spine radius surgical technique - select your location … surgical technique sets forth detailed,...
TRANSCRIPT

Spine
Radius®
Surgical Technique
Precision
•Zoneoflockingsecurity•Non-threadedlockingmechanism•Simple,lowtorqueclosure•Lowprofile,lowvolumemulti-anglescrew
2
Important:TheRadius®implantsandinstrumentsaredesignedandtestedforuseonlywiththeRadius®SpinalSystem.Thissurgicaltechniquesetsforthdetailed,recommendedproceduresforusingtheRadius®PrecisionSystemimplantsandinstruments.Itoffersguidancethatyoushouldheedbut,aswithanysuchtechnicalguide,eachsurgeonmustconsidertheparticularneedsofeachpatientandmakeappropriateadjustmentswhennecessaryandasrequired.
Note:This is intended as a guide only. There are multiple techniques for the insertion of pedicle screws and, as with any surgical procedure, a surgeon should be thoroughly trained before proceeding.
Minimallyinvasivesystemshavebeendesignedtoreducetissuetraumathroughsmallerincisions.TheRadius®PrecisionSystemforminimallyinvasivesurgerycontainscannulatedscrewsthathavebeendevelopedtofacilitatescrewimplantationduetothereducedvisualizationwithinthesenarrowerworkingchannels.
TheRadius®PrecisionSystemhelpssurgeonsimplanttheRadius®cannulatedpolyaxialtitaniumscrewsthroughalessinvasiveposteriorapproachbyfollowingthepathofaguidewire.Thisisaccomplishedwithstreamlinedinstrumentationdesignedtomaximizevisualizationwhileminimizingthecomplexityofthesystem.
Introduction
3
Table of Contents
Precision Surgical Technique
Introduction 02
Key Design Features 04
I. Pedicle Preparation 06
II. Screw Insertion 12
III. Rod Insertion 14
IV. Final Tightening 15
Implants 16
Instruments 17

Low profile screw head designed to enhance visualization of the anatomy
Follows pathof K-Wire
Color coded
40˚ polyaxial freedom
35˚ tip
3 cutting flutesfacilitate boneinsertion
4
Radius® Precision ScrewBiomechanical Strength
• Equivalentstrengthtonon-cannulatedscrewunderstaticcorpectomyconditions*
• TitaniumAlloy(Ti6Al4V)
Self-Tapping Screw
ScrewSizes:Ø5.75x35-50mm(5mmincrements)Ø6.75x30-55mm(5mmincrements)Ø7.75x30-55mm(5mmincrements)
Radius® Locking Cap
Ø5.5mm Pre-Cut / Pre-Bent Rods
• Shortlengthswithtightbendforsinglelevelfusions
• Mediumlengthswithgradualbendfor1and2levelfusions
• Longerlengthstoaccommodate2and3levelfusions
• TitaniumAlloy(Ti6Al4V)
*DataonfileatStryker®Spine:EngineeringAnalysisK060705
Key Design Features - Implants
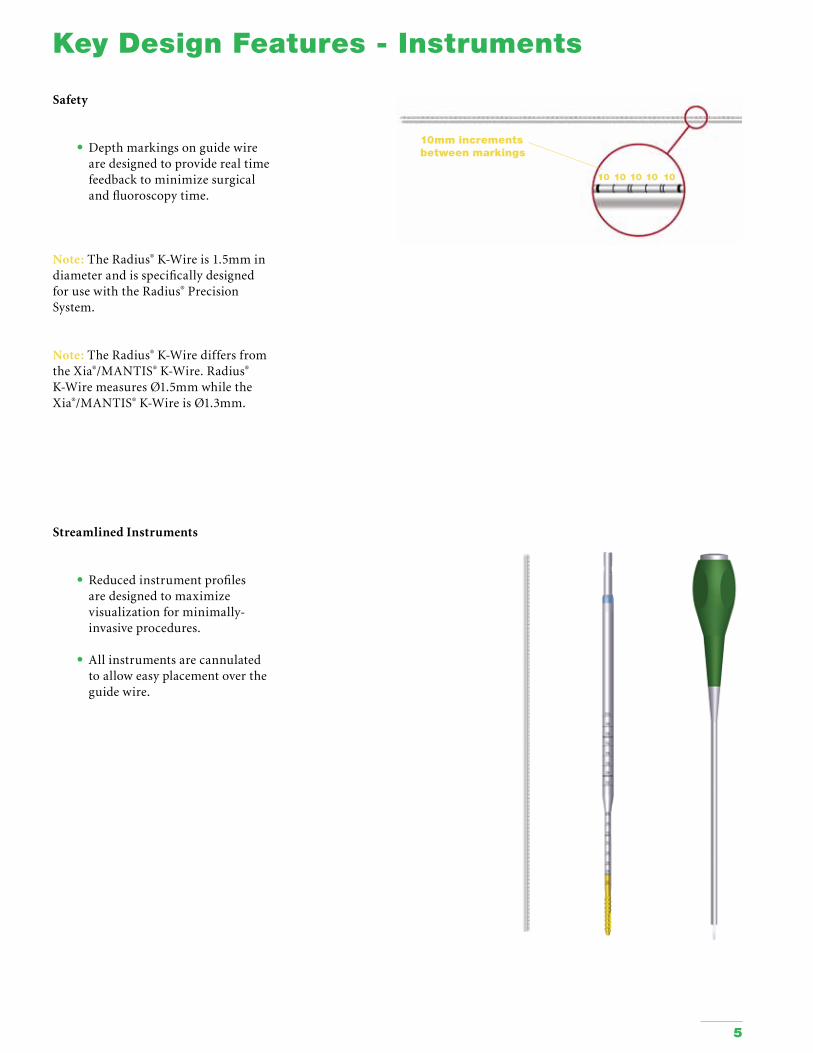
Safety
• Depthmarkingsonguidewirearedesignedtoproviderealtimefeedbacktominimizesurgicalandfluoroscopytime.
