stopping the revolving door of adhf - american...
TRANSCRIPT

Stopping the Revolving Door of ADHF
Ileana L. Piña, MD, MPHProfessor of Medicine and Epidemiology/Population Health
Associate Chief for Academic Affairs -- CardiologyMontefiore-Einstein Medical Center
Bronx, NY
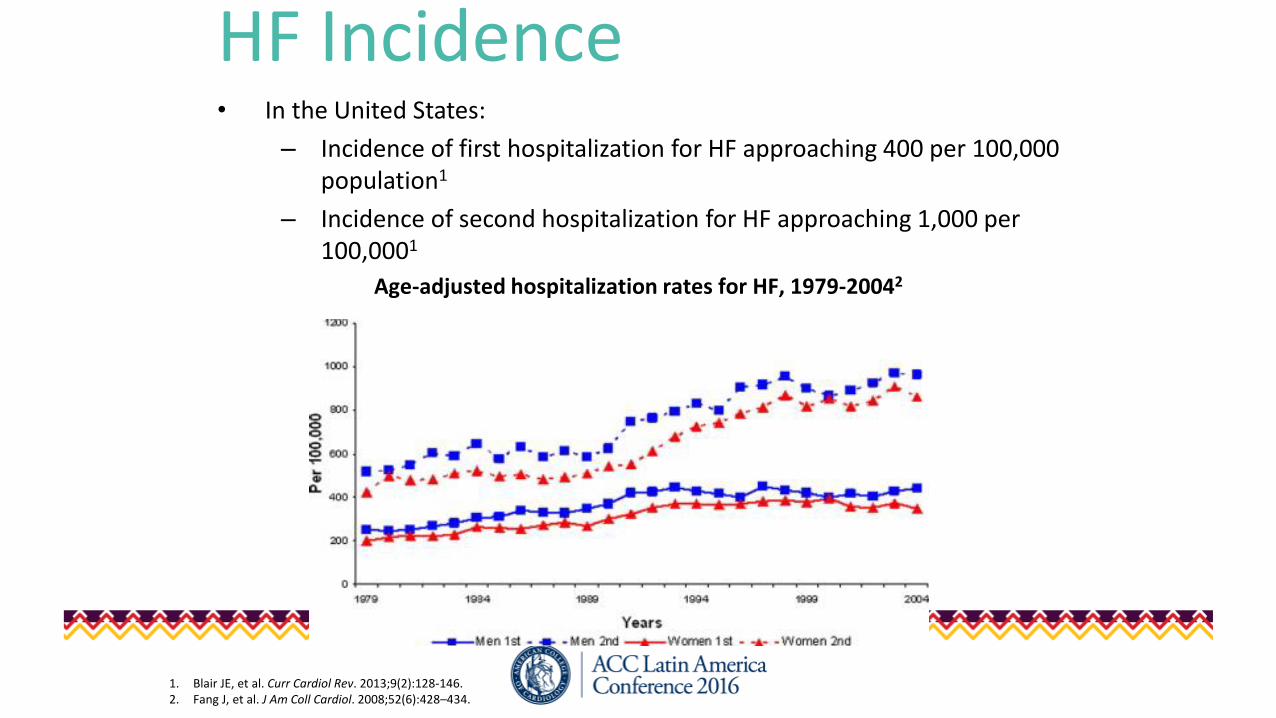
HF Incidence• In the United States:
– Incidence of first hospitalization for HF approaching 400 per 100,000 population1
– Incidence of second hospitalization for HF approaching 1,000 per 100,0001
Age-adjusted hospitalization rates for HF, 1979-20042
1. Blair JE, et al. Curr Cardiol Rev. 2013;9(2):128-146.2. Fang J, et al. J Am Coll Cardiol. 2008;52(6):428–434.
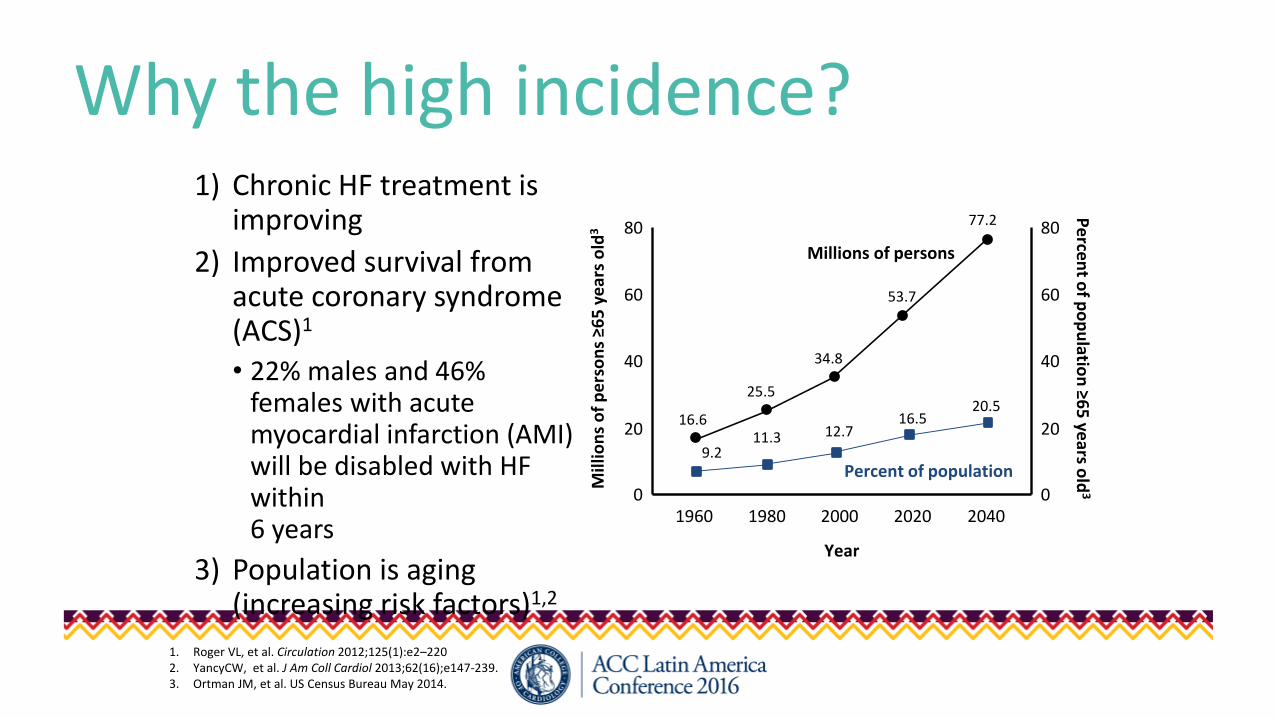
Why the high incidence?1) Chronic HF treatment is
improving
2) Improved survival from acute coronary syndrome (ACS)1
• 22% males and 46% females with acute myocardial infarction (AMI) will be disabled with HF within 6 years
3) Population is aging (increasing risk factors)1,2
1. Roger VL, et al. Circulation 2012;125(1):e2–2202. YancyCW, et al. J Am Coll Cardiol 2013;62(16);e147-239.3. Ortman JM, et al. US Census Bureau May 2014.
