statistical report - cleveland clinic
TRANSCRIPT

Our Mission is to provide better care of the sick, investigation of their problems, and further education of those who serve.
Cancer ProgramStatistical Report
Cleveland Clinic, located in Weston, Florida, is a not-
for-profit, multi-specialty, academic medical center
that integrates clinical and hospital care with research
and education. Cleveland Clinic in Florida has
approximately 120 physicians with expertise in more
than 35 specialties. The medical campus is fully
integrated and includes diagnostic centers, outpatient
surgery, and a state-of-the-art hospital with a 24-hour
emergency department. Named one of the nation’s
100 Top Hospitals® by Solucient®, Cleveland Clinic in
Florida is an integral part of Cleveland Clinic in Ohio,
where providing outstanding patient care is based
upon the principles of quality, innovation, teamwork
and service.
About Cleveland Clinic in Florida
2950 Cleveland Clinic Blvd.Weston, Florida 33331954-659-5000
For a full list of Cleveland Clinic staff and services, visit clevelandclinicflorida.org
08/07

Mark E. Sesto, MD, FACS, Chairman, General and Oncologic Surgery
Elizabeth Stone, MD, Cancer Liaison Physician, OncologyChristopher Chen, MD, Quality Control Coordinator,
Radiation OncologyChieh-Lin Fu, MD, Quality Improvement Coordinator,
HematologyMaria Artze, MD, Radiology Viviana Behncke, MD, Clinical ResearchMariana Berho, MD, PathologyKeith Mortman, MD, FACS, Thoracic Surgery
Nicolas Muruve, MD, FACS, UrologyCarron Bramwell, Director of TelemetryVicki Cotto, Director of NursingLee Ghezzi, Director of Quality AssuranceMohammed Ibrahim, PharmacyCara Kondaki, LCSW, ACSW, Oncology Social Worker Kelly Large, CTR, Cancer Registry CoordinatorKerry Major, Medical/Surgical ServicesDiane Turnbull, Director of Laboratory ServicesSharon Wilson, Tumor Registrar
3
Cancer Committee
The Cancer Program at Cleveland Clinic in Florida is dedicated to bringing patientsthe best cancer care available. Our priority is to provide multidisciplinary,integrated and comprehensive oncology services.
To facilitate patient and family adjustment to a cancer diagnosis, its treatment, andrehabilitation, the oncology social worker is available to provide support with avariety of issues including psychological, financial or emotional concerns. Based onyour specific needs, your social worker will help identify appropriate resources.Services are also available to assist people who are under insured, have prescriptiondrug coverage concerns or patients with home health needs including but notlimited to meals, nursing and medical equipment.
Cleveland Clinic’s Cancer Program offers a variety of support groups including aBreast Cancer Book Club, Multiple Myeloma Support Group and a patient andfamily support group that allow people facing cancer and their families to shareexperiences and concerns with others facing the disease. The support groups also
offer education about cancer, treatment options, and alternative services such asyoga classes and networking opportunities. The Cancer Program is planning several additional groups including“Look Good Feel Better” affiliated with the American Cancer Society and a Leukemia & Lymphoma Society group toinclude all blood cancers.
The Oncology social worker can serve as a link between you and the health care system, and the community. Ourgoal is to provide a variety of services to aide in the long-term adjustment to a cancer diagnosis.
