statement of acute pancreatitis: hospital physician ... pancreatitis: review of contemporary...
TRANSCRIPT
Hospital Physician Board review Manual www.turner-white.com
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2risk of recurrence . . . . . . . . . . . . . . . . . . . . . . . .6Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . .6Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Prognostic Factors/Predictors . . . . . . . . . . . . . . .9Management . . . . . . . . . . . . . . . . . . . . . . . . . . . .11Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14Board review Questions . . . . . . . . . . . . . . . . . . .15references . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
table of Contents
GastroenteroloGy BoarD revIew Manual
acute Pancreatitis: review of Contemporary Diagnosis and Management
Contributors:Douglas G. adler, MD, FaCG, aGaF, FasGeAssociate Professor of Medicine, University of Utah School of Medicine, Salt Lake City, UT
ryan C. van woerkom, MDOregon Health and Science University, Department of Internal Medicine, Portland, OR
Statement of editorial PurPoSe
The Hospital Physician Gastroenterology Board Review Manual is a study guide for fellows and practicing physicians preparing for board examinations in gastroenterology. Each manual reviews a topic essential to the current practice of oncology.
PuBliSHinG Staff
PRESIDENT, GRouP PuBLISHERBruce M. White
SENIoR EDIToRRobert Litchkofski
ExEcuTIvE vIcE PRESIDENTBarbara T. White
ExEcuTIvE DIREcToR of oPERaTIoNS
Jean M. Gaul
NoTE fRoM THE PuBLISHER:This publication has been developed without involvement of or review by the American Board of Internal Medicine.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 1
GastroenteroloGy BoarD revIew Manual
acute Pancreatitis: review of Contemporary Diagnosis and Management
Douglas G. Adler, MD, FACG, AGAF, FASGE, and Ryan C. Van Woerkom, MD
introduCtion
Acute pancreatitis describes an acute inflamma-tory process of the pancreas that rapidly depletes intravascular water and, if unchecked, promotes regional inflammation. The severity spectrum of acute pancreatitis ranges from mild interstitial pancreatitis to a more severe form that includes pancreatic necrosis, which is frequently associated with concomitant multi-organ failure. Mild interstitial pancreatitis has the highest prevalence, and acute pancreatitis is typically rapid in onset. In 2005 and 2007, an estimated 230,000 patients were treated for acute pancreatitis in hospitals in the United States.1,2 Recent studies have demonstrated an increase in the incidence of acute pancreatitis, and some have projected the incidence to be sub-stantially higher than previously reported rates, al-though case-fatalities have remained stable since 1970.3 The increased frequency of acute pancre-atitis may be due to the rising incidence of obesity, a risk factor for the development of gallstones and, by extension, gallstone pancreatitis,4 although an increase in surveillance bias cannot be excluded.
Acute pancreatitis confers a heavy financial burden. A recent study estimated that the aver-age cost per hospitalization for acute pancreatitis is $9870.5 It is responsible for $2.2 billion in U.S. health care expenditures annually. The average length of hospital stay for a patient with acute pan-creatitis is approximately 5 to 6 days; children had shorter hospital stays and adults aged 45 to 64 years had hospital stays that were 1 day longer, on average.3,6,7 Acute pancreatitis may be ac-companied by life-threatening complications as well as significant morbidity and mortality. This article reviews the diagnosis and man-agement of patients with acute pancreatitis.
ClaSSifiCation
A revision of the Atlanta classification schema for acute pancreatitis was recently published.6 The revised classification delineates 2 phases of acute pancreatitis: early and late. Severity of pancreatitis can be classified as mild, moderate, or severe. Mild acute pancreatitis is not associated with organ failure or local or systemic complications
copyright 2013, Turner White communications, Inc., Strafford avenue, Suite 220, Wayne, Pa 19087-3391, www.turner-white.com. all rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White communications. The preparation and distribution of this publication are sup-ported by sponsorship subject to written agreements that stipulate and ensure the editorial independence of Turner White communications. Turner White communications retains full control over the design and production of all published materials, including selection of topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White communications. Turner White communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
2 Hospital Physician Board review Manual www.turner-white.com
and clinically resolves in 7 days in most patients. Moderately severe acute pancreatitis is defined by the development of transient organ failure as well as complications or exacerbations of comorbid dis-ease. Severe acute pancreatitis is associated with organ failure that persists for more than 48 hours. Local complications of acute pancreatitis include peripancreatic fluid collections, sterile or infected pancreatic and peripancreatic necrosis, pseudo-cyst formation, or the development of sterile or infected walled-off pancreatic necrosis.8
etioloGy
Gallstones or Biliary Pancreatitis
Biliary pancreatitis, synonymous with gallstone pancreatitis, is a form of acute pancreatitis caused by the passage of gallstones through the cystic duct and into the distal common bile duct where they can obstruct the flow of digestive enzymes from the biliary and pancreatic ducts into the duo-denum. Pancreatic ductal obstruction is felt to be the inciting event in gallstone pancreatitis.8 One study that evaluated data on consecutive patients admitted with acute pancreatitis to a community hospital reported an incidence rate of 45 cases per 100,000 person-years for gallstone acute pancre-atitis.9 Incidence is highest in patients with small gallstones or microlithiasis, as these stones are more likely to escape the gallbladder and transit the cystic duct to reach the common bile duct.10 A recent study noted that the incidence of all causes of acute pancreatitis rose between 1994 and 2001 from 33.2 cases to 43.8 cases per 100,000 adults, without a reduction of mortality rate. The increase in acute pancreatitis was felt to be mainly due to the rise in the incidence of biliary pancreatitis.7 Large stones are more likely to be retained in the gallbladder.
Some data suggests that patients with confirmed gallstone pancreatitis should undergo cholecystec-tomy during their initial hospitalization (once the acute event has resolved) rather than at a later date, although in practice this can be hard to coordinate in all patients.11 Patients with gallstones and bile duct stones (choledocholithiasis) should undergo cholecystectomy and endoscopic retrograde chol-angiopancreatography (ERCP), although the tim-ing of these procedures should be individualized. Some institutions combine cholecystectomy and ERCP into a single procedure, although this can be difficult to do as it requires significant coordination between the gastroenterology and surgical teams.
Caucasians, Hispanics, and American Indians are more likely than African Americans to develop biliary acute pancreatitis.7,9,12 One study demon-strated that gallstone pancreatitis typically present-ed at a younger age in Hispanics; this population had a more benign clinical course with infrequent intensive care unit (ICU) admissions.13 Obesity is a risk factor for the development of gallstone pan-creatitis and may increase the risk for the develop-ment of severe pancreatitis, including pancreatic necrosis.14 Obesity also increases the risk of de-veloping local complications, such as pancreatic fluid collections.12 However, obesity is not associ-ated with increased mortality in acute pancreatitis. Pregnancy is also a risk factor for the development of gallstone pancreatitis, with an incidence ranging from 1 case per 1000 to 3333 pregnancies.15–17 El-evated alanine aminotransferase (ALT), advancing age, weight gain, female sex, and rapid weight loss are all risk factors associated with the development of biliary acute pancreatitis.7,18 Unsaturated fats, coffee, and moderate alcohol consumption appear to reduce the risk of developing gallstones and, thus, biliary acute pancreatitis.19–21 Elevated ALT, in a patient with suspected acute pancreatitis, may

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 3
lead to the diagnosis of a biliary etiology; varying thresholds have been utilized and sensitivity in distinguishing between alcohol-related and non–alcohol-related acute pancreatitis ranges between 72% and 84%. Microlithiasis can be a potential cause of acute pancreatitis as well.