80
60
40
20
01960 1980 2000 2020 2040
Year
Mill
ion
s o
f p
ers
on
s ≥6
5 y
ear
s o
ld3
16.6
Pe
rcen
t of p
op
ulatio
n ≥6
5 ye
ars old
3
80
60
40
20
0
25.5
34.8
53.7
77.2
20.516.5
12.711.39.2
Millions of persons
Percent of population
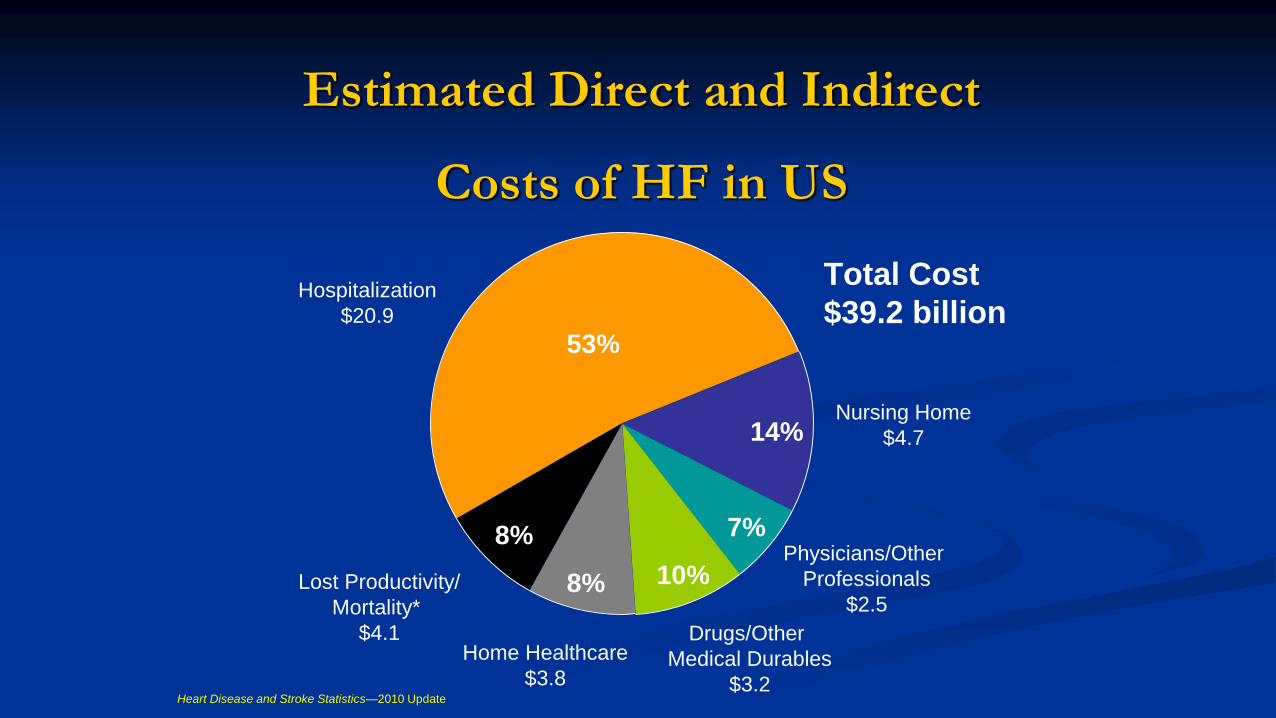
Estimated Direct and Indirect
Costs of HF in US
8%
8% 10%
7%
14%
53%
Hospitalization
$20.9
Lost Productivity/
Mortality*
$4.1Home Healthcare
$3.8
Drugs/Other
Medical Durables
$3.2
Physicians/Other
Professionals
$2.5
Nursing Home
$4.7
Heart Disease and Stroke Statistics—2010 Update
Total Cost
$39.2 billion
6
• Defined as a rapid or gradual change in signs and symptoms in patients with chronic HF or de novo HF that necessitates urgent therapy and/or hospitalization1
• Leading medical cause of hospitalization among people ≥65 years2
• Presentation of AHF represents a period of very high risk, during which the likelihood of death and re-hospitalization is significantly greater than for a comparable period of chronic but stable HF