Note:TheRadius®K-Wireis1.5mmindiameterandisspecificallydesignedforusewiththeRadius®PrecisionSystem.
Note:TheRadius®K-WirediffersfromtheXia®/MANTIS®K-Wire.Radius®K-WiremeasuresØ1.5mmwhiletheXia®/MANTIS®K-WireisØ1.3mm.
10mm increments between markings
1010101010
Streamlined Instruments
• Reducedinstrumentprofilesaredesignedtomaximizevisualizationforminimally-invasiveprocedures.
• Allinstrumentsarecannulatedtoalloweasyplacementovertheguidewire.
5
Key Design Features - Instruments
6
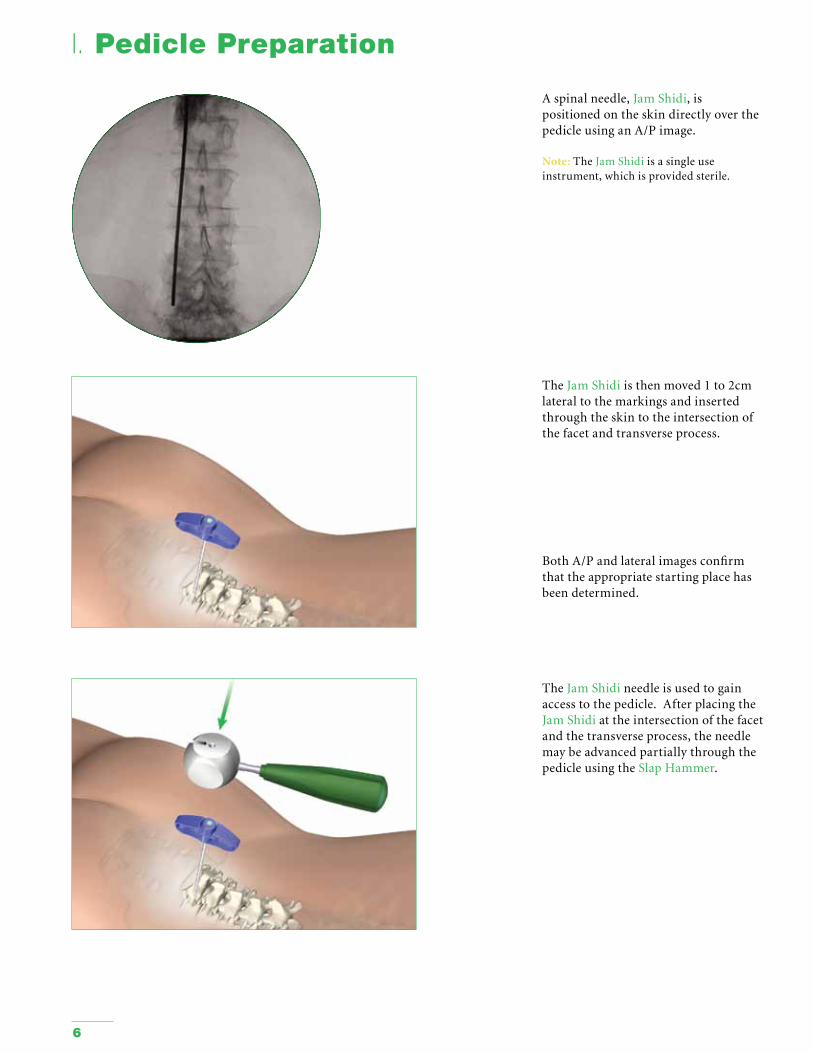
Aspinalneedle,JamShidi,ispositionedontheskindirectlyoverthepedicleusinganA/Pimage.
Note: TheJamShidiisasingleuseinstrument,whichisprovidedsterile.
I. Pedicle Preparation
TheJamShidiisthenmoved1to2cmlateraltothemarkingsandinsertedthroughtheskintotheintersectionofthefacetandtransverseprocess.
BothA/Pandlateralimagesconfirmthattheappropriatestartingplacehasbeendetermined.
TheJamShidineedleisusedtogainaccesstothepedicle.AfterplacingtheJamShidiattheintersectionofthefacetandthetransverseprocess,theneedlemaybeadvancedpartiallythroughthepedicleusingtheSlapHammer.