Cara S. Kondaki, LCSW, ACSWLicensed Clinical Social Worker-Oncology
Oncology Social Worker Report
Diagnostic Imaging Services:
Digital Mammography
MRI/Breast MRI
CT/PET Scanning
Enterostomal Therapy
Hereditary Prevention Clinic/
Genetic Testing
Home Health
Hospice
Invasive Radiology Services:
Stereotactic/Ultrasound Guided Core
Needle Breast Biosies
CT Guided Radiofrequency Ablation
Chemoembolization of Liver Tumors
Laboratory
Nutritional Services
Oncology Social Services
Outpatient Services
Pain Management
Pastoral Care
Pharmacy
Photodynamic Therapy
Rehabilitation
Special Transportation
Wound Care
Hospital Services
I’m proud to present the second Cancer Program Annual Reportreflecting 2005 data and activities at Cleveland Clinic in Florida.Our Cancer Program continues its commitment to providecomprehensive quality multidisciplinary and patient orientedcare to patients diagnosed with cancer. The Program providesclinical services adept in the prevention, early diagnosis,pretreatment evaluation, staging, optimal treatment,rehabilitation, and surveillance for recurrent disease, supportservices, and end-of-life care for our patients. Patients referred toCleveland Clinic for diagnosis, staging, and treatment of theircancers receive the advantages of inpatient areas dedicated onlyfor the care of cancer patients, an outpatient chemotherapyinfusion unit, and a Cancer Prevention Clinic that offers genetic
testing, family phenotyping, and counseling.
Comprehensive and multidisciplinary services are only one aspect of the Program. Thisreport will update you on the activity of our weekly cancer conferences, quality improvementprogram, cancer registry and database, community outreach programs, patient educationand support groups, and clinical trials.
In 2004, breast cancer was the most common cancer treated at Cleveland Clinic in Florida andits management was highlighted in last year’s report. In 2005, prostate cancer became themost common cancer treated at our institution. The change in incidence was not the result ofa change in the actual demographics of the disease but was the result of the addition of asurgeon expert in minimally invasive robotic prostate surgery. Eighty-three percent ofprostate cancer surgeries performed at Cleveland Clinic in Florida in 2005 were performedusing the robot. Also, a number of new radiation treatment options have become available forprostate cancer, which provide more accurate and efficient radiation delivery, decreasedpotential side effects, and optimized patient safety and comfort. For these reasons, we havechosen to review Cleveland Clinic’s management of prostate cancer in this Annual Report.
It is my pleasure to present this report for your review of the 2005 activities of our CancerProgram. The Cancer Committee is proud of the strides that we have made for our patientsensuring that they continue to receive the best and most personalized care possible.
Mark E. Sesto, MD, FACSCancer Committee Chairman
2
Cancer Committee Chairman’s Report

5
BREAST Adjuvant, Node (+) NSABP B-38 Docetaxel/Adria/Cytoxan (TAC) Q 3 wks x 6 vs. dose dense AC Q 2 wks x
4 ➝ Taxol vs. AC Q 2 wks x 4 ➝ Taxol/Gemcitabine Q 2 weeks x4
Other, Bone Loss CALGB 79809 Breast cancer stages I-III actively menstruating or last menstruation within 6 Prevention months: 2 schedules of Zometa/Calcium and Vitamin D (Closed to Enrollment)
GIGastric/GE Junction CALGB 80101 Resected, adjuvant chemoRT: 5-FU/LV with RT vs. E/C/5-FU with RT
GUProstate, Stage D2 CALGB 9594 Intermittent vs continuous combined androgen deprivation
Prostate, High Risk CALGB 99904 Adjuvant androgen deprivation vs Mitoxantrone plus prednisone following radical prostatectomy.
Prostate, Hormone CALGB 90401 Docetaxel and Prednisone with or without Bevacizumab. Refractory
LEUKEMIA / MDSCLL, untreated CALGB 10101 Stages I-IV b-cell, intermediate risk with active disease or high-risk:
Fludarabine/Rituxan ➝ Campath-1H
MDS CALGB 10105 Primary or secondary MDS: Oral VEGF TKI (PTK787/ZK222584)
LYMPHOMAHodgkin’s Disease, CALGB 59905 Locally extensive and advanced: ABVD vs. Stanford V +/- RTuntreated
MYELOMACleveland Clinic Biologic and Clinical Role of COX-2 Inhibitor (celecoxib) in the Management
Foundation of MGUS nad Smoldering Myeloma
OTHERPharm Sponsored Alexion EXTENSION: A Phase III, Open-Label, Extension Study of Eculizumab in
Patients with Transfusion Dependent, Hemolytic Paroxysmal NocturnalHempglobinuria (PNH) Who Have Participated in the TRIUMPH (C04-001),SHEPHERD (C04-002) or X03-001 Studies.
