stat - irp-cdn.multiscreensite.com · nada de comer o beber por 4 horas antes de! examen....
TRANSCRIPT

X-RAY (WALK-INS ACCEPTED 8 A.M. TO 4 P.M)______________________________________________________________________ ULTRASOUND ______________________________________________________________________________________________________ EKG _________________________________________________________ ECHOCARDIOGRAM __________________________________________ DEXASCAN __________________________________________________ FLUOROSCOPY_______________________________________________ VIRTUAL COLONOSCOPY______________________________________ OTHER SCAN_________________________________________________
CT SCAN______________CONTRAST: W W/O W/WO CT Contrast (Iodinated)
If patient is over 65, has a history of diabetes, renal disease, hypertension,proteinuria, or gout please include:Creatinine:_______Date Drawn:________( Must be within the past 90 days)
MRI__________________________________________________________MRI CONTRAST: W W/O W/WO ARTHROGRAMMRI Contrast (Gadolinium)
If patient is over 65, has a history of diabetes, renal disease, hypertension,proteinuria, or gout please include:GFR:_________ Date Drawn:__________(Must be within the past 90 days)If you have a surgically implanted device such as a pacemaker, stent, painpump, neurostimulator, brain aneurysm clips, or recently implanted metal inyour body, inform the scheduler while making your appointment. Pleasebring any documentation regarding your device with you to yourappointment.
MRA_______________CONTRAST: W W/O W/WO NUCLEAR MEDICINE__________________________________________ CARDIOLITE/TREADMILL_____________________________________ CARDIOLITE/LEXISCAN_______________________________________WHOLE BODY BONE SCAN (WITH PLAIN FILMS IF INDICATED)
CTA ____________________________________________
CTA CORONARY CTA CORONARIES AND RENAL ARTERIES CTA CHEST (PULMONARY ARTERIES OR
THORACIC AORTA) CTA ABDOMEN (INCLUDING RENALS) CTA AORTOGRAM W/RUNOFF CTA BRAIN CTA NECK CAROTIDS
3D MAMMOGRAPHY (SCREENING) _________________
3D MAMMOGRAPHY (DIAGNOSTIC)________________ ULTRASOUND / AS NEEDED_______________________ MIRALUMA/AS NEEDED___________________________ STEREOTACTIC BREAST BIOPSY / AS NEEDED_______ US GUIDED BIOPSY/AS NEEDED ___________________
3025 S. RAINBOW BLVD.LAS VEGAS, NEVADA 89146 PHONE:(702) 222-3544
FAX: (702) 889-0422
FAX: (702) 948-6305
WEST VALLEY IMAGING 2611 HORIZON RIDGE PKWY. HENDERSON, NEVADA 89052 PHONE: (702) 990-7240
FAX: (702) 990-7250
WEST VALLEY IMAGING SEND CD AND REPORTS SEND FILMS AND REPORT
REPORT ONLY
DIGITALLY SEND IMAGES TO OFFICEOFFICE EMAIL:_____________________________________
FAX RESULTS TO OFFICE, FAX#:_____________________ PATIENT TO WAIT FOR RESULTS
RETURN PATIENT AND FILMS TO OFFICE
ANGIOGRAPHY
MAMMOGRAPHY
PET PET SCAN_______________________________________PET/CT ROUTINE (SKULL TO THIGH)______________PET/CT BRAIN___________________________________ PET/CT WHOLE BODY____________________________
(MELANOMA, METASTASIS ONLY)
SCHEDULING PHONE #: (702) 222-3544 SCHEDULING FAX #: (702) 889-0422WWW.WVIMAGING.COM
STAT
COMPARISON REQUESTED LAST EXAM PERFORMED:_____________________DATE:__________LOCATION:____________________
ORDER DATE:____________PATIENTS NAME:_______________________________DOB: (REQUIRED) ____________ PHONE #:_____________________ PRIMARY INSURANCE__________________________SECONDARY INSURANCE_____________________________________ AUTHORIZATION#: ____________________________APPT DATE: _______________________APPT TIME: _______________ HISTORY/SYMPTOMS:__________________________________________DIAGNOSIS/ICD-10:____________________________
SIGNATURE REQUIRED, STAMPED SIGNATURES ARE NOT ACCEPTEDREFERRING PHYSICIAN NAME:_________________________________SIGNATURE:__________________________________ REFERRING OFFICE CONTACT NAME:__________________________OFFICE PHONE#:_______________________________
FOR THE PATIENT
Please foil ow the instructions marked by your Physician.
UPPER GI, SMALL BOWEL, ESOPHAGUS: -- Nothing to eat or drink after midnight on the day before exam. No breakfast. No Liquids,
smoking or chewing gum on the morning of the exam.
BARIUM ENEMA: Follow the "24" hour directions on the prep kit. Please follow closely.
__ CT GUIDED BIOPSY/ PORT PLACEMENT:No blood thinners three days prior to exam.
__ ULTRASOUND: (ABDOMINAL LIVER, GALL BLADDER, PANCREAS). Nothing to eat or drink 4 hours prior to exam.
OB & PELVIC ULTRASOUND: Patient must start drinking 32 oz. of water I hour before the appointment. Do not empty bladder. A full bladder is necessary for the exam.
