spotorno hip stem
TRANSCRIPT
Nature as Model
CLS® Spotorno®
Hip Stem
Surgical Technique

Disclaimer This document is intended exclusively for experts in the field, i.e. physicians in particular, and is expressly not for the information of laypersons.The information on the products and/or procedures contained in this document is of a general nature and does notrepresent medical advice or recommendations. Since this information does not constitute any diagnostic or therapeuticstatement with regard to any individual medical case, individual examination and advising of the respective patientare absolutely necessary and are not replaced by this document in whole or in part.The information contained in this document was gathered and compiled by medical experts and qualified Zimmeremployees to the best of their knowledge. The greatest care was taken to ensure the accuracy and ease of understanding of the information used and presented. Zimmer does not assume any liability, however, for the up-to-dateness, accuracy, completeness or quality of the information and excludes any liability for tangible or intangible losses that maybe caused by the use of this information.In the event that this document could be construed as an offer at any time, such offer shall not be binding in any eventand shall require subsequent confirmation in writing.
Surgical Technique CLS Spotorno Stem
Developed in cooperation with
Prof. Lorenzo SpotornoFinale Ligure, It
Table of Contents
CLS Spotorno Stem 4
Indications for the CLS Spotorno Stem 5
Preoperative Planning 10
Surgical Technique 12
Case Study 21
Ordering Information 22
3CLS Spotorno Hip Stem
4 CLS Spotorno Hip Stem
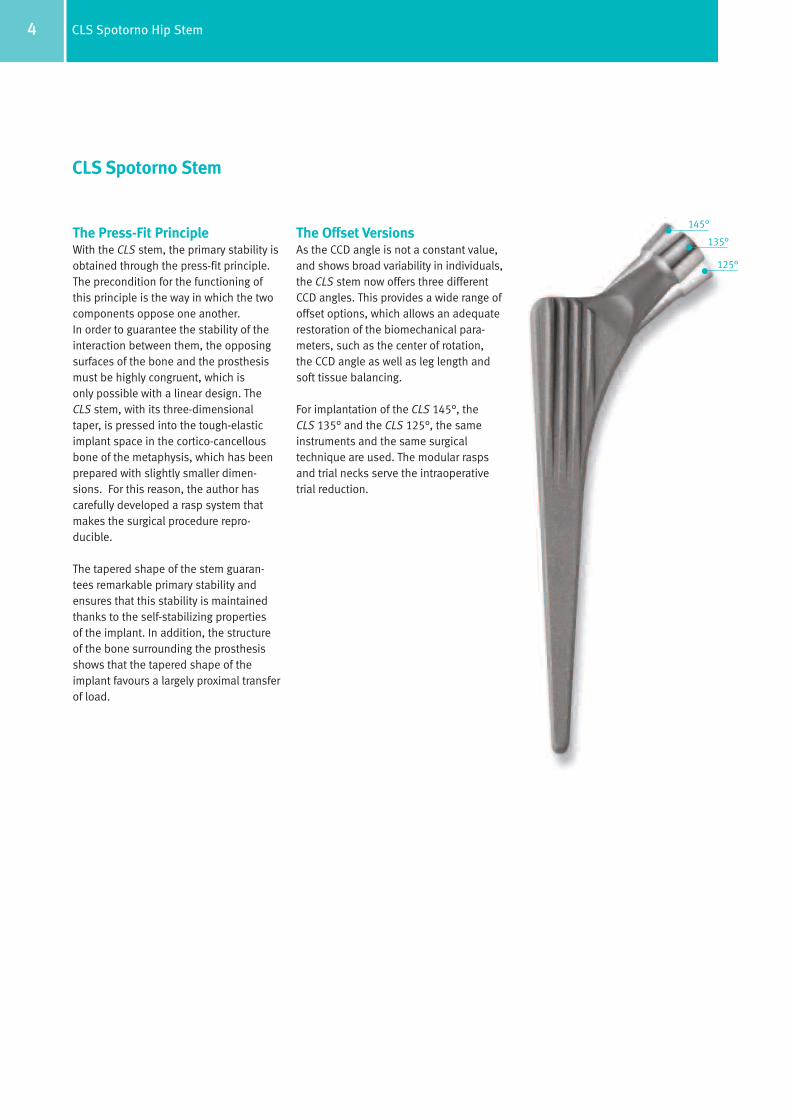
The Press-Fit PrincipleWith the CLS stem, the primary stability isobtained through the press-fit principle. The precondition for the functioning ofthis principle is the way in which the two components oppose one another. In order to guarantee the stability of the interaction between them, the opposing surfaces of the bone and the prosthesismust be highly congruent, which isonly possible with a linear design. The CLS stem, with its three-dimensionaltaper, is pressed into the tough-elasticimplant space in the cortico-cancellousbone of the metaphysis, which has beenprepared with slightly smaller dimen-sions. For this reason, the author hascarefully developed a rasp system thatmakes the surgical procedure repro-ducible.
The tapered shape of the stem guaran-tees remarkable primary stability and ensures that this stability is maintained thanks to the self-stabilizing propertiesof the implant. In addition, the structureof the bone surrounding the prosthesisshows that the tapered shape of the implant favours a largely proximal transfer of load.
The Offset VersionsAs the CCD angle is not a constant value,and shows broad variability in individuals,the CLS stem now offers three differentCCD angles. This provides a wide range ofoffset options, which allows an adequaterestoration of the biomechanical para-meters, such as the center of rotation, the CCD angle as well as leg length andsoft tissue balancing.
For implantation of the CLS 145°, the CLS 135° and the CLS 125°, the same instruments and the same surgicaltechnique are used. The modular raspsand trial necks serve the intraoperativetrial reduction.
CLS Spotorno Stem
145°
135°
125°

5CLS Spotorno Hip Stem
The Question: Cemented or Uncemented?The decision between a cemented andan uncemented hip stem is a choice thatmust be made by the surgeon. Based onthe personal experience by the designingsurgeon implanting over 9,000 CLSstems, it was possible to carry outextensive research into the indicationsfor this stem as well as to define itslimitations.
Indications for the CLS Spotorno StemA Guideline by Prof. Lorenzo Spotorno
The results obtained with the CLS stemsince 1984 are extremely encouraging.For a number of years, we have seen a broadening of the range of indicationsin favour of uncemented stems, both inprimary and revision surgery. Even thoughexcellent results have been achieved(even under critical conditions), it is stillrecommended that surgeons use a setof standard, reliable criteria to help makethe decision between cemented anduncemented stems.