PNH Registry
Gemzyme Protocol CLO-341-00405, A Phase III Randomized, Double-Blind, Controlled Study Comparing Clofarabine and Cytarabine versus Cytarabine Alone in Adult Patients ≥ 60 Years Old with Acute Myelogenous Leukemia (AML) who have Relapsed or are Refractory after Receiving up to Two Prior Induction Regimens
Alexion Examination of PNH, by Level of CD59 on Red and white blood cells, in bone marrow failure syndromes (EXPLORE)
ONCOLOGY AND HEMATOLOGY CLINICAL RESEARCH PROTOCOLS2005 marked my second year as the Cancer Liaison Physician at Cleveland Clinic inFlorida. Once again, the hospital sponsored many important cancer relatedcommunity outreach programs. Cara Kondaki, LCSW, ACSW, FSOSW, joined theDepartment of Hematology and Oncology as the oncology social worker and greatlyfacilitated participation in these events as well as helped organize new cancersurvivor support groups.
Our first multiple myeloma support group was held in March. In August, ClevelandClinic hosted an early detection program for colorectal cancer screening.Questionnaires were completed by patients and based upon risks, were referred forappropriate screening studies. In October, Cleveland Clinic participated in theMaking Strides Against Breast Cancer Walk and hosted an early detection andprevention program for breast cancer, which included instruction in self-breastexamination provided by the American Cancer Society. During the Annual Cleveland
Clinic Health Fair held in November, PSA screening was carried out. To round out theyear, the Department of Dermatology held their annual skin cancer-screening program.
Most importantly, in June 2005, Cleveland Clinic’s Florida campus went smoke-free along with the entire ClevelandClinic Health System. This was a major initiative to stress the importance of a healthy lifestyle and to decrease therisks associated with an increase in cancer occurrence for the Clinic’s patients, employees and professional staff.Smoking cessation programs were offered to those interested.
Elizabeth Stone, MDCancer Liaison Physician
4
Cancer Liaison Physician Report

7
Prostate Cancer - Radiation Therapy Options
Over the past few years, there have been a number of new radiation treatmentoptions that have become available for prostate cancer. These include externalbeam radiation therapy, brachytherapy, and Samarium-153 radioisotope therapy.
Our new developments in external beam radiation therapy include the use of theVarian Trilogy image-guided radiation therapy system. This machine allows fortreatment to be delivered with real-time image guidance for the most accurateradiation delivery. This technology allows us to maximize dose to the target ofinterest and minimize the critical normal structures. It also allows for us to performimage-guided stereotactic CNS and body radiosurgery on previously radiated sites.The versatile Trilogy system combines imaging and treatment technologies, and canbe used to deliver the widest range of external beam radiotherapies: 3D conformalradiotherapy, IMRT, stereotactic radiosurgery, fractionated stereotactic radiationtherapy and intensity-modulated radiosurgery for cancer and neurosurgical
treatments.
Advanced imaging capabilities built into the system allow therapists to position patients for treatment withsubmillimeter accuracy. A respiratory gating system compensates for any tumor movement that occurs as a patientbreathes.
The Trilogy system can deliver radiotherapy doses at least 60 percent faster than conventional accelerators. Thisshortens the length of time patients need to spend undergoing treatment. In addition, the radiation beam is highlyprecise, allowing clinicians to deliver treatments with unprecedented accuracy.Another new treatment approach includes prostate brachytherapy, including Pd-103 seeds, I-125 seeds, and the Ir-192 high dose rate (HDR) seed.
There are several key advantages to prostate seed and HDR brachytherapy :
• It is a convenient outpatient procedure. The patient generally can resume normal daily activities quickly. • Radioactive seeds are inserted directly into the prostate, minimizing radiation exposure to surrounding tissues
while permitting an escalation of the dose concentrated in the area of the prostate cancer. HDR brachytherapyhas the additional advantage of even more accurate delivery of radiation, without any post-treatmentradioactivity.
