standardization of heart failure care through a cross-hospital … · 2018-10-08 · heart failure...
TRANSCRIPT

Standardization of Heart Failure Care Through a Cross-Hospital Effort
Matthew Oberhardt, PhD Kelly Axsom, MDKumudha Ramasubbu, MD
October 2, 2018

Disclosures
§ Matt Oberhardt, PhD– None
§ Kelly Axsom, MD– Consultant Abbott
2

3
NewYork-Presbyterian Healthcare System

4
NewYork-Presbyterian Healthcare System

5
NewYork-Presbyterian Healthcare System

Heart Failure is a Syndrome
Complex clinical syndrome due to structural or functional cardiac disorder impairs the ability of heart to fill or pump
The heart is unable to meet metabolic demands leading to symptoms of fatigue, shortness of breath and volume overload

Heart Failure
Incidence Treatments NYHA Class
5-year Survival
A ~65 million pts/year High Risk of HF Prevention none 97%B ~10 million pts/year Asymptomatic Medications NYHA I 96%C ~5 million pts/year Symptomatic Medications
Procedures NYHA I-IV 75%
D ~200,000 pts/year End-Stage Specialized Care NYHA IV 20%Yancy CW, et al. Circulation. 2013;128: e240-e327 .
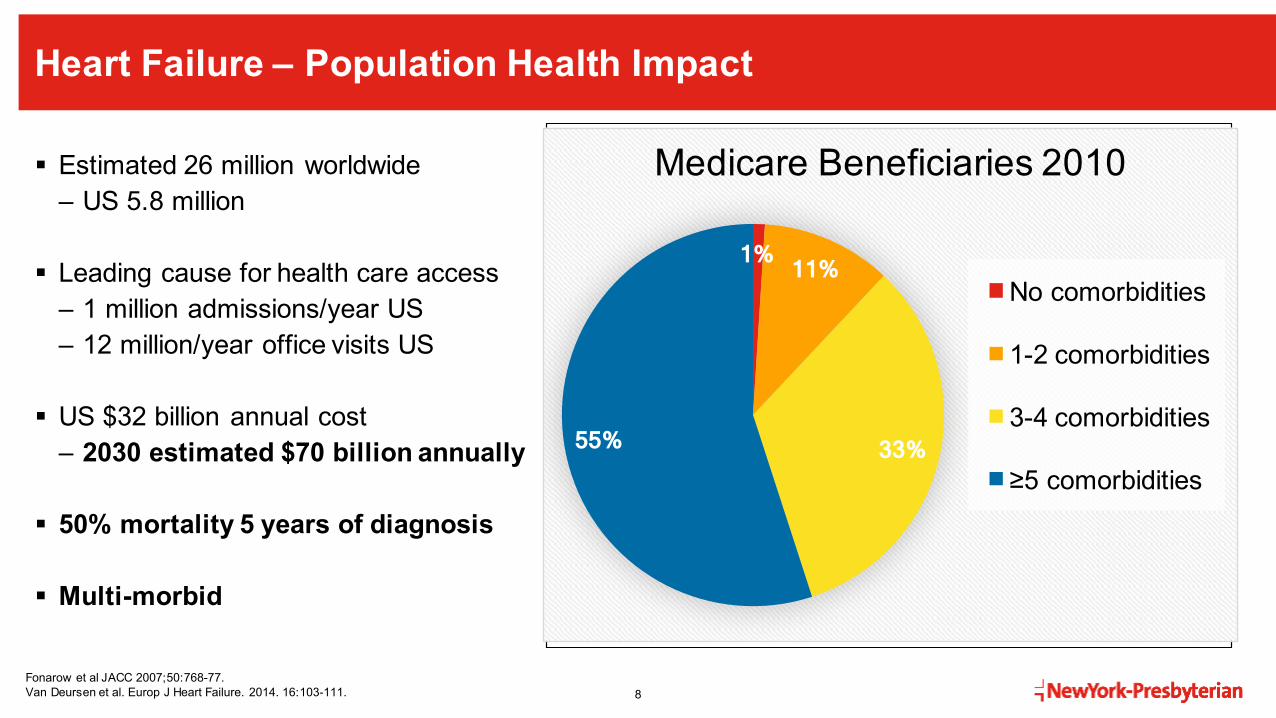
Heart Failure – Population Health Impact
§ Estimated 26 million worldwide– US 5.8 million
§ Leading cause for health care access– 1 million admissions/year US– 12 million/year office visits US
§ US $32 billion annual cost– 2030 estimated $70 billion annually
§ 50% mortality 5 years of diagnosis
§ Multi-morbid
8
0
2
4
6
8
10
12
1991 2000 2037H
eart
Fai
lure
Pat
ient
s in
the
US
(Mill
ions
)
Fonarow et al JACC 2007;50:768-77.Van Deursen et al. Europ J Heart Failure. 2014. 16:103-111.
1% 11%
33% 55%
Medicare Beneficiaries 2010
No comorbidities
1-2 comorbidities
3-4 comorbidities
≥5 comorbidities
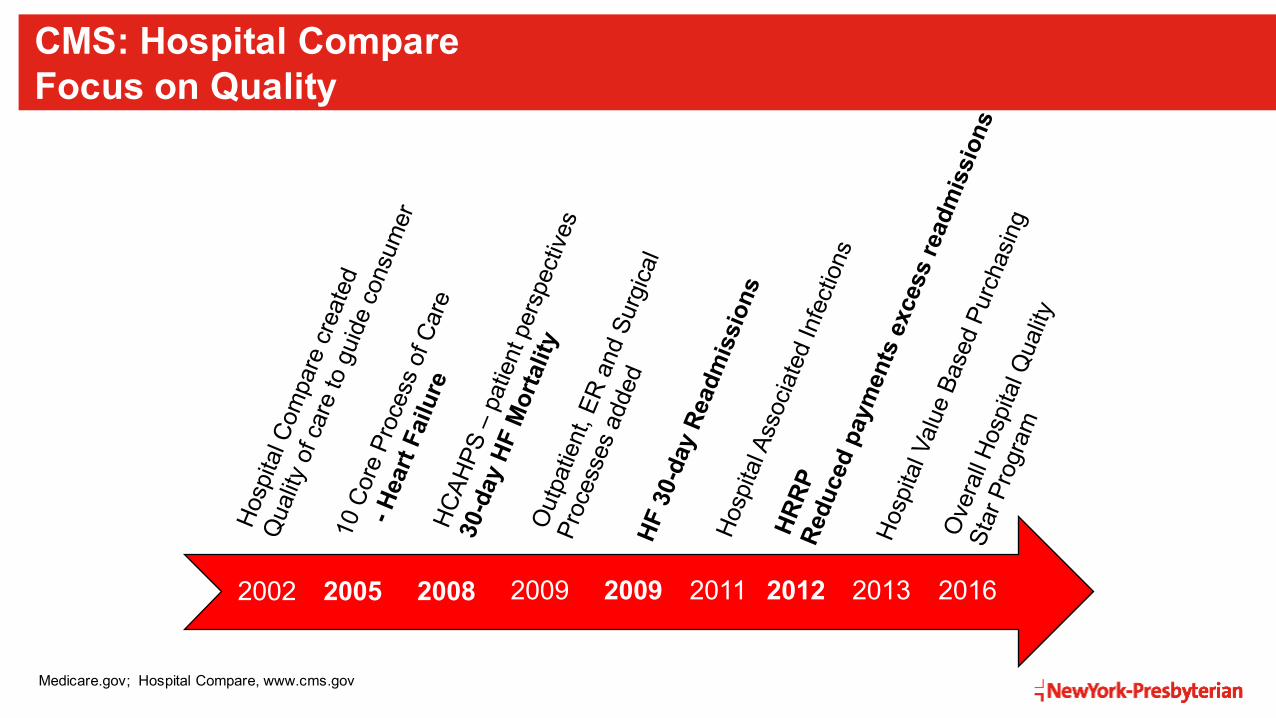
CMS: Hospital Compare Focus on Quality
2002 2005 2008 2009 2009 2011 2012 2013 2016
Medicare.gov; Hospital Compare, www.cms.gov

