souvenir - ewubd.edu · souvenir international conference on physics in medicine and clinical...
TRANSCRIPT


SOUVENIR
INTERNATIONAL CONFERENCE ON PHYSICS IN MEDICINE AND
CLINICAL NEUROELECTROPHYSIOLOGY
PMCN2015
19-20 February, 2015 Dhaka, Bangladesh
<www.pmcn2015.info>
Venue
Nabab Nawab Ali Chowdhury Senate Bhaban
University of Dhaka
Organised by
Bangladesh Medical Physics Association (BMPA)
Bangladesh Clinical Neuro Electrophysiologist Society (BCNEPS)
Dept of Biomedical Physics & Technology (BMPT) University of Dhaka
Endorsed by
International Organisation of Medical Physics (IOMP)
American Association of Physicists in Medicine (AAPM)
Cover design: Prof K Siddique-e Rabbani Cover picture acknowledgement: web.mediamit.edu, its.uvm.edu, www.ob-ultrasound.net

I

II

III
IV
V

VI

VII

VIII

IX
X
XI

XII

XIII

XIV

XV

PROGRAMME &
ABSTRACTS

INTERNATIONAL CONFERENCE ON PHYSICS IN MEDICINE AND
CLINICAL NEUROELECTROPHYSIOLOGY (PMCN-2015)
19-20 February, 2015
Dhaka, Bangladesh
Venue: Nabab Nawab Ali Chowdhury Senate Bhaban, University of Dhaka
Registration : Lobby of Seminar room (1
st floor)
Inauguration : Main Auditorium (2nd
floor)
Scientific Sessions I – VII (Tack I) : Main Auditorium (2nd
floor)
Scientific Sessions I – VII (Tack II) : Conference room (1st floor)
Exhibition : Outside Lobby (1st floor)
Food and snacks : Dining Hall (1st floor)
Plenary Session : Main Auditorium (2nd
floor) AGM (BMPA) : Main Auditorium (2
nd floor)
AGM (BCNEPS) : Conference room (1st floor)
Schedule
19 February 2015 08:00 – 08:30 Registration
08:30 – 09:50 Scientific Session I (Track I, II)
10:00 – 11:20 Inauguration Ceremony
11:21 – 11:45 Refreshment
11:46 – 13:15 Scientific Session II (Track I, II)
13:16 – 14:30 Special Lunch & Prayer break
14:31 – 16:00 Scientific Session III (Track I, II)
16:01 – 17:00 Scientific Session IV (Track I, II)
17:01 – 17:15 Tea break & Prayer break
17:16 – 18:20 Scientific Session V (Track I, II)
20 February 2015
08:30 – 10:15 Scientific Session VI (Track I, II)
10:16 – 10:30 Tea Break
10:31 – 12:30 Scientific Session VII (Track I, II)
12:31 – 14:00 Lunch & Prayer break
14:01 – 16:00 Plenary Session
16:01 – 17:00 Open Floor Discussion
17:01 – 17:10 Certificate Distribution to Volunteers
17:11 – 17:30 Closing Tea
17:16 – 18:20 Annual General Meeting (AGM)
BMPA & BCNEP
Inauguration Ceremony & Opening of Exhibition
10:00: Welcome Address by Dr. Kamila Afroj Quadir, Secretary – I, Organizing Committee
10:05: Theme Lecture – 1 by Professor Sadiq R Malik, Chief Radiation Oncology Physicist, Delta
Medical College & Hospital, Dhaka.
10:15: Theme Lecture – 2 Address by Professor Naila Zaman Khan, Head, Dept of Pediatric
Neurosciences, Dhaka Shishu (Children‘s) Hospital and President, BCNEPS
10:25 Theme Lecture – 3 Address by Professor K Siddique-e Rabbani, President, BMPA, &
Chairperson, Dept. of BMPT, University of Dhaka
10:35: Award for Pioneering Research in Medical Physics in Bangladesh to Dr. Abdus Sattar Syed
10:40: Award for Lifetime contribution in Medical Physics to Dr Syed Reza Husain
10:45 Address by Mr. Mir Mahaboob Ali, Special Guest, Managing Director, Tradevision Ltd.
10:50: Address by Prof Syed Mukarram Ali, Special Guest, Chairman, Delta Medical College &
Hospital, Dhaka.
10:55: Address by Dr M R Khan, Chief Guest, National Professor, Bangladesh
11:05: Address by Professor K Siddique-e Rabbani, Co-Chair, Organizing Committee, President,
BMPA, & Chairperson, Dept. of BMPT, University of Dhaka
11:15: Vote of thanks by Dr. Nahid Nabi, Secretary-II, Organizing Committee
11:20: Refreshment

PMCN-2015: Programme
19 February, 2015, Thursday
From 8:00 am: Registration
8:30 - 9:50 am: Scientific Session – I (80 mins) TRACK-I (Main Hall)
TRACK –II (Conference Room)
Paper
ID Presenter Paper Title
Paper
ID Presenter Paper Title
RT-1 M.N. Sharmin Performance of the First ELEKTA Precise Linear Accelerator in Bangladesh
CN-1
Naheed Nabi
Recognizing normal Electrophysiological criteria and deviation to dysfunction in neonates
RT-2 Md. Anisuzzman Bhuiyan
Influence of Jaw tracking in Intensity Modulated and
Volumetric Modulated Arc Radiotherapy for Head and Neck
Cancers – A Dosimetric Study
CN-2 Mosiul Azam Co-relation of Neurodevelopmental status, seizures, EEG and neuroimaging findings of children having neurological problem
RT-3 Mahmud Hassan
Low Cost Proton Therapy for the Cancer Patients
CN-3
Shahjahan
Chowdhury Variation of Electroencephalographic Pattern in West syndrome
Invited
IPM-1 Saiful Huq, USA
Radiation therapy: state of the art and the future
(Through Skype Link + VIDEO, 50 min)
CN-4 Sahifa Nazia Role of EEG in children with febrile seizures.
CN-5 Kaniz Fatema Clinical Spectrum, Electrophysiologic Profile and Medical Treatment of Children with Nonconvulsive Status Epilepticus.
CN-6 Abu Saleh Musa Portable EEG service and epilepsy camps to reach the unreached
CN-7 Shanta Yesmin
Reporting the multiple EEG findings and clinical outcome in
children with and without overt seizure
CN-8
Khondakar Mamun
Dynamic Topographic Visualization and quantification of a
multichannel surface EMG grid array
Invited
ICN-1
Rahsan Gocmen,
Turkey
Technical aspect of neuroradiology and their clinical evaluation in
children presenting with seizures and neurodevelopmental comorbidities
(Proxy presentation-20 min)
10:00 - 11:20: INAUGURATION (80 mins) 10:00
10:05
10:15
10:25
10:35
10:40
10:45
10:50
10:55
11:05
11:15
Welcome Address Theme Lecture-1
Theme Lecture-2
Theme Lecture-3
Award
Award
Address, Special Guest
Address, Special Guest
Address, Chief Guest
Address, Co-Chair
Vote of Thanks
Dr. Kamila Afroj Quadir, Secretary-I, Organising Committee Role Of Medical Physicists In Nuclear Medicine, Radiology & Imaging And Radiotherapy Services, by Professor Sadiq R Malik, Chief Radiation Oncology Physicist, Delta
Medical College & Hospital, Dhaka.
Low Cost High Quality Technology Based Health Service For The Resource Poor Countries; Our Experience, by Professor Naila Zaman Khan, Head, Dept of Pediatric
Neurosciences, Dhaka Shishu (Children‘s) Hospital and President, BCNEPS
Empowering People - Developing Indigenous Design And Manufacture Capability For Medical Devices In Low Resource Countries For Affordable And Sustained Solution, by
Professor K Siddique-e Rabbani, Professor & Chairperson, Dept of BMPT, Dhaka University and President, BMPA Award for Pioneering Research in Medical Physics in Bangladesh to Dr. Abdus Sattar Syed
Award for Lifetime contribution in Medical Physics to Dr Syed Reza Husain
Mr. Mir Mahaboob Ali, Managing Director, Tradevision Ltd. Prof Syed Mukarram Ali, Chairman, Delta Medical College & Hospital, Dhaka.
Dr M R Khan, National Professor, Bangladesh
Professor K Siddique-e Rabbani, Professor & Chairperson, Dept of BMPT, Dhaka University and President, BMPA
Dr. Naheed Nabi, Secretary-II, Organising Committee
11:20 - 11:45: Refreshment (25 min)

19 February, 2015, Thursday
11:45 - 1:15: Scientific Session-II (90 mins)
Invited
IPM-2 Lutfun Nisa, Bangladesh Problems and Pitfalls in PET/CT imaging (30 mins)
Invited
ICN-2
Naila Zaman
Khan, Bangladesh Transfer of medical technology in resource poor situation (20 min)
RI-1 Meherun Nahar Mammographic Breast Glandularity in Bangladeshi Women: Data Derived from Generic Radiography
Invited
ICN-3
Khondokar
Mamun,
Bangladesh
Advancement of human machine interface for rehabilitation
engineering (30 min) RI-2 Nasreen Sultana
3D/4D Ultrasound for Evaluation of Normal and Abnormal
Fetal Anatomy in 2nd & 3rd Trimester Pregnancy : Experience of
Level III ultrasound
NM-1 Mohammad Anwar-Ul Azim
Development of PET Vesicular Acetylcholine Transporter
(VAChT) Neuroimaging probe for the diagnosis of Neurodegenerative
diseases Invited
ICN-4
Sania Ahsan,
Bangladesh
MRI use in early childhood and post operative evaluation in Moya Moya disease (20 min)
NM-2 M.M.M. Siraz
Assessment of Effective Dose to Occupational workers in
Nuclear Medicine Practices
NM-3 Lutfun Nisa Introducing Targeted Alpha Therapy in Bangladesh
Invited
ICN-5
Osman Gony,
Bangladesh
Neurofeedback Brain training technology: Hemoencephalography
(20 min ) NM-4 Md. Nahid Hossain
Motion Correction of SPECT by employing frame-to-frame correlation functions with Linogram and Sinogram projection
technique
1:15 – 2:30: Special Lunch
2:30 – 4:00: Scientific Session-III (90 mins)
Invited
IPM-3
Md Adnan Kiber,
Bangladesh
Review of Electrical Impedance Tomography: Advantages and
Pitfalls (30 min)
CN-9 Sania Ahsan Fetal MRI (20 min)
El-1 Ariful Islam Development of Algorithm of Simplified Sensitivity Matrix for Electrical Impedance Imaging
CN-10 Mostafa Mahbub Electrmyographic finding (EMG) in the children of Spinal muscular atrophy.
El-2 Sayed Parvez Ahmed
Focused Impedance Method for Measurement of the Volume of
an Object Embedded in a Volume Conductor
CN-11 Shipra Rani
Transfer of Technology: Experience in Providing a Short Course
Of Training and Doing EEG Recording in, Tanzania, Ghana and Cox‘s Bazar
El-3 Md. Shariful Islam
Optimum Electrode Configuration to Study the Human Kidneys
Using Electrical Impedance Techniques: a Simulation study
CN-12 Humaira Rafiqa
Title: Evaluation of the prolonged EEG and clinical correlation in
35 children.
El-4 Sumana Shahidunnahar Use of Focused Impedance Method (FIM) in the Detection
of Cervical Cancer
CN-13 Naheed Nabi
Role of EEG in children with non-seizure clinical problems: An
electro-clinical correlation
El-5 Abdullah Al Amin
Electrical Impedance Method for Breast Tumour
Characterisation
CN-14 Shanta Yesmin
Posterior slow waves on eye closure: are they precursors of
epileptiform discharges in certain cases?
El-6 A.R. Abir Development of simple Pigeon hole imaging modality for medical applications
CN-15 Abdus Salam Video-EEG data analysis and electro-clinical correlation.
El-7 Tasnim Zerin Simulation Study on Electrical Impedance Imaging of Different Sizes for Human Breast Screening for Cancer
CN-16 Mostafa Mahbub Neuroradiology : A mandatory subspeciality for clinicians.

19 February, 2015, Thursday
4:00- 5:00: Scientific Session-IV (60 mins)
Invited
IPM-4
John Damilakis, Greece
(IOMP)
IOMP perspective on education and training of Medical
Physicists (40 min)
Invited
ICN-6
Mr. Kazi Tanvir
Ahmmed,
Bangladesh
Learning Kit for children with special Needs: The RGACD
learning kit (20 min)
CN-17 Shayla Imam
Kanta
Can early detection of predictors of poor seizure outcomes
change the course of neurodevelopement ?
CN-18 Osman Gony
NeuroFeedback Brain Training (NFBT) Technology for
ADHD in Bangladesh: Single Case Study.
RDP-1 A. Begum Radiation Protection in Medical Practices in Bangladesh
CN-19 Eshtiak Ahmed
Identification of cognitive states based on Transcranial
Doppler Ultrasonography
RDP-2 A. Hoque
Effective Dose to Patient during Interventional Cardiac
Procedures
CN-20 Mehedi Masood
Fundamentals of PET-CT (Positron Emission
Tomography-Computed Tomography) and it’s application
in Oncology
5:00 - 5:15: Tea Break
5:15 - 6:20: Scientific Session-V (65 mins)
RDP-3 R.K. Khan Radiation dose of patient during CT scan
AIM-1 Mousumi Bala Study of the Broca Region of Brain to Analyze Autism
RDP-4 A. N. Monika Assessment of Radioactivity of Soil in Madaripur District of
Bangladesh AIM-2 Zubair Barkat
Need Assessment of Tele-Palpation
RDP-5 M.S. Rahman Assessment of Occupational Exposure in Interventional
Cardiology practices AIM-3 Rezwan Hussain
Findings from Two Urban Field Trials of the Dhaka University Solar Water Pasteurizer
RDP-6 Sariful
Study of Radioactivity Level in Soil, Sand and Sediment
Samples of Coastal Area in Cox‘s Bazar, Bangladesh and
Evaluation of Radiation Hazard
AIM-4 Ehsan A Chowdhury
A double blind trial to establish Distribution of F-Latency
(DFL) as an indicator of Cervical Radiculopathy or
Myelopathy
RDP-7 S. Yeasmin To Study the Natural and Artificial Radionuclides in Soil
Samples from Oil and Gas Field Area of Bangladesh AIM-5 Z B Mahbub
Distribution of F-Latency and MRI Study of the Brachial
Plexus
RDP-8 S. Yeasmin
Assessment of Natural Radioactivity Level in Different
Vegetable Samples of Brahmanbaria District in East-Central Bangladesh
AIM-6 Z B Mahbub Diffusion Features of the Brachial Plexus
RDP-9 S. Yeasmin
Assessment of Radionuclide Transfer from Soil to Vegetable in
Brahmanbaria District, (Bangladesh) using Gamma-Ray
Spectrometry System
AIM-7 Z B Mahbub Investigation of Different F-response Parameters at Different
Positions of the Head
Close of the day

20 February, 2015
8:30 - 10:15 am: Scientific Session - VI (105 mins)
TRACK-I (Main Hall) TRACK –II (Conference Room)
Paper ID Presenter Paper Title Paper ID Presenter Paper Title
Invited
IPM-5
A Sattar Mollah,
Bangladesh
Lessons Learned From Major Radiotherapy Accidents: International and Bangladesh Perspectives (25 min)
LCD-1 Shekh Md Mahmudul Islam
Android Apps Based Intelligent Telemedicine System for Bangladesh Perspective
LCD-2 Md. Kamrul Hussain Indigenous Development of Ultrasound Doppler Based
Fetal Heart Monitor
RT-4 Md. Shakilur Rahman Dosimetry and Quality Assurance (QA) of photon and electron
beam of medical linear accelerator at Oncology Centers in
Bangladesh
LCD-3 Zisun Ahmed Introduction to PC Based ECG Acquisition Technique without
Switched Resistor Network at Input
RT-5 M A Sabur Beam Data Acquisition of an Accelerator and Commissioning of CMS XiO 4.8 Treatment Planning System
LCD-4 Zubair Barkat Alternative Solution of Manual Glob Top for Low Resource Countries
RT-6 Muhammad Masud Rana Verification of a Computer Treatment Plan by Manual Methods LCD-5 S. Ahmmed Decoding Movements from Human Subthalamic Local
Field Potentials Based on Neural Synchronization
RT-7 A.S. Mollah Verification of TPS dose calculation by means of measurements with virtual solid water phantom and ion
chamber: Preliminary results
LCD-6 M Obaidur Rahman Efficacy Study of DFL using large Number of F-Latency Recordings
RT-8 M.N. Sharmin, Evaluation Of Radiation Doses At Organ At Risk Due To Tangential Breast Cancer Radiotherapy At Kyamch Cancer Center During 2012-13
LCD-7 M Obaidur Rahman Determination of Distribution of Conduction Velocity (DCV) from measured Distribution of F-latency (DFL)
RT-9 Hirak Kumar Dey Comparison of Dosimetric studies of 3 Dimensional conformal
radiotherapy and Intensity Modulated Radiotherapy of Brain
Tumours from CMS XIO TPS in KYAMCH
LCD-8 Ismat Ara Roksana Development of an Electronic Stethoscope with Optimized
Frequency Response for Different Body Sounds
RT-10 Motiur Rahman Planning and Delivery of 3D Conformal, Classic and fitting
PTV (C3DCRT and f3DCRT) vs. Intensity Modulated
Radiation Therapy (IMRT): A Dosimetric Evaluation and Comparison of Case Studies
LCD-9 Maruf Ahmad Implementations of a system of transferring electronic
stethoscope sound over mobile phone call for live auscultation
in Telemedicine.
RT-11 Md. Harun Or Roshid Calibration of 192Ir high dose rate brachytherapy source using
different calibration procedures
LCD-10 Susmita Afruz Investigation of X-ray Image Quality for Telemedicine
RT-12 Md. Jamal Uddin Treatment Outcome Of Radiation Alone Versus Concurrent Chemoradiation On Unresectable Non- Small Cell Lung
Cancer
LCD-11 Mohammad Abu Yousuf Talukder
Phaco-Emulsifcation Using Rotating Needles: A New Technique
RT-13 Kazi Manzur Kader Stereotactic Body Radiation Therapy (SBRT)- Advancement of
Radiation Oncology – a review
10:15 - 10:30 : Tea

20 February, 2015
10:30-12:30: Scientific Session-VII (120 mins)
Invited
IPM-6 Sadiq R Malik,
Bangladesh Radiotherapy Physics: Practical perspective (30 mins)
LCD-12 MO Rahman Low cost Dynamic Pedograph and customized shoe for diabetic
patients
LCD-13 K M A Hussain A Study of Nuclear Detector Materials Using Thermal Evaporation Method
LCD-14 A Al Amin A PC based Data Acquisition System for Bio-medical
Instrumentation
Invited
IPM-7
Salahuddin Ahmad,
USA
Treatment Plan Evaluation and Optimization Based on
Radiobiologic Parameters (30 mins)
LCD-15 Ahamad Imtiaz Khan Development of user friendly software in Bangla for a PC based
rural health monitor with option for telemedicine
LCD-16 M Abu Yousuf Solar Water Pasteurizer and Rain Water Collector for provision of
safe drinking water in urban slums and rural areas
LCD-17 Sharmin Zaman Low Cost Technology for Inactivation of Diarrhoeal Pathogens in Drinking Water Using Metals
Invited
IPM-8
S Akram Hussain,
Bangladesh Accidents and their prevention in Radiotherapy (20 mins)
LCD-18 EA Chowdhury A low cost mechanical prosthetic hand
LCD-19 Md. Nazimul Kadir A Low Cost Prosthetic Bionic Hand
Invited
IPM-9
Taposundar
Majumdar, INDIA End to End Solution - from Training, Education and Clinical Helpdesk to handle the cutting edge technology in modern cancer care (40 mins)
12:30 – 2:00 Lunch and Prayer break
2:00 – 4:00 : Plenary Session (120 mins)
Invited
IPM-10 K S Rabbani,
Bangladesh New methods in peripheral Nerve conduction measurement from Dhaka University (35 mins)
Invited
IPM-11
John Damilakis, Greece
(IOMP) Accreditation, certification and Recognition issues (45 mins)
Invited
IPM-12
Kamila Afroj Quadir
Bangladesh Education, Accreditation of Medical Physics & Biomedical Engineering in Bangladesh (20 mins)
Invited
IPM-13 M A Hai, Bangladesh
Clinical demand on Medical Physicists in Radiation Oncology (20 mins)
4:00-5:00 : Open Floor Discussion:
How to promote Physics in Medicine and Clinical Neuroelectrophysiology in Bangladesh? Compilation of Recommendations
Moderators: K Siddique-e Rabbani, Kamila Afroj Quadir, Naheed Nabi
5:00 – 5:10 : Certificate Distribution to Volunteers
5:10 -5:30 : Closing Tea
5:30 – 6:30 Annual General Meeting : BMPA (Main Hall), BCNEPS (Conference Room)
Close of the Conference

PHYSICS IN MEDICINE PAPERS

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
29
RT-1: Performance of the First ELEKTA Precise Linear Accelerator in
Bangladesh
M.N. Sharmin1, A.S. Mollah
2, Prof. M.A. Hai
1 and Dr. M.A. Bari
1
1KYAMCH Cancer Center, Enayetpur, Sirajgonj
2Khwaja Yunus Ali University, Enayetpur, Sirajgonj
Introduction: The first medical linear accelerator manufactured by Elekta Limited was installed in
the KYMCH Cancer Center, Enayetpur, Sirajgonj, and put into clinical operation in 2007. The aim of
this paper is to show the performance of the medical linear accelerator installed in the KYMCH
Cancer Center. This work describes the first Elekta Precise Treatment System installed in Bangladesh
as well as presents the results of some measurements. The main aim of this study was to show the
technical specifications of the accelerator and dosimetric performance of the LINAC by taking into
consideration of the stability of the performance for the last 8 years of clinical work. The results of
some acceptance tests and clinical performance checks are presented and discussed.
Materials and Methods: Measurements of percent depth doses and beam profiles were performed
using the PTW radiation field analyser (RFA). Beam quality parameters of photon and electron beams
were determined on the basis of the IAEA TRS 398 report. A Farmer type ionization chamber was
used with a PTW Unidose electrometer. The study presents the most important features of the system
as well as the results of dosimetric measurements for photon beams of nominal energies 6 and 15MV
and electron beams of energies 4, 6,8,10, 15 and 18 MeV.
Results and Discussion: Results gathered within a period of 6 years (2007-2013) have shown very
good stability of basic parameters of the machine. Most performance parameters were exceptionally
good having reproducibility of <0.1%, proportionality <0.5% with stability throughout the day for
photons (<0.2%) and electrons (<0.5%). Besides, angular dependence has been observed to vary a
maximum of 0.6% for photons and 0.8% for electrons with a very good uniformity of electron beams
(<105%).
Conclusions: Dosimetric measurements demonstrated the agreement of checked parameters with the
manufacturer‘s specification and IEC standards as well as national recommendations. Medical
accelerator Elekta Precise Treatment System demonstrated its full usefulness for clinical applications.
The machine parameters and functionality meet the requirements of the modern radiotherapy facility.
This machine is being used for treatment of cancer patient with negligible downtime at KYAMCH
Cancer Center since 2007.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
30
RT-2: Influence of Jaw tracking in Intensity Modulated and Volumetric
Modulated Arc Radiotherapy for Head and Neck Cancers – A Dosimetric
Study
Md Anisuzzman Bhuiyan1, Karthick Raj Mani
1, Sagar Upadhayay
2 and Kh Anamuel Haque
1
1Department of Radiation Oncology, United Hospital, Dhaka, Bangladesh
2 Gono Bishwabidyalay, Savar, Bangladesh
Introduction: To Study the dosimetric advantage of the Jaw tracking technique in Intensity
Modulated Radiotherapy (IMRT) and Volumetric Modulated Arc Therapy (VMAT) for Head and
Neck Cancers.
Materials & Methods: We retrospectively selected ten previously treated Head and Neck cancer
patients stage (T1/T2, N1, M0) in this study. All the patients were planned for IMRT and VMAT with
Simultaneous Integrated Boost (SIB) technique to deliver a differential dose per fraction to the high,
intermediate and low risk volume using a single plan. We intend to deliver 70Gy to the high risk
volume, 64Gy to the intermediate risk volume and 56Gy to the low risk volumes in 35 fractions. All
the critical structures were delineated which includes both parotids, spinal cord and both sub
mandibular glands. Eclipse treatment planning system, version 11.0 (Varian Medical Systems, Palo
Alto, CA), was used in this study. All the plans were planned with 6MV photons using Millennium
120 MLC. Both IMRT and VMAT plans were planned with and without jaw tracking by keeping the
same constraints and priorities for the target volumes and critical structures for a particular patient.
Plans were normalized at the target mean of the high risk volumes. All the plans were accepted with
the criteria of parotid glands mean dose <25Gy and spinal cord maximum point dose <45Gy without
compromising the target volumes. Target conformity, dose to the critical structures and low dose
volumes were recorded and analyzed for IMRT and VMAT plans with and without jaw tracking for
all the patients.
Results & Discussion: Jaw tracking resulted in decreased dose to critical structures in IMRT and
VMAT plans. But significant dose reductions were observed for critical structure in the IMRT
Technique with jaw tracking compared to IMRT Technique without jaw tracking. In VMAT with jaw
tracking technique the dose reduction to the critical structure were not significant compared to the
without jaw tracking technique due to relatively lesser monitor units. Gamma analysis showed greater
than 97% of pixels were passed within 3mm distance and 3% dose criteria for all the plans.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
31
RT-3: Low Cost Proton Therapy for the Cancer Patients
Mahmud Hassan
Dept of ECE, East West University, Aftabnagar, Dhaka, E-mail: [email protected]
Introduction: Although photon therapy saves lives of millions of cancer patient over the globe, the
quality of life of a patient may be compromised as the high energy photon beam (x-ray or gamma ray)
can damage adjacent tissues as it crosses the tumor. For particular types of cancer (eye, brain, liver,
lungs etc.) or for children or young adults photon therapy is not preferable. On the other hand proton
therapy can be a much better choice for these groups as protons slow down relatively fast when
entering biological tissues, and most of their energy is deposited, with little scatter, at the end of their
path in a peak called a Bragg peak (Fig. 1). Proton therapy is however very expensive and available in
only about 50 facilities around the world compared to several thousand photon therapy centres.
Fig. 1: Bragg peak for photon beam (pink line) and proton beam (red line). The blue line shows the
modified Bragg peak for proton beam of same energy. The modification is done to irradiate the
whole tumor and the thickness can be varied as per need.
Methods: Laser driven proton beams can reduce the cost of proton therapy by at least ten times in
future. When high intensity laser beam (I> 1019
W/cm2) is incident on a thin (few 10‘s of microns)
metal film, MeV proton beam comes out of the other side through a process known as TNSA.1We
used Halbach permanent quadruple magnets for focusing the proton beam. Initially GEANT4 and
Tosca Opera simulations were carried out to determine the positioning of the quadruple magnets. The
quadruple arrangements were used in the Forschungzentrum Rossendorf Tandem Accelerator in
Dresden, Germany and could successfully focus the beam.
Results: The quality of the beam was checked using the VULCAN petawatt laser beam in the
Rutherford Appleton Lab, Didcot, Oxfordshire, UK and we could produce up to 1011
protons per shot.
Although the proton beam was not mono-energetic, simulations show that at higher intensities, RPA
(radiation pressure acceleration) can produce quasi mono-energetic protons beams.2 With ELI
(extreme light infrastructure) to start in 2018, we expect to see GeV proton beam as a result of direct
acceleration from the intense (1022
W/cm2) laser beam.
Conclusion: Together with the Halbach quadruple magnet arrays we expect to see tabletop low cost
proton accelerators for proton therapy in not so distant future.
References: 1. S. C. Wilks et al., Physics of Plasmas, AIP, 2001, 8, 542-549
2. Keith Markey, CLF, STFC, STFC report (http://www.stfc.ac.uk/CLF/science/40078.aspx).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
32
Invited Talk
IPM-1: Radiation therapy: State of the art and the future
M. Saiful Huq, PhD, FAAPM, FInstP Professor and Director of Medical Physics
Department of Radiation Oncology
University of Pittsburgh Cancer Institute and UPMC CancerCenter
Pittsburgh, Pennsylvania, USA E-mail: [email protected]
During the last two decades there has been significant advances in technical innovations in radiation
therapy such as stereotactic radiosurgery (SRS), stereotactic body radiotherapy (SBRT), intensity
modulated radiotherapy (IMRT), and image guided brachytherapy (IGBT). Biologic information from
various physiologic imaging modalities are now routinely used to delineate target volumes accurately
and has become an integral part of the treatment design process. These advances have made it
possible to develop radiotherapy treatment plans based on 3D and 4D images that describe cancerous
targets and normal tissues and their movements. Linear accelerators are now integrated with
kilovoltage imaging devices to provide a means of seamless target identification and image guided
radiotherapy (IGRT), real time or near real time target monitoring, flattening-filter free beams and
volumetric modulated arc therapy. These technological innovations have enabled the delivery of
ideally distributed radiation dose to the target with great precision and accuracy while sparing the
adjacent organs at risk. The next generation linear accelerators will be integrated with MRI to provide
better contrast of various tissues in MRI for accurate targeting and normal tissue delineation and the
potential for real-time MRI-based tumor tracking and doing adaptive radiotherapy. In parallel
significant development is taking place in the world of nanotechnology, molecular imaging, genomic
analysis in the understanding of biology of cancer, targeted therapies, biologic therapies and systemic
therapies using novel chemotherapeutic agents. Trends in cancer therapy are moving from
population-based approaches to personalized approaches. It is likely that all these various modalities
will work together to provide evidence based highly personalized form of cancer medicine. This
presentation will provide an overview of these exciting advances in radiotherapy technology and
suggest how these innovations might work synergistically with advances in other field of oncology in
the years ahead of us.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
33
RI-1: Mammographic Breast Glandularity in Bangladeshi Women: Data
Derived from Generic Radiography
M. Nahar1, M. Sazzad
2, M.M.A. Zaman
2, A.S. Mollah
3
1Bangladesh Atomic Energy Regulatory Authority, Dhaka
2 Department of Physics, Jahangirnagar University
3Department of Medical Physics, Khwaja Yunus Ali University, Enayetpur, Sirajgonj.
Introduction: Breasts are made up of adipose, glandular and areolar tissues together with the
overlying skin. Of these, the glandular tissue is the most vulnerable and a common site for cancers. In
breast imaging with mammography, the percentage of glandular tissue is known as mammographic
breast glandularity. For calculation of the mean glandular radiation dose from a mammography
procedure, knowledge of the breast glandularity and compressed breast thickness for each breast is
required in order to choose mean glandular dose conversion factors. The amount of glandular tissue is
also linked to breast cancer risk. Thus, an objective quantitative analysis of glandular tissue can aid in
risk estimation.
The primary objective of this study was to determine the percentage of breast granularity of
Bangladeshi women which will affect mean glandular dose (MGD) during diagnostic mammography.
The secondary objective was to evaluate some of the factors affecting women‘s glandular tissue.
Materials and Method: Estimation of mammographic breast glandularity in Bangladeshi women
was done from generic radiographic data. A fitted equation was applied for 78 women who underwent
diagnostic mammography. A mammography X-ray unit was used to expose different thicknesses of
phantom material of varying glandular and adipose composition to develop this equation. Values of
compressed breast thickness (CBT), tube voltage kV, mAs and target/filter combination, were
collected for 78 women ranging in age from 16 to 70. The expected dependence of breast density on
age and CBT were analyzed.
Results: The average breast glandularity in women included in this study sample was 50.92% ±
17.45%. Breast glandularity was found to decrease with compressed breast thickness and age. A 15%
reduction of breast glandularity from 36 to 70 years was observed. Women above the age of 40 years
showed the greatest rate of change in glandularity. The average breast glandularity obtained in our
study was higher than that reported in studies from the United States, but comparable to values
reported for women in Australia, Germany and Malaysia. No significant variation of mean
glandularity has been found with Body Mass Index (BMI).
Conclusion: A method has been tested for estimation of mammographic breast glandularity in
Bangladeshi women from generic radiographic data. It provides a preliminary approach for
estimation of glandular tissue. This information will permit mean glandular dose calculations to be
extended from breasts of average composition (50% glandular and 50% adipose) to breasts of
individually determined composition. Image processing technique or quantitative interpretation of
fibro glandular and adipose tissue on mammogram remains to be developed in future studies.
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
34
RI-2: 3D/4D Ultrasound for Evaluation of Normal and Abnormal Fetal
Anatomy in 2nd
& 3rd
Trimester Pregnancy: Experience of Level III
ultrasound
N Sultana1, A Ihsan
2
1National Institute of Nuclear Medicine & Allied Sciences (NINMAS)
Bangladesh Atomic energy Commission 2Amimul Ihsan. IUT (Islamic university of technology)
E-mail: [email protected]
Introduction: Invent of 3D/4D ultrasound (US) has made a dramatic improvement in fetal imaging.
On 3D ultrasound, multiple 2D ultrasound sections are taken. Software like magic cut and
tomographic ultrasound imaging (TUI) helps to understand the anatomy better. Volume ultrasound is
an excellent tool for diagnosis of facial defects, spinal abnormalities and limb abnormalities etc. 4D
US shows fetal movements and expression that are basis for the neurodevelopment of the fetus. The
purpose of this study is to present the refined anatomical details obtained with 3D/ 4D ultrasound
over the classic 2D ultrasound in obstetrics and to emphasize the usefulness of this new technique
for the study of fetal anomaly.
Material & Method: Between May 2014 and October 2014 a total number of 350 fetuses were
evaluated by 2D & 3D/4D ultrasonography. Only consenting patients with singleton pregnancies
referred for anomaly scans were subjected to the 3D/4D imaging technique.
All examination was carried out as part of a detailed level III US procedure for fetal anomaly study.
The gestational age was between 18-30 weeks. We used a Voluson S6 advanced ultrasound machine
from GE with A RAB 4D abdominal probe (4-8MHz). Various viewing directions, rendering modes,
multiplanar modes and volume ultrasound modes were employed for visualization of fetal anatomy
and detection of malformations.
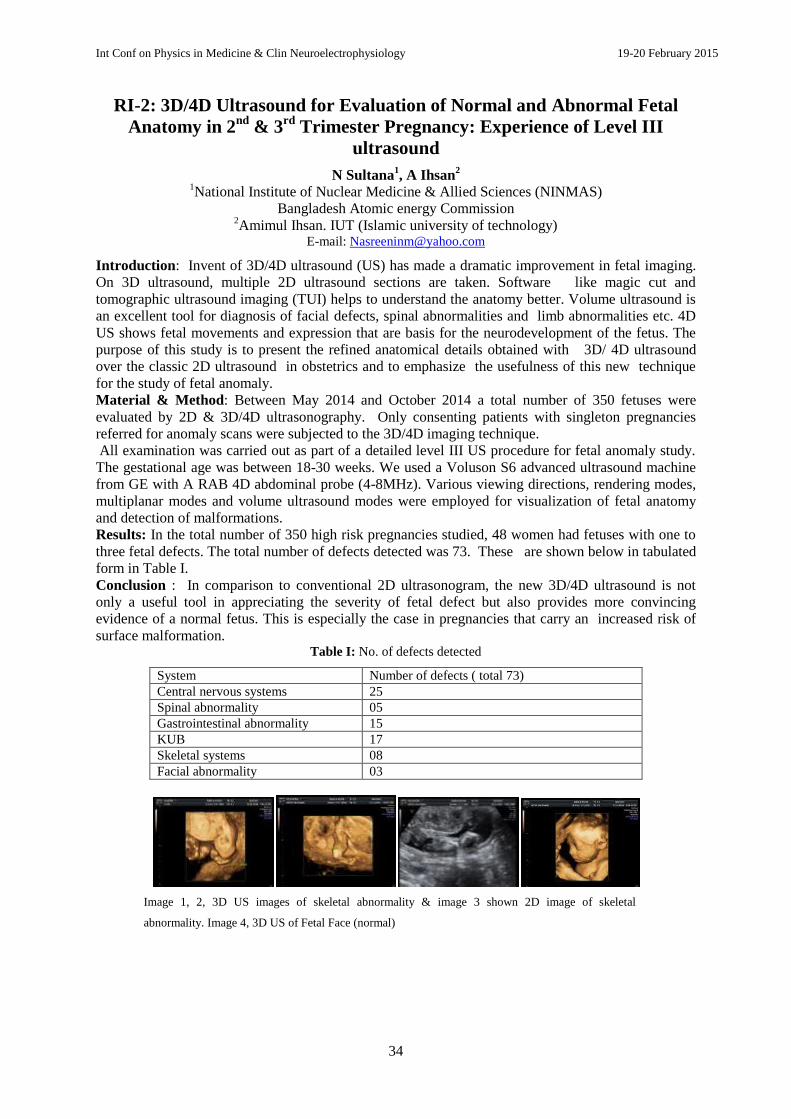
Results: In the total number of 350 high risk pregnancies studied, 48 women had fetuses with one to
three fetal defects. The total number of defects detected was 73. These are shown below in tabulated
form in Table I.
Conclusion : In comparison to conventional 2D ultrasonogram, the new 3D/4D ultrasound is not
only a useful tool in appreciating the severity of fetal defect but also provides more convincing
evidence of a normal fetus. This is especially the case in pregnancies that carry an increased risk of
surface malformation. Table I: No. of defects detected
System Number of defects ( total 73)
Central nervous systems 25
Spinal abnormality 05
Gastrointestinal abnormality 15
KUB 17
Skeletal systems 08
Facial abnormality 03
Image 1, 2, 3D US images of skeletal abnormality & image 3 shown 2D image of skeletal
abnormality. Image 4, 3D US of Fetal Face (normal)

