strategies for preventing and treating uncontrolled perioperative bleeding
TRANSCRIPT

Strategies for Preventing and Treating UncontrolledPerioperative Bleeding

2

3
Strategies for Preventing and Treating Uncontrolled Perioperative Bleeding
CE/CME Visiting Faculty Series• Faculty includes renowned surgeons, anesthesiologists, blood
banking specialists, and other experts in operative hemostasis and transfusion management
• Combination of didactic, specialty-specific case evaluations and your interactivity
• Part of a multicomponent educational initiative that can be accessed via
www.bloodcmecenter.org

4
Learning Objectives
Upon completion of this activity, participants should be better able to:
1. Discuss specific patient types who may be at increased risk for perioperative bleeding and complications from acquired coagulopathy
2. Explain the essentials of surgical hemostasis and current guidelines for achieving balance between bleeding and clotting
3. Explain the benefits and risks of blood products as a therapeutic modality
4. Explain the therapeutic benefits and risks of alternative hemostatic treatment modalities
5. Explain how to initiate appropriate strategies for achieving optimal operative hemostasis

5
Bleeding Is a Complication of Many Types of Surgery
• Surgery is the most common cause of major blood loss in a medical setting1 and can increase both morbidity and mortality2,3
• Unexpected perioperative bleeding is largely caused by impaired inherited or drug-induced primary hemostasis4
1. Mannucci PM, et al. N Engl J Med. 32007;56:2301-2311; 2. Hall TS, et al. Ann Thorac Cardiovasc Surg. 2001;7: 352-357; 3. D’Amico G, et al. Hepatology. 2003;38:599-612; 4. Pfanner G, et al. Anaesthesist. 2007;56:604-611.

6
Definition of Hemostasis
Hemostasis: “The Arrest of Bleeding”Stedman’s Medical Dictionary
Hemostasis: “Life in the Balance”
Lawson JH, et al. Semin Hematol. 2004;41(suppl 1):55-64.
TraumaMajor SurgeryHemophilia
StrokeMIThrombosis
Bleedingto Death
Clottingto Death

7
Definition of Significant Bleeding
• >2 L within the first 24 post-op hours1
• Surgical or vascular component: corrected by surgical
intervention or embolization2
• Coagulopathic component: more difficult to control due to
several interrelated mechanisms2
Consumption of coagulation factors and platelets
Dilution of coagulation factors
Metabolic disorders (eg, hypothermia, acidosis)
1. Despotis GJ, et al. Ann Thorac Surg. 2000;70(2 suppl):S20-S32; 2. Vincent J-L, et al. Crit Care. 2006;10:1-12.

8
Prevalence of Uncontrolled Bleeding
Surgical Discipline Uncontrolled Bleeding Rate
Cardiovascular 5%-7% Post-op1
General 1.9% Laparoscopic cholecystectomy2
Obstetric 3.9% (vaginal); 6.4% (cesarean)3,4
Orthopedic 2%-6.3% Hip/knee arthroplasty5-7
Urologic 4%-8% TURP8; 3.3%-9.9% URL9
Trauma 30%-40%10,11
1. Despotis GJ, et al. Anesth Analg. 1996;82:13-21; 2. Erol DD, et al. The Internet Journal of Anesthesiology. 2005;9:2; 3. Combs CA, et al. Obstet Gynecol. 1991;77:69-76; 4.Combs CA, et al. Obstet Gynecol. 1991;77:77-82; 5. Hull R, et al. N Engl J Med. 1993;329:1370-1376; 6. Leclerc JR, et al. Ann Intern Med. 1996;124:619-626; 7. Strebel N, et al. Arch Intern Med. 2002;162:1451-1455; 8. Daniels PR. Nat Clin Pract Urol. 2005;2:343-350; 9.Rosevear HM, et al. J Urol. 2006;176:1458-1462; 10. Holcomb JB. Crit Care. 2004;8(suppl 2):S57-S60; 11. Sauaia A, et al. J Trauma. 1995;38: 185-193.

9
Prevalence of Uncontrolled Bleeding (cont)
Surgical Discipline Uncontrolled Bleeding Rate
Cardiovascular 5%-7% Post-op1
General 1.9% Laparoscopic cholecystectomy2
Obstetric 3.9% (vaginal); 6.4% (cesarean)3,4
Orthopedic 2%-6.3% Hip/knee arthroplasty5-7
Urologic 4%-8% TURP8; 3.3%-9.9% URL9
Trauma 30%-40%10,11
1. Despotis GJ, et al. Anesth Analg. 1996;82:13-21; 2. Erol DD, et al. The Internet Journal of Anesthesiology. 2005;9:2; 3. Combs CA, et al. Obstet Gynecol. 1991;77:69-76; 4.Combs CA, et al. Obstet Gynecol. 1991;77:77-82; 5. Hull R, et al. N Engl J Med. 1993;329:1370-1376; 6. Leclerc JR, et al. Ann Intern Med. 1996;124:619-626; 7. Strebel N, et al. Arch Intern Med. 2002;162:1451-1455; 8. Daniels PR. Nat Clin Pract Urol. 2005;2:343-350; 9.Rosevear HM, et al. J Urol. 2006;176:1458-1462; 10. Holcomb JB. Crit Care. 2004;8(suppl 2):S57-S60; 11. Sauaia A, et al. J Trauma. 1995;38: 185-193.
10
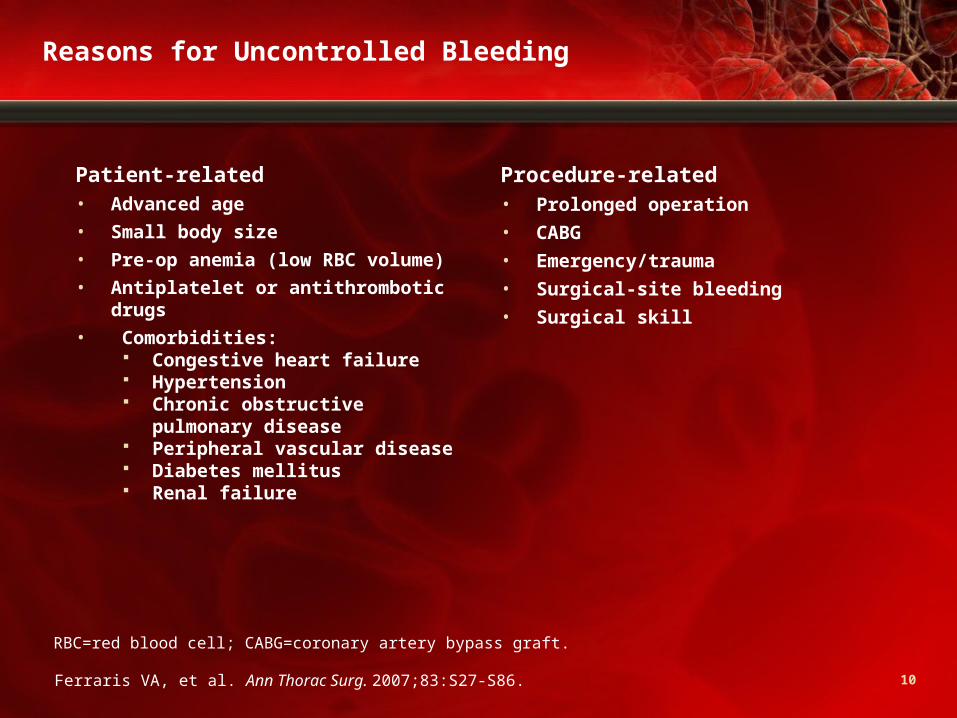
Reasons for Uncontrolled Bleeding
Patient-related• Advanced age
• Small body size
• Pre-op anemia (low RBC volume)
• Antiplatelet or antithrombotic drugs
• Comorbidities: Congestive heart failure Hypertension Chronic obstructive
pulmonary disease Peripheral vascular disease Diabetes mellitus Renal failure
Procedure-related• Prolonged operation
• CABG
• Emergency/trauma
• Surgical-site bleeding
• Surgical skill
Ferraris VA, et al. Ann Thorac Surg. 2007;83:S27-S86.
RBC=red blood cell; CABG=coronary artery bypass graft.

