spinal cord injury without radiographic -
TRANSCRIPT
RESEARCH REVIEW
Spinal Cord Injury without RadiographicAhdnormalities SCIWORASynopsis by: William J. Owens, DC, DAAMLP
Mark E, Studin, DC, FASBE(C), DAAPM, DAAMLP
USE: To demonstrate the importance of thorough diagnostic exarrif-
nation of trauma patients.
TITLE: The Adult Spinal Cord Injury Without Radiographic Abnor-
malities Syndrome: Magnetic Resonance Imaging and Ciinical
Findings in Adults with Spinal Cord Injuries Having Normal
Radiographs and Computed Tomography Studies
CITATION: J Trauma. 2008; 65:86-93.
AUTHORS: Georglos B. Kasimatis, MD; Ellas Panagíotopoulos, MD, PhD;
Panagiotis Megas, MD, PhD; Charalambos Matzaroglou, MD;
John Gliatis, MD, PhD; Minos Tyliianakis, MD, PhD; and Elias
Lambiris, MD, PhD.
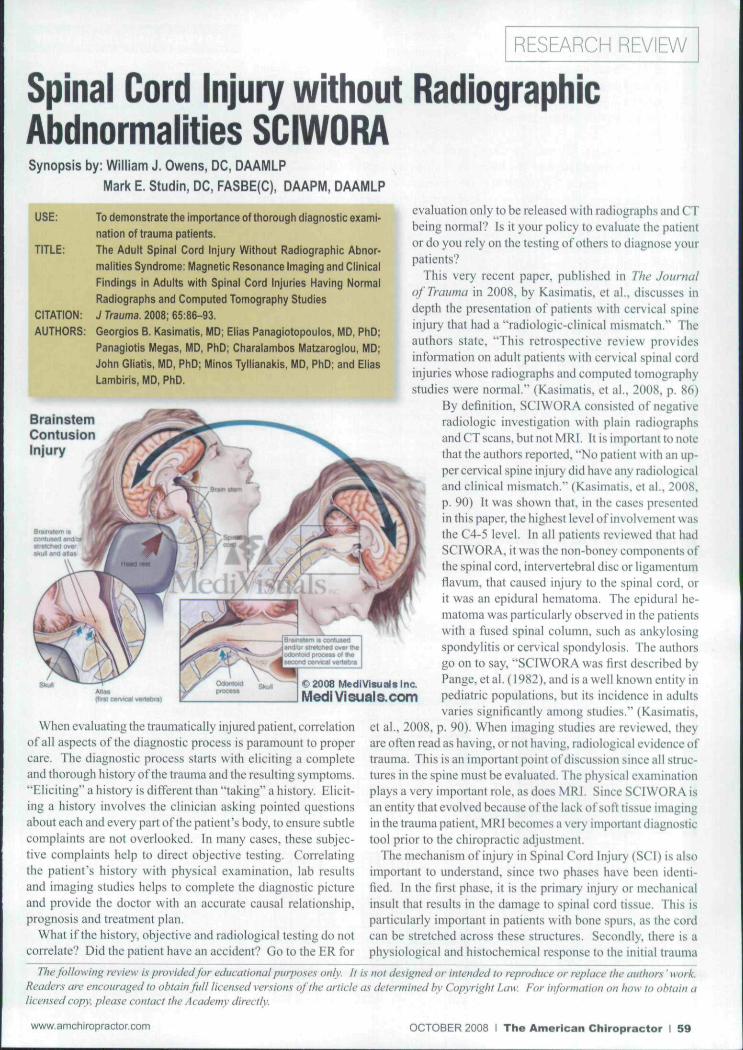
Brain StemContusionInjury
MedJVisualslnc.