7
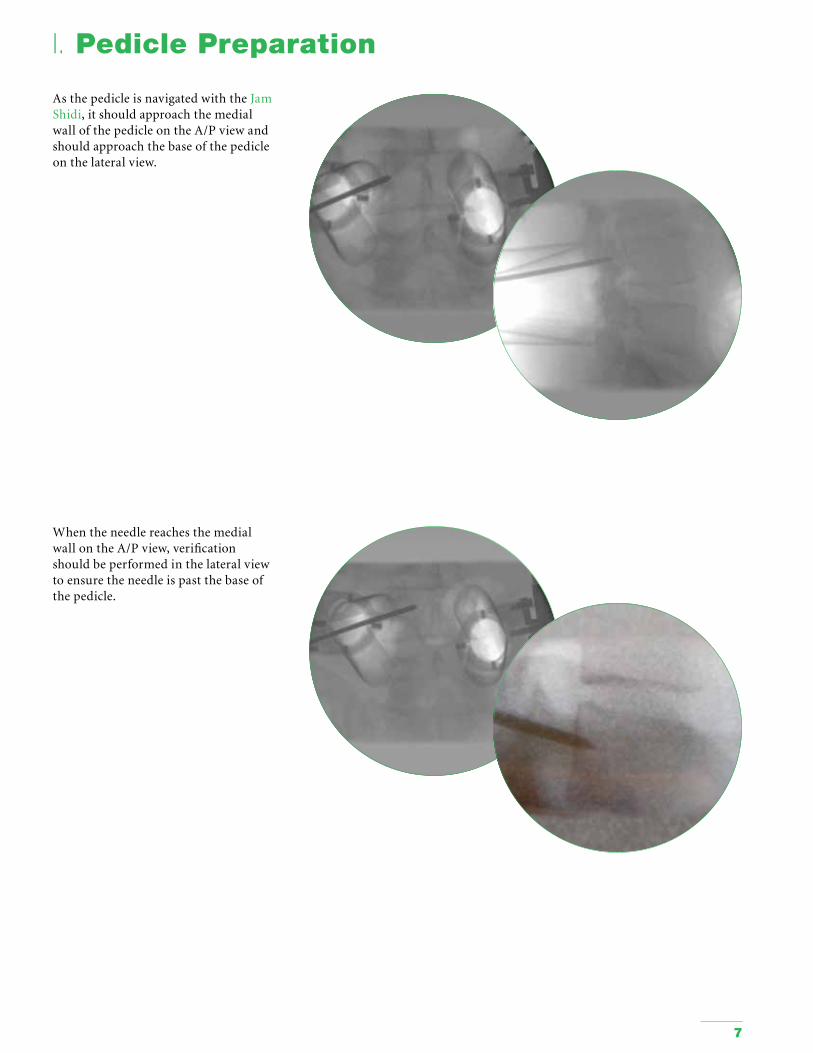
WhentheneedlereachesthemedialwallontheA/Pview,verificationshouldbeperformedinthelateralviewtoensuretheneedleispastthebaseofthepedicle.
I. Pedicle Preparation
AsthepedicleisnavigatedwiththeJamShidi,itshouldapproachthemedialwallofthepedicleontheA/Pviewandshouldapproachthebaseofthepedicleonthelateralview.

8
TheinnertrocaroftheJamShidiisremoved.
I. Pedicle Preparation
TheremovaloftheJamShidiinnertrocarallowstheK-Wire(SharporBlunt)tobeinsertedintothepedicle.
CautionmustbepracticedwithregardtothepositionoftheK-WireinordertoavoidadvancementoftheK-Wire.
Note:TheRadius®K-Wireis1.5mmin
diameter.TheMANTIS®andXia®K-Wireis1.3mmindiameter.
Note:TheK-Wireisasingleuseinstrument.
TheK-WireGuideTubecanbeusedtopreventtheK-Wirefrombendingormovingduringinsertion.PlacetheK-WireGuideTubeovertheK-WireanddockitontheJamShidi.
TheSlapHammercanthenbeusedtoimpacttheK-Wire.

9
ThepedicleispreparedbyplacingtheCannulatedPedicleAwlovertheK-Wireandtwistingitintothepedicle.
HoldtheK-WireinpositionwhenremovingtheAwl.
UsethecannulatedSlapHammertoimpacttheAwl.
Note:TheCannulatedPedicleAwlhasastopat12.0mm.
I. Pedicle Preparation
OncetheK-Wireisinserted,theoutershaftoftheJamShidimayberemoved.
HoldtheK-WireinpositionwhenremovingtheJamShidi.

10
Iftheboneistoohard,theappropriateCannulatedTapmaybeusedtopreparethepediclescrewcanal.
TheRadius®CannulatedTapsarelaseretchedwith10mmintervalstohelpindicatethedepthatwhichtheCannulatedTaphasbeeninsertedaswellastohelpdetermineproperscrewlength.
TheCannulatedTapshavebeencoloredgoldupto40mmtoallowforeasyvisualizationof40mmdepth,whichrepresentsthemostcommonscrewlength.
Note:ThelengthoftheCannulatedTapthreadis25mm.
I. Pedicle Preparation
Note: The1cmintervalmarkingsontheK-Wireprovidethecannulatedinstrument’s
depthinthepedicle.