• It can be done alone or in conjunction with 3D conformal radiation therapy or IMRT (intensity modulatedradiation therapy).
• 10-year results show that the vast majority of patients remain disease-free, making it an attractive alternative toboth radical surgery and full-course external beam radiotherapy.
• Incontinence of urine occurs in only a tiny subset of patients, and impotence rates are less than with the othercurative therapies.
Chris Chen, MDRadiation Oncologist
Cancer Registry Report 2005
The Cancer Registry plays an integral role in the success of our Cancer Program,providing data management services to meet mandatory state cancer reportingrequirements as well as data needs for clinicians and administrators. Data collectedincludes demographic information, stage of disease, type of treatment and survivalinformation. The Cancer Registry maintains data on all cancer patients seen sinceJanuary 1, 2004 and the data is made available to the medical staff for special studies,audits and research.
In 2005, a total of 697 tumors were reported to the Florida Central Cancer Registry,the Florida Cancer Data System (FCDS). Of these, 468 were analytic cases and 229were non-analytic. Included in the top five analytic sites are prostate, breast, colon &rectum, bronchus & lung, and kidney. These represent sixty-six percent of our totalanalytic caseload. The following figure compares Cleveland Clinic’s percentage ofcases to the rest of Florida, as well as the United States.
The multidisciplinary Cancer Committee provides the leadership for our Cancer Program and assures optimalpatient care by ensuring compliance with the American College of Surgeons Cancer Program Standards, and byinitiating plans for improvement and change. The Committee is composed of multidisciplinary staff physicians aswell as allied health professionals involved in cancer patient care. The physicians assist the Cancer Registry withquality control by chart review and are also the key members of weekly Cancer Conferences.
Various types of malignancies are selected for presentation at Cancer Conference on the basis of complexity, unusualmanifestation of the disease or special interest. The Conference format includes a complete presentation of medicalhistory, physical findings, clinical course, radiographic studies and pathologic interpretation. Cancer Conferencesare approved for one hour of Category 1 Continuing Medical Education credit.