• Treatment is highly variable and needs to improve1
1. Gheorghiade M, et al. Circulation. 2005;112(25):3958-3968.2. Gheorghiade M, et al. J Am Coll Cardiol. 2009;53(7):557-573.
Acute Heart Failure (AHF)
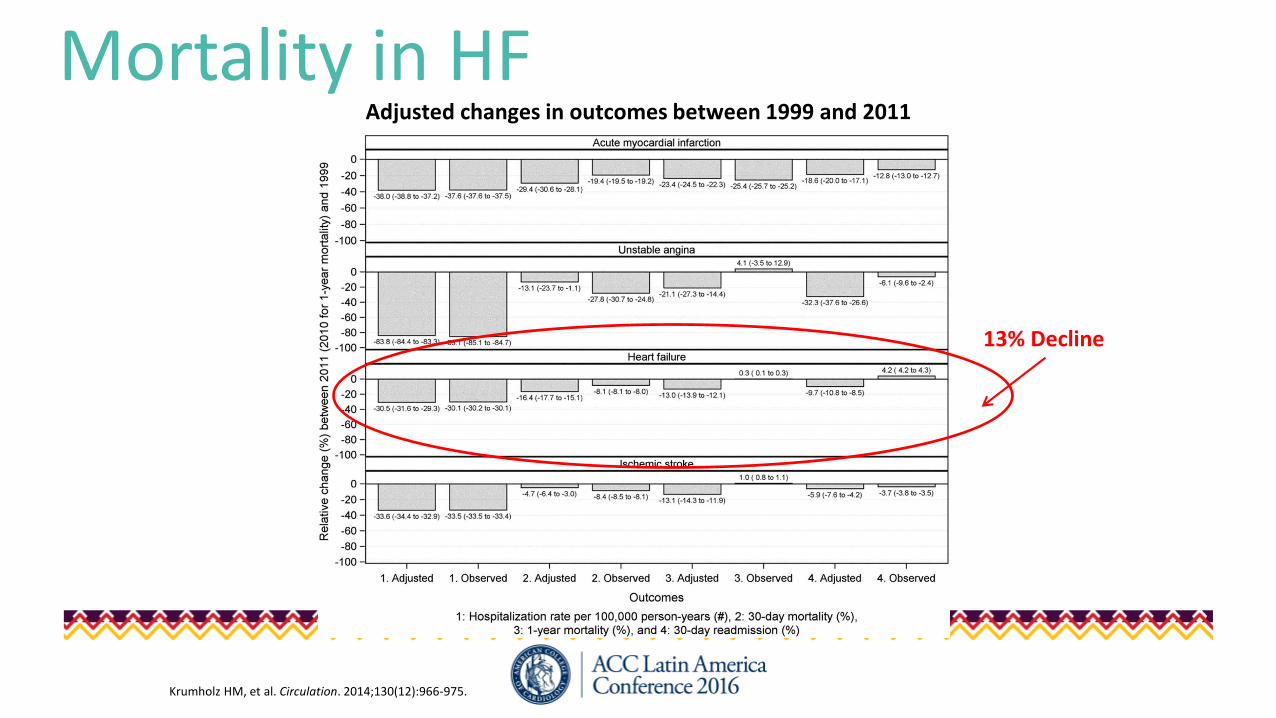
Mortality in HFAdjusted changes in outcomes between 1999 and 2011
13% Decline
Krumholz HM, et al. Circulation. 2014;130(12):966-975.
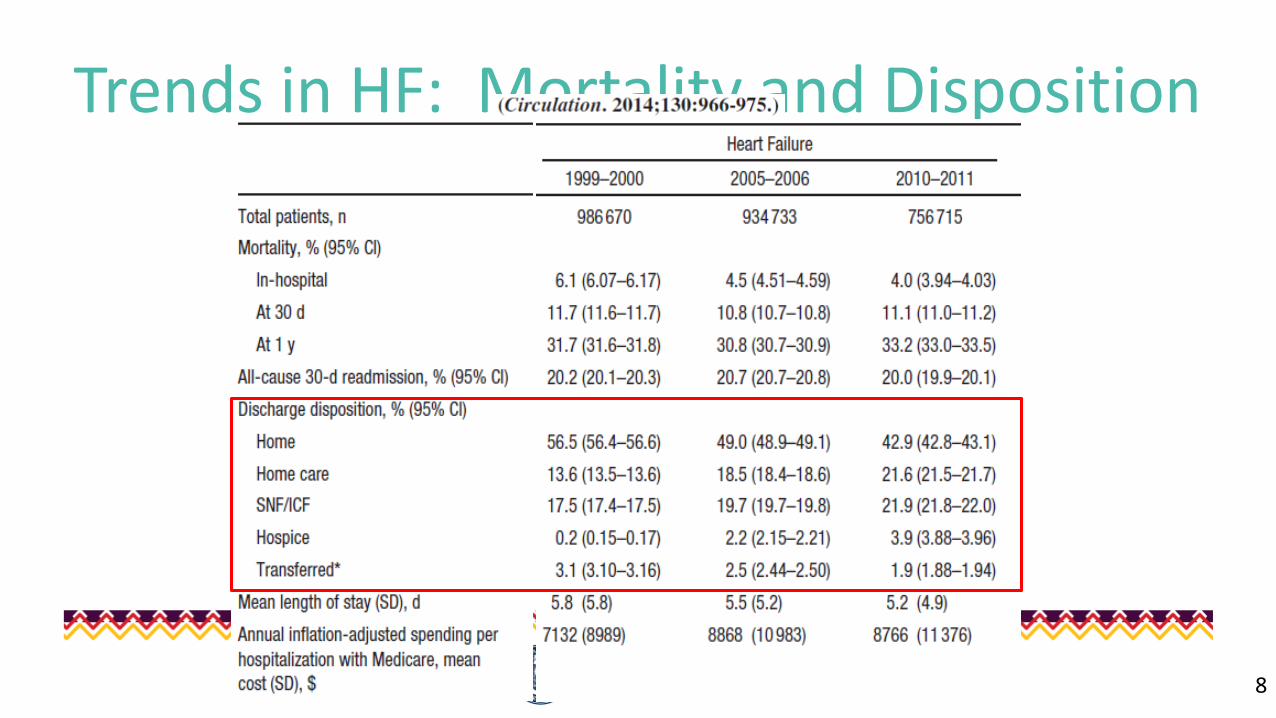
Trends in HF: Mortality and Disposition
8
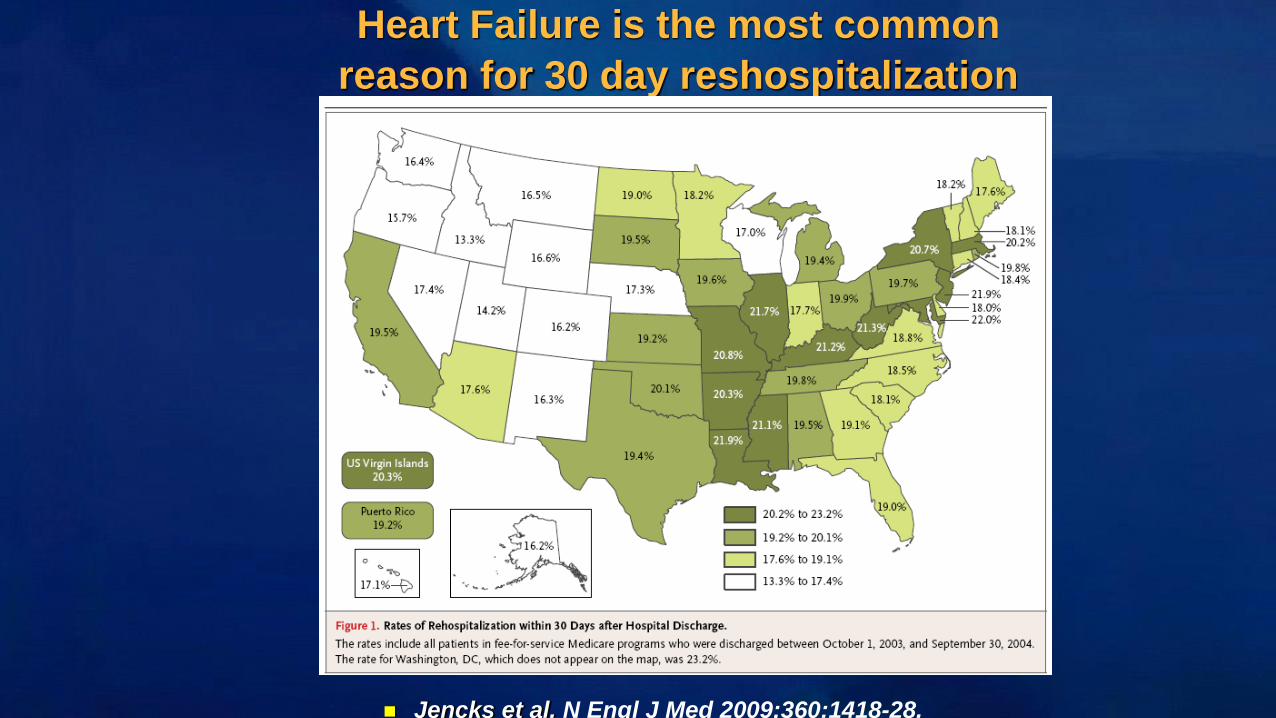
Heart Failure is the most common
reason for 30 day reshospitalization
Jencks et al. N Engl J Med 2009;360:1418-28.
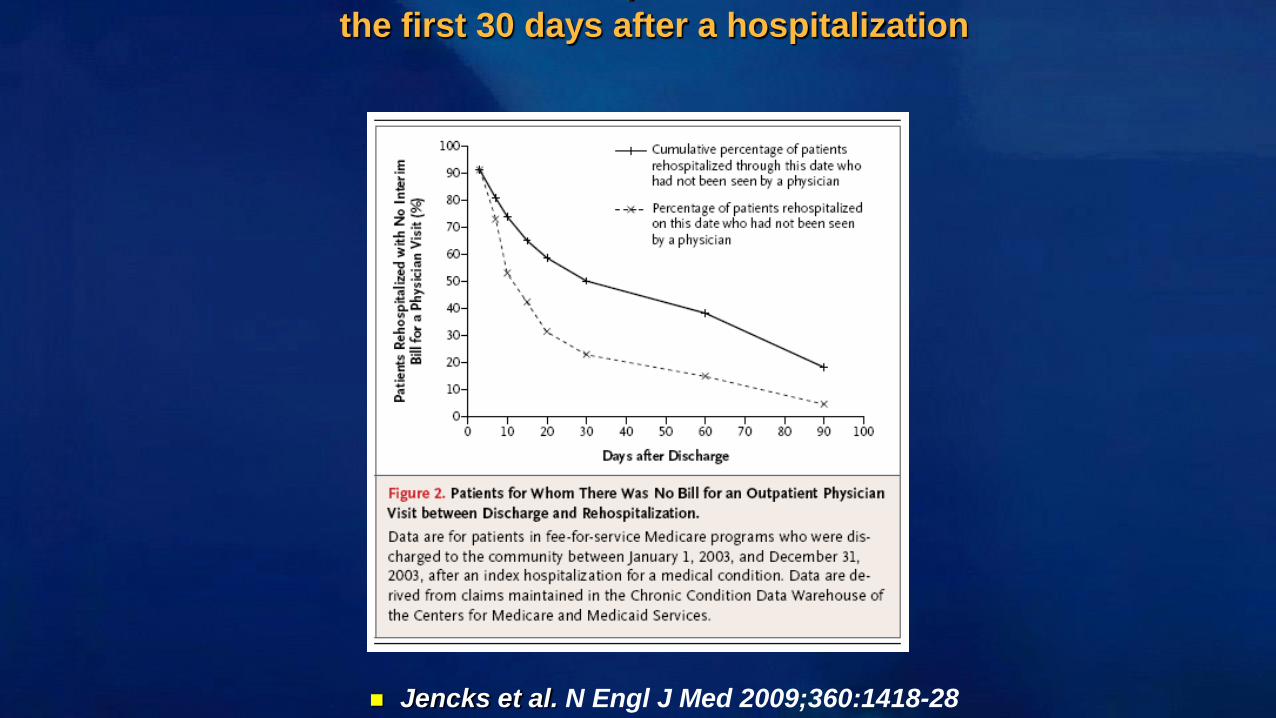
52% of heart failure patients are not seen in
the first 30 days after a hospitalization
Jencks et al. N Engl J Med 2009;360:1418-28
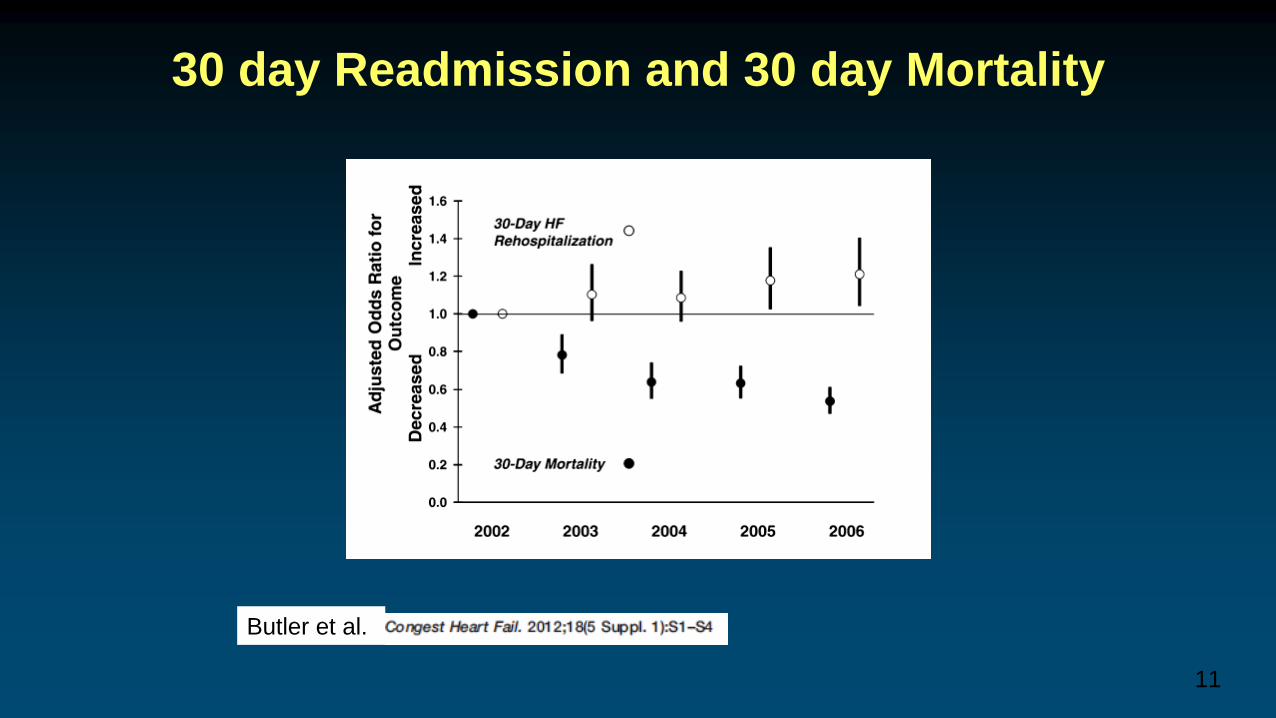
30 day Readmission and 30 day Mortality
11
Butler et al.