MediVisual3.com
When evaluating the traumatically injured patient, correlationof all aspects of the diagnostic process is paramount to propercare. The diagnostic process starts with eliciting a completeand thorough history of the trauma and the resulting symptoms."Eliciting" a history is different than "taking" a history. Elicit-ing a history involves the clinician asking pointed questionsabout each and every part of the patient's body, to ensure subtlecomplaints are not overlooked. In many cases, these subjec-tive complaints help to direct objective testing. Correlatingthe patient's history with physical examination, tab resultsand imaging studies helps to complete the diagnostic pictureand provide the doctor with an accurate causal relationship,prognosis and treatment plan.
What if the history, objective and radiological testing do notcorrelate? Did the patient have an accident? Go to the HR for
evaluation only to be released with radiographs and CTbeing normal? Is it your policy to evaluate the patientor do you rely on the testing of others to diagnose yourpatients?
This very recent paper, published in The Journalof Trauma in 2008, by Kasimatis. et al., discusses indepth the presentation of patients with cervical spineinjury that had a "radiologic-clinical mismatch." Theauthors state, "This retrospective review providesinformation on adult patients with cervical spinal cordinjuries whose radiographs and computed tomographystudies were nomial." {Kasimatis, et al., 2008. p. 86)
By definition, SCIWORA consisted of negativeradiologie investigation with plain radiographsand CT scans, but not MRI. It is important to notethat the authors reported, "No patient with an up-per cervical spine injur>' did have any radiologicaland clinical mismatch." {Kasimatis. et al.. 2008,p. 90) It was shown that, in the cases presentedin this paper, the highest level of involvement wasthe C4-5 level, ln all patients reviewed that hadSCIWORA. it was the non-boney components ofthe spinal cord, intenertebral disc or ligamentumflavum, that caused injury to the spinal cord, orit was an epidural hematoma. The epidural he-matoma was particularly observed in the patientswith a fused spinal column, such as ankylosingspondylitis or cervical spondylosis. The authorsgo on to say. "SCIWORA was first described byPange, et al. ( 1982). and is a well known entity inpédiatrie populations, but its incidence in adultsvaries significantly among studies." {Kasimatis,
et al.. 2008. p. 90). When imaging studies are reviewed, theyarc often read as having, or not having, radiological evidence oftrauma. This is an important point of discussion since all struc-tures in the spine must be evaluated. The physical examinationplays a very important role, as does MRI. Since SCIWORA isan entity that evolved because of the lack of soft tissue imagingin the trauma patient, MRI becomes a very important diagnostictool prior to the chiropractic adjustment.
The mechanism of injtiry in Spinal Cord Injury (SCI) is alsoimportant to understand, since two phases have been identi-fied. In the first phase, it is the primary injury or mechanicalinsult that results in the damage to spinal cord tissue. This isparticularly important in patients with bone spurs, as the cordcan be stretched across these structures. Secondly, there is aphysiological and histochemical response to the initial trauma
The following review is provided for educational purposes only. It is not designed or intended to reproduce or replace ihe authors ' work.Readers are encouraged to obtain full licen.sed version.s of the anide as determined by Copyright Law. For information on how to obtain a
py, please contact the Academy directly.
www.amchiropractor.com OCTOBER 2008 I The American Chiropractor I 59
that causes further damage to the spinalcord, "...among which free radical forma-tion, vascular disttirbances and apoptosisare the principal ones." (Kasimatis, et a!..2008. p. 91).
This study reports some interestingfinal points:1. "A rate of around 5% may be con-
sidered as representative of the tmeincidence of cervical SWIWORA."(Kasimatis, et al., 2008. p. 90).
2. "Children beiow 8 years and the el-derly above 60 are mostly affected,but the two populations have differentcharacteristics." (Kasimatis. et al.,2008, p. 90). In children, the dispro-portionate size of the head related tothe neck causes excessive injury, whilein the elderly it has more to do v ithpre-existing degenerative changes andloss of disc height. Since the pre-exist-ing changes in the spine are the issue,consideration of this phenomenonin any patient that has pre-existingchanges in the spine, regardless of age,is appropriate.