6 CLS Spotorno Hip Stem
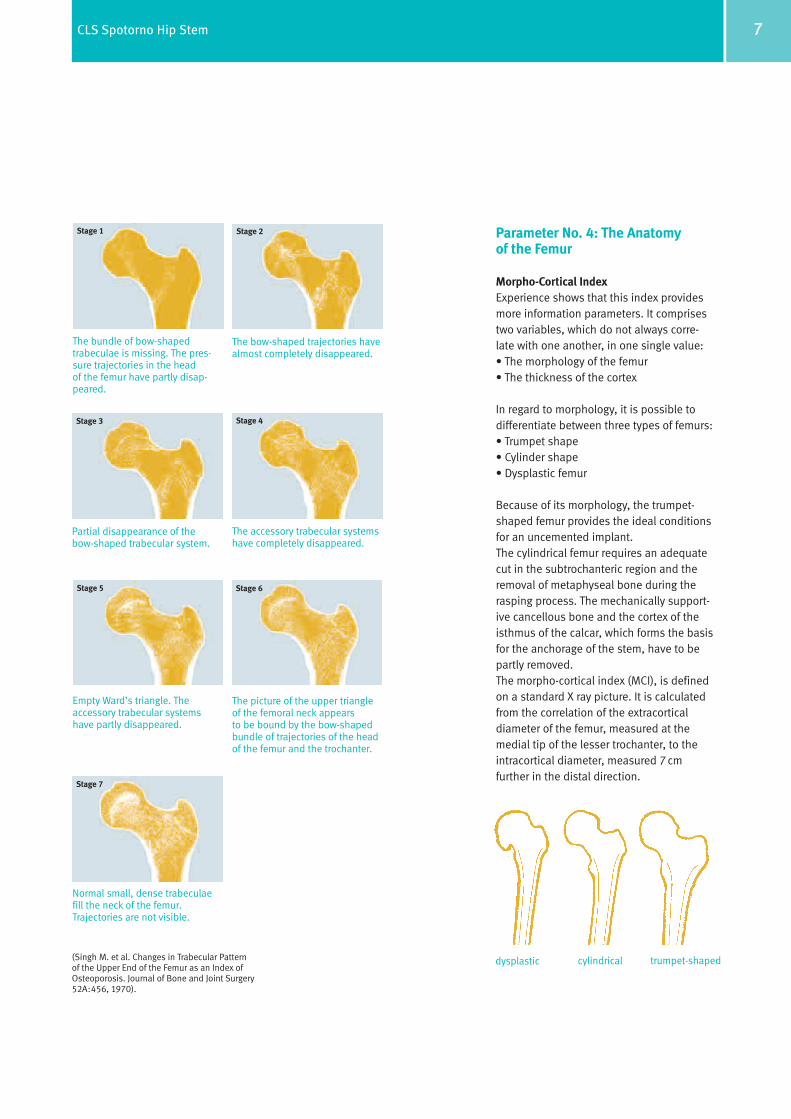
Parameter No. 3: OsteoporosisSevere osteoporosis represents a majordisadvantage in regard to the primarystability of the implant, or requires the use of an over-dimensioned stem with anchorage in the lower metaphysealand diaphyseal region. This, in turn, hasa negative effect on the blood supplyto the bone. Radiological methods such as computer tomography and densio-metry are available for the assessmentof the severity of the osteoporosis. A suitable method for a conclusive assessment is the modified analysisof the trabeculae in the neck of the femur according to Singh – a processthat is easy to carry out.
Femoral Neck IndexOn the basis of these assessments, four degrees of severity of osteoporosiscan be defined:
Severe (Singh 1–2): 4 points
Moderate (Singh 3–4): 2 points
Slight (Singh 5–6): 1 point
Physiological (Singh 7): 0 points
(Singh M. et al. Changes in Trabecular Patternof the Upper End of the Femur as an Indexof Osteoporosis. Journal of Bone and JointSurgery 52A: 456, 1970).
Parameter No. 1: AgeAs far as skeletal changes are con-cerned, it is generally known that age cannot be considered as a purelychronological parameter, but has to beassessed from a biological point of view.In simple terms, it can be said that forpatients under the age of 50 years, acementless stem is the routine solution,while after the age of 70, a cemented stem is generally preferred.
Points Allocated
>70 years: 4 points
61–70 years: 2 points
51–60 years: 1 point
<50 years: 0 points
Parameter No. 2: GenderDue to the increasing osteoporosisresulting from the hormonal changesoccurring during menopause, older women generally have poorer bone quality.
Points Allocated
Women: 1 point
Men: 0 points
In 1985, an indication protocol wasestablished that is based on the assess-ment of four clinical and radiologicalparameters in the patient investigated.Each parameter is given a point score.The final value obtained from the sum ofthe points establishes the indication and thus, provides a valuable guidelinefor the surgeon. The parameters are age,gender, severity of the osteoporosis andthe anatomical characteristics of thefemur.
Reliable Decision-Making Through Methodology
7CLS Spotorno Hip Stem
The bundle of bow-shaped trabeculae is missing. The pres-sure trajectories in the head of the femur have partly disap-peared.
The bow-shaped trajectories havealmost completely disappeared.
Partial disappearance of the bow-shaped trabecular system.
The accessory trabecular systemshave completely disappeared.
Empty Ward’s triangle. The accessory trabecular systemshave partly disappeared.
The picture of the upper triangleof the femoral neck appearsto be bound by the bow-shapedbundle of trajectories of the headof the femur and the trochanter.
Normal small, dense trabeculaefill the neck of the femur.Trajectories are not visible.
Stage 1 Stage 2
Stage 3 Stage 4
Stage 5
Stage 7
Stage 6
Parameter No. 4: The Anatomyof the Femur
Morpho-Cortical IndexExperience shows that this index providesmore information parameters. It comprisestwo variables, which do not always corre-late with one another, in one single value:• The morphology of the femur• The thickness of the cortex
In regard to morphology, it is possible todifferentiate between three types of femurs: • Trumpet shape• Cylinder shape• Dysplastic femur
Because of its morphology, the trumpet-shaped femur provides the ideal conditionsfor an uncemented implant. The cylindrical femur requires an adequatecut in the subtrochanteric region and theremoval of metaphyseal bone during therasping process. The mechanically support-ive cancellous bone and the cortex of theisthmus of the calcar, which forms the basisfor the anchorage of the stem, have to be partly removed.The morpho-cortical index (MCI), is definedon a standard X ray picture. It is calculatedfrom the correlation of the extracorticaldiameter of the femur, measured at themedial tip of the lesser trochanter, to theintracortical diameter, measured 7 cm further in the distal direction.
trumpet-shapedcylindricaldysplastic(Singh M. et al. Changes in Trabecular Pattern of the Upper End of the Femur as an Index ofOsteoporosis. Journal of Bone and Joint Surgery52A:456, 1970).
