spine surgery lecture ulbd
TRANSCRIPT

ULBD: Unilateral Laminectomy Bilateral
Decompression
December 1, 2017
Upper Chesapeake Medical Center

72 woman with R buttock painLBP

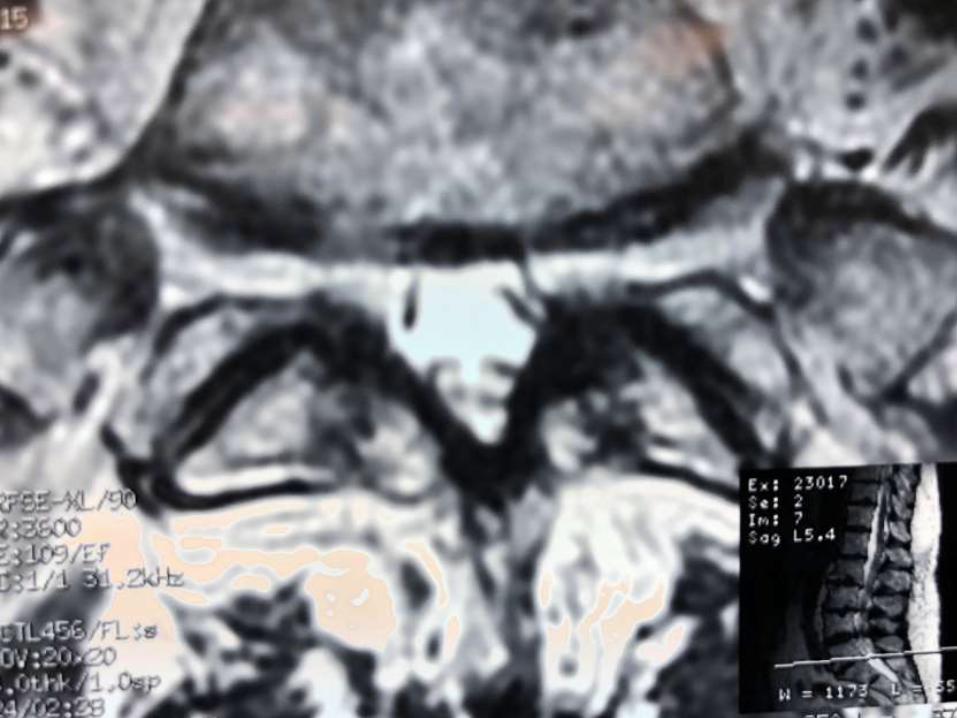
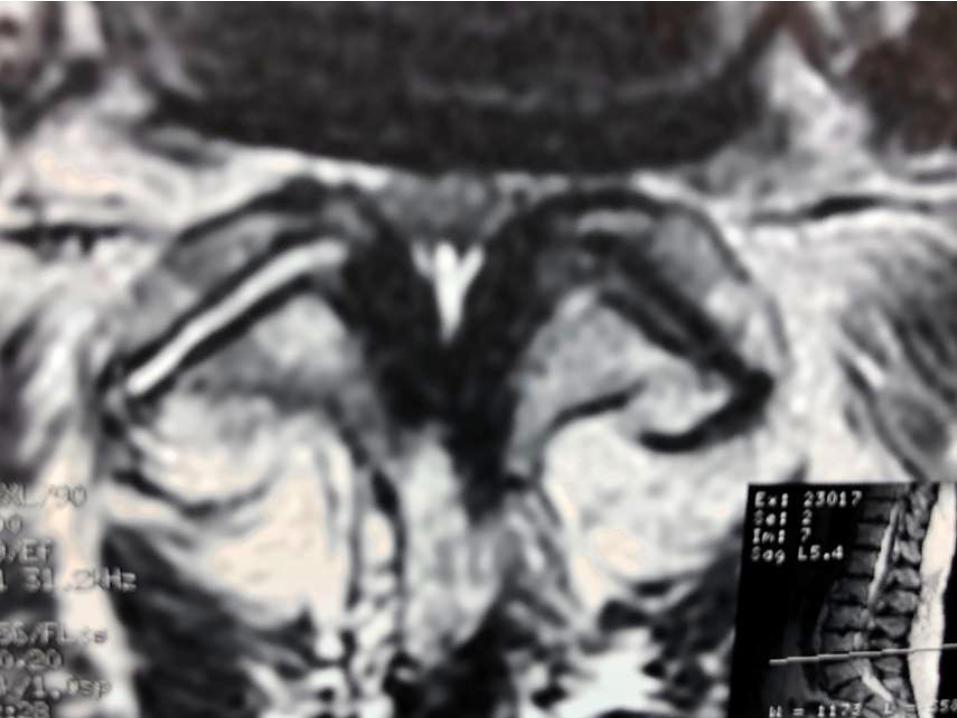
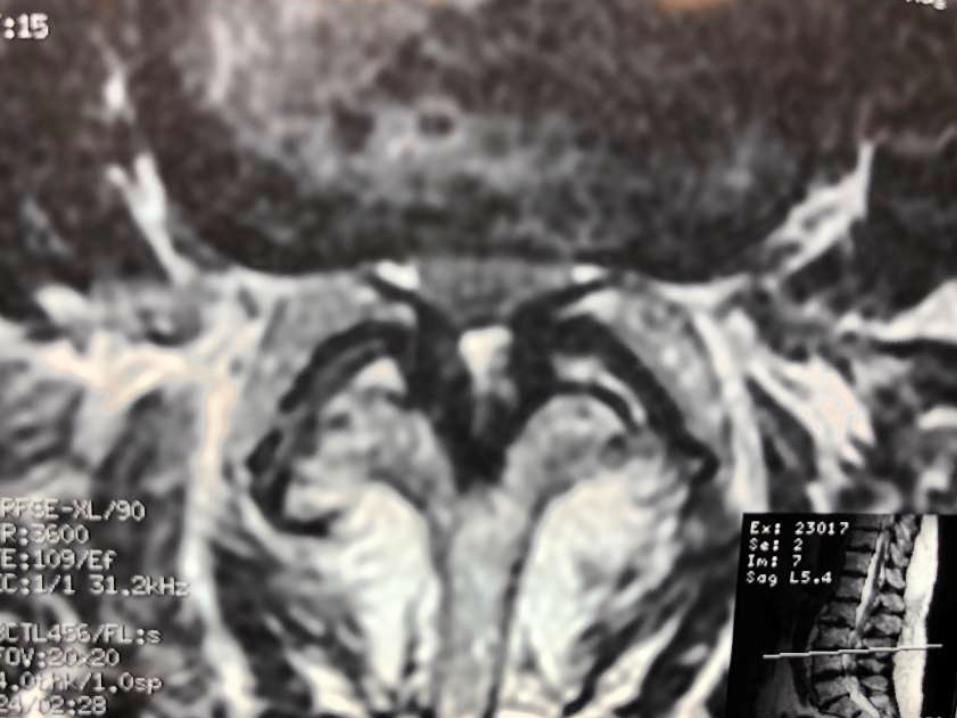