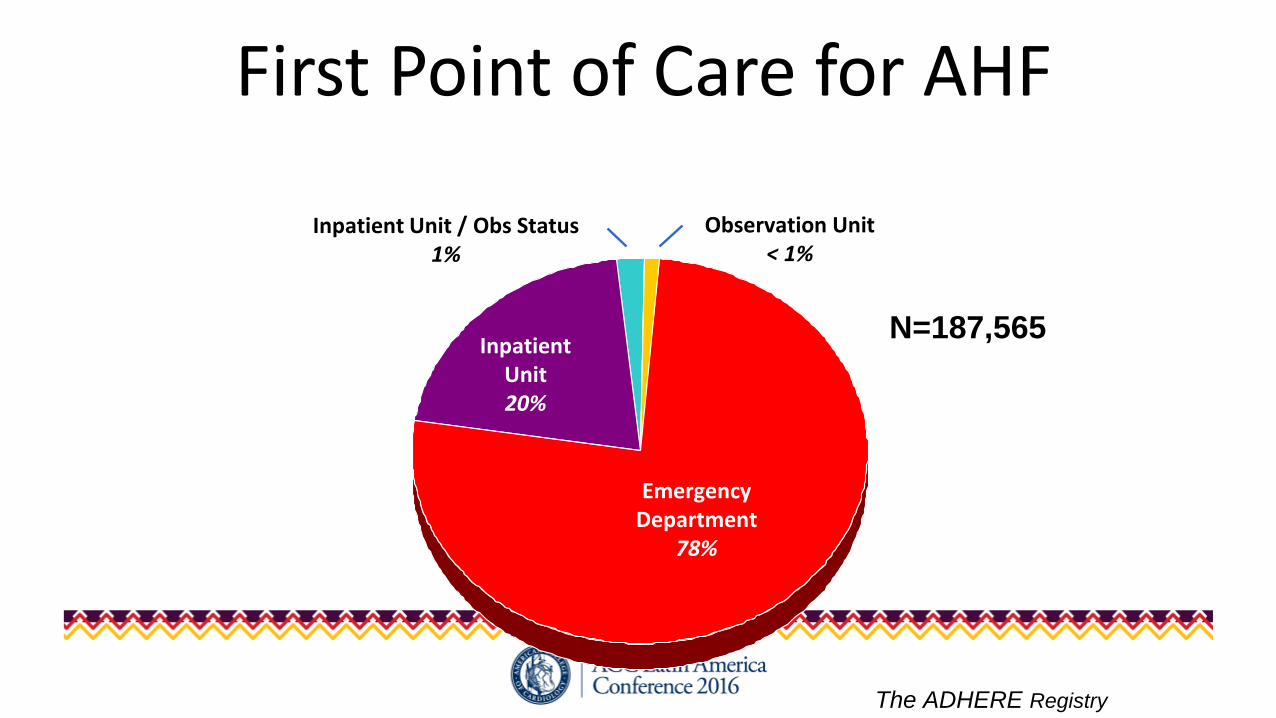
First Point of Care for AHF
InpatientUnit20%
Inpatient Unit / Obs Status1%
Observation Unit< 1%
Emergency Department
78%
N=187,565
The ADHERE Registry
• “Lower-risk” patients exist
• Are ED MDs ready to discharge from ED?
• 23 hours → clinical stability and self-care barriers addressed
13Collins JACC 2013 61(2):121-6
14
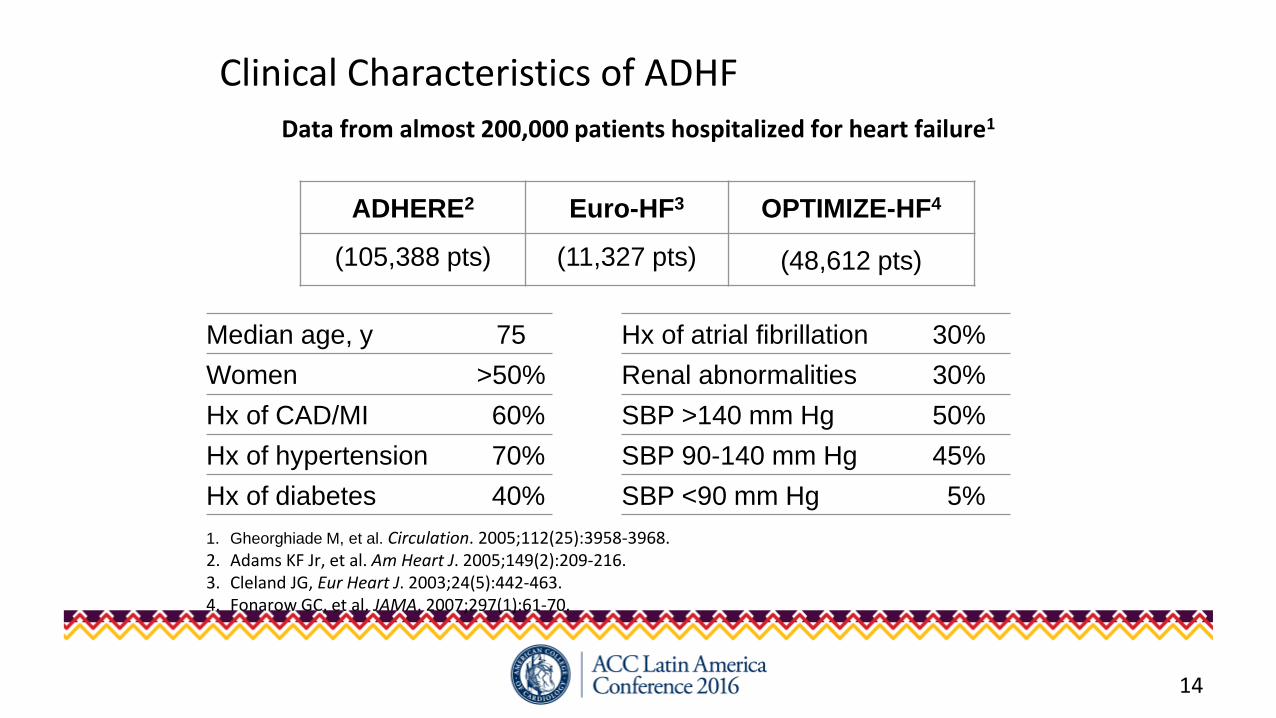
Clinical Characteristics of ADHF
Median age, y 75 Hx of atrial fibrillation 30%
Women >50% Renal abnormalities 30%
Hx of CAD/MI 60% SBP >140 mm Hg 50%
Hx of hypertension 70% SBP 90-140 mm Hg 45%
Hx of diabetes 40% SBP <90 mm Hg 5%
ADHERE2 Euro-HF3 OPTIMIZE-HF4
(105,388 pts) (11,327 pts) (48,612 pts)
1. Gheorghiade M, et al. Circulation. 2005;112(25):3958-3968.2. Adams KF Jr, et al. Am Heart J. 2005;149(2):209-216.3. Cleland JG, Eur Heart J. 2003;24(5):442-463.4. Fonarow GC, et al. JAMA. 2007;297(1):61-70.