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
35
NM-1: Development of PET Vesicular Acetylcholine Transporter (VAChT)
Neuroimaging probe for the diagnosis of Neurodegenerative diseases
Mohammad Anwar-Ul Azim1,2
, Takashi Kozaka2, Izumi Uno
2, Daisuke Miwa
2, Yoji Kitamura
2,
Kazuma Ogawa3, Yasushi Kiyono
4, Kahuhiro Shiba
2
1National Institute of Nuclear Medicine and Allied Sciences, BAEC, BSMMU, Shahbagh, Dhaka. 2Division of Tracer Kinetics, Advanced Science Research Center, Kanazawa University, Japan.
3Institute of Medical, Pharmaceutical and Health Sciences, Kanazawa University, Japan.
4Biomedical Imaging Research Center, University of Fukui, Fukui, Japan.
Introduction: Neurodegenerative diseases are generally characterized by progressive diminution in
cognitive function. The decreased cognitive function and level of dementia are associated with the
loss of cholinergic neurons and synapses accompanied by deficiencies in cholinergic
neurotransmission. In cholinergic neurotransmission, a marked diminution of VAChT is sufficient to
interfere with the release of Acetylcholine (Ach) in the brain and affects cognitive behavior. Hence,
positron labeled VAChT imaging probe might be a tool for the diagnosis of neurodegenerative
diseases using Positron Emission Tomography (PET).
The outcome of PET neuroimaging depends on: the number of receptors available for binding with
the PET radioligand; the affinity of available receptors toward the PET radioligand and the
concentration of molecules other than the PET radioligand that bind to those receptors. Challenges
involved in the development of VAChT PET neuroimaging probe includes short half-life of
conventional positron emitters; synthesis of highly purified radioligands of high specific activity;
reasonable lipophilicity of the radioligand to access blood brain barrier (BBB) and high specific
regional accumulation in VAChT rich regions in the brain.
Objectives: The objective of the present study is to report the prospect of a newly synthesized
decalinvesamicol (DV) analogue radiolabeled with the unconventional long-lived positron emitter
(77
Br) as a potential VAChT PET imaging probe.
Method: [77
Br]OBDV was synthesized by a standard halogenation reaction from o-trimethylstannyl-
trans-decalinvesamicol (OTDV) and this [77
Br]OBDV was injected intravenously into 12 rats. These
rats were sacrificed in groups of four at intervals of 2 min, 30 min and at 60 min post-injection. The
blood, brain regions, and the organs of interest were harvested, weighed and radioactivity was counted
to investigate the in vivo biodistribution. In vivo blocking study was performed to check the binding
selectivity of [77
Br]OBDV for VAChT. Ex-vivo autoradiography was performed to reveal the regional
brain distribution of [77
Br]OBDV at 30 min post-injection.
Results: In- vivo biodistribution study showed rapid penetration of [77
Br]OBDV through the blood-
brain barrier. At 2 min and 60 min post- injection the accumulation of radioactivity in the brain was
found to be > 0.6 % ID/g and 0.45 ~ 0.53 % ID/g respectively. The uptake of [77
Br]OBDV in brain
was blocked by about 41% after co-administration of 0.250 μmol vesamicol (VAChT ligand) in the
in- vivo blocking study. In ex-vivo autoradiography, accumulation of [77
Br]OBDV in striatum and
cortex was observed visually.
Conclusion: Selective binding and high affinity of [77
Br]OBDV to VAChT in rat brain in- vivo
suggests that OBDV radiolabeled with 77
Br can be a potent VAChT imaging probe for PET.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
36
NM-2: Assessment of Effective Dose to Occupational workers in Nuclear
Medicine Practices
M.M.M. Siraz, R.K. Khan, A. Hoque and A. Begum
Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh E-mail: [email protected]
Introduction: Nuclear medicine is a medical specialty involving application of radioactive substances
in diagnosis and treatment of disease. The most commonly used radioisotopes in nuclear medicine
facilities in Bangladesh are Tc-99m and I-131. The medical use of ionizing radiation, while offering
great benefits to patients also contributes significantly to radiation exposure to individuals and
populations. This report describes occupational radiation doses of nuclear medicine personnel in 17
nuclear medicine facilities in Bangladesh.
Materials and Methods: Calibrated thermoluminescent dosimeters (TLD-100, LiF: Mg,Ti) were
used to determine radiation dose and were worn by nuclear medicine personnel on their torso for 3
months. Harshaw TLD reader (Model 4500) had been used for reading out the TLD cards.
Result and Discussion: In this study it was observed that the dose received by all the occupational
workers was within the occupational dose limit of 20 mSv per year. Average dose received by the
occupational workers is shown in Figure-1 and their dose range distribution is tabulated in Table-1.
Figure-1. Average dose received by Nuclear Medicine personnel from 2010 to 2013
Table-1. Distribution of workers on different dose range (mSv) from 2010 to 2013
Year Total
Worker
<MDL MDL-
0.99
1-
2.99
3-
4.99
5-
9.99
10-
14.99
2010 264 132 121 9 2
2011 304 162 125 14 2 1
2012 320 168 130 20 2
2013 294 202 75 12 3 2
Conclusion: The dose received was within the maximum annual dose limit for occupational workers.
Nevertheless, for continued radiation protection, the occupational workers must remain vigilant about
procedures and practices to keep radiation exposure dose as low as possible.
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Avera
ge D
ose (
mS
v)
2010 2011 2012 2013
Physician
Scientist
Staff

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
37
NM-3: Introducing Targeted Alpha Therapy in Bangladesh
Lutfun Nisa1, Kamila Afroj Quadir
1 and K Siddique-e Rabbani
2
1National Institute of Nuclear Medicine & Allied Science, BAEC
BSM Medical University, Dhaka, Bangladesh. 2Department of Biomedical Physics & Technology, University of Dhaka, Bangladesh
E-mail: [email protected]
Introduction/Background: Targeted alpha therapy (TAT) is a new experimental, systemic therapy
that targets cancer cells and tumor capillary endothelial cells by intravenous injection of an alpha
immunoconjugate (AIC). The AIC is formed by labeling the cancer targeting monoclonal antibody
with the alpha emitting radioisotope Bi-213 using a bifunctional chelator. The monoclonal antibody is
raised against antigens that are over expressed by cancer cells. There are several centers for TAT,
notably in Europe, the US and Australia. Bangladesh recently obtained ethical clearance for a Clinical
Phase 1 trial of TAT in patients with MUC1 antigen positive cancers. The TAT technique will be
discussed and highlighted in this presentation.
Objective: The aim of the study is to introduce and establish TAT technology in Bangladesh as a safe
therapeutic option for management of patients with advanced MUC1 positive cancers.
Method: The study will be done in collaboration with Australia. The monoclonal antibody C595
against MUC1 and the Actinium:Bismuth generator required for the study will be obtained through
the collaborating partner. Patients with stage four MUC1 positive cancers having progressive disease
and those who have either completed or have declined other systemic therapies will be included in the
trial. Cohorts of 3 subjects with end-stage cancer will be treated with escalating doses of 5 mCi, then
10, 15, 20, 25, 30 mCi every 2 months. If adverse events are seen in one patient then the maximum
tolerance dose will be the preceding dose. Patients will be followed up for 12 months with emphasis
on the detection of delayed radiation nephrosis.
Result: The proposed study will bring together the highly selective features of a unique targeting
system with the high cytotoxicity of alpha particles for treatment of mucin (MUCI) expressing tumors
of the breast, ovary, pancreas and prostate. It will optimize the key parameters of targeted alpha
therapy, ie stability and specific activity of the alpha – conjugate and maximum tolerance dose that
may lead to a much higher rate of tumor control.
Conclusion: Currently there is no systemic treatment that can inhibit the progression of cancer that
leads invariably to the death of the patient. If successful, TAT would be indicated for durable
therapeutic responses in stage four cancer patients.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
38
NM-4: Motion Correction of SPECT by employing frame-to-frame
correlation functions with Linogram and Sinogram projection technique
Md. Nahid Hossain1, Kamila Afroj Quadir
1, Ferdoushi Begum
1, Tanvir Ahmed Biman
1,
Md. Nurul Islam1 and Adnan Kiber
2
1National Institute of Nuclear Medicine & Allied Sciences, BAEC. BSM Medical University campus.
Shahbagh, Dhaka, Bangladesh 2Department of Electrical and Electronic Engineering, University of Dhaka, Bangladesh.
E-mail: [email protected]
Introduction: Single Photon Emission Computed Tomography (SPECT) study involves data
acquisition over a relatively long time, typically in the range of 5-30 minutes. For good image
quality, the patient must ideally lie still during this period but quite frequently patient movement
occurs during aclinical procedure. This movement causes misalignment of the projection frames,
which degrades the image quality and may introduce artifacts in reconstructed images. The ability to
detect and correct for the motion using a computational method is valuable for quality assurance of
SPECT imaging. In this work, a frame-to-frame correlation function based on linogram and sinogram
of the projection technique was evaluated to estimate the occurrence of motion and to make correction
for best alignment.
Methods: A Technetium-99m point source was placed at 15cm radius of rotation and images were
obtained with a rotating dual head gamma camera. Data was acquired with 32 views over 360 into a
128 x 128 acquisition matrix. To evaluate the process, some axial displacements and frame-to-frame
correlation functions were applied on several frames of the point source object.
Results: Misalignment of the source was detected in 16 frames in projection data. The results showed
that misalignment due to motion between the projections can be corrected with the application of
frame-to-frame correlation method. The linogram and sinogram were used to show better alignment.
The motion artifacts of images were reduced considerably after motion correction.
Conclusion: The frame-to-frame correlation technique represents a sensitive method for the
correction of patient motion during a tomographic scan. Patient motion as small as 1 pixel could
easily be distinguished by this method and thus, the motion artifacts of images were reduced
significantly which eventual improvement of the image quality.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
39
EI-1: Development of Algorithm of Simplified Sensitivity Matrix for
Electrical Impedance Imaging
Ariful Islam, Sabbir Akhanda & Dr. Md. Adnan Kiber
Dept of Electrical and Electronic Engineering, University of Dhaka, Dhaka, Bangladesh E-mail: [email protected], [email protected], [email protected]
Introduction: Electrical impedance tomography (EIT) is a kind of medical imaging technique in
which conductivity distribution within the object is estimated from the boundary voltage and current
measurements. Electrodes are placed on the surface of the body and by applying low currents
resultant voltages are calculated from these surface electrodes. We can only measure boundary
voltages in real life. Many developed algorithms are very complex and failed to real life data. We
offered a very simple and innovative way to calculate the discretized sensitivity matrix to estimate the
conductivity distribution.
Methods: The boundary voltage (V) data and the conductivity (C) distribution are related by the
equation V=SC, where S is the sensitivity matrix of the considered section. For simplicity, we have
assumed a square section and placed one electrode at each corner of the section (Figure 1). We also
have assumed that the conductivity distribution is equal to 1 S\m. So we can write V=S. Here V is a
vector (size 16×1) and S is a matrix (size 16×16). To find the elements of the matrix at first we drive
two successive electrodes and consider middle point as the output point of any two successive
electrodes. The voltage induced at this point is equal to the total contribution of each small square
voltage and the value will depend on the relative distances between the squares and the middle point.
For infinite medium it will change inversely according to
, where r and d are the corresponding
distances from driving and receiving point to the center of each small square. These distance values
are the coefficients of the sensitivity matrix. Firstly we have calculated the distance values according
to the analytical formula
then modified it by
since our considered medium is finite. We
have formed the sensitivity matrix by the distance values as its coefficients. Then we have multiplied
the sensitivity matrix with unity conductivity to measure the analytical voltage and compared with the
voltage data simulated by COMSOL Multiphysics 4.3 to compute the percentage of error (Figure 2).
Figure 1: Considered section. Figure 2: Data comparison. Figure 3: Error estimation.
Results and Observations: It is found that the voltage data obtained by simulation from COMSOL
and voltage data (analytical) calculated from our sensitivity matrix results an error, =6.59% .The
analytical formula is based on infinite medium. However medium considered here is finite. So we
argued that the distance function
should be changed by
. We have changed the parameter
from m=1.8 to m=2.7 and calculated respectively. Minimum error occurs when m=2.2 which is
equal to =.762% (Figure- 3).
Conclusion: So our suggested model of developing the simplified sensitivity matrix from V=SC by
assuming uniform conductivity can be considered to be a good estimation of the true theoretical
sensitivity matrix.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
40
EI-2: Focused Impedance Method for Measurement of the Volume of an
Object Embedded in a Volume Conductor: Finite Element Simulation
Sayed Parvez Ahmed1, 2
, M Abdul Kadir1, Golam Dastegir Al Quaderi
3, Rubina Rahman
2 and K
Siddique-e Rabbani1
1Department of Biomedical Physics & Technology, University of Dhaka, Dhaka-1000, Bangladesh
2Department of Physics, Jahangirnagar University, Savar, Dhaka, Bangladesh
3Department of Physics, University of Dhaka, Dhaka-1000, Bangladesh
E-mail: [email protected], [email protected]
Introduction: In many applications the volume of a target organ inside the body needs to be
measured from outside non-invasively. The present work aims at developing such a method using a
localized impedance measuring technique called the Focused Impedance Method (FIM) which was
innovated by the Biomedical Physics group of the University of Dhaka.
Methods: The present method is based on the 4-electrode FIM version where the electrodes are
placed at the corners of a square region. In this method multiple concentric FIM electrode sets having
different separations are placed centrally over the region with the target object underneath. Using
Finite Element simulation using a software package named
Comsol Multiphysics (version 4.3) FIM values were obtained
with and without objects of different conductivity, size and depth
embedded in a volume of uniform and known conductivity and
the change in impedance were obtained. Simulations indicated
that these impedance-change decreased with electrode separation
almost linearly up to a certain value. The top figure shows such
changes for object conductivities less and more than the
background conductivity, and for varying object diameters (d),
using spherical objects. The slopes in the early part of this figure
were then plotted with 1/d which appears to be a straight line as
the lower figure shows. From this finding an equation was
developed as:
|
|
where K and C are constants which
depend on the conductivity and permittivity of the object and the
volume conductor under investigation, dimension of the volume
conductor and the electrodes used and the electrode separations
chosen.
Results: Using the above method simulation and
phantom experiments were carried out respectively. In
the first case the obtained volume was compared with
the modeled object volume while in the latter the
obtained volume was compared with the actual object
used in a phantom of uniform conductivity. The two
tables give the values obtained (top: simulation, bottom:
actual phantom experiment).
Discussion: It may be seen that the error values are very
small. Of course, this method needs a knowledge of the
conductivities and permittivities of the object and the
background, which may be obtained using other means.
The present work gives a method which may be useful
not only in medical field but also in other areas like
geology, oceanography, etc.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
Electrode separation
Ch
ang
e in
Fo
cuse
d i
mp
Inverse of depth
Slo
pe
val
ue
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
41
EI-3: Optimum Electrode Configuration to Study the Human Kidneys
Using Electrical Impedance Techniques: a Simulation study
Md. Shariful Islam, M Abdul Kadir and K Siddique-e Rabbani Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh
E-mail: [email protected], [email protected]
Introduction: There is a growing interest on non-invasive examination of living tissue using
electrical impedance techniques. Impedance measurements using skin surface electrode can sense the
change in transfer impedance of an organ within the body. Electrical impedance properties of human
kidney may give useful information about its functionality. The present work was taken up to find an
optimum electrode configuration to study electrical properties of human kidneys using electrical
impedance techniques.
Methods: A Finite Element simulation software package (COMSOL Multiphysics) was used for all
the simulated measurements in the present work. A cylindrical (diameter: 28cm, height: 30cm)
thorax-abdomen model with a uniform background conductivity (equal to that of typical values for
muscles) was assumed with the kidney (assumed rectangular, of size 11cm x 6cm x 3 cm) having a
different conductivity and placed at a depth of 5cm from the surface. Total impedance of this thorax-
abdomen model with and without a kidney were measured using conventional Tetrapolar Impedance
Method (TPIM) and three versions of Focused Impedance Method (FIM with 8, 6 and 4 electrode
versions)> These FIM techniques were conceived and developed by the Biomedical Physics group of
the University of Dhaka. For the desired measurements in the simulation, electrodes were placed on
the body surface at various positions to determine the contribution of the kidney. To obtain the
optimum electrode configuration, the measurements were simulated with different electrode positions
for all the measurement techniques.
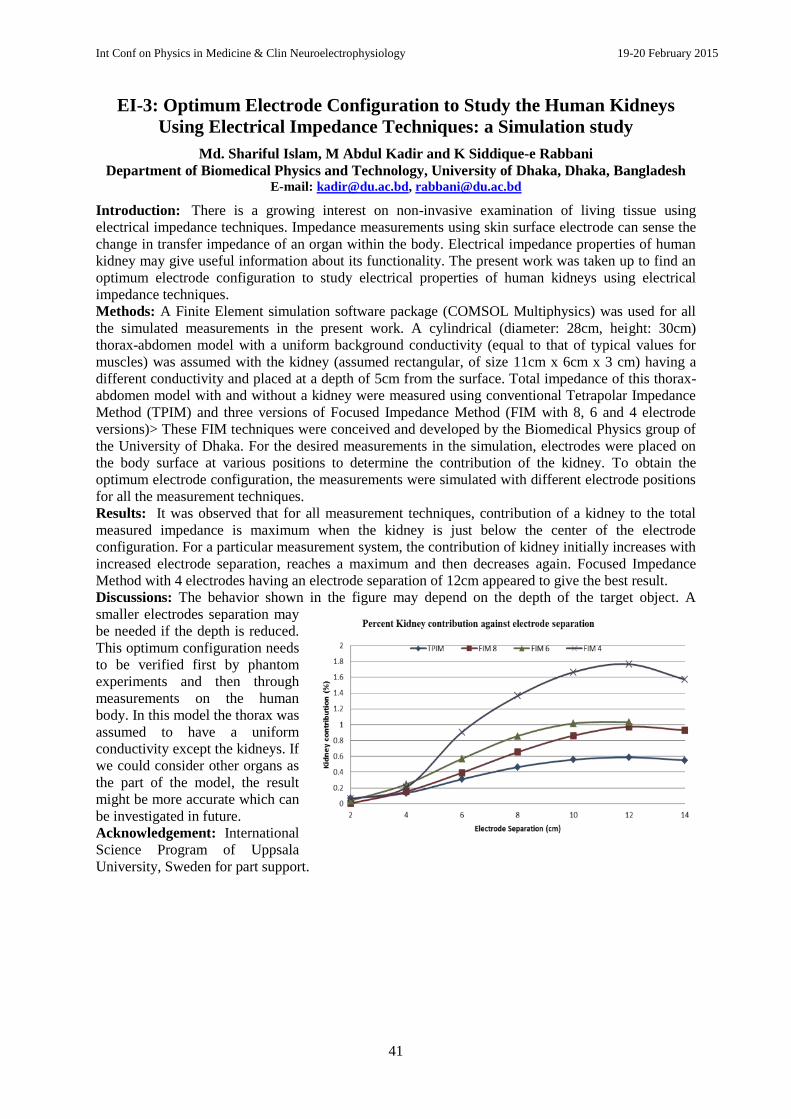
Results: It was observed that for all measurement techniques, contribution of a kidney to the total
measured impedance is maximum when the kidney is just below the center of the electrode
configuration. For a particular measurement system, the contribution of kidney initially increases with
increased electrode separation, reaches a maximum and then decreases again. Focused Impedance
Method with 4 electrodes having an electrode separation of 12cm appeared to give the best result.
Discussions: The behavior shown in the figure may depend on the depth of the target object. A
smaller electrodes separation may
be needed if the depth is reduced.
This optimum configuration needs
to be verified first by phantom
experiments and then through
measurements on the human
body. In this model the thorax was
assumed to have a uniform
conductivity except the kidneys. If
we could consider other organs as
the part of the model, the result
might be more accurate which can
be investigated in future.
Acknowledgement: International
Science Program of Uppsala
University, Sweden for part support.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
42
EI-4: Use of Focused Impedance Method (FIM) in the Detection of Cervical
Cancer
Sumana Shahidunnahar, M A Kadir, Shahnaj Parvin and K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka 1000,
Bangladesh E-mail: [email protected], [email protected]
Introduction: In Bangladesh approximately 200,000 new female cancer cases are added each year in
which the prevalence of cervical cancer (21.5%) comes only second to that of breast cancer (25.6%).
In cancer changes occur at cellular level as shown in Fig.1 for which the electrical impedance at
different frequencies differ significantly from that of the healthy cells.
Methods: The thickness of epithelium layer of cervix is about 0.5 mm which
is affected by cancer. Based on the above information a group in Sheffield,
UK developed a pencil like impedance probe with four tiny gold electrodes
placed at the corners of a square region with 2mm sides. They showed that
the peak sensitivity of such a probe is at one third the electrode separation,
which guided the choice of the electrode geometry. Using multi-frequency
Tetra Polar Impedance Measurement (TPIM) this group succeeded in
detecting cervical cancer at early stage, known as CIN-1, as shown in fig.2.
Results: The present work was taken up in laboratory of Department of
Biomedical Physics & Technology, University of Dhaka, to apply Focused
Impedance Method (FIM), a recent innovation of our extended group, in the detection of Cervical
Cancer. The geometrical sensitivity distribution of FIM is more localised than that of TPIM, and this
localisation may bring advantages to this technique. Besides, to make the measurement simpler the
measurement would be made at only two frequencies, one around 5kHz and the other around 500kHz.
A pencil impedance probe similar to that of the Sheffield group but with 1.5mm sides has been made.
Discussions: Since the current density may be high with small electrodes, an FIM instrument is being
developed with small currents, of the order of 10µA. Measurements will be made first on phantoms
and other biological samples before applying on human subjects. If successful, this work may produce
a cost effective device for use in the Third World.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
Normal CIN 1 CIN 3 InvasiveCIN 2
Fig.1: Normal cervix and a
cervix with an early form of
cancer (cervical dysplasia)
Fig.2: Cellular structure of cervical epithelial cells for normal, cancerous, and
intermediate stages (surface at the top).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
43
EI-5: Electrical Impedance Method for Breast Tumour Characterisation
Abdullah Al-Amin1, Shahnaj Parvin
1, M A Kadir
1, Tasmia Tahmid
2, S Kaisar Alam
3,
K Siddique-e Rabbani1
1Department of Biomedical Physics & Technology, University of Dhaka, Dhaka 1000,
Bangladesh. 2Tasmia Tahmid Breast Care, Dhaka.
3Center for Computational Biomedicine Imaging and Modeling
(CBIM), Rutgers University, Piscataway, NJ 08854, USA
E-mail: [email protected], [email protected]
Introduction: Cell morphology and blood flow are significantly different in malignant and benign
conditions in breast tumours contributing to significant differences in electrical impedance at a
particular frequency of measurement, as well as in the frequency spectrum of impedance. The aim of
the present work was to explore the feasibility of using Focused Impedance Method (FIM), a
localized measurement technique conceived and developed by the Biomedical Physics group of the
University of Dhaka, to characterize a breast tumour non-invasively, i.e., to determine whether a
tumour is malignant or benign. The only existing alternative is needle or core biopsy, which are not
hazard free; in a few percent of cases where the tumour is cancerous, tissue adhering to the tip of the
needle sometimes introduces cancer at the upper layers
Methods: A 4-electrode probe as shown in the figure (left)
with an adjacent electrode separation of 5cm was used to
obtain transfer impedance values using the traditional
Tetrapolar Impedance Method (TPIM) in both horizontal
and vertical directions. These were combined to get FIM
values too. Measurements were carried out at two
frequencies, 5kHz and 200kHz, keeping the tumour at the
centre of the electrode geometry as far as possible. Data
were obtained from 23 consenting subjects in the age range 17 - 55 years who had palpated lumps.
Location and size of the tumours were determined earlier through ultrasound scan and some patients
had core biopsy afterwards. The data were analysed using statistical and Feature classification
methods, which used 12 features in this case. Classification using K-Nearest Neighbour (K-NN)
method was performed.
Results and observations: 4 patients out of the
23 had malignancy, based on core biopsy
results. The statistical analysis showed
significant variation between the affected and
unaffected sides of a particular patient but there
was a large person to person variation. The plot
obtained with the Feature classification method,
as shown in the bottom figure, provided a
reasonable distinction between benign (dotted
lines) and malignant cases (solid lines) when
the impedance data were divided by the age of
the patients. A positive predictive value of 60%
and a negative predictive value of 93% was
obtained in this preliminary study.
Conclusion: This method has scope to improve and may provide a new technique for non-invasive
biopsy of breast tumours.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
H
Vt

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
44
EI-6: Development of simple Pigeon hole imaging modality for medical
applications
A.R. Abir, K.S. Rabbani, A.I. Khan, K. Hossain
Department of Biomedical Physics and Technology, University of Dhaka, Bangladesh. E-mail: [email protected]
Introduction: Pigeon Hole Imaging (PHI) is a new and simple imaging modality to give a low
resolution electrical impedance image conceived and developed in our laboratory earlier. This may be
used to perform measurements on large organs inside the body whose positions are not accurately
known, or which moves during measurement. This earlier version of PHI was conceived as an
extension of the 6-electrode Focused Impedance Method (6-FIM). Two pairs of orthogonal current
electrodes, and a number of diagonal electrodes at the central zone were required for the PHI.
However, the images away from the diagonal had to be corrected based on several empirical rules. A
newer version of PHI has recently been conceived based on 4 electrode Focused Impedance Method
(4-FIM). Both 6-FIM and 4-FIM were developed by extended groups of our department earlier.
Methods: In the current version of the PHI, many electrodes are arranged in a square matrix as shown
in figure 1 (dots represent electrodes). Using the 4 electrodes at the corners of each square matrix
element, a 4-FIM measurement is made which gives the respective impedance within the individual
matrix position with negligible contribution from the neighboring zones. Thus all the results
combined, arranged and assigned to respective matrix positions, gives the desired PHI image directly.
Because of the inherent 3D sensitivity, large internal body organs may be imaged by placing the
electrodes on the chest or on the back of a human thorax.
Results and Discussion: For PHI, when objects are far apart, the straightforward image is reasonably
good. However, when a single object extends beyond a single pixel, or when several objects lie in
close proximity, some uncertainties occur in the image generation. Some rules have been developed to
generate images in such cases to include these effects and necessary software has been developed.
Figure 2 shows such an image with four simulated objects in different positions in a 5x5 matrix. PHI
is suited to surface electrodes looking at organs within certain depths. It should be useful in locating a
reasonable large organ inside the body, and for following it if it changes positions or size with time.
This may have use in the application of electrical impedance for diagnosis or for applying precise
radiotherapy dose to a particular organ that is moving with breathing. It is conceptually simple, and
the instrumentation necessary is simple too. Therefore, the instrumentation can be developed and
made in a low resource country, at a considerably low cost.
Z11
Z12
Z13
Z21
Z22
Z23
Z31
Z32
Z33
Z14
Z24
Z34
Z41
Z42
Z43
Z44
Figure 2: PHI for four objects
positioned at different places in a
5x5 matrix.
Figure 1: Concept of PHI based on
4 electrode FIM. This shows a 4x4
imaging method.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
45
El-7: Simulation Study on Electrical Impedance Imaging of Different Sizes
for Human Breast Screening for Cancer
Tasnim Zerin, Selina Akter and Md. Adnan Kiber Department of Electrical & Electronic Engineering, University of Dhaka.
Email: [email protected], [email protected], [email protected]
Introduction: Breast cancer is the most common invasive cancer in females worldwide. However,
early diagnosis and detection by screening method can save life.
Methods: At present, commonly mammography is used as screening method for detecting breast
tumor which uses low-energy X-ray radiation. Although the radiation exposure is low, the repeated x-
rays have the potential to cause cancer along with the high probability of false diagnosis.Ideally, a
non-invasive, no health hazard, simple and inexpensive method for breast cancer screening is needed
and Electrical Impedance Tomography (EIT) meets these requirements, however its resolution is low.
Most image reconstruction method in EIT uses sensitivity matrix and this matrix has a dependency on
size and shape of the object. It is known from the works of other researchers that size of breast do
vary from one woman to other woman. Here, we used ‗Comsol multiphysics‘, a simulation software
to observe the corresponding voltage distribution EIT data by varying the size of the object in both 2D
& 3D. The half-sphere shaped object model rather than cylindrical shaped object is used, which
mimics closely the shape of the human breast.
Results and Observations: In this work, 16 equidistant electrodes have been placed at the mid-level
on the surface of the objects having radius of 5cm , 6cm, 7cm, 8cm, 9cm and 10cm for 2D circular
object and 3D half-sphere models. For every object for 16 electrodes, there is a corresponding 13 EIT
voltage data. For uniform conductivity, we summed all the 13 EIT data and got Vtot for each size
object for both 2D and 3D object. Then we have introduced a small object having volume 26 cm^3 for
all cases at the center having conductivity 100 times of uniform conductivity. After that we have used
equation
∑
) ) , where Vc and Vu implies 13 EIT data for non-uniform and
uniform conductivity. For uniform conductivity, it is seen from the graph in fig-1 & fig-2, Vtot is
practically constant for 2D object and fall almost linearly as the size increases in case of 3D. While
for non-uniform conductivity, Vd changes in 3D shown in fig-3 and the rate of decrease is faster.
Fig-1: Vtot for different sizes of object for Fig-2 : Vtot for different sizes of object for Fig-3 : Vd for different sizes of object for
2D uniform conductivity. 3D uniform conductivity. 3D uniform & non-uniform
conductivity
Discussions: From this work, it is clear that for 3D object (breast), size information need to be
incorporated in calculating sensitivity matrix to get a better EIT image.
References: 1. http://www.cancer.gov/cancertopics/factsheet/detection/mammograms
2. http://www.mobecomm.com/docs/pubs/A_3D_electrical_impedance_tomography-(EIT)-
system_for_breast_cancer_detection.pdf)