Normal?
Boden article: JBJS Vol. 72-A, No. 8, Sept 1990
<40 years N=167
<40 years >40 years N=97
>40 years
MAJOR MINOR
Herniated disc
3% 4% 1% 4%
Bulging disc 0 5% 1% 5%
Foraminalstenosis
3% 4% 9% 14%
Disc space narrowing
2% 11% 16% 22%
Degenerative disc
8% 37%
Spurs 3% 14% 6% 34%
Abnormal cord
9% 9% 1% 18%



Mixter and Barr JBJS 1934 was the first description of herniated discs causing sciatica with surgery as a successful treatment

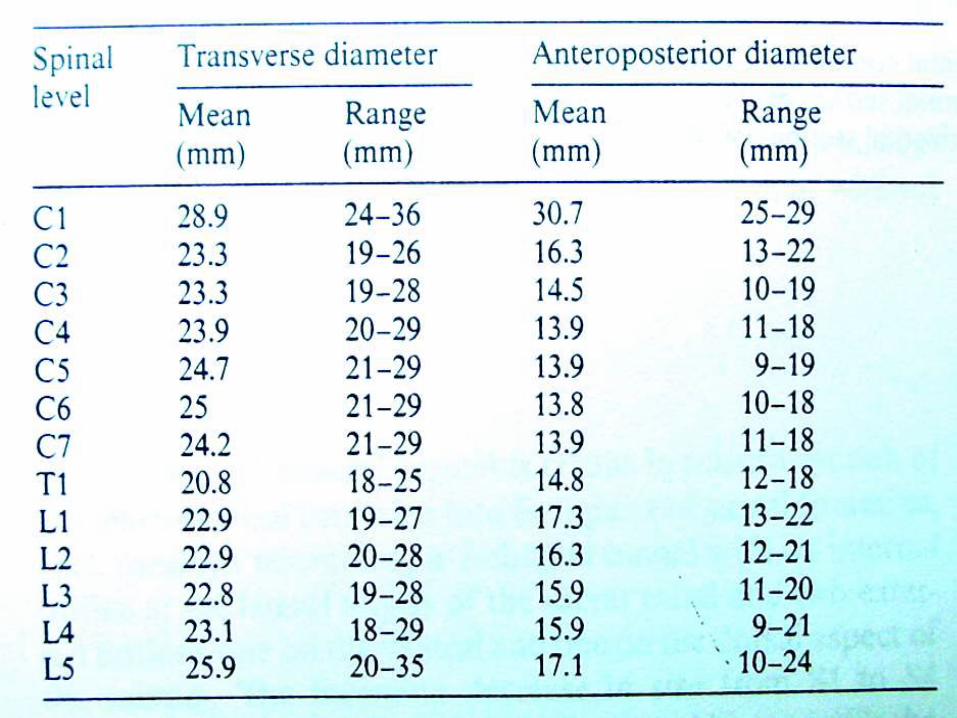
Henk Verbiest1909-1997Dutch neurosurgeon introduced the concept of a developmental spinal stenosis 1940 due to a small AP diameter spinal canal





Red flag
Nocturnal pain
Pain at rest
Progressive neurological deficit
Suspicious for cancer or infection

High index of suspicion
H/O cancer
Osteoporosis/steroids/immunosuppression
AS
10/10
Weight loss
IVDA
UTI/sepsis