8 CLS Spotorno Hip Stem
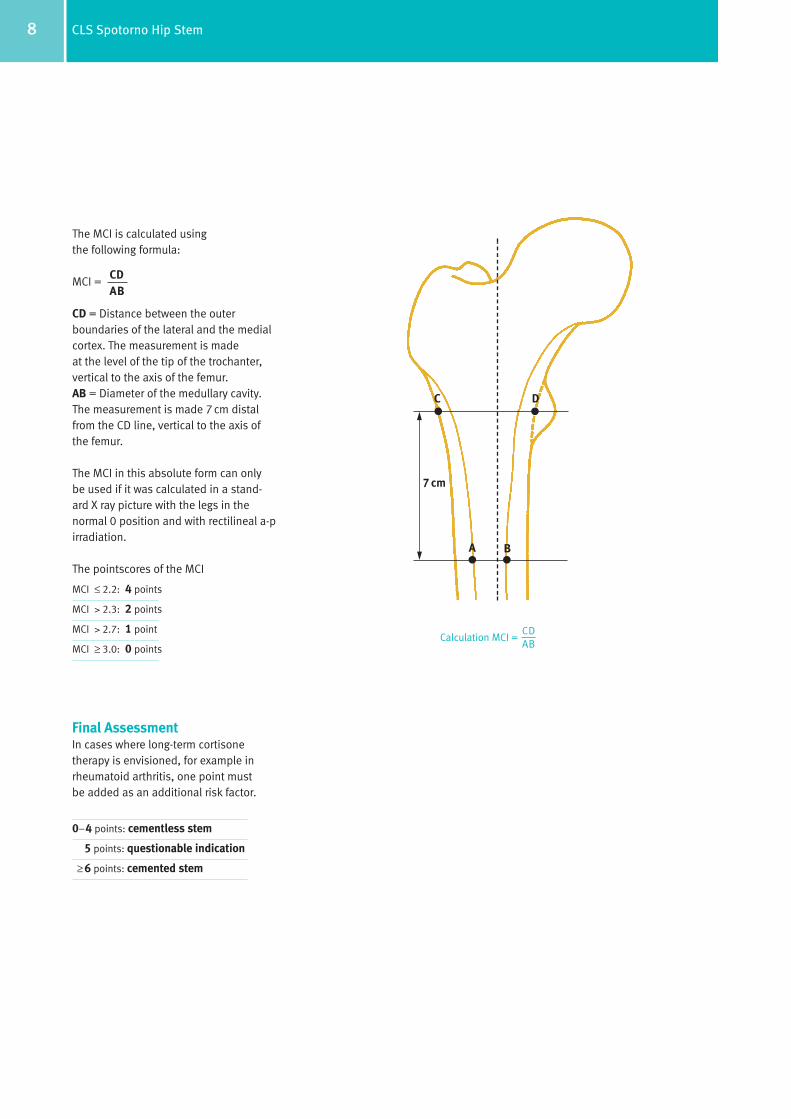
The MCI is calculated using the following formula:
MCI =
CD = Distance between the outer boundaries of the lateral and the medialcortex. The measurement is made at the level of the tip of the trochanter, vertical to the axis of the femur.AB = Diameter of the medullary cavity. The measurement is made 7 cm distalfrom the CD line, vertical to the axis ofthe femur.
The MCI in this absolute form can onlybe used if it was calculated in a stand-ard X ray picture with the legs in the normal 0 position and with rectilineal a-p irradiation.
The pointscores of the MCI
MCI ≤ 2.2: 4 points
MCI > 2.3: 2 points
MCI > 2.7: 1 point
MCI ≥ 3.0: 0 points
Final AssessmentIn cases where long-term cortisone therapy is envisioned, for example in rheumatoid arthritis, one point mustbe added as an additional risk factor.
0–4 points: cementless stem
5 points: questionable indication
≥ 6 points: cemented stem
CDAB
C D
A B
7 cm
CDCalculation MCI =
AB

9CLS Spotorno Hip Stem
The uncemented stem in general, and the CLS stem in particular, have definiti-vely proven their worth. In comparisonwith the cemented stem, the uncementedsolution is far more bone conserving. This becomes an important factor if revi-sion surgery is necessary.
The insertion of the uncemented stem isless invasive and takes the biomechanicsof the femur into account. The bone andthe prosthesis combine to form a unit. As a result, the blood supply and vitalityof the bone are maintained.
In principle, the uncemented stem ispreferably used in younger patients. It is, however, not contraindicated in theelderly – especially for patients in poorgeneral health. It can be implanted morerapidly and there is no thermal damage to the tissue due to the cement.
The use of a cemented stem is never-theless justified in elderly patients for a number of reasons: The life expectancy of the patient is oftenshorter than the average survival time of a cemented stem. In the presence ofpoor bone quality, the cement allowsunproblematic correction of defects. Withcementing, faster restoration of the abilityto walk is also to be expected, since – at least within certain limits – it does notinvolve the reparative phase, which, inthe case of the cementless stem, leads tothe definitive anchorage of the bone.Finally, the economic factor plays a rolethat is not to be underestimated.
It can generally be said that if one adheresto the classical indications – while stillallowing the possibility of further indica-tions in the future – good and very goodresults can be obtained. In this respect,the use of the MCI is of fundamentalimportance because it follows the basicbiomechanical ideas used in the designof the CLS prosthesis. It has been proventhat the CLS can be readily combinedwith the trumpet-shaped femur. In contrast, with a cylindrical medullarycavity, it is normally necessary to use amore invasive prosthesis, which has anunfavourable bone-prosthesis interaction.
Comparison has shown that the MCI and the cortical index (CI) after Gruen aregood indicators for the quality of thebone. There seems to be a connectionboth between the CI and the MCI andbetween the MCI and the measurementof the mineral content of the bone bythe Dexa method.
Conclusion: There is a Broad Indication for Uncemented Anchorage
10 CLS Spotorno Hip Stem
Determination of the Size andPosition of the CupThe center of rotation of the joint to beoperated on is determined by transposingthe two lines that have been drawn on the opposite side. The cup template is then placed on the side that is to beoperated on. The position of the acetabu-lar components is determined by the outline of the cup, the center of rotationthat was determined, the level of the“teardrop” and the required abductionangle of 40°–45°.