alcoholic Pancreatitis
Alcohol is a common precipitant of acute pancre-atitis, although the incidence of acute pancreatitis in heavy alcohol consumers is not more than 2% to 3% per year.22 This suggests that there are as yet undetermined environmental or genetic factors that influence the development of acute pancreati-tis in this population. Yadav and Whitcomb found that alcoholic acute pancreatitis usually occurred after more than 5 years of heavy drinking; the role of tobacco use in relation to alcoholic acute pancreatitis is still being investigated, although it is thought to propagate an accelerated course in established acute pancreatitis.23 Currently, 17.6 mil-lion Americans have a form of an alcohol use dis-order, and some data suggest that the incidence of alcoholic acute pancreatitis is on the rise.6,24 Of note, the alcoholic acute pancreatitis incidence rate may be similar in heavy drinkers of both sexes (91.5 cases per 100,000 persons in men versus 81.9 in women). Alcoholic acute pancreatitis inci-dence rates peak between the ages of 35 and 44 years.10 Furthermore, alcoholic acute pancreatitis has the highest associated risk of overall mortal-ity, a 90% increased odds compared to biliary pancreatitis,10 possibly due to poor baseline nutri-tion. Tobacco use has been recently implicated in the development of nonbiliary acute pancreatitis.25 Its strength as an independent risk factor in acute pancreatitis appears synergistic with concomitant alcohol use.23 Interventions to reduce alcohol use in patients with acute pancreatitis are critical to
help to reduce the development of chronic pancre-atitis. Alcohol elimination in patients with chronic pancreatitis can be very difficult and may require multimodality therapy.26
idioPathic acute Pancreatitis
Between 10% and 30% of cases of acute pancre-atitis may be idiopathic in nature.27 African Ameri-cans have the highest age- and sex-standardized incidence rate of idiopathic pancreatitis.10 A sub-stantial proportion of acute pancreatitis of unclear cause may be explained by such etiologies as un-detected microlithiasis, unrecognized drug-induced pancreatitis,28 or the controversial sphincter of Oddi dysfunction, among other possibilities.29
inherited Forms
Hereditary pancreatitis, first reported in 1952, is a rare disease characterized by mutations in the pancreatic secretory cationic trypsinogen inhibi-tor (PTSI or PRSS1) gene, R122H or N29I, or the serine protease inhibitor, Kazal type 1 (SPINK1) gene, resulting most often in an autosomal domi-nant phenotype.30,31 It should be considered in patients with recurrent pancreatitis who also have a family history of pancreatitis. This recurrent form of acute, relapsing pancreatitis often manifests first in childhood (although it may not manifest until age 30), with a cumulative incidence of pancreatic cancer of 40% by the age of 70 years.32 Hereditary pancreatitis almost always develops into chronic pancreatitis and is associated with an increased incidence of pancreatic cancer. Other rare genetic sequences are risk factors for severity of acute pancreatitis such as the MCP-1-2518 G allele; the individual PRSS1 mutation does not appear to contribute to severity risk.33,34
Mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) allele have been

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
4 Hospital Physician Board review Manual www.turner-white.com
associated with the development of pancreatitis. Mutations in CFTR can be present in as many as 10% of patients with acute pancreatitis, although it is often difficult to exclusively attribute the de-velopment of pancreatitis to CFTR mutations.35 Abnormally functioning CFTR genes may cause inspissation of pancreatic secretions, leading to pancreatic ductal obstruction and pancreatitis.36 CFTR gene mutations are often associated with recurrent acute pancreatitis and/or chronic pancre-atitis. A single episode of acute pancreatitis should not prompt genetic testing for CFTR mutations.37 Recurrent idiopathic pancreatitis that results from CFTR mutations may be more aptly classified as, and often develops into, chronic pancreatitis in this population.
druG-induced Pancreatitis
Drug-induced pancreatitis may account for as much as 7% of all cases of acute pancreatitis,38 and may represent the third most common cause of acute pancreatitis. Medications implicated (al-beit with varying levels of evidence) in the devel-opment of drug-induced pancreatitis are listed in the table.39 Women, children, the elderly, and persons with underlying Crohn’s disease, hema-tologic malignancies, and multiple cancer chemo-
therapy agents appear to comprise populations with an increased risk of drug-associated acute pancreatitis.40 Many drugs have been implicated as causes of acute pancreatitis, and a careful evaluation of the patient’s medications is war-ranted in all patients with acute pancreatitis of unclear etiology. Drug-induced acute pancreatitis may occur any time during the course of the im-plicated pharmaceutical agent. Classification sys-tems have been developed which may assist the clinician in determining the level of evidence that implicates a given drug because of the potential for both over and under diagnosing.41,42 As rules of thumb, the development of acute pancreatitis must occur during treatment with the drug, all other causes of acute pancreatitis must be exclud-ed, and the acute pancreatitis should be seen to resolve with discontinuation of the offending drug. Additionally, acute pancreatitis recurs when the drug is readministered, although medico-ethical concerns often prevent clinical testing of this—the drug may be reintroduced when it is crucial for the patient’s health, the character of the disease is concerning, and/or when the etiology is not clearly defined.43 A commonly encountered difficulty in patients with suspected drug-induced pancreatitis is that the link between the drug and pancreatitis
table. Medications Implicated in the Development of Drug-Induced Pancreatitis
class drug(s)
Antimicrobials Tetracycline, sulfonamide, pentamidine, didanosine, metronidazole
Anticonvulsant Valproic acid
Diuretic Furosemide, thiazides
Immunosuppressant Azathioprine, 6-mercaptopurine
Nonsteroidal antiinflammatory Sulindac, salicylate, indomethacin
Antiproliferative Tamoxifen, L-asparaginase
Other Estrogen, bethanechol, oral contraceptives, angiotensin-converting enzyme inhibitors, selec-tive serotonin reuptake inhibitors, angiotensin II receptor blockers, statins

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 5
may be weak, and the patient may have a strong indication to be on the drug (ie, a patient with coro-nary artery disease who takes a statin or a patient with gastroesophageal reflux disease who takes omeprazole).44 It can often be problematic to iden-tify a causative agent in patients on multiple agents with a predisposition to causing drug-induced pancreatitis.
iatroGenic Pancreatitis
Iatrogenic pancreatitis most commonly occurs following ERCP procedures.45 One review that evaluated complication rates reported in pro-spective studies of ERCP computed a 3.47% incidence rate of iatrogenic acute pancreatitis, although the rate is dependent on the type of procedure performed and individual patient risk factors.46 Studies evaluating a variety of medica-tions to reduce the risk of post-ERCP pancreatitis have been largely unrevealing, and no currently available agent has been shown to clearly reduce the incidence of post-ERCP pancreatitis (PEP). Recent data have demonstrated that prophylactic stent placement in the pancreatic duct of high-risk patients reduces the risk of developing PEP and reduces the severity of PEP in patients who de-velop it.47,48 This is further supported by a contem-porary meta-analysis that found that regardless of the severity of PEP, prophylactic stents were beneficial.49 Furthermore, careful patient selection and minimally traumatic endoscopic techniques appear to offer additional protection against the development of post-ERCP pancreatitis.44,50 Pan-creatitis may also occur following abdominal surgery, cardiac surgery (ischemia related with bypass surgery), liver biopsy, and abdominal pro-cedures performed by interventional radiologists and can be caused by retained intra-abdominal foreign bodies as well as iatrogenic hypercalce-
mia due to total parental nutrition, among other causes.51–55
inFectious causes
Infectious causes of acute pancreatitis are rare and have mostly been described in case reports. The most common parasitic infections linked to the development of acute pancreatitis are Toxo-plasma, Cryptosporidium, and Ascaris.56 Viruses known to cause acute pancreatitis include mumps, Coxsackie, hepatitis B, Cytomegalovirus, and the varicella zoster virus.56 Only a few bacteria are well established as causes of acute pancreatitis: Mycoplasma, Legionella, Leptospira, and Sal-monella.56 Aspergillus is the only fungus that has been strongly associated with causing acute pancreatitis.56
hyPertriGlyceridemia and hyPercalcemia
Elevated triglyceride levels, typically exceeding 500 mg/dL, can be seen in various conditions, in-cluding poorly controlled type 2 diabetes, obesity, alcoholism, third trimester pregnancy, renal dis-ease, hypothyroidism, and familial hypertriglyceri-demia.57,58 Patients should have fasting triglyceride levels checked after their pancreatitis has resolved before diagnosing hypertriglyceridemia, as serum triglycerides can be artificially elevated during an episode of acute pancreatitis.
Hypercalcemia is also a recognized etiology of acute pancreatitis.59 Hypercalcemia can be associ-ated with a malignancy (often in the setting of bony metastases or multiple myeloma), total parenteral nutrition (as mentioned above), sarcoidosis, vita-min D toxicity, and infusions of perioperative high-dose calcium during cardiopulmonary bypass.60 If muscular/myopathic, urologic, or nervous system symptoms coexist with acute pancreatitis, patients should be evaluated for hyperparathyroidism.61

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
6 Hospital Physician Board review Manual www.turner-white.com
other causes
Less commonly encountered causes of acute pancreatitis include autoimmune pancreatitis, most often seen in Asian populations, trauma-induced pancreatitis (often following motor vehicle acci-dents), and scorpion stings.62 Autoimmune pan-creatitis should be suspected in patients with inflammatory bowel disease.63 Pediatric acute pan-creatitis can also be seen and can be associated with multisystem disease and systemic infection.64 Rarely, tumors such as ampullary cancer or intra-ductal papillary mucinous neoplasm of the pan-creas can cause acute pancreatitis. Congenital malformations, including pancreas divisum, an-nular pancreas, and anomalous pancreaticobiliary union, among others, have also been implicated.