The Ask
January 2017 Executive Steering Committee• Dr. Corwin (President and Chief Executive Officer) • Dr. Forese (Executive Vice President and Chief Operating Officer)
10
1. Understand heart failure protocols & programs at each of the 8 NYP hospitals2. Develop referral criteria & regional program strategies 3. Develop standards of care for heart failure
à Help patients live longer, live better

The Ask – NewYork-Presbyterian 2018 Kick-Off Goals
11

The Process Improvement Challenge
Clinician engagement
Goals of leadership
Physicians engaged primarily in clinical work don’t think this way

Fee For Service
Large Hospital NetworksHospital Systems as the Insurer
Value Based Care

The Stakeholders
14
Multidisciplinary, clinician-led group Leader: Shunichi Homma, MD CMO, Columbia Faculty Practice Organization
Hospital Based Clinicians Transitions of CareNYPH Support
Weill Cornell§ Dr. Evelyn Horn§ Dr. Maria Karas
Columbia§ Dr. Nick Homma§ Dr. Paolo Colombo§ Dr. Kelly Axsom
Lower Manhattan§ Dr. Yuliya Kats
Allen § Dr. Gerald Neuberg
Queens§ Dr. David Slotwiner§ Dr. Alex Volodarskiy
Lawrence§ Dr. Tony Mercando§ Dr. Douglas Hart
Hudson Valley§ Dr. Howard Tarkin
Methodist§ Dr. Kumudha
Ramasubbu
NYP§ Dr. Deepa Kumaraiah (SL)§ Carolyn Halik (SL)§ Sonia Bandrowski (SL)§ Eileen Kieran (SL)§ Julie Mirkin (CM)§ Matthew Oberhardt (Analytics)§ Denise McLaughlin (Analytics)§ Harry Sherman (Marketing)ACO§ Dr. Paul Casale
ACN§ Claudia Beck
RN and Care Management
§ Caryn Donocoff§ Lena Ileodes§ Jeanette Melchor§ Cathy Halliday§ Deena Schmidt§ Tim McGarvey§ Lisa McIntyre§ Theresa Quarless§ Jenny Li§ Brigid§ Darlene Adaire§ Virgina Bjorton
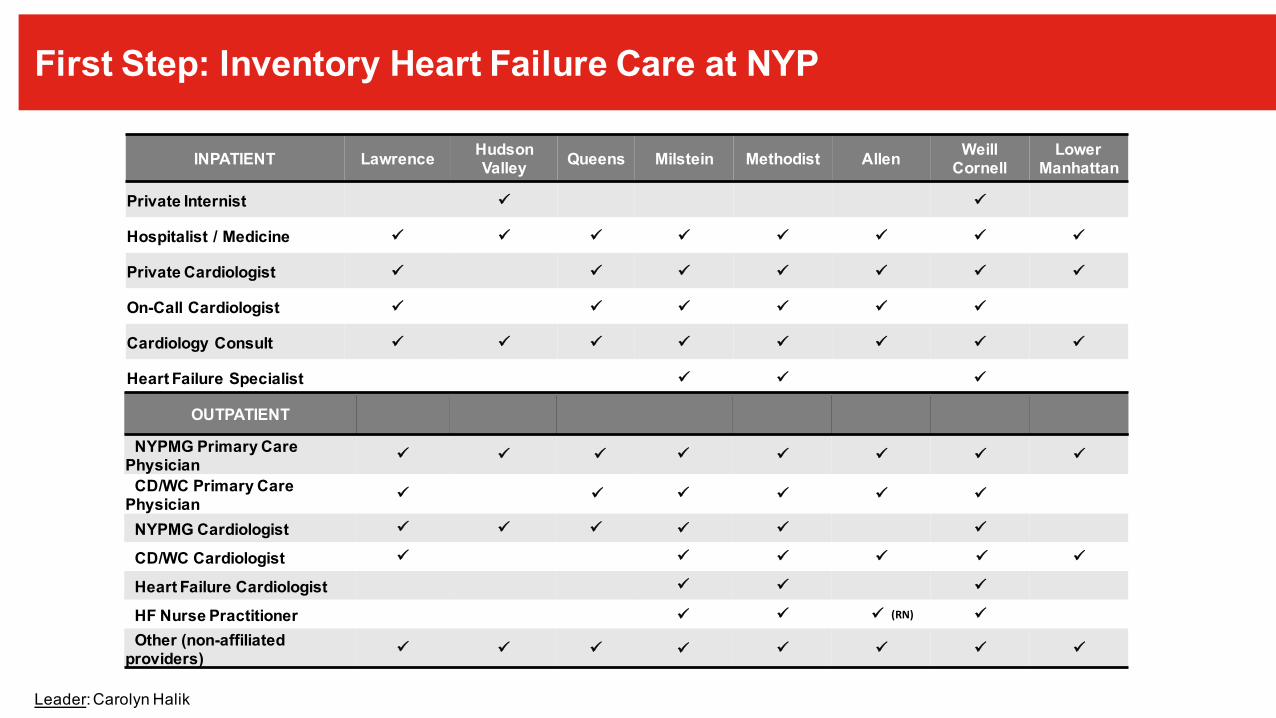
First Step: Inventory Heart Failure Care at NYP
INPATIENT Lawrence HudsonValley Queens Milstein Methodist Allen Weill
CornellLower
Manhattan
Private Internist ü ü
Hospitalist / Medicine ü ü ü ü ü ü ü ü
Private Cardiologist ü ü ü ü ü ü ü
On-Call Cardiologist ü ü ü ü ü ü
Cardiology Consult ü ü ü ü ü ü ü ü
Heart Failure Specialist ü ü ü
HF Discharges (2016 MS DRG) 479 374 711 827 1080 357 640 176OUTPATIENT
NYPMG Primary Care Physician ü ü ü ü ü ü ü ü
CD/WC Primary Care Physician ü ü ü ü ü ü
NYPMG Cardiologist ü ü ü ü ü ü
CD/WC Cardiologist ü ü ü ü ü ü
Heart Failure Cardiologist ü ü ü
HF Nurse Practitioner ü ü ü (RN) ü
Other (non-affiliated providers) ü ü ü ü ü ü ü ü
Leader: Carolyn Halik