During 2005, thirty-one Cancer Conferences were held in a facility-wide format. A total of fifty-seven cases werepresented, with fifty-five, or 96%, of those presented prospectively. The number of cases presented represents 12% ofthe 2005 analytic caseload.
Kelly Large, CTRCancer Program Coordinator
6
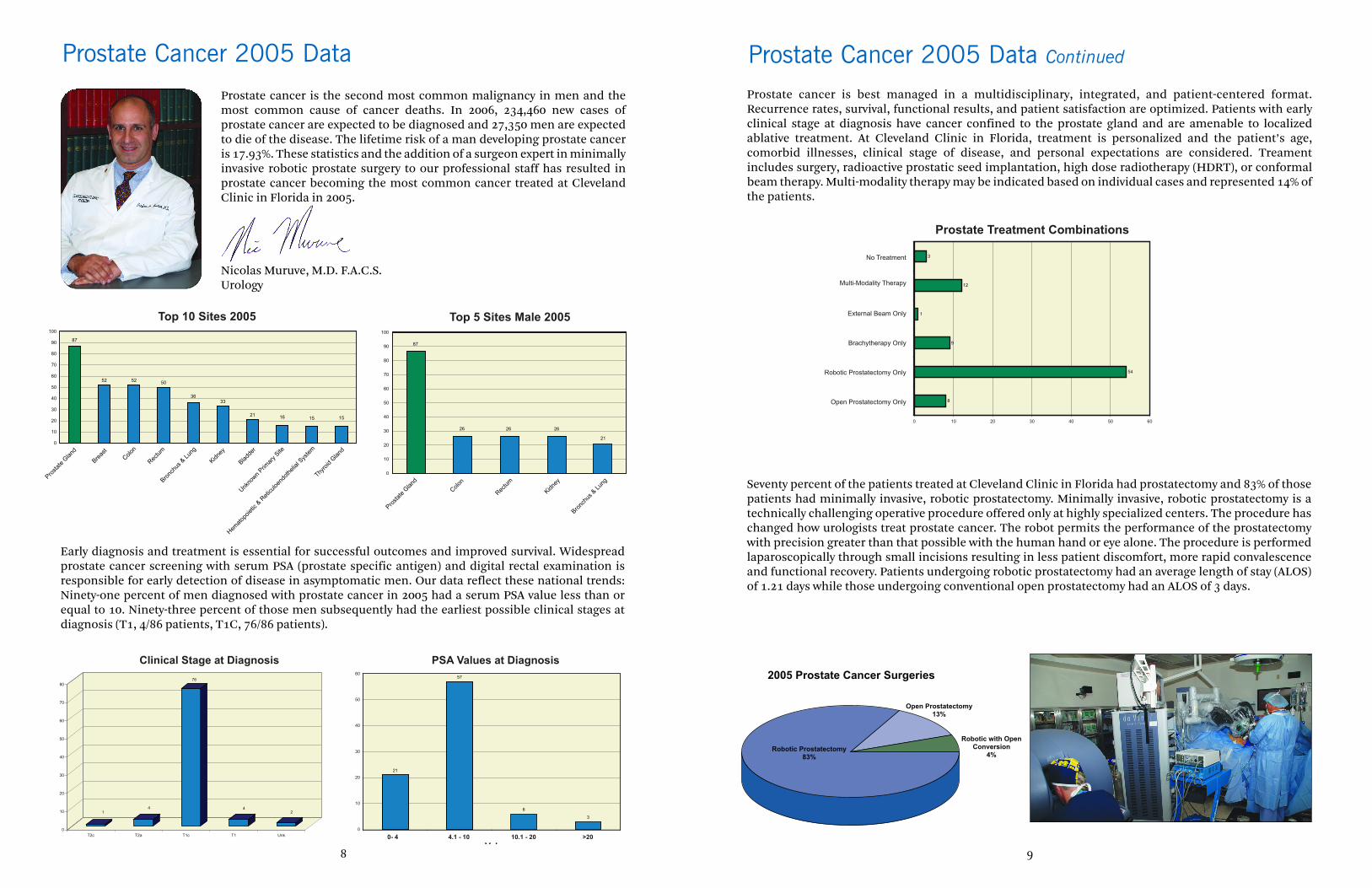
Seventy percent of the patients treated at Cleveland Clinic in Florida had prostatectomy and 83% of thosepatients had minimally invasive, robotic prostatectomy. Minimally invasive, robotic prostatectomy is atechnically challenging operative procedure offered only at highly specialized centers. The procedure haschanged how urologists treat prostate cancer. The robot permits the performance of the prostatectomywith precision greater than that possible with the human hand or eye alone. The procedure is performedlaparoscopically through small incisions resulting in less patient discomfort, more rapid convalescenceand functional recovery. Patients undergoing robotic prostatectomy had an average length of stay (ALOS)of 1.21 days while those undergoing conventional open prostatectomy had an ALOS of 3 days.
Prostate cancer is best managed in a multidisciplinary, integrated, and patient-centered format.Recurrence rates, survival, functional results, and patient satisfaction are optimized. Patients with earlyclinical stage at diagnosis have cancer confined to the prostate gland and are amenable to localizedablative treatment. At Cleveland Clinic in Florida, treatment is personalized and the patient’s age,comorbid illnesses, clinical stage of disease, and personal expectations are considered. Treamentincludes surgery, radioactive prostatic seed implantation, high dose radiotherapy (HDRT), or conformalbeam therapy. Multi-modality therapy may be indicated based on individual cases and represented 14% ofthe patients.
9
2005 Prostate Cancer Surgeries
Robotic Prostatectomy83%
Open Prostatectomy13%
Robotic with OpenConversion
4%
Prostate Treatment Combinations
Prostate cancer is the second most common malignancy in men and themost common cause of cancer deaths. In 2006, 234,460 new cases ofprostate cancer are expected to be diagnosed and 27,350 men are expectedto die of the disease. The lifetime risk of a man developing prostate canceris 17.93%. These statistics and the addition of a surgeon expert in minimallyinvasive robotic prostate surgery to our professional staff has resulted inprostate cancer becoming the most common cancer treated at ClevelandClinic in Florida in 2005.