Kleeman, T.J., Hiscoe, A.C., Berg, E.E.: “Patient Outcomes Following Minimally DestabilizingLumbar Stenosis Decompression: The ‘Port Hole’ Technique”, Spine, April 2000.
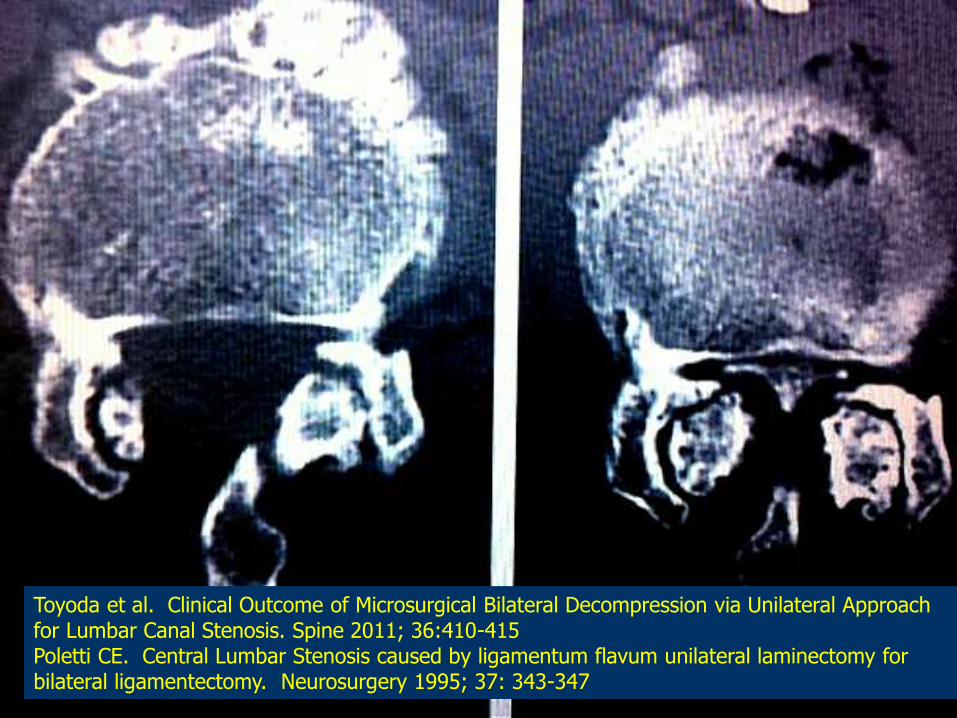
Toyoda et al. Clinical Outcome of Microsurgical Bilateral Decompression via Unilateral Approach for Lumbar Canal Stenosis. Spine 2011; 36:410-415 Poletti CE. Central Lumbar Stenosis caused by ligamentum flavum unilateral laminectomy for bilateral ligamentectomy. Neurosurgery 1995; 37: 343-347