Asaninstrumentadvancesintothepedicle,theproximalendoftheinstrumentwillmoverelativetothemarkings.IfthisdoesnotoccurduringinsertiontheprocedureshouldbestoppedandfluoroscopyshouldbeusedtoverifythepositionoftheK-WireinrelationtotheAwlorTap.

11
I. Pedicle Preparation
TheTapSleevecanbeusedtopreventsofttissuefromcontactingthethreadsoftheTap.
CheckpedicledepthwitheitherfluoroscopyorreadthedepthfromtheTapSleeveasitmovesalongtheproximalshaftoftheTap.Therearemarkingsat30,40,and50mm.
Note:TheTapSleeveismadeofradiolucentUltemPolyEtherImide.
Note:SlidetheTapSleeveproximaltothe
tapshafttoengagethefrictionfit.
HoldtheK-WireinpositionwhenremovingthePrecisionTap.

12
Withthepediclepathwayspreparedandproperscrewlengthanddiameterdetermined,thescrewisreadyforinsertion.
TheRadius®CannulatedMulti-AngleScrewInserterisdesignedtoprovidearigidconnectionbetweenthepolyaxialscrewandthescrewdriver.Thescrewdrivercanbeattachedtoanyofthecannulatedmodularhandlesusingthequickreleasemechanism.
Cannulated Multi-Angle Screws
ToassembletheCannulatedMulti-AngleScrewInserter:1.InserttheinnershaftthroughthebodyoftheCannulatedMulti-AngleScrewInserter.2.InserttheratchetdowntheshaftoftheCannulatedMulti-AngleScrewInserter.Verifythattheratchetisbottomedout.3.Connecttothedesiredhandle.4.EnsurethattheCannulatedMulti-AngleScrewInserterisfullyunlocked.5.AlignthetabsontheCannulatedMulti-AngleScrewInsertershaftwiththeexternalquadonthescrewheadwhileholdingthebonescrew.6.RotatethedialontheCannulatedMulti-AngleScrewInserterclockwisetofirmlyseatthescrewontotheCannulatedMulti-AngleScrewInserter.
II. Screw Insertion
Step 1
Step 2
Step 3
Step 4
Cannulated Multi-Angle Screw Inserter
13
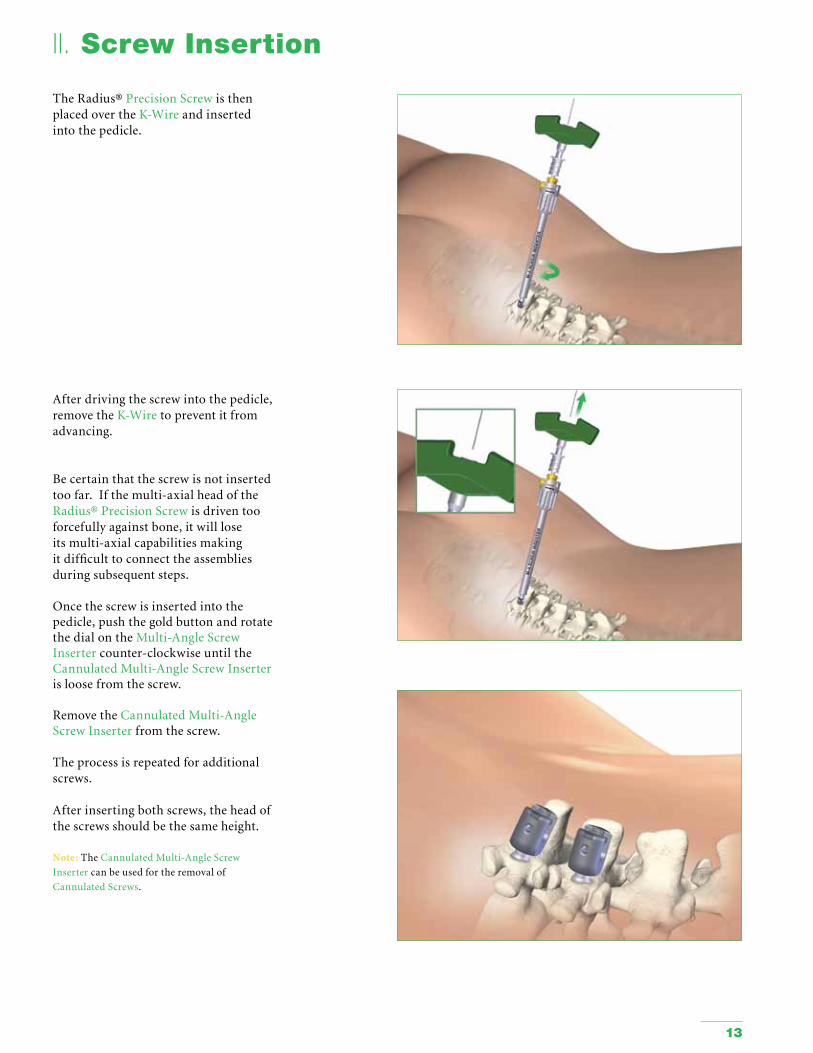
TheRadius®PrecisionScrewisthenplacedovertheK-Wireandinsertedintothepedicle.