11
Types of Uncontrolled Bleeding
• Surgical bleeding results from failure to control bleeding from the operative site; signs include expanding hematoma and saturated dressings (75%-90%)1,2
• Nonsurgical bleeding is caused by failure of hemostatic pathways; often manifested as generalized oozing (10%-25%)1,2
1. Adams GL, et al. Hematol Oncol Clin North Am. 2007;21:13-24;2. Shander A. Surgery. 2007;142(4 suppl):S20-S25.

12
Costs of Uncontrolled Bleeding
• Estimating blood costs is a complex undertaking1,2
Blood costs increase due to shrinking donor availability and precautions to minimize transfusion risks1
Great variation among institutions in reoperation and return-to-operating-room rates2
Total cost per unit is >$4002
• “Clinical costs” of sustained bleeding3: Consumption of coagulation factors Hemodilution, hypothermia, and acidosis Compound factor consumption More bleeding
1. Shander A, et al. Best Pract Res Clin Anaesthesiol. 2007;21:271-289;2. Shander A. Surgery. 2007;142:S20-S25;3. Armand R, et al. Transfus Med Rev. 2003;17:223-231.

13
Outcomes of Uncontrolled Bleeding
Clinical• Massive blood loss is associated
with mortality
• Transfusion itself may have independent detrimental effects
Financial• Death
• Average LOS is 2X to 2.5X
• Cost of blood
• Costs of transfusion
• Costs of adverse outcomes
Adapted from Shander A. Surgery. 2007;142(4 suppl):S20-S25.
LOS=length of stay.

14
SurgeryPost-op Recovery
Thrombosis
Clotting
Bleeding
Hemorrhage
Can We Predict Who Will Bleed?
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl 1):55-64.
1. Who is likely to bleed or clot too much?2. How do we optimize the patient’s physiology?3. Which topical agents are effective?4. Which biologic agents are effective?
There Is a Difference Between Who Is At Risk and Who Will Bleed

15
Who Bleeds Without Warning?
STS Guidelines: Aspirin…the Dilemma• Aspirin causes increased bleeding• Amount of bleeding is small (0.5-1 U/patient)• Aspirin important for better outcome in acute coronary
syndromes• Nothing more important than aspirin, including heparin,
thrombolytics, IIb/IIIa, and PCI• STS recommendation: Stop aspirin for a few days in very-low-
risk patients; continue in all others
Ferraris VA, et al. Ann Thorac Surg. 2005;79:1454-1461.
STS=Society of Thoracic Surgeons; PCI=percutaneous coronary intervention.

16
Who Bleeds Without Warning? (cont)
Do Thienopyridines Cause Post-op Bleeding?• Evidence is more compelling than for aspirin1
• 11 studies with clopidogrel and CABG1 • All studies show increased bleeding when clopidogrel given
within 5 days of CABGsome with increased mortality1 • AHA/ACC and STS guidelines recommend stopping clopidogrel
for 5 days before operation, if possible2
1. Ferraris VA, et al. Ann Thorac Surg. 2005;79:1454-1461; 2. Braunwald E, et al. J Am Coll Cardiol. 2002;40:1366-1374.
AHA=American Heart Association; ACC=American College of Cardiology.

17
“Cascade” Model of Hemostasis
Intrinsic Pathway Extrinsic Pathway
factor XIIHMKPK
factor XI factor XIa
factor IXfactor IXa
factor VIIIaPL, Ca+2
factor Xfactor Xafactor VaPL, Ca+2
prothrombin thrombin
fibrinogen fibrin
factor VIIatissue factor
PL, Ca+2
factor X
Adapted from Hoffman M, et al. Thromb Haemost .2001;85:958-965.

18Hoffman M, et al. Blood Coag Fibrinol. 1998;9(suppl 1):S61-S65.
TF-Bearing Cell
Activated Platelet
Platelet
TF
VIIIa Va
VIIIaVa
Va
VIIa
TF VIIa Xa
X II
IIa
IXV Va
II
VIII/vWF
VIIIa
II
IXa
XIX
X
IXa
IXaVIIa
Xa
IIa
IIa
Xa
Normal Hemostasis: Pivotal Role of TF/VIIa
TF=tissue factor; vWF=von Willebrand factor.

