement a home visiting model include: (a) home visitors don’t always have the knowledge needed to use assessments to plan services for families; (b) home visitors are not consistently trained on model content; and (c) supervision in adherence with model requirements can be challenging.
Finally, in relation to home visiting service delivery and receipt, the review found that home visitors feel that they lack information on referral sources and that they face challenges reaching the intended population, completing the required number of home visits, and working with families who miss appointments or drop out of the program.
HomVEE also synthesized some lessons learned about gaps in research on home
visiting and suggestions for strengthening future research in this area (see Learn More).
Research and Evaluation
Although home visiting has a rich history of research and evaluation, there remain many gaps in the
knowledge base that need to be explored. The MIECHV program has an exceptional focus on research and evaluation. All of the program’s research and evaluation activities aim to address gaps in the research knowledge as well as answer questions the field is asking to improve practice and outcomes for families.
First, the legislation requires a national evaluation of this new program. The Mother and Infant Home Visiting Program Evaluation (MIHOPE) will include the four models chosen by at least 10 states for their MIECHV funds: Early Head Start-Home Visiting, Healthy Families America, Nurse-Family Partnership, and Parents as Teachers. The evaluation will include approximately 12 states, 85 local implementing agencies (about 20 sites per model), and 5,100 pregnant women or families with infants less than 6 months old (approximately 60 families per site on average). The study is using a random assignment design. The study design includes three main foci: an impact study, an implementation study, and a cost study. Questions for the impact study include: What is the impact of MIECHV? How do impacts vary among different populations? Questions for the implementation study include: Which program aspects are associated with impacts? How do program sites actually operate? How do programs recruit, retain, and engage families? Questions for the cost study include: What does it cost to implement an evidence-based home visiting program? The MIHOPE study provides an unprecedented opportunity to examine evidence-based home visiting at scale. The design will allow researchers to better understand how program features are related to impacts (e.g., does home visitor training in content on child health relate to stronger impacts on child health?). Finally, although HomVEE found a rich literature on home visiting, the effects vary substantially both across models and within models across studies. This variation may be due to using different measures, measuring outcomes at different times, or varying focus or curriculum of home visiting models (e.g., as adaptations to differing populations). The MIHOPE study provides the opportunity for consistent measures and consistent follow-up to capture program operation at scale (see Learn More).
In addition, the Centers for Medicare and Medicaid services, ACF, and HRSA have
initiated the MIHOPE-Strong Start evalua-tion. This evaluation builds from MIHOPE to examine the effectiveness of some home visiting programs to reduce preterm birth, increase birth weight, and improve infant health. This partnership will expand the MIHOPE sample to include 20,000 pregnant women. Like the core MIHOPE study, it will use a random assignment design. Outcomes will be assessed through administrative data including birth and medical records.
Second, the legislation also calls for a con-tinuous program of research designed to increase knowledge about the implemen-tation and effectiveness of home visiting programs. In response to this call, two new research programs have been established. The first is a multisite, interdisciplinary Home Visiting Research Network (HVRN), which was awarded in July 2012. The goals of the HVRN include: developing an infrastruc-ture to serve as the basis for collaborative efforts; identifying a national research agenda in order to advance the field; generat-ing research proposals based on that agenda; providing opportunities to mentor future home visiting researchers; and disseminating findings to researchers, professionals, and the public (see Learn More).
The second new research program sup-ports investigator-initiated research that shows promise of advancing knowledge regarding the implementation and effective-ness of home visiting in order to improve life outcomes among mothers, infants,
Home visiting includes programs in which services are offered on a voluntary basis to pregnant women, expectant fathers, and parents and caregivers of children.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.C
om
/J
os
eG
ir
ar
te
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

4 8 Z e r o t o T h r e e J a n u a r y 2 0 1 3
initiatives; infrastructure supports such as state- or county-level centralized intake systems; and organizational culture and climates necessary to support staff to imple-ment with fidelity.
In addition to these requirements for rig-orous evaluation, the legislation requires grantees to collect regular benchmark data on a range of domains and demonstrate improvement in those domains within 3 years. The domains include maternal and child health, child development and school readiness, child maltreatment, family eco-nomic self-sufficiency, crime or domestic violence, and increases in coordination of resources and referrals. Each grantee has worked to develop benchmark plans that
potential linkages between project activ-ities and improved outcomes. The intent of these rigorous evaluations is to build the evidence of effectiveness for promis-ing approaches. Some of the programs being evaluated as promising approaches include: Maternal Infant Health Outreach Worker (West Virginia), Family Spirit (Arizona), Team for Infants Endangered by Substance Abuse (Missouri), and Resource Mothers (Virginia). In MIECHV a portion of the funds are allocated through formula grants to states and a portion of the funds are allocated competitively to states. In addition, states that received competitive grants in FY11 and FY12 to expand services or to enhance exist-ing services are also required to rigorously evaluate their grant activities. These eval-uations will build knowledge in the field of home visiting. Some examples of foci of these evaluations include the scale up of evidence-based home visiting; enhancements on home visiting models, such as Doula programs, community-peer liaisons, or fatherhood
and young children. Three initial awards were made in September 2012, to support research around: book sharing in Early Head Start (EHS), the use of cell phone technol-ogy to improve parent engagement in EHS, and reducing parental stress and increas-ing parenting competence in a home visiting program (see box 2012 Maternal and Child Health Home Visiting Research Grants). More information regarding the new investi-gator-initiated home visiting research grant program will be available from the HRSA Maternal and Child Health Research pro-gram (see Learn More).
The MIECHV program is also focusing on research and evaluation by making rig-orous evaluation, data collection and data systems, and continuous quality improve-ment (CQI) integral parts of grantees’ activities. For example, if a grantee chooses to implement a promising approach, the grantee must conduct a rigorous evaluation (see box Definition of Rigorous Evaluation) of that approach that ideally demonstrates
Definition of Rigorous
Evaluation
Health Resources and Services
Administration (HRSA) and Administration
for Children and Families (ACF) have
established the following four criteria for
rigorous research:
1. Credibility: Ensuring what is intended
to be evaluated is actually what is being
evaluated; making sure that descriptions
of the phenomena or experience being
studied are accurate and recognizable to
others; ensuring that the method used is
the most definitive and compelling
approach that is available and feasible
for the question being addressed. If
conclusions about program efficacy
are being examined, the study design
should include a comparison group
(i.e., randomized control trial or
quasi-experimental design); see the
HomVEE Web site for standards for
study design in estimating program
impacts: www.acf.hhs.gov/programs/
opre/homvee);
2. Applicability: Generalizability of
findings beyond current project
(i.e., when findings “fit” into contexts
outside the study situation). Ensuring
the population being studied represents
one or more of the population being
served by the program;
3. Consistency: When processes and
methods are consistently followed and
clearly described, someone else could
replicate the approach, and other
studies can confirm what is found; and
4. Neutrality: Producing results that are
as objective as possible and that
acknowledge the bias brought to the
collection, analysis, and interpretation
of the results.
Source: HRSA grant HRSA-11-187, pp. 41–42
2012 Maternal and Child Health Home Visiting
Research Grants
The Maternal and Child Health Home
Visiting Research program awarded
grants in September 2012, to:
a. Lehigh University to conduct random-
ized controlled trials investigating the
efficacy of an intervention that assists
families in formulating book sharing
routines and engaging their children
through dialogic techniques; this
intervention, Little Talks, will be
integrated into an Early Head Start
(EHS) home visiting program that
serves a largely Latino population.
The goals of this intervention include:
(a) enhancing the roles and responsibili-
ties of home visitors so they are
effective in providing and supporting
EHS caregivers in the implementation of
Little Talks; (b) formulating a data-
based supervision process for support-
ing EHS home visitors in their imple-
mentation of Little Talks; (c) applying
multifaceted fidelity monitoring
procedures to home visitors’ delivery
of Little Talks to EHS families; and
(d) adapting and applying the Little
Talks intervention to an EHS home
visiting program that largely serves
Latino families;
b. University of Kansas for a randomized
controlled trial examining how use of
cell phone technology can be used by
home visitors to: (a) improve parent
participation and engagement in an
evidence-based naturalistic language
intervention through the use of text
messaging and phone calls between
home visits; (b) increase the dosage of
the intervention received by the parent
to facilitate their use of the language-
promoting intervention strategies; and
(c) improve the early language
outcomes for infants and toddlers
receiving home visiting through EHS
through an increase in parents’ use of
the intervention; and
c. Washington University St. Louis to study
the impact of an intervention enhance-
ment on reducing maternal stress and
depression, and increasing parenting
competency among low-income women
in rural counties who are experiencing
postpartum depression or significant
stress; the intervention, Problem
Solving Therapy, will be used with the
experimental groups in conjunction with
an evidence-based parenting group
(Incredible Years), and a promising
model home visiting program, Nurses
for Newborns. It is hoped that this
model will contribute to knowledge of
home visiting through: (a) enhancing
home visiting with an intervention that
addresses maternal depression and
stress; (b) promoting child maltreat-
ment prevention with evidence-based
parenting; and (c) improving under-
standing of linkages and referrals
among services in rural areas.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 4 9
Research and Evaluation in Tribes
In addition to the state program, MIECHV has a 3% set-aside for tribes, tribal organizations, and urban Indian
organizations. The tribal home visiting program has a strong focus on building capacity of tribes to conduct research and evaluation that is meaningful for the tribe. The tribes are collecting benchmark data similar to that collected by the state grantees. In addition, because HomVEE did not find any home visiting model to have evidence of effectiveness for tribes, each tribal grantee is conducting a rigorous evaluation of its home visiting program, or its implementation, or both. These evaluations will help grantees determine the value of the program for their own communities and contribute to the knowledge base about what works for AIAN communities. To facilitate success with these activities, the Tribal Home Visiting Evaluation Institute was established to provide technical assistance to tribal home visiting grantees in measuring benchmarks, building data systems, CQI, and designing locally driven rigorous evaluations of home visiting (Strader et al., this issue, p. 51). Tribal Home Visiting Evaluation Institute aims to provide individualized, culturally relevant technical assistance that empowers grantees to have ownership over data collection and use.
Finally, in a joint project between MIECHV and Head Start, the Tribal Early Childhood Research Center was funded to address gaps in early childhood research with American Indian and Alaskan Natives. The goals of the Tribal Early Childhood Research Center are: to engage in a participatory process of consultations with key stakeholders to foster a community of learning; to support and conduct research particularly around measure adaptation and development; to enhance research to practice; and to build capacity within AIAN communities for conducting research on programs to promote healthy maternal, infant, and early childhood development (see Learn More).
Expanding the Knowledge Base
Through the activities above, MIECHV has an unprecedented opportunity to expand the knowledge
base about home visiting. The research and evaluation work aims to produce knowledge that will support the home visiting field broadly. The activities examine efficacy of programs or enhancements to programs, expanding the evidence-base for the field. The research and evaluation projects aim to contribute much needed information on the best ways to support the implementation of home visiting programs at multiple levels—
reflect the diversity of models in their state, state goals, and achievable goals for the pro-gram. Though challenging, the process has enabled grantees to develop ownership over the data collected and to have the poten-tial to use the data for more than federal reporting requirements. Building on the legis-latively mandated benchmark data collection, grantees have been required to establish con-tinuous quality improvement (CQI) plans to specify the processes and outcomes of the grantees’ MIECHV program through regu-lar data collection, the use of data to inform administration, and monitoring the appli-cation of changes to improve performance. It is anticipated that the use of CQI meth-ods in the MIECHV program will result in more effective program implementation and improved participant outcomes.