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
46
Invited Talk
IPM-4: IOMP perspective on education and training of Medical Physicists
John Damilakis
Professor of Medical Physics
Faculty of Medicine, University of Crete, Greece E-mail: [email protected]
Abstract: The International Organization for Medical Physics (IOMP) has recently published policy
statements on the principal functions and responsibilities of medical physicists (1) and on basic
requirements for education and training of Medical Physicists (2). IOMP states that ‗Medical
physicists (MPs) working as health professionals shall demonstrate competency in their discipline by
obtaining the appropriate educational qualification and clinical competency training in one or more
sub-fields of medical physics. Basic knowledge of the other sub-fields is also required. MPs
practicing in hospitals/clinical environments shall also participate in a continual professional
development program. Recommendations on the minimum levels of education and professional
training for MPs are given in the following sections‘ (2). In another paragraph of the same policy
statement, IOMP states that ‗Educational qualification could be accomplished in two phases. The first
phase of the education program is completion of a bachelor‘s degree in physics or an equivalent
degree in a relevant physical or engineering science subject. The second phase of the program is
completion of a postgraduate program2 at a master‘s degree level in medical physics or an equivalent
degree in an appropriate physical science subject‘.
The European Federation of Organizations for Medical Physics (EFOMP) has published policy
statement no. 12 on ‗The present status of Medical Physics education and training in Europe. New
perspectives and EFOMP recommendations‘ (3). Moreover, the International Atomic Energy Agency
(IAEA) has published a document entitled ‗Roles and Responsibilities and education and Training
Requirements for Clinically Qualified Medical Physicists‘ (4).
Large variations in the education and professional development of Medical Physicists exist in Europe.
In 2010, the European Commission (EC) launched a 2-year project on the Medical Physics Expert
(MPE) to provide for improved implementation of the Medical Exposures Directive (MED)
provisions related to the MPE and to facilitate the harmonization of the MPE among the member
states aiming at their cross-border mobility. The MPE project has distinguished between 3 levels of
medical physics education and training:
(1) the level of the graduate with a Master‘s degree in Medical Physics or equivalent,
(2) the Medical Physicist level in one specialty area of medical physics after having followed two
years of training in the particular specialty of medical physics,
(3) the MPE level in a given specialty after two additional years of advanced training and practice.
Eutempe RX is a new EC project launched on August 2013. The aim of EUTEMPE is to provide the
best possible training opportunities to European Medical Physics professionals to become MPEs
working in Diagnostic and Interventional Radiology.
References 1. IOMP Policy Statement No.1. The medical physicist: roles and responsibilities.
http://www.iomp.org/?q=node/5.
2. IOMP Policy Statement No.2. Basic requirements for Education and Training of Medical Physicists.
http://www.iomp.org/?q=node/5.
3. EFOMP Policy statement No 12. The present status of Medical Physics education and training in
Europe. New perspectives and EFOMP recommendations‘. www.efomp.org.
4. Roles and responsibilities and education and training requirements for clinically qualified
medical physicists. IAEA Human Health Series, No. 25

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
47
RDP-1: Radiation Protection in Medical Practices in Bangladesh
A. Begum, M.S. Rahman, A. Hoque, J. Ferdous and R.K. Khan
Health Physics Division, Atomic Energy Centre, GPO Box 164, Shahbag, Dhaka-1000. E-mail: [email protected]
Introduction: Ionizing radiations have many beneficial applications in medicine but undue usage of it
may cause adverse health effect. Radioactive sources and radiation generating equipments are being
widely used in different medical practices such as radiology, interventional cardiology, nuclear
medicine, radiotherapy, etc. in Bangladesh for diagnosis and treatment purposes. The implementation
of as low as Reasonably Achievable (ALARA) concept in medical practices following the three basic
radiation protection principles, namely justification, optimization and dose limitation is required as
per requirements of the IAEA GSR Part-3 [1]. These principles must be followed, first to reduce the
dose to patients without compromising the image quality and second to reduce the dose to
occupational workers. The dose assessment of occupational workers in medical practices is mandatory
as per requirements of the Nuclear Safety and Radiation Control (NSRC) Rules-1997 of Bangladesh.
Methods: Radiation protection in medical practice is performed by the following monitoring
methods:
(I) External monitoring by using Harshaw two element TLD-100 (LiF:Mg,Ti) cards for quarterly
basis throughout the country and TL chips for extremity and patient-dose monitoring;
(II) Workplace monitoring by using beta/gamma & neutron survey meters. Prime responsibility of
this method belongs to the licensee but is initiated by Health Physics division;
(III). Internal monitoring by indirect bio-assay method (urine samples of workers who are using
unsealed radioactive sources) and collection of air particulates at workplace by suction of indoor air
through filter paper using Staplex air sampler. The samples were measured by High Purity
Germanium (HPGe) Detector;
(IV) Arrangement of National Training Courses for occupational workers on radiation protection for
dissemination of knowledge through comprehensive theoretical and practical classes.
Results: The annual average dose for most (about 99 %) occupational workers was below the average
annual permissible dose limit. For a few (about 1 %) workers, the annual dose exceeded the average
annual dose limit of 20 mSv. The average annual dose of workers in four medical practices, namely
nuclear medicine, interventional cardiology, radiotherapy and radiology were found to be 0.34, 1.54,
0.24, and 0.18 mSv respectively. From this study, it is observed that the highest annual individual
dose incurred by the worker in interventional cardiology department is 49.37 mSv. The activity
concentration of artificial radionuclides in air filter ranged from 0.19 to 60.67 mBq/m3 with average
of 6.4 ± 0.0 mBq/m3 for
131I; from 0.25 to 40.27 mBq/m
3 with average 4.17 mBq/m
3 for
99mTc. The
activity concentration of 99m
Tc and 131
I in urine samples of workers ranged from 8.58 to 314.92 Bq/l
and 6.47 to 283.27 Bq/l respectively. The effective dose of 99m
Tc ranged from 0.402 to 14.7 µSv and
those of 131
I ranged from 0.12 to 5.58 µSv
Discussion: Although effective dose of an individual worker complies with the requirements of
NSRC Rules-1997 of Bangladesh, workers should follow the radiation protection procedures at
workplace in order to implement the ALARA concept.
Acknowledgement: Authors would like to thanks the GOB and IAEA for providing financial &
technical supports through the national projects to strengthen radiation protection infrastructure.
Reference: [1] Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards, IAEA, GSR
Part-3 (July 2014).
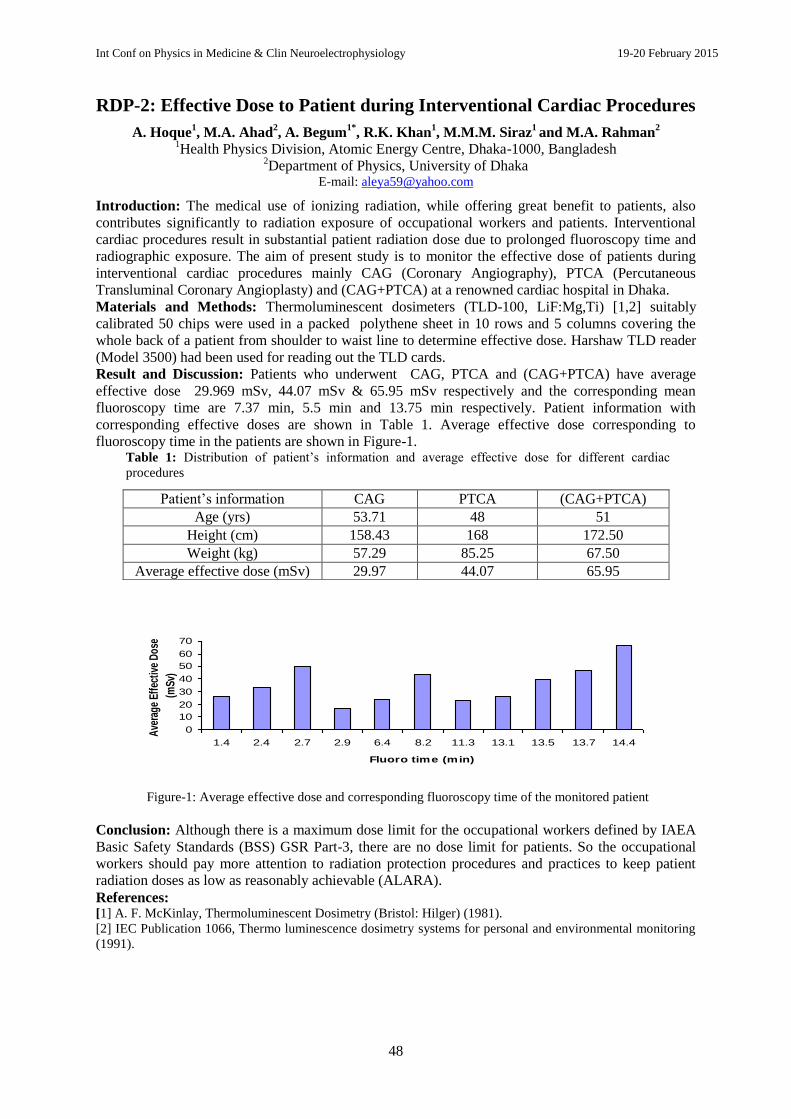
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
48
RDP-2: Effective Dose to Patient during Interventional Cardiac Procedures
A. Hoque1, M.A. Ahad
2, A. Begum
1*, R.K. Khan
1, M.M.M. Siraz
1 and M.A. Rahman
2
1Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh
2Department of Physics, University of Dhaka
E-mail: [email protected]
Introduction: The medical use of ionizing radiation, while offering great benefit to patients, also
contributes significantly to radiation exposure of occupational workers and patients. Interventional
cardiac procedures result in substantial patient radiation dose due to prolonged fluoroscopy time and
radiographic exposure. The aim of present study is to monitor the effective dose of patients during
interventional cardiac procedures mainly CAG (Coronary Angiography), PTCA (Percutaneous
Transluminal Coronary Angioplasty) and (CAG+PTCA) at a renowned cardiac hospital in Dhaka.
Materials and Methods: Thermoluminescent dosimeters (TLD-100, LiF:Mg,Ti) [1,2] suitably
calibrated 50 chips were used in a packed polythene sheet in 10 rows and 5 columns covering the
whole back of a patient from shoulder to waist line to determine effective dose. Harshaw TLD reader
(Model 3500) had been used for reading out the TLD cards.
Result and Discussion: Patients who underwent CAG, PTCA and (CAG+PTCA) have average
effective dose 29.969 mSv, 44.07 mSv & 65.95 mSv respectively and the corresponding mean
fluoroscopy time are 7.37 min, 5.5 min and 13.75 min respectively. Patient information with
corresponding effective doses are shown in Table 1. Average effective dose corresponding to
fluoroscopy time in the patients are shown in Figure-1. Table 1: Distribution of patient‘s information and average effective dose for different cardiac
procedures
Figure-1: Average effective dose and corresponding fluoroscopy time of the monitored patient
Conclusion: Although there is a maximum dose limit for the occupational workers defined by IAEA
Basic Safety Standards (BSS) GSR Part-3, there are no dose limit for patients. So the occupational
workers should pay more attention to radiation protection procedures and practices to keep patient
radiation doses as low as reasonably achievable (ALARA).
References: [1] A. F. McKinlay, Thermoluminescent Dosimetry (Bristol: Hilger) (1981).
[2] IEC Publication 1066, Thermo luminescence dosimetry systems for personal and environmental monitoring
(1991).
Patient‘s information CAG PTCA (CAG+PTCA)
Age (yrs) 53.71 48 51
Height (cm) 158.43 168 172.50
Weight (kg) 57.29 85.25 67.50
Average effective dose (mSv) 29.97 44.07 65.95
0
10
20
30
40
50
60
70
1.4 2.4 2.7 2.9 6.4 8.2 11.3 13.1 13.5 13.7 14.4
Fluoro time (min)
Ave
rage
Eff
ectiv
e D
ose
(mSv
)

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
49
RDP-3: Radiation dose of patient during CT scan
R.K. Khan1, Robiul Islam
2, A.Begum
1, A.Hoque
1 and N.Ferdous
2
1Health Physics Division, Bangladesh Atomic Energy Commission;
2Department of Physics, University of Dhaka.
E-mail: [email protected]
Introduction: CT (Computed tomography), also known as "computerized tomography" or "computed
axial tomography" (CAT) is a noninvasive medical procedure that uses specialized X-ray equipment
to produce cross-sectional images of the body. Figure 1 shows a typical CT scan [1]. Concern about
CT scans includes the risks from exposure to ionizing radiation. Organ doses from CT scanning are
considerably larger than those from corresponding conventional radiography [2]. The purpose of this
study was to measure the ionizing radiation dose to different organs of human body during CT scan.
Figure 1: Typical diagram of CT scan.
Methodology: Radiation dose obtained by the patients during CT procedures were measured at a
famous hospital in Bangladesh. For this purpose 50 calibrated chips arranged on a polythene sheet in
10 rows and 5 columns were used. The radiation exposures were read by using TLD reader
(HARSHAW 3500 Manual TLD reader) with hot nitrogen gas flow.
Results: Total 19 male and female patients were monitored. The dose range was from 0 to 233.1 mSv
and the average dose was found 42.80 mSv. The highest maximum dose, 233.1 mSv, was received by
a female patient during chest CT scan with 100ml contrast agent. Information regarding patient dose
for different regions of body is shown in Table 1. The maximum average dose to the patient incurred
during an abdomen scan. Table 1: CT scan of different regions of body and corresponding radiation dose.
Region of body Head Neck Chest Abdomen Ureter
Maximum dose (mSv) 89.23 152.00 233.10 233.00 26.15
Minimum dose (mSv) 0.23 0.00 0.36 0.71 0.00
Average dose (mSv) 22.81 41.37 30.50 72.94 10.98
Conclusion: The widespread use of CT probably represents the single most important advance in
diagnostic radiology. However, as compared with plain-film radiography, CT involves higher doses
of radiation. Since there is no dose limit which can be considered safe, strict measures should be
taken to avoid any unnecessary radiation exposure not only to patients but also to occupational
workers.
References:
[1] U.S. Food and Drug Administration, web link: Description, Computed Tomography.
[2] Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med.
2007 Nov 29;357(22):2277–2284.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
50
RDP-4: Assessment of Radioactivity of Soil in Madaripur District of
Bangladesh
A. N. Monika1, M.M. Rhaman
2, J. Ferdous
2*, A. Begum
2, N. Ferdous
3
1Medical Physics Unit, Bangladesh Atomic Energy Commission, Agargon, Dhaka, Bangladesh.
2Health Physics Division, Atomic Energy Centre, Shabagh, Dhaka-1000, Bangladesh.
3Department of Physics, University of Dhaka, Shabagh, Dhaka-1000, Bangladesh.
E-mail: [email protected]
Introduction: Human population are exposed to radiation that originates from a variety of sources,
such as exposure from natural sources and from manmade sources. Radiation from natural sources in
the environment is the major cause of radiation exposure to men. Uranium and thorium are two
dominant elements in the radioactive series that decays to many interesting isotopes such as radium
and radon along with radioactive lead. The specific activities of natural radionuclides in 12 soil
samples collected from Madaripur district of Bangladesh, have been studied and evaluated.
MATERIALS AND METHODS: Soil samples are collected at the depth of 0-5 inch from each
location with the use of a crowbar with great care. About 1 Kg of sample from each location is
collected in separate dry polythene bag labeled with proper identification code. At the lab, the
collected samples are transferred from the polyethylene bags to the acetone-cleaned stainless steel
bucket and dried in an oven at 100-105 0C until a constant weight is achieved. Each of the dried
samples were grounded to fine powder in an agate motor separately and sieved using a fine aperture
mesh screen in order to remove extraneous items like plant materials, roots, pebbles etc. and to obtain
a fine-grained sample that would present a uniform matrix to the detector. Each of the samples is
transferred to cylindrical plastic-container. The net weight of each sample is calculated using a
microbalance. The sealed containers of sample were stored for at least four weeks to reach secular
equilibrium between the 238
U and 232
Th series and their respective progenies to get ready for
measurements.The activity concentration of gamma ray emitting radioisotopes in the samples were
measured by using a gamma ray spectrometer with a high-resolution HPGe coaxial detector coupled
with a Silena Emcaplus multichannel analyzer (MCA).
RESULTS AND DISCUSSION: The activity concentration of 238
U ranged from 51.08 to 97. 35
Bq.kg-1
with mean 59.62 ± 12.62Bq.kg-1
. Activity concentration of 232
Th ranged from 16.60 to 59.44
Bq.kg-1
with mean 40.26 ±11.12 Bq.kg-1
. Activity concentration of 40
K ranged from 301 to 437 Bq.kg-
1 with mean 385 ± 37.15 Bq.kg
-1.
CONCLUSIONS: Soil is one of the major source and pathways of radio nuclides to living beings.
The average activities of 238
U and 232
Th in soil samples of the present study are higher than the world
average. On the other hand, the average activity of 40
K was found to be lower than the world average.
In addition, no evidence of 137
Cs was found in the collected samples. These findings are in
conformity with absent nuclear fallout in the places of study. Therefore it may be concluded that
natural radioactivity in soil samples of Madaripur district poses no health-hazards to the population
living there.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
51
RDP-5: Assessment of Occupational Exposure in Interventional Cardiology
practices
M.S. Rahman*, A. Begum. A. Hoque, R.K. Khan and M.M.M. Siraz
Health Physics Division, Atomic Energy Centre, GPO Box 164, Shahbag, Dhaka, Bangladesh E-mail: [email protected]
Introduction: Interventional cardiologists work in the catheterization laboratory for many hours,
some on a daily basis, usually for many years. Several reports found that the effective dose of ionizing
radiation in interventional cardiology practices were the highest ones registered among medical staff
using x-rays [1]. There is particular concern regarding occupational dose to the lens of the eye in
interventional cardiology practices. ICRP in April 2011 [2] recommended a new occupational dose
limit of 20 mSv/yr for the lens of the eye (100 mSv for 5 years and maximum 50 mSv in a year). This
recommendation has been incorporated into the International Basic Safety Standards, IAEA GSR
Part-3 [3]. Methods for reducing or minimizing occupational radiation dose includes: minimizing
fluoroscopy time and the number of acquired images; using available patient dose reduction
technologies; using good imaging-chain geometry; collimating; avoiding high-scatter areas; using
protective shielding; using imaging instruments that has equipment performance controlled through a
quality assurance programme; and wearing personal dosimeters. Effective use of these methods
requires both appropriate education and training on radiation protection for all interventional
cardiology personnel, and the availability of appropriate protective tools and equipment.
Methods: Occupational workers were monitored by using calibrated Harshaw two element TLD-100
(LiF:Mg,Ti) cards for quarterly basis. The workers wear the TLD badges (TLD-100 card with holder)
on torso during exposure to ionizing radiation. The quarterly effective doses of occupational workers
were assessed by measuring the TLD-100 cards with Harshaw TLD Reader Model 4500.
Results: The average annual effective dose of the occupational workers in interventional cardiology
practices is 1.54 mSv. The maximum annual dose of individual worker is 49.37 mSv. Table 1: Number of monitored workers in interventional cardiology by year
and received total dose.
Year Total Worker Total dose (mSv)
2010 104 108.29
2011 95 127.50
2012 95 208.03
2013 91 150.15
Discussion: Radiation dose of the workers are below the maximum permissible limit in a year.
However, workers must be aware about radiological protection in every procedure to keep the doses
below the average annual dose limit.
References: [1] Vano E, Gonzalez L, Guibelalde E, Fernandez JM, Ten JI. Radiation exposure to medical staff in
interventional and cardiac radiology, Br. J. Radiol, Vol. 71, pp. 954-60 (1998).
[2] International Commission on Radiological Protection (ICRP), the 2011 Recommendations of the
International Commission on Radiological Protection.
[3] Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards, IAEA, GSR
Part-3 (July 2014).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
52
RDP-6: Study of Radioactivity Level in Soil, Sand and Sediment Samples of
Coastal Area in Cox’s Bazar, Bangladesh and Evaluation of Radiation
Hazard
Sariful1, M.M.M. Siraz
2, S. Pervin
2, S. K. Das
1 and S. Yeasmin
2*
1Department of Environmental Sciences, Jahangirnagar University, Savar, Dhaka, Bangladesh
2Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh
E-mail: [email protected]
Introduction: Radiation is present in all environment of the earth‘s surface, beneath the earth and in
the atmosphere. According to UNSCEAR [1], about 87% of the radiation dose received by mankind is
due to natural radiation sources and the remaining is due to anthropogenic radiation.
Materials and Methods: Activity concentrations of natural and artificial radionuclide‘s (238
U, 226
Ra, 232
Th, 40
K and 137
Cs), outdoor and indoor annual effective dose rates and radiation hazard indices were
investigated using a high-purity germanium (HPGe) detector [2] in twenty four soil, sand and
sediment samples (each category consists of eight samples) collected from different coastal area of
Cox‘Bazar ranging about thirty kilometer.
Result and Discussion: Mean activity concentrations of the measured radionuclide is shown in
Figure-1 and annual effective dose rate & radiation hazard indices [3] are enumerated in Table-1.
Figure-1. Mean activity concentrations (Bqkg
-1) of the measured radionuclide‘s
Table-1. Annual effective dose rate and radiation hazard indices of the measured radionuclide‘s
Category Radium
equivalen
t activity
(Bqkg-1
)
Externa
l hazard
index
(Hex)
Interna
l
hazard
index
(Hin)
Outdoor
absorbe
d dose
rate
(nGy/h)
Indoor
absorbe
d dose
rate
(nGy/h)
Outdoor
annual
effectiv
e dose
rate
(mSv/y)
Indoor
annual
effectiv
e dose
rate
(mSv/y)
Total
annual
effectiv
e dose
rate
(mSv/y)
Maximu
m
174.54 0.47 0.56 85.31 102.37 0.13 0.50 0.63
Minimum 60.51 0.16 0.19 30.39 36.46 0.04 0.18 0.22
Average 122.75 0.33 0.40 59.73 71.67 0.09 0.35 0.44
Conclusion: In this study, no fallout of 137Cs was noted. Mean activity concentrations, annual
effective dose rates and radiation hazard indices of the measured radionuclides were below the
recommended value set by IAEA. Results obtained indicates that the study area is safe from
radiation hazard.
Reference: [1] United Nations Scientific Committee on the Effects of Atomic Radiation. Sources, effects and risk of
ionization radiation. Report to General Assembly. UNSCEAR (2000).
[2] Knoll, G. F. Radiation Detection and Measurement (3rd edition), USA: John Wiley & Sons Inc.
[3] International Atomic Energy Agency. Measurement of radio-nuclides in food and the environment.
Technical Report Series No. 295. IAEA (1989).
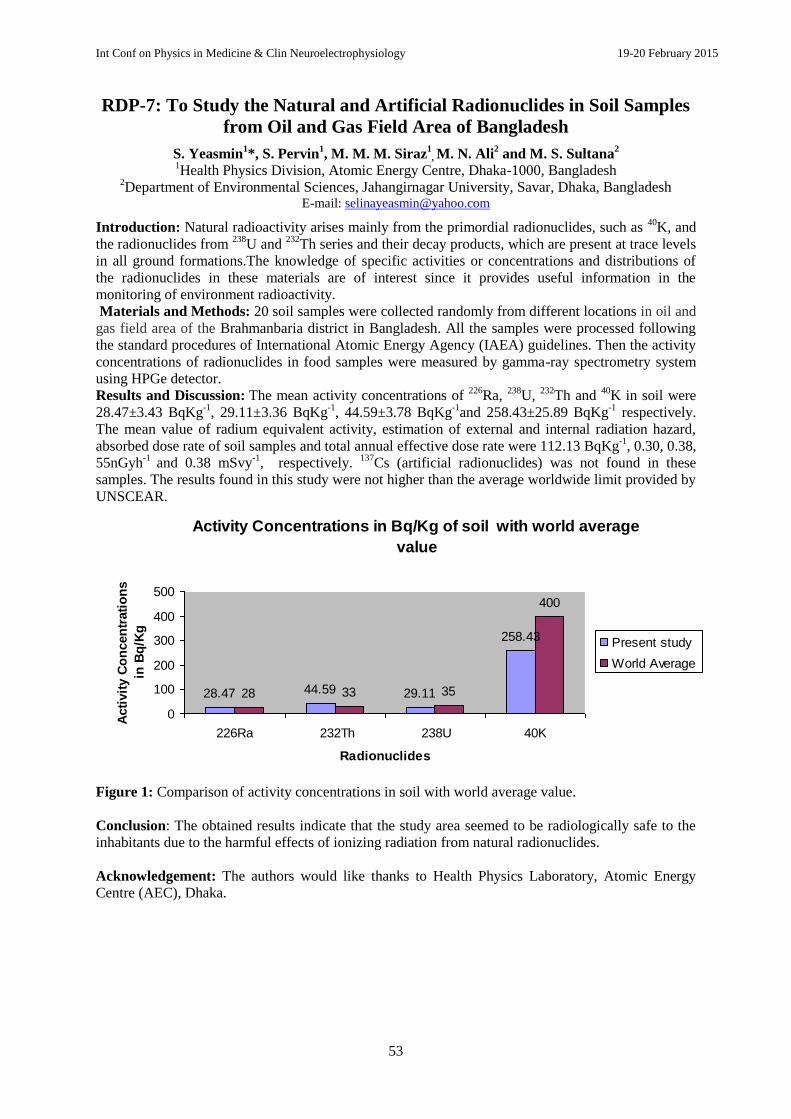
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
53
RDP-7: To Study the Natural and Artificial Radionuclides in Soil Samples
from Oil and Gas Field Area of Bangladesh
S. Yeasmin1*, S. Pervin
1, M. M. M. Siraz
1, M. N. Ali
2 and M. S. Sultana
2
1Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh
2Department of Environmental Sciences, Jahangirnagar University, Savar, Dhaka, Bangladesh
E-mail: [email protected]
Introduction: Natural radioactivity arises mainly from the primordial radionuclides, such as 40
K, and
the radionuclides from 238
U and 232
Th series and their decay products, which are present at trace levels
in all ground formations.The knowledge of specific activities or concentrations and distributions of
the radionuclides in these materials are of interest since it provides useful information in the
monitoring of environment radioactivity.
Materials and Methods: 20 soil samples were collected randomly from different locations in oil and
gas field area of the Brahmanbaria district in Bangladesh. All the samples were processed following
the standard procedures of International Atomic Energy Agency (IAEA) guidelines. Then the activity
concentrations of radionuclides in food samples were measured by gamma-ray spectrometry system
using HPGe detector.
Results and Discussion: The mean activity concentrations of 226
Ra, 238
U, 232
Th and 40
K in soil were
28.47±3.43 BqKg-1
, 29.11±3.36 BqKg-1
, 44.59±3.78 BqKg-1
and 258.43±25.89 BqKg-1
respectively.
The mean value of radium equivalent activity, estimation of external and internal radiation hazard,
absorbed dose rate of soil samples and total annual effective dose rate were 112.13 BqKg-1
, 0.30, 0.38,
55nGyh-1
and 0.38 mSvy-1
, respectively. 137
Cs (artificial radionuclides) was not found in these
samples. The results found in this study were not higher than the average worldwide limit provided by
UNSCEAR.
Figure 1: Comparison of activity concentrations in soil with world average value.
Conclusion: The obtained results indicate that the study area seemed to be radiologically safe to the
inhabitants due to the harmful effects of ionizing radiation from natural radionuclides.
Acknowledgement: The authors would like thanks to Health Physics Laboratory, Atomic Energy
Centre (AEC), Dhaka.
Activity Concentrations in Bq/Kg of soil with world average
value
28.47 44.59 29.11
258.43
28 33 35
400
0
100
200
300
400
500
226Ra 232Th 238U 40K
Radionuclides
Acti
vit
y C
on
cen
trati
on
s
in B
q/K
g
Present study
World Average

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
54
RDP-8: Assessment of Natural Radioactivity Level in Different Vegetable
Samples of Brahmanbaria District in East-Central Bangladesh
S. Yeasmin1*, S. Pervin
1, M. M. M. Siraz
1, M. N. Ali
2 and M. S. Sultana
2
1Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh
2Department of Environmental Sciences, Jahangirnagar University, Savar, Dhaka, Bangladesh
E-mail: [email protected]
Introduction: Naturally occurring radioactive materials exists in soil, water, air, food, and even in
our own bodies. The activity concentrations of natural radionuclides such as 226
Ra, 238
U, 232
Th and 40
K were measured for 20 vegetable samples from Brahmanbaria district of Bangladesh.
Materials and Methods: A total of 20 vegetable samples were collected from 20 different points of
the of Brahmanbaria district which is in east-central Bangladesh. The vegetable samples were first
washed with water to remove all attached dust particles. Next, the samples were kept in a tray to be
sun dried for 48 hours. After that, further drying was done in the oven at 105°-110° C temperature for
48 hours. Then all the samples were kept at room temperature for about 30 days to ensure that 238
U
and its daughter products were in secular equilibrium. Then the activity concentrations of
radionuclides in food samples were measured by gamma-ray spectrometry system using HPGe
detector.
Results and Discussion: The mean activity concentrations of 226
Ra, 238
U, 232
Th and 40
K in vegetables
samples were found to be 62.50±16.39 BqKg-1
, 52.91±16.19 BqKg-1
, 67.13±13.60 BqKg-1
and
1412.10±153.81 BqKg-1
respectively. The radioactive 137
Cs was not found in these samples. In this
study the result for 232
Th was slightly higher than the average worldwide limit provided by
UNSCEAR whereas the results for other radionuclides were below the international level. The
slightly increased 232
Th level is however not significant.
Figure 1: Graphical representation of activity concentrations in vegetable with world average value.
Conclusion: The results of the radioactivity levels measured in east-central Bangladesh can be
considered as baseline data for reference in any future studies.
Reference: [1] UNSCEAR Ionizing Radiation, Sources and Biological effects, United Nations Scientific Committee on the
Effect of Atomic Radiation, United Nations, New York (1982).
[2] G. F. Knoll, Radiation Detection and Measurement, 2nd Edition (USA: John Wiley and Sons) (1989).
[3] International Atomic Energy Agency, Measurement of radionuclides in food and the environment.
Technical Report Series No. 295 (Vienna: IAEA) (1989).
62.5
318
67.13 53 52.91
318
0
50
100
150
200
250
300
350
Acti
vit
y
Co
ncen
trati
on
s in
Bq
/Kg
226Ra 232Th 238U
Radionuclides
Present study
World Average