Prone Position

OSI Jackson Table 2bends, rotates, secure






Slide a Ligamentumflavum

Optimal anatomy
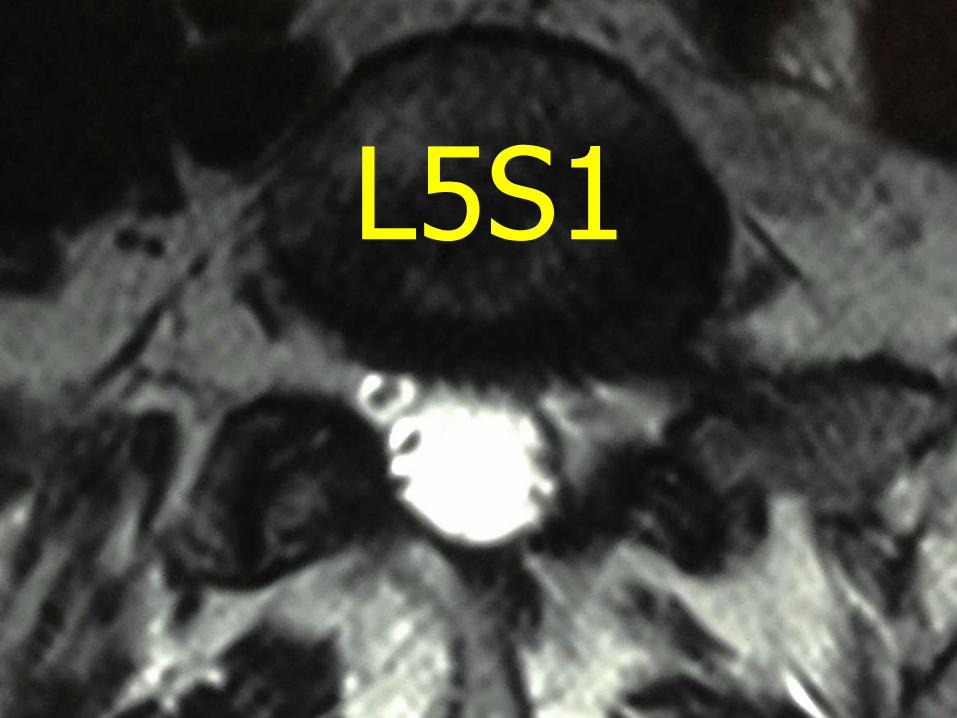
L5S1

L4L5