The MIECHV program has also shown a particular focus on research and evaluation through its provision of extensive technical assistance (Strader, Counts, & Filene, this issue, p. 51) to grantees as needed. Technical assistance being provided by the Design Options for Home Visiting Evaluation team is helping grantees design rigorous evaluations that meet the requirements of the MIECHV program as well as contribute to the home visiting research literature; develop benchmark plans that meet the individual needs and interests of the grantee as well as the legislatively mandated requirements of the MIECHV program; and design CQI systems that will help programs continually improve.
Finally, MIECHV funds support the continuation of the Supporting Evidence-Based Home Visiting (EBHV) initiative. In 2008, the Children’s Bureau within ACF funded 17 cooperative agreements to support the infrastructure needed for the widespread adoption, implementation, and sustainability of evidence-based home visitation programs that aim to prevent child maltreatment. Grantees are supporting the implementation of EBHV programs with fidelity, the scaling up of the high-fidelity home visiting models, and the sustainability of the models. Grantees are also conducting local implementation and outcome evaluations. The program’s overarching goal is to generate knowledge about the use of evidence-based home visiting programs to prevent child maltreatment, including obstacles and opportunities for their wider implementation. In 2011, the EBHV grant program was formally incorporated into the MIECHV Program. A cross-site evaluation of EBHV aims to identify successful strategies for adopting, implementing, and sustaining high-quality home visiting programs to prevent child maltreatment (see Learn More).
Learn More
Home Visiting Evidence of Effectiveness
(HomVEE)
Systematic Reviewhttp://homvee.acf.hhs.gov/
Executive Summaryhttp://homvee.acf.hhs.gov/HomVEE_Executive_Summary_2012.pdf
Tribal Reporthttp://homvee.acf.hhs.gov/TribalReport.pdf
Lessons Learnedhttp://homvee.acf.hhs.gov/Lessons_Learned.pdf
Mother and Infant Home Visiting
Program Evaluation (MIHOPE)
www.acf.hhs.gov/programs/opre/other_resrch/miece/index.htm
Home Visiting Research Network (HVRN)
www.hopkinschildrens.org/home-visiting-research-network.aspx
Health Resources and Services
Administration, Maternal and Child
Health Research
http://mchb.hrsa.gov/research/
Supporting Evidence-Based Home
Visiting (EBHV)
http://supportingebhv.org/
Tribal Early Childhood Research Center
www.ucdenver.edu/academics/colleges/PublicHealth/research/centers/CAIANH/trc/Pages/TRC.aspx
The Home Visiting Evidence of Effectiveness project conducted a systematic review specifically to assess evidence of effectiveness of home visiting for American Indian and Alaskan Native populations.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/M
on
aM
ak
el
a
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

5 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Strategy Consultants under contract to OPRE. She works on projects related to home visiting, Head Start, and child care. Currently, her main projects include the development of a measure of Family-Provider Relationship Quality in early care and education programs; the provision of research and evaluation technical assistance to the Maternal, Infant and Early Childhood Home Visiting grantees; the Child Care and Early Education Quality Features, Thresholds and Dosage and Child Outcomes project; and the Head Start Graduate Student Research grants. Nancy came to OPRE as an SRCD Executive Branch Policy Fellow after earning her doctorate from the University of Maryland. Before attending graduate school, she was a research assistant at the National Academies for the report From Neurons to Neighborhoods and at Child Trends working on topics related to early childhood development, child care, and education.
Aleta L. Meyer, PhD, is a senior social science research analyst at the Administration for Children and Families, in the Office of Planning, Research, and Evaluation, in the Division of Family Strengthening; her areas of responsibility include evaluation of home visiting in American Indian/Alaska Native communities, youth development, prevention, implementation science, and foster care. From 2007–2010, Dr. Meyer was a health scientist administrator in the Prevention Research Branch at the National Institute on Drug Abuse (NIDA). Prior to joining NIDA, she was an associate professor of psychology in the Clark-Hill Institute for Positive Youth Development at Virginia Commonwealth University. The focus of her research has been to translate theory and empirical research across multiple health outcomes into effective and feasible prevention programs.
Indiana University in educational psychology with a specialization in family-focused early intervention services. Her personal research interests include evidence-based policy, social–emotional development in early childhood, parenting, prevention/intervention programs for children at-risk, and implementation research. Prior to joining ACF, she worked as a research associate at the University of Pittsburgh directing a clinical trial of a multisite early intervention home visiting program for the prevention of early behavioral issues in toddlers.
Robin L. Harwood, PhD, is a health scientist in the Division of Research, Maternal and Child Health Bureau, Health Resources and Services Administration. She is the federal liaison and project officer for the Home Visiting Research Network, and project officer for the Maternal and Child Health Home Visiting Research Grants, an investigator-initiated program. In addition to home visiting, Robin’s portfolio also includes research grants and networks from the Combating Autism Act Initiative, and the Maternal and Child Health Research Program. Prior to joining the federal government, she was an associate professor in the School of Family Studies at the University of Connecticut. During her years in academia, she was principal investigator for two separate grants from NICHD examining culture, attachment, and parenting beliefs among mothers in Puerto Rico, Germany, and the United States. She has published numerous articles in peer-reviewed journals, as well as two books on child development, culture, and attachment. She received her doctorate from Yale University.
Nancy Geyelin Margie, PhD, is a research fellow, Office of Planning, Research and Evaluation (OPRE), Administration for Children and Families, U.S. Department of Health and Human Services. Nancy works at Business
with families, home visitors, supervisors, organizations, and others. The body of research and evaluation work has a strong emphasis on capacity building, both for grantees and for the research community as a whole. This ensures that high-quality work will continue to support the field. HRSA and ACF have also emphasized dissemination through translating research into formats that will be used and useful to the practice community. Ultimately, the research and evaluation activities are intended to be meaningful to both the research and the practice communities. A
Lauren H. Supplee, PhD, is a senior social science research analyst within the Division of Family Strengthening in the Office of Planning, Research and Evaluation for the Administration for Children and Families. She is the home visiting research team lead. At the Office of Planning, Research and Evaluation her portfolio includes projects such as: Head Start CARES, a national group-randomized trial of evidence-based social–emotional promotion programs in Head Start classrooms; Home Visiting Evidence of Effectiveness (HomVEE), a transparent systematic review of the evidence on home visitation programs; Mothers and Infants Home Visiting Program Evaluation (MIHOPE), a Congressionally mandated national evaluation of the new Maternal, Infant and Early Childhood Home Visiting program; MIHOPE-SS, an evaluation in partnership with Centers for Medicaid and Medicare Services Strong Start Initiative; the Society for Research in Child Development Policy Fellowship project officer; and she co-leads the federal Interagency Workgroup on Research on Evidence-Based Policies and Programs. She received her doctorate from
References
Lee, S., Aos, S., Drake, E., Pennucci, A.,
Miller, M., & Anderson, L. (2012). Return on investment: Evidence-based options to improve statewide outcomes. Olympia: Washington State Institute for Public Policy. Retrieved August 20, 2012, from www.wsipp.wa.gov/pub.asp?docid=12-04-1201
Patient Protection and Affordable Care Act.
(2010). Pub. L. No. 111-148, §2702, 124 Stat. 119, 318–319.
Paulsell, D., DelGrosso, P., & Supplee, L. H.
(2012). Supporting replication and scale-up of evidence-based programs: Assessing the implementation knowledge base. Manuscript in preparation for publication.
Stoltzfus, E., & Lynch, K. (2009). Home visitation for families with young children. Washington, DC: Congressional Research Service.
Strader, K., Counts, J., & Filene, J. (2013) Federal home visiting under the Affordable Care Act. Zero to Three, 33(3), 51–57.
Weiss, H. B. (1993). Home visits: Necessary but not sufficient. The Future of Children 3(3), 113–128.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5 1
Federal Home Visiting Under the Affordable Care Act
KATHLEEN STRADERZERO TO THREE
Washington, DC
JACQUELINE COUNTSHealth Resources and Services Administration
Kansas City, Missouri
JILL FILENEJames Bell Associates
Arlington, Virginia
Holly fondly remembers receiving support from a home visitor while pregnant with her son. With her husband deployed in Iraq, she lived near a remote military base more than 12 hours from any family. Guidance received from her home visitor still sticks with her today, “Parenting is tough, no one has all the answers, and it is okay not to know everything.”
That message helped motivate Holly to become a home visitor years later when the opportunity arose with the recent Maternal, Infant, and Early Childhood Home Visiting (MIECHV) effort in her home state of Ohio.
AbstractThe Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Program is part of The Patient Protection and Affordable Care Act and provides $1.5 billion over 5 years to states, territories, and tribes with the goal of delivering evidence-based home visiting services as part of a high-quality, comprehensive early childhood system that promotes health and well-being for pregnant women, parents, caregivers, and children from birth to 5 years old. The authors share promising results through anecdotal information from families, states, and tribes on progress made thus far.
Holly does not suggest she now knows everything about parenting, but she has been “paying it forward” with parents like Ashley and Jonathon. Both parents stress they ini-tially were “not interested” and “leery” about having a home visitor, adding “We just don’t get involved in things like that.” Ashley was in her doctor’s office, pregnant with her second child, when she was greeted by a persua-sive program person handing out flyers. “She explained how the program could help us get connected to different resources,” Ashley says. With some reluctance, they decided to give it a try. Eight months later, they credit the program with helping them make signifi-cant strides.
Jonathon, Ashley, and their two children, Madison (3 years) and Peyton (6 months) live in Pike County, Ohio. According to 2011 statistics, Pike County has one of the worst mortality rates in Ohio (84th out of Ohio’s 88 counties) and ranks at the very bottom (88th out of 88 counties) for high school graduation rate, unemployment rate, number of children living in poverty, and number of single parent households (Ohio’s Kids Count, 2011). Jonathon and Ashley’s situation was particularly challenging because neither was employed and they were without a car. They live in a community with very limited public transportation, and services like health care and groceries are 30–45 minutes away. Since
Holly has started working with the family, she has shared child development information and parenting tips. She has also helped them achieve goals, such as getting a car. Taking one step at a time, they identified a plan to get a job and to set and stick to a budget, which allowed them to save enough to buy a car. In
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

5 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
evidence-based or promising approach home visiting services, establishing data collection and continuous quality improvement (CQI) processes, strengthening linkages and coor-dination with other services, and assessing outcomes.