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
55
RDP-9: Assessment of Radionuclide Transfer from Soil to Vegetable in
Brahmanbaria District, (Bangladesh) using Gamma-Ray Spectrometry
System
S. Yeasmin1*, S. Pervin
1, M. M. M. Siraz
1, M. N. Ali
2 and M. S. Sultana
2
1Health Physics Division, Atomic Energy Centre, Dhaka-1000, Bangladesh
2Department of Environmental Sciences, Jahangirnagar University, Savar, Dhaka, Bangladesh
*E-mail: [email protected]
Introduction: Soil-vegetables are recognized as one of the major pathways for the transfer of
radionuclides to human beings. Transmission of uranium and thorium along with nutrients through the
absorption of minerals, and accumulate in various parts or even up to the edible parts. Transfer factor
(TF) is a useful parameter for the radiological assessment. Radionuclide is necessary to determine and
estimate the activity of various radionuclides present in soil and their transfer factors are different in
different food samples. This difference helps assess the radiation doses in human beings, the ultimate
consumers of food. Three adjoining upazila Saril, Ashugonj and Brhmanbaria Sadar upazila of
Brhmanbaria district, situated at the central East part of Bangladesh and about 90 Km East to the
Capital were selected as the study area.
Materials and Method: Total 40 samples (20 soil samples and 20 associated vegetable samples)
were collected from locations of Brhmanbaria district. Brinjal (Solanum melongena), Winter melon
(Benincasa hispida), Ladysfinger (Abelmoschus esculentus), Bitter gourd (Momordica charantia),
starfruit (Averrhoa carambola), Data Shakh (Amaranthus gangeticus), Banana (Musa sapientum),
Pomelo (Citrus grandis), Papaya (Carica papaya), Pumpkin (Cucurbita maxima), Mango (Mangifera
indica), Kidney bean (Vigna sinensis) were the selected vegetable samples. All prepared samples were
measured by means of gamma-ray spectrometry system using high purity Ge-detector (HPGe).
Transfer factor (TF) is defined as the ratio of radionuclide concentration in a soil (in Bq kg-1
dry
weight) and concentration of the radionuclide in the vegetable (in Bq kg-1
dry weight).
Results and Discussion: The transfer factor soil-to-vegetable was observed 2.43, 1.92, 1.56 and 5.66
respectively for 226
Ra, 238
U, 232
Th and 40
K. The highest transfer factor of 226
Ra and 238
U were found in
the Papaya and Brinjal respectively and 232
Th and 40
K were found in Data Shakh. The sequence of the
transfer factors is in order of 40
K 226
Ra 238
U 232
Th. While the lowest transfer factor of was found
in Pumpkin and 238
U, 232
Th and 40
K were found in Mango. The results are low and within the range of
internationally recommended limits and no significant radiological hazard was found.
Conclusion: The results of this study may be considered as the baseline levels of radio activities in
the foodstuffs in these studied areas of Bangladesh to check future activities in the area.
Acknowledgement: The authors thankful to all stuff of Health Physics Division, Atomic Energy
Centre (AEC), Dhaka, for helping to perform this experiment successfully.
Reference: [1] UNSCEAR Sources and effects of ionizing radiation, A Report to the general assembly with scientific
annexes (New York: United Nations) (2000).
[2] International Atomic Energy Agency, Measurement of radionuclides in food and the environment. Technical
Report Series No. 295 (Vienna: IAEA) (1989).
[3] G. F. Knoll, Radiation Detection and Measurement, 2nd Edition (USA: John Wiley and Sons) (1989).
[4] International Atomic Energy Egency, generic models and parameters for assessing the environmental
transfer of radionuclides from routine releases. Exposure of Critical Groups Safety Series, Vienna (1982).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
56
Invited Talk
IPM-5: Lessons Learned From Major Radiotherapy Accidents:
International and Bangladesh Perspectives
A. S. Mollah
Department of Medical Physics,
Khwaja Yunus Ali University, Enayetpur, Sirajgonj, Bangladesh E-mail: [email protected]
Background: In order to avoid accidents in radiotherapy, it is very important to remember the lessons
that can be learned from previous radiotherapy accidents and to ensure that preventive actions are
applied in a clinical setting.
Case Histories of Radiation Accidents in Radiotherapy Practices: A number of accidents have
been thoroughly investigated and the lessons learned have been disseminated by the International
Atomic Energy Agency (IAEA). The complexity of medical radiation technology has created new
avenues for error-through software flaws, faulty programming, poor safety procedures or inadequate
staffing and training. When those errors occur, they can be deadly. Regulators and researchers can
only guess how often radiotherapy accidents occur. Accidents are chronically underreported, and
some countries do not require that they be reported at all. In USA (2013), a Philadelphia hospital gave
the wrong radiation dose to more than 90 patients with prostate cancer—and then kept quiet about it.
In 2005, a Florida hospital disclosed that 77 brain cancer patients had received 50 percent more
radiation than prescribed because a powerful linear accelerator had been programmed incorrectly for
nearly a year. Preventing errors in the delivery of radiation therapy involves not only understanding
and appropriately utilizing new advances in technology, but also utilizing established patient safety
procedures that optimize safe healthcare delivery. Major accidental exposures occurred in the absence
of quality assurance programme and written procedures and checks.
Specific lessons learned from some of the major radiotherapy accidents are reviewed and discussed in
this paper to create awareness in the radiotherapy practices in order to prevent radiation accidents in
Bangladesh.
Procedures for Radiation Accident Prevention: Accidental exposures have occurred when there is a
lack of procedures and checks, or when they are not comprehensive, documented or fully
implemented, e.g. independent checks. Accidental exposures have occurred when there is a lack of
qualified and well-trained staff or lack of staff overall), with necessary educational background and
specialized training. Accidental exposures have occurred owing to inattention to details, and lack of
alertness and awareness. The major recommendations to be implemented for overall preventive
measure are: i) Quality Assurance Program, ii) Education and training, iii) Acceptance testing and
commissioning, iv) Follow-up of equipment faults, v) Written communication policy, and vi) External
independent audits.
Conclusion: Lessons have been learned from investigations into a relatively large number of
accidents that have occurred in radiotherapy practices. Radiation accident in radiotherapy practices is
normally caused by poor education and training of radiotherapy medical physicists and by a lack of
quality assurance which allowed the error to remain undetected. The absence of written procedures
and protocols for acceptance tests and the commissioning of new equipment have led to the use of
incorrect values of basic parameters subsequently used for the treatment of patients. Given the
complexity of radiotherapy and its sensitivity to errors and mistakes, nothing should be left to chance,
but rather, a structured and systematic approach is needed. Licensing of a radiotherapy department
should be conditional on a comprehensive quality assurance program being in place. At the licensing
stage, regulatory authorities should verify that managers are fully aware of the potential for accidents
and their consequences and that this awareness is reflected in an unambiguous policy and appropriate
supervision. Regulatory authorities can actively contribute to this awareness by disseminating
information on real accidents, case histories and pictures of the effects of radiation from accidents.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
57
RT-4: Dosimetry and Quality Assurance (QA) of photon and electron beam
of medical linear accelerator at Oncology Centers in Bangladesh
Md. Shakilur Rahman1*
, Md. Abdus. Sattar2, S. M. Enamul Kabir
3, Debasish Paul
1,
M. Shamsuzzaman1, M. Mosharraf Hossain Bhuyian
1, M. Abdullah-Al Maruf
4,
Md. Mushtaq. Ahmed4, AKM Moinul Haque Meaze
2
1Secondary Standard Dosimetry Laboratory, Institute of Nuclear Science & Technology,
Bangladesh Atomic Energy Commission, Savar, Dhaka, Bangladesh 2Department of Physics, University of Chittagong, Chittagong, Bangladesh
3Department of Radiation Oncology, National Institute of Cancer Research and Hospital, Dhaka,
Bangladesh 4Department of Radiotherapy, Dhaka Medical College Hospital, Dhaka, Bangladesh
*E-mail : [email protected]
Introduction: Medical linear accelerator (LINAC), a potential source of photon and electron beam
are being used in curative and palliative treatment modality for a variety of cancers. It provides the
facility of treatment with high energy x-rays for tumor at depth and electron beam for superficial
structure near the skin and soft tissue. The aim of radiation therapy by LINAC is to maximize killing
of cancer cells in a tissue by radiation beam keeping the sparing of healthy cells at acceptable level.
The effectiveness of the output of treatment is highly dependent on the radiation dose being delivered
to the treatment site. Tumor eradication and normal tissue complications correlate to dose absorbed in
tissue. The clinical practice leads to generally agreed recommendations on the required accuracy in
clinical dosimetry for radical curative being given in ICRU report-24 (1976) for at least accuracy of
±5%.
Materials and Methods: The output dose measurement of Clinac 2100 of photon beam of energy
6, and 15 MV and electron beam of energy 6, 9, 12, 15, and 18-MeV of Dhaka Medical College and
Hospital, and National Institute of Cancer Research and Hospital have been measured with semiflex
ionization thimble chamber TW31010 and parallel plate ionization chamber TW23343, & A10 using
PTW water phantom at reference condition. Two different dosimetry protocols TRS-398 and AAPM
TG-51 were used in the present measurement.
Results: The measured dose of 6 MV and 15 MV photon beams have also been verified with the
international system by the participation of the IAEA/WHO TLD postal dose intercomparison
program for radiotherapy level dosimetry. The ratios found in that intercomparison program of IAEA
mean dose to user stated dose were 1.00 and 1.01 which lies with an excellent agreement within IAEA
limit 0.95-1.05. The dosimetry of electron beam has been measured by thimble and parallel plate
ionization chamber and a deviation between the chambers have been observed with a maximum
3.22% at lower electron energy 6 MeV. The perturbation effect in respect to electron beam energies
are also described.
Conclusions: The dose ratios of TRS 398 in comparison with AAPM codes of practice TG-51 were
in good agreement with IAEA-TECDOC-1455. The accuracy of dose determination using absorbed
dose to water based protocol will reduce the uncertainty of dose measurement. The dosimetry of
electron beam by two different chambers; parallel plate and cylindrical type shows a large variation of
doses at lower electron energy due to Pwall correction factor in determination of kQ,Qo. This large
variation could be reduced while using parallel plate chamber below 15 MeV.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
58
RT-5: Beam Data Acquisition of an Accelerator and Commissioning of
CMS XiO 4.8 Treatment Planning System
MA Sabur1, Hirak Kumar Dey
1, M A Hai
2, M A Bari
3, Basu Saumen
2, S Deepak Ray
2
1Department of Medical Physics, Kyamch Cancer Center, Sirajgonj, Bangladesh.
2Department of Radiation Oncology, Kyamch Cancer Center, Sirajgonj, Bangladesh.
3Department of Oncology, BSMMU, Dhaka, Bangladesh.
Introduction: Cancer is one of the most significant health problems with respect to its incidence and
mortality alike. Globally more than 50% cancer managements are carried out using ionizing radiation
or its combination with surgery and or chemotherapy. The main goal of the radiation therapy is to kill
the cancerous cell and save the surrounding normal structures. Accurate beam data acquisition
during commissioning is essential for modeling the treatment planning system (TPS) and dose
calculation in radiotherapy.
Methods: All the basic data of linear accelerator and Comercial Medical System (CMS) XiO 4.8 have
been used as input data for the TPS. The Machine data, Percentage Depth Dose (PDD), Beam
Profiles, Total Scatter Correction Factor (TSCF), Collimator Factor (Sc), Peak Scatter Correction
Factor (PSCF), and Wedge Factor (WF) have been collected according to CMS XiO instructions and
the above data have been transferred to the TPS.
Results: The information in the data files of the accelerator was found to agree in all aspects with the
output data obtained from the TPS. The absolute doses calculated at the reference point for photon
beam were in agreement with those of measurements for both open and wedged fields. The errors
were within the limit of truncation errors. It should be noted that this error includes uncertainties due
to the phantom setup and the difference of the protocol such as step size, measurement time and
scanning methods.
Conclusions: It is concluded that implementation of a CMS XiO 4.8 Treatment Planning System is
very suitable for accurate radiation therapy treatment planning and its practical use would decrease
the uncertainty in radiotherapy.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
59
RT-6: Verification of a Computer Treatment Plan by Manual Methods
Muhammad Masud Rana1, G. A. Zakaria
2, Gϋnther Hartmann
3, Sarwar Alam
1,
Zillur Rahman Bhuiyan1, Jamal Uddin
1
1Oncology Department, Bangabandhu Shekh Mujib Medical University, Shahbagh, Dhaka,
Bangladesh 2Gummersbach Hospital, Academic Teaching Hospital of the University of Cologne, Germany,
3German Cancer Research Center, Heidelberg, Germany.
E-mail: [email protected], [email protected], [email protected]
Introduction: Treatment planning prior to the 1970s was generally carried out through the manual
calculation from the charts onto patient body contours that were generated by direct tracing or lead
wire. The simultaneous development of computerized tomography lead to the development of CT-
based computerized treatment planning providing the ability to view dose distributions directly
superimposed upon patients axial anatomy.
Methods and Materials: Different dosimetric quantities such as dose rate in phantom, percentage
depth dose and output factor were measured in PTW water phantom for a Linear Accelerator
PRIMUS II (Siemens) using a Farmer ionization chamber of Type PTW 3006. The applied photon
beam energy was 6 MV. In addition, a patient equivalent phantom was used to calculate dose
distribution using computerized treatment planning system (TPS). The computer treatment planning
dose distributions have been verified with manual dose calculation. A three-field techniques such as
Field 1 at 0°, field 2 at 120° and field 3 at 240° with three different field sizes of 8.6x12 cm2, 11.2x12
cm2 and 10.7x12 cm
2 of isometric technique have been used for treatment planning purpose at the
Alderson phantom in the thorax level. Computerized TPS used in this study was KONRAD of the
German Cancer Research Centre (DKFZ). Simple treatment planning based on a hardcopy of the CT
slice through the lung region of the Alderson phantom showing the position of the target volume, the
point and the central ray of the three fields.
Figure 1 Results: About 75 MU (Monitor unit) was required to apply 2 Gy by TPS calculation for field 1, 2 &
3 respectively. On the other hand, monitor units required to apply 2 Gy by manual calculation for field
1, 2 & 3 were found to be 67 MU, 76 MU and 86 MU, respectively.
Discussion: The results of manual calculations deviate from TPS calculations by 10%, 1 % and 12%
for field 1, field 2 and field 3 respectively. In case of field 2 both results coincide well but of the other
two they do not because the pathways of beams are more inhomogeneous densities.
Conclusion: Central axis calculations can be performed very easily and straight forward. They agree
very well with results of computer-based TPS. Therefore, manual calculations should be used to
check the computer results, especially if a new TPS is being to be commissioned.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
60
RT-7: Verification of TPS dose calculation by means of measurements with
virtual solid water phantom and ion chamber: Preliminary results
A.S. Mollah* and M.N. Sharmeen
KYAMCH Cancer Center, Enayetpur, Sirajgonj *Department of Medical Physics, Khwaja Yunus Ali University, Enayetpur, Sirajgonj.
Introduction: The administration of radiation therapy (RT) in the management of any cancer calls for
a quality assurance (QA) program to ensure the best possible treatment for the individual patient.
Quantitative verification of the prescribed daily dose is of paramount importance during RT to ensure
precision in patient setup and accuracy in dose delivery. The verification of dosimetric accuracy
requires the comparison of the prescription dose to the patient as determined by a customized
treatment plan to the dose that is actually delivered. The verification of accuracy in dose delivery
involves the comparison of prescribed dose as determined from a customized treatment plan [monitor
units (MU), minutes etc.] to the dose that is actually received by the patient. In an effort to implement
a comprehensive QA program via dose verification at our cancer center, as a first step, we tested the
feasibility of using a commercial virtual solid water phantom with ion chamber for patient dose
verification against TPS dose values. It is widely accepted that an accuracy of dose delivery of about
3.5% (1σ) is required in modern radiotherapy. This paper describes our preliminary experience with
the control of dose delivery and TPS dose calculations at the reference point in the phantom.
Materials and methods: The calculations of dose at the reference point performed with the treatment
planning systems (such as PrecisePlan, CMS XiO and Ergo++) were checked by measurements carried
out in the virtual solid water phantom. All measurements were performed with the ion chamber
positioned in the phantom, at the central axis of the beam, at standard depth and with the UNIDOS
electrometer. The dose was measured according to IAEA TRS 398 report for measurements in solid
phantoms. The measurement results were corrected with the actual accelerator‘s output factor and for
the non-full scatter conditions. Measurements were made for 10 fields on the Elekta Synergy linear
accelerators for each photon treatment field.
Preliminary results: The average differences between measurements and calculations were 3.2%
(SD = 1.1%) for total dose measurements. The greatest advantage of the dose verification with the
solid water phantom is that it allows verification of dose calculation and delivery directly to the point
of interest. Further works on total dose measurements are in progress for patient specific fields.
Conclusion: A method has been developed for verification of TPS dose calculation by means of
measurements with virtual solid water phantom and ion chamber. The verification method provides an
instantaneous verification of dose calculations before the beginning of a patient‘s treatment. It allows
detecting differences smaller than 3.5%.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
61
RT-8: Evaluation of Radiation Doses at Organ-at-Risk Due to Tangential
Breast Cancer Radiotherapy at Kyamch Cancer Center During 2012-13
Sharmin, MN, Mollah, AS*, Hai, MA and Bari, MA
Khwaja Yunus Ali Medical College Hospital Cancer Center, Enayetpur, Sirajgonj. *Department of Medical Physics, Khwaja Ynus Ali University, Enayetpur, Sirajgonj.
E-mail: [email protected]
Introduction: Radiation dose distribution plays an important role in the outcome of radiation
treatment. The objective of this study is to quantify the radiation doses received by the organ at risk
(OAR) from such a tangential breast or chest wall radiotherapy.
Methods: Ten patients were selected for this study having left/right-sided breast cancer treated at
KYAMCH Cancer Center during 2012-2013. All patients were positioned on a breast board with the
sternum horizontal to the treatment couch and both arms above the head. Patients were scanned with a
wide-bore simulator, with 5-mm slices, from the clavicle to the diaphragm. Computerized tomography
data and treatment parameters were exported to a computerized treatment-planning system. All
patients were irradiated with 6 MV tangential beams to the breast or chest wall. All patients had
isocentric treatment with a tumor dose of 50 Gy per 25 fractions in 5 days per week. For each
treatment plan, dose–volume histograms (DVHs) for the heart and for the lung were generated using
treatment planning system.
Results: For left-sided 5 patients, the heart was close to the tangential fields and the average mean
heart dose was 7.52 Gy. In contrast, for the 5 patients who received right-sided irradiation, the heart
was distant from the fields. It received scattered dose alone (i.e., dose from radiation outside the
radiotherapy beams), and the average mean heart dose was observed to be 1.5 Gy. Mean heart dose
ranged from 1.5 to 7.52 Gy for all left- and right-sided irradiation. Thus the mean heart dose from left-
sided irradiation was approximately five times higher than the dose from right-sided irradiation. For
the 5 patients who were given left-sided irradiation, the average mean dose was 19.3 Gy to the Lt.
Lung and for the 5 patients given right-sided irradiation, the average mean dose was 18.8 Gy to the
Lung. Patient-to-patient dose variability was observed and was largely determined by differences in
patient anatomy.
Conclusion: The breast cancer patients have been treated with a 2-field radiotherapy technique,
which includes the axillary, supraclavicular and internal mammary nodes as well as the chest wall.
The study has provided satisfactory dose homogeneity within the volume of interest, and an
acceptable dose to critical structures such as the heart and lung.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
62
RT-9: Comparison of Dosimetric studies of 3 Dimensional conformal
radiotherapy and Intensity Modulated Radiotherapy of Brain Tumours
from CMS XIO TPS in KYAMCH
Hirak Kumar Dey, Md. Abdus Sabur, Saumen Basu, Deepak S. Ray, M.A. Hai, M.A. Bari
Khwaja Yunus Ali Medical College Hospital Cancer Centre, Enayetpur, Sirajgonj
Introduction: Radiotherapy aims to give the prescribed dose to the tumour and to protect as much as
possible the organs at risk and surrounding healthy tissue. The radiotherapy nowadays, together with
chemotherapy and surgery, is a way to treat the patients which have different kind of tumours.
Intensity-modulated radiation therapy (IMRT) is an advanced technique of high-precision
radiotherapy that uses computer-controlled linear accelerator to deliver precise radiation doses to a
malignant tumour or specific areas within the tumour. IMRT allows for the radiation dose to conform
more precisely to the three-dimensional (3-D) shape of the tumour by modulating or controlling the
intensity of the radiation beam in multiple small volumes. Also it allows higher radiation doses to be
focused to regions within the tumour while minimizing the dose to surrounding normal critical
structures. The main advantage of IMRT is 70% of the tumours do have a concave shape where 3D
CRT gives more doses to the OAR (Organ at risk) and cannot follow the shape of the tumour where
IMRT can cover the shape of the tumour providing better tumour control and minimal doses to the
OAR‘s.
Methods and Materials: In this study are taken into account five patients with Brain tumours. The
patients are scanned in the Phillips CT simulator. The slices‘ thickness is 3 mm and then the images
are transferred to the Monaco Sim. Also from the Hospital MRI machine we take the MRI images for
the same patients and send them to Monaco Sim. The Monaco Sim is the system where the
oncologists delineate the target volumes and the organs at risk by Fusing the Images of CT and MRI.
Then the images go from Monaco Sim to the CMS XIO treatment planning system. It is composed of
several modules; the most important are module of patients‘ data, including patient demographic and
anatomic data and the teletherapy planning module.
Results and Discussion: Three dimensional conformal radiotherapy and intensity modulated
radiotherapy plans were performed for five patients with Brain tumours. Dosimetric comparison is
done first according to dose-volume histograms and then according to time consuming QC checks.
For all organs at risk such as Retina, Eye Lens, Pituitary, Optic Chiasma, Brain Stem, Optic Nerve,
Temporal Lobes the Maximum Dose, Mean Dose and the desired dose for the specific OAR volume
were all taken into account. It is observed that the average doses, for all patients, are much lower in
IMRT technique then in 3D CRT giving better tumour coverage.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
63
RT-10: Planning and Delivery of 3D Conformal, Classic and fitting PTV
(C3DCRT and f3DCRT) vs. Intensity Modulated Radiation Therapy
(IMRT): A Dosimetric Evaluation and Comparison of Case Studies
Sadiq R. Malik, Motiur Rahman, Shohel Reza, A. Jobber, Mohsin Mia,
M. S. Sarwar Alam and Parvin A. Banu
Radiation Oncology Division, Delta Hospital Ltd., Bangladesh; E-mail: [email protected]
Introduction: Treatment plans for Cancer Patients are executed by examining combinations of
Software, Hardware and Human ware. This paper enunciates the fundamental protocols and
guidelines to review a treatment plan before accepting it by Radiation Oncologists. This requires
flawless imaging (CT, MRI and PET), target volume delineation, organ at risk identification, dose
overlap and dose inhomogeneity correction, DVH of all adjacent organs and tolerance doses of
relevant organs and, finally, avoidance of hot or cold spots. Differential DVH curve is examined
before accepting the treatment plan.
In our study at DHL we observe that in some cases (i.e. prostate Larynx with N.N Mets and Neck
Node Mets) it needs very complex plan to save the organ at risk. In that case it is better to use IMRT
instead of 3DCRT. In DVH study we can see the dose differences in all of our studies. Since 1991
oncologists started to consider partial organ doses to limit uncertainties and limitations to fulfill a
clinical need. QUANTEC summary presents the Dose/Volume/Outcome of several organs following
conventional fractionation.
Methods: Image quality is of paramount importance in securing the quality of the plan with an
accurate contouring. A number of patients are chosen where 3DCRT and IMRT plans were executed.
The comparable data on DVH, OAR, Dose-Volume data and the prognosis of the choice of modality
of treatment were evaluated and explained. Target coverage and target dose distribution were
evaluated in the GTV, CTV, and PTV to determine the target dose. The minimal dose to 95% of the
volume (GTV95, CTV95, and PTV95) is assured. OAR and normal tissue avoidance ware evaluated
using the parameters of organ volume and the minimal dose received by 5% or less of the volume e.g.
bladder D5. Optimization of a treatment plan is completed before the acceptance of the treatment
plan.
Results: Target Coverage and Target Dose Distribution using 3DCRT and IMRT plans on similar
anatomical sites are compared and tabulated for prescription Dose (Rx), Dose Coverage 95% volume
of PTV and the doses at the organs at risk for the above two modalities of treatment. DVH and the
differential DVH are also examined by the treatment planner and the physician where the target
coverage, hot and cold spots are viewed when the treatment plan is modified to be acceptable for
delivery of the plan to treat the patient.
Conclusion: Optimization of a treatment plan is critically examined to meet those constraints before
acceptance of the plan. IMRT plan algorithm uses small beams of non-uniform fluence and gantry
angles where the volume of target is judged. The beam angles are optimized to avoid overlap of
beams. 3DCRT has capabilities of using wedges and transmission blocks to shape the isodose
coverage of the target even at an irregular site of a body shape.
Plan Quality Variation (PQV) is significant which can involve cancer patients. Treatment Plan Dose
and Dose Volume Histogram predictions (pDVH) use patient-specific anatomical (OAR) DVH for a
Quality Plan (QP). The study is designed to compare the degree of target coverage and target dose
distribution, Rx, conformality, normal tissue avoidance and amount of irradiated body volume in
IMRT, c3DCRT and f3DCRT.The Quality Plan is then approved for the delivery of treatment at the
prescription dose (Rx).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
64
RT-11: Calibration Of 192
ir High Dose Rate Brachytherapy Source Using
Different Calibration Procedures 1Md.
Harun Or Roshid,
1 Muhammad Masud Rana,
1Taskin Dilshad,
2Mohammad Abdullah Al
Maruf, 1Jamal Uddin,
1Sarwar Alam,
1Shamsun Nahar,
4Md. Shakilur Rahman
1 Dept of Oncology, Bangabandhu Sheikh Muzib Medical University, Shabagh, Dhaka, Bangladesh
2Dhaka Medical College Hospital,Dhaka
4Secondary Standard Dosimetry Laboratory (SSDL), Bangladesh Atomic Energy Commission, Savar,
Dhaka E-mail: [email protected]
Introduction: Calibration of Ir-192 high dose rate (HDR) brachytherapy source using different
calibration methods and to determine the accuracy and the suitability of each method for routine
calibrations are described here. The source calibration is an essential part of the quality assurance
programme for dosimetry of brachytherapy sources. The clinical use of brachytherapy source requires
an independent measurement of the air kerma strength according to the recommendations.
Materials and methods: Sources are calibrated in three techniques- Free in air Measurement, Well
type ionization chamber, Solid phantom (Krieger Phantom). Well type and and Free in air
measurement techniques are recommended by IAEA(International Atomic Energy Agency) and Solid
phantom technique is recommended by German Society of Medical Physics (DGMP). In this paper
we have calibrated the HDR Ir- 192 source by using three techniques. For Free in air measurement &
Solid phantom techniques. We have used Microselectron HDR machine, Microselectron V2
Iridium192 HDR source, Serial Number (S/N) –D36B1582, Farmer type Ionization chamber 0.6cm3
type PTW M30002, S/N- 0209 and PTW 0.3cm3 rigid chamber which type PTW M23332, serial
number 067 and a Unidos Electrometer. For Well type ionization chamber technique We have used
Gamma Med Plus HDR machine, 192-Ir source which type IR-192 GAMMAMED PLUS 0.9MM,
S/N-NLF-01D24B-088, a Well Type Ionization Chamber –HDR 1000PlLUS, S/N- A03447 (Standard
Imaging) and an Electrometer Type CD2x2000B, S/N- JO33354 (standard Imaging).
Results: The RAKR determined using different calibration methods were in good agreement with the
manufacturer stated value. The deviation between measured and quoted source strength by
manufacturers was found to be 0.46% for solid phantom technique, 0.469% for Well type ionization
chamber technique and 2.78% in free in air measurement technique, which was within tolerance the
limit (±3%).
Conclusion: Measurements with a well-type chamber are relatively simple to perform. For in-air
measurements, the indigenously designed calibration jig provides an accurate positioning of the
source and chamber with minimum scatter contribution. The room scatter correction factor was
determined by a method based on the inverse square law. Various other correction factors were
applied on measured air kerma values at multiple distances and mean value was taken to determine
the reference air kerma rate of the source. The solid phantom system has an advantage that no
additional phantom and chamber are required other than those used for Rectum and Bladder point
dosimetry. All the methods of calibration discussed in this study are effective to be used for routine
calibration purposes.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
65
RT-12: Treatment Outcome Of Radiation Alone Versus Concurrent
Chemoradiation On Unresectable Non- Small Cell Lung Cancer 1 Md. Jamal Uddin,
1Sarwar Alam,
1Md Shahidul Islam,
1M. A. Bari,
2Toufiq Hassan Firoz,
3Mustafa Aziz Sumon,
1Muhammad Masud Rana,
1Md. Harun Or Roshid and
1Taskin Dilshad
1Dept. of Oncology, Bangabandhu Sheikh Muzib Medical University, Shabagh, Dhaka
2National Institute for Cancer Research & Hospital, Dhaka,
3Kurmitola General Hospital, Dhaka
Introduction: Lung cancer develops from pulmonary parenchymal or bronchial supportive tissues. It
is the most common and deadly tumor worldwide and approximately 1.3 million patients a year die of
it (Cancer statistics 2011).According to ―GLOBOCAN – 2008‖ lung cancer is the leading cause of
cancer and 19529 patients were diagnosed as lung cancer (13%) in the year 2008 in Bangladesh. The
Hospital-based ―Cancer Registry Report 2005-07of National Institute of Cancer Research and
Hospital‖ published in December 2009 indicates that lung cancer is the leading cancer and a total
number of 3209 (Cancer Registry Report 2007) lung cancer patients attended NICRH during the last
three years(2005-2007), Most of the lung cancers are Non-Small Cell Lung Cancer(NSCLC) that
accounts for approximately 85% of all lung cancers.
Materials &Method: The prospective observational study was carried out among 60 unresectable
NSCLC patients attending at NICRH and DMCH from July 2012 to June 2013.The study was
designed to observe: i) the radiological response of 50Gy RT and 50 Gy CCRT(Cisplatin 30 mg/m2
weekly) to assess the local control as a strong predictor of overall survival , ii) To compare the
effectiveness of RT alone (50Gy) versus CCRT in NSCLC, iii) To compare the morbidity of RT
alone and CCRT in NSCLC. The patients were from 35 to 72 years age range where 95.2% patients
were male, 91.9 % were smoker and 88.7% oral tobacco user. About 78.3 % patients were suffering
from squamous cell carcinoma and 21.7% adenocarcinoma. Regarding grading, 8.3% well
differentiated, 71.7% moderately differentiated, 20% poorly differentiated based on
histopathologicaly data. Complete response was 16.7%% in CCRT arm while in the 50Gy RT alone
arm it was only 9%. Partial response was 56.6% and 43.3% respectively. No response was seen in 13
patients, 5 in CCRT arm and 8 in RT alone arm. Only 10%patients in the CCRT arm and 20%patients
in RT alone arm was reported with progressive disease. No statistical significance was found
regarding the radiological response between these two arms (P 0.512). No significant difference was
found in mean size at day 0 (P 0.75), day 45 (P 0.41 and day 180 (P 0.43) between these two arms.
Treatment related morbidity was observed in the CCRT arm with 53.3% Grade ≥3 Pneumonitis
(p<0.001), 56.7% Grade ≥3 Leucocytopenia (p<0.001), 53.3% Grade ≥3 Neutropenia (p<0.001) and
6.7% Grade ≥3 anemia (p<0.001). Regarding metastasis, 10 patients in CCRT arm and 12 patients in
RT alone arm had presented with metastasis at different sites within this period. No statistically
significance was found between these two groups (P 0 .792). Death during follow up was observed in
34.7% patients in CCRT arm and 36.4 % patients in RT arm; this difference was not statistically
significant (P 0 .851).
Results & Conclusion: 50Gy Radiotherapy concurrently with weekly Cisplatin results in improved
the treatment response but does increased toxicities compared with the 50Gy Radiotherapy alone in
unresectable Non-Small Cell Lung Cancer. In this study CCRT gives better result than RT alone in
unresectable NSCLC with more toxicities in acceptable range. If we can use this protocol for
palliation and better quality of life of the patient it will be easier to give treatment in unresectable
NSCLC within a short time in the context of developing countries like Bangladesh.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
66
RT-13: Stereotactic Body Radiation Therapy (SBRT)- Advancement of
Radiation Oncology – a review
Kazi Manzur Kader
Department of Radiation Oncology, National Institute of cancer research and Hospital, Mohakhali,
Dhaka
Abstract: Approximately 60% of all cancer patients received Radiation therapy each year as definite,
palliative, or adjuvant to surgery or Chemotherapy. Management of the patient with cancer is complex
& requires close integration of basic concept & sophisticated technology to evaluate the stage of the
tumor & by using various modalities to obtain the therapeutic results.
Official figure indicates that in Bangladesh about 12 lacs people suffers from various types of cancer
is any point of time. Newly diagnosed cancer patients in each year is about 0.2 million & long then
0.15 million are dying.
Stereotactic body radiation therapy (SBRT) refers to an emerging radiotherapy procedure that is
highly effective in controlling early stage primary & oligometastatic cancer at locations throught the
abdomino pelvic and thoracic cavities, and at spinal and para spinal sites. The major feature that
separates SBRT from conventional Radiation treatment is the delivery of larger doses in a few
fractions, which results in a high Biological Effective Dose(BED). In order to minimize the normal
tissue toxicity, conformation of high doses to the target and rapid fall – off doses away from the target
is critical. The Practice of SBRT therefore requires a high level of confidence in the accuracy of the
entire treatment delivery process. In SBRT, confidence in this accuracy is accomplished by the
integration of modern imaging, simulation, treatment planning, and delivery technologies into all
phases of the treatment process; from treatment simulation and planning, and continuing throughout
beam delivery.
In addition to this major features, there are other characteristics that distinguish SBRT from
conventional radiation therapy. These include a general increase in the number of beams used for
treatment, the frequency use of non-coplanar beam arrangements, small or no beam margins for
penumbra, and the use of in homogeneous dose distribution and dose painting techniques(including
IMRT). All of these technology improvements result in the highly conformal dose distribution that
characterizes the SBRT technique.
Over 4000 publications spanning several decades have affirmed the clinical usefulness of stereotactic
radiosurgery (SRS) in the treatment of benign and malignant lesions, as well as functional disorders .
The radiobiological rationale for SBRT in similar to that for SRS; delivering a few fractions of large
dose in relatively short overall treatment time results in a more potent biological effect. The clinical
outcomes of SBRT for both primary and metastatic disease compare favourably to surgery with
minimal adverse effect. In addition , the limited number of treatment fractions makes SBRT more
convenient or the patient, and a potentially more cost- effective treatment modality than traditional
radiation therapy.
The majority of the patients treated with SBRT are those with lung, liver, and spinal tumors. Most
investigations limit eligibility to well-circumscribed tumors with maximum cross-sectional diameter
of up to 5cm, although some centers have reported results for tumors as large as 7cm. The use of
SBRT as a boost in addition to regional nodal irradiation has been proposed. Even with the
expectation that small volumes of adjacent organs at risk(OARs) will be irradiated during SBRT , an
assessment of patient eligibility should include a careful evaluation of normal tissue function and dose
distribution. Typically , pulmonary function and the volume of normal liver that is irradiated are the
most immediate considerations. Tumors proximal to mainstem bronchi, trachea, esophagus, gastric
wall, bowel, blood vessels, or spinal cord should be approached with great caution, or not at all, if the
lack of spatial separation places them within the high-dose gradient region of treatment, which can
lead to potentially devastating clinical outcomes.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
67
RT-14: Planning experience of radiosurgery using a LINAC in Guatemala
city
Hernández, E1. Contreras, R.
1 Ortega, M.
2 Ureta, L.
2
1Physics Department, Faculty of Engineering, San Carlos University from Guatemala
2Clinica de Radioterapia La Asunción, Guatemala
Introduction: The Clinica de radioterapia La Asuncion (Radiotherapy clinic La Asuncion) was the
first clinic in Guatemala, to provide radiosurgery services since 2007, and among the diseases that
were treated, arteriovenous malformations is the most frequent. The radiosurgery treatment planning
is carried out with the MNPS system of Mevis, treatment is administered with a linear accelerator
Clinac 1800 and Clinac 6EX using beams of 6 MV X-ray and cone system. The criteria used in
deciding the treatment plan are: Jackie Wessels conformity index, Ian Paddick conformity index,
integral dose, dose volume histogram and volume coverage. This paper shows the results of
experience gained since the treatments were initiated in 2007, until 2014 (94 cases), focusing on study
arteriovenous malformations, as the lesion most frequent.
Materials and methods: In this paper, we present the experience with 94 cases of radiosurgery with a
linear accelerator of Varian Clinac 1800 and recently (last 15 cases) with a Varian 6EX. System of
cones to collimate was adapted to the accelerator; the diameters of the cones used is 30 mm, 27 mm,
24 mm, 21 mm, 18 mm. 15 mm, 12 mm and 9 mm at isocenter. Photons of 6 MV was used in every
case. The TPS used is MNPS developed by Mevis and a stereotaxic system used to fix the patient
made by FiMe. In every patient treated initially was studied his case by the radiation oncologist and
neurosurgeon, who decided the treatment to administer, dose, and risk organs. The stereotaxic frame
is placed to the patient by radiation oncologist used local anesthesia. After placed the frame, a CT
image is acquired, with the frame how reference system. The CT image is processed with the MNPS
treatment planning system; this is a special TPS used to planning the radiosurgery cases. The MNPS
brings the information of Jackie Wessels conformity index, Ian Paddick conformity index, integral
dose, dose volume histogram and volume coverage, used to choose the acceptance of the plan. The
patient is fixed to the couch with a special system; the MNPS brings the coordinates of every
isocenter to place the target in position of treatment. A support of cones is attached to the collimator
exit used to the isocenter corresponding. The treatment is administered using the control console of
the Linac. When the treatment is finished, the frame is retired of the patient.
Results: Graphics of Integral dose versus target volume for arteriovenous malformations (AVM) is
presented, Jackie Wessels Index versus target volume, frequency of isocenters used, Ian Paddick
index versus target volume, age frequency of the patients treated, and frequency of target volume is
presented.
Conclusion: Arteriovenous malformations, was the lesion most frequent treated (53%). The volume
more frequently treated is menor to 5 cc. A relation of integral dose and target volume for the AMVs
treated was obtained with 0.9837 of correlation

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
68
Invited Talk
IPM-7: Treatment Plan Evaluation and Optimization Based on
Radiobiologic Parameters
Salahuddin Ahmad, Ph.D., DABR, FACMP, FAAPM
Professor and Director of Medical Physics
Department of Radiation Oncology
University of Oklahoma Health Sciences Center
Oklahoma City, USA
Abstract: Treatment plan optimization using radiobiological parameters is an improvement to
optimization based on physical dose constraints evaluated on the basis of dose volume histograms.
Such optimization enables the comparison of treatment plans based on the estimation of the
equivalent uniform dose (EUD), Tumor Control Probability (TCP) which provides a quantitative
biophysical measure of tumor dose, Normal Tissue Complication Probability (NTCP) which provides
the percentage of the patient population with unfavorable reactions in the contiguous tissue at a
particular dose, Therapeutic Index or Ratio (TI or TR) referring to the ratio of the TCP and NTCP at a
specific level of response for normal tissues, Uncomplicated Tumor Control Probability (UTCP)
referring to the probability of tumor control without complications, and the Therapeutic Gain (TG)
referring to the ratio of relative biological effectiveness in tumor to normal tissue. However, lack of
accurate knowledge of spatial distributions of clonogenic cells within the tumor, the tumor
radiosensitivity and the variability in cell surviving fractions are factors that impede accurate
radiobiologic estimations. The biological estimation along with the spatial information of tumor and
normal tissue cells are expected to generate the novel technique of biologically optimized image
guided radiation therapy.
Invited Talk
IPM-8: Challenges of Patient Safety in Radiation Oncology Practices In
Bangladesh
Prof Syed Md Akram Hussain,
Senior Consultant,Ahsania Mission Cancer Hospital
Introduction: Radiotherapy plays a major role for cancer management, particularly in the Indian
sub- continent. In Bangladesh, around eighty percent patients require radiation therapy. Radiation
treatment is teamwork. Quality care could only ensure patients' safety. It is highly important for
high dose rate treatment such as CFRT, IMRT, IGRT, SRT, and SBRT. Patient safety in
radiotherapy is a critical and challenging issue worldwide. National agencies and international
organizations such as IAEA, IOMP, and WHO are involved with this matter.
Methodology: Review of national and international relevant documents.
Result and Discussion: Quality control has utmost importance for ensuring patient's safety. Error may
occur in different steps and stages of human and technical interactions. Quality assurance requires
appropriate skill, education, qualification, and training of radiation medical physicists following
international guidelines and framework. Over the last three decades, at least 3,000 patients have been
affected by radiotherapy incidents and accidents, which have been accounted for more acute radiation
deaths than any other source, including Chernobyl.
Quality assurance activities could ensure patient's safety. Radiation Oncologists, Clinical Radiation
Medical Physicists, and Dosimetrists are responsible for technical quality assurance of radiation
treatment. International Labour Organization (ILO) has recognized medical physicist as an
occupation; and OMP, IAEA, and AAPM have defined who will be a medical physicist and what will
be their role and responsibilities. The Fundamental Safety Principles issued by IAEA is, "The
fundamental safety objective is to protect people and the environment from harmful effects of
ionizing radiation" which is stated in IAEA Basic Safety Standards ( BSS).