19
Normal Hemostasis Is a Balance
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl 1):55-64.
TraumaMajor SurgeryHemophilia
StrokeMIThrombosis
Bleedingto Death
Clottingto Death
• Blood coagulation• Anticoagulation• Fibrinolysis• Antifibrinolysis• Vascular tone and blood flow• Endothelial cells and platelets

20
“Keeping On Center”
NormalHemostasis
ProcoagulantActivity
AnticoagulantActivity
FibrinolyticActivity
AntifibrinolyticActivity
Bleeding
Clotting
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl):55-64.
21
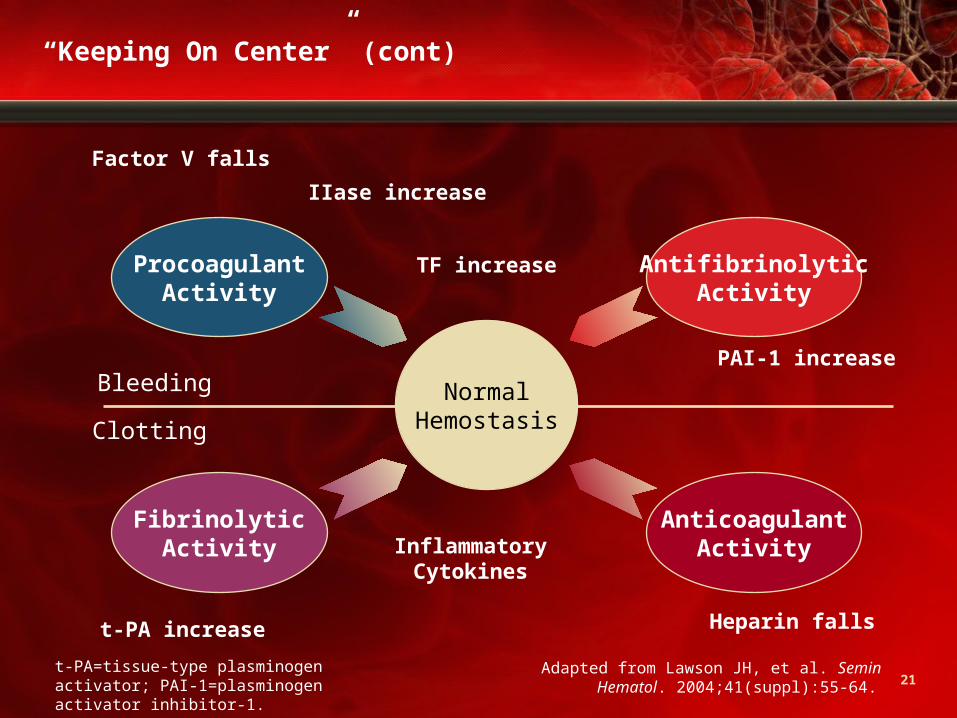
“Keeping On Center” (cont)
NormalHemostasis
Factor V falls
t-PA increase
IIase increase
TF increase
PAI-1 increase
Heparin falls
InflammatoryCytokines
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl):55-64.
ProcoagulantActivity
AnticoagulantActivity
FibrinolyticActivity
AntifibrinolyticActivity
Bleeding
Clotting
t-PA=tissue-type plasminogen activator; PAI-1=plasminogen activator inhibitor-1.

22
“Keeping On Center” (cont)
Topical HemostaticsPurified Factors, FFP, Cryo, PLTs
Aminocaproic acid,Tranexamic acid, Aprotinin
Heparin, WarfarinLMWH, Argatroban
t-PA, SK, UPA
NormalHemostasis
Bleeding
Clotting
FFP=fresh frozen plasma; Cryo=cryoprecipitate; PLTs=platelets; SK=streptokinase; UPA=urinary-type plasminogen activator; LMWH=low-molecular-weight heparin.
ProcoagulantActivity
AnticoagulantActivity
FibrinolyticActivity
AntifibrinolyticActivity
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl):55-64.

23
Thrombosis
Clotting
Bleeding
Hemorrhage
Physiology and Good Surgery
Topical Hemostatic Agents
Systemic Biologic Therapies
Achieving Optimal Operative Hemostasis
Adapted from Lawson JH, et al. Semin Hematol. 2004;41(suppl):55-64.

Treatment Modalities:Blood ProductsProhemostatic Agents

Blood Products in the Treatment of HemorrhageTransfusion Benefits, Risks, and Trends

26
Postoperative Blood Transfusion
Benefits:• Blood volume replacement
• Oxygen-carrying
• Clotting factors
Risks:• TACO
• TRALI
• Disease transmission (especially platelets)
• TRIM
• Transfusion errors
Evidence: Not enough data about benefits
Adapted from Ferraris VA, et al. Ann Thorac Surg. 2007;83:S27-S86.
TACO=transfusion-associated circulatory overload; TRALI=transfusion-related acute lung injury; TRIM=transfusion-related immunomodulation.

27
Benefits of Blood Transfusion
• Useful in certain situations−ASA criteria Transfuse patients on CPB with Hb ≤6 g/dL Transfusion justified when Hb ≤7 g/dL in patients older
than 65 years and patients with chronic CVD or
respiratory disease Benefit unclear for stable patients with Hb between 7 and
10 g/dL Transfusion recommended for patients with acute blood loss
>1500 mL or >30% of blood volume Evidence of rapid blood loss without immediate control
warrants transfusion
• Issue of “triggers”—have come a long way since “10/30” rule,
but still a long way to go
Adapted from Ferraris VA, et al. Ann Thorac Surg. 2007;83:S27-S86.
ASA=American Society of Anesthesiologists; CPB=cardiopulmonary bypass; Hb=hemoglobin; CVD=cardiovascular disease.

28
Risks of Blood Transfusion
TACO• Common reaction from rapid or massive transfusion of blood1 • Usually occurs within several hours after start of transfusion• Manifested in signs and symptoms that include:
Dyspnea Orthopnea Peripheral edema Rapid increase in BP
• Incidence difficult to determine due to underreporting2
• Patients at risk include3,4: Infants and elderly >60/years Those with chronic anemia Those with cardiac/pulmonary/renal failure
1. Popovsky MA. Transfusion Clin Biol. 2001; 8:272-277;2. American Association of Blood Banks. Technical Manual. 1999:577-600;3. Gresens CJ, et al. New York, NY: Marcel Dekker, Inc; 2001:71-86;4. Popovsky MA. Transfus Clin Biol. 2001;8:272-277.