The HRSA and ACF collaboration uses a multipronged approach intended to pro-mote a culture of learning that fosters grantee ownership of MIECHV priorities. First, col-laborative decision-making at the federal level models how state and local entities can organize around a collective impact frame-work, by focusing on achievement of broad cross-sector coordination instead of focusing on the isolated interventions of individ-ual organizations (Kania & Kramer, 2011). Second, the federal and regional project offi-cers, who are responsible for most closely overseeing the grants, provide ongoing con-sultation and monitoring, serving as a conduit through which federal expectations are com-municated to grantees, and a link to support grantees’ receipt of technical assistance (TA). Finally, HRSA and ACF are working to cre-ate an integrated system of TA providers that are capable of providing TA at whatever level of intensity a grantee needs, from gen-eral webinars open to all grantees and smaller cross-state communities of practice around specific issues, to intensive and targeted TA with individual grantees.
Home Visiting Can Make a Difference
Research has found that factors such as neglect, abuse, and household dysfunction experienced during
childhood contribute to poor physical and
based home visiting models and promising home visiting approaches. MIECHV was established as part of The Patient Protection and Affordable Care Act (2010) and provides $1.5 billion over 5 years to states, territories, and tribes to provide home visiting services for at-risk pregnant women and children from birth to 5 years old. The Act stipulates that at least 75% of the funds received by states must be used for home visiting programs with evidence of effectiveness based on rigorous evaluation research. To date, 12 home visiting models have met the evidence of effectiveness criteria defined by the U.S. Department of Health and Human Services (HHS) as required by the legislation (see box 12 Evidence-Based Home Visiting Models). All 50 states, the District of Columbia, and the five U.S. territories were eligible to apply for state grants administered by the Health Resources and Services Administration (HRSA). MIECHV grants to Indian tribes, tribal organizations, and urban Indian organizations are administered by the Administration for Children and Families (ACF). HRSA and ACF are agencies within HHS.
As outlined in the Affordable Care Act leg-islation, a goal of the MIECHV program is the integration of home visiting services into a high quality, comprehensive early childhood system that promotes health and well-being for pregnant women, parents, caregivers, and children from birth to 5 years old (HRSA, n.d.). To this end, HRSA and ACF are working closely to develop congruent policy, practice, and research agendas that support the capac-ity-building efforts of grantees. The intent of these efforts is to support states, territo-ries, and tribes in meeting requirements for
addition, Ashley starts college in January. Jonathon says, “We’ve learned to be patient, things don’t always happen as fast as you want them to, but will happen if you stick to it.”
Jonathon and Ashley are passionate when talking about their children and family life. Ashley says “I wish I would have had this sup-port when I was pregnant with Madison. I was a lot healthier during this last pregnancy, because Holly was there reminding me to eat healthier and take care of myself. And I doubt Madison would be starting preschool now if not for Holly.” Jonathon says being involved with the program “has opened so many doors for us” and “our family is so much stronger. We do so many more things together as a fam-ily now. We love the program. My children are learning, just like we have now learned, that you don’t have to be afraid to ask for help.” When asked how they got over their initial reluctance to be involved in a program like this, both parents are quick to state, “Our worker really cares about us. She is there for us, and it doesn’t matter what kind of ques-tions we have…right from the first visit she was genuinely interested in us.” MIECHV-funded home visiting programs like the one in Pike County, Ohio, aim to strengthen parent–child relationships, increase family economic self-sufficiency, support enriched child-learning environments, and reduce social isolation.
What Is MIECHV?
A lthough the pronunciation of MIECHV may vary around the country, the meaning is the same:
the program is an unprecedented federal investment in the nation’s youngest children through the implementation of evidence-
Guidance Holly (left) received from her home visitor still sticks with her today, “Parenting is tough, no one has all the answers, and it is okay not to know everything.” That message helped motivate Holly to become a home visitor years later.
Ph
ot
o: T
am
my
F
yf
fe
12 Evidence-Based Home
Visiting Models
Adolescent Mothers (EIP)
Preschool Youngsters (HIPPY)
(PALS)
Evidence–based models approved by U.S. Department of Health and Human Services as of 11/1/12
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5 3
assessment. Results of the survey showed that, although home visiting services were being provided across the state, there was significant variability in these services, including number of visits, eligibility, fidelity, curriculum, intensity, intake, and duration. State administrators report that, prior to MIECHV, the Nebraska Department of Health and Human Services had limited experience with large-scale implementation of evidence-based home visiting programming. In addition, they noted a lack of capacity and infrastructure to implement such models with fidelity, along with limited data available to demonstrate evidence of positive outcomes.
On the basis of the needs assessment in their MIECHV plan, Nebraska chose to focus on one rural area in western Nebraska to develop local capacity to implement an evidence-based model with fidelity. Concurrently, Nebraska stakeholders collaborated to develop online home visiting training modules that are broad enough in scope to provide basic information across a variety of MIECHV and non-MIECHV funded home visiting models and accessible to rural and urban areas. The Nebraska team said they plan to address data gaps by developing a shared measurement system to document outcomes for the children and families served by home visiting programs. Nebraska state administrators stated that they now embrace a continuous improvement philosophy, and the result is a focused approach that first assesses community readiness to implement an evidence-based program and then provides appropriate infrastructure supports.
get, and Solveig has helped big time.”
Scaling Up: A State Experience
A s part of the MIECHV grant application process, each state, territory, and tribal grantee was
required to complete a comprehensive needs assessment. This process was intended to maximize the use of available funds by identifying the highest risk communities to which MIECHV home visiting funds could be directed.
In Nebraska—a state that, according to state MIECHV administrators, values fiscal prudence, local choice, and early childhood—some of its early childhood leaders joined forces as Together for Kids and Families (TFKF) and developed a systems approach that knit together programmatic goals, fund-ing streams, and infrastructure elements. They crafted a strategic plan as part of their Early Childhood Comprehensive Systems ini-tiative, a federal grant program designed to help states and communities build and inte-grate early childhood service systems to better meet the needs of children and fami-lies. Ultimately the TFKF strategic plan was adopted as the early childhood strategic plan for the entire state.
State administrators reported that having the TFKF plan already in place when the MIECHV legislation was enacted meant that Nebraska was poised to take action. For example, TFKF had previously conducted a survey to determine the number of home visitation programs, their locations, and the services provided. This work formed part of the foundation for the MIECHV needs
mental health decades later as an adult (Felitti et al., 1998). Home visiting has a long history of delivering services to pregnant women and families with young children to prevent child abuse and neglect, promote child and family health, support parenting, and promote education for both children and their parents (Daro, 2009; Gomby, 1999). A recent review of the home visiting research literature found that home visiting programs can improve outcomes for young children and their families (Paulsell, Avellar, Sama Martin, & Del Grosso, 2011). Because of this strong research base, there has been a growing emphasis on the use of evidence-based home visiting models (Boller, Strong, & Daro, 2010). Knowledge of the sustained and detrimental results of negative early childhood experiences—and the evidence that culturally sensitive, relationship-based home visiting can mitigate these effects— are convincing motivators for implementing evidence-based home visiting programs focused on pregnant women and families of infants and young children.
Another Family Shares Their Story
Helen and Isaac live in Anchorage, Alaska, with their 1-month-old son, Ray. They each have an older daughter (6 and 4 years old, respectively) with a previous partner, though neither of the older children currently resides with Helen and Isaac. As Helen described it, having not taken care of a child in a long time, she felt unprepared to parent a new baby. This feeling was intensified because she had just moved to Anchorage when she became pregnant, and she had no one to turn to for help. And Helen and Isaac say they were in desperate need of help. Lack of finances and housing were huge stressors. When Helen was 4 months pregnant, her prenatal care provider connected her to Nutaqsiivik (which means “a place of renewal”), a program of nurse home visitors in Anchorage that is part of the tribal health system. The program serves Alaska Native and American Indian pregnant women with recent funding support from a tribal MIECHV grant.
Solveig, a nurse home visitor, became involved with the family at that time, providing support and education and extending their formal support system by connecting them to many needed services. Now, Helen and Isaac say life has improved dramatically and they can’t imagine what it would have been like if Solveig had not been involved. Helen and Isaac report having a healthy baby boy, a place of their own to live, and some income (Isaac has a part-time job). Helen describes that with regular visits from Solveig, she has learned how to take care of Ray and to successfully breastfeed. As Isaac described, “we needed all the help we could
The Maternal, Infant, and Early Childhood Home Visiting program is an unprecedented federal investment in the nation’s youngest children through the implementation of evidence-based home visiting models and promising home visiting approaches.
Ph
ot
o: T
am
my
F
yf
fe
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

5 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
The MIECHV Technical Assistance Coordinating Center (MIECHV TACC)
The TACC provides support to grantees to implement MIECHV-funded home visiting programs. Supportive services include (a) facilitating connections with technical experts; (b) offering opportunities for shared learning; (c) promoting the integration of home visiting within statewide comprehen-sive early childhood systems; (d) identifying best practices; (e) helping grantees develop leadership skills and sustain strong inter-agency collaborations; (f ) incorporating key strategies around issues such as workforce development systems, centralized intake sys-tems, a continuum of home visiting models/services, challenges of working with especially vulnerable populations, financial strategizing and fiscal sustainability planning; and, (g) assisting the advancement of all program models by creating robust research-to-practice and peer-to-peer learning communities for evidence-based home visiting model develop-ers. Services are provided in multiple formats including webinars, phone calls, email, an interactive Web site portal, along with in-
formal Memorandums of Understanding established, the stage is set for continued col-laborative and integrated efforts in the future.
A National Strategy
A ny effort to take home visiting programs to scale faces inherent challenges related to infrastructure
development and ensuring consistent implementation across multiple models and multiple disciplines. But MIECHV also involves integrating state-level home visiting within a comprehensive early childhood system and has rigorous measurement requirements (see box Maternal, Infant, and Early Childhood Home Visiting Measurement Requirements). These dimensions increase the complexity of scale-up efforts.
Each grantee has developed an individu-alized plan for use of MIECHV funds, and all are expected to reach new heights, whether expanding geographic areas served, adding new models, implementing service enhance-ments to existing models, or establishing more comprehensive data systems. To pro-vide additional support to grantees in this work, HRSA and ACF have established a net-work of MIECHV TA providers (see box Maternal, Infant, and Early Childhood Home Visiting Technical Assistance Providers).
Scaling Up: A Tribal Experience
W ith their Tribal MIEHCV grant, San Felipe Pueblo in New Mexico created Project KEVA
(Katishtya Eh-wahs Valued Always), which is implementing Family Spirit, a 15-month home visiting program administered by Native paraprofessionals and designed to promote maternal and child health and parent education for adolescent and first-time parents. With Family Spirit model developers, Project KEVA is adapting the program to make it more culturally relevant for their tribe. For example, they are incorporating their native language, Keresan, into every lesson and encouraging parents to speak to their children in their native tongue. They are also working storytelling into the lessons and teaching traditional child-rearing techniques to which this younger generation of parents has not necessarily been exposed, such as how to use a wrap to carry a child on the parent’s back. These cultural adaptations strengthen the connections between the participants and their tribal elders and traditions.