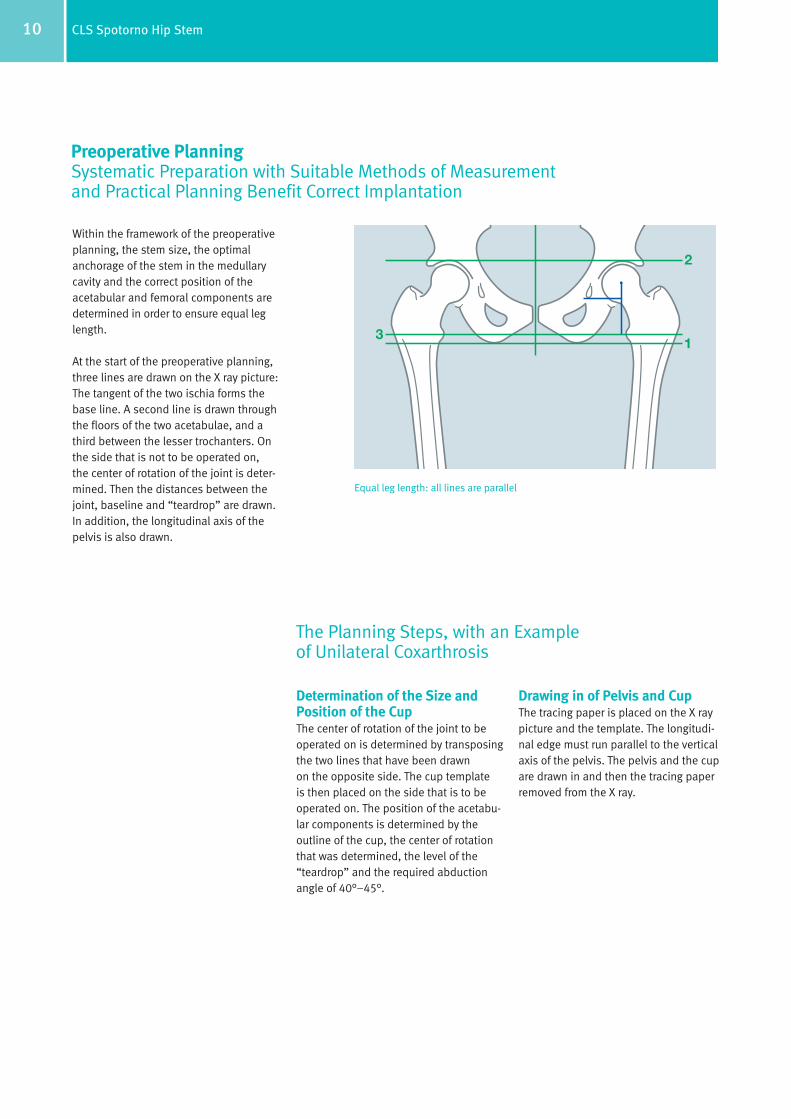
Within the framework of the preoperativeplanning, the stem size, the optimalanchorage of the stem in the medullarycavity and the correct position of theacetabular and femoral components aredetermined in order to ensure equal leglength.
At the start of the preoperative planning,three lines are drawn on the X ray picture:The tangent of the two ischia forms thebase line. A second line is drawn throughthe floors of the two acetabulae, and athird between the lesser trochanters. Onthe side that is not to be operated on, the center of rotation of the joint is deter-mined. Then the distances between thejoint, baseline and “teardrop” are drawn.In addition, the longitudinal axis of thepelvis is also drawn.
Equal leg length: all lines are parallel
Drawing in of Pelvis and CupThe tracing paper is placed on the X raypicture and the template. The longitudi-nal edge must run parallel to the verticalaxis of the pelvis. The pelvis and the cupare drawn in and then the tracing paperremoved from the X ray.
Preoperative PlanningSystematic Preparation with Suitable Methods of Measurementand Practical Planning Benefit Correct Implantation
The Planning Steps, with an Example of Unilateral Coxarthrosis

11CLS Spotorno Hip Stem
Height of the PelvisThe femoral template is to be left in place.The drawing of the pelvis is placed withthe acetabular components on the X raypicture. If lengthening of a leg is neces-sary, the drawing of the pelvis lies higherthan the pelvis on the X ray picture, bythe difference in the length to be corrected.In the case of planned shortening of aleg, the drawing must be correspondinglylower by the distance to be corrected.Stem size and length must be selected sothat the differences correspond to themeasurements that are to be corrected.
Final ResultThe outlines of the femur and the cortexand the selected implant/femoral headcombination are drawn on the transparentpaper. The distance between the proximalend of the taper of the stem and the lessertrochanter is measured and entered. The line from the shoulder of the stem tothe greater trochanter is extended and measured. The line between the tip of thegreater trochanter and the center ofrotation is drawn in.
Determination of the CCD Angle,the Size and Position of the StemFirst, the most adapted CCD angle of theCLS stem (125°, 135° or 145°) to fit intothe proximal part of the femur is selected.The selected stem template is placed on the femur so that the stem fits into themedullary canal displaying the correcttype of anchorage. The size of the stemmust be selected so that at least 3/4 of theproximal ribbed structure is anchored in the cancellous bone. Ideally, one of the four lines from the rotation centerstouches the tip of the greater trochanter.
12 CLS Spotorno Hip Stem
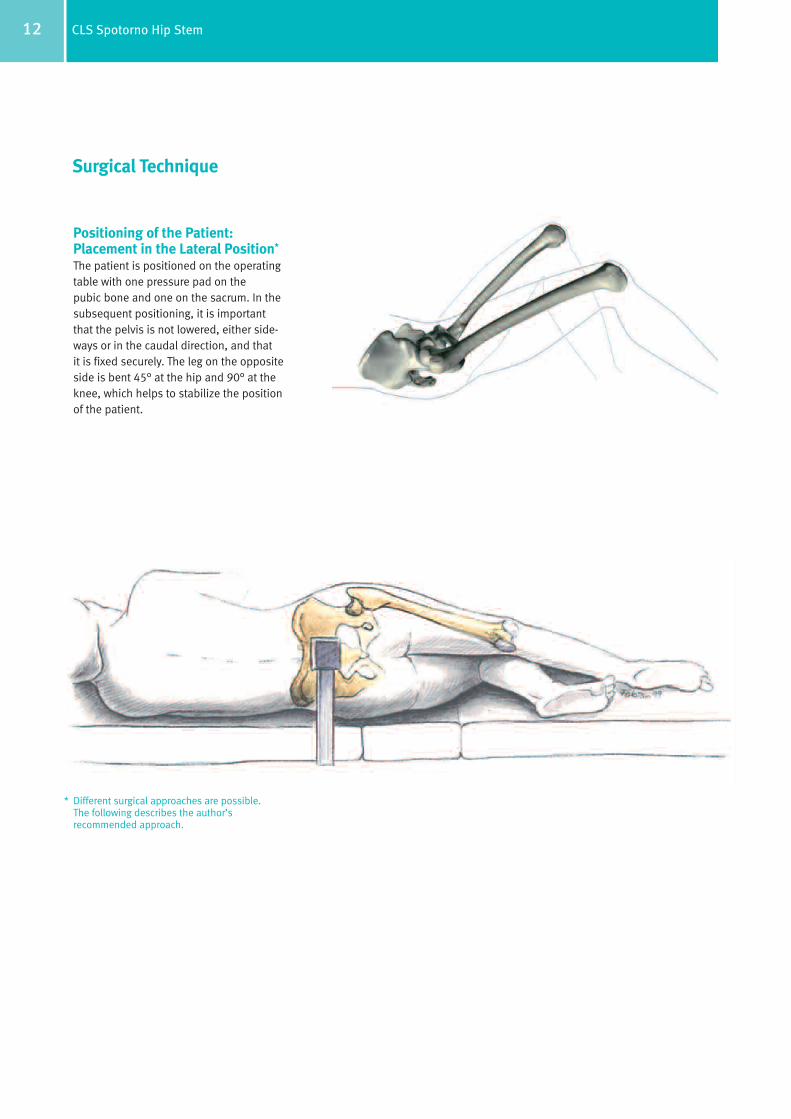
Positioning of the Patient: Placement in the Lateral Position*
The patient is positioned on the operatingtable with one pressure pad on the pubic bone and one on the sacrum. In the subsequent positioning, it is importantthat the pelvis is not lowered, either side-ways or in the caudal direction, and thatit is fixed securely. The leg on the oppositeside is bent 45° at the hip and 90° at theknee, which helps to stabilize the positionof the patient.