Data from almost 200,000 patients hospitalized for heart failure1
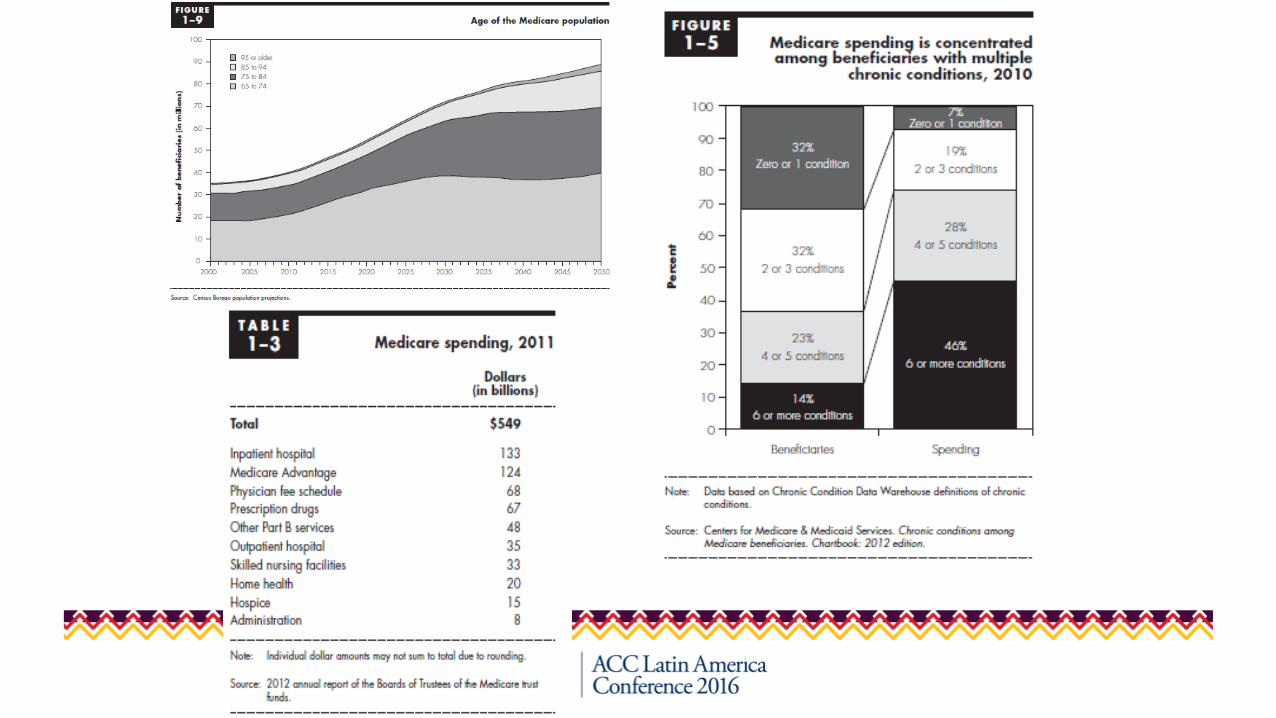
MedPac report March 2013
Comorbidities in AHF• >40% of patients age 65 years and up with HF have
more than 5 comorbidities1
• Significant independent predictors of mortality:1
– Chronic kidney disease– Chronic obstructive pulmonary disease– Peripheral arterial disease
• Warrants heightened level of clinical suspicion and appropriate screening
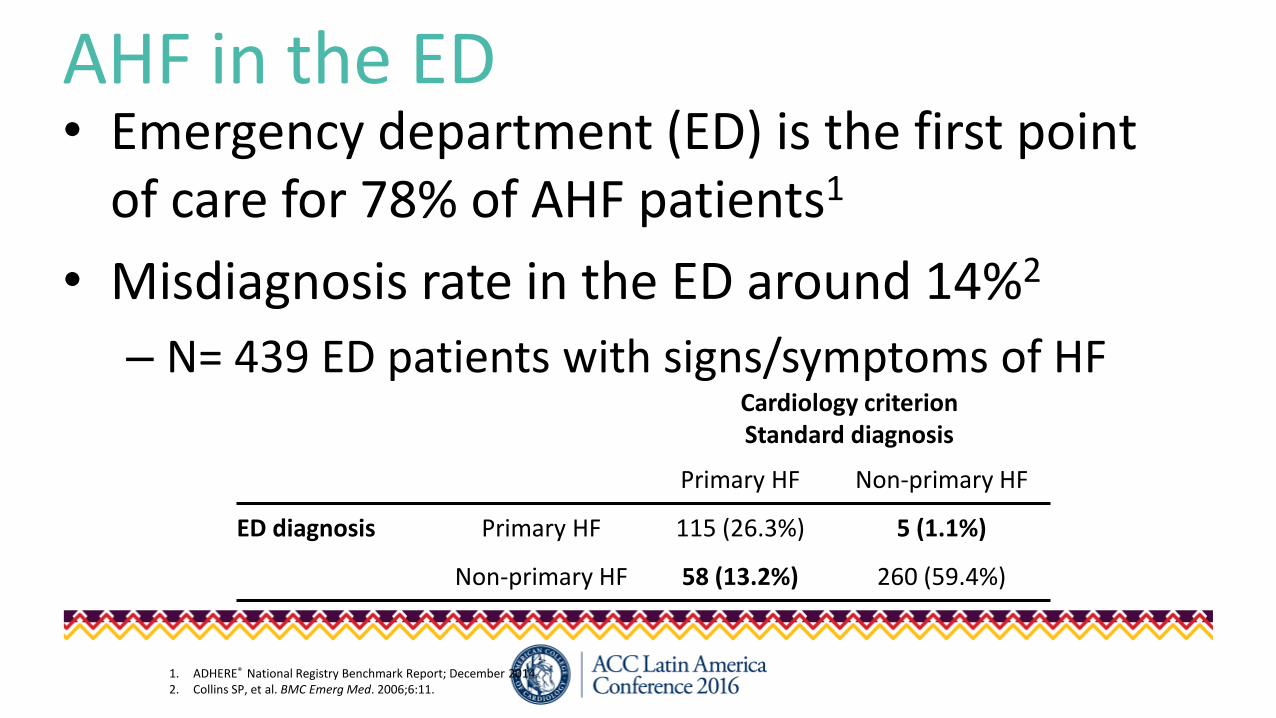
AHF in the ED• Emergency department (ED) is the first point
of care for 78% of AHF patients1
• Misdiagnosis rate in the ED around 14%2
– N= 439 ED patients with signs/symptoms of HFCardiology criterionStandard diagnosis
Primary HF Non-primary HF
ED diagnosis Primary HF 115 (26.3%) 5 (1.1%)
Non-primary HF 58 (13.2%) 260 (59.4%)
1. ADHERE® National Registry Benchmark Report; December 2014.2. Collins SP, et al. BMC Emerg Med. 2006;6:11.
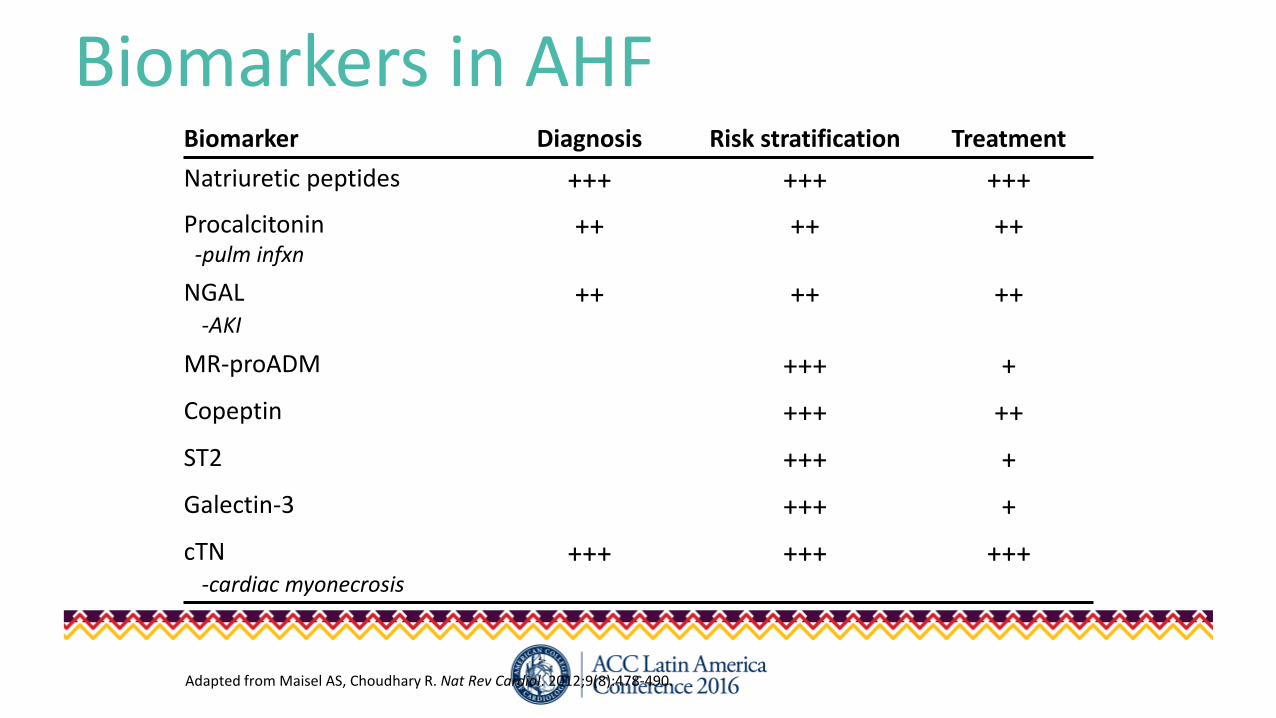
Biomarkers in AHFBiomarker Diagnosis Risk stratification Treatment
Natriuretic peptides +++ +++ +++
Procalcitonin-pulm infxn
++ ++ ++
NGAL-AKI
++ ++ ++
MR-proADM +++ +
Copeptin +++ ++
ST2 +++ +
Galectin-3 +++ +
cTN-cardiac myonecrosis
+++ +++ +++
Adapted from Maisel AS, Choudhary R. Nat Rev Cardiol. 2012;9(8):478-490.

Initial Assessment and Management: 5 Questions to Ask1) Stable?
– NIV, IV vasoactives
2) SBP >140 mmHg?– Yes? SLNTG followed by IV NTG– No? 2x home diuretic
3) Vitals?– Tachycardia, low BP (not shock)
4) Cause? – Nonadherence (self-care)?– ACS, Infxn?
5) Test results?– Tn, Na2+
– BUN/Cr– Response to therapy
Gheorghiade M, Braunwald E. JAMA. 2011;305(16):1702-1703.