3. "... .the physician dealing with a pos-sible SCIWORA patient should be
aware that the correlation of physicalexamination with the radiologicalstudies is mandatory, and he shouldperform MRI in all cases."" (Kasimatis,etal.,2008, p. 92)
When evaluating patients that are trau-matically injured, correlation of all clini-cal findings is mandatory, especially priorlo chiropractic adjustment. In the caseof spinal cord compromise, direct andspeedy neurosurgical referral is critical.
Each issue, a clinical topic will be providedby Drs. Mark Studin & William J. Owens ofthe American Academy of Medical Legal Pro-fe.Ksionats (AA MLP), which is a national non-profit oi'ganizafion comprised of doctors andlawyers. The purpose oj the organization is toprovide its members with current research intrauma and spinal-related topics to keep theprofe.ssional on file cutting edge of healfhcarc.Members may also sit for a Diplomate ex-amination and be conferred a DA A MLP. Theorganization also offers .support to the indi-vidual member s practice. To team more, go towww.aamlp.org or call f-7!6-22H-3847.\
Crossword Puzzle Answers
Al
T
U
N
1
T
U
P
B
{^
p
jgust Is
J
sue
M A R K
U
EG
U
L
A
T
^
N
S
A
0 F 1 C
L fA)N
1 1 D
C
r
E
R C
S
,P
1
N
A
L
Ü
t
,C,
0
M
P
R
E
S
S
1
0N
T M
E N
G 1
L 1
R E
C \R)
T
E
R
A
P
E
U
T
1
C
E
X
L
R
, -1
E
T
R
A
N
E
D
E
|T
S
R
A
Y
D E
N
E
W
E
A
L
A
N
D
G
S
P
CT'
N
M
E;D
1
{C,A
L
L
Y
N
E
C
E
5
S
A
R
Y
V
V
r 1 A
~
0
W
T
E
C
ïï:
B
L
00
F
1
E
L
D
September Issue
M 1 G R
SH0E
TAND1NG
B
U
E
s|^p)
R 0
TITR)
0 D 1
ARCH1V1NGFUNC
T10N
1 NtE
T R U M
N
X
T
E
A
THYR01D
F
L
E
0
E
N
"R"
N
E
E
B
SADERS
RESP0NS
L
E
V
T
THREE
C0UR
SGE
1
G0A
¿¿x'
ADVERTISING DIRECTORY
RS#
50
68
19
N/A
86
10
78
83
69
22
5
36
37
26
95
17
76
59
2
4
98
23
55
31
52
88
N/A
57
43
38
72
81
64
21
35
13
29
27
67
16
54
49
99
42
N/A
73
ADVERTISER
3 Care Therapeutics. LLC
Access Heatlh Consultants
AC Grace
AMC
Amrex- Zetron
Antalgic Trak
Anthony Robbins
Atrium
Axiom Worldwide
Biopharma Scientific
Bonaparte Galleries
Breakthrough Coaching
Chiropractie Leadership Alliance
Chirotouch
Chopra Centers
CMCS
Demartini Seminars
Disc Force
Douglas Laboratories
Enzyme Formulations
Eon Systems
Erchonia
Fernandez Consultiing
Foot Levelers
Footmaxx
F4CP
Freedom Awaits
Human Touch. Lie
Impac
!n Phase Technologies
Integrated Orthotics Labs
King Bio
Kool N' Fit
Leander Health Tech
Life West University
Matlin
Multi Radiance
Nutri-West
Oxyhealth Inc-
Parker College Of Chiropractic
PBI / Myovision
Sombra
Stately Creations
Texas Beautiful Image, Inc.
Ulan Nutritional Systems
Universal Del Medical
Pt)/;
30
18
7
BB
51
27
48
1
28
43
28
30,31
C4
33
52
54
31
21
3.25
37
24
5
56
02,23
C3
61
11
39
44,45
9
17
29
48
2
57
47
36
13
16
53
49
41
18
38
19
56
60 I The American Chiropractor I OCTOBER 2008 www.amchiropractor.com