29
Risks of Blood Transfusion (cont)
TRALI• Rare and life-threatening complication• Associated with transfusion of blood components containing
RBCs, platelets, granulocytes, and cryoprecipitates1
• Usually occurs within 1-2 hours after start of transfusion2
• Characterized by acute respiratory distress2
• Symptoms include2: Severe bilateral pulmonary edema Cyanosis Severe hypoxemia Tachycardia Hypotension Fever
• Incidence varies considerably from 1/5000 to 16/10,0001
• Fatality rate ranges from 5% to 14%2
1. Kopko PM, et al. Transfusion. 2001;41:1244-1248;2. Popovsky MA. Transfus Clin Biol. 2001;8:272-277.

30
Risks of Blood Transfusion (cont)
TypeOccurrence in RBC Units Transfused
Infectious:Human immunodeficiency virusHepatitis B Hepatitis C Bacterial infection
1 in 1.4-2.4 x 106
1 in 58,000-149,0001 in 872,000-1.7 x106
1 in 2,000
Immunologic Reactions:Febrile nonhemolytic transfusion reactionsAnaphylactic transfusion reactionsABO mismatchHemolysisDeathLeukocyte-related target organ injuryTransfusion-related acute lung injury Post-transfusion purpura
1 in 1001 in 20,000-50,000
1 in 60,0001 in 600,0001 in 20 to 1 in 501 in 2,000Rare
Transfusion Services Error:Donor screening error (malaria, T cruzi, babesioses, Creutzfeld-Jakob disease)Transfusion services error (other)
1 in 4 x 106
1 in 14,000
Adapted from Ferraris VA, et al. Ann Thorac Surg. 2007;83 S27-S86.

31
How to Reduce Transfusions?
Blood conservation: general principles• Devise an individual plan of care to minimize blood loss• Employ multidisciplinary, multimodal treatment approach• The lead clinician should provide proactive management• Modify routine practices if necessary• Screen for, investigate, and treat anemia before and
after surgery• Minimize iatrogenic blood loss, including phlebotomies• Employ a restrictive transfusion strategy• Reassess preoperative/postoperative use of anticoagulant and
antiplatelet agents• Consult transfusion experts early• Establish in advance a management plan for rapid control of
hemorrhage and transfusion
Shander A, et al. Curr Opin Hematol. 2006;13:462-470.

32
Pharmacologic Agents in Treatment of Hemorrhage
Prohemostatic Agents
• Antifibrinolytics
Lysine analogues
Aprotinin
• Topical hemostatics
• Protamine
• Desmopressin (DDAVP)
• Recombinant factor VIIa (rVIIa)

AntifibrinolyticsA Brief Review

34
Fibrinolysis
Every rise is followed by a fall.
a The coagulation cascade b Plasmin-mediated fibrinolysis
Summary of the coagulation and fibrinolysis cascades
Expert Reviews in Molecular Medicine © 2002 Cambridge University Press
α-2-APTAFI
PAI-1
Prothrombinasecomplex
+
+
+
+
–
–
Tissue factor FVIIa
FX
FXaFVa
Prothrombin
Thrombin
FibrinogenFibrin
+aggregated
platelets
Thrombus
Plasminogen
Plasmin
tPA
Fibrindegradation
products
35
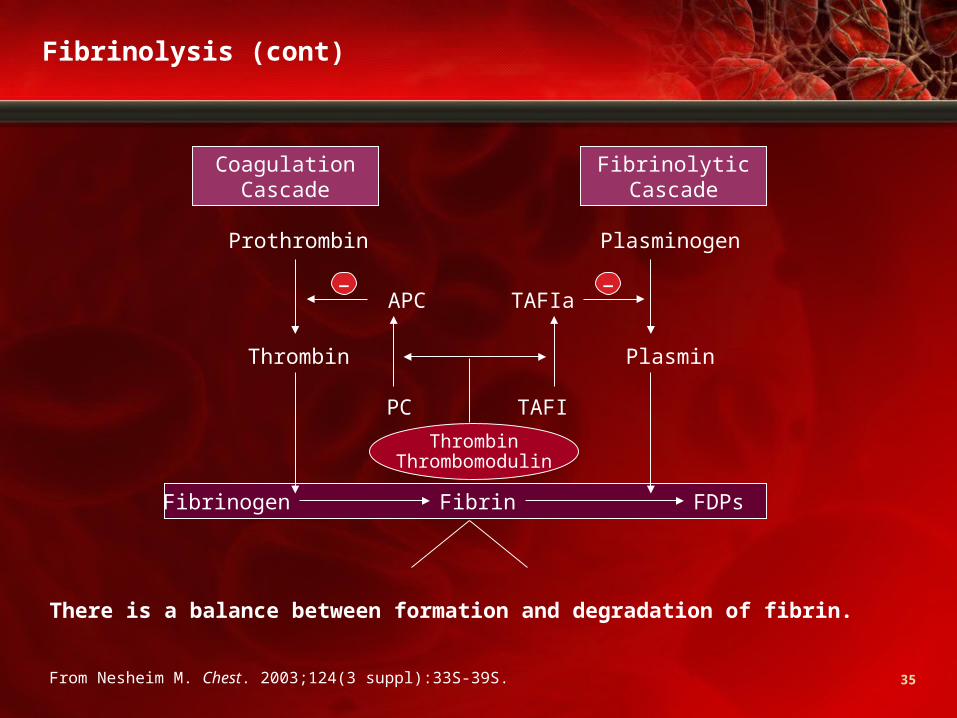
Fibrinolysis (cont)
There is a balance between formation and degradation of fibrin.
From Nesheim M. Chest. 2003;124(3 suppl):33S-39S.
Prothrombin Plasminogen
Thrombin Plasmin
APC TAFIa
TAFIPC
CoagulationCascade
FibrinolyticCascade
ThrombinThrombomodulin
Fibrinogen Fibrin FDPs
– –

36
Fibrinolysis (cont)
Antifibrinolytic Agents
Tip the balance against fibrinolysis More clot Less bleeding
Prothrombin Plasminogen
Thrombin Plasmin
APC TAFIa
TAFIPC
CoagulationCascade
FibrinolyticCascade
ThrombinThrombomodulin
Fibrinogen Fibrin FDP’s
– –
Adapted from Nesheim M. Chest. 2003;124:33S-39S.