II. Screw Insertion
Afterdrivingthescrewintothepedicle,removetheK-Wiretopreventitfromadvancing.
Becertainthatthescrewisnotinsertedtoofar.Ifthemulti-axialheadoftheRadius®PrecisionScrewisdriventooforcefullyagainstbone,itwillloseitsmulti-axialcapabilitiesmakingitdifficulttoconnecttheassembliesduringsubsequentsteps.
Oncethescrewisinsertedintothepedicle,pushthegoldbuttonandrotatethedialontheMulti-AngleScrewInsertercounter-clockwiseuntiltheCannulatedMulti-AngleScrewInserterisloosefromthescrew.
RemovetheCannulatedMulti-AngleScrewInserterfromthescrew.
Theprocessisrepeatedforadditionalscrews.
Afterinsertingbothscrews,theheadofthescrewsshouldbethesameheight.
Note:TheCannulatedMulti-AngleScrew
Insertercanbeusedfortheremovalof
CannulatedScrews.

IV. Final Tightening
14
AfterverifyingwithA/P,lateral,andobliqueviewsthattherodisseatedintheheadsofbothscrews,theLockingCapmustbeinsertedintothescrewheadusingtheInitialInserter.ApplydownwardpressuretoensuretheLockingCapisfirmlyseatedagainsttherod,thenturntheLockingCaptoitsprovisionallylockedposition.TheLockingCapisprovisionallylockedwhenthelaseretchedlinesontheLockingCapareparalleltotherod.
Note:TheInitialInserterTubecanbeusedtoguidetheLockingCapintothescrewhead.
Tip:Itisrecommendedtobeginclosureattheeasiestpointintheconstruct.Thismayhelpfacilitatetheseatingoftherodinadjacentimplants.
Whenarodthatissittingslightlyproudisforceddownduringtightening,ensurethatthelockingcapisfullyengagedintothescrewhead.Thiswillhelpresistthehighreactiveforcesgeneratedduringfinaltightening.
Extra caution is advised when:1. Therodisnothorizontallyplaced intothescrewhead.2. Therodishighinthescrewhead.3. Anacuteconvexorconcavebend iscontouredintotherod.
III. Rod Insertion
Oncetherodisbenttothedesiredcontour,itisplacedintothetulipheadsofthescrewusingarodinserter.
15
IV. Final Tightening
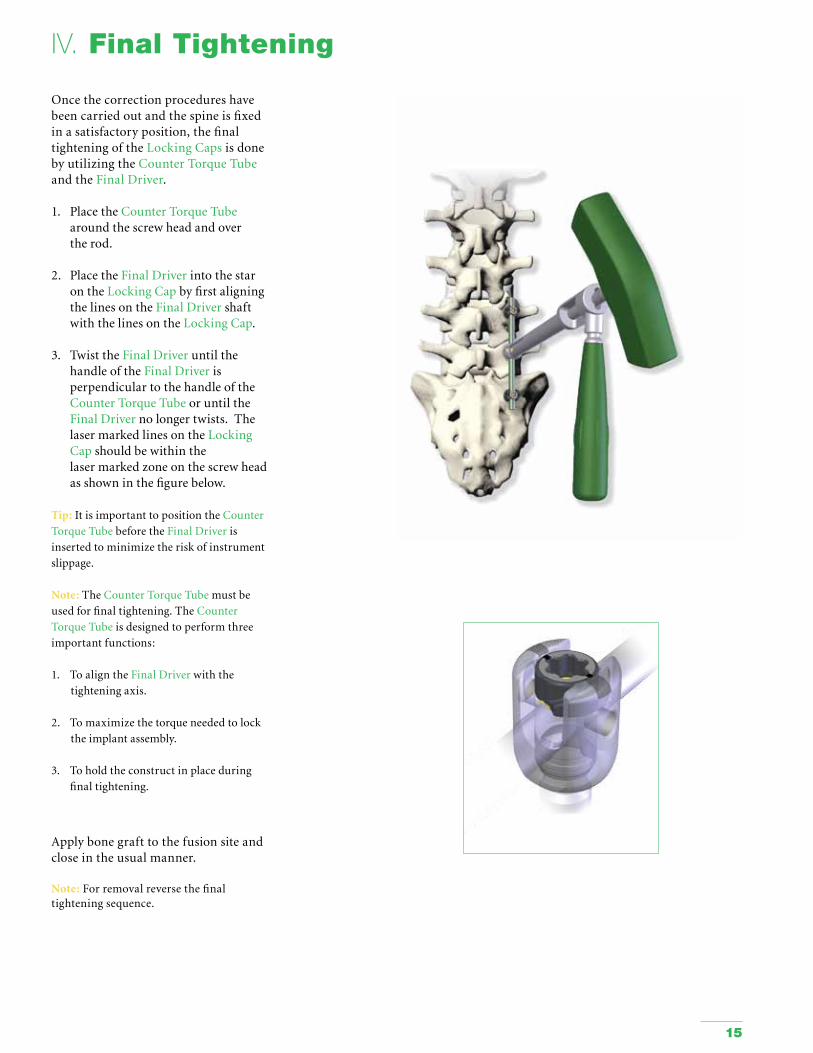
Oncethecorrectionprocedureshavebeencarriedoutandthespineisfixedinasatisfactoryposition,thefinaltighteningoftheLockingCapsisdonebyutilizingtheCounterTorqueTubeandtheFinalDriver.