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
69
In Bangladesh, advanced radiotherapy technologies have both in government and privet sectors.
So, patient safety issue becomes more crucial. Bangladesh Atomic Energy Regulatory Authority
(BAERA) is responsible for enforcing rules and regulations for radiation safety in Bangladesh. Safety
is everyone's responsibility.
Conclusion: To achieve adequate patient safety, internationally standard certification and a legal
framework such as licensing would be pertinent by the competent authority in Bangladesh.
Invited Talk
IPM-10: New methods in peripheral Nerve conduction measurement from
Dhaka University
K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Bangladesh Email: [email protected]
Abstract: Distribution of F-Latency (DFL) is a new nerve conduction parameter conceived by the author
and developed by his team at Dhaka University. Work has been going on since 2002 on DFL and it appears
to be a very useful technique in the screening or diagnosis of peripheral neuropathy. Already research
groups in Singapore and UK have started working on DFL. It is expected that this measurement parameter
will become a first line testing method in peripheral neuropathy in the near future.
Invited Talk
IPM-11: Accreditation, Certification and Recognition Issues
John Damilakis
Professor of Medical Physics
Faculty of Medicine, University of Crete, Greece E-mail: [email protected].
Abstract: An increasing number of higher education institutions have in recent years started to offer
courses on Medical Physics. Moreover, Continuing Professional Development (CPD) for medical
physicists is of great professional interest. CPD courses is an excellent way to ensure that Medical
Physicists become knowledgeable about all current issues in their field and to provide the necessary
knowledge, skills and competences for certified Medical Physicists to become Medical Physics
Experts. However, external assessment of the quality of education or training provision is needed.
Accreditation is the formal recognition that education and training on medical physics provided by an
institution meets acceptable levels of quality. Accreditation should be based upon standards and
guidelines. Requirements for accreditation of a training programme should take into account several
aspects including facilities, staff, educational material and teaching methods. In Europe, ENQA
(European Network for Quality Assurance) promotes European co-operation in the field of Quality
Assurance in higher education. ENQA members are national agencies and organizations, which play a
major role in the accreditation process. A European organization is needed to offer accreditation of
medical physics CPD and training programs. Certification is the recognition of knowledge of a
professional who has completed his/her education or training. The EC has developed tools and
frameworks to promote training and facilitate mobility. ECVET is a European system of accumulation
and transfer of credits designed for vocational education and training in Europe.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
70
Invited Talk
IPM-12: Clinical Training of Medical Physicists and Accreditation: Efforts
in Bangladesh
Kamila Afroj Quadir
National Institute of Nuclear Medicine & Allied Science, BAEC, Block D, BSM Medical University,
Dhaka, Bangladesh E-mail: [email protected].
Introduction: Medical physicists are fundamental to any radiation medicine discipline. With the
development and sophistication of radiation medicines in both diagnosis and therapy, the role of
medical physicist is increasingly becoming ever more important. In hospitals with radiation medicine
services either for diagnosis or therapy, physicists play an important role for the optimization of
image and dose, radiation safety, instrumentation, quality control and quality assurance. As actions of
medical physicists working in the hospitals directly impact human life, therefore, it is very important
that they are clinically competent.
Clinical training efforts in Bangladesh: Clinical guide books TCS series 371, 47
2 and 50
3 published
by IAEA, are of international standard for structured clinical training in radiation oncology, diagnostic
radiology and nuclear medicine training respectively. Bangladesh, for the first time, completed a 2
years structured in-service clinical training program for nuclear medicine physicists with the support
of IAEA following guide book TCS-503 in 2012. This was carried out by the National Institute of
Nuclear Medicine and Allied Sciences (NINMAS) of the Bangladesh Atomic Energy Commission.
Physicists who qualified in the clinical training program were evaluated by IAEA expert by written,
practical and oral examination. Later these Physicists were given certification by the Bangladesh
Medical Physics Association (BMPA) after they successfully passed an examination taken by
BMPA.
Initiative for Accreditation: The Department of Biomedical Physics and Technology of Dhaka
University and Bangladesh Medical Physics Association took an initiative for a round table meeting
in the beginning of this year on Accreditation and Certification issues in the field of Medical Physics
and Biomedical Engineering, both for relevant courses and for clinical residency programmes. The
meeting resolved that an independent Board should be created under the leadership of University of
Dhaka with membership from individual specialists, relevant associations, Government and non-
Government organisations. Later, arguments came that since the University gives a course, there may
be a conflict of interest and an independent body or institute be formed to provide such Accreditation.
For this purpose a suggestion for an ‗Institute of Medical Physics and Biomedical Engineering‘, to be
registered as a social organization came through a couple of meetings held later. Efforts should then
be taken to have the Government endorse the accreditation given by this Institute. Further steps in this
direction are being awaited.
Conclusion: If the suggested Institute is formed it will fill up a great void that exists today in
Bangladesh in the quality assurance of clinically qualified Medical Physicists and Biomedical
Engineering.
References 1. Clinical Training of Medical Physicists Specializing in Radiation Oncology; Training Course Series
(TCS) 37, IAEA, Vienna, 2009.
2. Clinical Training of Medical Physicists Specializing in Diagnostic Radiology; Training Course
Series (TCS) 47, IAEA, Vienna, 2010.
3. Clinical Training of Medical Physicists Specializing in Nuclear Medicine; Training Course Series
(TCS) 50, IAEA, Vienna, 2011.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
71
AIM-1: Study of the Broca Region of Brain to Analyze Autism
Mousumi Bala, Mohammad Hanif Ali
Department of Computer Science and Engineering, Jahangirnagar University, Savar, Dhaka,
Bangladesh. E-mail: [email protected], [email protected].
Introduction: Autism is of great concern in the present world. It is a neuro-developmental disorder
that occurs in the early age of a child. Autism is characterized by impairment of verbal and nonverbal
communication, social interaction, and imagination, whose origin is largely unknown. Recent studies
show abnormalities in the various regions of brain in autistic persons. To investigate the causes of
autism, the study of Broca region of brain is carried out among the control and autistic individuals. In
carrying out the work, advanced diffusion-weighted magnetic resonance imaging (MRI) is performed
on control and autistic individuals. Using a validated automatic method, white matter in Broca region
are identified and micro-structural characteristics including fractional anisotropy (FA) and mean
diffusivity (MD) are examined. Broca‘s area is a region of the hominid brain with functions linked to
speech production. Functional MRI (fMRI) studies have identified activation patterns in Broca‘s area
associated with various language tasks. Functions of Broca‘s area i) Language comprehension ii)
Action recognition and production ii) Speech-associated gestures. Furthermore, the degree of
synchronization between the various participating areas was consistently lower for the autistic than
the control participants. So, Autistic patients do not integrate and synchronize information as
effectively as healthy controls during language processing.
Materials and Methods: In carrying out the work, the broca region is divided into anterior, long and
posterior segment. Using validated automatic selection method, fractional anisotropy (FA) and mean
diffusivity (MD) are calculated for the control and autistic individuals. The MRI scan image is taken
as input and the experiment is implemented in MATLAB 7.12.0.635.
Figure: shows the FA for control and autistic
Results: Fractional Anisotropy (FA) and Mean Diffusivity (MD) in the anterior segment, long
segment and posterior segment in the broca region for control and autistic individuals have been
calculated using validated automatic method. From the study it is clearly observed that autistic
individuals have a lower FA and greater MD than controls in the Broca region.
Conclusion: From the experiment it is very much clear that FA in control and autistic are different.
The cause of these differences needs to be investigated in details which demands further study.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
72
AIM-2: Need Assessment of Tele-Palpation
Zubair Barkat and K Siddique-e Rabbani,
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh. E-mail: [email protected], [email protected].
Introduction: Because of the geographical maldistribution of healthcare resources due to a great
disparity in economy, about two thirds of the world‘s population, mostly living in the least developed
countries (LDCs), lacks adequate access to quality health care. Telemedicine appears to be a solution
where the doctor is situated at a distance from the patient and two way audio-visual communication
together with real time diagnostic support using appropriate digital equipment is provided. A
significant part of a primary medical examination is ‗Palpation‘ in which a doctor touches and presses
onto different anatomical sites for diagnosis, for which no equivalent solution has come up so far for
telemedicine. The challenge of the present work is to give the remote doctor an experience of virtual
palpation in real time through development of appropriate hardware and software technologies. In this
article, we present study results of need assessment of tele-palpation for remote healthcare. The study
has been conducted on ten practicing doctors including professors from various medical units like
Cardiology, surgery, pediatrics.
Methods: The participants were first introduced with the project information. Then, they were asked
to fill up the questionnaire containing ten different questions covering different tele-palpation issues.
Results and Observations: Given in the figure a series of comparative graphs were drawn, combined
and opinions of specific medical units are presented. All of them agreed on usefulness of palpation in
clinical diagnosis and examinations. Different kind of tumor appears to show highest importance in
terms of diseases relevant for Bangladesh and LDCs that can be identified using palpation.
Pneumonia, malaria diarrheas, appendicitis, pancreatitis, breast lump tuberculosis, thalassemia are
among the diseases that are among the priorities identified by the doctors. In terms of skill in
palapation measurement Training of remote technicians got highest priority among all medical units.
Conclusions: Despite the challenges this project gives hope of better future and worth developing.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
73
AIM-3: Findings from Two Urban Field Trials of the Dhaka University
Solar Water Pasteurizer
Rezwan Hussain1, M Abu Yousuf
2 and K Siddique-e Rabbani
2
1 University of Liberal Arts, Dhaka, Bangladesh
2 Dept of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh
E-mail: [email protected], [email protected], [email protected]
Introduction: The academic literature indicates that uptake or adoption of point-of-use health
interventions, even when they offer measurable health benefits, tends to be poor. Chlorination and SODIS
bottles [1] are two such interventions that have fared poorly, whether due to burden of use or other reasons.
Accordingly, two recent field trials of an affordable, portable solar water pasteurizer, developed by the
Department of Biomedical Physics and Technology at Dhaka University [2], sought to answer two
questions: (i) will impoverished, resource-poor urban households use the device with any regularity, and
(ii) will it offer health benefits to those most at risk from unsafe drinking water i.e. young children?
Methods: To answer these two questions, two field trials were conducted, in September, 2014, and
December 2014, in two Dhaka slums, located in Rayer Bazar. Each trial lasted three weeks, and ten
households, located within the same community, were selected to participate in each trial. There were three
selection criteria: the monthly rent not to exceed Tk.1500, no gas supply to the household, and the
household water supply to be contaminated with E-coli bacteria, as confirmed by lab tests.
Each household was supplied with one device, and training in its use. A baseline survey was conducted,
followed by weekly surveys for the three-week duration of each trial. One survey measured frequency of
use of pasteurizer, and gathered feedback from trial participants; the other survey gathered data on child
health outcomes. The picture shows the devices in actual use.
Results and Discussion: Both trials indicate significant uptake
and adoption by the pilot households, with approximately 90%
of households in both trials reporting regular usage during the
trial period. This may be partly due to due to site selection,
given the significant E-coli contamination of the drinking water
at both locations. Nevertheless, the rates of adoption indicate
that the device is effective and usable in the field.
Most importantly, both trials suggest that child health outcomes
were affected in a positive manner. In the first trial, the rate of
incidence (RI) of diarrhea or watery stool among children five
or under fell from 19 cases at baseline to 10 cases at trial end. In the second trial, the RI of diarrhea or
watery stool fell from 3 cases at baseline, to 0 cases at trial end. While findings for the second trial are less
conclusive, the first trial, conducted during the warmer month of September, when water quality is
typically worse, suggests that the pasteurizer may significantly reduce rates of diarrhea and water stool
among young children living in urban poverty.
Conclusion: The two field trials of the Dhaka University solar water pasteurizer offered proof of concept,
and demonstrated significant potential for uptake and adoption by poor, urban slum households with access
to only poor quality drinking water. The trials also suggest that pasteurizer use can significantly benefit
health outcomes in children five and under, who tend to be most at risk from poor quality drinking water.
These findings suggest that a larger study studying the impact and efficacy of the solar water pasteurizer is
warranted.
References: 1. http://www.sodis.ch/index as on 31 Jan 2015
2. MA Yousuf, RB Hussain and KS Rabbani, Solar Water Pasteurizer and Rain Water Collector for provision
of safe drinking water in urban slums and rural areas, Abstracts, International Conference on Physics in
Medicine and Clinical Neuroelectrophysiology (PMCN2015), Dhaka, Feb 19-20, 2015.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
74
AIM-4: A double blind trial to establish Distribution of F-Latency (DFL) as
an indicator of Cervical Radiculopathy or Myelopathy
Ehsan Alam Chowdhury and K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh E-mail: [email protected], [email protected].
Introduction: The research group now at the Department of Biomedical Physics & Technology of the
University of Dhaka developed a new nerve conduction technique more than a decade back given the
name of ‗Distribution of F-Latency (DFL)‘ and had found that it could be useful for identification of
peripheral Neuropathy due to compression of nerve roots (Radiculopathy) or compression of the
spinal cord (Myelopathy) at the cervical and lumbo-sacral regions [1,2]. The aim of the present work
was to study the effectiveness of DFL for diagnosis or screening of cervical Radiculopathy or
Myelopathy (CRM). In the diagnosis of CRM, MRI is the standard investigation carried out. So we
decided to do carry out a double blind trial of DFL where MRI would be taken as the gold standard.
Methods: The investigation was performed on median nerves of both hands of 31 informed
volunteers chosen randomly between the ages 20 and 64. So that made it 62 cases to study. It was
noted whether the patient had any history of cervical pain or prior diagnosis of cervical radiculopathy
or myelopathy. The Radiologist conducting MRI was not informed of the DFL findings. Also the
investigator assessing the DFLs was unaware of the MRI results. This was done to keep the trial
double blind and minimize bias. The identification of patterns of DFL went through some refinements
through a work done in Singapore earlier [3] and the present work used these refinements.
Results: Row 2 of the Table below shows the results of the study on all 62 nerves (cases here) of the
31 subjects, while Row 3 is for age group < 50yrs (no. of cases: 44) and Row 3 for >50 yrs (no. of
cases: 18). Age
group
No. of
nerves
(cases)
TP TN FP FN Correctly
Predicted % Wrongly
Predicted % Sensitivity
% Specificity
%
20-64 62 45 2 2 13 76 24 78 50
20-50 44 29 2 2 11 70 30 73 50
50-64 18 16 0 0 2 89 11 89 *
TP: True positive, TN: True negative, FP: False positive, FN: False negative
Sensitivity = True positives/All positives; Specificity = True negatives/ All negatives
* Number of TN cases was zero, so specificity could not be calculated
Discussion: The results show that DFL gives a reasonably good indication of CRM. In fact it was
found that even in cases where the effect was almost subclinical and MRI only reported mild
compressions that normally would be ignored by doctors, DFL showed the abnormality clearly.
Therefore, DFL can be used as a first line screening test for identification of CRM, giving a cost
effective solution. MRI, a very expensive and bulky machine, is not widely available and has a very
high consumable cost, making DFL attractive for screening patients for CRM since DFL requires
standard nerve conduction equipment that can be made into a portable unit at low cost and has almost
zero consumable cost.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support. References: [1] Rabbani KS et al: Frequency Distribution of F-Latencies (DFL) has Physiological Significance and Gives
Distribution of Conduction Velocity (DCV) of Motor Nerve Fibres With Implications for DIagnosis. J Biol
Phys 2007, 33:291-303.
[2] Alam MJ and Rabbani KS: Possible detection of cervical spondylotic neuropathy using Distribution of F-
latency (DFL), a new neurophysilogical parameter. BMC Research Notes 2010, 3(112).
[3] KS Rabbani, N Yassin and Y L Lo, Identification of Cervical Spondylotic Radiculo-Myelopathy using
Distribution of F-Latency (DFL), a new nerve conduction parameter, Submitted, BMC Research Notes.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
75
AIM-5: Distribution of F-Latency and MRI Study of the Brachial Plexus
Z B Mahbub1, P A Gowland
2
1Department of Arts & Sciences, Ahsanullah University of Science & Technology, Bangladesh
2School of Physics & Astronomy, University of Nottingham, United Kingdom
Introduction: Brachial plexus imaging by MRI can efficiently detect disorders and study the
microstructures qualitatively and quantitatively. EMG can detect the peripheral neuropathies using
time dependent behaviour of nerve conduction. Thus the combination of EMG and MRI could provide
important insight and information about the brachial plexus1. The objective of this work is to measure
the distribution of F-response latencies (DFL) as a new parameter2 in EMG and combine it with MRI
at different head positions of the normal subjects.
Figure 1: MRI of brachial plexus using STIR TSE sequence
Methods: This study was approved by the local ethics committee. MR images of the brachial plexus
were acquired from six healthy subjects on a 3T Philips Achieva scanner using the torso XL 16
channel array coil. Short tau inversion recovery turbo spin echo (STIR TSE) sequence was
implemented for acquiring MR images. Sizes of the DRG, Rami and trunks were calculated from the
intensity profiles fitted with Gaussian curves. DFLs were measured from the same subjects based on
the F-responses by stimulating the median nerve at the wrist using surface electrodes stimulator with
12mA, 220V and 500µs pulses. Elicited F-responses were recorded with sampling rate 5kHz,
resolution 0.5μV, and low/high cut-off=10/1000Hz from the abductor pollicis brevis (APB) muscle
using the BrainAmp amplifier and Brain Vision Recorder software, Brain products, Germany. Nerves
were supramaximally stimulated for 30 times, the DFLs were calculated between 20ms to 40ms F-
latencies with 2ms bin size, and then fitted to Gaussian function to find corresponding peak (DFLpeak).
To observe the effects the different head positions, all the MRI and F-responses were measured at
normal position of the head and tipped to left and right for compressed and extended positions. Page‘s
L trend tests3 were used to assess the effects of head positioning on the DFLpeak and MRI parameters
for individual measurements, and then correlation between averaged DFL and MRI measurements
calculated.
Results: Table1 shows the Page‘s L trend test values for DFL and MRI measurements. Figure 2
shows the correlation between DFLpeak and MRI parameters. Table 2 shows the coefficients.
Figure 2: Correlation between DFL peak and MRI measurements from brachial plexus
Discussion: Combined DFL and MRI measurements was carried out successfully for the first time.
Clear decreasing trend for DFLpeak, DRG_C7 and trunks were observed for compressed-normal-
extended positions of the head. Strong correlation between DFLpeak, Rami and DFLpeak, lower trunk
were detected, that could relate the eliciting nerve roots and conduction path of the F-responses. Thus
the combination of two complimentary techniques MRI and DFL can provide a great clinical
applications in quantitative and qualitative peripheral neurophysiology.
Table 1 Table 2
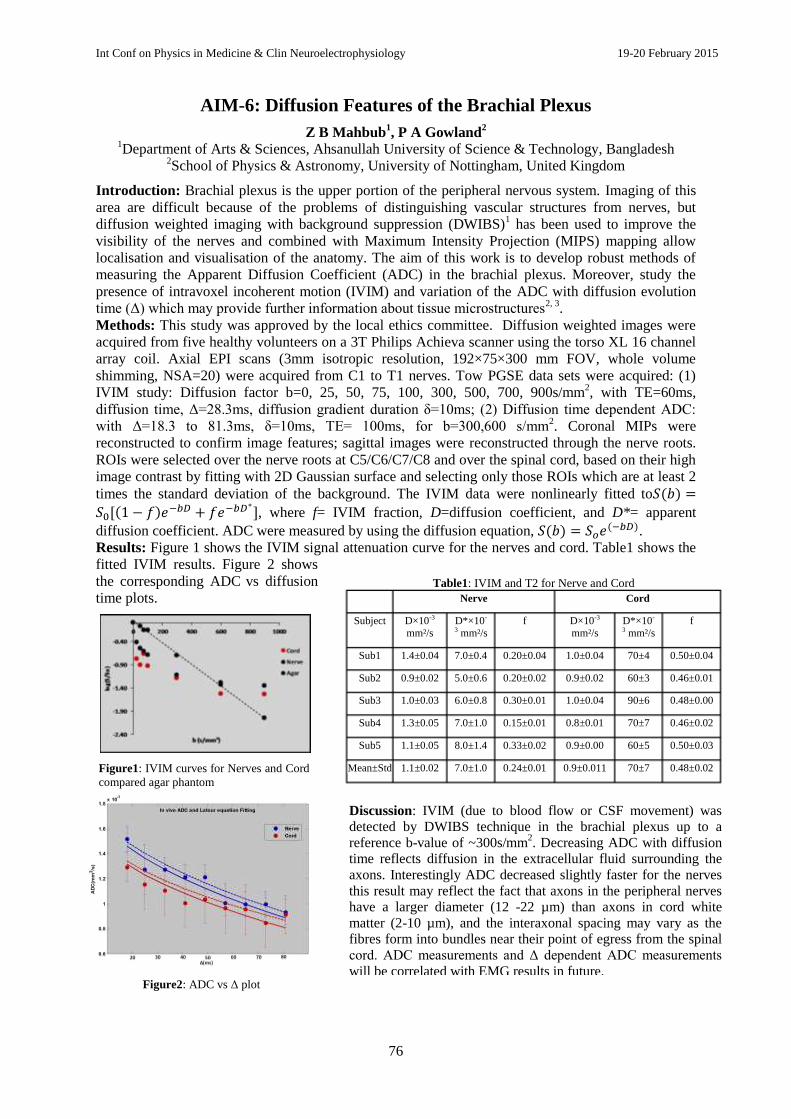
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
76
AIM-6: Diffusion Features of the Brachial Plexus
Z B Mahbub1, P A Gowland
2
1Department of Arts & Sciences, Ahsanullah University of Science & Technology, Bangladesh
2School of Physics & Astronomy, University of Nottingham, United Kingdom
Introduction: Brachial plexus is the upper portion of the peripheral nervous system. Imaging of this
area are difficult because of the problems of distinguishing vascular structures from nerves, but
diffusion weighted imaging with background suppression (DWIBS)1 has been used to improve the
visibility of the nerves and combined with Maximum Intensity Projection (MIPS) mapping allow
localisation and visualisation of the anatomy. The aim of this work is to develop robust methods of
measuring the Apparent Diffusion Coefficient (ADC) in the brachial plexus. Moreover, study the
presence of intravoxel incoherent motion (IVIM) and variation of the ADC with diffusion evolution
time (Δ) which may provide further information about tissue microstructures2, 3
.
Methods: This study was approved by the local ethics committee. Diffusion weighted images were
acquired from five healthy volunteers on a 3T Philips Achieva scanner using the torso XL 16 channel
array coil. Axial EPI scans (3mm isotropic resolution, 192×75×300 mm FOV, whole volume
shimming, NSA=20) were acquired from C1 to T1 nerves. Tow PGSE data sets were acquired: (1)
IVIM study: Diffusion factor b=0, 25, 50, 75, 100, 300, 500, 700, 900s/mm2, with TE=60ms,
diffusion time, Δ=28.3ms, diffusion gradient duration δ=10ms; (2) Diffusion time dependent ADC:
with Δ=18.3 to 81.3ms, δ=10ms, TE= 100ms, for b=300,600 s/mm2. Coronal MIPs were
reconstructed to confirm image features; sagittal images were reconstructed through the nerve roots.
ROIs were selected over the nerve roots at C5/C6/C7/C8 and over the spinal cord, based on their high
image contrast by fitting with 2D Gaussian surface and selecting only those ROIs which are at least 2
times the standard deviation of the background. The IVIM data were nonlinearly fitted to
, where f= IVIM fraction, D=diffusion coefficient, and D*= apparent
diffusion coefficient. ADC were measured by using the diffusion equation, .
Results: Figure 1 shows the IVIM signal attenuation curve for the nerves and cord. Table1 shows the
fitted IVIM results. Figure 2 shows
the corresponding ADC vs diffusion
time plots.
Figure1: IVIM curves for Nerves and Cord
compared agar phantom
Table1: IVIM and T2 for Nerve and Cord
Nerve Cord
Subject D×10-3
mm²/s
D*×10-
3 mm²/s
f D×10-3
mm²/s
D*×10-
3 mm²/s
f
Sub1 1.4±0.04 7.0±0.4 0.20±0.04 1.0±0.04 70±4 0.50±0.04
Sub2 0.9±0.02 5.0±0.6 0.20±0.02 0.9±0.02 60±3 0.46±0.01
Sub3 1.0±0.03 6.0±0.8 0.30±0.01 1.0±0.04 90±6 0.48±0.00
Sub4 1.3±0.05 7.0±1.0 0.15±0.01 0.8±0.01 70±7 0.46±0.02
Sub5 1.1±0.05 8.0±1.4 0.33±0.02 0.9±0.00 60±5 0.50±0.03
Mean±Std 1.1±0.02 7.0±1.0 0.24±0.01 0.9±0.011 70±7 0.48±0.02
Figure2: ADC vs Δ plot
Discussion: IVIM (due to blood flow or CSF movement) was
detected by DWIBS technique in the brachial plexus up to a
reference b-value of ~300s/mm2. Decreasing ADC with diffusion
time reflects diffusion in the extracellular fluid surrounding the
axons. Interestingly ADC decreased slightly faster for the nerves
this result may reflect the fact that axons in the peripheral nerves
have a larger diameter (12 -22 µm) than axons in cord white
matter (2-10 µm), and the interaxonal spacing may vary as the
fibres form into bundles near their point of egress from the spinal
cord. ADC measurements and Δ dependent ADC measurements
will be correlated with EMG results in future.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
77
AIM-7: Investigation of Different F-response Parameters at Different
Positions of the Head
Z B Mahbub, M H R Khan, M S A Khan, M K Sarkar, M M Billah
Department of Arts & Sciences, Ahsanullah University of Science & Technology
Introduction: The F-responses results from the backfiring of antidromically activated anterior horn cells.
Thus its measurement helps in assessing motor conduction characteristics along the entire length of the
peripheral axons. The inherent variability of the latency and configuration of the F responses makes its use
as a technically demanding neurophysiological parameter1. Physically it is expected to observe distinctive
changes in latencies of motor responses with different positions of the head that can cause temporary
compression or extension over the brachial plexus nerve roots, such conditions could reflect similar
neurological disorders. Objective of this study is to estimate the variations of different F-response
parameters such as maximum and minimum latencies, chronodispersion and recently introduced
distribution of F-latency (DFL) 2, 3
at different head positions of the normal subject.
Methods: This study had local ethics committee approval. F-responses were recorded at room temperature
(~200C) from four healthy subjects (age limit 25-45 years) by stimulating the median nerve at the wrist
using surface electrodes (cathode proximal) attached to a constant current (~20mA), high voltage (220V)
stimulator. Elicited F-responses were recorded (sampling rate 5kHz, resolution 0.5μV, and low/high cut-
off=10/1000Hz) by placing the active/reference/ground electrodes over the abductor pollicis brevis (APB)
muscle, at the thumb, and at the back of the palm respectively using the Brain Amp amplifier and Brain Vision Recorder software, Brain products, Germany. Nerves were supramaximally stimulated for 30 times
at each of the normal, extended and compressed positions of the head and resulting F-responses were
recorded from which following parameters were calculated: minimum, maximum and mean F-latencies
(Fmin, Fmax, Fmean), chronodispersion, Fchrono = Fmax - Fmin, amplitude (FAmp) and DFL with 2ms bin size
from 20ms to 40ms. DFL were fitted to Gaussian function to find corresponding peak and width (DFLpeak ,
DFLwidth). To observe any trend with head positions in the above parameters Page‘s L trend test4 were
implemented.
Results: Figure 1 shows the measuring parameters from
different F-responses. The probability values from Page‘s
L trend test shown in Table 1.
Discussions: Different F-response parameters were measured at different head positions successfully.
For compressed-normal-extended positions of the head clear decreasing trends in DFLpeak, DFLwidth and
Fmin, adequate decreasing trends in FAmp and Fmean were observed. These observations reflect the temporary
compressions and extensions of the nerve roots at brachial plexus which in turn controls the F-latencies of
the fastest nerve fibres. However, the Fchrono, Fmax were not showing similar trend, may be due to
variability of number of participating backfiring neurons at spinal cord that reach the APB muscle later. F-
response measurements and different angular position dependent parameters will be correlated with EMG
results, cervical spondylotic patients in future.
Acknowledgement: Professor Penny Gowland, University of Nottingham, Professor K S Rabbani,
University of Dhaka for excellent ideas and supervision.
References: 1. D C. Preston, Electro. & Neuro. disorders, 2nd Ed. 2005;
2. M Fisher, F-waves phys. uses, The Sci. world 2007(7);
3. Rabbani et al, DFL physiol. parameter, J Biol. Physics 2007(33); 4.
Cuzick, J. Statistics in medicine 1985(4).
Figure 2: Different F-response
parameters shown in three responses
Table1: Page‘s L trend P-values for different parameters

