stewardship mirata ai farmaci o alla patologia? rosa.pdf · •definire dosaggio e durata della...
TRANSCRIPT

Stewardship Mirata ai Farmaci o Alla
Patologia?
Francesco G. De Rosa

Disclosures
Consultant/Advisory Board
• Pfizer, MSD, AstraZeneca, Astellas Pharma, Basilea
Speaker fees
• Pfizer, MSD, Astellas Pharma, Novartis, Gilead Sciences, AstraZeneca, Thermo Fisher

Insegnamenti Tradizionali
• Definire la diagnosi
• Scegliere l’antibiotico
• Definire dosaggio e durata della terapia
• Prevenire gli effetti collaterali
• Ridurre la comparsa di antibiotico-resistenza

Purpose of Antimicrobial
Stewardship
• Optimize antibiotic use and clinical outcome
• Limit emergence of antibiotic resistance
• Limit adverse events:
• i.e. Antibiotic-associated diarrhea
• Reduce health-care associated infections
• Reduce costs
• Restrictive versus Persuasive Strategies

Prescriptions
Patients
Pharmacies
Inappropriate Antibiotic Use
Resistant Infections
Treatment failures
Increased
morbidity
Increased mortality
Increased costs
Lack of Infection Control
Diagnosis
Patient Expectations
Economic incentives
Lack of knowledge
Lack of diagnostics
No updated guidelines
Lack of time /
convenience
On / off-label
Costs
Economic incentives
Prescription control
Ward pharmacist
Prophylaxis
Empiric Treatment
Targeted Treatment

Does Antibiotic Stewardship Work?
• Yes • According to a Cochrane review and meta-analysis
• Interventions to reduce excessive antibioticprescribing to patients in hospitals can:– Decrease antimicrobial resistance
– Reduce hospital-acquired infections
– Improve clinical outcome
– Reduce costs– Direct & indirect
– Davey P et al. Interventions to improve antibioticprescribing practices for hospital inpatients. CochraneDatabase Syst Rev 2013; 4: CD003543