1. PlacetheCounterTorqueTube aroundthescrewheadandover therod.
2. PlacetheFinalDriverintothestar ontheLockingCapbyfirstaligning thelinesontheFinalDrivershaft withthelinesontheLockingCap.
3. TwisttheFinalDriveruntilthe handleoftheFinalDriveris perpendiculartothehandleofthe CounterTorqueTubeoruntilthe FinalDrivernolongertwists.The lasermarkedlinesontheLocking Capshouldbewithinthe lasermarkedzoneonthescrewhead asshowninthefigurebelow.
Tip:ItisimportanttopositiontheCounter
TorqueTubebeforetheFinalDriveris
insertedtominimizetheriskofinstrument
slippage.
Note:TheCounterTorqueTubemustbe
usedforfinaltightening.TheCounter
TorqueTubeisdesignedtoperformthree
importantfunctions:
1. ToaligntheFinalDriverwiththe
tighteningaxis.
2. Tomaximizethetorqueneededtolock
theimplantassembly.
3. Toholdtheconstructinplaceduring
finaltightening.
Applybonegrafttothefusionsiteandcloseintheusualmanner.
Note:Forremovalreversethefinaltighteningsequence.

Par t number Descript ion
486610000 Locking Cap
4866125 (35) - (50)Screw, Multi-Angle, Cannulated Ø5.75 x 35mm-50mm
4866126 (30) - (55)Screw, Multi-Angle, Cannulated Ø6.75 x 30mm-55mm
4866127 (30) - (55)Screw, Multi-Angle, Cannulated Ø7.75 x 30mm-55mm
4866150 (30) - (90)Ø5.5mm Titanium Rad Rod30mm-90mm lengths
4866155 (50) - (80)Ø5.5mm Titanium Max Rad Rod50mm-80mm lengths
Implants
16
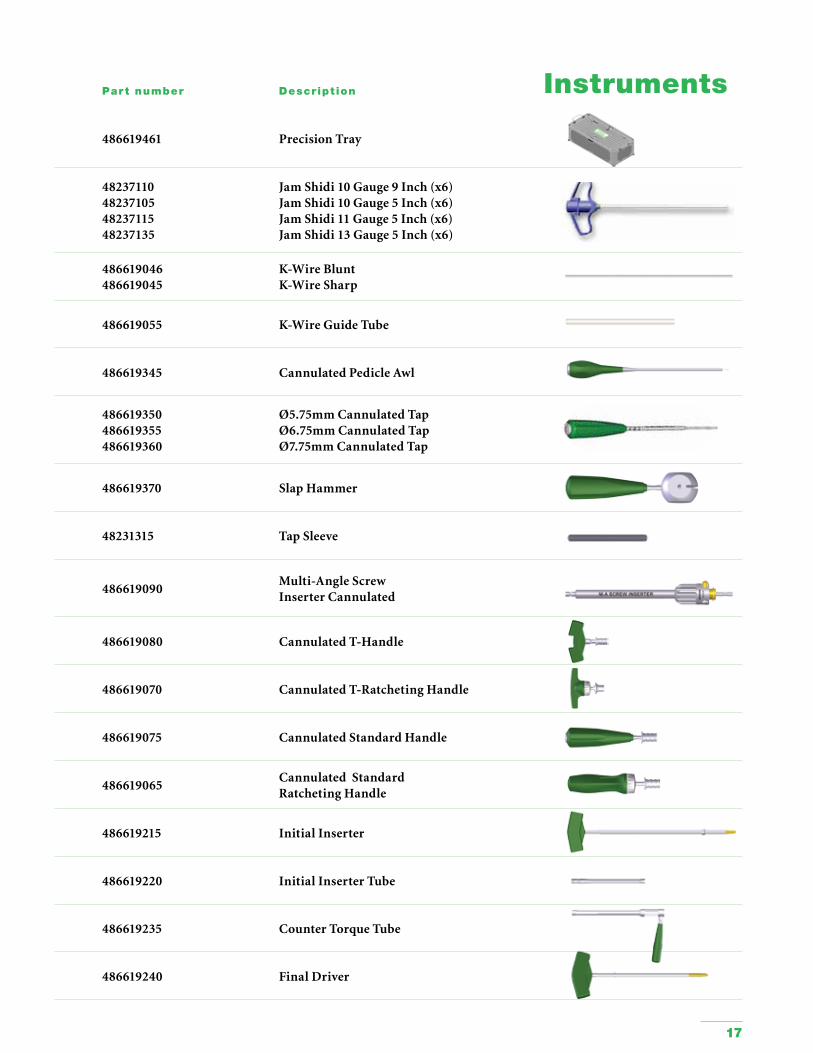
Par t number Descript ion
486619461 Precision Tray
48237110482371054823711548237135
Jam Shidi 10 Gauge 9 Inch (x6) Jam Shidi 10 Gauge 5 Inch (x6) Jam Shidi 11 Gauge 5 Inch (x6) Jam Shidi 13 Gauge 5 Inch (x6)
486619046486619045
K-Wire BluntK-Wire Sharp
486619055 K-Wire Guide Tube
486619345 Cannulated Pedicle Awl
486619350486619355486619360
Ø5.75mm Cannulated TapØ6.75mm Cannulated TapØ7.75mm Cannulated Tap
486619370 Slap Hammer
48231315 Tap Sleeve
486619090Multi-Angle Screw Inserter Cannulated
486619080 Cannulated T-Handle
486619070 Cannulated T-Ratcheting Handle
486619075 Cannulated Standard Handle
486619065Cannulated Standard Ratcheting Handle
486619215 Initial Inserter
486619220 Initial Inserter Tube
486619235 Counter Torque Tube
486619240 Final Driver
Instruments
17

18
IndicationsTheRadius®SpinalSystemisintendedforuseinthenoncervicalspine.Whenusedasananterior/anterolateralandposterior,noncervicalpedicleandnon-pediclefixationsystem,theRadius®SpinalSystemisintendedtoprovideadditionalsupportduringfusionusingautograftorallograftinskeletallymaturepatientsinthetreatmentofthefollowingacuteandchronicinstabilitiesordeformities:• Degenerativediscdisease(DDD)(definedasbackpainofdiscogenicoriginwithdegenerationofthediscconfirmedby
historyandradiographicstudies);• Spondylolisthesis;• Trauma(i.e.,fractureordislocation);• Spinalstenosis;• Curvature(i.e.,scoliosis,kyphosis,and/orlordosis);• Tumor;• Pseudoarthrosis;and• Failedpreviousfusion.TheRadius®SpinalSystemcanalsobelinkedtotheXia®TitaniumSpinalSystemviatheØ5.5mmtoØ6.0mmRadius®rod-to-rodconnector.