Inpatient Guidelines
Website
Dashboard
Regional Support
OutpatientGuidelines
Transitions of Care
NYP HF Standardization
NYP HF Standardization

Creating Clinical GuidelinesIn-PatientTransitions of CareOut-Patient
17

Standardizing Heart Failure: In-Patient Guidelines
§ Core group of 3§ Bigger sub-group of 6§ Weekly calls§ Required hospital-specific feedback
– Physician Leaders– Residents/PA/RN/NPs/Non-Cardiologist– Pharmacy
§ Created 7 cards with identical processes and site specific content
18Committee Leaders: Gerry Neuberg, MD; Kelly Axsom, MD; Eileen Kieran
Aug2017
Jan2017
April2017
Feb2017 Initial draft Final

Initial Draft of Guidelines
19Leaders: Evelyn Horn, MD; Paolo Colombo, MD; Kelly Axsom; MD
AHA Get With The Guidelines DataBetter Survival:- Advanced Heart Failure- Cardiac Surgery - Percutanenous Coronary Interventions
Pandey et al JAMA Cardiol 2018 epub

The Joint Commission:BEST PRACTICES LIBRARY

Standardizing Heart Failure: Transitions of Care
§ Inventory– Practice patterns varied greatly– Some sites without resources
§ Core group of 3 providers § Bigger sub-group of 6§ Weekly calls§ Required feedback and input from committee members
§ Biggest challenge is real-time patient identification
21Committee Co-Chairs: Julie Mirkin, RN, PhD; Kelly Axsom, MD
Aug2018
Jan2017
Nov2017
Jan2018
May2018First meeting Draft 1 Draft 8 Final

Medical Literature: Transitions of Care HOT TOPIC
Jencks et al NEJM 2009;360:1418 Hernandez et al JAMA 2010.303:1716Van Spall et al Eu Heart J. 2017. 19:1427-1443
• 30-Day Readmissions – linked to post discharge visits• 30-day readmission rates are lower if outpatient visit within 7-d of discharge• No outpatient visit within 30-d associated with >50% readmission rate
• Mortality Reduction – Disease Management Clinics and Home Nursing Visits

23Transitions of Care Guideline Committee: Virgina Bjorton RN (Allen), Lena Ileodes RN (NYP); Caryn DonocoffRN (ACO)

Standardizing Heart Failure: Outpatient Guidelines
§ Core group of 3§ Bigger sub-group of 6§ Twice monthly calls§ Individual hospital feedback
– Physician – Outpatient providers– PA/Residents/Internal Medicine
§ Currently defining dissemination process
Committee: Gerry Neuberg, MD; Kelly Axsom, MD; Kumudha Ramasubbu MD; Paolo Colombo; MD; Evelyn Horn, MD; Eileen Kieran
24
Oct2018
Jan2017
March2018
April2018First meeting Draft 1 Final

25IN PROGRESS
Roll Out Planned for Oct 2018

Weill Cornell Columbia Lawrence
Hudson ValleyLMH Queens Brooklyn
MethodistThe Allen Hospital
Evelyn Horn, MD & Maria
Karas, MD
Paolo Colombo, MD & Kelly Axsom, MD
Tony Mercando,
MD and Douglas Hart, MD
Howie Tarkin, MD
Yuliya Kats, MD
David Slotwiner,
MD
Kumudha Ramasubbu,
MD
Gerald Neuberg,
MD
David Ramos Group
Mel Weiss Group
Warren Rosenblum, MDAinat Beniaminovitz, MD
Columbia Doctors
Change Management – Can Be Difficult
Distribution & Communication
Success measured by - Frequency of request of materials and updates- Dashboard measurements

Building a Heart Failure Dashboard
27Leaders: Matthew Oberhardt, PhD, Denise Mclaughlin, , Natalia Goldenberg
Designing a Heart Failure Dashboard
28
• Incorporate metrics the clinicians identify
• Design tool that is sufficiently flexible, specific, and powerful
• Negotiate between feasibility (the ‘wish list’) and practicality• Our data is siloed and not always consistent!