Nicolas Muruve, M.D. F.A.C.S.Urology
8
Top 10 Sites 2005 Top 5 Sites Male 2005
Prostate Cancer 2005 Data
Clinical Stage at Diagnosis PSA Values at Diagnosis
V l
Early diagnosis and treatment is essential for successful outcomes and improved survival. Widespreadprostate cancer screening with serum PSA (prostate specific antigen) and digital rectal examination isresponsible for early detection of disease in asymptomatic men. Our data reflect these national trends:Ninety-one percent of men diagnosed with prostate cancer in 2005 had a serum PSA value less than orequal to 10. Ninety-three percent of those men subsequently had the earliest possible clinical stages atdiagnosis (T1, 4/86 patients, T1C, 76/86 patients).
Prostate Cancer 2005 Data Continued
2
12
1
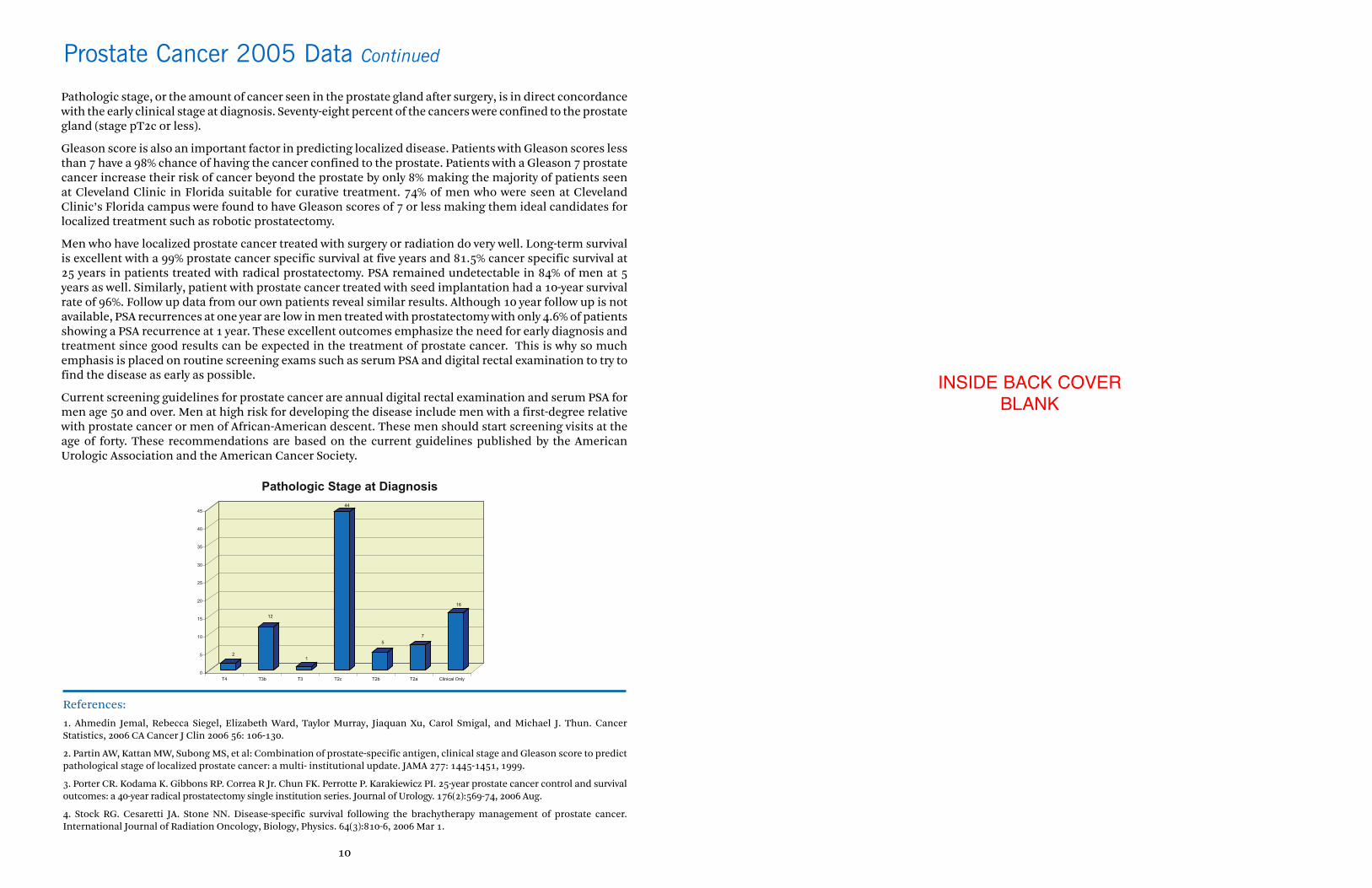
44
5
7
16
0
5
10
15
20
25
30
35
40
45
T4 T3b T3 T2c T2b T2a Clinical Only
Pathologic Stage at Diagnosis
Pathologic stage, or the amount of cancer seen in the prostate gland after surgery, is in direct concordancewith the early clinical stage at diagnosis. Seventy-eight percent of the cancers were confined to the prostategland (stage pT2c or less).
Gleason score is also an important factor in predicting localized disease. Patients with Gleason scores lessthan 7 have a 98% chance of having the cancer confined to the prostate. Patients with a Gleason 7 prostatecancer increase their risk of cancer beyond the prostate by only 8% making the majority of patients seenat Cleveland Clinic in Florida suitable for curative treatment. 74% of men who were seen at ClevelandClinic’s Florida campus were found to have Gleason scores of 7 or less making them ideal candidates forlocalized treatment such as robotic prostatectomy.
Men who have localized prostate cancer treated with surgery or radiation do very well. Long-term survivalis excellent with a 99% prostate cancer specific survival at five years and 81.5% cancer specific survival at25 years in patients treated with radical prostatectomy. PSA remained undetectable in 84% of men at 5years as