Project KEVA has hired a cultural advisor whose primary responsibility is to ensure the cultural appropriateness of the program. To achieve this task, the cultural advisor works in collaboration with the program coordinator, the parent educators, and the cultural advisory committee (which is comprised of tribal mem-bers, tribal leaders, and representatives from other early childhood programs in San Felipe Pueblo). In addition, the cultural advisor is responsible for continually looking for ways to improve or adapt the program to make it more effective, efficient, and culturally appropriate.
During their first year of funding, Project KEVA staff reported that they concentrated in part on building relationships and connec-tions with other early childhood programs serving San Felipe Pueblo, such as Head Start, child care, family services, behavioral health, and the Woman, Infants and Children pro-gram. The project’s referral system connects families to other needed services and uses a team approach with these agencies to provide coordinated care. Project KEVA also devel-oped a task force, comprised of tribal elders and representatives from the other early childhood programs, that meets monthly to discuss and resolve any issues that arise during implementation of Project KEVA. Staff report that, based on their positive experience with this task force, other early childhood programs have started similar task forces for their programs, in which MIECHV staff participate. According to Project KEVA staff, this work has significantly strengthened San Felipe Pueblo’s integrated system of care for young children and families that was in its infancy when they first received MIECHV funding. With the connections made and
Maternal, Infant, and
Early Childhood Home
Visiting (MIECHV)
Measurement
Requirements
The legislation states that all grantees
supported with MIECHV funds must
collect quantifiable data for all families
enrolled in the program across six
benchmark areas:
1. maternal and newborn health;
2. child injuries, child abuse, neglect, or
maltreatment, and emergency
department visits;
3. school readiness and achievement;
4. crime or domestic violence;
5. family economic self-sufficiency; and
6. the coordination and referrals for other
community resources and supports.
Grantees are expected to demonstrate
improvements in four of the six benchmark
areas by October 2014 (Year Three of the
program). Each benchmark area includes
multiple constructs, and HHS has defined
improvement in a benchmark area as
demonstrating improvement in at least
half of the constructs within a benchmark
area.
Maternal, Infant, and
Early Childhood Home
Visiting (MIECHV)
Technical Assistance
Providers
THREE in partnership with Association of
Maternal and Child Health Programs,
Chapin Hall at the University of Chicago,
and Walter R McDonald & Associates
http://mchb.hrsa.gov/programs/
homevisiting/ta/index.html
Evaluation (DOHVE) at MDRC, James
Bell Associates, and the Cincinnati
Children’s Hospital Medical Center www.
mdrc.org/dohve/dohve_resources.html
Technical Assistance Center (VisTA) at
Walter R. McDonald & Associates, and
their partners, Chapel Hill Training-
Outreach Project, Inc.’s FRIENDS
National Resource Center for
Community-Based Child Abuse
Prevention, and Arizona State University’s
Office of American Indian Projects at the
School of Social Work
Institute (TEI) at MDRC, James Bell
Associates, Johns Hopkins University and
University of Colorado at Denver
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5 5
an increased focus on data and outcomes for children and families at the community-level (see box Online Benchmark Resources).
In addition, some grantees are building on their MIECHV program through state policy and practice intended to improve the quality of home visiting services. Iowa, Maryland, and Michigan have recently passed legislation that directs state general funds toward evidence-based home visiting programs. Specifically, Iowa passed legislation requiring that 90% of state funding for family support programs tar-geting children birth to 5 years old be allocated to programs that meet the MIECHV defini-tion of evidence-based or promising programs by July 1, 2016. In addition, beginning in 2014, Iowa will require that family support programs
research and evaluation of MIECHV initia-tives that serve AIAN children and families. TEI conducts activities that support tribal grantees to identify and develop effective practices and systems for integrated services for home visiting in tribal communities. Focal areas include: (a) developing and implement-ing a rigorous evaluation of home visiting; (b) selecting, adapting, and developing cul-turally appropriate data collection tools and measures; (c) tracking and measuring bench-marks; (d) developing and modifying existing data systems; (e) CQI; (f ) data protection and privacy; (g) ethical dissemination and trans-lation of evaluation findings derived from research with AIAN to external audiences; and, (g) working with grantees on efforts to disseminate and share.
Federal Research and Evaluation Activities
In addition to TA, HRSA and ACF are also supporting the implementation of MIECHV through a set of rigorous research and eval-uation activities. For instance, a national evaluation, Mother and Infant Home Visiting Program Evaluation, is being conducted; Home Visiting Research Network has been created to support the development of a national research agenda to advance the field; and an investigator-initiated research grant program has been established (Supplee, Harwood, Margie, & Meyer, this issue, p. 45).
Building on Opportunity and Potential
A s detailed in the family, state, and tribal examples above, the work that grantees have done to date—with
the support of HRSA, ACF, model develop-ers, and TA providers—is already providing meaningful help to families. In addition, state administrators report that the process of developing benchmark data collection plans, a federally required activity, provided opportunities for improved relationships and collaboration between state agencies, local home visiting program sites, and other com-munity organizations. For example, many grantees developed data workgroups or advi-sory committees with members from local program sites and other community organiza-tions and agencies across various disciplines such as education, maternal and child health, child welfare, and law enforcement. These groups enabled grantees to build on the knowledge and expertise of a larger group of stakeholders to ensure that benchmark plans are contextually and culturally appropriate and are coordinated with other early child-hood programs and initiatives in the state, as a critical component to a long-term system of care strategy. State administrators report that cross-agency collaboration has also led to
person opportunities for regional meetings and individual on-site support.
Design Options for Home Visiting Evaluation (DOHVE)
DOHVE provides research- and evalua-tion-related TA and assists MIECHV grantees with: (a) developing plans for collecting data on benchmarks; (b) designing and strength-ening evaluations of promising approaches and evaluations being done as part of compet-itive grant projects; (c) selecting, adapting, and developing data collection tools and measures; (d) developing and adapting data systems to facilitate tracking and reporting on federal benchmarks; (e) designing and imple-menting CQI systems; and, (f ) establishing data protection and privacy policies and pro-cedures. TA is provided through webinars; facilitated group calls with multiple grant-ees; technical assistance briefs; and individual grantee calls, meetings, and written feedback.
Tribal Home Visiting Training and Technical Assistance Center (VisTA)
Tribal Home VisTA provides TA and train-ing services for tribal grantees to support the implementation of evidence-based practices and promising approaches within tribal com-munities. The overall goal of VisTA is to build the capacity of the tribal grantees to conduct activities such as strategic planning, train-ing, and CQI to implement evidence-based programs effectively and with fidelity. VisTA works with grantees to promote excellence in community-based maternal, infant, and early childhood initiatives; systems of care for health and well-being promotion; and systems that support parent, family, and community engagement. VisTA employs an “empowerment” TA approach. VisTA views the core principles of empowerment TA as: (a) emphasizing capacity-building for grant-ees; (b) committing to American Indian and Alaska Native (AIAN) community ownership of TA; (c) fostering the inclusion of multiple stakeholders to achieve the goals and bench-marks of the program; (d) maintaining a focus on program improvement; (e) promoting democratic participation in the determination and analysis of TA needs and delivery chan-nels and content; (f ) facilitating the interplay of community knowledge and the transla-tion of evidence-based practice to social and cultural realities; (g) encouraging commu-nity, organizational, and program learning; (h) respecting issues of economic and social justice; and, (i) sustaining accountability to multiple stakeholders.
Tribal Home Visiting Evaluation Institute (TEI)
TEI provides TA, leadership, and support to promote excellence in community-based
Online Benchmark
Resources
Resources developed by Design Options
for Home Visiting Evaluation (DOHVE) to
identify standardized measurement tools
and minimize data collection burden
1. Evidence-Based Model Crosswalk to
Benchmarks
2. The DOHVE Compendium of
Measurement Tools for Maternal, Infant,
and Early Childhood Home Visiting
(MIECHV) Grantees
3. The Benchmark Constructs Crosswalk
to Compendium of Measurement Tools
for MIECHV Grantees
Source: www.mdrc.org/dohve/dohve_
resources.html
Helen, Isaac, and baby Ray. Helen describes that with regular visits from their home visitor, she has learned how to take care of Ray and to successfully breastfeed.
Ph
ot
o: S
ol
ve
ig
J
oh
ns
on
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

5 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Kathleen Strader, MSW, IMH-E® is assistant director, Maternal, Infant, and Early Childhood Home Visiting (MIECHV) Technical Assistance Coordinating Center (TACC) at ZERO TO THREE. Kathleen provides direction and oversight to the technical assistance (TA) work of the TACC, including supervision of TACC TA specialists and senior information specialist, and the coordination of TA from other resources including numer-ous national content experts that are part of an approved consultant pool working with TACC. She has been in the home visiting field for more than 20 years, working at the local, state, and national levels providing training and TA related to the implemen-tation of an evidence-based home visiting model.
Jacqueline Counts, MSW, PhD, is Region VII project officer for the Early Childhood Health and Development Branch of the Maternal Child Health Bureau of Health Resources and Services Administration (HRSA). She serves as a project officer for the Maternal, Infant, and Early Childhood Home Visiting Program and the Early Childhood Comprehensive Systems grants. In addition to project officer responsibili-ties, she is also involved with the Data Reporting and Technical Assistance workgroups. Prior to coming to HRSA, Dr. Counts served as the asso-ciate director of programming at the Institute for Educational Research and Public Service, University of Kansas. She was principal inves-tigator on numerous early childhood and child maltreatment prevention projects, including the Early Childhood Comprehensive Systems evalua-tion, Project LAUNCH, Community-based Child Abuse and Neglect, several National Governor’s Association early childhood grants, and others. She also designed an accountability framework for the Children’s Initiative Fund or Tobacco Master Settlement in Kansas. The framework included an evidence-based rating for each funded program, review of the evaluation design, and impact of the funding. Counts has extensive experience con-ducting and presenting research, including the development of the Protective Factors Survey.
Jill Filene, MPH, is senior research associ-ate at James Bell Associates. She has more than 15 years of experience in applied research, pro-gram evaluation, and technical assistance (TA) to home visitation, child maltreatment preven-tion, and early childhood development programs. Ms. Filene currently directs the Design Options for Home Visiting Evaluation TA project and works on the Mother and Infant Home Visiting Program Evaluation study. She recently completed two meta-analyses examining components associated with effective home visiting and parent training programs for pregnant women and families with young children.
a larger early childhood system, extending the reach of home visiting services to fam-ilies beyond those that can be served with MIECHV funds alone. States are redesigning shared data systems; initiating compre-hensive interagency centralized intake, screening, and referral processes; structur-ing CQI through local and state committees to review progress on benchmarks and implementation with fidelity; establish-ing cross-discipline workforce development strategies; and preparing fiscal sustainability plans, and much more.
Another aim of the MIECHV program is to conduct and use research and evaluation not only to inform and improve MIECHV efforts but to contribute to the broader knowledge base and advance the field of home visiting. To that end, TA has been provided using mul-tiple modalities to assist grantees regardless of their initial capacity and has sought to par-allel the same trusting relationship that is promoted between home visitors and fami-lies. As simply stated by Holly, “it is okay not to know everything.” The work that has been done to build collaborative relationships between HRSA and ACF, the TA providers, and grantees is intended to create a culture where it is “okay to ask for help”, which in turn will support the development of a home visiting system that can be sustained over the long-term and achieve improvements in maternal and child health, school readi-ness, family economic self-sufficiency, and prevention of child maltreatment and family violence. A
funded by the state participate in a Web-based data collection system and implement a coordinated intake process. The legisla-tion also establishes minimum competency requirements for family support workers and supervisors and background check require-ments for family support workers.