Designing a Heart Failure Dashboard
• Incorporate metrics the clinicians identify
• Design tool that is sufficiently flexible, specific, and powerful
• Negotiate between feasibility (the ‘wish list’) and practicality• Our data is siloed and not always consistent!
Ø Drugs upon discharge• beta blockers?• ACEI/ARB/ARNI?
Ø Follow-up visit within 10 days?Ø 30-day post-discharge Mortality?Ø 30-day readmission to any facility?
Records inconsistent in EHR…
Data not available
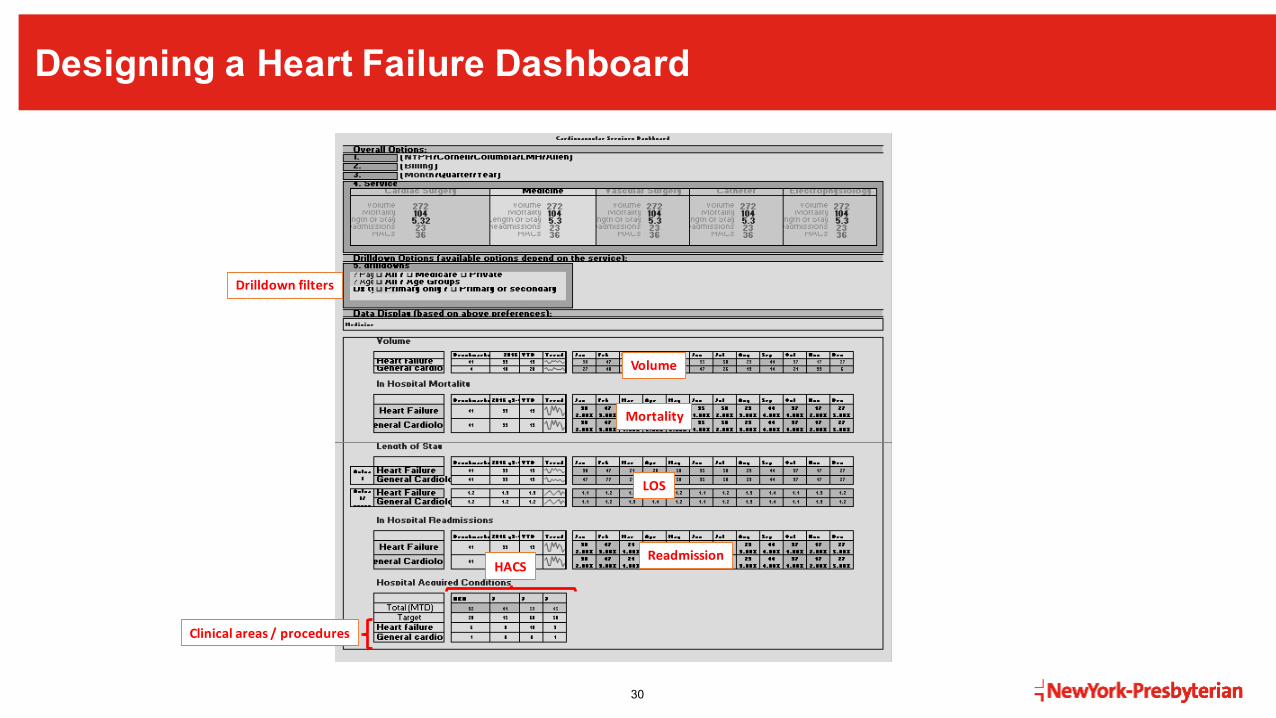
Designing a Heart Failure Dashboard
30
Volume
Mortality
LOS
ReadmissionHACS
Clinicalareas/procedures
Drilldownfilters

Designing a Heart Failure Dashboard
31
Includes:
• Filters• Volume• Mortality• 30-day readmission, HF• 30-day readmission, all • 60-day readmission, all• Associated diagnoses:
o Ventricular tachycardiao Demand ischemiao Myocardial infarctiono Atrial fibrillation/flutter
• Follow-up appointment• MRNs of selected patients

Designing a Heart Failure Dashboard
32
Includes:
• Filters• Volume• Mortality• 30-day readmission, HF• 30-day readmission, all • 60-day readmission, all• Associated diagnoses:
o Ventricular tachycardiao Demand ischemiao Myocardial infarctiono Atrial fibrillation/flutter
• Follow-up appointment• MRNs of selected patients
Heart Failure patients broken into 6 categories:• HF – all• HFrEF• HFpEF• EF unspecified• Cardiogenic shock• HF with pulmonary hypertension

Designing a Heart Failure Dashboard
33
Includes:
• Filters• Volume• Mortality• 30-day readmission, HF• 30-day readmission, all • 60-day readmission, all• Associated diagnoses:
o Ventricular tachycardiao Demand ischemiao Myocardial infarctiono Atrial fibrillation/flutter
• Follow-up appointment• MRNs of selected patients

Validation
• During construction: vet each ICD code & clinical element with clinicians
• Internal validations of dashboard by unit tests
• Validation against Vizient data
• Validation by clinician chart review