* Different surgical approaches are possible. The following describes the author’srecommended approach.
Surgical Technique

13CLS Spotorno Hip Stem
Surgical Approach to the Hip:Incision The posterolateral approach is recom-mended. The joint is bent at an anglebetween 30° and 40°. A rectilinear incisionis made to the tip of the greater trochanterand is then continued for about 6 cm on the diaphysis. After transection of thesubcutis, the fascia lata is exposed.
The Approach to the Deeper LayersThe fascia lata is incised and dissociatedof the fibers of the M. gluteus maximusand the Charnley wound retractor is placeddirectly on the fascia.
In this way, the plane of the external rotatormuscles and the tendon attachment ofthe M. gluteus maximus are exposed onthe linea aspera of the femur. The tendonattachment is partly released in order torelax the soft parts. This favours the displacement of the femur in the ventraldirection and also its internal rotation.
Transection of the ExternalRotator Muscles and Dislocation of the HipAfter inserting a bent Hohmann retractorunder the M. gluteus medius, the tendonof the M. piriformis is located and transected, as are some of the tendons ofthe external rotator muscles. The jointcapsule is then opened from the dorsocra-nial direction. With a combined flexion,adduction and internal rotation move-ment, the head of the femur can now bedislocated from the acetabulum.
14 CLS Spotorno Hip Stem
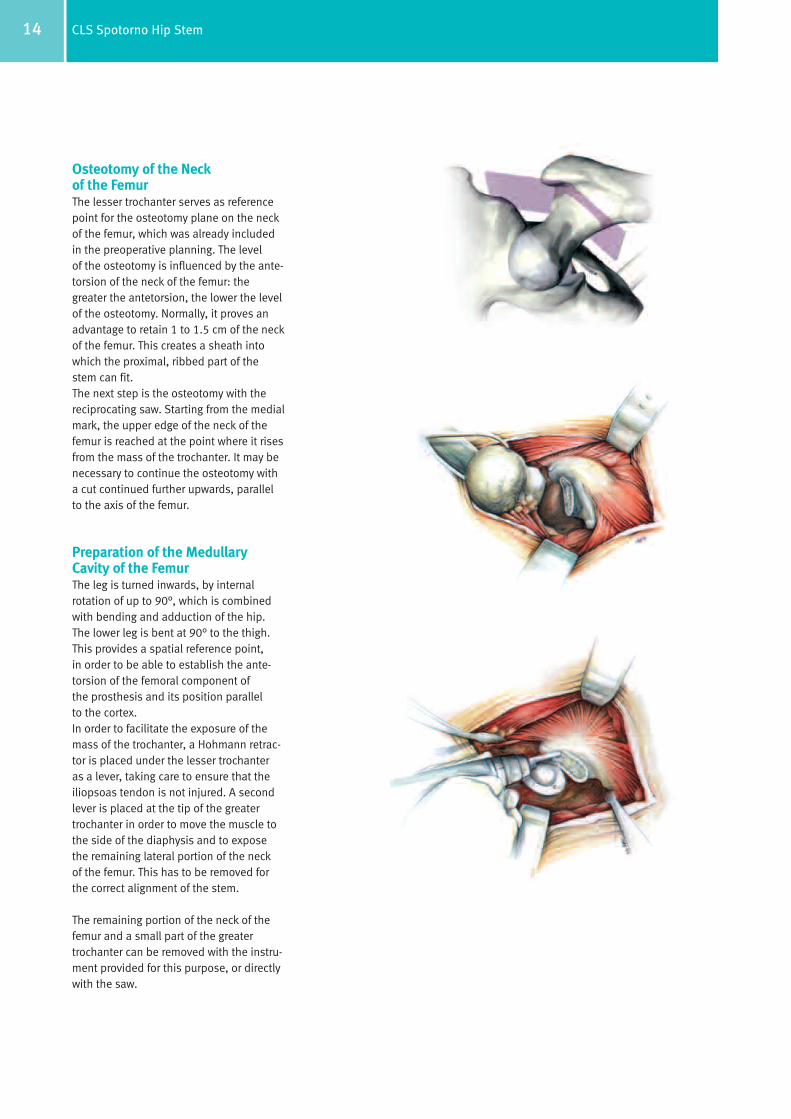
Osteotomy of the Neckof the FemurThe lesser trochanter serves as referencepoint for the osteotomy plane on the neckof the femur, which was already includedin the preoperative planning. The levelof the osteotomy is influenced by the ante-torsion of the neck of the femur: thegreater the antetorsion, the lower the levelof the osteotomy. Normally, it proves anadvantage to retain 1 to 1.5 cm of the neckof the femur. This creates a sheath intowhich the proximal, ribbed part of thestem can fit. The next step is the osteotomy with thereciprocating saw. Starting from the medialmark, the upper edge of the neck of thefemur is reached at the point where it risesfrom the mass of the trochanter. It may benecessary to continue the osteotomy witha cut continued further upwards, parallelto the axis of the femur.
Preparation of the MedullaryCavity of the FemurThe leg is turned inwards, by internalrotation of up to 90°, which is combinedwith bending and adduction of the hip.The lower leg is bent at 90° to the thigh.This provides a spatial reference point, in order to be able to establish the ante-torsion of the femoral component ofthe prosthesis and its position parallelto the cortex.In order to facilitate the exposure of themass of the trochanter, a Hohmann retrac-tor is placed under the lesser trochanter as a lever, taking care to ensure that theiliopsoas tendon is not injured. A secondlever is placed at the tip of the greatertrochanter in order to move the muscle tothe side of the diaphysis and to exposethe remaining lateral portion of the neckof the femur. This has to be removed forthe correct alignment of the stem.
The remaining portion of the neck of thefemur and a small part of the greatertrochanter can be removed with the instru-ment provided for this purpose, or directlywith the saw.

15CLS Spotorno Hip Stem
Use of the Awl and Rasping TechniqueThe proximal notches on the awl mark theheight of the shoulder of the implant. The awl has to be inserted laterally andslightly dorsal. The attachment of the M. piriformis provides a reference pointfor this. As a rule, this corresponds to the point at which, in the preoperativeplanning, the tangent of the endostealedge of the outer cortex meets the greatertrochanter. It provides an accurate, measurable conception of the obstacle to the prosthesis. After the medullary space has been prepared in this way, the awl is inserteddeep, for centering in the canal, takingcare to ensure that it is pressed in thedirection of the greater trochanter. The aimis to follow the predetermined line towardsthe lateral cortex, parallel to the axis ofthe femur and to avoid a varus deformity.The bed for the stem is now prepared,using rasps of increasing size, until thehighest possible degree of stability isobtained. The preoperatively measureddistance between the proximal shoulder ofthe prosthesis and the greater trochanterserves as orientation.