riSk of reCurrenCe
If underlying causes are not identified and treated, the risk of recurrent acute pancreatitis can be as high as 40% within 6 years. Gallstone pancreatitis carries a significantly lower risk of recurrence of approxi-mately 10%65 because recognition of gallstones as a cause is usually followed by a procedure to clear the bile duct and subsequent cholecystectomy. There-fore, a watch-and-wait approach cannot be advocat-ed in these patients given the high risk of recurrence. A recent well-constructed meta-analysis showed a decrease in mortality following cholecystectomy in patients undergoing biliary sphincterotomy and duct clearance, further bolstering this argument.66 Most studies report a negative correlation between mor-tality and recurrent acute pancreatitis.4
PatHoPHySioloGy
In pancreatic acinar cells, a primary injury pro-motes compartmentalization of lysozomal enzymes
(eg, cathepsin B and exocrine pancreatic en-zymes);67 catalytic proteins are then activated with subsequent enzymatic “spilling,” which leads to the typical inflammatory cascade seen in acute pancreatitis.68 Trypsin activates other proteases like elastase and chymotrypsin, components of the complement and coagulation cascades, and kinins.69 The enzymes diffuse into the interstitial and endothelial spaces and begin autodigestion of the gland. Acute pancreatitis can be thought of as a breakdown of regulatory pathways which can be predominantly attributed to overproduction or inappropriate activation of pancreatic zymogens or defective inactivation by the serine protease inhibi-tors.70 Tissue breakdown products potentiate vas-cular injury, with local recruitment of cytokine and arachidonic acid metabolite–secreting leukocytes, with TNFα acting as a central mediator.68 These agents produce edema and reactive oxidation spe-cies which are thought to be mediators of systemic organic dysfunction; interestingly, patients with diminished glutathione S transferase activity due to polymorphisms have a higher incidence of de-veloping severe acute pancreatitis.71 The increase in vascular permeability promotes thrombosis and hemorrhage and can lead to pancreatic ischemia and necrosis.67 Increased vascular permeability can lead to bacterial translocation into the pancre-atic bed and result in infected pancreatic necrosis, a life-threatening complication of acute pancre-atitis. In severe cases, systemic inflammatory response syndrome (SIRS), renal failure, shock, myocardial stress, fever, or acute respiratory dis-tress syndrome may develop.
Most of the final inflammatory pathways are identical regardless of etiology, although alco-holic acute pancreatitis may slightly vary. Alcohol potently stimulates the release of secretin and cholecystokinin, which are the major contributors

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 7
to pancreatic secretion.72 Also, the rising ethanol concentration in acinar cells causes an increase in cytosolic calcium, which is required for vesicular zymogen activation. This relationship between cy-tosolic calcium and zymogen activation may also help to explain the association between hypercal-cemia and acute pancreatitis.71
diaGnoSiS
The classic presentation of acute pancreatitis includes mild to severe epigastric abdominal pain (often radiating to the back) as well as nausea and vomiting. The pain is typically constant in nature and is not aggravated by coughing, movement, or respiration. The pain tends to be more severe in a supine position and may lessen if the patient leans forward in a sitting position. On presentation, jaun-dice or tachycardia may be present, and patients may appear pale and distressed, be febrile, and have a distended abdomen.73 Turner’s sign (flank bruising) or Cullen’s sign (bruising surrounding the umbilicus) may be present in severe cases. Some patients may have a more florid presenta-tion that includes hypotension or shock due to intravascular volume depletion and third spacing of fluids.
Commonly accepted criteria for a clinical diagno-sis of acute pancreatitis necessitate the presence of 2 of the 3 following features: serum amylase and lipase elevated at least 3 times above the upper limit of normal; characteristic eipigastric abdominal pain as described above; and typical radiologic features as found on computed tomography (CT), magnetic resonance imaging (MRI), or transab-dominal ultrasound (US). Other clinical findings that can be present in acute pancreatitis include dehy-dration, which may manifest with elevated blood urea nitrogen and hematocrit and decreased urine
output. Findings that may be seen in more severe presentations include hypotension despite volume replacement and a corresponding rise in hematocrit secondary to hemoconcentration, metabolic acido-sis, acute respiratory distress syndrome/respiratory failure, renal failure, and fluctuation in serum calcium levels.74,75
Classification systems are currently being re-vised, including a 4-tier system with a moderate severe acute pancreatitis category defined as pan-creatitis with complications but without multi-organ system dysfunction.76
Biochemical diaGnostic Parameters
Elevation of serum amylase and lipase to at least greater than 3 times the upper limit of normal in conjunction with the appropriate clinical history are mainstays in the diagnosis of acute pancreatitis. Prospective studies comparing the selective evalu-ation of lipase versus amylase demonstrate a slight diagnostic advantage to lipase because amylase may have a lower sensitivity (ie, it may be normal in patients with acute pancreatitis).77–79 In general, amylase and lipase levels do not correlate with either the severity of the attack or with overall prog-nosis. In addition, serum amylase and lipase levels neither assist in generating an overall prognosis nor in predicting complications of acute pancre-atitis.80–82 Most practicing physicians do not follow serum amylase and lipase levels beyond the first few days once the diagnosis has been established. A fall in enzymes, however, accompanied by clini-cal improvement often adequately demonstrates a resolving acute pancreatitis in most patients. Persistent elevation of serum amylase and lipase may suggest pancreatic ductal disruption and/or necrosis. Finally, amylase and lipase assays do not need to be ordered simultaneously as this may incur higher health care costs.83

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
8 Hospital Physician Board review Manual www.turner-white.com
Serum alkaline phosphatase and bilirubin levels are not useful in isolation in the diagnosis of acute biliary pancreatitis, although a 3-fold elevation of ALT has a positive predictive value of 96%, and aspartate transaminase is nearly as useful as ALT according to one meta-analysis.84 If liver function enzymes and amylase and lipase levels are el-evated, an etiology of biliary pancreatitis is more likely, although pancreatic edema causing extrin-sic compression of the distal common bile duct can produce similar laboratory findings. Currently, serum hematocrit and C-reactive protein (48 hr after onset) have assumed greater predictive roles in determination of vascular and gastrointestinal complications (see below).85,86
imaGinG
When clinicians suspect that acute pancreatitis may be atypical in presentation, imaging may be particularly helpful. Abdominal radiographs are of some value in patients with pancreatitis. The pres-ence of calcifications may suggest chronic pancre-atitis as an underlying diagnosis. Signs that may be seen on radiograph in acute pancreatitis include a
“sentinel loop,” or a dilated segment of small intestine or colon displaying ileus, and “colon cut-off sign,” a functional spasm in the descending colon resulting in a termination of air in the distal colon near the splenic flexure. Plain radiographs may not be as sensitive as other imaging modalities and not quanti-tate the amount of pancreatic necrosis or completely describe complications like pancreatic pseudocyst.
A hyperechoic, diffusely enlarged pancreas is often seen on transabdominal ultrasound in acute pancreatitis. Ultrasonography is also a useful and economic choice for evaluating patients with suspected gallstone pancreatitis. This study can visualize gallstones in the gallbladder, evidence of acute cholecystitis (gallbladder wall thickening or pericholecystic fluid), and common bile duct dila-tion (often suggestive of an obstructing common bile duct stone) and in some cases can directly visualize choledocholithiasis. Bowel gas and the pancreas’ retroperitoneal location may obscure the organ on ultrasound imaging.87 Ultrasonography does not assist in diagnosing the extent of pancre-atic necrosis or inflammation.
CT scans with intravenous contrast should be strongly considered in patients with suspected pancreatic necrosis because CTs may assist in triaging the patient within the hospital. The entire pancreas, including necrotic changes, can be well visualized, and complications of pancreatitis such as fluid collections and/or pseudocysts can be rapidly identified (Figure 1). CT findings such as peripancreatic stranding and an enlargement of part or all of the pancreas may suggest acute pan-creatitis. Contrast-enhanced CT demonstrated an excellent correlation between imaging results and the development of early and late necrosis.88 The degree of necrosis is also an excellent prognostic factor. Small areas of necrosis can still be missed via contrast CT imaging.89
Figure 1. Computed tomography image showing mild acute pan-creatitis. Note swelling of pancreatic tail and peripancreatic fat stranding (arrow).
A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 9
Abdominal MRI is typically utilized when CTs are contraindicated or to search for common bile duct stones via magnetic resonance cholangio-pancreatography (MRCP). Studies performed with MRI use gadolinium for contrast, which carries a lower risk of side effects or renal injury than contrast used with CT scans. MRI is also highly effective at identifying fluid collections and pan-creatic necrosis.87 MRI has a greater sensitivity for detecting mild acute pancreatitis as compared with CT scan.88 MRI may be preferred over CT scan if biliary pancreatitis is suspected as MRCP can be performed at the same time and stones within the common bile duct can be readily identified.88 Cost and accessibility limit the availability and use of MRI in rural areas.