Validation
Automated?
• During construction: vet each ICD code & clinical element with clinicians
• Internal validations of dashboard by unit tests
• Validation against Vizient data
• Validation by clinician chart review
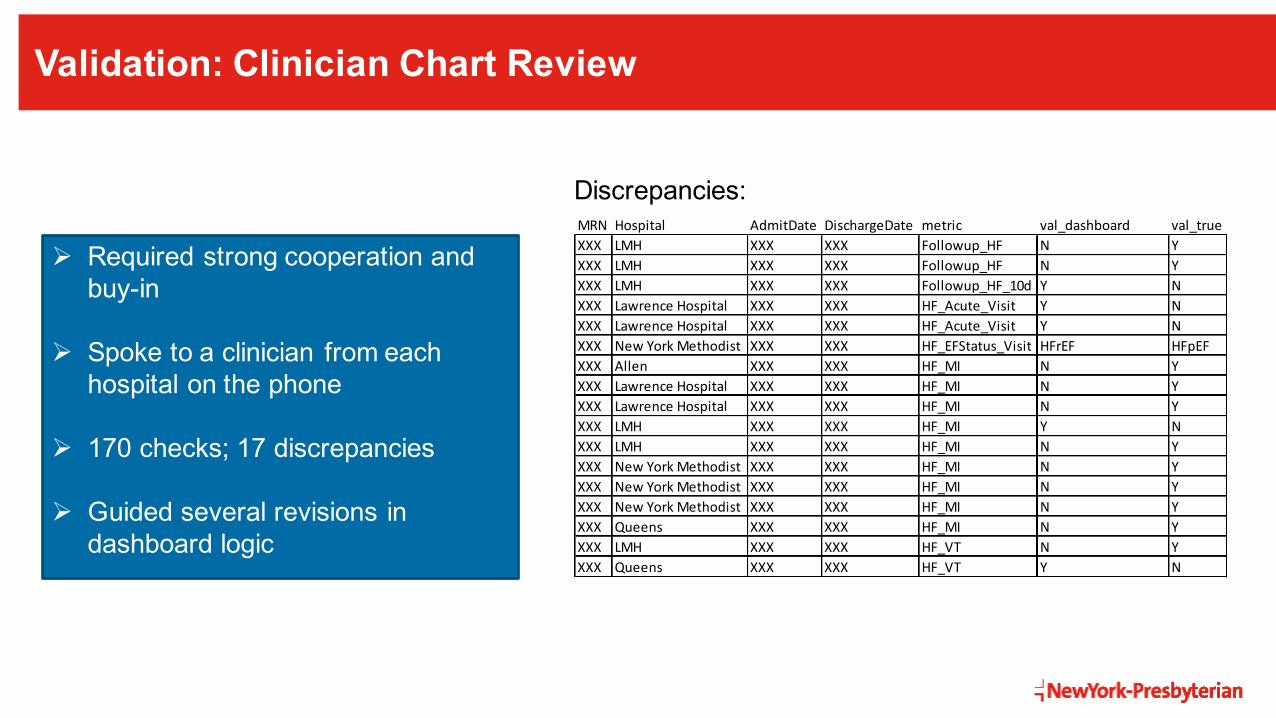
Validation: Clinician Chart Review
Ø Required strong cooperation and buy-in
Ø Spoke to a clinician from each hospital on the phone
Ø 170 checks; 17 discrepancies
Ø Guided several revisions in dashboard logic
MRN Hospital AdmitDate DischargeDate metric val_dashboard val_trueXXX LMH XXX XXX Followup_HF N YXXX LMH XXX XXX Followup_HF N YXXX LMH XXX XXX Followup_HF_10d Y NXXX LawrenceHospital XXX XXX HF_Acute_Visit Y NXXX LawrenceHospital XXX XXX HF_Acute_Visit Y NXXX NewYorkMethodist XXX XXX HF_EFStatus_Visit HFrEF HFpEFXXX Allen XXX XXX HF_MI N YXXX LawrenceHospital XXX XXX HF_MI N YXXX LawrenceHospital XXX XXX HF_MI N YXXX LMH XXX XXX HF_MI Y NXXX LMH XXX XXX HF_MI N YXXX NewYorkMethodist XXX XXX HF_MI N YXXX NewYorkMethodist XXX XXX HF_MI N YXXX NewYorkMethodist XXX XXX HF_MI N YXXX Queens XXX XXX HF_MI N YXXX LMH XXX XXX HF_VT N YXXX Queens XXX XXX HF_VT Y N
Discrepancies:
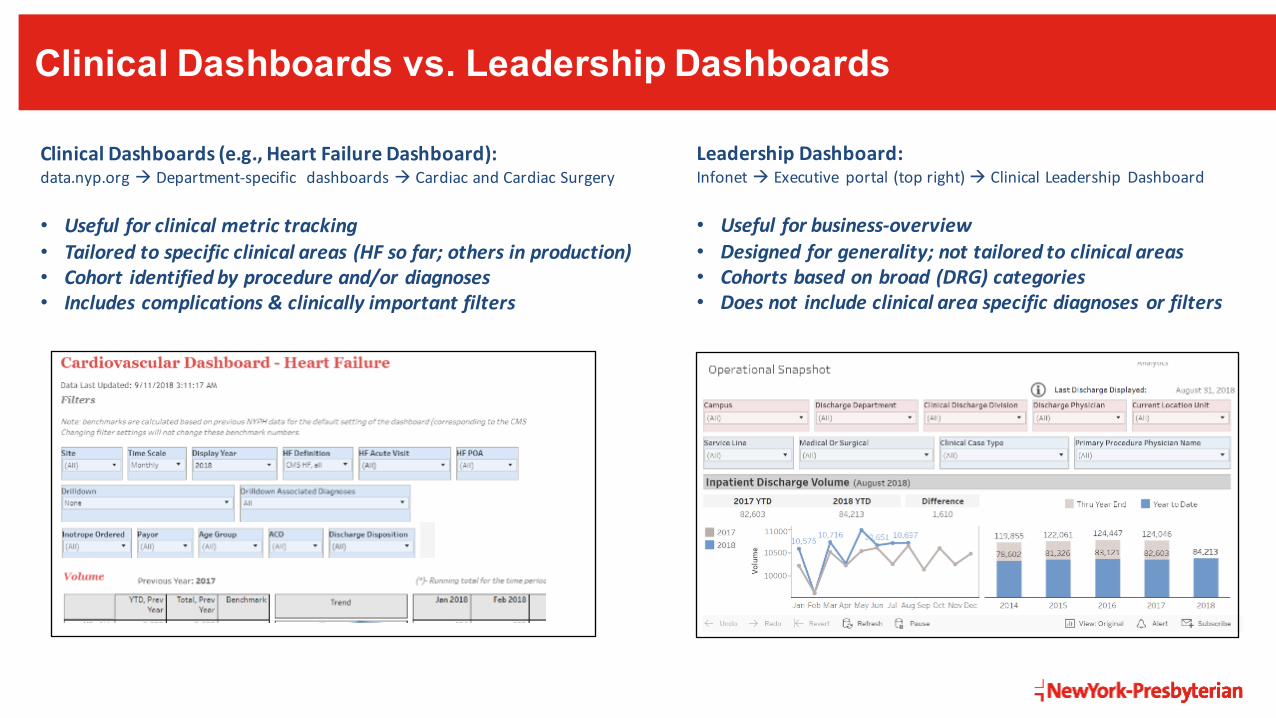
Clinical Dashboards vs. Leadership Dashboards
LeadershipDashboard:Infonet à Executive portal(topright)à ClinicalLeadership Dashboard
• Usefulforbusiness-overview• Designedforgenerality;nottailoredtoclinicalareas• Cohortsbasedonbroad(DRG)categories• Doesnot includeclinicalareaspecificdiagnoses orfilters
ClinicalDashboards(e.g.,HeartFailureDashboard):data.nyp.orgà Department-specific dashboardsà CardiacandCardiacSurgery
• Usefulforclinicalmetrictracking• Tailoredtospecificclinicalareas(HFsofar;othersinproduction)• Cohort identifiedbyprocedureand/ordiagnoses• Includescomplications&clinicallyimportantfilters