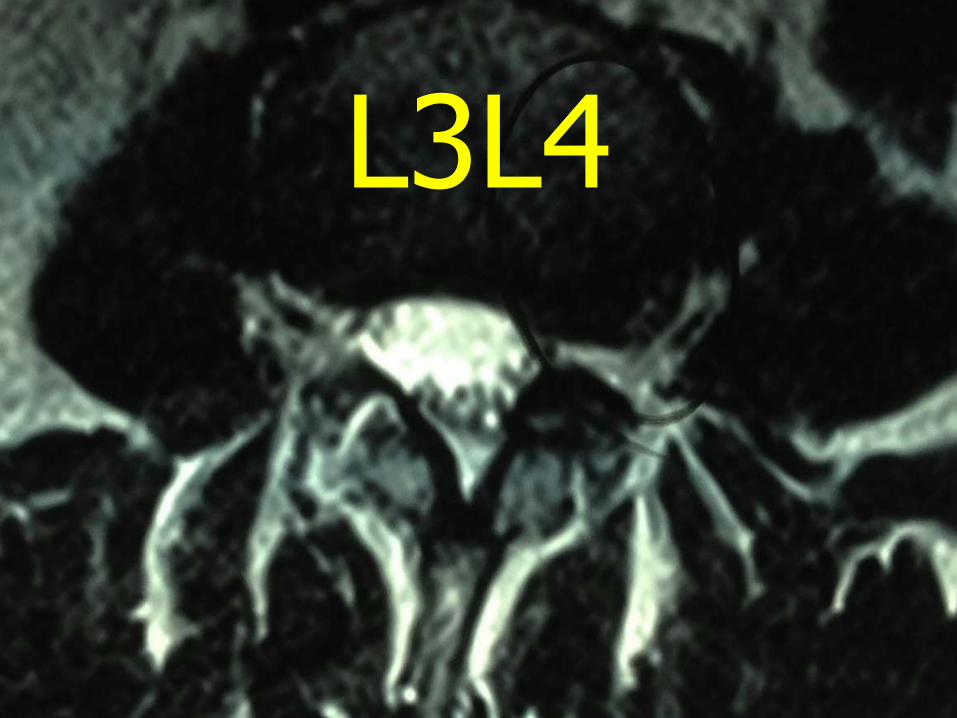
L3L4

L2L3

L1L2

T12L1
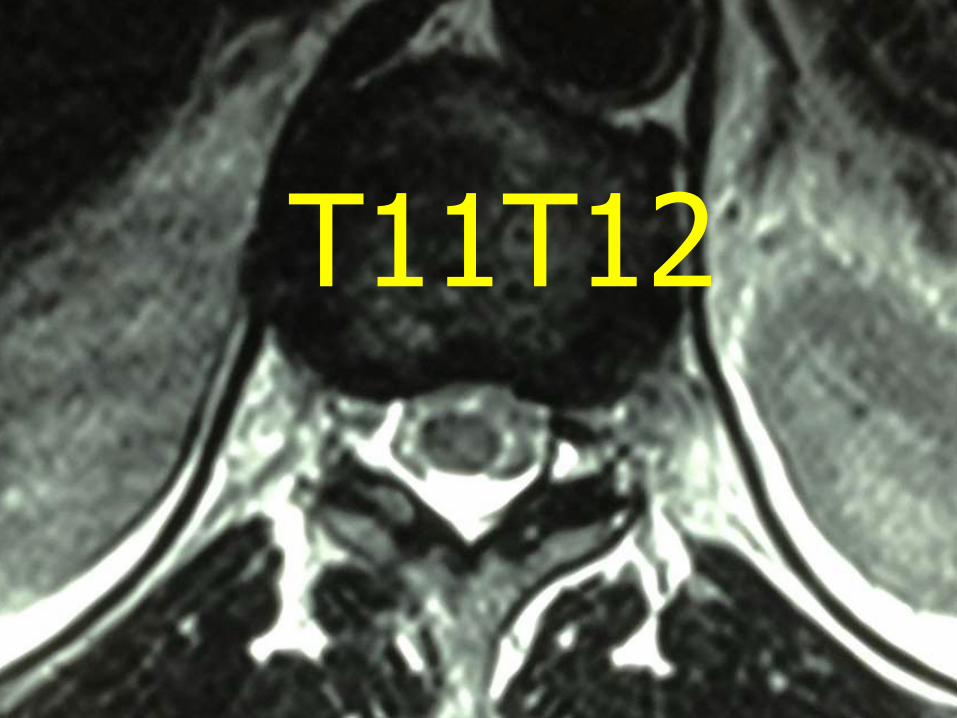
T11T12

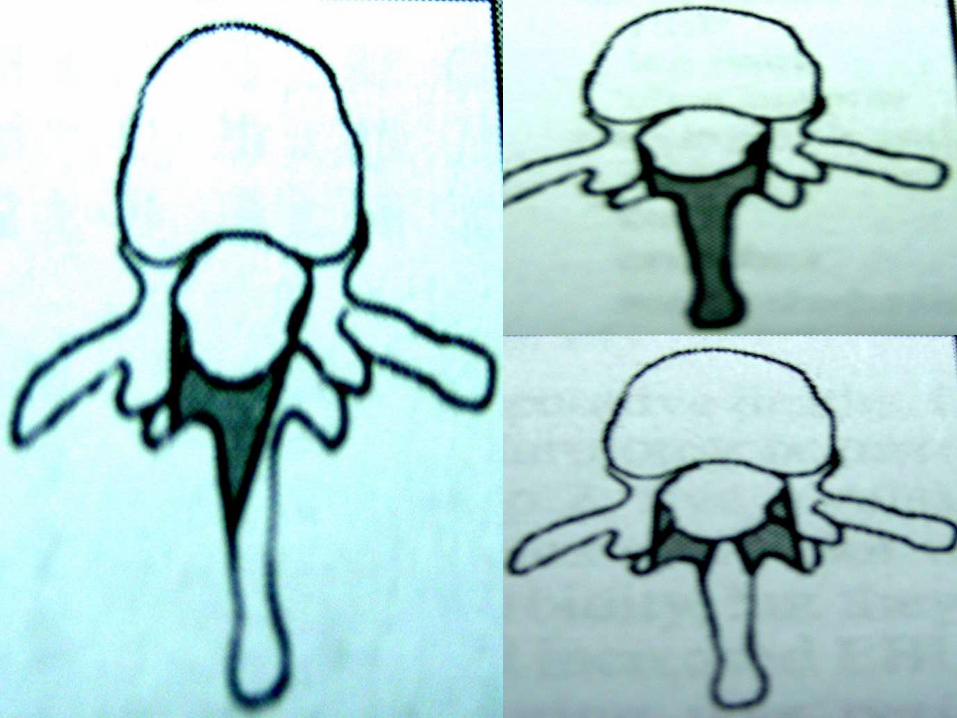