Endoscopic ultrasound (EUS) has a defined role in AP—it is useful to evaluate the common bile duct for the presence of stones if gallstone pancre-atitis with choledocholithiasis is suspected. EUS can be followed by therapeutic ERCP if a common bile duct stone is identified (to remove said stone). ERCP can also be used to place a stent if biliary obstruction is seen (due to a mass, edema). In bili-ary pancreatitis, the best timing of when to use EUS versus ERCP is controversial. Current evidence is showing a trend of early EUS imaging over ERCP due to better cost-benefit ratios (especially in se-vere biliary pancreatitis),90,91 improved diagnoses (positive predictive value),92,93 and outcomes (ac-cording to a recent meta-analysis).94 ERCP should be used before (or in place of) EUS when acute pancreatitis is accompanied by signs of cholangi-tis. If impacted stones are suspected, they are, in addition to cholangitis, another potential indication for ERCP. EUS has some additional diagnostic ad-vantages over CT and transabdominal US: it may show the presence of microlithiasis, occult malig-nancies of the pancreas,95 and pancreas divisum.
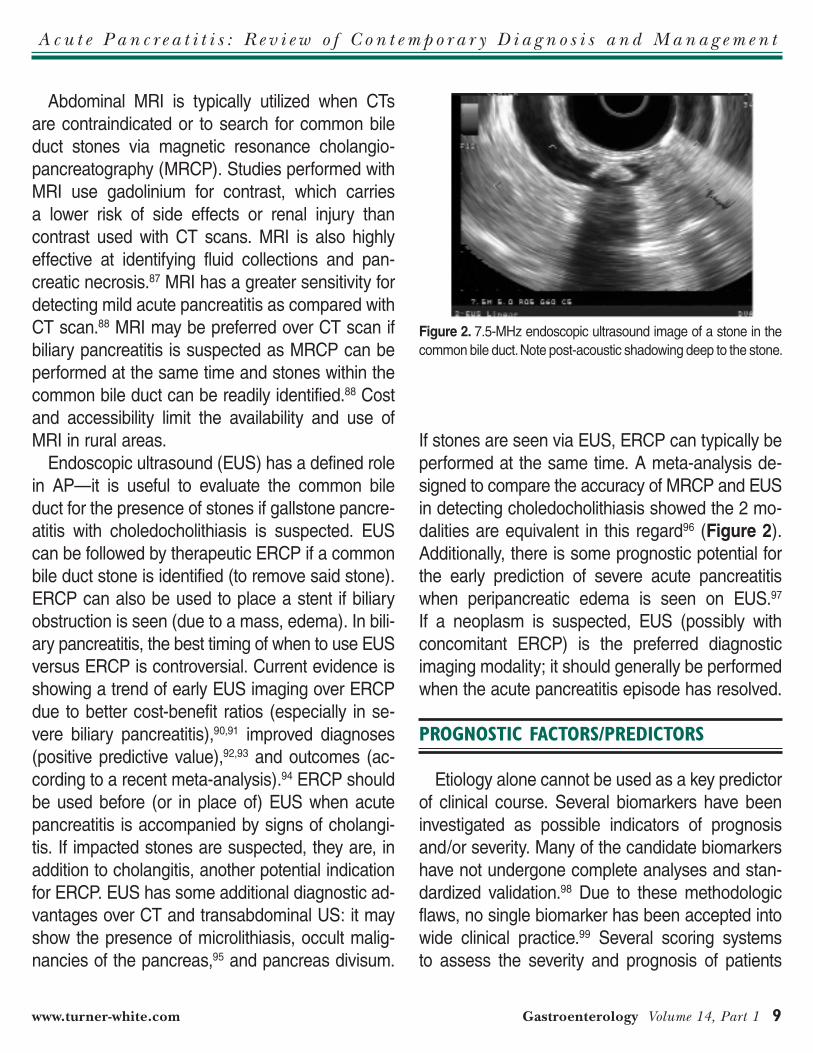
If stones are seen via EUS, ERCP can typically be performed at the same time. A meta-analysis de-signed to compare the accuracy of MRCP and EUS in detecting choledocholithiasis showed the 2 mo-dalities are equivalent in this regard96 (Figure 2). Additionally, there is some prognostic potential for the early prediction of severe acute pancreatitis when peripancreatic edema is seen on EUS.97 If a neoplasm is suspected, EUS (possibly with concomitant ERCP) is the preferred diagnostic imaging modality; it should generally be performed when the acute pancreatitis episode has resolved.
ProGnoStiC faCtorS/PrediCtorS
Etiology alone cannot be used as a key predictor of clinical course. Several biomarkers have been investigated as possible indicators of prognosis and/or severity. Many of the candidate biomarkers have not undergone complete analyses and stan-dardized validation.98 Due to these methodologic flaws, no single biomarker has been accepted into wide clinical practice.99 Several scoring systems to assess the severity and prognosis of patients
Figure 2. 7.5-MHz endoscopic ultrasound image of a stone in the common bile duct. Note post-acoustic shadowing deep to the stone.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 11
with acute pancreatitis (eg, Ranson criteria, Imrie scoring system, and Acute Physiology and Chronic Health Evaluation II [APACHE-II]) have been de-veloped.100–102 In 1976, Ranson reported the use of a series of 11 objective findings that correlate with severity in patients with acute pancreatitis (eg, age, serum levels of various markers, and serum calcium levels). APACHE II is most recommended by society guidelines,103–105 although it is rarely uti-lized in clinical practice outside of research studies. These scoring systems may help early in the clini-cal course of a patient with acute pancreatitis, al-though their usefulness diminishes as the disease progresses.101 Generally, renal failure, respiratory failure, multi-organ system failure, fluid collections, necrosis, increased ICU length of stay, and shock are all poor prognostic factors.106 In a study that as-sessed the use of scoring systems, CT, and serum markers to predict acute pancreatitis outcomes, imaging the pancreas alone was poorly predictive of outcome.107
Although these systems are excellent predic-tors of the severity of acute pancreatitis, they can be cumbersome to use. CRP may predict need for further supportive care within 24 to 48 hours of admission: it has better negative predictive value than Ranson’s criteria with preserved good positive predictive value,108 but not in all studies.109 Brown and colleagues have demonstrated that hemoconcentration is an early marker for organ failure and pancreatic necrosis when evaluated 24 hours after hospital admission, again suggest-ing the importance of adequate hydration in acute pancreatitis.75 Hemoconcentration markers have a sensitivity of 94% for detecting necrotizing pan-creatitis and a negative predictive value of 96%.75 Adequate hydration should be expected to reverse hemoconcentration and may reduce the risk of developing severe pancreatitis by increasing perfu-
sion of the gland. When used as a prognostic fac-tor, hematocrit determination is at least as accurate as APACHE-II scores but is available in less than half the time of the scoring systems and is much easier to use. Follow-up studies, unfortunately, have failed to validate the accuracy of hemocon-centration in prognosis of acute pancreatitis.110–112 Blood urea nitrogen (BUN) at admission, as well as an increase during the first 24 hours of hospi-talization, indicated higher mortality and may direct fluid resuscitation in the management of acute pancreatitis in 1 retrospective study.113 A newer scoring system that incorporates BUN >25 mg/dL, impaired mental status, SIRS, age >60 years, or the presence of a pleural effusion (BISAP) can predict mortality prior to organ failure within the first 24 hours but is not more simplistic or accurate than existing scoring systems.114,115 The harmless acute pancreatitis score (HAPS) measures only creatinine, hematocrit, and signs of peritonitis and appears to be the simplest of the scoring systems while maintaining accuracy in detecting mild pan-creatitis, though it has not yet undergone vigorous validation.
manaGement
treatment
Fluid resuscitation Most patients with mild acute pancreatitis recov-
er with supportive measures. Patients should have NPO status for at least 24 to 48 hours in mild acute pancreatitis and longer in severe acute pancreati-tis. In the absence of cardiopulmonary complica-tions, vigorous hydration with intravenous fluids should be administered until adequate urine output is achieved and maintained.75 Published studies have suggested rates from 250 to 1000 mL/hr with careful monitoring and ongoing reassessment

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
12 Hospital Physician Board review Manual www.turner-white.com
of the patient in order to establish adequate fluid resuscitation and to avoid fluid overload, although care must be individualized; obese patients may need greater fluid resuscitation.116,117 The exact volume, rate, and type of aggressive hydration have not been universally defined, and ultimately care must be individualized; as discussed above, hematocrit and BUN can be used to aid in tailoring fluid resuscitation. Early fluid resuscitation (defined as receiving ≥ one-third of the total 72-hour fluid volume within 24 hours of presentation) promotes lower rates of SIRS, organ failure, and ICU admis-sions and shorter hospitalizations in patients with interstitial acute pancreatitis.118 Wu et al recently suggested the superiority of lactated ringers so-lution when compared against normal saline in a small randomized control study, but treatment should be individualized.119
nutritionNutrition, as defined by total parenteral nutrition
(TPN) and enteral nutrition, plays a critical and central role in the therapy of acute pancreatitis. If pancreatic necrosis is seen, enteral feeding using a nasoenteric tube with the distal tip placed beyond the ligament of Treitz (enteral) is often performed to reduce the risk of bacterial transloca-tion from the gut to the necrotic pancreatic bed, improve intestinal wall integrity, and promote gut motility.120,121 Although nasogastric tube feeding in severe acute pancreatitis appears safe according to a recent meta-analysis, an adequately pow-ered randomized controlled study comparing it to nasojejunal feeding has been recommended and would prove useful in further investigation.122 One recent randomized control trial comparing naso-gastric versus nasojejunal feeding did not demon-strate inferiority of nasogastric feeding.123 Although clinical guidelines are available, practice greatly
depends upon regional, institutional, and provider preferences and tailoring to individual patients.124 TPN was once recommended in patients with se-vere pancreatitis, but it has been associated with increased length of stay, costs, and complication and mortality rates as well as increased systemic and local infections as compared with enteral nutri-tion.120,125 If the patient has not tolerated oral intake by day 7, one may consider beginning nasojejunal feeding.