Risk Assessment and Disposition• Two pieces to risk-stratification:
1. Immediate risk – measures of ACUTE severity
•Hypoxia, hypotension, respiratory distress, hypertension?
• Immediate ≠ intermediate2. Intermediate risk (5-days through 30−60 days)
• Renal dysfunction
•Hyponatremia
• Ischemia on ECG / elevated Tn
• Low BP (not shock)
•BNP
Collins SP, et al. Crit Pathways Cardiol. 2008;7(2):96-102.
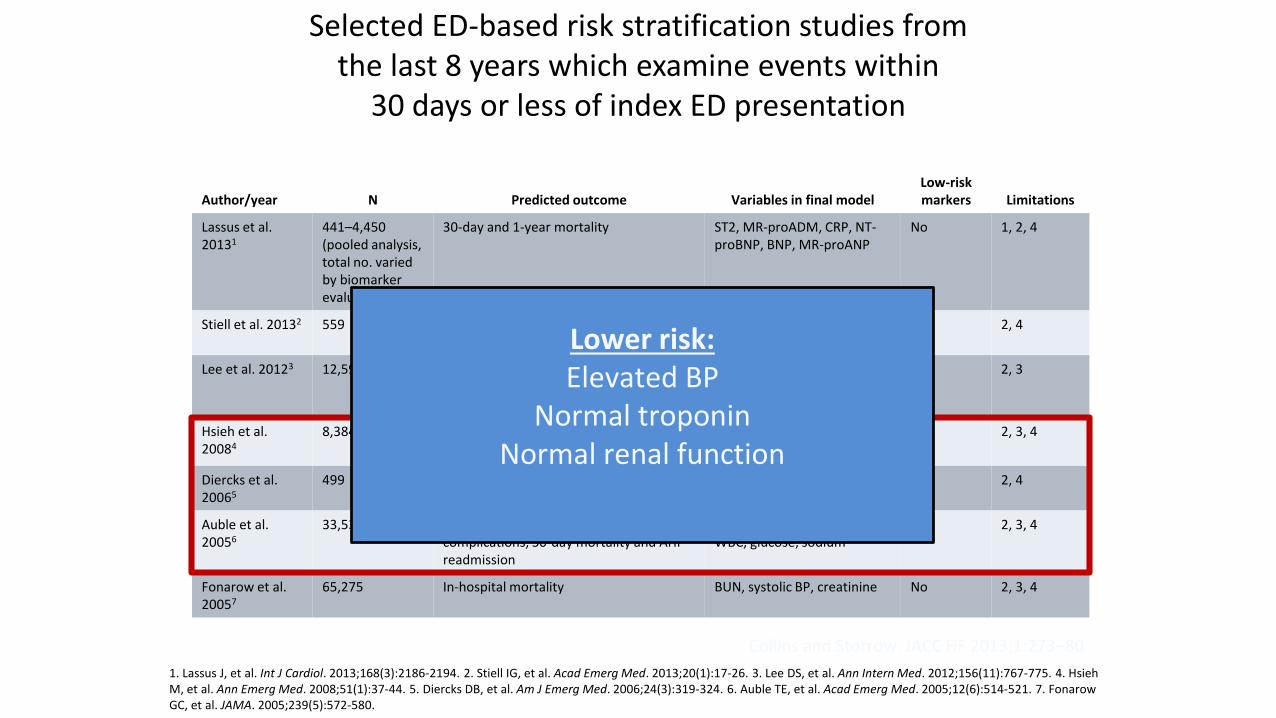
Selected ED-based risk stratification studies fromthe last 8 years which examine events within
30 days or less of index ED presentation
Collins and Storrow. JACC HF 2013;1:273–80
Author/year N Predicted outcome Variables in final modelLow-risk markers Limitations
Lassus et al. 20131
441–4,450 (pooled analysis, total no. varied by biomarker evaluated)
30-day and 1-year mortality ST2, MR-proADM, CRP, NT-proBNP, BNP, MR-proANP
No 1, 2, 4
Stiell et al. 20132 559 30-day death and 14-day serious nonfatal events
h/o TIA/CVA, vital signs, ECG and laboratory findings
No 2, 4
Lee et al. 20123 12,591 7-day mortality Creatinine, BP, O2 satn, Tn, h/o cancer, home metolazone, EMS, transport
Yes 2, 3
Hsieh et al. 20084
8,384 In patient mortality or serious medical complications, 30-day mortality
pH, pulse, renal function, WBC, glucose, sodium
Yes 2, 3, 4
Diercks et al. 20065
499 Stay <24 h in observation and no 30-day adverse cardiac events
Tn, systolic BP Yes 2, 4
Auble et al. 20056
33,533 In patient mortality or serious medical complications, 30-day mortality and AHF readmission
pH, pulse, renal function, WBC, glucose, sodium
Yes 2, 3, 4
Fonarow et al. 20057
65,275 In-hospital mortality BUN, systolic BP, creatinine No 2, 3, 4
Lower risk:Elevated BP
Normal troponin Normal renal function
1. Lassus J, et al. Int J Cardiol. 2013;168(3):2186-2194. 2. Stiell IG, et al. Acad Emerg Med. 2013;20(1):17-26. 3. Lee DS, et al. Ann Intern Med. 2012;156(11):767-775. 4. Hsieh M, et al. Ann Emerg Med. 2008;51(1):37-44. 5. Diercks DB, et al. Am J Emerg Med. 2006;24(3):319-324. 6. Auble TE, et al. Acad Emerg Med. 2005;12(6):514-521. 7. FonarowGC, et al. JAMA. 2005;239(5):572-580.
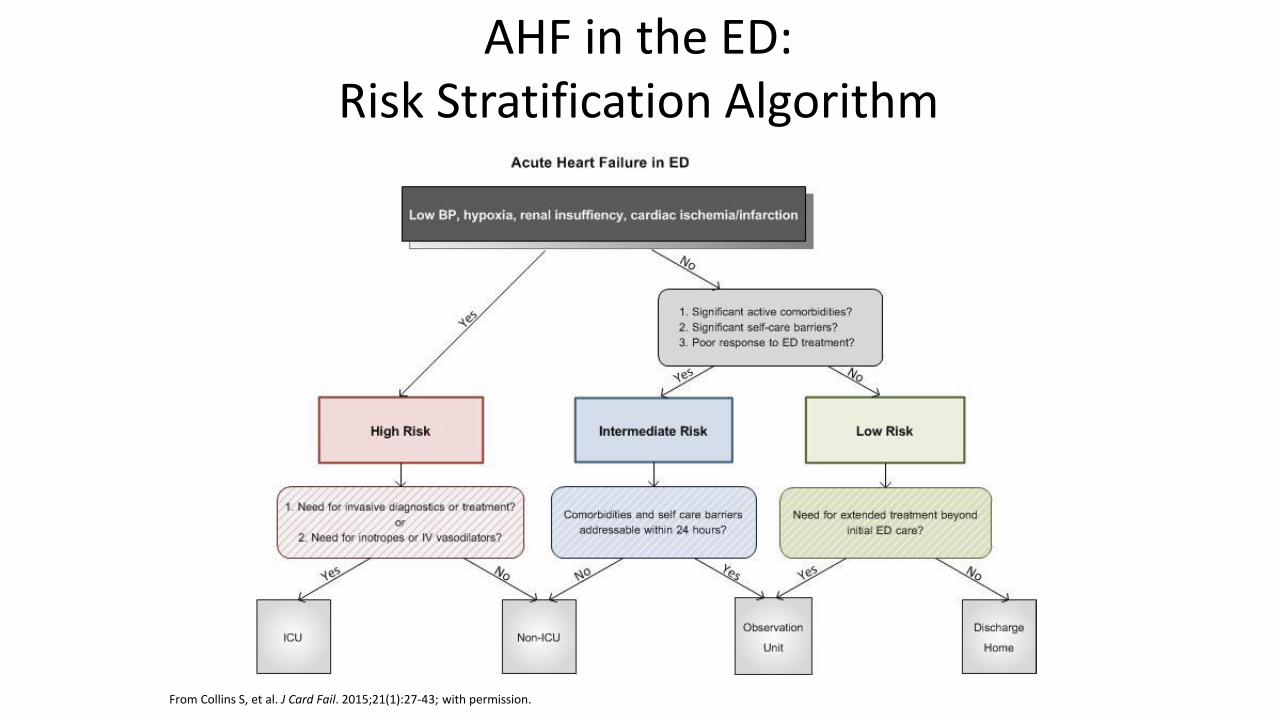
AHF in the ED: Risk Stratification Algorithm
From Collins S, et al. J Card Fail. 2015;21(1):27-43; with permission.

Therapy: No new therapies approved since
nesiritide● Diuretics!
● Diuretics!
● Diuretics!