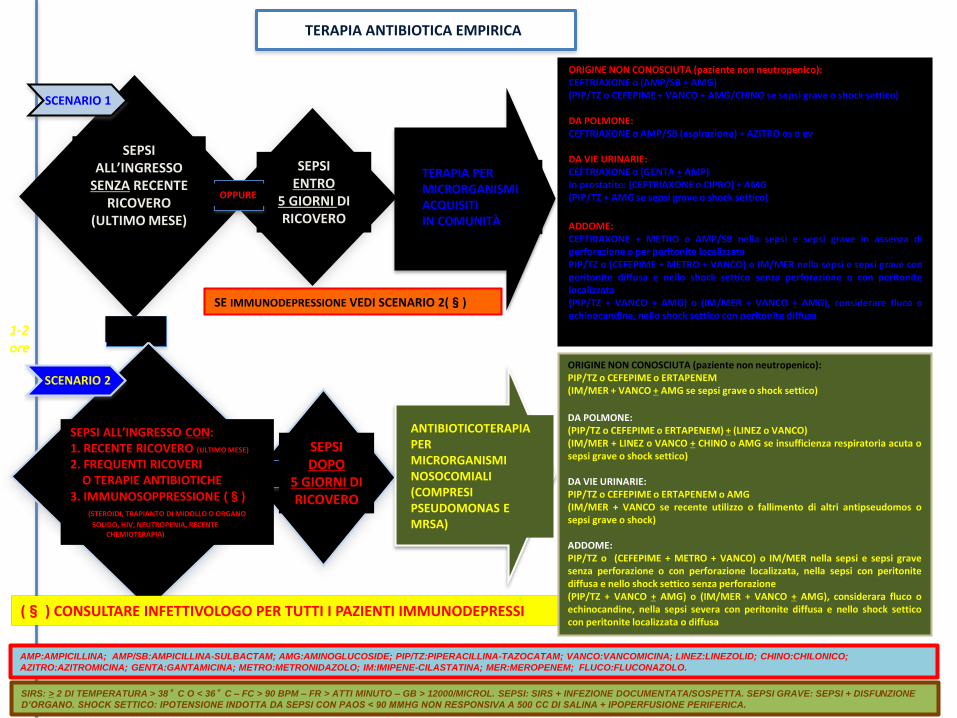
SEPSI ENTRO
5 GIORNI DI RICOVERO
SEPSI ALL’INGRESSO CON:1. RECENTE RICOVERO (ULTIMO MESE)
2. FREQUENTI RICOVERI O TERAPIE ANTIBIOTICHE
3. IMMUNOSOPPRESSIONE (§) (STEROIDI, TRAPIANTO DI MIDOLLO O ORGANO
SOLIDO, HIV, NEUTROPENIA, RECENTE CHEMIOTERAPIA)
OPPURE
SEPSI ALL’INGRESSO
SENZA RECENTE RICOVERO
(ULTIMO MESE)
SEPSI DOPO
5 GIORNI DI RICOVERO
OPPURE
TERAPIA ANTIBIOTICA EMPIRICA
SCENARIO 2
TERAPIA PER MICRORGANISMI ACQUISITI IN COMUNITÀ
(§ ) CONSULTARE INFETTIVOLOGO PER TUTTI I PAZIENTI IMMUNODEPRESSI
SE IMMUNODEPRESSIONE VEDI SCENARIO 2(§)
SCENARIO 1
ORIGINE NON CONOSCIUTA (paziente non neutropenico):CEFTRIAXONE o (AMP/SB + AMG)(PIP/TZ o CEFEPIME + VANCO + AMG/CHINO se sepsi grave o shock settico)
DA POLMONE:CEFTRIAXONE o AMP/SB (aspirazione) + AZITRO os o ev
DA VIE URINARIE:CEFTRIAXONE o (GENTA + AMP)In prostatite: (CEFTRIAXONE o CIPRO) + AMG(PIP/TZ + AMG se sepsi grave o shock settico)
ADDOME:CEFTRIAXONE + METRO o AMP/SB nella sepsi e sepsi grave in assenza diperforazione o per peritonite localizzataPIP/TZ o (CEFEPIME + METRO + VANCO) o IM/MER nella sepsi e sepsi grave conperitonite diffusa e nello shock settico senza perforazione o con peritonitelocalizzata(PIP/TZ + VANCO + AMG) o (IM/MER + VANCO + AMG), considerare fluco oechinocandine, nello shock settico con peritonite diffusa
ANTIBIOTICOTERAPIAPER MICRORGANISMI NOSOCOMIALI(COMPRESIPSEUDOMONAS EMRSA)
1-2ore
OPPURE
ORIGINE NON CONOSCIUTA (paziente non neutropenico):PIP/TZ o CEFEPIME o ERTAPENEM(IM/MER + VANCO + AMG se sepsi grave o shock settico)
DA POLMONE:(PIP/TZ o CEFEPIME o ERTAPENEM) + (LINEZ o VANCO)(IM/MER + LINEZ o VANCO + CHINO o AMG se insufficienza respiratoria acuta osepsi grave o shock settico)
DA VIE URINARIE:PIP/TZ o CEFEPIME o ERTAPENEM o AMG(IM/MER + VANCO se recente utilizzo o fallimento di altri antipseudomos osepsi grave o shock)
ADDOME:PIP/TZ o (CEFEPIME + METRO + VANCO) o IM/MER nella sepsi e sepsi gravesenza perforazione o con perforazione localizzata, nella sepsi con peritonitediffusa e nello shock settico senza perforazione(PIP/TZ + VANCO + AMG) o (IM/MER + VANCO + AMG), considerara fluco oechinocandine, nella sepsi severa con peritonite diffusa e nello shock setticocon peritonite localizzata o diffusa
AMP:AMPICILLINA; AMP/SB:AMPICILLINA-SULBACTAM; AMG:AMINOGLUCOSIDE; PIP/TZ:PIPERACILLINA-TAZOCATAM; VANCO:VANCOMICINA; LINEZ:LINEZOLID; CHINO:CHILONICO;
AZITRO:AZITROMICINA; GENTA:GANTAMICINA; METRO:METRONIDAZOLO; IM:IMIPENE-CILASTATINA; MER:MEROPENEM; FLUCO:FLUCONAZOLO.
SIRS: > 2 DI TEMPERATURA > 38°C O < 36°C – FC > 90 BPM – FR > ATTI MINUTO – GB > 12000/MICROL. SEPSI: SIRS + INFEZIONE DOCUMENTATA/SOSPETTA. SEPSI GRAVE: SEPSI + DISFUNZIONE
D’ORGANO. SHOCK SETTICO: IPOTENSIONE INDOTTA DA SEPSI CON PAOS < 90 MMHG NON RESPONSIVA A 500 CC DI SALINA + IPOPERFUSIONE PERIFERICA.