well. Similarly, patient with prostate cancer treated with seed implantation had a 10-year survivalrate of 96%. Follow up data from our own patients reveal similar results. Although 10 year follow up is notavailable, PSA recurrences at one year are low in men treated with prostatectomy with only 4.6% of patientsshowing a PSA recurrence at 1 year. These excellent outcomes emphasize the need for early diagnosis andtreatment since good results can be expected in the treatment of prostate cancer. This is why so muchemphasis is placed on routine screening exams such as serum PSA and digital rectal examination to try tofind the disease as early as possible.
Current screening guidelines for prostate cancer are annual digital rectal examination and serum PSA formen age 50 and over. Men at high risk for developing the disease include men with a first-degree relativewith prostate cancer or men of African-American descent. These men should start screening visits at theage of forty. These recommendations are based on the current guidelines published by the AmericanUrologic Association and the American Cancer Society.
10
INSIDE BACK COVERBLANK
Prostate Cancer 2005 Data Continued
References:
1. Ahmedin Jemal, Rebecca Siegel, Elizabeth Ward, Taylor Murray, Jiaquan Xu, Carol Smigal, and Michael J. Thun. CancerStatistics, 2006 CA Cancer J Clin 2006 56: 106-130.
2. Partin AW, Kattan MW, Subong MS, et al: Combination of prostate-specific antigen, clinical stage and Gleason score to predictpathological stage of localized prostate cancer: a multi- institutional update. JAMA 277: 1445-1451, 1999.
3. Porter CR. Kodama K. Gibbons RP. Correa R Jr. Chun FK. Perrotte P. Karakiewicz PI. 25-year prostate cancer control and survivaloutcomes: a 40-year radical prostatectomy single institution series. Journal of Urology. 176(2):569-74, 2006 Aug.
4. Stock RG. Cesaretti JA. Stone NN. Disease-specific survival following the brachytherapy management of prostate cancer.International Journal of Radiation Oncology, Biology, Physics. 64(3):810-6, 2006 Mar 1.