● Vasodilators
– Nitrates
– Nesiritide
– Nitroprusside
● Inodilators
– Milrinone
● Inotropes
– Dobutamine, dopamine
● Novel agents
– serelaxin 23
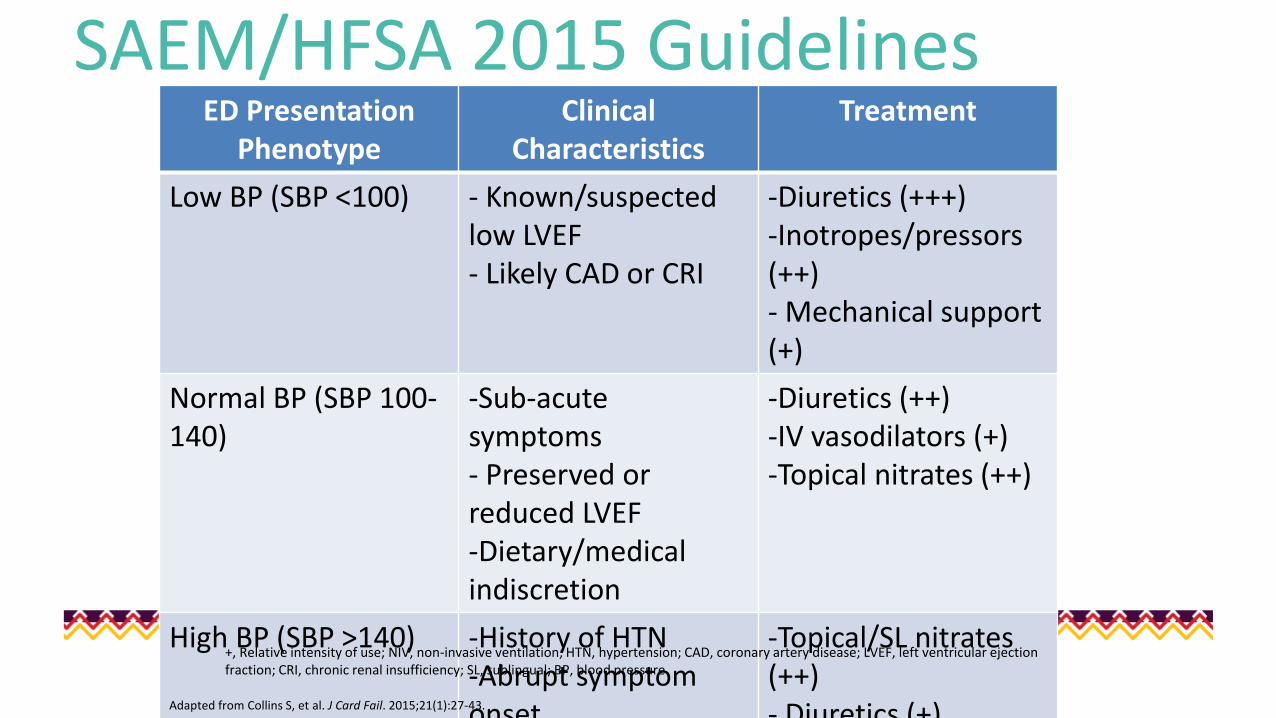
SAEM/HFSA 2015 GuidelinesED Presentation
PhenotypeClinical
CharacteristicsTreatment
Low BP (SBP <100) - Known/suspected low LVEF- Likely CAD or CRI
-Diuretics (+++)-Inotropes/pressors(++)- Mechanical support (+)
Normal BP (SBP 100-140)
-Sub-acute symptoms- Preserved or reduced LVEF-Dietary/medical indiscretion
-Diuretics (++)-IV vasodilators (+)-Topical nitrates (++)
High BP (SBP >140) -History of HTN-Abrupt symptom onset
-Topical/SL nitrates (++)- Diuretics (+)
+, Relative intensity of use; NIV, non-invasive ventilation; HTN, hypertension; CAD, coronary artery disease; LVEF, left ventricular ejection fraction; CRI, chronic renal insufficiency; SL, sublingual; BP, blood pressure
Adapted from Collins S, et al. J Card Fail. 2015;21(1):27-43.
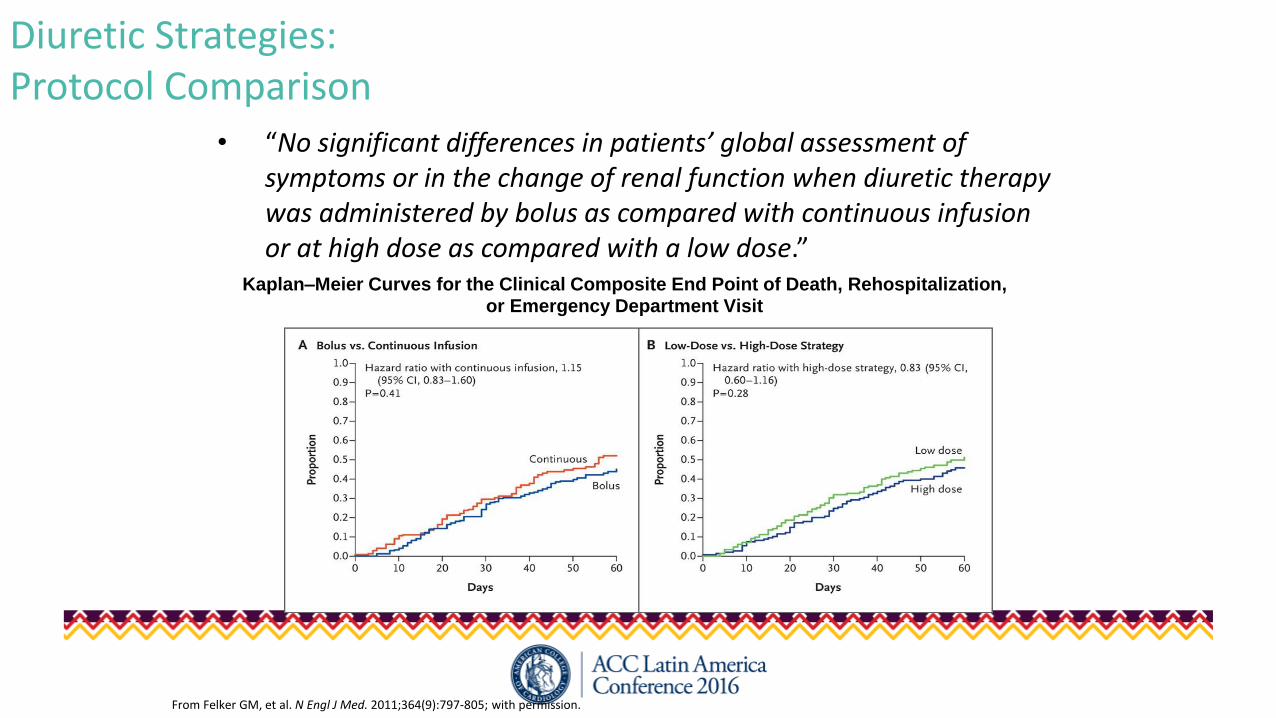
Diuretic Strategies: Protocol Comparison
• “No significant differences in patients’ global assessment of symptoms or in the change of renal function when diuretic therapy was administered by bolus as compared with continuous infusion or at high dose as compared with a low dose.”
Kaplan–Meier Curves for the Clinical Composite End Point of Death, Rehospitalization, or Emergency Department Visit
From Felker GM, et al. N Engl J Med. 2011;364(9):797-805; with permission.
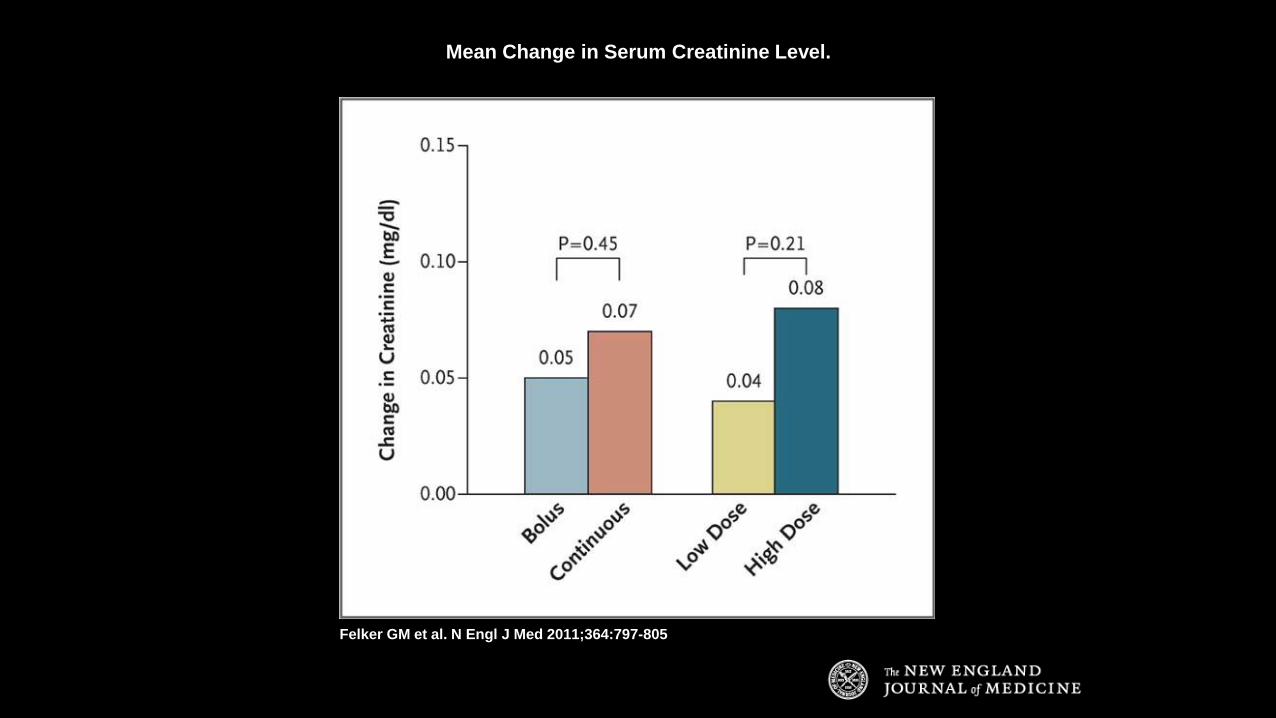
Mean Change in Serum Creatinine Level.