16 CLS Spotorno Hip Stem
The desired stability is based on the concept of a press-fit in the cortex andcancellous bone. This is why the raspshave smooth zones for compression of the cancellous bone and cutting zonesfor rasping of parts of the cortex.*
After the surgeon has established the sizeof the prosthesis during the planning, thedefinite size is determined by progressive,stepwise rasping, starting with 3 to 4smaller rasp sizes. In this way, using theincreasing dimensions, the cancellousbone is compressed. Where necessary, the cortex has to be reamed. The rasps areinserted with small, precise hammer blows,and then withdrawn.
The final, definitive reaming must be carried out only with the rasp planned forthis. The last rasp should be operatedmanually.
* The rasp is designed to lead to a defined smaller dimen-sion in relation to the bony structure of the femur.Generally, it is underdimensioned in the proximal portionof the rasp – that is, the portion with which cancellousbone is to be compressed.
At the distal end, the rasp is slightly oversized, in order toprevent stress peaks on the end of the prosthesis.
17CLS Spotorno Hip Stem
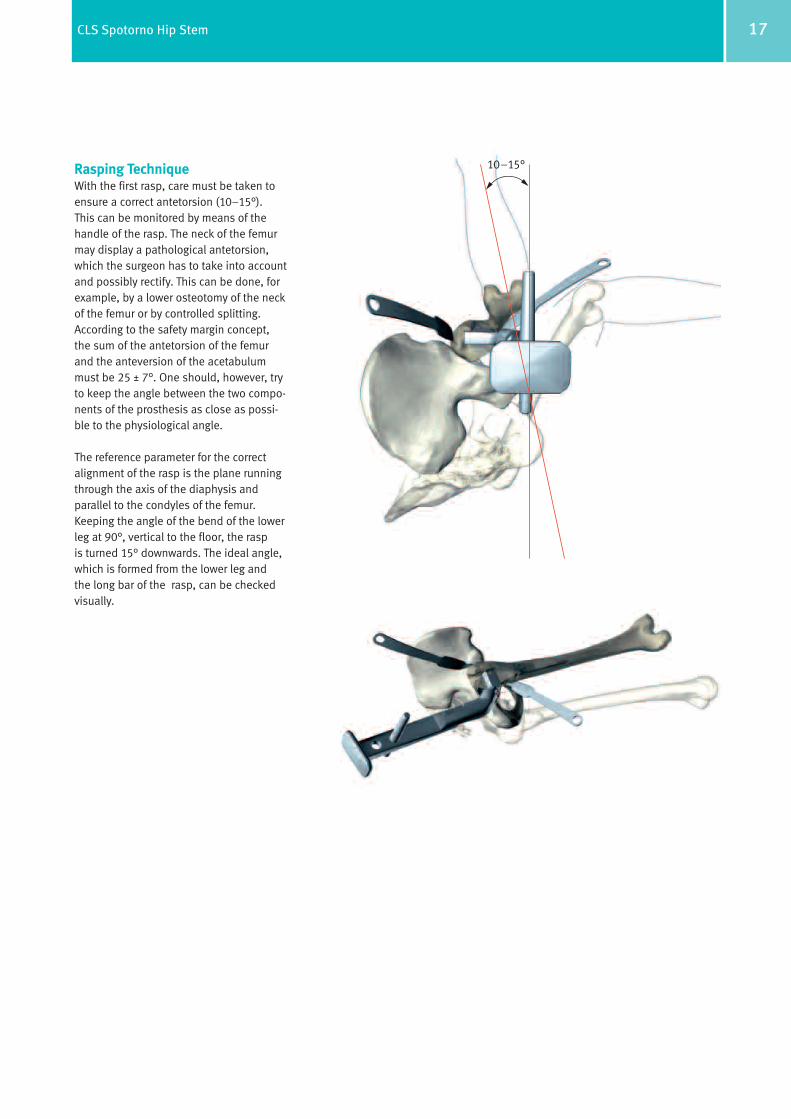
Rasping TechniqueWith the first rasp, care must be taken toensure a correct antetorsion (10–15°). This can be monitored by means of thehandle of the rasp. The neck of the femurmay display a pathological antetorsion,which the surgeon has to take into accountand possibly rectify. This can be done, forexample, by a lower osteotomy of the neckof the femur or by controlled splitting.According to the safety margin concept,the sum of the antetorsion of the femurand the anteversion of the acetabulummust be 25 ± 7°. One should, however, tryto keep the angle between the two compo-nents of the prosthesis as close as possi-ble to the physiological angle.
The reference parameter for the correctalignment of the rasp is the plane runningthrough the axis of the diaphysis and parallel to the condyles of the femur.Keeping the angle of the bend of the lowerleg at 90°, vertical to the floor, the rasp is turned 15° downwards. The ideal angle,which is formed from the lower leg and the long bar of the rasp, can be checkedvisually.
10–15°

18 CLS Spotorno Hip Stem
Trial Repositioning with Trial NeckTrial reduction of the CLS stem may beaccomplished with the rasp.
This is done by removing the rasp handleand leaving the rasp in the femoralcanal. A trial neck is then inserted intothe rasp hole. Once the trial neck isselected, any of the trial heads may beused in conjunction with the trial neck.
For the CLS stem, different trial neckshave to be used in order to correctlyreproduce the different offset options.
Once the trial neck and the appropriatetrial head are selected, the hip is reduced.Leg length and offset are checked. Thisprocedure is repeated as necessary,using trial heads of different lengths, untiloptimal offset, leg length and stabilityare established. A trial reduction shouldnot allow significant push-pull or “shuck”of the joint in full extension. The range ofmotion is checked to avoid bony impinge-ment and instability.
Insertion of the StemAfter removal of the rasp, a prosthesisof the appropriate size is inserted anddriven in until it is completely stable. In this process, it is important to proceedwith the necessary light touch. This islearned with experience. It should beremembered that because of the wedgemechanism, an excessive load may beexerted that can bear on the trochanter tothe point that it might cause a fracture.
It is important to adjust the force of thehammer blows, according to the qualityof the bone and to stop the hammerblows immediately if a change in thesound of the blows, from dull (cancellousbone) to sharp (cortex) is perceived.

19CLS Spotorno Hip Stem
Assembly of the Femoral Headand Repositioning After insertion of the prosthesis, thedefinitive femoral head is established onthe basis of the measurements laid down in the preoperative planning and bytrial repositioning using trial heads. The last step in the assembly is the fittingof the previously defined head onto the stem. After thoroughly cleaning anddrying the taper, the femoral head ismounted with a light rotational movementand rotated further with axial force untilit is firmly seated. The femoral head isseated with one light hammer blow onthe head impactor in axial direction.
Upon reducing the joint, the surgeonchecks the range of motion and stabilityof the joint. This should be checked with both internal and external rotation.
With the placing of drains and suturing of the different layers, the operation isnow complete.
Intraoperative Extraction of the StemIf the stem needs to be removed intra-operatively only the specific extractioninstrument has to be used, which protects the neck and the cone of thestem. Slide the extraction instrument overthe stem taper, until the plastic jawsreache the neck of the stem. It is veryimportant that the plastic jaws touch onlythe neck and not the taper. Afterwardstighten the plastic jaws with the ball hexscrewdriver, until the extraction instrument is firmly fixed on the stem.Remove the stem by hammering on the extraction instrument.