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
78
LCD-1: Android Apps Based Intelligent Telemedicine System: Bangladesh
Perspective
Shekh Md Mahmudul Islam and Md Adnan Kiber Department of Electrical & Electronic Engineering, University of Dhaka, Dhaka.Bangladesh
E-mail: [email protected].
Introduction: Health is a fundamental human right although more than one billion people are
unreached in terms of quality healthcare services. Insufficient healthcare facilities and unavailability
of medical experts in rural areas are the two major reasons that kept the rural people unreached to
healthcare services in developing countries like Bangladesh. According to the World Health
Organization (WHO) statistics, the doctor to population ratio is 1: 1500 in urban areas and 1:15000 in
rural areas of Bangladesh. This scenario can be dramatically changed if we can simply convey
medical tips using ICT infrastructure to the targeted unreached community. Due to the recent
development of Information and Communication Technologies (ICT) the digital divide has been
reduced and these technologies have the great potential to address contemporary global health
problems. Telemedicine refers to the use of information and communication technologies to distribute
information and or expertise necessary for healthcare services provision, collaboration and or delivery
among geographically separated participants including physicians and patients.
Methods: DICOT (Digital Imaging and Communication for Telemedicine) is the name of the
machine which has been built by the Telemedicine Working Group (TWG) of Bangladesh, and is in
use at some telemedicine centers. One of the major problems of the DICOT users is long cumbersome
registration process. In this thesis work we have developed android apps which will provide
opportunity of health care at home. After logging in apps, user can update their basic medical records
and can choose and get a confirmation of appointment of specialist doctors. Different medical records
can be updated like body temperature, glucometer, ECG, personal information and others. After
updating with database then a confirmation message of assigned appointed day and time will be sent
to the patient through android app. So, patients need not experience a long cumbersome process of
registration.
Results and Observations: Some snapshots of our designed Android App for registration purposes
are given below:
Conclusion and Future Work: In our developed android app medical records like Blood Pressure,
Glucometer, and Temperature can be updated manually through smart phone as embedded sensor
devices are not available in our country, so automated android app with diagnosis device could be
implemented in our future work.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
79
LCD-2: Indigenous Development of Ultrasound Doppler Based Fetal Heart
Monitor
Md. Kamrul Hussain and K Siddique-e Rabbani
Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh Email: [email protected], [email protected]
Introduction: A foetal heart monitor gives general information on foetal development through
determination of its heart rate which can improve the scenario of neonatal and perinatal death besides
maternal mortality. Antenatal care in the rural areas of Bangladesh still needs a lot of improvement
through technology but foreign equipment are expensive and do not provide sustained service because
these are not designed to suit our weather conditions and extreme power line abnormalities. The goal
of this research work is to design and develop a Fetal Heart Monitor based on Ultrasound Doppler
technique indigenously as a solution to the above problem.
Methods: Two ultrasound Doppler sensors - a transmitter and a receiver - were fabricated using
piezoelectric transducers, available commercially. Backing layers for the mounting of the transducers
were designed to get high efficiency, and fabricated using locally available materials. Electronic
circuitry were developed to retrieve the movement of an object in the path of the ultrasound beam
which involved the following: i) excitation signal for the transmitter, ii) amplification of the weak
received signals, iii) appropriate filtering, iv) conditioning of the output, v) demodulation using a
PLL. To test the developed prototype a water phantom was designed with an object inside that moved
with time (Fig a). Pulsed wave unipolar drive technique was used with two separate transducers as
transmitter and receiver. The movement of the object inside the phantom simulated the contraction
and expansion of the baby‘s heart inside a fetus.
Results: The tests revealed that the outputs of the transducers and different stages of the circuitry
behaved as expected. The transducer has sharp excitation and the ringing is reduced significantly (Fig
b) showing success of the mounting method. The output was fairly stable and the demodulator was
capable of recovering the movement of the object inside the phantom (Fig c).
Discussions: It was a success to construct the transducers and the electronic circuitry for the
ultrasound Foetal Heart Monitor with limited resources locally. The overall system performance can
only be verified by experimenting on the human body. In that stage, the demodulator has to be tuned
precisely to capture the slightest change of Doppler frequency due to heart movement. Further
development work is required for experiments on human body. Once it is successful, further work will
be carried out to make the device portable and linking this device to telemedicine.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
(a) Transducer
(b) Received pulse signal: receiver o/p
(lower trace) and conditioned o/p (top
trace)
(c) Output due to a moving object (top
trace)and demodulated o/p (lower trace)
representing the movement of the object

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
80
LCD-3: Introduction to PC Based ECG Acquisition Technique without
Switched Resistor Network at Input
Zisun Ahmed, K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh. E-mail: [email protected]
Introduction: In the standardized ECG system ten electrodes are needed to produce 12 electrical
views of the heart. To obtain all 12 Lead signals it is required to have different combination of analog
signal switching for positive and negative input of the instrumentation amplifier. This switched
resistor network at the input is responsible for a number of inevitable problems such as- non-uniform
amplification of different leads due to resistance mismatch, degradation of CMRR due to unequal
impedance seen by the two inputs amplifier, lead reversal during switching, increased hardware bulk,
decreased reliability over time due to changes in resistance. Though it has been more than a century,
the basic principle of acquiring ECG signals from the body has remained almost the same.
Methods: As ECG is a very slow moving signal, it is fairly easy to sample the signal and transfer it to
a computer without losing any important information. If, somehow, we can associate a PC with the
ECG acquisition system in such a way that the computer will take signals from different portion of the
body with respect to a reference point and after some amplification, necessary filtering and
digitization, the PC can have enough samples to calculate different lead signals within its processing
unit. A multiplexer can be incorporated to switch between the signals coming from different position
of the body before comparing it to the reference point. That way the total resistive network switching
process can be avoided.
To investigate the feasibility of this alternate method of acquiring different ECG leads which will be
based on PC without needing any switched resistor network at input an experiment was set up and
was tested on a couple of subjects. Two different ECG amplifiers were constructed and signals from
different limbs associated with certain leads were sampled using multiplexers and filtered to
differentially amplify with respect to a reference using instrumentation amplifiers. The amplified
signal was filtered and then using opto-isolators transmitted to an oscilloscope. The outputs of both
the ECG amplifiers were then subtracted using the math function of the oscilloscope.
Results: After the successful conduction of the experiment, the results were acquired and analyzed.
The results showed very strong resemblance to the result from a conventional ECG, proving the
possibility of existence of an alternate method of acquiring ECG.
Figure 3(a): Lead I Figure 4(b): Lead II Figure 5(c): Lead III
Conclusions: If this method can be implied the hardware bulk of resistor switched network and the
limitations associated with it can be eliminated completely. As there is no resistor network needed the
system will be more reliable to use over time and it will require less maintenance. This method will
also make it easier for ECG to be calculated in personal devices, which can be helpful for providing
health care to the people of the under privileged countries.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
81
LCD-4: Alternative Solution of Manual Glob Top for Low Resource
Countries
Zubair Barkat
Institute for micro and sensor system (IMOS), Otto-von-Guericke university of Magdeburg, Germany.
*Currently working at Department of Biomedical Physics & Technology, University of Dhaka. E-mail: [email protected]
Introduction: Glob-top is a variant of conformal coating used in chip-on-board assembly
(COB).Manual glob top is always challenging especially for small diameter sensors. In This article we
have proposed a solution for manual glob top for differential pressure sensor. These sensors can be
used in different medical applications. This invention has the potential to solve manual glob top
challenges for low resource countries. Glob top is made of a drop of specially formulated epoxy or
resin deposited over a semiconductor chip and its wire bonds, to maintain mechanical support and
exclude contaminants such as fingerprint residues which could disrupt circuit operation. Looking into
the details of the failure of the experimental setup due to manual glob top application, excess adhesive
was observed in the top surface of the sensor. This adhesive comes from manual glob top using a
needle.
Methods: Given in the figure, the first step was to protect the pressure sensor from outside
contaminants and provide mechanical support, as we do not want to do the glob top on the sensor top
surface due to the risk of excess adhesive might come to the surface because of manual glob top. So,
we made a roof like structure using copper plate to protect the sensor. To maintain the balance of the
packaged sample a similar kind of supporting structure was made on the rightmost corner of the
packaged sample.
Results: The experimental setup for differential pressure sensor was tested later on and provides
accurate output voltage as suggested in the data sheet of First sensor (IL20M-40MP-G08).
Conclusions: This solution has the potential to solve the manual glob top challenges faced by low
resource countries and can be used for various medical applications.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
82
LCD-5: Decoding Movements from Human Subthalamic Local Field
Potentials Based on Neural Synchronization
S. Ahmmed1, F. Ahamed
1, M. Mace
2, R. Vaidyanathan
2, J. Stein
3, T. Aziz
3, S. Wang
4, K.A.
Mamun1
1Department of Computer Science & Engineering, United International University, Dhaka, Bangladesh,
2Department of Mechanical Engineering, Imperial College London, UK,
3Functional Neurosurgery and Experimental Neurology Group, University of Oxford, UK,
4Suzhou Institute of Biomedical Engineering and Technology, Chinese Academy of Sciences, Suzhou,
China.
Introduction: Neuro-motor prosthesis is a device to provide movement commands from brain
signals so that neurologically impaired patients are able to perform daily tasks to interact with
environment. Studies in monkey [1] and human [2] have shown that the primary motor cortex (M1)
could potentially provide movement-related signals to control assistive devices for paralyzed patients.
However, other areas of the brain may provide alternative or additional information. Deep brain
stimulation (DBS) offers a unique interface to sense and intervene the human brain circuits. Oscillatory
local field potentials (LFPs) activity in the sub thalamic nucleus (STN) is directly or indirectly
involved in motor preparation and control [3], which suggests that useful movement signals may be
available in this area as well. This study aims to decode the neural activity related to human voluntary
movements by identifying neural synchronization features and patterns related to movement execution and
laterality.
Methods: LFPs were recorded from bilateral STN via implanted DBS electrodes in patients with
Parkinson‘s disease while they performed left or right finger clicking task guided by visual cues. The STN
LFPs were low-pass filtered at 90Hz and then the frequency dependent components were extracted
as = 0-4Hz, θ = 4-8Hz, α = 8-12Hz, low β = 12-20Hz, high β = 20-32Hz, low γ = 32-60Hz and high γ =
60-90Hz frequency bands using wavelet packet transform. In each frequency band signal features were
extracted based on instantaneous power and neural synchronization. The instantaneous power of each
component was computed using the Hilbert transform. The power features were defined as the
average amplitude within each of five consecutive 100ms windows located around the motor response [4].
The long range neural synchronization based features for motor response were computed by analyzing
Granger causality between the left and right STN [5]. A Bayesian classifier incorporating these features
was designed for optimal feature selection and classification. The features were ranked (highest to
lowest) according to their individual classification accuracies and then a subset of features was
accumulatively selected either when the classification rate reached maximum or plateaued. The classifier
was validated using ten-fold cross-validation.
Results: Consistent significant power decreases in the β bands and increases in and γ bands, as well as
significant contralateral causal synchronization in β and γ bands were observed during the motor
response. Both movement, i.e. resting or action, and laterality, i.e., left or right clicking were evaluated from
four subjects. The average accuracy obtained was 90% for identifying movement, with significant
contribution from , β and high γ bands features. The following laterality classification achieved 81%
average accuracy with significant contribution from β and γ bands features.
Conclusions: The results suggest that the neural activity in human STN contain movement information. The
bilateral synchronization features significantly facilitated to identify movement laterality. These findings
may enhance our understanding on the underlying processes in STN for voluntary movement control and
its important implications for the development of neuro-motor prostheses in humans. Movement
related information in STN might be useful for developing more advanced neuro-prostheses in combination
with motor cortex activity.
References: [1] Musallam S, Corneil BD, Greger B, Scherberger H, Andersen RA: Cognitive control signals for neural
prosthetics. Science 2004, 305(5681):258-262.
[2] Patil PG, Turner DA: The development of brain-machine interface neuroprosthetic devices. Neurotherapeutics
2008, 5:137–146.
[3] Loukas C, Brown P: Online prediction of self-paced hand-movements from subthalamic activity using neural
networks in Parkinson's disease. J Neurosci Methods 2004, 137(2):193-205.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
83
LCD-6: Efficacy Study of DFL using large Number of F-Latency
Recordings
M Obaidur Rahman, Ehsan Alam Chowdhury and K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh.
E-mail: [email protected], [email protected]
Introduction: Distribution of F-Latencies (DFL) is a method conceived and developed by the
Department of Biomedical Physics and technology, Dhaka University group to diagnose Cervical
Spondylosis Neuropathy (CSN) in early stage. Since there is a inverse relation between F-latency and
conduction velocity, so DFL could provide the information about the conduction velocity distribution
of peripheral nerves. Forty successive supramaximal stimulations with a time interval of one second
were applied to the median nerve at wrist. A smaller response which follows the M-response is called
the F-response. This response is randomly generated and has varying latencies. A distribution plotted
using these latency values give the Distribution of F-Latency (DFL). This study attempts to test the
reproducibility of DFL using various combinations of recorded data.
Methods: Three median nerves of two male volunteers aged 41 and 42 were selected and stimulated
for more than 200 times. The room temperature was recorded as 30°C. From this set of data values
about 200 non-zero data points were chosen. This gives us an option to generate multiple sets of DFL
with a combination of 40 data points at a time. Five individual DFL patterns with 40 data values each
were then checked with each other and the pattern generated from 200 data values. For all of the
patterns the corresponding bin size was chosen 2ms. A simple program was developed for doing this
study in Microsoft Excel 2007.
Results and Observations: The following table presented the outcome of DFL for three median
nerves. The black line indicates the DFL pattern generated with about 200 data points. The other five
different colors (Blue, Brown, Green, Purple and Red) were used to represent the 5 DFL patterns by
choosing 40 data values randomly for five times from the 200 data values.
Nerve N1 Nerve N2 Nerve N3
DFL
Patterns
Discussions: Multiple DFL patterns with 40 data values were generated from a large number (about
200) of recorded F-latency values. The bin size was chosen 2ms. Several attempts were taken to
verify each of the patterns. The outcome of this study enhances our confidence to the use of DFL for
the diagnosis of the neuropathy with 40 data values.
Acknowledgement: Ministry of Science and Technology, Government of the People‘s Republic of
Bangladesh and International Science Program of Uppsala University, Sweden for part support.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
84
LCD-7: Determination of Distribution of Conduction Velocity (DCV) from
measured Distribution of F-latency (DFL)
M Obaidur Rahman and K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh E-mail: [email protected], [email protected]
Introduction: Distribution of Conduction Velocity (DCV) of nerve fibres in a peripheral nerve is
required for a proper diagnosis of neuropathy. In the previous work of our extended group at Dhaka
University, DCV of motor nerve fibres in a peripheral nerve trunk was shown to be an approximate
mirror image of Distribution of F-Latency (DFL), a new nerve conduction parameter conceived and
developed by that group as well. To obtain DFL, 30 to 40 consecutive F-latencies were obtained
through multiple stimulation of a peripheral nerve trunk. However, because of the inverse relationship
between latency and velocity, this mirror image is not exact, a small variation can be expected,
particularly when discrete bin sizes are used to obtain the frequency distribution. In the present work
it is intended to determine DCV from individual conduction velocity (CV) values that are obtained by
converting the corresponding individual F-latencies, obtained experimentally. The effect of bin size
for DCV in relationship to that in DFL will also be studied in order to go for an optimum value.
Methods: For experimental DFL, bin-size of F-latencies is usually taken as 2ms. Since latency is
inversely proportional to CV, if bin sizes for DCV are chosen to correspond to the constant F-latency
bins over the whole range, varied bin sizes for DCV will result, which is not a desired situation. A bin
size which gives a justified correspondence between the two distributions is necessary. Therefore, a
constant bin size of DCV was chosen based on the following parameters of the F-latency data for the
range of non-zero values: the average of the minimum and maximum, the weighted average, median
and mode. The correspondence between DFL and DCV was assessed visually from the plots for a
choice among these.
The bin-sizes for DFL were also varied between 0.5ms to 2ms although the distributions for the
smaller bin sizes may have variations that are not statistically significant for the limited number of
experimental events (30 to 40). This exercise would help choose an optimum value of a constant bin
size for DCV. A program in EXCEL was developed to perform the above studies.
Results: DCVs corresponding to DFLs were obtained for several subjects with or without neuropathy,
using different constant bin sizes chosen according to the methods suggested above. The plots were
compared and assessed visually to look for a reasonable correspondence. For different subjects
slightly different bin sizes for DCV appeared to be appropriate. The study on the several subjects gave
an indication of appropriate bin sizes which would help in further studies.
Conclusion: The present technique gives an acceptable DCV from measured F-latencies, which is a
parameter required for a proper diagnosis of neuropathy.
Acknowledgement: Ministry of Science and Technology, Government of the People‘s Republic of
Bangladesh and International Science Program of Uppsala University, Sweden for part support.
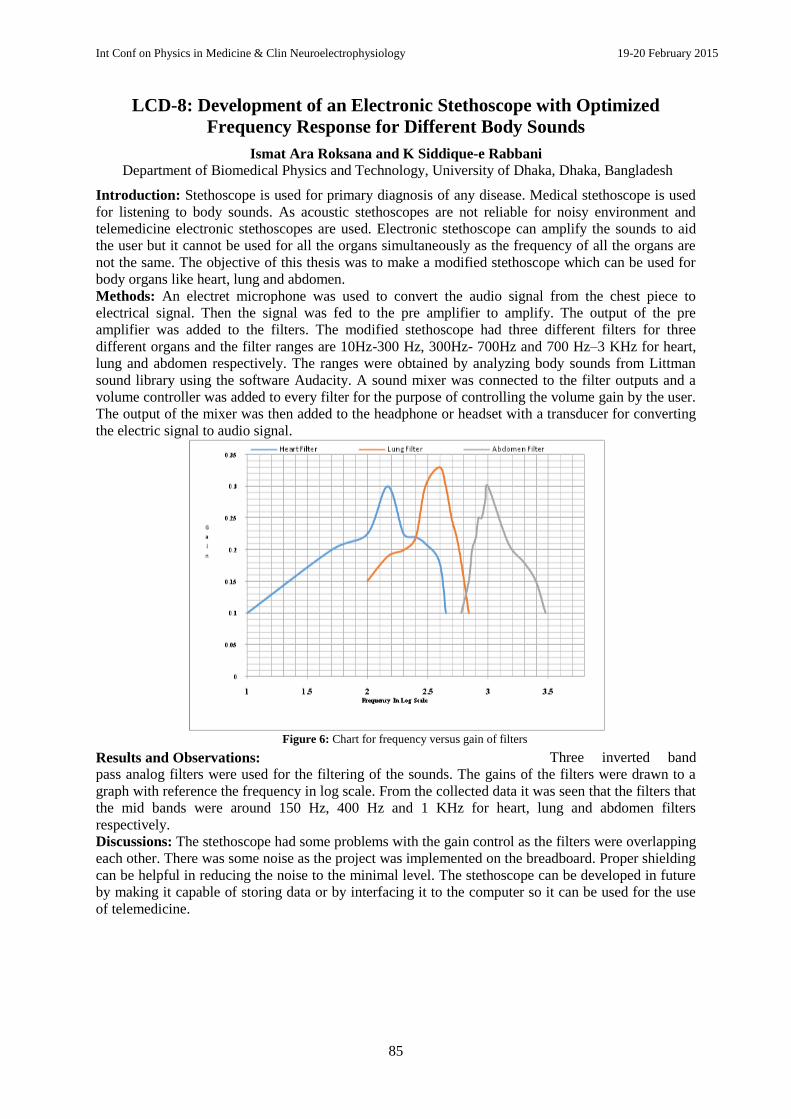
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
85
LCD-8: Development of an Electronic Stethoscope with Optimized
Frequency Response for Different Body Sounds
Ismat Ara Roksana and K Siddique-e Rabbani
Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh
Introduction: Stethoscope is used for primary diagnosis of any disease. Medical stethoscope is used
for listening to body sounds. As acoustic stethoscopes are not reliable for noisy environment and
telemedicine electronic stethoscopes are used. Electronic stethoscope can amplify the sounds to aid
the user but it cannot be used for all the organs simultaneously as the frequency of all the organs are
not the same. The objective of this thesis was to make a modified stethoscope which can be used for
body organs like heart, lung and abdomen.
Methods: An electret microphone was used to convert the audio signal from the chest piece to
electrical signal. Then the signal was fed to the pre amplifier to amplify. The output of the pre
amplifier was added to the filters. The modified stethoscope had three different filters for three
different organs and the filter ranges are 10Hz-300 Hz, 300Hz- 700Hz and 700 Hz–3 KHz for heart,
lung and abdomen respectively. The ranges were obtained by analyzing body sounds from Littman
sound library using the software Audacity. A sound mixer was connected to the filter outputs and a
volume controller was added to every filter for the purpose of controlling the volume gain by the user.
The output of the mixer was then added to the headphone or headset with a transducer for converting
the electric signal to audio signal.
Results and Observations: Three inverted band
pass analog filters were used for the filtering of the sounds. The gains of the filters were drawn to a
graph with reference the frequency in log scale. From the collected data it was seen that the filters that
the mid bands were around 150 Hz, 400 Hz and 1 KHz for heart, lung and abdomen filters
respectively.
Discussions: The stethoscope had some problems with the gain control as the filters were overlapping
each other. There was some noise as the project was implemented on the breadboard. Proper shielding
can be helpful in reducing the noise to the minimal level. The stethoscope can be developed in future
by making it capable of storing data or by interfacing it to the computer so it can be used for the use
of telemedicine.
Figure 6: Chart for frequency versus gain of filters

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
86
LCD-9: Implementations of a system of transferring electronic stethoscope
sound over mobile phone call for live auscultation in Telemedicine
Maruf Ahmad1, Md. Kamrul Hussain
2 and K Siddique-e Rabbani
Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh E-mail:
Introduction: Electronic stethoscope is being used in telemedicine for many years. But most of the
time, stethoscope sound is first recorded on computer then it is sent to the destination computer for
doctor‘s hearing. Because, real time auscultation wouldn‘t be possible for many reason – one of this is
most videoconferencing system and voice transfer protocol perform audio compression technique and
limit the passes of low frequency signal that reduce the quality of the heart sound [1]. With this
challenge, much research has so far been done for live auscultation in telemedicine. Here we represent
an easy and low cost solution for it.
Methods: The system consist of two main edges – i)
Patient end for sensing and transmitting stethoscope
sound ii) Doctor end for receiving and hearing the
sound [see figure-1]. The frequency range of the
human internal body sounds – mostly heard heart
sounds is between 20 Hz to 200 Hz and lung is
between 25 Hz to 1.5 KHz [2] and same output is
given by electronic stethoscope but audio frequency
range of mobile phone call is limited. For
narrowband the range is from 300 Hz to 3.4 KHz
and for wideband the range is from 50 Hz to 7 KHz [3]. Most of the telecom providers of our country
are using narrowband audio frequency range for voice call transmission. So, as most of the sounds of
electronic stethoscope are low frequencies which are unable to transfer over mobile phone call. To
overcome this, in the transmitting side, low frequency stethoscope signal is modulated with high
frequency carrier signal typically it is 2.5 KHz so that it meets the audio frequency limit of the mobile
phone call and in the receiver side, received signal is first gone through demodulation process for
extracting stethoscope signal. Patient end consists of i) electronics stethoscope with appropriate filters
ii) modulation using PLL iii) sender‘s mobile phone and doctors end consists of i) receiver‘s mobile
phone ii) demodulation using PLL iii) headphone for hearing sound.
Results: Initially we have tested the modulation and demodulation process over mobile phone call for
different input frequency range and found the result quite impressive. The figure-2 shows CH-1
(yellow) represents the shape of the output signal and CH-
2 (blue) represents shape of the input signal. Though
output signal is somewhat noisy, it is actually high
frequency carrier signal and would be further canceled by
using second order high pass filter.
Conclusion: As we found a satisfactory result from the
test, we, therefore, are expecting that overall system will
work successfully and will be able to transfer stethoscope
sound using mobile phone call and it would also be a low
cost solution for live auscultation in telemedicine.
Acknowledgement: International Science Program of
Uppsala University, Sweden for part support. References:
[1] http://www.thinklabs.com/#!telemedicine/c1q1a
[2] Ara, Ismat ―Development of an electronic stethoscope with optimized frequency response for different body
sound.‖ A Thesis submitted to Department of Biomedical Physics & Technology University of Dhaka. 2014.
[3] http://en.wikipedia.org/wiki/Wideband_audio

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
87
LCD-10: Investigation of X-ray Image Quality for Telemedicine
Susmita Afruz, M Abdul Kadir and K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka 1000 Bangladesh
Introduction: Because of being overpopulated and underprivileged, most of the people of third world
countries, especially the rural people are deprived of modern medical facilities. Telemedicine may be
an easier and cheaper way to disseminate healthcare facilities to the rural areas. Department of
Biomedical Physics and Technology, University of Dhaka has been working for the development of a
telemedicine system with integrated diagnostic equipment, mostly designed and fabricated locally. X-
ray imaging is widely used in disease diagnosis and for telemedicine; this image quality should be
excellent, as it is required to transfer the image to a distance through any medium. The present work
was taken to evaluate quality of such images.
Methods: X-rays attenuates exponentially with thickness while passing through a material. A wedge
shaped piece of aluminium was used for this study whose X-ray image was taken on a film at a
conventional clinic. It was assumed that the exposure on the film after passing the aluminum piece
would be exponential. A digital image of this X-ray film was created by photographing the X-ray
film, placed over the illuminated X-ray view box. It uses a reasonably high resolution webcam to take
picture of an X-ray film image illuminated using a conventional X-ray view-box. The piece of
aluminium provided a gradual change in the level of darkness of the image. The digital image was
analyzed using MATLAB software to study the variation of the level of darkness of the image with
the thickness of the piece of aluminium. Besides, the resolution of the image was also studied.
Results: The results of the analyses would provide a quantitative assessment of the quality of the
digital image captured using this device. This would be helpful in giving interpretations of the digital
image and also in improving the quality of the system in the future. Characteristics of the digital
image reasonably follow the characteristics of real X-ray film grayscale image. It also provides an
exponential relation between image pixel value and object thickness. This relation supports the
expected behavior based on basic principles. It can also provide information about granular object. In
this research work, X-ray image Quality was found good enough for diagnosis and for making any
medical decision.
Discussion: This research work explains the procedure as well as the result of X-ray image quality
investigation. X-ray image as well as the digitized image both can articulate sufficient information.
Theoretically, we accepted that pixel value is exponentially related to the distance and from the
experimental graph, we can also establish that. 14 vertically situated grooves indicated a continuous
thickness variation for which, we have found nearly a sinusoidal waveform that retain the particular
object information.
Figure: Pixel value Vs distance graph for horizontal thickness
difference.
Figure 1: Pixel value vs distance for vertical thickness difference.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
88
LCD-11: Phaco-Emulsifcation Using Rotating Needles: A New Technique
Mohammad Abu Yousuf Talukder1 and Sirajum Monir
2
1 Medical College for Women & Hospital,
2 Department of Physics, Gofforgaon Govt. College
Introduction: Cataract is a leading cause of blindness which can be corrected by extracting
cataractous lens and by introducing PCIOL. Modern technique extraction of cataractous lens is phaco-
emulsification which is very expensive and can no longer be done if the patient attains the hyper –
matured stage of life cycle. To make the process safer, a new machine has been recommended. The
recommended new device is very simple in nature yet very effective in achieving the goal, and also
very cost effective for the vast number patients. The machine will work by rotating a special type of
needle (Yusuf‘s needle) which is made by incorporating 3-4 hypodermic needles. Material and method: The Machine has two parts namely BODY and the TUBE. The Body is again
divided into two parts. It houses the power sources and a small motor. The motor has a shaft enabling
the needle to rotate in circular motion at the speed of 700-1400 rpm. The base of the body there is a
contact switch to activate the circuit. The diameter of the tapered end of the tube is about 2 to 2.5mm,
so during the micro incision the tube bearing the needle will enter the anterior chamber of the eye ball
with only 2.5 to 3 mm incision. Three different tests have been carried out successfully which read as
under: with wood, with goats eye and with human crystalline lens in vitro. These tests were carried
out with a view to evaluating the performance of the referred machine in different medium.
Result: The first test is fitted for the penetration capacity which is seen satisfactory. The second test is
done to evaluate the efficiency of the machine which is again found to be very inspiring with no major
complication detected. While the last one is carried out with human crystalline lens in vitro in which
it is seen that in immature cases lens become jelly like substance very quickly , on the other hand in
matured and hyper matured cases lens become jelly like substance slowly and very slowly
respectively. So, that is to say that the lenses have been emulsified optimally as expected.
Discussion/Conclusion: The result thus obtained satisfies the ophthalmological standard, and by
following this new machine, a large number of people who are left with no treatment for want of
money in the poor countries like Bangladesh, can be brought under treatment in a very cost effective
way. It is to propose here that we may effectively start using the new device in rural areas with the
effective training process imparted to qualified ophthalmologists.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
89
LCD-12: Low cost Dynamic Pedograph and customized shoe for diabetic
patients
MO Rahman and KS Rabbani
Department of Biomedical Physics and Technology, Dhaka University E-mail: [email protected], [email protected]
Introduction: Diabetic patients usually suffer from lack of nerve sensation, especi ally in the feet.
Therefore, their gait on standing and during walking may deviate from that of a normal person and points
of high pressure develop under the feet. However, due to neuropathy they do not feel any pain which
would have been felt had the nerve functions were alright. Later, ulcers form at these high pressure points;
gangrene and amputation of the leg follow suit. Therefore, a simple device to assess and measure the
pressure distribution under the feet would be very helpful in early detection of high pressure points.
Special insoles can then be prepared to spread the pressure away from the hot spots, thus saving the patient
from the eventual traumatic amputation, crippling the person for the entire life. Again, pressure points and
pattern may differ while standing and during walking, usually it is the latter which put the soles on greater
burden, and a dynamic pressure measurement during walking has more importance from a clinical point of
view.
Methods & Results: A low cost Dynamic Pedograph, including hardware and computer software, suitable
for the Third World was developed [2,3]. Giving due consideration of various factors, a Pedograph based
on an optical sensor was the choice of our group. The idea was borrowed from an earlier work in Sheffield,
UK [4]. Figure below on left shows an installed unit and printouts of foot pressure distribution.
After clinical evaluation of the patients an attempt was also made to provide them insoles
for customized shoes such that the pressure at the high pressure points are distributed over
a larger area, thus decreasing the localized pressure points. Initially a manual system was
developed which is cost effective and is suitable for countries like Bangladesh where cost
of labour is low. In this method firstly a grayscale printout of the foot pressure distribution,
as shown in Figure on right is placed over a 3 to 4 mm thick rubber sheet, which will be
used to make insoles of shoes. At the high pressure points, easily recognizable through the
density of the print, dents are made using a spherical grinding bit attached to a drilling machine. This
produces a final customized insole (furthest right photo) that can be used to make a customized shoe for
the individual patient.
Conclusion: In future, the insole may be prepared automatically using a CNC machine getting data
directly from the computerized Pedograph unit. A 3D printer may also be used to print out a customized
insole. Thus a low cost solution for foot problems of diabetic patients may be obtained through the
developed technology.
Acknowledgement:
Diabetic Hospital of Baqai Medical University, Karachi, Pakistan and Bangladesh Institute for Biomedical
Engineering & Appropriate Technology for funding for the first prototype of the Pedograph. References: 1. Tekscan, Inc. website (2010). [Online]. Available: http://www.tekscan.com/medical/system- matscan1.html
2. KS Rabbani, SMZ Ishraque, MS Islam, RM Rabbani, Improvisation of an optical pressure sensor based dynamic foot
pressure measurement system, Bangladesh Journal of Medical Physics, Vol. 4, No.1, 2011, p.51-58
3. WHO Compendium of Medical Devices for Low Resource Countries, 2011
4. C. I. Franks, R. P. Bens, and T. Duckworth, “Microprocessor based image processing system for dynamic foot pressure studies”, Med. and Biol. Engg. And Comput. Vol. 21, pp. 566 - 572, 1983.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
90
LCD-13: A Study of Nuclear Detector Materials Using Thermal
Evaporation Method
K M A Hussain1, Z. H. Mahmood
2, S. M. Ishtiaque
3, T. Begum
4, J. Begum
1, F. A. Chowdhury
1,
T. Faruqe1 & S Ahmed
1
1Experimental Physics Division, Atomic Energy Centre, Dhaka
2Department of Electrical and Electronic Engineering, University of Dhaka,
3Department of Physics, University of Dhaka,
4Atomic Energy Centre, Dhaka.
E-mail: [email protected]
Introduction: Patient dose optimization is a great challenge in the present medical field. Digital
sensors have shown importance in this challenge. CdTe have favorable physical characteristics for
medical applications which have been investigated in the 1980s.The material is considered to be one
of the most effective materials for the fabrication of X-ray and γ-ray detectors operating at room
temperature due to specific properties of high average atomic number, good charge-transport
properties, high resistivity, and relatively large band gap energy. However, new CdTe detector
designs are promising greater potential for the application of CdTe detectors to X-ray and γ-ray
applications. The present investigation is preparation and characterization of CdTe thin film
semiconductor with new deposition parameters.
Methods: The CdTe thin film was prepared by thermal evaporation method. A vacuum unit
(Edwards, E306A, UK) was used to prepare the films. The thickness of the CdTe thin film was
measured by a quartz crystal monitor Edward model FTM 5. The transmittance (T %) of the CdTe
films with wavelength of light incident on them were recorded using a dual-beam UV-VIS-NIR
recording spectrophotometer (Shimadzu, UV-3100, Japan) in the photon wavelength range from 300-
2500 nm. The absorption co-efficient and optical band gaps were found from the transmittance data.
Results and Observations: The figure-1 showed that the transmittance was varied with photon
wavelength of 400nm to 2500nm. It is observed that high transmittance (90.54%) in the visible region
is obtained for all films. The films of thickness 500 nm shows good interference pattern which
indicates better homogeneity and good quality of CdTe thin films. The X-ray diffraction analysis in
figure-2 shows that the (111) diffraction plane is localized at approximately 23.7º and the two weak
peaks are at approximately 39.3º and 46.6º match with the (220) and (311) diffraction plane of cubic
phase CdTe films which is in good agreement with the reported literature.
Figure 1: Optical transmittance and XRD spectra of CdTe thin films.
Conclusions: The CdTe thin film detector material is successfully deposited using thermal
evaporation method. The insitu technique shows digital thickness. The structural and optical
properties of vacuum evaporated CdTe thin films with varying film thickness (500-700 nm) were
investigated. The high transmittance showed all the films have high absorption coefficient above the
fundamental absorption edge. Each film shows a preferred orientation along (111) plane of cubic
phase, in addition two other prominent planes (220) & (311). The crystalline quality is observed at
optimum substrate temperature.
0
20
40
60
80
100
0 1000 2000 3000
Wave length (nm)
Tran
smitt
ance
(%)
500 nm600 nm700 nm