MAMMOGRAPHY: Do not wear any perfume, deodorant or talcum powder. Bring all available previous films for comparison.
MRI: (BRING ANY IMPLANT INFORMATION TO YOUR APPOINTMENT)If you have a pacemaker, aneursym clips, bio-nerve stimulator, loose metal fragments near spine or eyes, infusion pumps, or are in first trimester of pregnancy, you may not be able to have the MRI exam.
PET SCAN: Nothing to eat or drink for four hours prior to exam.
SERIE GASTROINTESTINAL SUPERIOR, INTESTINO DELGADO, ESOFAGO: Nada de comer o beber despues de la media noche, el dia antes del examen. No desayunar, fumar, o masticar chicle, en la manana de] examen.
ENEMA DE BARIO: Siga las instrucciones de "24" horas, en el estuche de preparacion. Por favor de sequir con cuidado.
CT BIOPSIA GUIADA/Colocación de los puertos MÉDICA:No hay anticoagulantes tres días antes de la cita.
ULTRASONIDO: (ABDOMINAL, HIGADO, VESICULA BILIAR, PANCREAS) Nada de comer o beber por 4 horas antes de! examen.
ULTRASONIDO OBSTETRICO O PELVICO: -- Debe tomar 32 onzas de agua, comenzando I hora antes de su cita. No vacie la vejiga. Una vejiga llena es necesaria
para el examen.
MAMOGRAFIA: -- No use perfume, desodorante, o talco. Traiga todas disponibles mamografias anteriores.
MRI: (LLEVAR LA INFORMACIÓN DE IMPLANTES)-- Si tiene un marcapasos, clips de aneurisma, estimulador bio-nervio, fragmentos de metal cerca de la espina o los ojos,
bombas de infusion, o si esta en el primer trimestre de su embarazo, es posible que no pueda tener un examen de MRI.
PET SCAN: -- Nada de comer o beber por 4 horas antes del examen.
0 0
..
... = =
·;IX
..., 1-215
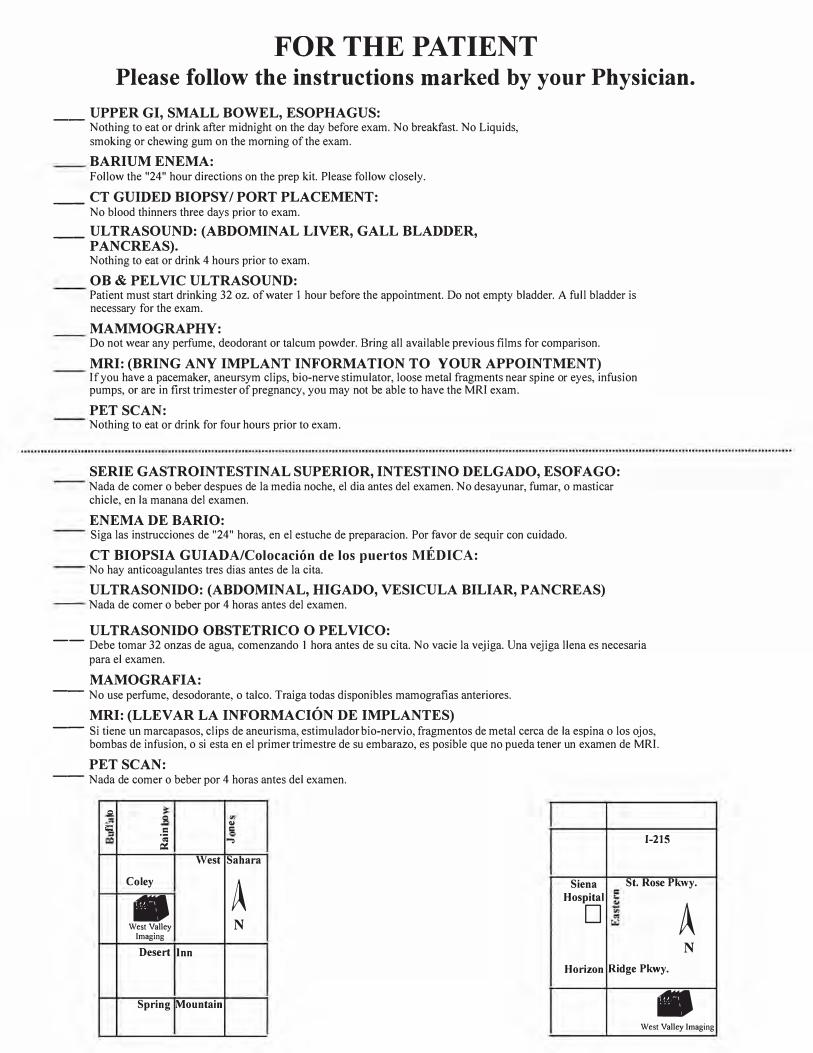
West Sahara
Coley
ASiena St. Rose Pkwy.
• West Valley N
Imaging
Hospital
A D
Desert Inn N
Horizon Ridge Pkwy.
Spring Mountain • West Valley Imaging
~ ~ "' ..c,
= C c=