Determining Acuity
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter

Determining Acuity
…………………………………. ……………………………………….….
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes

Determining Acuity
The three-combination codes that include heart failure also require additional coding from the I50 series to specify the type and acuity of the failure…
https://www.aafp.org/fpm/2014/0300/p5.htmlHow to Document and Code for Hypertensive Diseases in ICD-10 -- FPMwww.aafp.org
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes

Determining Acuity
The three-combination codes that include heart failure also require additional coding from the I50 series to specify the type and acuity of the failure…
https://www.aafp.org/fpm/2014/0300/p5.htmlHow to Document and Code for Hypertensive Diseases in ICD-10 -- FPMwww.aafp.org
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes

Determining Acuity
IsitacuteHF?(clinician
assessment)
minrankforacuteHFcode
minrankforany HFcode CMS-definedHF DRG-definedHF
yes 1 1 1 0yes 2 1 1 1yes 4 1 1 1yes 5 1 1 0yes 6 1 1 1yes 7 1 1 0yes 2 2 0 0yes 2 2 0 0yes 2 2 0 0yes 2 2 0 0yes 2 2 0 0yes 2 2 0 0yes 2 2 0 0yes 3 3 0 0yes 3 3 0 0yes 3 3 0 0no 1 1 1 1no 1 1 1 0no 2 1 1 1no 2 1 1 1no 2 1 1 1no 2 1 1 1no 2 1 1 1no 2 1 1 0no 6 1 1 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 2 2 0 0no 3 3 0 0no 3 3 0 0no 3 3 0 0no 3 3 0 0no 3 3 0 0
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes
• Broader analysis showed no clear predictor of clinician defined ‘acute HF’

Determining Acuity
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes
• Broader analysis showed no clear predictor of clinician defined ‘acute HF’
• Current solution: offer multiple definitions of HF + remove ‘primary Dx is acute’ filter