ContraindicationsContraindicationsmayberelativeorabsolute.Thechoiceofaparticulardevicemustbecarefullyweighedagainstthepatient’soverallevaluation.Circumstanceslistedbelowmayreducethechancesofasuccessfuloutcome:• Anyabnormalitypresentwhichaffectsthenormalprocessofboneremodelingincluding,butnotlimitedto,severe osteoporosisinvolvingthespine,boneabsorption,osteopenia,primaryormetastatictumorsinvolvingthespine,active infectionatthesiteorcertainmetabolicdisordersaffectingosteogenesis.• Insufficientqualityorquantityofbonewhichwouldinhibitrigiddevicefixation.• Previoushistoryofinfection.• Excessivelocalinflammation.• Openwounds.• Anyneuromusculardeficitwhichplacesanunusuallyheavyloadonthedeviceduringthehealingperiod.• Obesity.Anoverweightorobesepatientcanproduceloadsonthespinalsystemwhichcanleadtofailureofthe fixationofthedeviceortofailureofthedeviceitself.• Patientshavinginadequatetissuecoverageoftheoperativesite.• Pregnancy.• Aconditionofsenility,mentalillness,orsubstanceabuse.Theseconditions,amongothers,maycausethe patienttoignorecertainnecessarylimitationsandprecautionsintheuseoftheimplant,leadingtofailure,or othercomplications.• Foreignbodysensitivity.Wherematerialsensitivityissuspected,appropriatetestsshouldbemadepriorto materialselectionorimplantation.• Othermedicalorsurgicalconditionwhichwouldprecludethepotentialbenefitofspinalimplantsurgery,such asthepresenceoftumors,congenitalabnormalities,elevationofsedimentationrateunexplainedbyother diseases,elevationofwhitebloodcellcount(WBC),ormarkedleftshiftintheWBCdifferentialcount.Thesecontraindicationscanberelativeorabsoluteandmustbetakenintoaccountbythephysicianwhenmakingadecision.Theabovelistisnotexhaustive.
19
Cautions and WarningsCAUTIONS (U.S.A.)Federallaw(U.S.A)restrictsthisdevicetosalebyorontheorderofalicensedphysician.Theimplantationofpediclescrewspinalsystemsmustbeperformedonlybyexperiencedspinalsurgeonswithspecifictrainingintheuseofthispediclescrewspinalsystembecausethisisatechnicallydemandingprocedurepresentingariskofseriousinjurytothepatient.Basedonthefatiguetestingresults,thephysician/surgeonmustconsiderthelevelsofimplantation,patientweight,patientactivitylevel,otherpatientconditions,etc.,whichmayimpactontheperformanceofthesystem.
WARNING (U.S.A.)Thesafetyandeffectivenessofpediclescrewspinalsystemshavebeenestablishedonlyforspinalconditionswithsignificantmechanicalinstabilityordeformityrequiringfusionwithinstrumentation.Theseconditionsaresignificantmechanicalinstabilityordeformityofthethoracic,lumbar,andsacralspinesecondarytospondylolisthesis(grades3and4)oftheL5-S1vertebrae,degenerativespondylolisthesiswithobjectiveevidenceofneurologicalimpairment,fracture,dislocation,scoliosis,kyphosis,spinaltumor,andfailedpreviousfusion(pseudoarthrosis).Thesafetyandeffectivenessofthesedevicesforanyotherconditionsareunknown.Radius®implantcomponentshavenotbeentestedforheatingormigrationinMRenvironment.