37
Antifibrinolytics
• As implied by the name, these agents enhance hemostasis
when fibrinolysis contributes to bleeding
• Lysine analogues
ε-Aminocaproic acid (EACA)
Tranexamic acid (TXA)
• Aprotinin: Approved by FDA to reduce blood loss and
transfusion in CABG but marketing suspended 11/5/07

38
Lysine Analogues
• Block the lysine- binding sites on plasminogen, inhibiting the formation of plasmin
• TXA is 6-10 times more potent than EACA
Mannucci PM, et al. N Engl J Med. 2007;356:2301-2311.

39
Lysine Analogues (cont)
• Lysine analogues1-3: EACA and TXA
Indicated for enhancing hemostasis when fibrinolysis
contributes to bleeding
Both competitively inhibit plasmin binding to fibrin
Widely used in cardiac surgery, but data supporting
safety and efficacy are limited
EACA associated with increased incidence of certain
neurologic deficits; concerns about rhabdomyolysis and
renal dysfunction
1. Mannucci PM, et al. N Engl J Med 2007;356:2301-2311;2. Levy JH. Am J Health-Syst Pharm. 2005;62(suppl 4):S15-S19;3. Adams GL, et al. Hematol Oncol Clin North Am. 2007;21:13-24.

40
Aprotinin
• A small protein isolated from bovine lung • A non-specific serine protease inhibitor
inhibits trypsin, plasmin, plasma/tissue kallikrein, etc
• Inhibits contact phase activation of coagulation that both initiates coagulation and promotes fibrinolysis
• In CPB, it reduces derangements in coagulation/fibrinolysis caused by negatively charged surface of CPB circuit
• Indirectly preserves platelet function in extracorporeal circulation
• Marketing suspended on 11/5/07 following FDA Advisory 2/8/06

41
Topical Hemostatic Agents
• Used to augment hemostasis in surgery/trauma• Available in a variety of forms (solutions, gels, granules,
sprays) and used in conjunction with collagen, gelatin, cellulose matrices
• Local thrombin and fibrinogen levels determine the rate of clot formation at wound site Many of these topical agents have thrombin or fibrinogen
as their active agent• Classification:
Tissue/fibrin sealants (contain thrombin, fibrin, etc) Absorbable hemostatic agents (contain matrices) Combination products (contain both groups above)

42
Some Topical Hemostatic Agents
Voils S. Pharmacotherapy. 2007;27:69S-84S.
Sealants and Combination Products:
Agent Topical Application Instructions Major Drawbacks or Comments
Bovine thrombin Dry, spray, or mixed with isotonic saline applied to bleeding or oozing surfaces; may also be used with absorbable gelatin sponge or with FloSeal NT
Prion disease transmission; autoantibodies may develop to impurities, potentially resulting in coagulopathy
Recombinant human thrombin
To be released 2008; presumably will be similar to bovine thrombin
Potentially less immunogenic than bovine thrombin
FloSeal Hemostatic Matrix: bovine gelatin granules and human thrombin
Reconstituted mixture is applied to bleeding or oozing surfaces
Infectious disease transmission similar to that with other human blood products; bovine sensitization
Virally inactivated aprotinin-free fibrin sealant (Crosseal): thrombin and fibrinogen (human)
Stored frozen, then thawed and sprayed
Contains no animal protein and is virally inactivated and highly purified; safety concerns minimized

43
Some Topical Hemostatic Agents (cont)
Agent Topical Application Instructions Major Drawbacks or Comments
CoStasis: microfibrillar collagen-fibrin (bovine)
Reconstituted mixture forms gel matrix
Similar to other bovine preparations
CoSeal Surgical Sealant: 2 synthetic polyethylene glycols
Reconstituted mixture forms a hydrogel that is applied to bleeding or oozing surfaces; forms mechanical seal
Swells up to 4x its volume; may cause compression of anatomic structures
Aprotinin and TXA Solutions containing 1 MU of aprotinin or 2.5 g of TXA in 250 mL of saline poured into pericardial cavity during CPB
Single study with minimal effectiveness of aprotinin; TXA was less effective in reducing blood product usage
Chitosan hemostatic bandage
Bandage that binds electrostatically to red blood cells; considered a device; used in combat
Floats off wound in severe hemorrhage
Zeolite Powder applied to wounded tissue; considered a device; used in combat
Local hyperthermia-induced tissue damage
Voils S. Pharmacotherapy. 2007;27:69S-84S.

44
Some Topical Hemostatic Agents (cont)
Gabay M. Am J Health-Syst Pharm. 2006;63:1244-1253.
Cellulose-, Collagen-, and Gelatin-Based
Topical Hemostatic Composition Approval Date
Surgicel (J&J)Regenerated oxidized cellulose
October 14, 1960
Gelfoam (Pfizer) Porcine gelatin molded into a sponge
Available 1945; approved July 8, 1983
Surgifoam (J&J) Porcine gelatin sponge September 30, 1999
Avitene (Davol) Bovine collagen August 26, 1976 (as a drug)October 24, 1980 (as a device)
Instat (J&J/Gateway) Bovine collagen October 10, 1985
Helistat (Integra LifeSciences) Bovine collagen November 8, 1985
Helitene (Integra LifeSciences) Bovine collagen November 8, 1985