Important: The extraction instrumentcan be used only for intraoperative stemextraction. It is not suitable for revisioncases. The plastic jaws can be exchanged ifnecessary.
Intraoperative extraction of the stem
20 CLS Spotorno Hip Stem
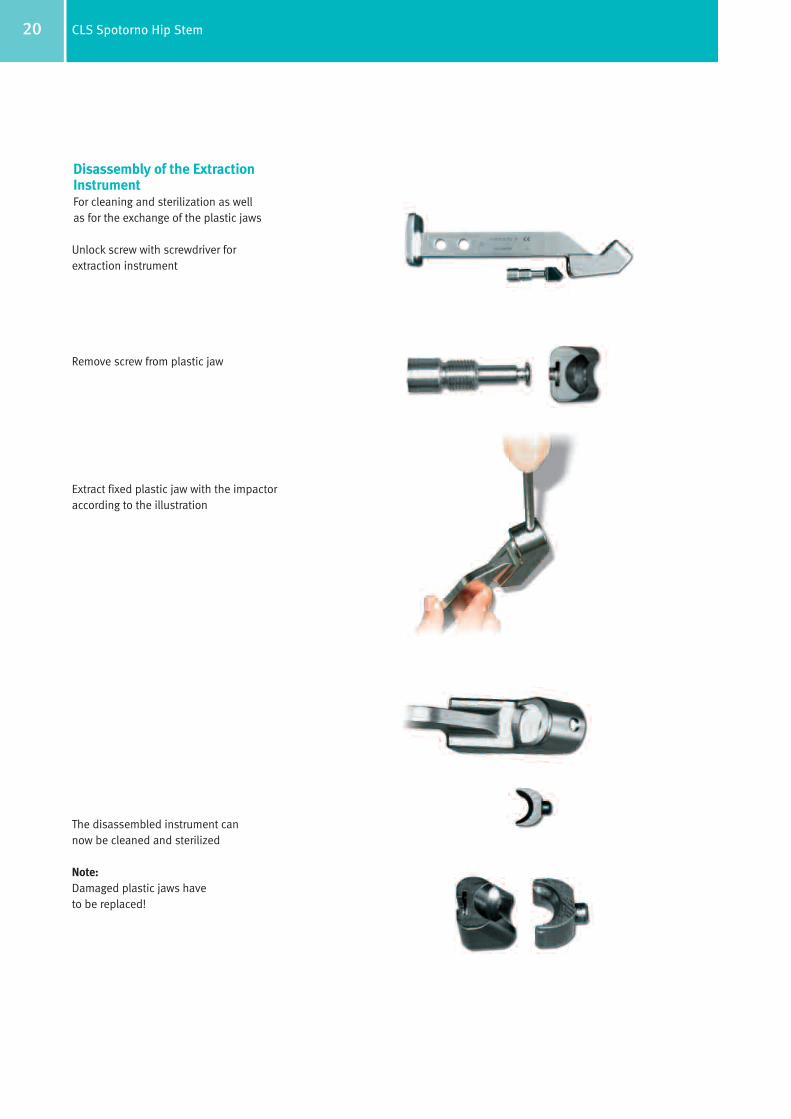
Unlock screw with screwdriver for extraction instrument
Remove screw from plastic jaw
Extract fixed plastic jaw with the impactor according to the illustration
The disassembled instrument can now be cleaned and sterilized
Note:Damaged plastic jaws have to be replaced!
Disassembly of the ExtractionInstrumentFor cleaning and sterilization as wellas for the exchange of the plastic jaws
21CLS Spotorno Hip Stem
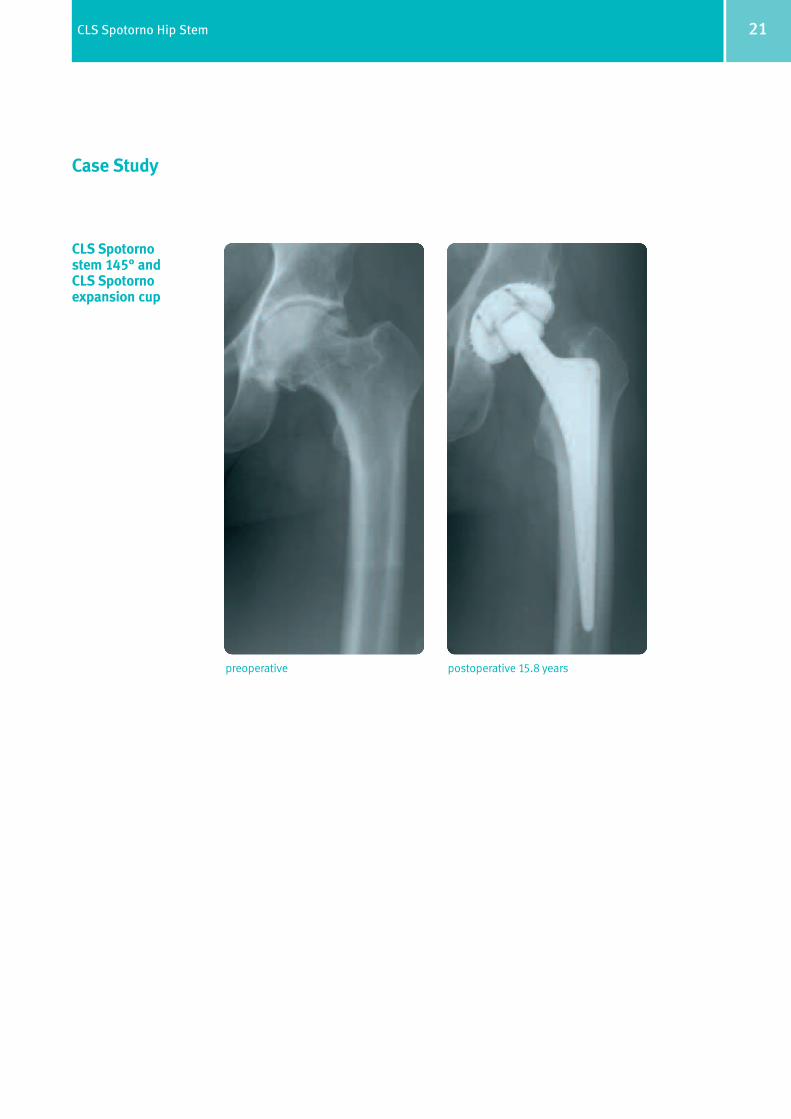
Case Study
CLS Spotorno stem 145° and CLS Spotorno expansion cup
preoperative postoperative 15.8 years
22 CLS Spotorno Hip Stem
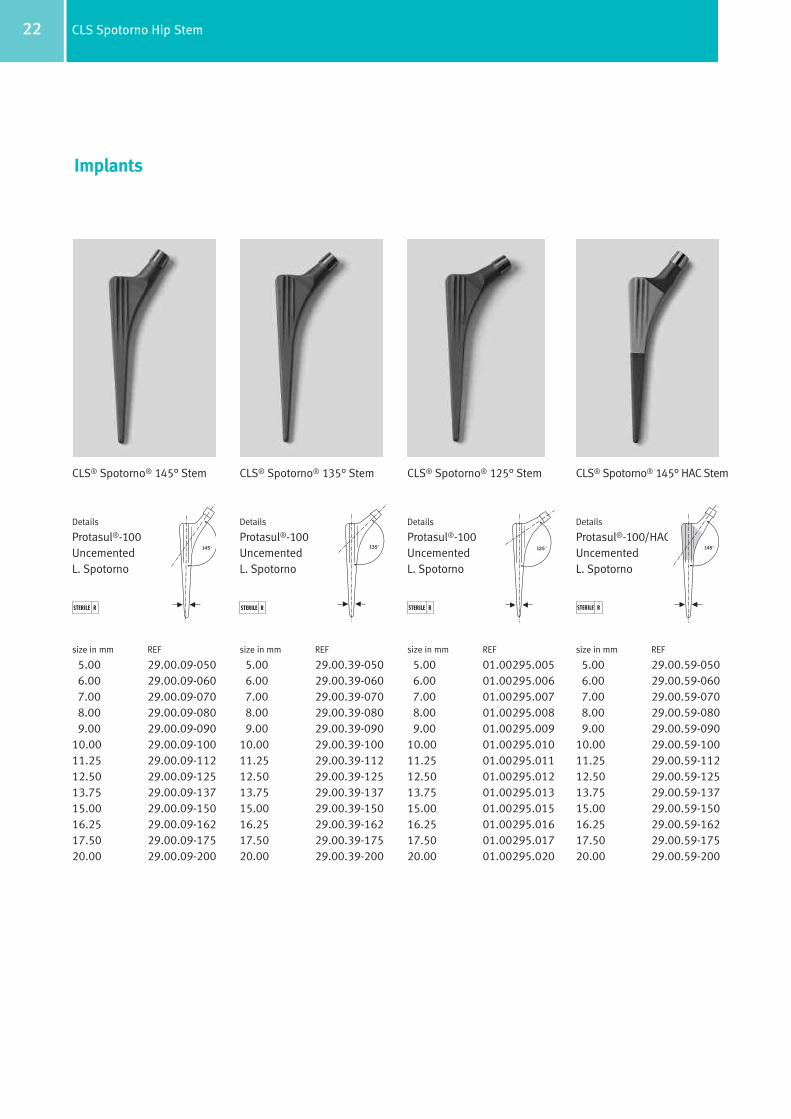
CLS® Spotorno® 125° Stem
Details
Protasul®-100UncementedL. Spotorno
size in mm REF
5.00 01.00295.0056.00 01.00295.0067.00 01.00295.0078.00 01.00295.0089.00 01.00295.009
10.00 01.00295.01011.25 01.00295.01112.50 01.00295.01213.75 01.00295.01315.00 01.00295.01516.25 01.00295.01617.50 01.00295.01720.00 01.00295.020
Implants
CLS® Spotorno® 135° Stem
Details
Protasul®-100UncementedL. Spotorno
size in mm REF
5.00 29.00.39-0506.00 29.00.39-0607.00 29.00.39-0708.00 29.00.39-0809.00 29.00.39-090
10.00 29.00.39-10011.25 29.00.39-11212.50 29.00.39-12513.75 29.00.39-13715.00 29.00.39-15016.25 29.00.39-16217.50 29.00.39-17520.00 29.00.39-200
135°
CLS® Spotorno® 145° Stem
Details
Protasul®-100UncementedL. Spotorno
size in mm REF
5.00 29.00.09-0506.00 29.00.09-0607.00 29.00.09-0708.00 29.00.09-0809.00 29.00.09-090
10.00 29.00.09-10011.25 29.00.09-11212.50 29.00.09-12513.75 29.00.09-13715.00 29.00.09-15016.25 29.00.09-16217.50 29.00.09-17520.00 29.00.09-200
STERILE RSTERILE R STERILE R
CLS® Spotorno® 145° HAC Stem
Details