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
91
LCD-14: A PC based Data Acquisition System for Bio-medical
Instrumentation
A Al Amin, A Imtiaz Khan, AKM Bodiuzzaman, K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh E-mail: [email protected], [email protected], [email protected], [email protected]
Introduction: Computer controlled data acquisition system is an essential part of biomedical
instrumentation. Most of the commercially available PC based Data Acquisition systems are of very
high cost, requires specific commercial software for data storage and analysis. Moreover if the data is
not stored in raw binary or known format, it is not possible for the user to use the data in other
software of their own choice. Therefore, a low cost, simple and open source PC based data acquisition
system for biomedical application would be very useful for instrument developers in the low resource
countries.
Methods: A low cost 8-bit Atmel AVR ATmega8 [Atmel
Corporation] microcontroller with integrated analog to digital
converter (ADC), four operational amplifiers, a MOSFET, a hand
wound high frequency toroidal transformer, an optocoupler, and a
few passive components are used for the hardware part. For
subject‘s safety and noise reduction an analog optical signal
isolator was designed and implemented [Rabbani et all, 2011].
The analog bioelectric signal from the human body is first
conditioned and fed to the non-isolated PC side through the
analogue isolation circuitry (Fig.1). Then the signal is
conditioned to meet the ADC input requirement and converted to digital values using the onboard 10-
bit ADC of the microcontroller. The digital data is then transferred to the PC through USB 1.1 low
speed HID Class interface [USBIF], implemented in the same microcontroller using firmware only
USB library V-USB [Objective Development Gmbh]. For powering the isolated circuitry in the
patient side, a medical grade isolated dc to dc converter is constructed which uses the non-isolated +5
volt supply available from the USB port of the PC. Therefore no external battery or power supply is
needed. The device was operated in two modes, Continuous conversion mode and Batch mode. The
former was for low frequencies up to a few hundred Hz, while the latter could work up to a few tens
of kHz. The software is a graphical user interface which allows viewing the bioelectrical signal in
selectable different time scale and can store data in raw binary format. It is developed using ‗JAVA‘
platform considering its operating system (OS) independent feature.
Results & Observation: A sinusoidal wave of 80 Hz is fed from a
signal generator to the data acquisition system and resulting PC
side software is shown in Figure-2. It is observed that the system
reproduces the signal very nicely in PC. Aliasing effect is seen
after 150 Hz and at 12 KHz and the system shows no significant
phase or amplitude change up to 100 Hz and 10 KHz for
continuous conversion and Batch mode respectively. The system is
used in ECG, EMG, NCV and FIM [Rabbani et al 1999] with
excellent satisfactory results.
Discussion: Most of the bioelectrical signals occur within the band
width of 0 to 10 KHz; therefore this system satisfies the biomedical instrumentation requirements.
The mode of operation is selected form PC, also sampling and data transfer is done simultaneously
and well synchronized, and thus form sampling to display has latency of approximately 10 ms, which
can be regarded as real time. This total system is open source and can be used conveniently in
research or development phase of biomedical instruments without need of extra isolated power source
and signal isolation circuitry.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
Figure 1: Block Diagram of Data Acquisition System
Figure 2: GUI software of Data
Acquisition System

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
92
LCD-15: Development of user friendly software in Bangla for a PC based
rural health monitor with option for telemedicine
Ahamad Imtiaz Khan, Abdullah Al-Amin, Zihad Tarafdar, AKM Bodiuzzaman,
Ahmed Raihan Abir, M Obaidur Rahman, K Siddique-e Rabbani
Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh. E-mail: [email protected], [email protected]
Introduction: Providing quality health service in rural areas is one of the major challenges for
developing countries like Bangladesh. Even if infrastructures are provided, retaining qualified medical
doctors in a village is almost impossible in the near future. The solution to this problem can be
Telemedicine, or ‗medicine at a distance‘. A doctor in a city anywhere in the world can advise a
patient at any remote village, if required communication channel is available. Bangladesh has a good
internet and mobile phone infrastructure spread almost all over the country which can be used to
advantage. Our department has already developed some basic diagnostic equipment the outputs of
which are all digitised and interfaced to a PC with the aim of integrating these facilities with the
telemedicine system. The present work takes care of the software aspect of the integrated telemedicine
system, and that in user friendly way, with some graphical user interface in Bangla, our local
language.
Methods: The diagnostic devices developed in our department to go with the telemedicine system
are: ECG, Respiration Monitor, X-ray viewer, Microscope, Colposcope and General purpose image
digitiser (a high quality webcam on a stand). To get information on temperature, blood pressure,
weight, height, etc., standard equipment are available at reasonably low cost and a rural technician can
type in the resulting values into the computer system.
In order to develop user friendly software for the whole system, firstly we developed necessary
software to acquire the data into a PC at the rural centre from the above mentioned equipment. For the
ECG equipment, which was developed in our laboratory from basics, we developed appropriate
software using Java programming language for data acquisition of all 12 lead signals in sequence,
display, signal processing and storage and for sending almost live data over internet. Outputs of
digital X-ray viewer, microscope and colposcope are images which were acquired using software for
the webcam used inside these devices. For transferring images we used our web application which we
developed for telemedicine.
We have developed a web based application for our telemedicine solution. The purpose of this
application is to maintain the whole system properly. It‘s like a hub of our telemedicine system.
Patient registration, request forwarding, prescription making with minimal mouse clicks, report
submission etc. can be done using this web based application. We used PHP and MySQL for
developing this application. The goal of our task was to make it user friendly and appropriate for
using in our rural areas. Graphical User Interface of both ECG software and web based application
was developed in both English and Bangla languages. Bangla will make it easier for the rural
operators to use it comfortably.
Results: The developed software appears to work well, as field tests were carried out in several
remote villages in Faridpur.
Discussion/Conclusion: The user friendly software, whether in English or Bangla, will enhance the
quality of diagnosis and the resulting treatment through telemedicine immensely.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
93
LCD-16: Solar Water Pasteurizer and Rain Water Collector for provision
of safe drinking water in urban slums and rural areas
M Abu Yousuf 1, Rezwan bin Hussain
2 and K Siddique-e Rabbani
1
1Department of Biomedical Physics & Technology, University of Dhaka, Dhaka, Bangladesh
2University of Liberal Arts, Dhaka, Bangladesh
E-mail: [email protected], [email protected], [email protected]
Introduction: Providing safe drinking water to rural people throughout the resource poor countries is still
a challenge. Our extended group at Dhaka University innovated a very low cost solar water Pasteuriser in
the eighties that can be made by people themselves using locally available materials like hay, bamboo tray,
transparent polythene bags and sheets. It uses well known ‗Green House Effect‘ to heat water to more than
600C which is needed to destroy all diarrhoeal germs as in Pasteurisation. In this design the UV ray in
sunshine also falls on the water and diarrhoeal germs were destroyed even at 45 to 500C. Hazardous
arsenic contamination is found in water form tube wells, but surface
water is free of arsenic. Therefore destroying diarrhoeal pathogens in
surface water using this Pasteuriser solves both the problems providing
safe drinking water. Besides, being domestic models, individual families
can maintain the device resulting in a sustained solution. Recently we
developed models more suited to the demands and taste of the urban
poor. Besides, it was designed to collect rainwater as well to make it
useful all the year round.
Methods: One model, a ground laid solar water Pasteuriser only, used
thick polystyrene foam blocks to make up a thermally insulated tray,
24‖x32‖ in area, as shown in the top figure. Its base is covered by a black
plastic sheet. A transparent polythene or polypropylene bag of size
24‖x36‖ is filled with about 10 litres of water and spread over the whole
of the inside base, to make a water depth of about 2 cm. The open side of
the bag rises over one of the edges. A rectangular frame made of
aluminium or uPVC pipes was covered on both sides by stretching
transparent PVC films. This frame was allowed to rest on the edges of the
plastic tray, thus providing two covered air gaps, each 2cm thick, on top
of the water bag for thermal insulation. This configured a low cost solar
flat plate water heater that employed ‗Green House Effect‘ as in the
previous design, but with improved insulation. It also allowed sun‘s UV
ray to reach the water layer.
A second table model was made which could perform both as a solar
water Pasteuriser and a clean rainwater collector, the collected water
being drinkable directly. For this the table top of a commercially
available folding table is used as a base, where the table top was chosen to have a black plastic finish.
Polystyrene foam was used to insulate the underside and the four sides of the table top, again to make a
tray. A small length of an aluminium tube was fixed at one of the sides to work as a drain pipe. When the
iron tube frame underneath is extended to mount it horizontally, as shown in the middle figure, it makes a
solar Pasteuriser in conjunction with a bag of water and rectangular frame covered by two transparent PVC
sheets as in the previous design. We provided a catch on the iron frame below to mount the table in a
slanting position as well, as shown in the bottom figure. With the bag and the top frame removed, this acts
as a rainwater collector. The cost was about US $20.
Results: The device could heat about 10 litres of water to about 900C under summer sun in Dhaka in about
two and a half hours. Only about an hour was needed to reach 600C. It would take slightly longer in winter.
Therefore, two or three harvests are possible making more than enough for a family. Amount of rainwater
that can be collected is about 4 litres for 10 mm rainfall.
Conclusion: This device can provide safe drinking water for urban slums as well as in rural areas. The
transparent bags would need occasional change but the main structure is expected to last for years. As
mentioned before, a family that owns it will maintain it providing a sustained solution.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
94
LCD-17: Low Cost Technology for Inactivation of Diarrhoeal Pathogens in
Drinking Water Using Metals
*Sharmin Zaman1, Anowara Begum
1, Md. Latiful Bari
1 and K Siddique-e Rabbani
2
1Centre for Advanced Research in Sciences, Department of Microbiology,
University of Dhaka, Bangladesh, 2Department of Biomedical Physics and Technology, University of Dhaka, Dhaka, Bangladesh
Introduction: Technology for safe drinking water for rural areas of the low resource countries is still
a big challenge for the humankind. The present study was designed to develop a simple technology,
employing the bactericidal effect of metals that can be implemented by rural households. The research
was initiated by reports that brass door knobs in hospitals contained less germs than on single metal
knobs, which was supplemented by the knowledge of the ancient practice in rural Bangladesh of
leaving water in a brass or bronze pitcher overnight.
Methods: Three thick metallic sheets made of Copper, Zinc and Brass (alloy of copper and Zinc)
respectively were placed in three plastic (polythene) containers with base areas 11cm x 7cm each so
that the metallic sheets covered the entire base areas of the respective containers. Four hundred (400)
ml of contaminated water from a public pond was added to each container, covered with lids and left
undisturbed at room temperature. The microbial analysis of Total Viable Bacteria (TVB), Total
Coliform Bacteria (TCC) and E. coli was done taking small samples initially and then every 24 hours
up to six days of storage at room temperature. E. coli is considered as the indicator for diarrhoeal
pathogens. Therefore, if E.Coli is completely inactivated, the water is said to be safe for drinking.
Other remaining bacteria are usually harmless.
Results and Observations: In a typical experiment, the initial bacterial counts were, TVB: 1.67 x
103, TCC: 1.4 x 10
3 and E.Coli: 1.38 x 10
3. TVB count did not reduce significantly for any of the
metals used in this study during the 144 hours of study. Total coliform counts decreased to almost half
the original in the first 24 hours for all the three metals, but remained almost the same afterwards.
However, E.Coli was completely inactivated on treatment with copper for 24h, and remained so
afterwards. On the other hand, Brass and Zinc reduced E. coli population by almost half in the first 24
hours, but this remained almost constant throughout the rest of the measured period.
Discussion: The above results suggest that a simple copper sheet could be useful in inactivating
diarrhoeal pathogens, producing safe drinking water in 24 hours. Therefore, this could give rise to a
simple technology to obtain safe drinking water in the rural areas of the low resource countries.
However, it needs to be ascertained whether the amount of copper present in water is within the safe
limit, since regular use in larger amounts may lead to copper poisoning. A future study will try to
optimize the relationship of the volume of water to the exposed surface area of the copper sheet and
the time of treatment so that the diarrhoeal pathogens are inactivated to a safe level while keeping the
copper level within the safe limit too.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
95
LCD-18: A Low Cost Mechanical Prosthetic Hand
Ehsan Alam Chowdhury, K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka. E-mail: [email protected], [email protected]
Introduction: Leg prostheses are available in Bangladesh from several sources but hand prostheses
are not. Those that are available are simply cosmetic, without any functional capability. The
department of Biomedical Physics & Technology of the University of Dhaka had developed a semi-
functional prosthetic hand for wrist amputees earlier as shown in the four photographs in the top row
of pictures. The hand of a mannequin was used for this purpose. The thumb was cut out and refitted
using a spring hinged mount. Normally the thumb kept closed but the user, who had an intact opposite
hand, could slip in a pen or other things to hold between the thumb and the forefinger. The subject
could write using this hand which is also shown in the picture. She could also type holding a pen with
the other end in front and could solder electronic circuits. This was a very successful design providing
both cosmetic purpose and some functionality. A similar hand was fitted to a rickshawpuller which is
shown in the bottom row of pictures. This comes out to be very cheap, about $US 30, which is
affordable to many in low resource countries like Bangladesh.
In the present work we intend to make the prosthesis body powered so that the user can open or close
the thumb through movement of the hands or the shoulder as shown in the right hand side photograph
in the bottom row. This picture is taken from the internet and such devices are available in the
advanced countries. However, these are not available in Bangladesh. Besides such body powered
prosthetic hands need individual customized fixing. in The
Methods: In the present work we tried to
develop the harness of the prosthetic hand using
belts and pads made of leather and woven
materials. The user would extend the shoulder
to open the thumb and when released will
automatically grip an object through the spring
mounted thumb as before. For transfer of power
to the hand we used brake cables of bicycles.
Results: When we tried to fix this prosthetic to
the girl who was given the prosthetic hand
earlier, we found that the extension provided by
her shoulder was not enough to pull the thumb open as she had a slim body. On the other hand
persons with a broad shoulder such as a grown up man could easily extend the thumb. Again the
harness needed is not liked by girls very much.
Discussion: The body powered prosthetic hand is a practical option mostly for grown up males. An
electrically driven prosthetic hand would be more suitable for girls and children.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
96
LCD-19: A Low Cost Prosthetic Bionic Hand
Md. Nazimul Kadir, Md. Kamrul Hussain, Zubair Barkat, K Siddique-e Rabbani
Department of Biomedical Physics & Technology, University of Dhaka.
E-mail: [email protected], [email protected]
Introduction: The study reported here explored the design of the prosthetic bionic hand to be made
by department of Biomedical Physics and technology, University of Dhaka. Prosthetic Bionic hand
will be installed and used in least developed countries (LDCs),the purpose is to realize a functional
and user friendly system, suitable for diverse group of users, with a cost of less than 80€. The
proposed project aims to make available to the populations of developing countries at affordable cost.
Methods: The developed prosthesis is composed of a light plastic and aluminum structure with
opposing fingers. We have obtained the movement of the prosthesis with a geared stepper motor. The
control system we have created is based on microcontroller based simple electronic circuit that
doesn‘t use advanced technological solutions but cheaper and easier to find circuit components; in this
way we have tried to achieve the best compromise between performance, convenience and durability.
Results and Observations: The mechanical part of the prosthesis is composed by light aluminum
structures and powered by a geared stepper motor. Prosthesis total weight is 250 grams. The stepper
DC motor block includes steeper motor; its nominal supply voltage is 12V and absorbs a maximum
current of 800 mA.
Discussions: The future work includes specific speed testing for various application, multiple finger
control as well as inclusion of force sensor for identify object and improved gripping.
Acknowledgement: International Science Program of Uppsala University, Sweden for part support.
9 Inch

CLINICAL NEUROPHYSIOLOGY PAPERS

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
98
Invited Talk
ICN-1: Technical Aspect of Neuroradiology and their Clinical Evaluation
in Children Presenting with Seizures and Neurodevelopmental
Comorbidities
Rakshan Gocmen
Professor Neuroradiology, Hekatteppi University Hospital, Ankara, Turkey
Magnetic resonance imaging (MRI) is the main structural imaging in epilepsy. Using a dedicated
MRI-protocol for epilepsy, it is possible to detect and characterize an epileptogenic focus in the
majority of patients with focal seizures. Its detection is crucial for subsequent diagnostic and
therapeutic planning and, in the event of a negative MR, one must always consider the possibility of
increasing image quality. Resection of these lesions can lead to seizure freedom in many patients.
Using together structural MRI techniques and functional MRI modalities such as diffusion tensor
imaging, BOLD imaging, magnetic resonance spectroscopy and magnetic resonance perfusion are
key technology in the presurgical evaluation of patients with focal epilepsy. Task-related functional
MRI techniques can be used to estimate language networks and lateralization and memory networks,
and may therefore inform the presurgical planning process. Similarly, diffusion tensor imaging is
becoming widely used in research settings to image white matter pathways and provide an alternative
structural view of connections between brain regions.
CN-1: Recognizing Normal Electrophysiological Criteria and Deviation to
Dysfunction in Neonatal EEGs.
Naheed Nabi1, Biplob Banerjee, Selina H. Banu
1Dept of Clinical Neurophysiology, Comfort Diagnostic Center, Green Road Dhaka
Background: Electrical activities of neonatal brain remain in a rapid progression that needs a careful
evaluation. Only an experienced neurophysiologist can differentiate a cerebral dysfunction during
this maturation process. Neonatal seizures might be idiopathic or with severe structural,
neurometabolic or transient metabolic disorder. Routine or continuous EEG monitoring can confirm
the diagnosis, predict the underlying cause and helps the clinician for further management planning.
This study describe the variable EEG features in neonates presented with neonatal seizures.
Method: We have complied retrospectively 195 neonatal recordings from EEG lab of Comfort
Hospital and Central Hospital from June‘13 to December‘14. The clinical presentation, birth related
information and EEG findings were correlated.
Result: Among total 195 neonates there was male preponderance (65.12%). The majority had h/o full
term (88.2%) hospital delivery, about 60% delivered by caesarean section. Home delivery was
reported in 17.4 %. The common reasons for EEG advise was definite seizures (26.7%), jerky
movement (24.6%) and inconsolable crying (18.5%). The EEG findings were categorized as
epileptogenic discharges in (35.1%) , non-epileptic dysfunction or inappropriate activities for the age
in ( 5% ) and no abnormality in ( 53.3% ).
Conclusion: Neonatal EEG should be read carefully and maturational changes should not be confused
with epileptiform patterns. It is a very simple and useful tool for the early capture of electrical
dysfunction of growing brain.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
99
CN-2: Co-Relation of Neurodevelopmental Status, Seizures,
Electroencephalography and Neuroimaging Findings of Children having
Neurological Problem
A.Z.M. Mosiul Azam, Mustafa Mahbub
Department of Paediatric Neurosciences, Dhaka Shishu Hospital.
Introduction: Electroencephalography (EEG) test has been advised for the children who are seeking
medical advice for seizure. EEG is important for classification of seizure (sz) typed also for selecting
appropriate anti-epileptic drugs. To observe the co-relation between neurodevelopmental status,
EEG Features and Neuroimaging finding in the children with epilepsy Method: A retrospective analysis of 200 children, attended in the year 2012 at department of
Paediatric Neurosciences, Dhaka Shishu Hospital. Neurodevelopmental status, seizure types, EEG
and neuroimaging (CT scan of brain or MRI of brain) findings along with age, sex and other socio-
demographic state were recorded and statistical analysis was done.
Result: EEG test was normal in 50% children and 50% showed different changes e.g. epileptiform
discharges and background abnormalities. Those who were having normal EEG, 24% had history of
perinatal asphyxia, 60% had seizures, 32% had motor dysfunction, 40% had speech problem, 40%
had cognitive deficit and a minor percentage had hearing and visual problem. Fifty percent showed
abnormality in Neuroimaging.
In abnormal EEG group, 35% had history of perinatal asphyxia, 70% had seizures, 61% had motor
dysfunction, 52% had speech problem, 52% had cognitive deficit and 75% showed abnormality in
Neuroimaging.
Conclusion: For clinician to evaluate the neuro-developmental impairments and disabilities. EEG as
well as neuroimaging study have a significant role.
CN-3: Variation of Electroencephalographic (EEG) Pattern in Children
Diagnosed with West Syndrome Md. Shahjahan chowdhury
Department of Paediatrics, Bangabandhu Sheikh Mujib Medical University
Dhaka, Bangladesh
Introduction: West syndrome (WS) is characterized by multiple seizures including central tonic,
myoclonic seizure and infantile spasms; global developmental delay or regression, and characteristic
EEG (electroencephalography) features. Early diagnosis and successful seizure control may halt
further developmental delay and regression. Seizure control and prognosis are best guided by EEG.
Hypsarrhythmic (HA) pattern is the most common feature in EEG. Elimination of hypsarrhythmic
pattern is a principal goal of therapy and a key outcome measure in clinical trials. After the initial
description of Gibbs and Gibbs, several variations of hypsarrhythmia have been described. To
describe the clinical profile and EEG patterns in children with clinical spasm.
Method: This is a retrospective type of study. Total 98 children having clinical spasm were included
in the study, attending Paediatric Neurology Unit, BSMMU during January 2013 to November 2014.
The EEG test findings were collected and correlated with clinical profile. Twenty one cases were
excluded from the study due to normal EEG.
Result: Out of 77 patients of HA, EEG showed episodes of voltage attenuation in 27(35.06%),
classical hypsarrythmia in 14(18.18%), hypsarrhythmia with suppression-burst pattern in
13(16.88 %), hypsarrhythmia with increased interhemispheric synchronization in 8(10.39%),
multifocal epileptic discharges in 7 (9.1%), hypsarrhythmia with a constant focus of abnormal
discharge in 5(6.5%), hypsarrhythmia with high voltage slow wave with little spike or sharp activity
in 3(3.9). Statistical analysis revealed that patients with perinatal asphyxia were more likely to have a
‗hypsarrythmia with voltage attenuation‘ pattern.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
100
Conclusion: These results indicate that interictal EEG of WS showed various patterns other than
classic hypsarrythmia. Moreover, some EEG patterns are related to specific underlying neurological
disorder.
CN-4: Role of EEG in Children with Febrile Seizures
Sahifa Nazia1, Selina H Banu
1, Monimul Haque
1Institute of Child Health & Shishu Shastho Foundation, Mirpur, Dhaka
Introduction: Febrile seizure is very common in our population for multiple reasons. There is a state
of confusion regarding the use of investigation tools particularly of Electroencephalography (EEG).
There is no national guideline about when to advise for EEG in such cases. This study describe the
EEG findings in children presented with complex febrile seizures. Identification of clinical factors,
which would help to develop a guide line for the clinicians.
Methods: A cross sectional study including children attending the inpatient and outpatient
department of the SSF hospital during November 2012 to April 2013. Children of age between 3
month to 5 years, with feature of complex febrile seizures (focal or secondarily generalized szs,
duration longer than 15 minute, multiple szs in 24 hours or more than one attack in one febrile
episode, transient neuro- deficit after the attack) were included. Children with simple febrile seizure,
suspected or diagnosed CNS infection, or preexisting major neurodeficits were excluded from the
study. All clinical and EEG findings were categorized and analised using the SPSS. Total number-
frequency and age at first seizure, family history of seizure or epilepsy, any history of hypoxic
ischemic encephalopathy were categorized and correlated with the EEG findings.
Result: About two third of the population were from middle and upper income families, 13% had
consanguineous parents and the majority were male child. Most of them were born at hospital
without any untoward history during peri-, and postnatal period. Mean age at 1st febrile seizure was
9.7 months, 77% had generalized tonic clonic seizure, 73% had two or more attacks in 24 hours.
About 47% had abnormality on their routine EEG test, of which 78.6% revealed definite epileptiform
discharges. The electro-clinical correlation was significant.
Conclusion: Our study supports the utility of performing EEG for the children presenting with
complex febrile seizures. Based on which further investigation, medical treatment and close
monitoring should be advised. However, further study with larger population is indicated.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
101
CN-5: Clinical Spectrum, Electrophysiologic Profile and Medical
Treatment of Children with Nonconvulsive Status Epilepticus
Kanij Fatema1, Md Mizanur Rahman
1Dept of Pediatric Neurology, Bangabandhu Sheikh Mujib Medical University
Introduction: Nonconvulsive status epilepticus(NCSE) is a term used to denote a range of conditions
in which electrographic seizure activity is prolonged and results in nonconvulsive clinical symptoms.
This study was done to describe the clinical spectrum, electroencephalographic (EEG) findings and
evaluate the efficacy of different therapeutic agents in children with NCSE.
Method: Clinical data of 33 patients with NCSE who attended the OPD and IPD of a tertiary care
centre were analyzed. All these patients had EEG before and after treatment. Treatment was given
between the period 2011 to 2014.
Result: Age range was 6 months to 14 year (mean 5.18 year), 25 were male and 8 were female. Thirty
two patients had prior seizure. Regarding development status, 48% had developmental delay, 22%
had normal development, 9% had regression and 21% had both developmental delay and regression.
The cases were previously diagnosed as epilepsy (29), cerebral palsy (9), developmental delay (5) and
behavioral disorder. EEG diagnosis was as follows: Electrical status epilepticus in slow wave sleep
(ESES) 16 (48.5%), Generalized NCSE 13(39%), Focal NCSE 3 (9%) and Lennox Gastout syndrome
1 patient.
Patients were treated with parenteral or oral drugs. Eighteen patients were treated with Midazolam
drip out of which 1 patient had complete remission in EEG, 6 had 80% remission, 5 had 50%
remission and 5 patients had minimal or no response. In one patient, drug was withdrawn due to side
effects. Thirteen patients was treated with methyl prednisolone bolus out of which 2 patients had
complete remission, 4 patients had 80% remission while 4 patients had 50% remission and 3 patients
showed no response. Other drugs used were sodium valproate, topiramate, phosphenytoin,
levetiracetum and clonazepam.
Conclusion: Pediatric NCSE is an entity with heterogeneous presentation. This study provides
clinical criteria which may guide for early EEG which is essential for diagnosis of NCSE. This study
also highlights the treatment protocol of NCSE which revealed that intravenous drugs were more
effective than oral antiepileptic drugs in remission.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
102
CN-6: Portable EEG Service and Epilepsy Camps to Reach the Unreached
Abu Saleh Musa1, Selina Husna Banu, Shipra Rani, Naila Z. Khan
1 Dept of Paediatrics, Gonoshashtho Medical College Hospital, Savar, Dhaka
Introduction: EEG is needed for diagnosis and prognostic evaluation of seizures,
neurodevelopmental disorders and encephalopathies; however, the service is only available in the
major cities while majority remain unreached. An outreach portable EEG service was introduced in
2008. Later prolonged EEG (pEEG) and emergency EEG (emEEG) for selected and critically ill
patients was added to the service. This study report the service outcomes and explore the usefulness of
the tool in reducing the epilepsy treatment gap.
Methods: We organized monthly epilepsy camp with a team of primary care physician, epileptologist,
technician, developmental therapist and a portable EEG machine at the community. Electro-clinical
correlation, management and cost-effectiveness was reviewed.
Results: Mean age of total 244 patients was 8.94 years, two third of the recordings were performed in
rural populations and in Child Development Centers within public hospitals across Bangladesh; the
rest were in-patients in wards or Intensive Care Units (ICUs) in hospitals within Dhaka city.
Clinical problems categorized as 1. Seizure disorder (SD) 37%, 2. Speech-communication- behavioral
disorders with suspected seizures (SCBD)(21%), 3. Non-seizure neurological disorders (NSD) (42%).
The EEGs revealed epileptiform discharges in 48%, features of encephalopathy in 31%, normal
activities in 21%. Epilepsy diagnosis was confirmed in 74%, 43% and 47% of SD, SCBD and NSD
group respectively. Outcome prediction was statistically significant among the ICU population.
Conclusion: Portable EEG is a cost-effective and useful tool for communities within low resource
settings to reduce the treatment gap. The tool has multiple uses at within hospital settings as well.
CN-7: Reporting the Multiple EEG Findings and Clinical Outcome in
Children with and Without Overt Seizure
Shanta Yesmeen1, Selina H Banu,
1Clinical Neurophysiology Lab, Central Hospital, Green Road, Dhaka
ABSTRACT
Introduction: Repeated routine EEG test is required in some situation for the diagnostic and
prognostic evaluation of seizure and related neurodevelopmental disorders, particularly in absence of
continuous monitoring facility. We have performed multiple EEGs on the same child after hospital
admission or as outpatient. Objective of this study was to review the electro-clinical outcome and
effect of multiple tests on the management plan.
Method: We studied clinical and EEG criteria of children having 3 and more records at the same
laboratory. Detail history of the seizure(s), related neurodevelopmental disorders and drug histories
were recorded during the EEG recording. Information collected during the first and last contacts were
categorized and compared. The prescribed drug list and other investigation findings if available were
also reviewed.
Result: Total 350 EEGs were performed in 74 children during January 2011 to November 2013, 30%
had more than five, 7% had >10 repeat tests. Main complaint were recorded as frequent seizure
attacks with comorbidity, seizures without comorbidity, and recent regression of functional quality
and behavioral change were recorded in 37%, 34% and 29% of the study population respectively. A
large population revealed no-significant electrographic change on the last EEGs, the possible reasons
will be discussed.
Conclusion: With increasing number of such cases in children, there should be special protocol at the
laboratory for those who would need frequent EEGs . The management should focus on finding and
address the underlying cause of uncontrolled seizures particularly in otherwise normal children. In
some specific cases close monitoring should be suggested while there should be EEG test without any
AED.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
103
CN-8: Dynamic Topographic Visualization and Quantification of a
Multichannel Surface EMG Grid Array 1Khondaker Mamun,
2Elizabeth Nguyen,
2Winston De Armas,
2Tom Chau
1Dept. of Computer Science & Engineering, United International University, Bangladesh
2Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Canada
Introduction: Low back pain (LBP) is a prevalent health problem for many people and is one of the
significant causes of disability. Muscle or myoelectric activity is measured by the action potentials
produced by motor units. Surface electromyography (sEMG) is a non invasive procedure used to
evaluate and record these muscle activities. The aim of this study is to develop a novel technique for
clinicians to use sEMG based method for diagnosing and making treatment plan for LBP, where
accurate information about areas of muscle contraction may be obtained in a non-invasive manner.
Methods: In this study, we recorded sEMG signals from a surface electrode array placed in the
lumbar region of the lower back to monitor muscle activities related to static and dynamic conditions.
The sEMG signals produced from the lower back were contaminated with artifacts such as
electrocardiogram (ECG), movement artifacts and/or other noise sources which required effective
filtering. We developed an integrated method to isolate information content related to muscle activity
from noisy sEMG signals. We also developed an algorithm to generate a dynamic topographical map
from the filtered sEMG signals to allow visualization of the lumbar myoelectric activity in a form that
is useful for clinical interpretation and assessment.
Results: The sEMG topographic pattern obtained for static and dynamic conditions from 10
participants showed that the approach is able to provide clinically useful information (e.g. muscle
intensity and spatial distribution) about the lumbar muscle activities.
Conclusion: The methods developed from this study may help to provide clinicians with a novel
means of diagnosing and treating LBP, such that sEMG topography will offer accurate information
about muscle contraction patterns in the lower back. The distribution and patterns of the lumbar
muscle activities may help to identify early signs of LBP and can offer insight into trunk stability of
clients with disability, such that the design of upper body supports can be improved upon.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
104
ICN-2: Establishing Low-Cost High-Quality Technology-Based Health
Services For Countries With Limited Resources – Our Experience
Naila Zaman Khan, MBBS, FCPS, PhD (London)
Professor and Head
Department of Pediatric Neuroscience
Bangladesh Institute of Child Health, Dhaka Shishu Hospital E-mail: [email protected]
Within health services increasing numbers of children and their families are presenting with acute and
acute-on-chronic neurological, neurodevelopmental, pervasive neurodevelopmental and mental health
disorders whose diagnosis and management require the availability of neurophysiological,
neuroradiological, biochemical and genetic laboratory services. This presentation will map the development of quality neurophysiological services in Bangladesh
over the last two decades, which has not only led to its availability within public hospitals across the
country, but also to the transfer of technology to other low and middle income countries (LAMICs).
The importance of multidisciplinary services and partnerships (between North-South and South-South
countries) for quicker transfer of technology will be discussed.
ICN-3: Advancement of Human Machine Interface for Rehabilitation
Engineering
Dr. Khondaker Abdullah Al Mamun
Associate Professor, Dept. of Computer Science and Engineering
Director, AIMS Lab
United International University,Dhaka, Bangladesh.
Email: [email protected]
The advancement in biomedical signal processing and machine learning has led us exploring the
human brain and developing assistive Human Machine Interface (HMI) as well as Brain Machine
Interface (BMI) for rehabilitation engineering. It created the opportunity to discover new
mechanisms and develop new devices for clinical and physical intervention that improves quality of
life for people with severe disabilities. The idea of assistive HMI is detection of patterns of
physiological signals and then transforms it into commands to operate assistive devices, such as
computer, wheelchair, or artificial limbs. When the development of assistive HMI system specifically
considers the pattern of neurophysiological activities of the brain, i.e. neural signals, it is
further categorised as BMI. BMI system not only identifies the pattern of neural signals but also it can
able to feed signals into the deep brain for neural modulation (i.e., bidirectional communication for
enabling Brain Machine Brain Interface (BMBI)). In addition to that, it will help us to understand the
neural circuit mechanisms and open up the possibilities to develop intelligent therapeutic
interventions. This talk will focus on recent advancement of different alternative modalities and
methods of HMI and BMI technology and its ranges of real life applications.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
105
ICN-4: Moya Moya disease: clinical features, pre- and post operative MRI
findings.
Sania Ahsan
Consultant Diagnostic and Investigational Radiology, Apollo Hospital, Dhaka, Bangladesh
Moyamoya disease is a vasculo-occlusive disease involving the circle of Willis, especially the
terminal ICA. It can be primary; sometimes familiar and known as moyamoya disease. Numerous
entities have been described which mimic the Radiologic appearance, in which case the term
moyamoya phenomenon, syndrome or pattern is used.
Moyamoya is not uncommon in Bangladesh. Moyamoya is a disease of children and young people,
with a bi-modal age distribution. The condition was initially described in Japanese patients.
Presentation is age dependent. Children presents with ischemic strokes and adult with hemorrhages.
MRI is the modality of choice for initial diagnosis of Moyamoya. Direct angiography is used only in
equivalent cases. CT angiogram with perfusion studies are used to see cerebrovascular reserve.
Pial synangiosis for treatment of Moyamoya disease is offered in Apollo Hospitals Dhaka. So far the
result has been satisfactory.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
106
ICN-5: Neurofeedback Brain Training (NFBT) Technology
Md Osman Gony
Founder Chairman, Institute of NeuroDevelopment & Research (INDR)
NeuroFeedback (NF) Brain Training is a relatively new treatment option for various
NeuroDevelopmental Disorders like Autism, ADHD etc. where normal development in respect of
brain function is impaired which may results in poor social communication, inappropriate behavior,
attention deficiency etc. NeuroFeedback, a specific form of biofeedback, is based on the idea that
human beings can consciously alter their brain function through training sessions in which they
attempt to change the signal generated by their brain and measured via some neurological feedback
mechanism. By so doing, participants increase cerebral blood flow to a specified region of the brain,
consequently increasing brain activity and performance on tasks involving that region of the brain.
There are mostly two types of popular NF technology in practice now a day. One is EEG NF and
another is HEG (Hemoencephalography) NF. Currently we are using HEG NF at Bangladesh to treat
special child and train their brain to function more optimally.
Hemoencephalography (HEG) was developed by Dr. Hershel Toomim, Near Infrared
Hemoencephalography (nirHEG) measures changes in the local oxygenation level of the blood.
Similar to fMRI, which uses changes in the magnetic properties of blood resulting from oxygenation
to form an image of brain activity, NIR utilizes the changes in blood translucence resulting from
oxygenation to generate a signal that can be consciously manipulated in NF sessions. At the most
basic level, nirHEG shines alternating red (660 nm) and near infra-red (850 nm) light on a specified
area of the brain, usually through the forehead. While the skull is largely translucent to these
wavelengths of light, blood is not. The red light is used as a probe, while the infrared light provides a
relatively stable baseline for comparison. Photoelectric cells in a spectrophotometer device worn on
the forehead measure the amount of each wavelength of light reflected by cerebral blood flow in the
activated cortical tissue and send the data to a computer, which then calculates the ratio of red to
infrared light and translates it into a visual signal of corresponding to oxygenation level on a graphical
interface the patient can see. The key nutrient monitored by NIR is oxygen. In NIR, as the ratio of
oxygenated hemoglobin (HbO2) to deoxygenated hemoglobin (Hb) increases, the blood becomes less
and less translucent and scatters more of the red light, instead of absorbing it. In contrast, the amount
of infrared light scattered by the blood is largely impermeable to changes in the oxygenation level of
hemoglobin.
HEG as NeuroFeedback: Using this above principal, HEG can be used to indirectly measure neural
activity based on neurovascular coupling. Neurovascular coupling is the mechanism by which
cerebral blood flow is matched to metabolic activity. When a region of the cortex is used in a specific
cognitive task, neuronal activity in that region increases, consequently increasing local metabolic rate.
To keep up with the nutritional and waste removal demands of a higher metabolic rate, cerebral blood
flow to the cortical area in use must increase proportionally. Along with the increase in flow,
hemoglobin molecules in the blood, which are responsible for the transport and transference of
oxygen to tissue throughout the body, must increase the amount of oxygen they deliver to the
activated region of the cortex, resulting in a greater local blood oxygenation level. This is also
referred to as the haemodynamic response.
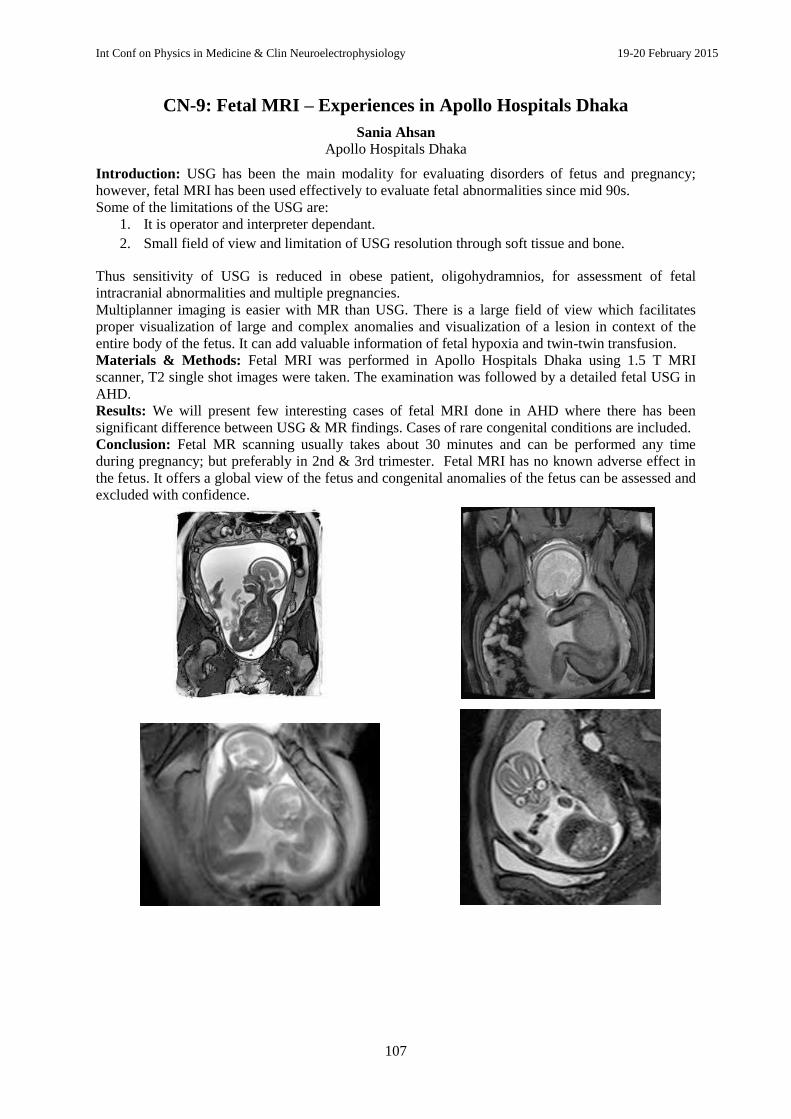
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
107
CN-9: Fetal MRI – Experiences in Apollo Hospitals Dhaka
Sania Ahsan
Apollo Hospitals Dhaka
Introduction: USG has been the main modality for evaluating disorders of fetus and pregnancy;
however, fetal MRI has been used effectively to evaluate fetal abnormalities since mid 90s.
Some of the limitations of the USG are:
1. It is operator and interpreter dependant.
2. Small field of view and limitation of USG resolution through soft tissue and bone.
Thus sensitivity of USG is reduced in obese patient, oligohydramnios, for assessment of fetal
intracranial abnormalities and multiple pregnancies.
Multiplanner imaging is easier with MR than USG. There is a large field of view which facilitates
proper visualization of large and complex anomalies and visualization of a lesion in context of the
entire body of the fetus. It can add valuable information of fetal hypoxia and twin-twin transfusion.
Materials & Methods: Fetal MRI was performed in Apollo Hospitals Dhaka using 1.5 T MRI
scanner, T2 single shot images were taken. The examination was followed by a detailed fetal USG in
AHD.
Results: We will present few interesting cases of fetal MRI done in AHD where there has been
significant difference between USG & MR findings. Cases of rare congenital conditions are included.
Conclusion: Fetal MR scanning usually takes about 30 minutes and can be performed any time
during pregnancy; but preferably in 2nd & 3rd trimester. Fetal MRI has no known adverse effect in
the fetus. It offers a global view of the fetus and congenital anomalies of the fetus can be assessed and
excluded with confidence.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
108
CN-10: Electrmyographic Finding (EMG) in the Children of Spinal
Muscular Atrophy
Mustafa Mahbub, Suraj Chandra Majumder, Mosiul Azam, Selina H. Banu, Naila Z Khan
Introduction: Spinal muscular atrophies (SMA) are the group of disorders, usually but not
invariably inherited as autosomal recessive characters and the basic lesion lies in the anterior horn
cells of the spinal cord. Neurophysiologic investigation ike nerve conduction study and
electromyography (NCV, EMG), may provide important information to come to the conclusive
diagnosis of SMA particulary in a situation where genetic tests are not available. The main objective
of this study is to distinguish between disorders of anterior horn cell, peripheral nerve, and muscle
and to relate neurophysiological abnormality to the clinical context.
Method: Total 11 children were admitted in the neuroscience department of Dhaka Shishu Hospital
from Feb 2010 to Sept. 2012. Consanginity, perinatal insult and important clinical features were
recorded. Serum CPK, EMG, NCV suggested for all and muscle biopsy for selected cases. EMG &
NCV was done in Bangladesh Protibondhi Foundation by trained person.
Result: EMG was performed in 8 of total 11 children. According to the findings of EMG, 4 (50%)
were suggestive of disease of motor neuron, 1 was myogenic disorder, 1 was neurogenic disorder, 2
were normal and 3 were either not done or not found.
Conclusion: In half of the cases EMG findings were in favor of the clinical diagnosis. So it is
necessary to supplement clinical examination by the study of electrical activity in nerve and muscle.
CN-11: Transfer of Technology: Experience in Providing a Short Course
Of Training and Doing EEG Recording in, Tanzania, Ghana and Cox’s
Bazar
Shipra Rani1, Shanta Yesmin
2, Selina H Banu
3
1Senior technologist Clinical Neurophysiology laboratory, Comfort Diagnostic Center, Dhaka
2Technologist Clincial neurophysiology laboratory, Central Hospital and Dhaka Shishu Hospital, Dhaka
3Clinical Neurophysiologist and Child Neurologist, Associate professor, ICH and SSF Hospital, Mirpur, Dhaka
Introduction: Electroencephalography (EEG) is highly sensitive technology. Long time training is
required on equipment and, accessory handling and recording technique, which is one to seven years.
This paper will discuss the experience of dispensing a short intense course and its outcome in recent
time.
Methods: This study was part of prospective neuro-cognitive evaluation study among the children
who had severe malaria eight years ago in Bangladesh, Tanzania and Ghana‖ A selected population
was supposed to have their EEG performed in site to explore any ongoing cerebral dysfunction
including seizure phenomena. According to study protocol, we organized intense training for
technicians and physicians of those particular places. The course included online preliminary training
for 3 months followed by hands on training in Dhaka for 2 wks. Same model of portable equipment
with similar accessories and technique of data collection was used for three countries. The equipment
setting with montages and calibration were done in Dhaka by our team. Experienced technologists
went in site to supervise and facilitate the activities within short period. The EEG data is in the
process of uploading and downloading through google drive and getting ready for re-reviewing in
Dhaka.
The data acquisition in site, transfer to reviewing site went quite smoothly with persistent and very
intense monitoring and involvement of the experienced neurophysiologists, physicists, computer
experts, equipment suppliers and the technologists in this country. We will discuss on the Cox/s
Bazar data.
Result: Targeted population was 226 in Cox‘s Bazar, 203 in Tanzania, 200 in Ghana. Performed
tests number was 222, 203 and 156 in Cox‘s Bazar, Tanzania and Ghana respectively. Among the
total 222, 219 are available for discussion from CB, 5 records had insufficient data and needed a
repeat test. The rest had good quality data for reviewing. The data were first reviewed by the newly
trained pediatricians or neurologists, and later re-reviewed by the experienced neurophysiologist.
About 90% of the records revealed normal recording for the age and state, 8% had epileptiform