Maryland and Michigan passed similar leg-islation based on the MIECHV evidence-based definitions and require that the states sup-port only evidence-based and promising home visiting programs for improving parent and child outcomes with state funding. Both states aligned the state home visiting outcomes with the MIECHV legislative outcomes and require regular reports on investments in home visit-ing beginning in December 2013.
Conclusion
W hile much work is yet to be done, grantees report significant early achievements and an encour-
aging outlook. Many grantees are creating a coordinated system of home visiting services using multiple models as a way to address the unique needs of families in high-risk com-munities. Similarly, the identification of a measurement plan to report outcomes across programs is a daunting task that many grant-ees have been working on for years and have now accomplished through MIECHV bench-mark requirements.
State administrators report that MIECHV funding and structural components are pro-viding an opportunity for grantees to build home visiting systems that are woven within
Jonathon says being involved with the home visiting program “has opened so many doors for us” and “our family is so much stronger. We do so many more things together as a family now.”
Ph
ot
o: T
am
my
F
yf
fe
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5 7
References
Boller, K., Strong, D. A., & Daro, D. (2010). Home visiting: Looking back and moving forward. Zero to Three, 30(6), 4–9.
Daro, D. (2009). Hearing on proposals to provide federal funding for early childhood home visitation programs. Written testimony for the House Subcommittee on Income Security and Family Support, Committee on Ways and Means.
Felitti, V., Anda, R., Nordenberg, D,
Williamson, D., Spitz, A. Edwards, V.,
Koss, M., & Marks, J. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. American Journal of Preventive Medicine, 14(4), 245–258.
Gomby, D. S. (1999). Understanding evaluations of home visiting programs. Future of Children, 9(1), 27–43.
Health Resources and Services Administration
(HRSA). (n.d.). Maternal, Infant, and Early Childhood Home Visiting Program. Retrieved November 19, 2012, from http://mchb.hrsa.gov/programs/homevisiting/
Kania, J., & Kramer, M. (2011) Collective impact. The Stanford Social Innovation Review, Winter, 36–41.
Ohio’s Kids Count. (2011). 2011 Data Book. Children’s Defense Fund – Ohio. Retrieved October 14, 2012, from www.cdfohio.org/assets/pdf-files/kids-count-update-7-5.pdf
Patient Protection and Affordable Care Act.
(2012). Pub. Law No.111-148. Government
Publications Office Web site. www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf
Paulsell, D., Avellar, S., Sama Martin, E., &
Del Grosso, P. (2011). Home Visiting Evidence of Effectiveness review: Executive summary. Office of Planning, Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services. Washington, DC. Retrieved September 10, 2012, from http://homvee.acf.hhs.gov/HomVEE_ExecutiveSummary_Rev10-15-2011.pdf
Supplee, L. H., Harwood, R. L., Margie, N. G.,
& Meyer, A. (2012). New opportunities and directions in home visiting research and evaluation. Zero to Three, 33(3), 45–50.
To order call toll-free 1-800-499-4301 www.zerotothree.org/bookstore
Bestselling Video Training Tools
Learning Happens features children with parents
30 VIGNETTESAPPROX. 60 MIN. ITEM: V507$26.99
Learning Happens 2features children with teachers and caregivers 25 VIGNETTES APPROX. 29 MIN. ITEM: V509 $22.95
Buy both and save!Order both
DVDs for only $40
A 20% SAVINGSITEM: V510
TheThe Learning HappensLearning Happens DVDs are DVDs arethe perfect toolsthe perfect tools
for your own enrichmentfor your own enrichment
for professional developmentfor professional developmentwith all levels of your staffwith all levels of your staff
for your work with familiesfor your work with families
Video clips show real-life interactions andVideo clips show real-life interactions andare presented without narration—makingare presented without narration—makingthem perfect for use in training.them perfect for use in training.
Each DVD includes a booklet whichEach DVD includes a booklet whichdescribes the video vignettes and presentsdescribes the video vignettes and presentsdiscussion questions to help you analyzediscussion questions to help you analyzethe videos.the videos.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
5 8 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Perspectives
Maternal Engagement in Home Visiting
The MOM Program
JERILYNN RADCLIFFEUniversity of Pennsylvania
DONALD F. SCHWARZ City of Philadelphia, Pennyslvania
Olds, Sadler, & Kitzman, 2007). However, maternal involvement requires more than simply remaining in a program until its completion (Korfmacher et al., 2008; Raikes et al., 2006). Receiving an acceptable level of services is also necessary for mothers to receive the benefits of program participation. Service “dosage” has been less often reported in the home visiting literature, but published reports have described rates of program dosage that range from 27% to 85% (Heinrichs, 2006; McFarlane et al., 2010). Even less has been reported in the home visiting literature on the staff effort required to promote mothers’ program participation, or to evaluate how these staff activities affect program outcomes. A better understanding of the relationship between staffing patterns, training, and outreach activities and maternal program involvement may lead to more targeted efforts to involve mothers in the home visiting intervention, and ultimately, to improved program outcomes.
The MOM Program
The MOM Program is an innovative home visiting program whose aim is to empower low-income urban mothers
to obtain health and early intervention services for their children (Schwarz et al., 2012). In the MOM program, mothers receive home visits
“risk” status (Fergusson, Grant, Horwood, & Ridder, 2006; Olds et al., 2002).
Home visiting programs have reported success in improving child and maternal health outcomes, child cognitive outcomes, delay of subsequent pregnancies, increased rates of maternal employment, and increases in subsequent family income (American Academy of Pediatrics Council on Child and Adolescent Health, 1998; Howard & Brooks-Gunn, 2009; Olds et al., 1997; Olds et al., 1999; Olds, Kitzman et al., 2007).
Evaluating Maternal Engagement
It is not surprising that, because of the variability among home visiting programs, mothers’ involvement
with the programs has been evaluated in a number of different ways. The most common approach to evaluating maternal involvement in home visiting programs has been to report retention rates for those who enroll in the programs (Paulsell et al., 2011). Typically, 50% of those mothers who enroll in home visiting programs complete the program, although well-established home visiting programs have reported retention rates that range from 20% upwards to 85%, (Gomby, 2005; Heinrichs, 2006; McFarlane et al., 2010;
Home visiting programs help moth-ers develop a clear understanding of the importance of health and developmental services as well as competence and persis-tence in accessing these services. However, for home visiting services to be effective in developing these and other skills, mothers must be well engaged in the program, both initially and on an ongoing basis.
An extensive literature supports the effectiveness of home visiting programs in promoting positive outcomes for mothers and children (Howard & Brooks-Gunn, 2009; Olds, Sadler, & Kitzman, 2007; Paulsell, Avellar, Sama Martin, & Del Grosso, 2011). Although these pro-grams have generally targeted mothers who are viewed as “at risk” for poor out-comes because of their age, income, or identified psychosocial issues, the specific target populations, goals, and outcomes of home visiting programs vary widely. Target populations for home visiting programs have included teen mothers (Barnet, Liu, DeVoe, Alperovitz-Bichell, & Duggan, 2007; Koniak-Griffin, Anderson, Verzemnieks, & Brecht, 2000), first-time mothers (Olds et al., 1997; Olds et al., 1999; Olds, Kitzman et al., 2007), mothers at risk for child abuse (Duggan et al., 1999), or mothers with a variety of indicators of
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 5 9
week. It is important to note that home visitors’ frustration from repeated failures to connect with an individual mother appear to be reduced when another home visitor steps in to help. The MOM program has never stopped attempting to contact participants unless a mother asks to be removed from the program. Home visitors keep detailed records of their efforts to contact mothers, noting the date, time, and outcome of each attempted contact.
Understanding Maternal Engagement
A recent evaluation of the MOM program sought to examine mater-nal involvement in the program.
We defined maternal involvement as including two components, program reten-tion (remaining in the program throughout its 33 month duration) and target pro-gram dosage (receiving at least 75% of the planned home visits). We examined the relationship between maternal involve-ment and other factors, including maternal demographic characteristics, child char-acteristics, and program activity. One area of focus was the the relationship between staff outreach activities and maternal pro-gram involvement.
a high level of training that includes group training and role play, the use of a procedure manual, and specific checklists for each home visit. The MOM program also created train-ing videotapes.
The MOM program holds a weekly group supervison meeting that includes all home visiting staff, as well as a multidisciplinary group of supervisors whose disciplines include pediatrics, nursing, and in original version of the program described here, psychology. Participants in the meetings review the progress of each mother in the program and attempt to solve any issues that arose in service delivery. The MOM program encourages home visitors to contact mothers in a variety of ways. These range from calling mothers at varying times (including weekends), using alternative contacts the mothers had provided when they enrolled in the program, or simply stopping by without an appointment at the mothers’ homes. Staff have sent brightly colored postcards with the message, “We miss you,” to hard-to-reach mothers. Having several staff members attempt to contact mothers was a strategy that proved effective in several ways. Sometimes mothers are more responsive to having a different style of voicemail left for them, or being called at a different time or day of the
just prior to the child’s scheduled primary health care visit on a schedule consistent with the recommendations of the American Academy of Pediatrics (2000). During the visits, home visitors follow a manualized visit protocol that includes providing information on what to expect at the upcoming health care visit in terms of immunizations and other procedures. The home visitors also review developmental expectations and discuss with mothers how their children are meeting these milestones. Home visitiors encourage mothers to plan questions for the health care provider about their child’s health and development. Mothers are to receive nine home visits over 33 months. If a child is found to have developmental delays, the MOM program provides two additional visits. The purpose of these additional visits is to support mothers in contacting an early intervention provider and completing the requisite screening visits and intervention planning.
In addition to the nine home visits, MOM staff also make frequent reminder telephone calls to the mothers. The home visitors remind mothers of upcoming home visits and health care visits. After a scheduled health care visit, staff call to ask if the visit occurred, if the child received appropriate immunizations, and if there were recommendations for developmental services. The MOM staff continue to call the mothers until all recommended services have been completed. For example, mothers receive a follow-up call if a well-child visit did not occur (to remind them to reschedule the appointment), if the child did not receive all of the recommended immunizations (to remind them to schedule another visit), or if developmental services were recommended (to remind them to contact or follow through with the early intervention provider).
The MOM team of home visitors currently includes nine home vistors, with a mix of nurses and trained community workers. (The original program had two nurse practitioners and two trained community workers.) The nurse practitioners and community workers alternate home visits with the mothers. The rationale for using a team approach is to offer participating mothers exposure to a range of interpersonal styles, and to ensure that if a staff member were to leave the program, each mother would have other staff mem-bers who were familiar to her. All staff receive
An extensive literature supports the effectiveness of home visiting programs in promoting positive outcomes for mothers and children.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/h
ar
tc
re
at
io
ns
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

6 0 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Perspectives
The views of mothers who decide to drop out of home visiting programs are also important to consider. Future research should also explore particular mother–home visitor dynamics that lead mothers to drop out prematurely as well as sensitive points in time during a mother’s participation in home visiting when she may be particularly vulnerable to dropping out. By analyzing maternal involvement both qualitatively and quantitatively and including information from mothers who fail to connect with home visiting programs, the field’s efforts to study maternal involvement will be better positioned to inform the design of future home visiting programs.