Determining Acuity
• Noticed (incorrect!) drop 2016à2017 when applying ‘primary Dx is acute’ filter
• Coding switched from acuity specific to acuity unspecified codes
• Broader analysis showed no clear predictor of clinician defined ‘acute HF’
• Current solution: offer multiple definitions of HF + remove ‘primary Dx is acute’ filter
Need to better align clinician + coding + quality assessment worlds!
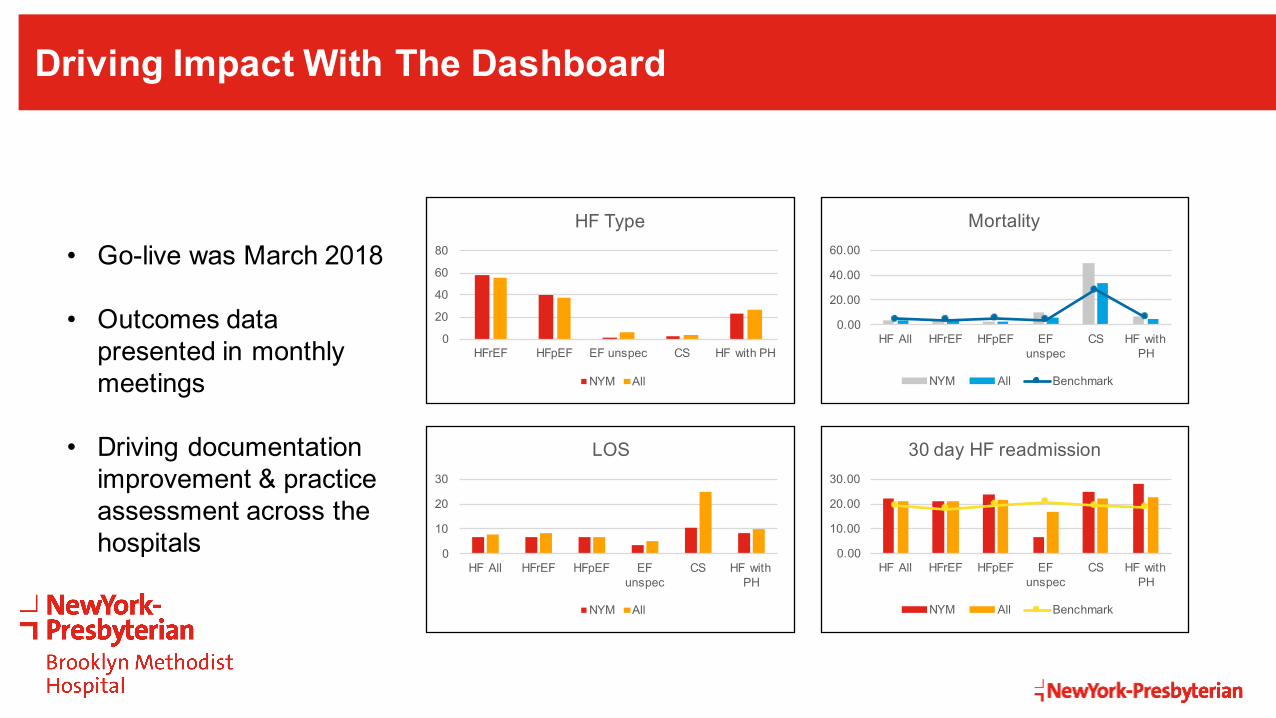
Driving Impact With The Dashboard
0
20
40
60
80
HFrEF HFpEF EF unspec CS HF with PH
HF Type
NYM All
0.00
20.00
40.00
60.00
HF All HFrEF HFpEF EF unspec
CS HF with PH
Mortality
NYM All Benchmark
0
10
20
30
HF All HFrEF HFpEF EF unspec
CS HF with PH
LOS
NYM All
0.00
10.00
20.00
30.00
HF All HFrEF HFpEF EF unspec
CS HF with PH
30 day HF readmission
NYM All Benchmark
• Go-live was March 2018
• Outcomes data presented in monthly meetings
• Driving documentation improvement & practice assessment across the hospitals
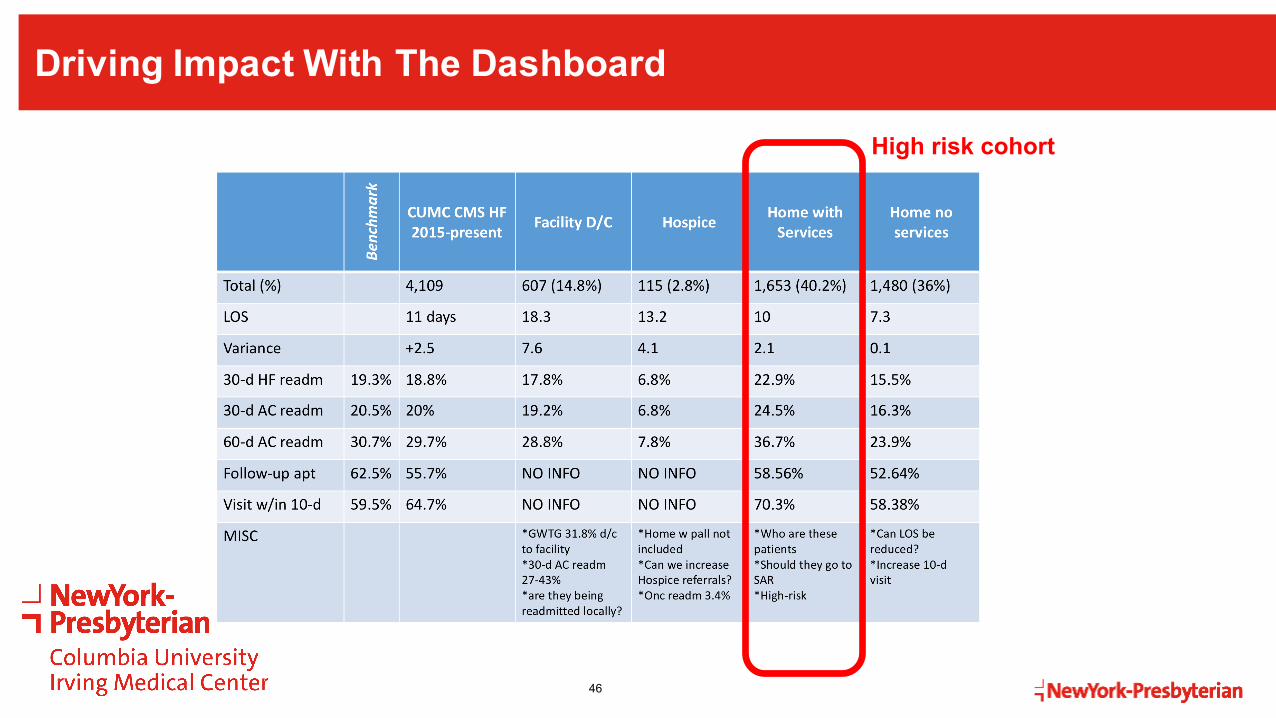
Driving Impact With The Dashboard
46
High risk cohort

Driving Impact With The Dashboard
47
High risk cohort
What can we do to prevent readmissions?
Driving Impact With The Dashboard
“We’ve come to depend upon the dashboard and particularly the ability itgives us to drill down to the individual patient level data. We have a multidisciplinaryteam that reviews the dashboard data – and we use the dashboard toidentify patients who fall out of the metrics. We then reviewthe chart to determine what could have been done moreeffectively. In addition, based upon our early findings through this process we haveinstituted a daily communication between our coding anddocumentation team and our CHF NP to determine if patients are beingcorrectly identified as having CHF. Prior to this practice we were finding many patientsbeing incorrectly labeled with CHF, and this was hurting our metrics.”
- David Slotwiner, MDDivision Chief of Cardiology,NewYork-Presbyterian Queens Hospital