Felker GM et al. N Engl J Med 2011;364:797-805
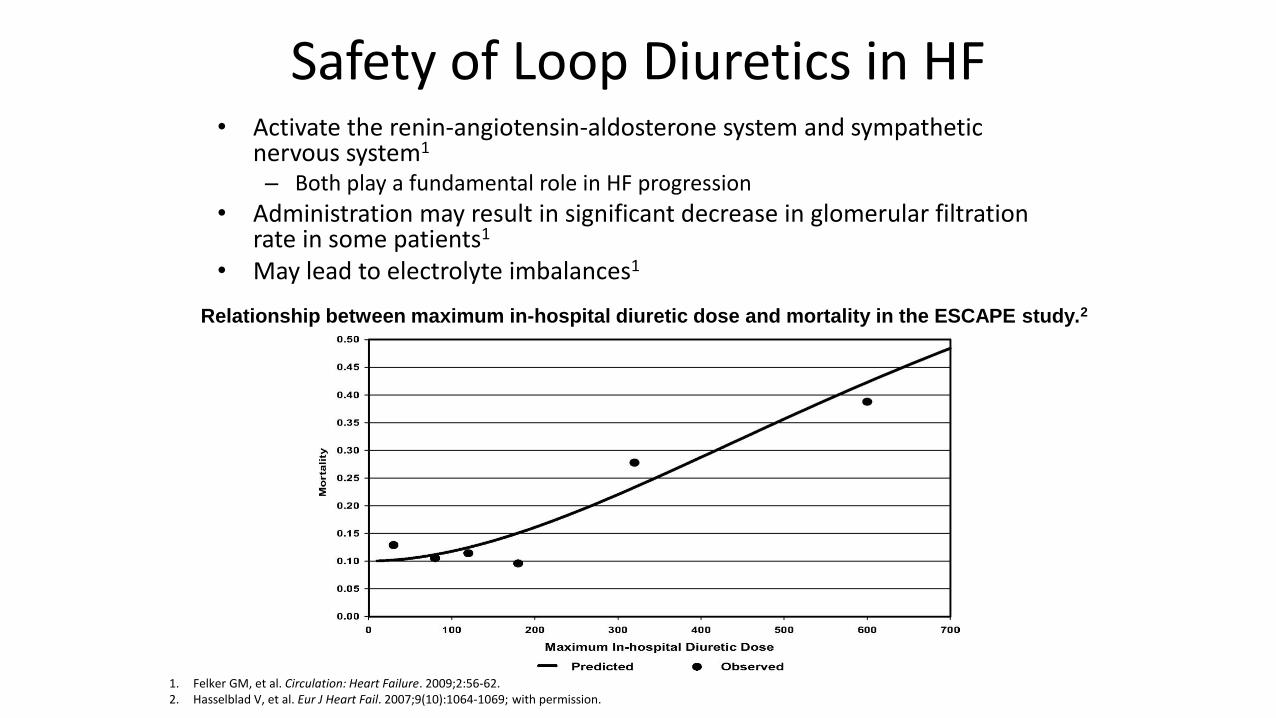
Safety of Loop Diuretics in HF• Activate the renin-angiotensin-aldosterone system and sympathetic
nervous system1
– Both play a fundamental role in HF progression
• Administration may result in significant decrease in glomerular filtration rate in some patients1
• May lead to electrolyte imbalances1
Relationship between maximum in-hospital diuretic dose and mortality in the ESCAPE study.2
1. Felker GM, et al. Circulation: Heart Failure. 2009;2:56-62.2. Hasselblad V, et al. Eur J Heart Fail. 2007;9(10):1064-1069; with permission.
2010 HFSA Recommendations for Vasodilator Therapy• IV vasodilators and diuretics recommended for rapid symptom relief in
patients with acute pulmonary edema or severe hypertension• In the absence of symptomatic hypotenstion, IV nitroglycerin,
nitroprusside, or nesiritide may be considered as an addition to diuretic therapy for rapid improvement of congestive symptoms
• Frequent blood pressure monitoring recommended– Decrease dosage if symptomatic hypotension develops
• IV nitroprusside, nitroglycerin, or nesiritide may be considered in patients with AHF and advanced HF who have persistent severe HF despite aggressive treatment with diuretics and standard oral therapies
Lindenfeld J, et al. J Card Fail. 2010;16(6):e1.
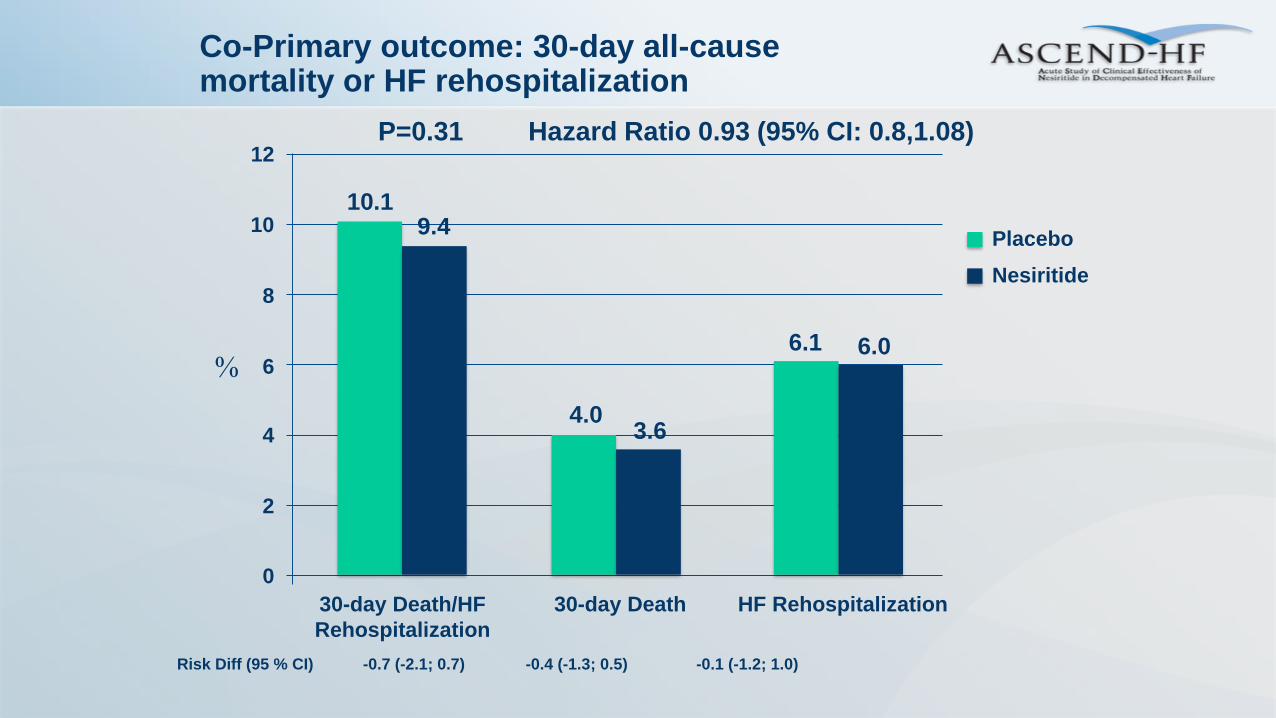
Co-Primary outcome: 30-day all-cause mortality or HF rehospitalization
10.1
4.0
6.1
Hazard Ratio 0.93 (95% CI: 0.8,1.08)
9.4
3.6
6.0
Placebo
Nesiritide
HF Rehospitalization30-day Death/HF
Rehospitalization
30-day Death
0
2
4
6
8
10
12
Risk Diff (95 % CI) -0.7 (-2.1; 0.7) -0.4 (-1.3; 0.5) -0.1 (-1.2; 1.0)
%
P=0.31