Another way to maximize home visiting programs’ likelihood of success is to develop ways (a) to collect data throughout the course of service delivery and (b) to use data to evaluate the accomplishment of program goals, including maternal involvement. Examples of research questions might include: how many contacts, on average, are necessary to reach a mother in a home visiting program and how much time, on average, does it take to deliver a home visiting intervention? This information will not only allow for optimal staffing of home visiting programs but will provide concrete information that may motivate home visitors as they make the repeated efforts needed to connect with mothers in their programs. Such data will also help supervisors and policymakers, who must evaluate staff and program effort against program results. User-friendly software may prove to be a helpful innovation in implementing and tracking results from home visiting programs, because data on the number and amount of time making contacts will more easily obtained and utilized.
The results from our new and small home visiting program, the MOM Program, raise important questions and call for larger efforts to more fully understand how to effectively mitigate the negative effects of poverty on children’s health and development and to promote the well-being of all children, particularly those living in poverty. A
Jerilynn Radcliffe, PhD, is associate professor of clinical psychology in pediatrics at The Children’s Hospital of Philadelphia and the Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania.
Associates, 2001. Staff turnover has been associated with decreased program effec-tiveness and increased rates of parents dropping out (Gomby, 2005). Given the importance of staff retention in home vis-iting programs, particularly as this may relate to maternal retention, additional research should address the relationships between staffing patterns and maternal program involvement.
Future Directions
R esults from the MOM Program suggest the need to distinguish maternal, staffing, and program
activity variables as these relate to maternal involvement and overall program outcomes. One aspect of program participation that was not included in this study was the emotional attachment to the program by both staff and participants, which could be an important area to explore in future research on the effectiveness of home visiting programs. For example, Brookes and colleagues’ (2006) results from a qualitative study of mothers’ experiences and reactions to participating in a home visiting program illustrated how mothers’ relationships to the program develop over the course of their participation, with some mothers becoming more attached to the program over time.
Staffing Patterns, Training, and Outreach
There continues to be considerable debate in the field on the issue of what constitutes appropriate staff training back-ground in home visiting programs (Duggan et al., 1999; Korfmacher, O’Brien, Hiatt, & Olds, 1999; Olds et al., 2002). Although our results are based on a very small program with only four home visitors, our findings offer some preliminary support for the use of multidisciplinary teams of home visitors. In addition, weekly supervisory meetings were essential in maintaining program integrity for the MOM Program and for providing cross-disciplinary training that emphasizes staff collaboration around maternal outreach efforts. In particular, the home visiting staff appreciated hav-ing more than one staff member attempt to contact nonresponsive mothers. It is noteworthy that there was no staff turn-over among the MOM staff of four during the implementation of the original home visiting program. Staff turnover has been a widespread problem in home visiting programs. For example, Healthy Families America reported a turnover rate of 30–35% in 1 year (Klagholz & Associates, LLC, 2005; Williams, Stern, & Associates, 2005), and similar programs have reported turnover rates of about 70% across 18–36 months (Landsverk et al. 2002;LPC Consulting
Target populations for home visiting programs have included teen mothers.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/q
ua
vo
nd
o
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 6 1
chairman of the Department of Pediatrics. He now spearheads efforts to implement the MOM Program within the city of Philadelphia.
Donald F. Schwarz, MD, MPH, is deputy mayor for health and opportunity and health commissioner for the City of Philadelphia. Dr. Schwarz was the original director of the MOM Program at The Children’s Hospital of Philadelphia, where he also served as deputy
She has been part of the MOM Program since its inception in 1999, and has directed outcome research on the MOM Program since 2008. Dr. Radcliffe is a founding member of the Board of Directors of the Pennsylvania Association for Infant Mental Health.
References
American Academy of Pediatrics. (2000). Recommendations for preventative pediatric healthcare. Pediatrics, 105(3), 645–646.
American Academy of Pediatrics Council on
Child and Adolescent Health. (1998). The role of home-visitation programs in improv-ing health outcomes for children and families. Pediatrics, 101(3), 486-489.
Barnet, B., Liu, J., DeVoe, M., Alperovitz-
Bichell, K., & Duggan, A. (2007). Home visit-ing for adolescent mothers: Effects on parenting, maternal life course, and primary care linkage. Annals of Family Medicine, 5(3), 224–232.
Brookes, S. J., Summers, J. A., Thornburg, K. R.,
Ispa, J. M., & Lane, V .J. (2006). Building suc-cessful home visitor-mother relationships and reaching program goals in two Early Head Start programs: A qualitative look at contributing fac-tors. Early Childhood Research Quarterly, 21, 25–45.
Duggan, A. K., McFarlane, E. C., Windham, A. M.,
Rohde, C. A., Salkever, D. S., Fuddy, L., &
Sia, C. J. (1999). Evaluation of Hawaii’s healthy start program. The Future of Children, 9(1), 66–90.
Fergusson, D. M., Grant, H., Horwood, L. J., &
Ridder, E. M. (2006). Randomized trial of the Early Start Program of Home Visitation: Parent and family outcomes. Pediatrics, 117, 781–787.
Gomby, D. S. (2005, July). Home visitation in 2005: Outcomes for children and parents (Invest in Kids Working Paper No. 7). Sunnyvale, CA: Invest in Kids Working Group.
Heinrichs, N. (2006). The effects of two differ-ent incentives on recruitment rates of families into a prevention program. Journal of Primary Prevention, 27(4), 345–365.
Howard, K. S., & Brooks-Gunn, J. (2009). The role of home-visiting programs in preventing child abuse and neglect. The Future of Children, 19(2), 119–146.
Klagholz, D. D., & Associates, LLC. (2005). Healthy Families Montgomery Year 8 annual
evaluation report, FY 2003-2004. Retrieved from www.healthyfamiliesamerica.org/downloads/eval_hfmont_2004.pdf
Koniak-Griffin, D., Anderson, N., Verzemnieks, I.,
& Brecht, M. (2000). A public health nursing early intervention program for adolescent moth-ers: Outcomes from pregnancy through 6 weeks postpartum. Nursing Research, 49, 130–138.
Korfmacher, J., Green, B., Staerkel, F.,
Peterson, C., Cook, G., Roggman, L., …
Schieffman, R. (2008). Parent involvement in early childhood home visiting. Child Youth Care Forum, 37, 171–196.
Korfmacher, J., O’Brien, R., Hiatt, S., & Olds, D.
(1999). Differences in program implementation between nurses and paraprofessionals providing home visits during pregnancy and infancy: A ran-domized trial. American Journal of Public Health, 89, 1847–1851.
Landsverk, J., Carillio, T., Connelly, C.,
Leslie, L., Ganger, W., & Sylmen, D. (2002). Healthy Families San Diego clinical trial: Technical report. San Diego, California: Child and Adolescent Services Research Center, Children’s Hospital—San Diego.
LPC Consulting Associates. (2001). Birth and beyond: Year two report. Submitted to Department of Health and Human Services.
McFarlane, E., Burrell, L., Fuddy, L., Tandon, D.,
Derauf, D. C., Leaf, P., & Duggan, A. (2010). Association of home visitors’ and mothers’ attachment style with family engagement. Journal of Community Psychology, 38(5), 541–556.
Olds, D. L., Eckenrode, J., Henderson, C. R.,
Kitzman, H., Powers, J., Cole, R., …Luckey, D.
(1997). Long-term effects of home visitation on maternal life course and child abuse and neglect –fifteen-year follow-up of a randomized trial. Journal of the American Medical Association, 278(8), 637–643.
Olds, D. L., Henderson, C. R., Kitzman, H. J.,
Eckenrode, J. J., Cole, R. E., & Tatelbaum, R. C. (1999). Prenatal and infancy home visitation by
nurses: Recent findings. The Future of Children, 9(1), 44–65.
Olds, D. L., Kitzman, H., Hanks, C., Cole, R.,
Anson, E., Sidora-Arcoleo, K.,…Bondy, J.
(2007). Effects of nurse home visiting on mater-nal and child functioning: Age-9 follow up of a randomized trial. Pediatrics, 120(4), e832–e845.
Olds, D. L., Robinson, J., O’Brien, R., Luckey, D. W.,
Pettitt, L. M., Henderson, C. R.,…Talmi, A.
(2002). Home visiting by paraprofessionals and by nurses: A randomized, controlled trial. Pediatrics, 110(3), 486–496.
Olds, D. L., Sadler, L., & Kitzman, H. (2007). Programs for parents of infants and toddlers: Recent evidence from randomized trials. Journal of Child Psychology and Psychiatry, 48(3/4), 355–391.
Paulsell, D., Avellar, S., Sama Martin, E., & Del
Grosso, P. (2011). Home visiting evidence of effec-tiveness review: Executive summary. Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families. U.S. Department of Health and Human Services.
Raikes, H., Green, B. L., Atwater, J., Kisker, E.,
Constantine, J., & Chazan-Cohen, R. (2006). Involvement in Early Head Start home visiting services: Demographic predictors and relations to child and parent outcomes. Early Childhood Research Quarterly, 21, 2–24.
Schwarz, D. F., O’Sullivan, A. L., Guinn, J.,
Mautone, J. A., Carlson, E.C., Zhao, H., …
Radcliffe, J. (2012). Promoting early interven-tion through a randomized controlled home visiting program. Journal of Early Intervention, 34(1), 20–39.
Williams, Stern, & Associates. (2005). Healthy Families Florida evaluation report: January 1, 1999–December 31, 2003. Retrieved from www.healthyfamiliesfla.org/resources/Final_Evaluation_1999-2003.pdf#
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
6 2 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Perspectives
Reflective PracticeLook, Listen, Wonder, and Respond
DEBORAH J. WEATHERSTONMichigan Association for Infant Mental Health
Southgate, Michigan
to be aware of is almost limitless. Beginning with the infant: What is the infant’s age, size, weight, and physical condition or health sta-tus? What social, emotional, motor, and cognitive capacities are observed during the first visits? How responsive is the infant to people who care for him? Does he smile in response to face and voice? Does he laugh? Does he relax comfortably when in his par-ent’s arms? Can he make eye contact that is sustained and purposeful? How active or inactive, responsive or unresponsive does he appear to be? How well does he signal his needs to be fed, comforted, played with, amused? Can he be comforted?
The parent as caregiver is important to observe, too: What is the parent’s age? How attentive and responsive is the parent to the infant’s cries and smiles? Does the parent hold the baby comfortably in effort to nur-ture, protect, and comfort? Does the parent respond to the infant’s needs to be fed? Does the parent respond sensitively and appro-priately to the infant with genuine warmth, affection, and gentleness? What does the par-ent bring to the care of the baby? What is the parent’s mood, or mental health status?