Aggressive pain management and intravenous fluid replacement are recommended.126 Vital signs and urine output should be monitored every few hours for the first 24 to 48 hours by a multidisci-plinary team.
antibioticsA strong preventative measure for reducing in-
fections in pancreatic necrosis is to avoid intrave-nous nutrition and use enteral nutrition.127 The risk of developing infected pancreatic necrosis rises as the proportion of the involved/necrotic pan-creas increases.119 The presence of physiologic organ failure may be a more important prognostic factor than the presence of sterile or infected ne-crosis.128 Infected pancreatic necrosis is generally seen after day 7 to 10 and can be seen with new fever spikes, leukocytosis, worsening pain, and SIRS development. CT-guided needle aspiration and Gram stain of the aspirate are often sufficient to make the diagnosis, though if the pancreas is sterile there is an increased risk of introducing infection. Infected pancreatic necrosis was tradi-tionally treated by surgical debridement. Minimal-ly invasive techniques such as percutaneous and endoscopic drainage and minimally invasive ret-roperitoneal necrosectomy applied in a stepwise methodology in patients with infected pancre-atic necrosis have shown efficacy while reducing

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 13
complication rates, although these procedures are not widely performed.129 The timing of surgical intervention is variable—if patients are septic and the infected pancreatic fossa is felt to be respon-sible, surgical therapy may be required urgently. Current trends include delaying surgery to at least 4 weeks after the onset of symptoms, if possible, which may allow necrotic pancreatic tissue to be well demarcated at the time of surgery.130 Multiple surgeries may be required to fully debride necrotic pancreatic tissue.131 Infected pancreatic necrosis, pancreatic abscesses, and infected pseudocysts are the most common indicators for surgery in the acute phase of the illness, with more minimally invasive techniques favored if possible, although open abdominal procedures may be required.132 Patients with known or suspected infected ne-crosis often undergo needle aspiration to confirm infection, which can be performed via CT- or ultrasound-guided biopsies.133,134 In rare cases, patients with infected necrosis can be treated conservatively with aggressive antibiotics and avoid or significantly delay surgical intervention.135
The use of prophylactic antibiotics in patients with pancreatic necrosis (in an attempt to avoid in-fection) has been and remains controversial. Some studies have demonstrated benefit in this regard, while others have not shown an advantage, and prevailing opinion on this topic has changed sev-eral times in the past 10 to 15 years.136–141 Imipe-nem, meropenem, and fluoroquinolones are com-monly used in this setting as these agents have a high degree of pancreatic penetrance. Antibiotic prophylaxis cannot be universally recommended in the setting of acute pancreatitis. Guidelines for administering antibiotics set by Lanksich and Lerch may assist the clinician in prophylactic antimicro-bial use: SIRS or sepsis, multisystem organ failure, proven extrapancreatic or pancreatic infections, or
an increase in C-reactive protein with evidence of pancreatic or extrapancreatic infection.142 In gen-eral, the current thinking does not favor the use of prophylactic antibiotics in patients with severe acute pancreatitis.
other considerations
Pain management, typically with narcotics, should be implemented as well. Some data suggest the superiority of a patient-controlled analgesia (PCA) pump with the agent meperidine instead of mor-phine in this setting as morphine may increase sphincter of Oddi pressure.143 If the underlying cause of the episode of acute pancreatitis is ame-nable to correction (eg, choledocholithiasis), thera-peutic interventions such as ERCP with biliary sphincterotomy and duct clearance and/or cho-lecystectomy may be indicated (Figure 3). Other important etiologies that may be correctable are alcohol use/abuse, hypercalcemia, hypertriglyc-eridemia, and drug-induced pancreatitis. There is little to be gained from daily monitoring of serum amylase and lipase.76,77 Patients can be gradually returned to oral intake as abdominal pain recedes and hunger returns. Over the course of mild acute pancreatitis, most laboratory abnormalities should show improvement and resolution without further intervention within 3 to 7 days.144
Patients with more severe acute pancreatitis, manifested as the development of peripancreatic fluid collection, pancreatic pseudocysts, pancreatic necrosis, and/or the development of respiratory, renal, or circulatory compromise, require more ag-gressive management, and ICU admission is often warranted (Figure 4). In general, a multidisciplinary approach with both medical and surgical teams is generally beneficial. Renal failure may warrant hemodialysis, and patients with respiratory failure may require mechanical ventilation.145–147 Most acute

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
14 Hospital Physician Board review Manual www.turner-white.com
fluid collections and/or pseudocysts do not require interventions unless they become infected or cause significant extrinsic compression of other organs. The management of chronic fluid collections such as pseudocysts is complex and controversial. In general, small pseudocysts are treated via obser-vation. Large cysts, cysts that become infected, or cysts that compress the stomach or bowel (causing
gastric outlet obstruction) or the bile duct (causing jaundice) are more likely to warrant drainage by endoscopic, surgical, or interventional radiology approaches.148,149 Surgical approaches can be per-formed in an open or laparoscopic manner. From an endoscopic point of view, transmural (through the stomach or the bowel wall) and transampullary (through the pancreatic duct) approaches are avail-able to drain pancreatic pseudocysts.
One Dutch multicenter, randomized controlled trial demonstrated that in patients with infected pancreatic necrosis, endoscopic or percutaneous drainage of infected fluid collections followed by minimally invasive retroperitoneal necrosectomy achieved superior outcomes as compared to tra-ditional open necrosectomy alone.150 Outcomes were defined in terms of lower total costs, resourc-es utilized, length of stay, long-term and major complications, and death.
ConCluSion
Acute pancreatitis remains a significant cause of morbidity and mortality. Most patients with mild
Figure 3. Endoscopic retrograde cholangiopancreatography for choledocholithiasis. (a) Endoscopic image of a biliary sphincterotomy being performed at the major papilla with a sphincterotome. (B) Endoscopic image of a large common bile duct (CBD) stone following balloon extraction. The stone is left in the CBD to pass on its own after removal.
Figure 4. 7.5-MHz endoscopic ultrasound image of a thick-walled pancreatic pseudocyst in a patient with moderate to severe acute pancreatitis.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 15
acute pancreatitis will recover with conservative measures, although patients who develop more severe pancreatitis, especially those with pancre-atic necrosis, require aggressive management and can still have a poor outcome. A multidisciplinary approach is warranted in patients with severe pancreatitis as input from intensivists, gastroen-terologists, surgeons, and radiologists and other specialists are usually required. Treatable causes of pancreatitis should be identified and managed appropriately. Despite investigations, a cause of pancreatitis may not be identified in all patients.
referenCeS
1. DeFrances CJ, Cullen KA, Kozak LJ. National hospital discharge survey: 2005 annual summary with detailed di-agnosis and procedure data. Vital Health Stat 2007;165:1–209.
2. Hall MJ, DeFrances CJ, Williams SN, et al. National Hos-pital Discharge Survey: 2007 summary. National Health Statistics reports; no 29. Hyattsville, MD: National Center for Health Statistics. 2010. www.cdc.gov/nchs/data/nhsr/nhsr029.pdf. Accessed June 13, 2013.
3. Goldacre MJ, Roberts SE. Hospital admission for acute pancreatitis in an English population, 1963–98: database study of incidence and mortality. BMJ 2004;328:1466–9.
4. Yadav D, Lowenfels AB. Trends in the epidemiology of the first attack of acute pancreatitis. Pancreas 2006;33:323–30.
5. Fagenholz PJ, Fernández-del Castillo C, Harris NS, et al. Direct medical costs of acute pancreatitis hospitalizations in the United States. Pancreas 2007;35:302–7.
6. Trapnell JE, Duncan EH. Patterns of incidence in acute pancreatitis. BMJ 1975;2:179–83.
7. Frey CF, Zhou H, Harvey DJ, White RH. The incidence and case-fatality rates of acute biliary, alcoholic, and id-iopathic pancreatitis in California, 1994-2001. Pancreas 2006;33:336–44.