45
Indications
Gabay M. Am J Health-Syst Pharm. 2006;63:1244-1253.
Hemostatic Agent Labeled Indication(s)
Surgicel For use in surgical procedures when conventional methods of hemostasis, such as pressure and ligature, are ineffective; for endoscopic procedures, may be used by cutting to size.
Gelfoam For use in in surgical procedures, including those that may result in calcellous bone bleeding, when conventional methods of hemostasis are ineffective or impractical.
Surgifoam For use in surgical procedures, except urologic and ophthalmic procedures, when conventional methods of hemostasis are ineffective or impractical.
Avitene For use in surgical procedures when conventional methods of hemostasis are ineffective or impractical.
Instat For use in surgical procedures, except ophthalmic procedures, when conventional methods of hemostasis are ineffective or impractical; for endoscopic procedures, may be used by cutting to size.
Helistat For use in surgical procedures, except urologic and ophthalmic procedures, when conventional methods of hemostasis are ineffective or impractical.
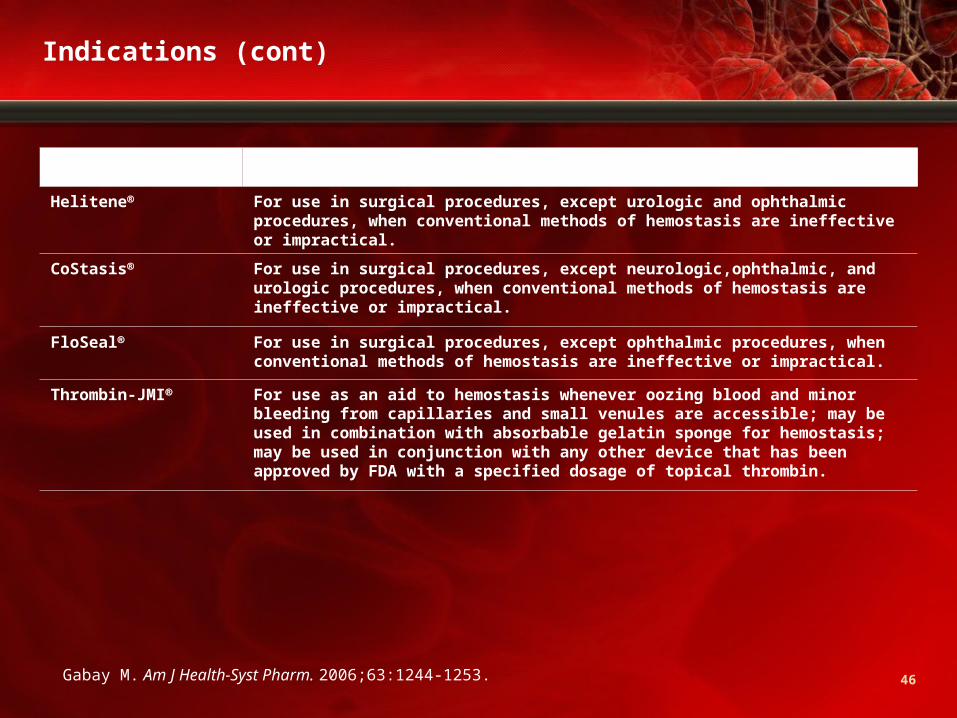
46
Hemostatic Agent Labeled Indication(s)
Helitene For use in surgical procedures, except urologic and ophthalmic procedures, when conventional methods of hemostasis are ineffective or impractical.
CoStasis For use in surgical procedures, except neurologic,ophthalmic, and urologic procedures, when conventional methods of hemostasis are ineffective or impractical.
FloSeal For use in surgical procedures, except ophthalmic procedures, when conventional methods of hemostasis are ineffective or impractical.
Thrombin-JMI For use as an aid to hemostasis whenever oozing blood and minor bleeding from capillaries and small venules are accessible; may be used in combination with absorbable gelatin sponge for hemostasis; may be used in conjunction with any other device that has been approved by FDA with a specified dosage of topical thrombin.
Gabay M. Am J Health-Syst Pharm. 2006;63:1244-1253.
Indications (cont)

47
Considerations
• Efficacy: Few randomized controlled trialsstudies have shown
beneficial effects in controlling capillary bleeding, achieving
hemostasis in vascular surgery, controlling bleeding from
fistula-puncture site in hemodialysis, etc
• Cost: No published study of cost-effectiveness
• Safety

48
Adverse Events
• Device failure (continued bleeding observed)• Device deployment failure • Infection• Granuloma • Abscess • Foreign body reaction • Allergic reaction • Interference with wound healing • Respiratory difficulty • Bowel obstruction • Hematoma • Intermittent ischemia • Stroke • Tissue necrosis • Erythema • Edema
www.fda.gov.

49
Adverse Events (cont)
• In 2004, FDA issued a notification on possible development of
paralysis following use of absorbable hemostatic agents
• If agent used and left on or near a bony or neural space, when
wetted, the material swelled and exerted pressure on neural
structures, resulting in pain, numbness, or paralysis
• Recommendations: Read labels carefully If used on or near bony/neural spaces, use the minimum
amount necessary to achieve hemostasis and remove as
much of the agent as possible after hemostasis is achieved
www.fda.gov.

50
Protamine
• Heparin antagonist indicated for heparin overdosage
• Rapid onset of action
• Has an anticoagulant effect when used alone; in the presence of
heparin, both drugs lose anticoagulant activity
• Too-rapid administration can cause severe hypotensive and
anaphylactoid-like reactions
51
DDAVP
• Originally developed and licensed for the treatment of inherited
defects of hemostasis1,2
• Several reviews suggest its effect is too small to influence the
need for transfusion and reoperation1,2
• Most evidence of efficacy is in mild hemophilia A and
von Willebrand’s disease1,2
• Not indicated for use in cardiac surgery patients1,2
Meta-analysis in cardiac patients: 2-fold increase in MI, a
small decrease in perioperative blood loss, and no added
benefits on clinical outcomes
1. Mannucci PM, et al. N Engl J Med. 2007;356:2301-2311;2. Levy JH. Am J Health-Syst Pharm. 2005; 62(suppl 4):S15-S19.
52
rVIIa
• Vitamin K-dependent glycoprotein structurally similar to human plasma-derived factor VIIa
• Approved in United States for treatment of bleeding in patients
with hemophilia A or B with inhibitors to factor VIII or IX
• Multiple reports of off-label use in cardiac surgery, trauma, liver
transplantation to secure hemostasis
• Promotes hemostasis by activating the coagulation cascade
• Believed to cause local thrombin generation and platelet
recruitment at sites of vascular and microvascular injury
53
rVIIa (cont)
• A central factor in coagulation
• A trypsin-like serine protease (characterized
by a serine residue in the active side of
the enzyme)
• Initiates coagulation in a complex with TF
• Once bound to TF, it is activated (FVIIa) by
different proteases
• Produced in liver; vitamin K–dependent (warfarin)