The relationship between parent and infant is import to notice as well: How much pleasure does there seem to be between them? Is there a sense of ease or reciprocity
and beside IMH home visitors, to be reflective—to observe, listen, wonder, and respond.
What follows is a discussion of these reflective components: observation, listen-ing, wondering, and response. Together, these components invite parents to dis-cover who their babies are as well as to understand the importance of nurturing relationships, past and present, to devel-opment, growth, and change. They support infants and very young children to expe-rience the possibility of secure and loving interactions and attachment relationships with their parents. Of equal interest, reflec-tive practice offers IMH home visitors opportunities to explore the meaning and mystery of early relationship development, to understand early experience, and to feel again the warmth or promise of relation-ships, personal and professional, as they engage and support others through their work (Tomlin, Sturm, & Koch, 2009).
Observation
Observation of the infant, the par-ent, and their interactions with one another guide the IMH home
visitor in understanding the strengths and the risks that a family faces in car-ing for an infant at home. The list of things
Selma Fraiberg’s pioneering work with infants, toddlers, and families more than 40 years ago helped to establish the field of infant mental health (IMH), providing attention to social and emotional health and the security of early developing parent–child relationships in the first years of life (Fraiberg, 1980). Fraiberg and her colleagues designed these IMH services to be carried out in the home, where parent(s) and child could be seen together by pro-fessionals who were trained in both child development and mental health strate-gies to offer emotional support, concrete resource assistance, developmental guid-ance, and infant–parent psychotherapy, as needed by the family (Weatherston, 2012). They placed the early developing attach-ment relationship at the center of their work. The intent was to share knowledge about infancy and early relationship devel-opment with parents as well as to provide preventive intervention and treatment services in the first years of a child’s life. Fraiberg referred to this knowledge as a gift from science, a treasure that should be returned to babies and their families. More specifically, the gift is offered within the context of a trusting working relationship and the treasure is returned as parents are invited, in the presence of their infants
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

J a n u a r y 2 0 1 3 Z e r o t o T h r e e 6 3
this safe space that a narrative may emerge for the parent and home visitor to wonder about:
• What is the infant or toddler’s experi-ence of the parent and their relation-ship?
• What is the parent’s experience of the infant?
• How able is the parent to understand the emotional needs of the infant?
• What does the baby bring to the relationship?
• What or who might the baby represent?
• What hopes or dreams did the parent have before the baby was born?
• What accounts for the sorrow and moments of pleasure in this parent–infant pair?
• Where does the hopefulness lie?
Responding
A s trust in one another deep-ens, parent and IMH home visitor become more engaged in the emo-
tional journey of IMH work, learning to be fully present, reflective, and self-aware. Each participates; each observes and lis-tens. The home visitor may respond by
Wondering
Close to the source, at the infant and parent’s side, the IMH home visitor learns so much. By staying open to
the details of their interactions and also the emotions contained (expressed and those unexpressed), the IMH home visitor wonders about what she sees and hears. It is within
between them? How well does the parent follow the infant’s lead? How well does the infant respond? Are their interactions smooth and synchronous or poorly timed? Is there a sense of warmth and affection expressed toward one another? Are they able to engage easily or are there miscues?
Though simple, these are remarkable indicators of the nature of the early develop-ing attachment relationship between parent and child and central to the IMH home visi-tor’s capacity to provide home based services that support social and emotional well-being during the first years of life. Observation is the bedrock on which all reflective practice is based. It is a core component of effective home visiting preventive intervention ser-vice and requires solid understanding of early development and relationship-centered work.
Listening
The IMH home visitor may invite the parent to talk and listens carefully to the details shared, remaining attuned,
curious, and open (Weatherston, 1998; see box, Listening: Reflective Process). By listen-ing carefully, the home visitor offers a safe space in which a parent may have and express thoughts and feelings, making a connection that deepens over time (Siegel & Shahmoon-Shanok, 2010). To the extent possible, the home visitor’s questions should not be intru-sive or deepen the parent’s pain. Rather, they should be nonjudgmental and lead to reflec-tion. Gentle reflective inquiry might include, “How are things going for you?” or “What would be most helpful to you to talk about today?” “Would you like to tell me about the baby’s week?” “What do you enjoy doing with your baby?” “What were the first weeks at home with the baby like for you? “Would it be helpful to talk about this?” “Have you ever taken care of a baby before?” “Who took care of you when you were little?”
Listening without interruption allows a home visitor to be fully present, to be curi-ous, to hold the awareness of thoughts and feelings that are awakened within the rela-tionship with the parent, and to empathize with what a parent or infant is experiencing. Listening makes it possible for the home vis-itor to take the perspective of the infant and parent, to think more deeply about what they share and to understand what a parent or infant is experiencing.
Observation of the infant, the parent, and their interactions with one another guide the IMH home visitor in understanding the strengths and the risks that a family faces in caring for an infant at home.
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/B
ro
sa
Listening: Reflective
Process
What follows are practical guidelines for home
visitors to follow when listening to parents
reflectively:
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions

6 4 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Perspectives
IMH home visitor and enhances the parent’s capacity to respond and reflect.
The IMH Home Visitor’s Emotional Response
The IMH home visitor who pays atten-tion to the emotional needs of infants and families must remain alert to his
or her own emotional response. Longings for relationship, memories, hopes and wishes, are continuously evoked in the presence of infants and parents who are negotiating early relationships. IMH home visitors may be affected deeply by individual infants and families enrolled; they need to have time to respond to what is seen and heard and felt, most often within a trusting, reflective super-visory relationship (Gatti, Watson & Siegel, 2011). A
Deborah J. Weatherston, PhD, IMH-E® is the executive director of the Michigan Association for Infant Mental Health (MI-AIMH) in Southgate, Michigan, where she leads the nationally recognized, professional develop-ment plan, the MI-AIMH Endorsement for Culturally-Sensitive, Relationship-Focused Practice Promoting Infant Mental Health®. She co-developed and directed the Graduate Certificate in Infant Mental Health from 1988–2004. She is a ZERO TO THREE Graduate Fellow (1999–2000), a member of the ZERO TO THREE Fellows Work Group and the WAIMH Board of Directors and is currently the editor of the WAIMH publication Perspectives in Infant Mental Health (formerly, The Signal). She has contributed to numerous publications including Case Studies in Infant Mental Health: Risk, Resiliency and Relationships, Zero to Three Journal, and the Infant Mental Health Journal.
offering gentle encouragement to the parent to talk about the infant or the dif-ficulties within their early developing relationship or about the parent’s experi-ences, past and present, which make the baby’s care problematic. Again, it is the presence of the infant or toddler within the context of the relationship with the IMH home visitor that invites a parent to have and express feelings about care for a baby and the challenges of early parenthood, past relationship experiences or traumas never spoken about before, disappoint-ments, and difficulties.
The emotional journey is often intense and complex, requiring courage on the part of both parent and home visitor to respond openly and honestly to one another in effort to reduce the risk of further devel-opmental, behavioral, or relationship failures. The home visitor must often tol-erate stories of abandonment and loss, grief surrounding the death of a child, early parental abuse or neglect, domestic vio-lence, or removal of children to foster care. Reflective practice requires allowing the full story to unfold, holding and contain-ing the emotions expressed, and, in time, empathic response.
The IMH home visitor is challenged to remain curious and tolerate uncertainty, to hold and contain the feelings expressed as the details unfold, to wonder and “not know” when presented with a difficult dilemma and to refrain from giving an immediate response if a question is asked. These strategies create opportunities for the parent to respond; for the parent’s words to fill the space; for the parent to share thoughts and feelings with the home visitor. All of these approaches strengthen the relationship between the parent and
The relationship between parent and infant is import to notice as well: How much pleasure does there seem to be between them?
Ph
ot
o: ©
iS
to
ck
ph
ot
o.c
om
/l
os
ti
nb
id
s
Learn More
Baby Stages, A Parent’s and Caregiver’s
Guide to the Social and Emotional
Development of Infants and Toddlers
www.mi-aimh.org/products/wheels
Everyday Ways to Support Your Baby’s
and Toddler’s Early Learning
www.zerotothree.org/about-us/areas-of-expertise/free-parent-brochures-and-guides
My Favorite Activities: Developmental
Time for Baby
pm@thepowerof nurturingcare.com
Reflective Supervision Video Training
Series DVD
www.mi-aimh.org/products/dvd
References
Fraiberg, S. (1980). Clinical studies in infant mental health. New York, NY: Basic Books.
Gatti, S., Watson, C., & Siegel, C. (2011). Step back and consider: Learning from reflective practice in infant mental health. Young Exceptional Children, 14(2), 32–45.
Siegel, D., & Shahmoon-Shanok, R. (2010). Reflective communication: Cultivating mind-sight through nurturing. Zero to Three, 31(2), 6–14.
Tomlin, A., Sturm, L., & Koch, S. (2009). Observe, listen, wonder, and respond: A preliminary explo-ration of reflective function skills in early care providers. Infant Mental Health Journal, 30(6), 634–647.
Weatherston, D. (1998). She needed to talk and I needed to listen: An infant mental health inter-vention. Zero to Three, 18(3), 6–12.
Weatherston, D. (2012). The gift of love: A birth-right. ChildLinks, Journal of Bernardos’ Training and Resource Services, 2, 2–7.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
Better Parenting in 3 Easy Steps Better Parenting in 3 Easy Steps What’s Best for My Baby and Me?A 3-Step Guide for ParentsCLAIRE LERNER and AMY LAURA DOMBRO
Raising a young child means making difficult decisions. This easy-to-read, plain language booklet is a great tool to help parents gainthe confidence they need to solve everyday problems.
Lerner and Dombro, early childhood and parenting experts, outlinea three-step approach for making sensitive and effective decisionsby presenting information on child development and vignettes thatshow the three-step approach in action. The book’s engaging styleand practical, research-based advice will make What’s Best for MyBaby and Me? a favorite resource for both professionals andparents alike. 2006. 39 pages.
ITEM #345 � ISBN 0-943657-94-6 � $30.00 for a pack of 12 bookletsITEM #355 � ISBN 0-943657-94-6 � $3.99 for a single copy
Order yours today! Call toll-free (800) 899-4301 or go to www.zerotothree.org/bookstore
Includes pull-out chart,highlighting age-baseddevelopmentalbehavior.
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
6 6 Z e r o t o T h r e e J a n u a r y 2 0 1 3
Goodwill Industries: An Unexpected, but Perfect Partner for Home
Visiting
Joanne Martin, Goodwill Industries of Central Indiana, Indianapolis, Indiana
Field NotesZERO TO THREE Fellows share news and information about research, policy, and practice innovations in their work with infants, toddlers, and families.