144 single level, korea, Trefoil canal stenosis patients were more difficult to decompression due to angle of approach and patients had worse outcomes
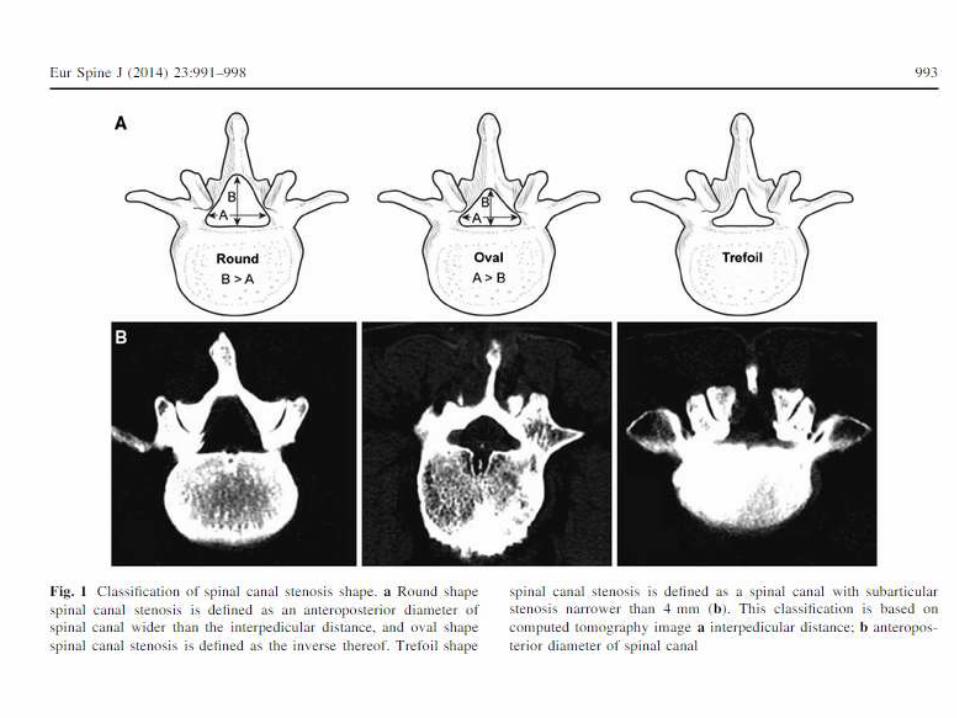