8. Banks PA, Bollen TL, Dervenis C, et al; Acute Pancreatitis Classification Working Group. Classification of acute pan-
creatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
9. Chwistek M, Roberts I, Amoateng-Adjepong Y. Gallstone pancreatitis: a community teaching hospital experience. J Clin Gastroenterol 2001;33:41–4.
10. Venneman NG, Buskens E, Besselink MG, et al. Small gallstones are associated with increased risk of acute pancreatitis: potential benefits of prophylactic cholecystec-tomy? Am J Gastroenterol 2005;100:2540–50.
11. van Baal MC, Besselink MG, Bakker OJ, et AL; Dutch Pancreatitis Study Group. Timing of cholecystectomy after mild biliary pancreatitis: a systematic review. Ann Surg 2012;255:860–6.
12. Shaffer EA. Gallstone disease: Epidemiology of gallblad-der stone disease. Best Pract Res Clin Gastroenterol 2006;20:981–96.
13. Yaghoubian A, De Virgilio C, El-Masry M, et al. Gallstone pancreatitis: a benign disease in Hispanics. Am Surg 2007;73:1071–4.
14. Martínez J, Sánchez-Payá J, Palazón JM, et al. Is obesity a risk factor in acute pancreatitis? A meta-analysis. Pan-creatology 2004;4:42–8.
15. Ramin KD, Ramin SM, Richey SD, Cunningham FG. Acute pancreatitis in pregnancy. Am J Obstet Gynecol 1995;173:187–91.
16. Corlett RC Jr, Mishell DR Jr. Pancreatitis in pregnancy. Am J Obstet Gynecol 1972;113:281–90.
17. Block P, Kelly TR. Management of gallstone pancreatitis during pregnancy and the postpartum period. Surg Gyne-col Obstet 1989;168:426–8.
18. Lévy P, Boruchowicz A, Hastier P, et al. Diagnostic criteria in predicting a biliary origin of acute pancreatitis in the era of endoscopic ultrasound: multicentre prospective evalua-tion of 213 patients. Pancreatology 2005;5:450–6.
19. Tsai CJ, Leitzmann MF, Willett WC, Giovannucci EL. The effect of long-term intake of cis unsaturated fats on the risk for gallstone disease in men: a prospective cohort study. Ann Intern Med 2004;141:514–22.
20. Leitzmann MF, Willett WC, Rimm EB, et al. A prospective study of coffee consumption and the risk of symptomatic gallstone disease in men. JAMA 1999;281:2106–12.
21. Leitzmann MF, Giovannucci EL, Stampfer MJ, et al. Pro-spective study of alcohol consumption patterns in relation to symptomatic gallstone disease in men. Alcohol Clin Exp Res 1999;23:835–41.
22. Lankisch PG, Lowenfels AB, Maisonneuve P. What is the risk of alcoholic pancreatitis in heavy drinkers? Pancreas 2002;25:411–2.
23. Yadav D, Whitcomb DC. The role of alcohol and smoking in pancreatitis. Nat Rev Gastroenterol Hepatol 2010;7:131–45.
24. National Institutes of Health. Drinking in the United States:
Board reVieW Questionstest your knowledge of this topic.
Go to www.turner-white.com and select Gastroenterologyfrom the drop-down menu of specialties.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
16 Hospital Physician Board review Manual www.turner-white.com
Main findings from the 1992 National Longitudinal Alcohol Epidemiologic Survey (NLAES). US Alcohol Epidemiologic Data Reference Manual. Vol 6. 1st ed. Nov 1998. NIH Pub No. 99-3519.
25. Sadr-Azodi O, Andrén-Sandberg A, Orsini N, Wolk A. Cig-arette smoking, smoking cessation and acute pancreatitis: a prospective population-based study. Gut 2011 Aug 11. [Epub ahead of print].
26. Lang MB, Segersvärd R, Grundsten M, et al. Management of alcohol use disorders in patients with chronic pancre-atitis. JOP 2012;13:654–9.
27. Levy MJ, Geenen JE. Idiopathic acute recurrent pancreati-tis. Am J Gastroenterol 2001;96:2540–55.
28. Banks PA, Freeman ML. Practice guidelines in acute pan-creatitis. Am J Gastroenterol 2006;101:2379–400.
29. Elta GH. Sphincter of Oddi dysfunction and bile duct micro-lithiasis in acute idiopathic pancreatitis. World J Gastroen-terol 2008;14:1023–6.
30. Whitcomb DC, Preston RA, Aston CE, et al. A gene for hereditary pancreatitis maps to chromosome 7q35. Gas-troenterology 1996;110:1975–80.
31. Whitcomb DC, Preston RA, Aston CE, et al. Hereditary pancreatitis is caused by a mutation in the cationic tryp-sinogen gene. Nat Genet 1996;14:141–5.
32. Lowenfels AB, Maisonneuve P, DiMagno EP, et al. Heredi-tary pancreatitis and the risk of pancreatic cancer. Interna-tional Hereditary Pancreatitis Study Group. J Natl Cancer Inst 1997;89:442–6.
33. Papachristou GI, Sass DA, Avula H, et al. Is the mono-cyte chemotactic protein-1 -2518 G allele a risk factor for severe acute pancreatitis? Clin Gastroenterol Hepatol 2005;3:475–81.
34. Howes N, Greenhalf W, Stocken DD, Neoptolemos JP. Cationic trypsinogen mutations and pancreatitis. Clin Lab Med 2005;25:39–59.
35. Zoller H, Egg M, Graziadei I, et al. CFTR gene mutations in pancreatitis: Frequency and clinical manifestations in an Austrian patient cohort. Wien Klin Wochenschr 2007;119:527–33.
36. Cohn JA, Friedman KJ, Noone PG, et al. Relation between mutations of the cystic fibrosis gene and idiopathic pancre-atitis. N Engl J Med 1998;339:653–8.
37. Pezzilli R, Morselli-Labate AM, Mantovani V, et al. Muta-tions of the CFTR gene in pancreatic disease. Pancreas 2003;27:332–6.
38. Mennecier D, Pons F, Arvers P, et al. Incidence and sever-ity of non alcoholic and non biliary pancreatitis in a gastro-enterology department. Gastroenterol Clin Biol 2007;31(Pt 1):664–7.
39. Badalov N, Baradarian R, Iswara K, et al. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastro-
enterol Hepatol 2007;5:648–61. 40. Vinklerova I, Prochazka M, Prochazka V, Urbanek K. Inci-
dence, severity and etiology of drug-induced acute pancre-atitis. Dig Dis Sci 2010;55:2977–81.
41. Badalov N, Baradarian R, Iswara K, et al. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastro-enterol Hepatol 2007;5:648–61.
42. Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol 2005;39:709–16.
43. Mallory A, Kern F. Drug-induced pancreatitis. Baillieres Clin Gastroenterol 1988;2:293–307.
44. Youssef SS, Iskandar SB, Scruggs J, Roy TM. Acute pan-creatitis associated with omeprazole. Int J Clin Pharmacol Ther 2005;43:558–61.
45. Frank CD, Adler DG. Post-ERCP pancreatitis and its pre-vention. Nat Clin Pract Gastroenterol Hepatol 2006;3:680–8.
46. Andriulli A, Loperfido S, Napolitano G, et al. Incidence rates of post-ERCP complications: a systematic survey of pro-spective studies. Am J Gastroenterol 2007;102:1781–8.
47. Singh P, Das A, Isenberg G, Wong RC, et al. Does prophy-lactic pancreatic stent placement reduce the risk of post-ERCP acute pancreatitis? A meta-analysis of controlled trials. Gastrointest Endosc 2004;60:544–50.
48. Das A, Singh P, Sivak MV Jr, Chak A. Pancreatic-stent placement for prevention of post-ERCP pancreati-tis: a cost-effectiveness analysis. Gastrointest Endosc 2007;65:960–8.
49. Mazaki T, Masuda H, Takayama T. Prophylactic pancreatic stent placement and post-ERCP pancreatitis: a systematic review and meta-analysis. Endoscopy 2010;42:842–53.
50. Elmunzer BJ, Waljee AK, Elta GH, et al. A meta-analysis of NSAIDs in the prevention of post-ERCP pancreatitis. Gut 2008;57:1262–7.
51. Halm MA. Acute gastrointestinal complications after car-diac surgery. Am J Crit Care 1996;5:109–18.
52. Van OS EC, Petersen BT. Pancreatitis secondary to per-cutaneous liver biopsy-associated hemobilia. Am J Gastro-enterol 1996;91:577–80.
53. Panicek DM, Ewing DK, Gottlieb RH, Chew FS. Gastros-tomy tube pancreatitis. Pediatr Radiol 1988;18:416–7.
54. Parsi MA, Sanaka MR, Dumot JA. Iatrogenic recurrent pancreatitis. Pancreatology 2007;7:539.
55. Izsak EM, Shike M, Roulet M, Jeejeebhoy KN. Pancreati-tis in association with hypercalcemia in patients receiving total parenteral nutrition.Gastroenterology 1980;79:555–8.