Goodwill Industries of Central Indiana (GWCI) is the imple-menting agency for a large-scale
Nurse-Family Partnership (NFP; n.d.) pro-gram in Indianapolis. This is the first time any Goodwill has implemented NFP, and it is the first NFP program in Indiana. Funded by the Maternal, Infant, and Early Child-hood Home Visitation component of the Affordable Care Act, GWCI has hired 18 of 24 nurse home visitors, 3 nurse home visi-tor supervisors, and an NFP nurse director. All nurse home visitors are bachelors- prepared nurses, 3 of whom are bilingual. By June 30, 2013, GWCI is expected to enroll 600 women who are pregnant with their first child and nurse home visitors will con-tinue to visit until the child is 2 years old. At the end of GWCI’s first full year of fund-ing (November 30, 2012), 280 women had enrolled and 86 babies had been born.
What makes GWCI a perfect partner? Goodwill is typically associated with retail stores that accept donated goods and pro-vide training and work opportunities for hard-to-employ persons. What most peo-ple don’t realize is that revenue generated from retail stores allows GWCI to invest
in community-based programs that sup-port their employees and others in the community. GWCI has developed recog-nized expertise in changing an individual’s life course trajectory. GWIC employees repeatedly say they had been given a second chance because opportunities for work and education were made available and some-one believed in them. Unique to GWCI, Goodwill Guides are available to support employees in order to ensure stability in finances, housing, child care, and trans-portation. Goodwill Guides offers GWCI employees what many families enrolled in NFP home visiting need. Through Goodwill Guides, GWCI enhances what NFP pro-grams usually provide. Thus, nurse home visitors are better able to optimize the health of women during and after preg-nancy, support mothers as they adjust to their maternal role, link children to appro-priate health care, and foster child growth and development. Meanwhile, Goodwill Guides work directly with other fam-ily members to stabilize the family and/or work through the nurse home visitor to sup-port mothers in areas such as employment, education, housing, and child care.
I am evaluating the extent to which Goodwill Guides contribute to achieving positive outcomes for families enrolled in NFP. So far it looks feasible and the results look promising. I am carefully tracking the stages of implementation and monitoring the development of Goodwill Guides, as an innovative best practice. GWIC is committed to measuring outcomes and evidence-based decision making. If Goodwill Guides proves to be an effective enhancement to an already evidence-based home visiting program, GWCI plans to share the results broadly. In addition, GWCI will be prepared to assist other Goodwill agencies to partner with home visiting programs and implement Goodwill Guides with fidelity to core components and flexibility to adapt to diverse communities. Stay tuned!
For more information, contact Joanne Martin at [email protected] or 317-517-1894
Nurse-Family Partnership. (n.d.). www.nursefamilypartnership.org
Coaching Parents in Promoting Child Learning Through Joint
Planning
Laura Hansen and M’Lisa Shelden, Family, Infant and Preschool Program, Morganton, North Carolina
The Family, Infant and Preschool Program (FIPP) provides Early Head Start supports and early
childhood intervention to children birth through 5 years old and their families through home visiting. Conceptually, FIPP approaches home visiting emphasizing methods that build child, parent, and family strengths using capacity-building approaches (Dunst, 2005). We do this by using evidence-based practices such as focusing on parent-mediated child learning in interest-based family and community activity settings and providing supports to
parents using capacity-building helpgiving practices (Dunst, 2005).
FIPP staff focus on parent-mediated child learning because development theory and research findings support the primary role of parents in young children’s devel-opment and learning throughout daily routine activities in their natural environ-ments (Bronfenbrenner, 1979; Mahoney & Wiggers, 2007). We use capacity-building helpgiving practices because they have been associated with increased parent reports of empowerment and positive family and child outcomes (Dunst, Trivette, & Hamby,
2007). Coaching parents represents one example of capacity-building helpgiving practices (Rush & Shelden, 2011).
One capacity-building characteristic of coaching is joint planning. The purpose of joint planning is to ensure parents’ active participation in gaining and using new skills or knowledge (Rush & Shelden, 2011). FIPP practitioners complete home visits by asking parents to develop a plan for activity-based strategies they will use between visits to continue promoting child learning and development around goals they desire. The second part of the plan includes deciding
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
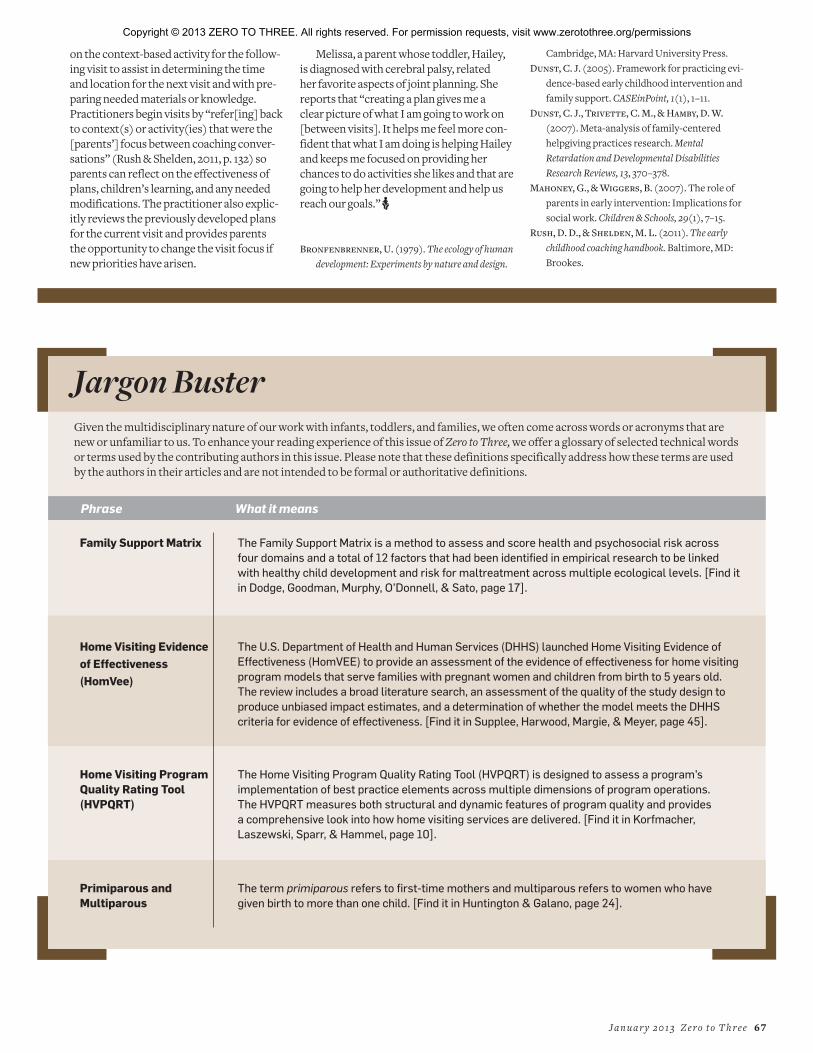
J a n u a r y 2 0 1 3 Z e r o t o T h r e e 6 7
on the context-based activity for the follow-ing visit to assist in determining the time and location for the next visit and with pre-paring needed materials or knowledge. Practitioners begin visits by “refer[ing] back to context(s) or activity(ies) that were the [parents’] focus between coaching conver-sations” (Rush & Shelden, 2011, p. 132) so parents can reflect on the effectiveness of plans, children’s learning, and any needed modifications. The practitioner also explic-itly reviews the previously developed plans for the current visit and provides parents the opportunity to change the visit focus if new priorities have arisen.
Melissa, a parent whose toddler, Hailey, is diagnosed with cerebral palsy, related her favorite aspects of joint planning. She reports that “creating a plan gives me a clear picture of what I am going to work on [between visits]. It helps me feel more con-fident that what I am doing is helping Hailey and keeps me focused on providing her chances to do activities she likes and that are going to help her development and help us reach our goals.” A
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design.
Cambridge, MA: Harvard University Press.Dunst, C. J. (2005). Framework for practicing evi-
dence-based early childhood intervention and family support. CASEinPoint, 1(1), 1–11.
Dunst, C. J., Trivette, C. M., & Hamby, D. W.
(2007). Meta-analysis of family-centered helpgiving practices research. Mental Retardation and Developmental Disabilities Research Reviews, 13, 370–378.
Mahoney, G., & Wiggers, B. (2007). The role of parents in early intervention: Implications for social work. Children & Schools, 29(1), 7–15.
Rush, D. D., & Shelden, M. L. (2011). The early childhood coaching handbook. Baltimore, MD: Brookes.
Jargon Buster
Given the multidisciplinary nature of our work with infants, toddlers, and families, we often come across words or acronyms that are new or unfamiliar to us. To enhance your reading experience of this issue of Zero to Three, we offer a glossary of selected technical words or terms used by the contributing authors in this issue. Please note that these definitions specifically address how these terms are used by the authors in their articles and are not intended to be formal or authoritative definitions.
Phrase What it means
Family Support Matrix The Family Support Matrix is a method to assess and score health and psychosocial risk across
four domains and a total of 12 factors that had been identified in empirical research to be linked
with healthy child development and risk for maltreatment across multiple ecological levels. [Find it
in Dodge, Goodman, Murphy, O’Donnell, & Sato, page 17].
Home Visiting Evidence
of Effectiveness
(HomVee)
The U.S. Department of Health and Human Services (DHHS) launched Home Visiting Evidence of
Effectiveness (HomVEE) to provide an assessment of the evidence of effectiveness for home visiting
program models that serve families with pregnant women and children from birth to 5 years old.
The review includes a broad literature search, an assessment of the quality of the study design to
produce unbiased impact estimates, and a determination of whether the model meets the DHHS
criteria for evidence of effectiveness. [Find it in Supplee, Harwood, Margie, & Meyer, page 45].
Home Visiting Program Quality Rating Tool (HVPQRT)
The Home Visiting Program Quality Rating Tool (HVPQRT) is designed to assess a program’s
implementation of best practice elements across multiple dimensions of program operations.
The HVPQRT measures both structural and dynamic features of program quality and provides
a comprehensive look into how home visiting services are delivered. [Find it in Korfmacher,
Laszewski, Sparr, & Hammel, page 10].
Primiparous and Multiparous
The term primiparous refers to first-time mothers and multiparous refers to women who have
given birth to more than one child. [Find it in Huntington & Galano, page 24].
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions
®
The Editorial Mission
of the Zero To Three Journal
To provide a forum for thoughtful
discussion of important research, practice,
professional development, and policy
issues in the multidisciplinary infant,
toddler, and family field.
ZERO TO THREE’s mission is to
promote the health and development
of infants and toddlers.
We are a national, nonprofit organization
that informs, trains and supports
professionals, policy makers and parents
in their efforts to improve the lives of
infants and toddlers.
How to Subscribe
• Call (800) 899-4301 between 9am–5pm,
Eastern Standard Time
• Visit www.zerotothree.org/estore to
place your order online day or night
• E-mail customer service staff at
Suite 350
1255 23rd Street, NW
Washington, DC 20037
Address service requested
UPCOMING ISSUES
March: Infants, Toddlers, and TechnologyMay: Early Childhood Mental Health Consultation July: Stories From the Field—2013
Non Profit Org.
US Postage
PAIDPermit No. 425
Southern, MD
Copyright © 2013 ZERO TO THREE. All rights reserved. For permission requests, visit www.zerotothree.org/permissions