54
Mechanism of Action
Mannucci PM, et al. N Engl J Med. 2007;356:2301-2311.

55
Approved Indications and Usage
• Date: March 25, 1999
Indication: Treatment of bleeding episodes in hemophilia A or B
patients with inhibitors to factor VIII or factor IX
• Date: October 13, 2006
Indication: Treatment of bleeding episodes and for the
prevention of bleeding in surgical interventions or invasive
procedures in patients with acquired hemophilia
http://www.fda.gov/cber/products/novoseven.htm.
56
Approved Indications and Usage (cont)
rVIIa is indicated for:• Treatment of bleeding episodes in hemophilia A or B patients
with inhibitors to factor VIII or factor IX and in patients with acquired hemophilia
• Prevention of bleeding in surgical interventions or invasive procedures in hemophilia A or B patients with inhibitors to factor VIII or factor IX and in patients with acquired hemophilia
• Treatment of bleeding episodes in patients with congenital factor VIII deficiency
• Prevention of bleeding in surgical interventions or invasive procedures in patients with congenital factor VIII deficiency
NovoSeven [ package insert]. Princeton, NJ: Novo Nordisk Pharmaceuticals; September 1999.

57
Approved Indications and Usage (cont)
Remember the mechanism…• IXa and VIIIa aid VIIa in
activating X• If IXa or VIIIa is missing (or
inhibited), rVIIa can replace their function by converting more X to Xa
Mannucci PM, et al. N Engl J Med. 2007;356:2301-2311.

58
Monitoring of Treatment
• Primarily, clinical evaluation of hemostasis
• Lab testsNo direct correlation to achieving hemostasis: PT: Shortening to a plateau in hemophilia A/B with inhibitors aPTT: Shortens the prolonged aPTT in hemophilia A/B with
inhibitors; normalization not usually observed in doses
shown to induce clinical improvement; clinical improvement
is associated with a shortening of aPTT of 15 to 20 seconds Plasma FVII clotting activity (FVII:C)

59
Adverse Reactions
Seems to be well tolerated (298 hemophilia A or B patientswith inhibitors)
Body System Event
No. of episodes reported(n=1939 treatments)
No. of unique patients(n=298)
Body as a whole FeverPlatelets, Bleeding, and Clotting Hemorrhage NOS Fibrinogen plasma decreasedSkin and Musculoskeletal HemarthrosisCardiovascular Hypertension
16
1510
14
9
13
85
8
6
NovoSeven [package insert]. Princeton, NJ: Princeton, NJ: Novo Nordisk Pharmaceuticals; September 1999.
60
“Off-label” Uses of rVIIa
• Increasingly being considered for: Reversal of oral anticoagulation Reversal of heparin, lepirudin, and fondaparinux Thrombocytopenia and thrombocytopathy Bleeding with impaired liver function Gastrointestinal bleeding Trauma Surgery: Non-traumarelated (hepatic resection,
prostatectomy, cardiac, spinal)
• These off-label uses are mostly based on anecdotal case reports Need better evidence

61
“Off-label” Uses of rVIIa (cont)
• Evidence is lagging behind the rising off-label use of rVIIa
• Multiple case series/reports: Benefits in obstetric bleeding, trauma, perioperative
bleeding Beware of perils of case reports: Subjective; no control; bias
(usually only positive experiences are reported)
• Some concerns: Thrombotic complications (eg,
myocardial/cerebral ischemia, DVT, pulmonary embolism)
• At a cost of $2000-$8000 per dose, annual costs of such off-label
uses can easily run into millions of dollars in hospitals
• Only few randomized controlled trials This is changing

62
Trial Title Study Design Phase
Total Enrollmen
tExpected
Completion
"Salvage Use" of Recombinant Activated Factor VII After Inadequate Haemostatic Response to Conventional Therapy in Complex Cardiac Surgery
Multicenter, Treatment, Randomized, Double-Blind, Placebo-Control, Parallel Assignment, Safety/Efficacy Study
Phase 3 40 June 2008
Evaluation of the Quality of the NovoSeven (rFVIIa) Treatment Practice at Rigs hospital, Copenhagen University Hospital
Natural History, Longitudinal, Defined Population, Retrospective/ Prospective Study
?? ?? December 2010
Effect of Recombinant Coagulation Factor VIIa on Peri-Operative Blood Loss in Patients Undergoing Major Burn Excision and Grafting
Randomized, Double-Blind (Subject, Caregiver,Investigator) Placebo-Control, Parallel Assignment, Efficacy Study
Phase 3 52 December 2009
Efficacy and Safety of Factor VIIa (Eptacog Alfa) on Rebleeding After Surgery for Spontaneous Supratentorial Intracerebral Hemorrhage.
Randomized, Controlled, Open-Label, Investigator-Blinded Pilot Study
Phase 2 30 January 2008
US National Institutes of Health. ClinicalTrials.gov. Available at: www.clinicaltrials.gov. Accessed February 10, 2008.
Current Ongoing Global Trials

63
Trial Title Study Design Phase
Total Enrollmen
tExpected
Completion
"Salvage Use" of Recombinant Activated Factor VII After Inadequate Haemostatic Response to Conventional Therapy in Complex Cardiac Surgery
Multicenter, Treatment, Randomized, Double-Blind, Placebo-Control, Parallel Assignment, Safety/Efficacy Study
Phase 3 40 June 2008
Effect of Recombinant Coagulation Factor VIIa on Peri-Operative Blood Loss in Patients Undergoing Major Burn Excision and Grafting
Randomized, Double-Blind (Subject, Caregiver, Investigator) Placebo-Control, Parallel Assignment, Efficacy Study
Phase 3 52 December 2009
Efficacy and Safety of Factor VIIa on Rebleeding After Surgery for Spontaneous Intracerebral Hemorrhage (ICH) (PRE-SICH).
Randomized, Controlled, Open-Label, Investigator-Blinded Pilot Study
Phase 2 30 January 2008
Current Ongoing Global Trials (cont)
US National Institutes of Health. ClinicalTrials.gov. Available at: www.clinicaltrials.gov. Accessed February 10, 2008.