J Neurosurg Spine. 2014 Aug;21(2):179-86. doi: 10.3171/2014.4.SPINE13420. Epub2014 May 30.
Outcomes after decompressive laminectomy for lumbar spinal stenosis: comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: clinical article.
Mobbs RJ1, Li J, Sivabalan P, Raley D, Rao PJ.
79 patients prospective 1:1 ULBD v. open laminectomy, oswestry disability andPatient satisfaction were similar, ULBD had shorter stay 55 h v 100 h, shorter timeTo mobilize 15h v 33 h and more people not requiring opiates 51% v 15%

Neurosurgery. 2006 Dec;59(6):1264-9; discussion 1269-70.Long-term results of microsurgical treatment of lumbar spinal stenosis by unilateral
laminotomy for bilateral decompression.Oertel MF1, Ryang YM, Korinth MC, Gilsbach JM, Rohde V.
133 patients mean fu 5.6 years up to 10 years
Reoperation 11%, 2 instability, 7 restenosis
85% excellent to fair long term results
Dr M F Oertel Department of Neurosurgery, University Hospital, School of Medicine, Aachen University, Pauwelsstrasse 30, 52057 Aachen, Germany

ULBD pitfalls complications
Restenosis( contralateral side)
Dural tear
Nerve injury
Instability
Persistent pain from facet
Pars fracture
Inadequate decompression
Persistent foramenal stenosis


Working windowWaxDown to lamina



Keep pars intactDura is 23 mm wideNeed 11 mm from midlineNo more than 3 burr diameters