56. Parenti DM, Steinberg W, Kang P. Infectious causes of acute pancreatitis. Pancreas 1996;13:356–71.
57. Fortson MR, Freedman SN, Webster PD 3rd. Clinical as-sessment of hyperlipidemic pancreatitis. Am J Gastroen-terol 1995;90:2134–9.
58. Yuan G, Al-Shali KZ, Hegele RA. Hypertriglyceridemia: its

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 17
etiology, effects and treatment. CMAJ 2007;176:1113–20. 59. Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis,
classification, and new genetic developments. Gastroen-terology 2001;120:682–707.
60. Fernández-del Castillo C, Harringer W, Warshaw AL, et al. Risk factors for pancreatic cellular injury after cardiopulmo-nary bypass. N Engl J Med 1991;325:382–7.
61. Michalopoulos A, Papadopoulos V, Apostolidis S, et al. Severe acute pancreatitis as a first symptom of primary hyperparathyroidism: a rare case report. Int J Surgery 2007;9.
62. Bartholomew C. Acute scorpion pancreatitis in Trinidad. Br Med J 1970;1:666–8.
63. Barrhet M. Acute pancreatitis: an emerging presentation for autoimmune pancreatitis in patients with inflammatory bowel disease. Gastroenterol Hepatol 2009;5:431–3.
64. Kandula L, Lowe ME. Etiology and outcome of acute pan-creatitis in infants and toddlers. J Pediatr 2008;152:106–10.
65. Lund H, Tonnesen H, Tonnesen MH, Olsen O. Long-term recurrence and death rates after acute pancreatitis. Scand J Gastroenterol 2006;41:234–8.
66. McAlister VC, Davenport E, Renouf E. Cholecystectomy deferral in patients with endoscopic sphincterotomy. Co-chrane Database Syst Rev 2007;(4):CD006233.
67. van Acker GJ, Perides G, Steer ML. Co-localization hy-pothesis: a mechanism for the intrapancreatic activation of digestive enzymes during the early phases of acute pancreatitis. World J Gastroenterol 2006;12:1985–90.
68. Bhatia M, Wong FL, Cao Y, et al. Pathophysiology of acute pancreatitis. Pancreatology 2005;5:132–44.
69. Harper SJ, Cheslyn-Curtis S. Acute pancreatitis. Ann Clin Biochem 2011;48(Pt 1):23–37.
70. Hirota M, Ohmuraya M, Baba H. The role of trypsin, trypsin inhibitor, and trypsin receptor in the onset and aggravation of pancreatitis. J Gastroenterol 2006;41:832–6.
71. Rahman SH, Ibrahim K, Larvin M, et al. Association of antioxidant enzyme gene polymorphisms and glutathione status with severe acute pancreatitis. Gastroenterology 2004;126:1312–22.
72. Gorelick FS. Alcohol and zymogen activation in the pan-creatic acinar cell. Pancreas 2003;27:305–10.
73. Staniland JR, Ditchburn J, De Dombal FT. Clinical pre-sentation of acute abdomen: study of 600 patients. BMJ 1972;3:393–8.
74. Hill MC, Barkin J, Isikoff MB, et al. Acute pancreatitis: clinical vs. CT findings. AJR Am J Roentgenol 1982;139:263–9.
75. Brown A, Orav J, Banks PA. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis. Pan-creas 2000;20:367–72.
76. Talukdar R, Vege SS. Recent developments in acute pan-creatitis. Clin Gastroenterol Hepatol 2009;S3–9.
77. Gumaste V, Dave P, Sereny G. Serum lipase: a better test to diagnose acute alcoholic pancreatitis. Am J Med 1992;92:239–42.
78. Clavé P, Guillaumes S, Blanco I, et al. Amylase, lipase, pancreatic isoamylase, and phospholipase A in diagnosis of acute pancreatitis. Clin Chem 1995;41(8 Pt 1):1129–34.
79. Orebaugh SL. Normal amylase levels in the presentation of acute pancreatitis. Am J Emerg Med 1994;12:21–4.
80. Lin XZ, Wang SS, Tsai YT, et al. Serum amylase, iso-amylase, and lipase in the acute abdomen. Their diag-nostic value for acute pancreatitis. J Clin Gastroenterol 1989;11:47–52.
81. Pezzilli R, Billi P, Miglioli M, Gullo L. Serum amylase and lipase concentrations and lipase/amylase ratio in assess-ment of etiology and severity of acute pancreatitis. Dig Dis Sci 1993;38:1265–9.
82. Vissers RJ, Abu-Laban RB, McHugh DF. Amylase and lipase in the emergency department evaluation of acute pancreatitis. J Emerg Med 1999;17:1027–37.
83. Sutton PA, Humes DJ, Purcell G, et al. The role of rou-tine assays of serum amylase and lipase for the diag-nosis of acute abdominal pain. Ann R Coll Surg Engl 2009;91:381e4.
84. Tenner S, Dubner H, Steinberg W. Predicting gallstone pancreatitis with laboratory parameters: a meta-analysis. Am J Gastroenterol 1994;89:1863–6.
85. Hagiwara A, Miyauchi H, Shimazaki S. Predictors of vas-cular and gastrointestinal complications in severe acute pancreatitis. Pancreatology 2008;8:211–8.
86. Brown A, Orav J, Banks PA. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis. Pan-creas 2000;20:367–72.
87. Dervenis C, Johnson CD, Bassi C, et al. Diagnosis, objec-tive assessment of severity, and management of acute pancreatitis. Santorini consensus conference. Int J Pancre-atol 1999;25:195–210.
88. Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990;174:331–6.
89. Arvanitakis M, Delhaye M, De Maertelaere V, et al. Com-puted tomography and magnetic resonance imaging in the assessment of acute pancreatitis. Gastroenterology 2004;126:715–23.
90. Buscarini E, Tansini P, Vallisa D, et al. EUS for sus-pected choledocholithiasis: do benefits outweigh costs? A prospective, controlled study. Gastrointest Endosc 2003;57:510–8.
91. Romagnuolo J, Currie G; Calgary Advanced Therapeutic Endoscopy Center Study Group. Noninvasive vs. selec-tive invasive biliary imaging for acute biliary pancreatitis: an economic evaluation by using decision tree analysis.
A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
18 Hospital Physician Board review Manual www.turner-white.com
Gastrointest Endosc 2005;61:86–97.92. Chak A, Hawes RH, Cooper GS, et al. Prospective as-
sessment of the utility of EUS in the evaluation of gallstone pancreatitis. Gastrointest Endosc 1999;49:599–604.
93. Stabuc B, Drobne D, Ferkolj I, et al. Acute biliary pancreati-tis: detection of common bile duct stones with endoscopic ultrasound. Eur J Gastroenterol Hepatol 2008;20:1171–5.
94. Uy MC, Daez ML, Sy PP, et al. Early ERCP in acute gall-stone pancreatitis without cholangitis: a meta-analysis. JOP 2009;10:299–305.
95. Vanwoerkom RC, Bentz J, Chen L, Adler DG. EUS diag-nosis of a primary pancreatic metastasis of alveolar rhab-domyosarcoma. JOP 2009;10:683–5.
96. Verma D, Kapadia A, Eisen GM, Adler DG. EUS vs MRCP for detection of choledocholithiasis. Gastrointest Endosc 2006;64:248–54.
97. Sotoudehmanesh R, Hooshyar A, Kolahdoozan S, et al. Prognostic value of endoscopic ultrasound in acute pan-creatitis. Pancreatology 2010;10:702–6.
98. Sigounas DE, Tatsioni A, Christodoulou DK, et al. New prog-nostic markers for outcome of acute pancreatitis: overview of reporting in 184 studies. Pancreas 2011;40:522–32.
99. Neoptolemos JP, Kemppainen EA, Mayer JM, et al. Early prediction of severity in acute pancreatitis by urinary tryp-sinogen activation peptide: a multicentre study. Lancet 2000;355:1955–60.
100. Ranson JH. Etiological and prognostic factors in human acute pancreatitis: a review. Am J Gastroenterol 1982;77:633–8.
101. Blamey SL, Imrie CW, O’Neill J, et al. Prognostic factors in acute pancreatitis. Gut 1984;25:1340–6.
102. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13:818–29.
103. Banks PA, Freeman ML; Practice Parameters Commit-tee of the American College of Gastroenterology. Prac-tice guidelines in acute pancreatitis. Am J Gastroenterol 2006;101:2379–400.
104. Forsmark CE, Baillie J; AGA Institute Clinical Practice and Economics Committee; AGA Institute Governing Board. AGA Institute technical review on acute pancreatitis. Gas-troenterology 2007;132:2022–44.
105. Working Party of the British Society of Gastroenterology; Association of Surgeons of Great Britain and Ireland; Pan-creatic Society of Great Britain and Ireland; Association of Upper GI Surgeons of Great Britain and Ireland. UK guidelines for the management of acute pancreatitis. Gut 2005;54(Suppl 3):iii1-iii9.