64
Trial Title Study Design PhaseTotal
EnrollmentExpected
Completion
Recombinant Human Activated Factor VII as Salvage Therapy in Women With Severe Postpartum Hemorrhage
Randomized, Open-Label, Active Control, Parallel Assignment, Safety/Efficacy Study
Phase 4 84 December 2009
Randomized, Open, Prospective, Multicenter Pilot Study to Evaluate the Efficacy and Safety of Activated Recombinant Factor VII in Acute Intracerebral Haemorrhage in Patients Treated With Oral Anticoagulants or Antiplatelets Agents.
Randomized, Single-Blind, Active Control, Parallel Assignment, Safety/Efficacy Study
Phase 2 32 September 2006
The Use of rFVIIa in Trauma Patients: A Multi-Center Case Registry
Natural History, Cross-Sectional, Case Control, Retrospective/Prospective Study
?? 1000 Not recruiting yet
Assessment of rFVIIa in Controlling Bleeding in Patients With Severe Trauma Injuries
Treatment, Randomized, Double-Blind, Placebo Control, Parallel Assignment, Safety/Efficacy Study
Phase 3 1502 Recruiting
US National Institutes of Health. ClinicalTrials.gov. Available at: www.clinicaltrials.gov. Accessed February 10, 2008.
Current Ongoing Global Trials (cont)

65
Patient Case: Adam B.
• Dx: Post-op coagulopathy and uncontrolled bleeding
• History: 50-year-old male; had antibodies to c and E Suffered excessive bleeding during surgery and narrowly
avoided transfusion of incompatible blood Ongoing chest tube drainage in the 2 weeks following
surgery required transfusion of 1 U QOD Last night, he developed coagulopathy and dramatically
increased bleeding Increasing clotting times not corrected by FFP HCT declined to 19% Antigen-negative PRBC were not immediately available
HCT=hematocrit; PRBC=packed red blood cells.

66
Patient Case: Adam B.
• First thoughts about continuing to transfuse Adam B. What are the risks associated with additional
transfusions?
What Would You Do Next?

67
Take-Away Points
• Achieving optimal operative hemostasis means maintaining balance between bleeding and clotting
• Preoperative risk assessment may predict who will bleed • Transfusion concerns include risks, costs, and impact on patient
quality of life• Look at patient’s risks for complications and think about the
balance• Incorporate blood conservation and prohemostatic therapy into
hemostasis strategy
“Keeping On Center”

68
For more CE/CME educational programs on the subject of operative hemostasis and transfusion medicine, including uniquely progressive learning designed for each clinical discipline, log on to:
www.bloodcmecenter.org

69
Specialty-Specific Clinical Cases
More Opportunities to Decide …
What You Would Do Next!

70
Patient Case: Brian C.
• Dx: Acute cholecystitis• History: 54-year-old male; 5’11,” 240 lb; third ED visit for
same reason H/O appendectomy; mild high BP (on BP meds and baby
aspirin) and borderline diabetes mellitus (no meds) Labsnormal PT and PTT; HCT 39%, platelets 410,000 Lap cholecystectomy was performed with difficult
establishment of pneumoperitoneum Bleeding began at base of gall bladder Cauterization failed to arrest bleeding Pressure and topical hemostatics failed to help
Consult: Agreed to switch to open procedure 2500 cc blood in abdomen on opening HCT 22%, platelets 140,000 Liver was packed; gall bladder was removed; and after
8 U of PRBC, 1 of cryoprecipitate and 1 of FFP, patient was still bleeding
What Would You Do Next?

71
Patient Case: Chaney D.
• Dx: Abdominal crush injury, fracture of both tibias, and closed head trauma
• History: Very fit 47-year-old male, no previous surgery, only med was baby aspirin Head-on collision, spun around, and hit head-on from rear
again; air bags deployed after first hit only Exploratory lap removed spleen, and liver laceration
repaired After 2 hours, 12 U PRBC, FFP, cryoprecipitate; bleeding
continued from liver Damage control planned and liver tightly packed
HCT 22%, platelets 85,000 Plan to re-explore the next day Bled through the packing and returned to OR HCT 16%, platelets 44,000
What Would You Do Next?

72
Patient Case: Deidre E.
• Dx: Postpartum hemorrhage• History: 38-year-old had C section for failure to progress with
delivery of 8 lb, 11 oz baby with mild preeclampsia Pre-op HCT was 31% and EBL was 600 cc 2 hours postpartum, patient showed signs of volume
depletion, with decreased urine output and low BP HCT was 20%, fibrinogen <100; FDP elevated and
platelets 75,000 Urine was grossly bloody, glucose 60 and LFT drawn Repeat platelet count was 30,000 and blood was not clotting HELLP syndrome was diagnosed and transfusions begun
What Would You Do Next?

73
Patient Case: Elvin F.
• Dx: Hip replacement from traumatic arthritis
• History: 54-year-old male with mild hypertension (on meds) Labs normal; received 5000 U heparin preoperatively Began bleeding heavily; received third and forth units of
blood, and cell saver used HCT 24 (37 pre-op), platelets 125,000 and fibrinogen 50 Urine blood tinged; according to patient’s wife, he was
taking 1600 mg ibuprofen and possibly a baby aspirin FDP was positive and patient developed a coagulopathy Patient was warmed; acidosis and volume status corrected
What Would You Do Next?

74
Patient Case: Fenton G.
• Dx: Urgent repeat on-pump CABG due to unstable angina• History: 68-year-old male with prior CABG, several MIs, CHF
(on lisinopril) 3-vessel disease noted with EF 25%; LMWH given in cath lab Patient had high BP (on BP meds and clopidogrel) and type 2
diabetes mellitus HCT 42%, platelets 220,000 1 g TXA given after intubation followed by 200 mg/min Heparin 10,000 U in CPB reservoir and 400 U/kg On separation from bypass, HCT 24%, with 1 L volume in
reservoir Intra-aortic balloon pump placed and patient given milrinone
and norepinephrine Protamine returns ACT to normal Patient oozy at closure Patient continues to bleed in PACU at rate of 200 cc per hour
What Would You Do Next?

75
Patient Case: Gavin H.
• Dx: Trabeculated bladder with UA stones• History: 70-year-old male with BPH; taking finasteride
and tamsulosin On BP med (amlodipine) and aspirin; PSA 1.2 Coagulation studies normal and platelets 225,000 TURP performed under general anesthesia Bleeding was encountered; attempts at cautery unsuccessful 60 cc foley placed on stretch with irrigation, which cleared
but then became bloody again Bleeding increased the next day HCT was 33% (39 pre-op); resection attempts failed to
arrest bleeding
What Would You Do Next?