Considerazioni Iniziali:
Patologia
• Batteriuria asintomatica in cateterizzati urinari
• CAP
• HAP & VAP
• Sepsi– S. aureus
– Enterococchi
– KPC-Kp
• Candidemia / candidosi invasive
Profilassi antibiotica in chirurgia
Profilassi antifungina nel trapianto di fegato

Sepsi da S. aureus
Deceduti (%) Vivi (%) p value
Età> 60 anni 47 (83,9) 143 (61,9) 0.002
HCA-infection 24 (42,9) 57 (24,9) 0.0075
Ricovero nei 6
mesi precedenti
37 (68,5) 119 (52,2) 0.003
Charlson index 4,50±2,13 3,31±2,15 0.0003
Rimozione CVC 7 (12,5) 75 (32,5) 0.0001
Sepsi grave 44 (78,6) 36 (15,9) 0.0001
Shock settico 38 (67,9) 6 (2,64) 0.0001
TTE 12 (21,4) 95 (41,1) 0.006
Consulenza
infettivologica
3 (5,4) 44 (19,1) 0.012
Appropriata
empirica
26 (47,3) 146 (64,9) 0.016
Appropriata mirata 41 (87,2) 212 (95,1) 0.045
56 / 289 i pazienti deceduti a 21 giorni dalla diagnosi

Stima puntuale Intervallo di confidenza al 95%
Ricovero nei 6 mesi
precedenti3,370 1,052 -10,796
Sepsi grave 3,555 1,176 – 10,743
Shock settico 46,536 9,549 – 226,780
Consulenza
infettivologica
«bedside»
0,172 0,031 – 0,951
Sepsi da S. aureus
56 / 289 i pazienti deceduti a 21 giorni dalla diagnosi

Healthcare Associated KPC-BSI:
The Time Has ComeCorcione S & De Rosa FG et al Clin Infect Dis 2014

Antimicrobial Stewardship:
Philosophy versus PracticeDodds Ashley ES et al Clin Infect Dis 2014; 59(S3): S112-121
• Impact difficult to measure
• Outcome and process measures as metrics
• Antimicrobial use & costs are indicators most used– By institutions to justify…. the effectiveness of AS programs
• Use of more meaningful outcomes constrained by:– Difficulties inherent to those measures
– Lack of funding and resoucres
– Inadequate study designs
• AS programs can be made more credible by:– Refocusing to target specific disease states
– Reassessing the usefulness of current metrics
– Integrating AS programs into institutional quality & safety efforts