Removal of ImplantsTheseimplantsaretemporaryinternalfixationdevicesdesignedtostabilizetheoperativesiteduringthenormalhealingprocess.Afterhealingoccurs,thesedevicesservenofunctionalpurposeandcanberemoved.Removalmayalsoberecommendedinothercases,suchas:• Corrosionwithapainfulreaction• Migrationoftheimplant,withsubsequentpainand/orneurological,articularorsofttissuelesions• Painorabnormalsensationsduetothepresenceoftheimplants• Infectionorinflammatoryreactions• Reductioninbonedensityduetothedifferentdistributionofmechanicalandphysiologicalstressesandstrains• FailureormobilizationoftheimplantStandardancillariesprovidedbyStrykerSpinecanbeusedtoremovetheimplants.Anydecisionbyaphysiciantoremovetheinternalfixationdevicemusttakeintoconsiderationsuchfactorsastherisktothepatientoftheadditionalsurgicalprocedureaswellasthedifficultyofremoval.Removalofanunloosenedspinalscrewmayrequiretheuseofspecialinstrumentstodisrupttheinterfaceattheimplantsurface.Thistechniquemayrequirepracticeinthelaboratorybeforebeingattemptedclinically.Implantremovalmustbefollowedbyadequatepostoperativemanagementtoavoidfractureorre-fracture.Removaloftheimplantafterfracturehealingishighlyrecommended.Metallicimplantscanloosen,bend,fracture,corrode,migrate,causepainorstressshieldbone.
Information for PatientsThesurgeonmustdiscussallphysicalandpsychologicallimitationsinherenttotheuseofthedevicewiththepatient.Thisincludestherehabilitationregimen,physicaltherapy,andwearinganappropriateorthosisasprescribedbythephysician.Particulardiscussionshouldbedirectedtotheissuesofprematureweightbearing,activitylevels,andthenecessityforperiodicmedicalfollow-up.Thepatientmustbewarnedofthesurgicalrisksandmadeawareofpossibleadverseeffects.Thepatientmustbewarnedthatthedevicecannotanddoesnotreplicatetheflexibility,strength,reliabilityordurabilityofnormalhealthybone,thattheimplantcanbreakorbecomedamagedasaresultofstrenuousactivityortrauma,andthatthedevicemayneedtobereplacedinthefuture.Ifthepatientisinvolvedinanoccupationoractivitywhichappliesinordinatestressupontheimplant(e.g.,substantialwalking,running,lifting,ormusclestrain)he/sheshouldbewarnedthatresultantforcescancausefailureofthedevice.Patientswhosmokehavebeenshowntohaveanincreasedincidenceofnon-unions.Suchpatientsshouldbeadvisedofthisfactandwarnedofthepotentialconsequences.Fordiseasedpatientswithdegenerativedisease,theprogressionofdegenerativediseasemaybesoadvancedatthetimeofimplantationthatitmaysubstantiallydecreasetheexpectedusefullifeoftheappliance.Insuchcases,orthopaedicdevicesmaybeconsideredonlyasadelayingtechniqueortoprovidetemporaryrelief.
REUSENeverreuseorreimplantspinalsurgicalimplants.Thesecouldbecomecontaminatedresultingininfection.Inaddition,eventhoughthedeviceappearsundamaged,itmayhavesmalldefectswhichcouldcompromisestructuralintegrityreducingitsservicelifeand/orleadingtopatientinjury.Itisrecommendedtoverifythattheinstrumentsareingoodconditionandoperatingorderpriortouseduringsurgery.
US Operations2 Pearl Court,Allendale, New Jersey 07401 - USAt: +1 201 760 8000f: +1 201 760 8108
www.stryker.com
EU OperationsZ.I. Marticot33610 Cestas, FRANCEt: +33 (0)5 57 97 06 30f: +33 (0)5 57 97 06 31
www.stryker.com
Asurgeonmustalwaysrelyonhisorherownprofessionalclinicaljudgmentwhendecidingwhethertouseaparticularproductwhentreatingaparticularpatient.Strykerdoesnotdispensemedicaladviceandrecommendsthatsurgeonsbetrainedintheuseofanyparticularproductbeforeusingitinsurgery.
TheinformationpresentedisintendedtodemonstratethebreadthofStrykerproductofferings.Asurgeonmustalwaysrefertothepackageinsert,productlabeland/orinstructionsforusebeforeusinganyStrykerproduct.Productsmaynotbeavailableinallmarketsbecauseproductavailabilityissubjecttotheregulatoryand/ormedicalpracticesinindividualmarkets.PleasecontactyourStrykerrepresentativeifyouhavequestionsabouttheavailabilityofStrykerproductsinyourarea.
StrykerCorporationoritsdivisionsorothercorporateaffiliatedentitiesown,useorhaveappliedforthefollowingtrademarksorservicemarks:Mantis®,Radius®,Stryker®,Xia®.Allothertrademarksaretrademarksoftheirrespectiveownersorholders.
LiteratureNumber:TLRADST08062SCGS07/10
Copyright©2010StrykerPrintedinUSA