Protasul®-100/HACUncementedL. Spotorno
size in mm REF
5.00 29.00.59-0506.00 29.00.59-0607.00 29.00.59-0708.00 29.00.59-0809.00 29.00.59-090
10.00 29.00.59-10011.25 29.00.59-11212.50 29.00.59-12513.75 29.00.59-13715.00 29.00.59-15016.25 29.00.59-16217.50 29.00.59-17520.00 29.00.59-200
STERILE R
145° 125° 145°

23CLS Spotorno Hip Stem
Instruments
Handle for modular raspREF
01.00299.100
Long barREF
70.00.01
Rasp modularsize in mm REF
5.00 01.00299.1056.00 01.00299.1067.00 01.00299.1078.00 01.00299.1089.00 01.00299.109
10.00 01.00299.11011.25 01.00299.11112.50 01.00299.11213.75 01.00299.11315.00 01.00299.11516.25 01.00299.11617.50 01.00299.11720.00 01.00299.120
Tray (complete)REF
ZS 01.00298.110
Standard container coverREF
01.00029.031
Tray (empty)REF
01.00298.110
Insert for tray (empty)REF
01.00298.102

24 CLS Spotorno Hip Stem
Trial neckCLS REF
125° 01.00299.125135° 01.00299.135145° 01.00299.145
Trial heads∅ 28 REF
12/14 S 01.01559.12812/14 M 01.01559.22812/14 L 01.01559.32812/14 XL 01.01559.428
∅ 32 REF
12/14 S 01.01559.13212/14 M 01.01559.23212/14 L 01.01559.33212/14 XL 01.01559.432
Repositioning leverREF
75.11.00-02
Repositioning topsmm REF
28 78.00.38-2832 78.00.38-32
Double-curved gaugemm REF
9 75.09.15
Boxed chiselREF
75.13.02-10
AwlREF
70.08.89
ImpactorREF
75.00.36
Rulermm REF
20 95.00.03
Extraction instrument for stemREF
01.00529.102
Screwdriver for extraction instrumentREF
01.00529.101

25CLS Spotorno Hip Stem
Trial heads∅ 36 REF
12/14 S 01.01559.13612/14 M 01.01559.23612/14 L 01.01559.33612/14 XL 01.01559.436
Handle for modular rasp with IMTREF
01.00299.101
Repositioning topsmm REF
36 78.00.38-36
Plastic jaws for 01.00529.102REF
01.00529.103
Upon Request
26 CLS Spotorno Hip Stem

Contact your Zimmer representative or visit us at www.zimmer.com
+H84406012970121/$061201L064
Lit. No. 06.01297.012 – Ed. 12/2006 ZHUB
©20
06by
Zim
mer
Gm
bHPr
inte
din
Sw
itze
rland
Subj
ectt
och
ange
wit
hout
noti
ce