Start lateral to know your parsStay medial to facetGo above facet and yellow lig


Connect two areas


Lig flavum protects duraKeep it on as long as possible
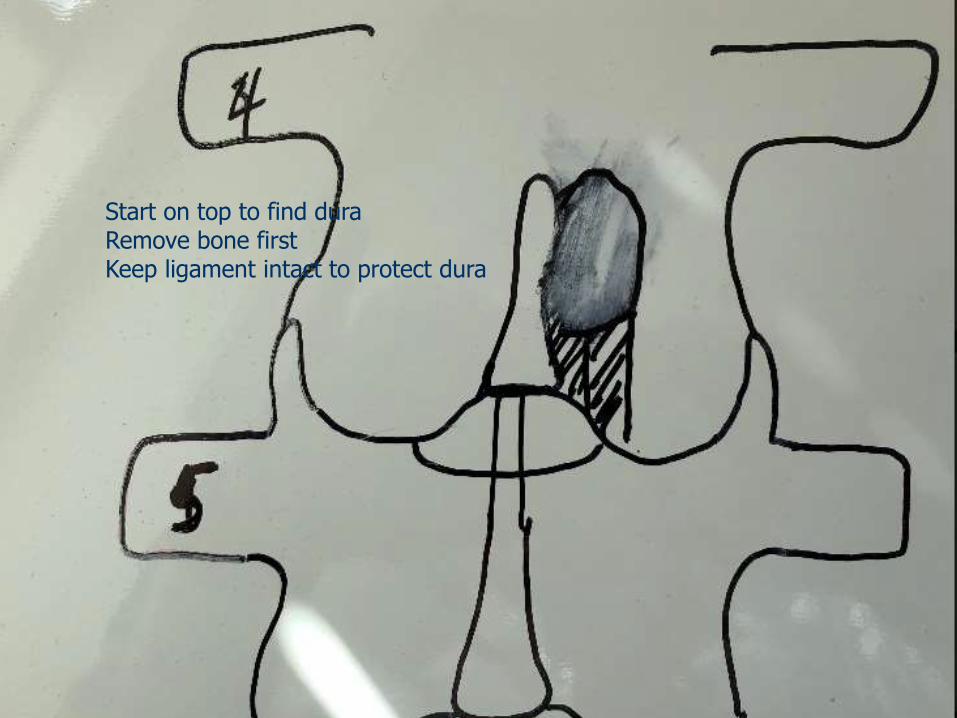
Start on top to find duraRemove bone firstKeep ligament intact to protect dura

You should be looking at yellow ligament at this point
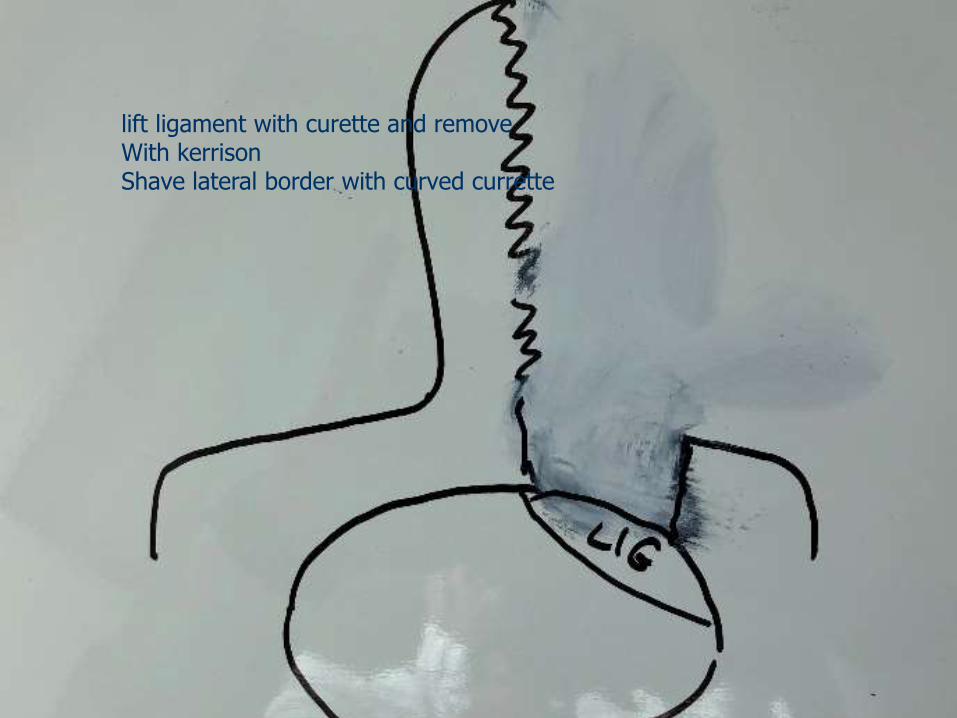
lift ligament with curette and removeWith kerrisonShave lateral border with curved currette

Dura exposed

Undermine lamina opposite side





Which side to approach?


THANKS