Part of a Larger Cardiovascular Regionalization Effort
49
Electrophysiology
Cath lab
Heart Failure
CT surgery
Vascular
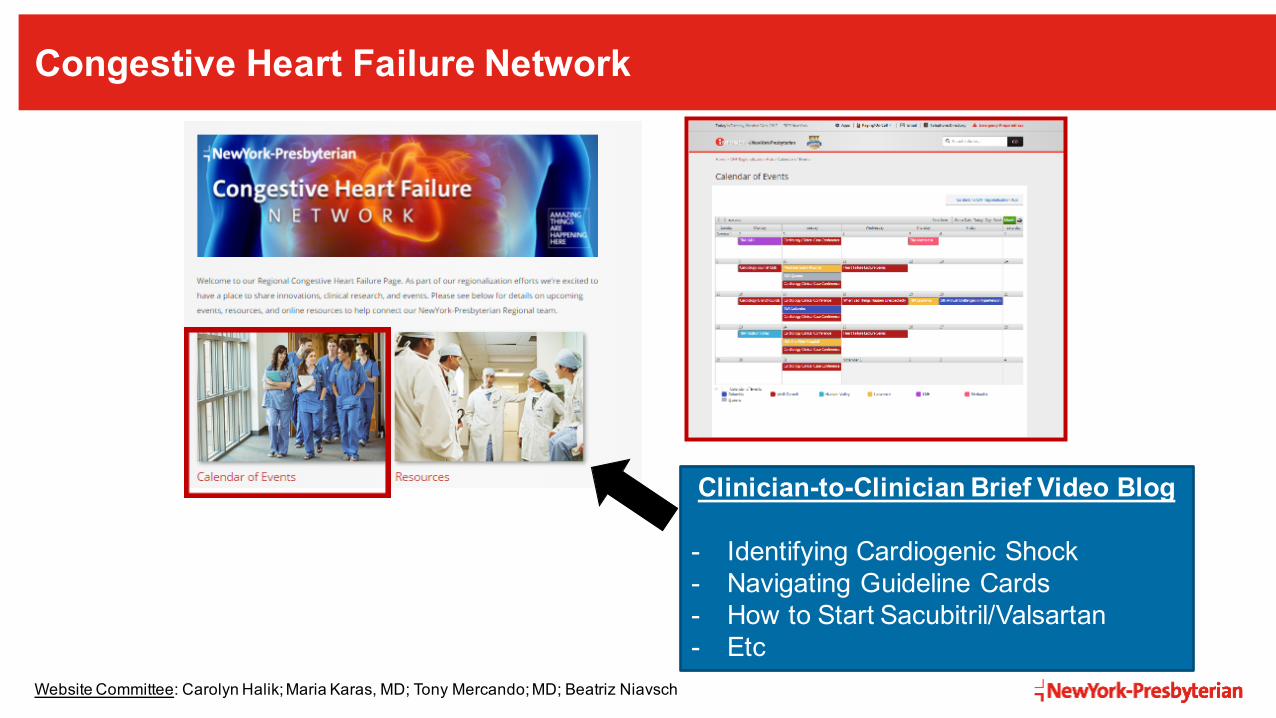
Congestive Heart Failure Network
50
Clinician-to-Clinician Brief Video Blog
- Identifying Cardiogenic Shock- Navigating Guideline Cards- How to Start Sacubitril/Valsartan- Etc
Website Committee: Carolyn Halik; Maria Karas, MD; Tony Mercando; MD; Beatriz Niavsch
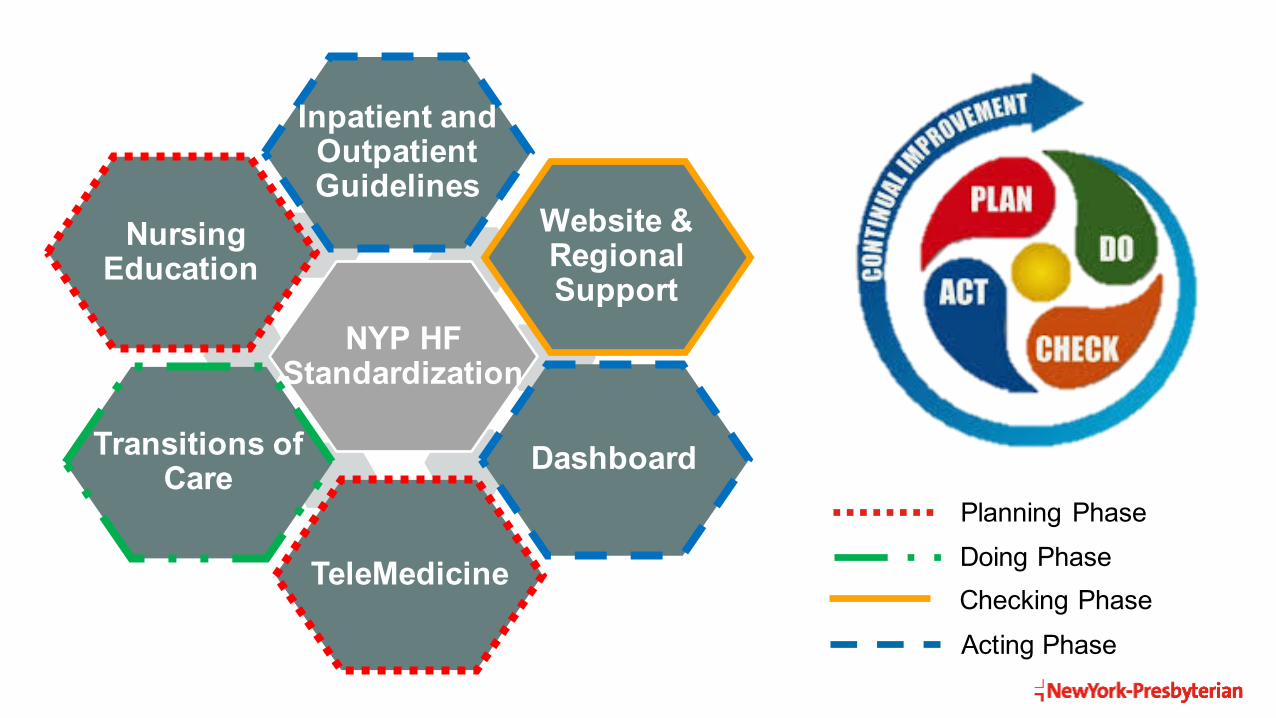
Inpatient and OutpatientGuidelines
Website &Regional Support
Dashboard
TeleMedicine
Nursing Education
Transitions of Care
NYP HF Standardization
Planning Phase
Acting PhaseChecking PhaseDoing Phase

Applying Technology Advances to Standardization
52
Heart Failure Guidelines

PerspectivesHub and Spoke
53Modify with Insert > Header & Footer

NewYork-Presbyterian 2018 Goals
54
ü Standardize– Guideline creation, next steps
revisionü Regionalize- Sharing ideas, sharing patients,
working together
ü Engagement– Key to Success– Focus on helping patients
“Live Longer, Live Better”

Virtualize – To Do’s
q Cross Campus NEW EMR – Incorporation of standards during
creation of NYP EMR
q Remote Disease Management– Sharing Protocols – Cross-Campus
Initiatives– Para-telemedicine Pilot– ”Wearables” and ”Implantables”
55
The Process Improvement Challenge
Clinician engagement
Goals of leadership
Physicians engaged primarily in clinical work don’t think this way
Physicians engaged primarily in clinical work and
given the right tools follow this
process

57
Thank You
58