Outcomes & Metrics for Antimicrobial Stewardship:
Survey of Physicians and Pharmacists Bumpass JB et al Clin Infect Dis. 2014 Oct 15;59 Suppl 3:S108-11
Survey to compare antimicrobial stewardship outcomes
Respondent opinion of important outcomes compared with those collected as metrics were – Antimicrobial use 15% vs 73%
– Antimicrobial cost 10% vs 73%
– Appropriateness of antimicrobial use 56% vs 51%
– Infection-related mortality rate 34% vs 7%
– Antibiotic-associated length of stay 22% vs 12%
Patient outcomes Important to many practitioners
But are rarely used as metrics

Antimicrobial Stewardship
Reparto
Chirurgia– Profilassi & Terapia
Medicina Interna
DEA
Terapia Intensiva
Oncoematologia
Molecole / Consumo• Vancomicina, Carbapenemi, Fluorochinoloni…
• Daptomicina, Linezolid, Pip/tazo, Tigeciclina…
• Antifungini……
Patologia
• CAP
• HCAP
• HAP / VAP
• EI / BSI
• Sepsi
• ….

Role of Pharmacokinetics & Pharmacodynamics in
Antimicrobial Susceptibility TestingLabreche JM et al, Clin Infect Dis 2015

The Examples of Vancomycin Vs. MRSA Labreche JM et al, Clin Infect Dis 2015
• Until the early 2000s
– Avoid trough levels >10 μg/mL, thought to promote toxicity
• More aggressive dosing emerged
– Mostly based on PK-PD data and the suggestion that AUC/MIC ≥ 400 improved
clinical outcomes in patients with S. aureus pneumonia
• In 2006, CLSI lowered the MRSA clinical breakpoint to ≤2 μg/mL
– Over concern for heteroresistance and worsened clinical outcomes at higher MICs
• IDSA guidelines subsequently recommended trough levels of 15–20
μg/mL for severe infections
– Considerable controversy regarding the ability of a vancomycin MIC of 1.5 to 2.0
μg/mL to predict vancomycin failure and whether or not current dosing strategies can
achieve the AUC/MIC target of ≥400 at these MICs
– A review and metanalysis … JAMA: No microbiological evidence for worse outcome

Bloodstream infection by ESBL-producing Gram-
negative bacteria: what’s the best treatment? Perez F & Bonomo RA Clin Infect Dis 2015 Jan 13
• Tremendous clinical significance of ESBL• Carbapenem treatment of choice
– The role of other agents is not well defined
• Evolving molecular biology– Genes that encode for ESBLs are usually found on large
plasmids accompanied by genetic determinants of resistance against other antibiotics, such as aminoglycosides, sulfa drugs, and fluoroquinolones
– We have also become aware that patients who develop colonization or infection with these pathogens often are previously treated with fluoroquinolones and third generation cephalosporins, usually are seriously ill, and are exposed heavily to nosocomial interventions and environment

Target de-escalation in Five Points
1. At diagnosis
2. At day 3-5 or at the earliest time available
3. With side effects
4. With microbiological data

Components of the de-Escalation Strategy Garnacho-Montero J et al Curr Opin Infect Dis 2015;28(2):193-8

Carbapenem-sparing Strategies
• Tigecycline
– Caution with monotherapy
– Combo: AG, pip-tazo, …meropenem
• New drugs
• Empiric & targeted treatment
– Ertapenem +/- AG
• De-escalation treatment
– Also including ertapenem



The best time to plant a tree
was 20 years ago……
The second best time
is now
«Chinese Proverb»

Australian AMR Objectives
• 1. Increased awareness and understanding of antimicrobial resistance, its implications and actions to combat it, through effective communication, education, and training
• 2. Implementation of effective antimicrobial stewardship practices across human health and animal care settings….
• 3. Develop nationally coordinated One Health surveillance of antimicrobial resistance and antimicrobial usage
• 4. Improve infection prevention and control measures across human health and animal care settings….
• 5. Agree a national research agenda and promote investment and…..
• 6. Strengthen international partnership and collaboration....
• 7. Establish and support clear governance arrangements