106. Kong L, Santiago N, Han TQ, Zhang SD. Clinical charac-teristics and prognostic factors of severe acute pancreati-tis. World J Gastroenterol 2004;10:3336–8.
107. Robert JH, Frossard JL, Mermillod B, et al. Early predic-tion of acute pancreatitis: prospective study comparing computed tomography scans, Ranson, Glascow, Acute Physiology and Chronic Health Evaluation II scores, and various serum markers. World J Surg 2002;26:612–9.
108. Duarte-Rojo A, Suazo-Barahona J, Ramírez-Iglesias MT, et al. Time frames for analysis of inflammatory mediators in acute pancreatitis: improving admission triage. Dig Dis Sci 2009;54:2282–7.
109. Riche FC, Cholley BP, Laisne MJ, et al. Inflammatory cyto-kines, C-reactive protein, and procalcitonin as early predic-tors of necrosis infection in acute necrotizing pancreatitis. Surgery 2003;133:257–62.
110. Lankisch PG, Mahlke R, Blum T, et al. Hemoconcentration: an early marker of severe and/or necrotizing pancreatitis? a critical appraisal. Am J Gastroenterol 2001;96:2081–5.
111. Remes-Troche JM, Duarte-Rojo A, Morales G, Robles-Dıaz G. Hemoconcentration is a poor predictor of severity in acute pancreatitis. World J Gastroenterol 2005;11:7018–23.
112. Gardner TB, Olenec CA, Chertoff JD, et al. Hemoconcen-tration and pancreatic necrosis: further defining the rela-tionship. Pancreas 2006;33:169–73.
113. Wu BU, Bakker OJ, Papachristou GI, et al. Blood urea ni-trogen in the early assessment of acute pancreatitis: an in-ternational validation study. Arch Intern Med 2011;171:669.
114. Wu BU, Johannes RS, Sun X, et al. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut 2008;57:1698–703.
115. Papachristou GI, Muddana V, Yadav D, et al. Comparison of BISAP, Ranson’s, APACHE-II, and CTSI scores in pre-dicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol 2010;105:435–41.
116. Gardner TB, Vege SS, Pearson RK, Chari ST. Fluid resus-citation in acute pancreatitis. Clin Gastroenterol Hepatol 2008;6:1070–6.
117. Wall I, Badalov N, Baradarian R, et al. Decreased mortality in acute pancreatitis related to early aggressive hydration. Pancreas 2011;40:547–50.
118. Warndorf MG, Kurtzman JT, Bartel MJ, et al. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. Clin Gastroenterol Hepatol 2011;9:705–9.
119. Wu BU, Hwang JQ, Gardner TH, et al. Lactated ringer’s solution reduces systemic inflammation compared with sa-line in patients with acute pancreatitis. Clin Gastroenterol Hepatol 2011;9:710–7.
120. Buchler MW, Gloor B, Muller CA, et al. Acute necrotizing pancreatitis: treatment strategy according to the status of infection. Ann Surg 2000;232:619–26.
121. Marik PE, Zaloga GP. Meta-analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis. BMJ 2004;328:1407.

A c u t e P a n c r e a t i t i s : R e v i e w o f C o n t e m p o r a r y D i a g n o s i s a n d M a n a g e m e n t
www.turner-white.com Gastroenterology Volume 14, Part 1 19
122. Petrov MS, Correia MI, Windsor JA. Nasogastric tube feed-ing in predicted severe acute pancreatitis. A systematic review of the literature to determine safety and tolerance. JOP 2008;9:440–8.
123. Singh N, Sharma B, Sharma M, et al. Evaluation of early enteral feeding through nasogastric and nasojejunal tube in severe acute pancreatitis: a noninferiority randomized controlled trial. Pancreas 2011 Jul 14 [Epub ahead of print].
124. Davies AR, Morrison SS, Ridley EJ, et al; ASAP Study Investigators. Nutritional therapy in patients with acute pancreatitis requiring critical care unit management: a prospective observational study in Australia and New Zea-land. Crit Care Med 2011;39:462–8.
125. Al-Omran M, Groof A, Wilke D. Enteral versus parenteral nutrition for acute pancreatitis. Cochrane Database Syst Rev 2003;(1):CD002837.
126. Tenner S. Initial management of acute pancreatitis: criti-cal issues during the first 72 hours. Am J Gastroenterol 2004;99:2489–94.
127. Zavyalov T, Khotsyna Y, Tenner S. The role of antibiotics in the management of patients with acute necrotizing pancre-atitis. Curr Infect Dis Rep 2010;12:13–8.
128. Malangoni MA, Martin AS. Outcome of severe acute pan-creatitis. Am J Surg 2005;189:273–7.
129. van Santvoort HC, Besselink MG, Bakker OJ, et al; Dutch Pancreatitis Study Group. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010;362:1491–502.
130. Werner J, Schneider L, Uhl W, Büchler MW. [Acute pancre-atitis: surgical therapy] Praxis (Bern 1994) 2005;94:825–30.
131. Werner J, Uhl W, Hartwig W, et al. Modern phase-specific management of acute pancreatitis. Dig Dis 2003;21:38–45.
132. Mayerle J, Hlouschek V, Lerch MM. Current management of acute pancreatitis. Nat Clin Pract Gastroenterol Hepatol 2005;2:473–83.
133. Banks PA, Gerzof SG, Langevin RE, et al. CT-guided aspi-ration of suspected pancreatic infection: bacteriology and clinical outcome. Int J Pancreatol 1995;18:265–70.
134. Rau B, Pralle U, Mayer JM, Beger HG. Role of ultraso-nographically guided fine-needle aspiration cytology in the diagnosis of infected pancreatic necrosis. Br J Surg 1998;85:179–84.
135. Adler DG, Chari ST, Dahl TJ, et al. Conservative manage-ment of infected necrosis complicating severe acute pan-creatitis. Am J Gastroenterol 2003;98:98–103.
136. Sainio V, Kemppainen E, Puolakkainen P, et al. Early an-tibiotic treatment in acute necrotising pancreatitis. Lancet
1995;346:663–7.137. Delcenserie R, Yzet T, Ducroix JP. Prophylactic antibiotics
in treatment of severe acute alcoholic pancreatitis. Pan-creas 1996;13:198–201.
138. Bassi C, Falconi M, Talamini G, et al. Controlled clinical trial of pefloxacin versus imipenem in severe acute pancreatitis. Gastroenterology 1998; 115:1513–7.
139. Isenmann R, Runzi M, Kron M, et al. Prophylactic antibiotic treatment in patients with predicted severe acute pancre-atitis: A placebo-controlled, double-blind trial. Gastroenter-ology 2004;126:997–1004.
140. Dellinger EP, Tellado JM, Soto NE, et al. Early antibiotic treatment for severe acute necrotizing pancreatitis: a ran-domized, double-blind, placebo-controlled study. Ann Surg 2007; 245:674–83.
141. García-Barrasa A, Borobia FG, Pallares R, et al. A double-blind, placebo-controlled trial of ciprofloxacin prophylaxis in patients with acute necrotizing pancreatitis. J Gastrointest Surg 2009;13:768–74.
142. Lankisch PG, Lerch MM. The role of antibiotic prophylaxis in the treatment of acute pancreatitis. J Clin Gastroenterol 2006; 40:149–55.
143. Helm JF, Venu RP, Geenen JE, et al. Effects of morphine on the human sphincter of Oddi. Gut 1988;29:1402–7.
144. Johnson C, Charnley R, Rowlands B, et al. UK guidelines for the management of acute pancreatitis. Gut 2005;54 Suppl 3:1–9.
145. Renner IG, Savage WT 3rd, Pantoja JL, Renner VJ. Death due to acute pancreatitis: a retrospective analysis of 405 autopsy cases. Dig Dis Sci 1985;30:1005–18.
146. Jaber S, Chanques G, Sebbane M, et al. Noninvasive positive pressure ventilation in patients with respira-tory failure due to severe acute pancreatitis. Respiration 2006;73:166–172.
147. Bolooki H, Gliedman ML. Peritoneal dialysis in treatment of acute pancreatitis. Surgery 1968;64:466–71.
148. Antillon MR, Shah RJ, Stiegmann G, Chen YK. Single-step EUS-guided transmural drainage of simple and complicated pancreatic pseudocysts. Gastrointest Endosc 2006;63:797–803.
149. Bergman S, Melvin WS. Operative and nonoperative man-agement of pancreatic pseudocysts. Surg Clin North Am 2007;87:1447–60, ix.
150. van Santvoort HC, Besselink MG, Bakker OJ, et al; Dutch Pancreatitis Study Group. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010;362:1491–502.
Copyright 2013 by Turner White Communications Inc., Wayne, PA. All rights reserved.