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
109
discharges and 4% had non-specific background dysfunction. Those cases were selected for further
evaluation. The only disagreement found in the description of the ongoing background activities.
Conclusion: The short time training on this highly sensitive technique is possible, however, previous
experience i.e., pre-selection of the trainees is important. The trainer‘s experience and coordination
between the trainee and trainers and intense interest and monitoring is needed.
CN-12: Evaluation of The Prolonged EEG and Clinical Correlation in 35
Children
Rafiqa Humaira1, Abu Saleh Musa
2, Khadiza Rahman
3, S.H. Banu
4
Dept of Neuroscience, Bangladesh Institute of Child Health, Dhaka Shishu Hospital,Dhaka
Introduction: Standard routine EEG recording runs for 30 minutes with sleep-wake and other
activation process. Different protocol is practiced in our laboratory for different clinical problems.
Some children need longer sleep recording beyond the routine test period to explore apparently
undetectable cerebral dysfunction. The prolonged EEG (p-EEG) protocol is more effective for certain
cases.
This study targeted reporting the electro-clinical condition of children who had the p-EEG to evaluate
the technique in clinical practice.
Methods: Prolonged EEG (p-EEG) test was organized for selective cases. The cases were selected
based on the child‘s clinical history of 1. Paroxysmal event, or increasing behavioral disorders, and/or
Suspected paroxysmal cerebral dysfunction in ASD, 2. questionable seizure disorder with normal
routine test, 3. Poorly controlled seizures with previous tests showing no abnormality.
Electro-clinical correlation and the final diagnosis and management plan will be discussed.
Result: Since 2010 total 35 p-EEGs were performed, mean age at recording was 7.8 years St
deviation 3.97, clinical problems were behavioral- speech-communication disorders in 17(49%),
non-specific jerking, limb flickering in sleep, eye blinking, staring, transient speech loss, transient
excessive sweating, cyanotic spells with normal routine EEG (R-EEGs) in 14 (40%) and poorly
controlled epilepsy with normal R-EEGs in 4 (11%). Mean duration of EEG data collection was 55
minutes, maximum 3.25 hours. In EEG any form of cerebral dysfunction was identified in 23(66%),
normal in 34%. The electro-clinical correlation in all and change of the management plan in a few
cases will be discussed.
Conclusion: Specialized technique for selected population is very helpful and should be used for
successful management.
CN-13: Role of EEG in Children With Non-Seizure Clinical Problems: an
Electro-Clinical Correlation
Naheed Nabi, Biplob Banergee, Selina H. Banu Introduction: Clinical presentation of continuous or paroxysmal cerebral dysfunctions may be
variable involving single or multiple function domains of children. A large number of children with
non-seizure complaints are referred to the neurophysiology laboratory, for which we have a definite
protocol for data collection and reviewing. This study was performed to describe the cerebral
dysfunctions found in children presenting with non-seizure clinical problems.
Method: We retrospectively reviewed the electroencephalographic criteria and clinical problems of
the children referred for routine EEG during June‘13 to June‘14. Children with history of overt
seizure(s) or epilepsy were excluded. History related to pregnancy, birth and early developmental
milestone, ongoing medical or other therapy are usually kept during r-EEG. We categorized the
clinical problems in a) behavioral problem group, b) speech delay or regression, d) sleep related

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
110
problems (sleep walking, terror, abnormal posturing in sleep), e) somato-sensory problem and fainting
attack. EEG findings were categorized as 1. Epileptiform discharges (focal, multifocal or
generalized), 2. Feature of encephalopathy (generalized, diffused or localized slowing of background
activities, and normal study.
Result: Total 993 EEGs were performed during last 1 year, 263 cases fulfilled the study criteria.
Mean age of the population was 5.4 years. Behavioral, speech, sleep related problem, somato-sensory
and fainting attacks were reported in 54.8%, 18%, 6.8%, 14.4% and 6.1% respectively. Definite
epileptiform discharges were reported in 20% among the total study population and 1.1% had features
of encephallopathy. This study will discuss the electro-clinical correlation.
Conclusion: This study suggests that a careful, optimum EEG data collection and their analysis is
helpful and should be routinely practiced for management of non-seizure clinical problems in
children.
CN-14: Posterior slow waves on eye closure: are they precursors of
epileptiform discharges in certain cases?
Shanta Yesmin, Khaleda Akhter, Selina H Banu
Introduction: Appearance of alpha rhythmic activity over posterior region is the normal findings on
eye closure, which is blocked on eye opening. Unusual finding of very slow waves over the posterior
region produced by eye closure was studied previously. Objective of this study was to evaluate the
posterior slow waves on eye closure and compare with those having other dysfunction, i.e.,
epileptogenic discharges.
Methods: We reviewed the EEG findings of those children having posterior slow waves on eye
closure. The records were performed since 2008 till recently. Children who had febrile seizures only,
febrile seizure plus and febrile seizures with mild comorbidities were included in this study. Children
with definite epileptic seizures, and or with severe comorbidity were excluded. The presenting
complaints were reviewed and correlated with the EEG findings.
Result: Total 70 children were included, male predominance (63%), mean age on the day of
recording was 4.8 years, standard deviation 2.45. Clinical complains were recorded as only febrile
seizure in 13(18.6%), febrile seizure plus in 35(50%) febrile seizure and mild comorbidity in 9(12.9)
and non-seizure problems (behavioral disorder, speech communication problems) in 13(18.6%). In
addition to PSW on eye closure definite epileptogenic discharges were recorded in 27(38.6%). A
significant correlation was found among those with febrile seizure with or without other problem and
EEG showing epileptiform discharges or no discharges.
Conclusion: Posterior slow waves provoked by eye closure, although not proved as definite
abnormality, we propose to consider this finding as an important pre-epileptic indicator. Close
monitoring and repeat EEG should be advised in such cases.
Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
111
CN-15: Video-EEG Data Analysis and Electro-Clinical Correlation
Abdus Salam
Department of Neurology, Shaheed Sheikh Abu Naser Specialized Hospital, Khulna
Introduction: Video-EEG is a very effective diagnostic tool for differentiation of seizure and pseudo-
seizure. Also this is helpful to classify various seizure types. In our institute this investigation has
been introduced since last February. The objective of this study is to evaluate the findings of Video-
EEGs, done over last 09 months since its introduction.
Method: This was a retrospective study. The electro-clinical information of the patients who had their
Video-EEGs performed in our laboratory were collected and reviewed. All patients from February,
2014 to October, 2014 were included in this study. Clinical diagnosis was made by taking the history
meticulously and doing clinical examination by the investigator. Video-EEGs were performed for
various durations, ranging from 30 minutes to 24 hours with a view to capture an event and classify it.
The seizures were classified following the International League against Epilepsy classification (ILAE
1989, 1993). The EEG findings were interpreted accordingly.
Result: Over last 09 months total 25 Video-EEGs have been done. The duration of these V-EEGs
were 30 minutes-24 hours. Age of the patients was 5 month-78 year. Male and female ratio was
12:13. In 14 cases clinical events could be captured. Various types of EEG pathology were found in
21 cases. The final diagnosis was, CPS-T(complex partial seizure-temporal) 7, PS (partial seizure)
with secondary generalization 4, IGE (idiopathic generalized epilepsy) 2, symptomatic generalized
epilepsy 3, childhood absence epilepsy 2, juvenile myoclonic epilepsy1, SSPE (subacute sclerosing
panencephalitis) 1, status epilepticus of Atypical Absence Seizure 1(Lennox Gastaut syndrome),
pseudo-seizure in 3 and seizure + pseudo-seizure 1. After analyzing the data it was seen that EEG was
positive in 96% cases in our study. In 56% cases it was possible to capture an event which provided
conclusive result of the presenting complain.
Conclusion: This result demands wide-spread use of Video-EEG in selected cases by trained experts
for the accurate diagnosis and classification of epilepsy and to differentiate seizures from pseudo-
seizures.
CN-16: Neuroradiology: a Mandatory Subspeciality for Clinicians
Mustafa Mahbub Department of Pediatric Neuroscience; Bangladesh Institute of Child Health (BICH), Dhaka Shishu
(Children‘s) Hospital (DSH), Dhaka E-mail: [email protected]
Introduction: Neuroimaging includes the use of various techniques to either directly or indirectly
image the structure, function/pharmacology of the nervous system. CT scan and MRI are the tool of
choice in the evaluation of brain pathology and particular attention is devoted to the role of diffusion-
weighted imaging and magnetic resonance spectroscopy. To observe the clinical diagnosis and
neuroimaging findings of children admitted with neurological problems is the main objective of this
study.
Materials and method: A retrospective analysis of 40 children from the records of the patients
admitted in the Child Neurology Unit, Dhaka Shishu Hospital during the period of November,2013
and December, 2014. Either CT scan or MRI of the brain was done in all 40 children.
Result : Neuroimaging finding showed encephalomalacia in 9, cortical atrophy in 8, demyelination
in 5 and normal finding in 4 children. Among these 40 children 12 was diagnosed as cerebral palsy of
different types, 9 was diagnosed as sequel of encephalitis , 7 diagnosed as seizure with developmental
delay and 4 as neurometabolic disorder.
Conclusion: Neuroimaging plays an important and growing role in the diagnosis and therapeutic
management of pediatric neurology disorders.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
112
Invited Talk
ICN-6: Learning Kit for Children with Special Needs: The RGACD
Learning Kit
Kazi Tanvir Ahmmed1, Md Rabiul Hossain
2, Kazi Abu Zubair
2, Bhuiyan Muhammad
Muktashif Anwar2, Sopan Sarkar
2, A.M. Mahmud Chowdhury
2, Sakibul Azam
2,
Mahmood Ahmed Chowdhury3
Department of Applied Physics, Electronics and Communication Engineering, University of Chittagong,
Bangladesh.
Department of Applied Physics, Electronics and Communication Engineering, University of Chittagong
Professor, Department of Child health, Chattagram Ma O Shishu Hospital Medical College, Chittagong.
Background: We, the Research Group to Aid Child Development (RGACD), are working in the
vein of converging various sides of medical and physical sciences. Here, we present a Microcontroller
based learning system, which has been named ―The RGACD Learning Kit‖.
Methods: It is a Microcontroller and Infrared sensor based unique portable, a plug and play styled
learning tool mainly targeted towards children with special needs to aid their physical and mental
development. The kit is equipped with 3-D models of everyday objects and other common
surroundings. Based on the response of the user it will show various knowledgeable videos about the
objects on a connected screen or Personal Computer. The kit has been made to be highly
interactive by introducing two modes: a) Learning mode- where the user picks a random object
and learns about it. b) Teaching mode- Where the kit‘s system randomly generates an object‘s
name in the screen and prompts the user to pick it up. If the wrong one is picked up, it will
inform the user that it is wrong and if the user is right he/she will be applauded by the kit‘s
system and the corresponding video will start to run.
An advantage of this system is that the code architecture has been made in such a way that
videos can be added or replaced easily. It can be updated to suit any culture by replacing or
adding videos too. The learning kit currently features various categories such as animals, shapes
etc. The interface and the videos of the kit are developed specially considering children with
visual, speech and hearing impairment. The videos contain text which helps children with hearing
impairment to get a clear hold of the object shown. It also helps the children with speech
difficulties by increasing their vocabulary with related pictures. The interface is colorful with bigger
fonts. The videos are also colorful, clear and attractive to children. Children with Autism are visual
learners and this kit helps to increase their cognition as well as communication level. As the kit is
equipped with 3-D models of various objects it helps the development of fine and gross motors of
the children. The children with visual impairment get proper orientation with the shapes of
everyday object and surroundings without even seeing them properly by holding the 3-D model
of an object and by hearing the essential information given about the objects in the videos. The
learning kit‘s functions were deliberately made easy so that it can be easily accessible for
children of every kind and the two modes of the kit are developed for enhancing the
development of the child‘s mind.
Results & Observations: The kit was tested on both children with special needs and normal
children. The kit has been successful in the primary stages. Our primary survey on doctors,
therapists and psychologists shows highly positive reactions. We are working on to extend the
scope of the survey by including parents and take data from various categories of children. Then
we will measure the efficiency of the system by comparing the children‘s development of mind
before and after using the kit.
Conclusions: In countries like Bangladesh where schools for children with special needs are
scarce our kit is of great help for their development. This kit is being used in a child development
center by speech, vision and hearing therapists successfully by making their work easier than
before. The kit can be used in home as well as schools. Currently, the kit‘s interface and videos
are all in Bengali language and the contents are mostly part of Bangladeshi culture. The kit is
cheap in price and it is ideal for developing and underdeveloped countries.
Acknowledgement: We acknowledge the Child Development Center of Chittagong Ma O Shishu
Hospital for financing and co-operation with our work on the kit.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
113
CN-17: Can Early Detection of Predictors of Poor Seizure Outcomes
Change the Course of Neurodevelopement?
Shayla Imam Kanta, Humaira Rafiqua Qaderi and Naila Z Khan
Introduction: In a previous study in Bangladesh Banu et al (2003) showed three factors, i.e., multiple
seizure types, cognitive deficits and abnormal EEGs, to be predictors of poor seizure remission.
Another study by Banu et al (2010) included motor disability as another clinical predictor. Both these
studies provide important indicators for multidisciplinary services as part of an epilepsy programme.
Objective of this study is to determine the early identification of known predictors of poor seizure
outcome influence the course of the seizures and of neurodevelopemental outcomes.
Methods: Children attending the Child Development Center, i.e., a multidisciplinary service, in
Dhaka Shishu Hospital < 2 years of age at first attendance to the Epilepsy Clinic between 2010-2012
with follow-up records including EEGs, were included. Initial seizure semiology, EEG findings,
neurodevelopemental profiles were compared with last follows up.
Results: Total 45 children were included. Among them 60% were male and 40% were female; 70%
had eventful birth history & 30% uneventful. EEG test revealed normal findings in 23.8%,
generalized epileptiform discharges with normal background 9.5%, multifocal epileptiform discharge
in 9.5%, focal epileptiform discharge in 38.1%, epilepticencephalopathy in 14.3%, encephalopathy in
4.8%. Seizure semiology was analysed in detail, neurodevelopemental deficits were graded in mild,
moderate and sever degrees and compared with the follow up records. Seizure criteria at the initial
and last follow up records were compared toeavaluate the poor predictive factors.
Conclusion: Identification of poor seizure outcome predictors at initial stage was helpful and
important for the immediate and long-term treatment plan in childhood epilepsy. Those with
poor predictor would need regular stimulation and follow up at the epilepsy clinic for better
neurodevelopemental outcome.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
114
CN-18: NeuroFeedback Brain Training (NFBT) Technology for ADHD in
Bangladesh: Single Case Study
Md Osman Gony
Founder Chairman, Institute of NeuroDevelopment & Research (INDR)
A Case Study: Our study subject was a seven years old child with severe symptom of ADHD. We
used pretest post test design to conduct the study. We conducted 20 HEG NF sessions, 3 sessions a
week. Specific custom designed software was used to analyze and project real-time brain activity on
dual screen.
Most frequently observed symptoms (all scored 7) with him were angry, compulsive behavior,
confused thinking, hyperactive, impatient, impulsive and inattentive. After twenty session of NFBT,
his symptoms were scored as follows: Angry (1), Compulsive Behavior (1), Confused Thinking (2),
Hyperactive (2), Impatient (2), Impulsive (1), Inattentive (2). [Progress graph is shown below]
As we can see from our result, NFBT induced marked improvement on our subject's manifesting
behavior. Even though the child got 20 sessions, the result is persistent still now.
Conclusion: NeuroFeedback can be answer to many Child‘s learning disability due to
NeuroDevelopmental Disorders like Autism, ADHD, CP etc. by training their brain. At least we now
can say, we do have a tool to train their brain which we can monitor real time and see changes
objectively.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
115
CN-19: Identification of Cognitive States based on Transcranial Doppler
Ultrasonography
Eshtiak Ahmed1, Ashraful Islam
1, Jie Lu
2, Khondaker A. Mamun
3
1Dept. Of CSE, Ahsanullah University of Science and Technology, Bangladesh,
2IBBME, University of Toronto, Canada,
3Dept. of CSE, United International University, Bangladesh
Introduction: Individuals, having cognitive awareness but severe motor disorders like muscular dystrophy
or spinal cord injuries face difficulties to communicate with their surroundings. In order to shorten this
communication gap, Brain-machine Interface (BMI) is an inspiring technique that allows the users to
communicate through their brain activities. Among the number of different modalities for BMI,
Transcranial Doppler Ultrasonography (TCD) has sparked great interest as a potential modality because it
is affordable and robust against environmental noises[1]. TCD is a non-invasive ultrasound technology that
can be able to identify the changes in cerebral blood flow velocity (CBFV) in the middle cerebral artery
(MCA) of human brain.
Methods: Five able-bodied participants with normal vision were recruited. A Multi-Dop X4 TCD unit and
dual 2 MHz ultrasonic transducers were placed over the left and right transtemporal windows to acquire
the blood flow velocity in the MCA. The probes were positioned over the transtemporal insonation
window with the established insonation procedure (Fig. 1) [2].
Fig. 1: Axial view of the ultrasound probe set Fig. 2: Visual cues for the activation (left)
at the transtemporal insonation window and the rest mental task (right)
Participants were asked to perform two tasks which are activation and rest task. For the activation task,
participants repetitively rehearsed the spelling of a word that visually cued while imagining writing it (Fig.
2). During the rest task, an hourglass was presented for visual tracking (Fig. 2). The CBFV was measured
and the Doppler spectra of blood flow were acquired. Total 44 features were extracted and among them 3
highly discriminative features were selected by Fisher Criterion. A Naïve Bayes classifier was evaluated
using selected features with 10-fold cross-validation for classification between rest and activation tasks.
Results: Classification results for identifying rest and activation tasks show an average accuracy,
specificity (rest) and sensitivity (activation) of 77.13± 1.5%, 74.75± 5.23% and 79.5± 4.63% respectively.
It is also noted that all participants attained more than 70% accuracy. The achieved results are very much
encouraging for further study and it also has scopes of substantial future improvements.
Conclusion: The accuracy achieved for identifying cognitive states using TCD is inspiring for future
studies. Also, the accuracies may increase as the participants get more familiar with experimental tasks and
instruments. The study can be cited as a success in differentiating activation and rest mental tasks in
human brain and opens doors to develop TCD based BMI for rehabilitations.
Acknowledgements: The authors are grateful to Prof. Tom Chau and PRISM lab for datasets and advices.
Reference: [1] A. J. B. Myrden, A. Kushki, E. Sejdić, A.-M. Guerguerian, and T. Chau, ―A brain-computer interface based
on bilateral transcranial Doppler ultrasound.,‖ PLoS One, vol. 6, no. 9, p. e24170, Jan. 2011.
[2] A. V Alexandrov, M. A. Sloan, L. K. S. Wong, C. Douville, A. Y. Razumovsky, W. J. Koroshetz, M. Kaps,
and C. H. Tegeler, ―Practice standards for transcranial Doppler ultrasound: part I--test performance.,‖ J.
Neuroimaging, vol. 17, no. 1, pp. 11–18, 2007.

Int Conf on Physics in Medicine & Clin Neuroelectrophysiology 19-20 February 2015
116
CN-20: Fundamentals of PET-CT (Positron Emission Tomography-
Computed Tomography) and it’s Application in Oncology
Md. Mehedi Masud
Department of Nuclear Medicine, United Hospital Ltd., Dhaka.
Introduction: The purpose was to demonstrate fundamentals of PET-CT (Positron Emission
Tomography) and its application in Oncology. PET-CT imaging is an important sophisticated nuclear
medicine technique to reveal organ energy metabolism in vivo in human as to contribute in the
Oncology (recent clinical application). PET-CT with administration of certain radiopharmaceutical
drug (18
FDG, fluorodeoxyglucose) to cancer patients would reveal the extent of disease process and
therapeutic plan for Oncologists.
Method: 18
F, a widely used radioisotope with physical half-life of 110 min is made by several nuclear
reactions. The nuclear reaction of 18
O (p, n) 18
F is often used by using enriched 18
O water. Fluorinated
deoxyglucose (18
FDG), an analogue of glucose with 18
F at 2nd
position of it‘s benzene ring has been
established as a tracer for glucose metabolism. 18
FDG is trapped metabolically in cells after being
administered intravenously into the body, and can be substantially used for evaluating functional
anatomy in vivo. 18
FDG and PET-CT imaging is used in assessing malignant lesions and staging-
restaging for therapeutic plan by inducing analytical procedure. Different malignant lesions of soft
tissue, haematological and skeletal organs are investigated.
Result & Discussion: An example of 18
FDG and PET-CT application to malignant lymphoma patient
was shown cervical lymphadenopathy with severe involvement of musculoskeletal system from
whole-body imaging for appropriate therapeutic plan (both chemo-radiotherapy and interval therapy).
Conclusion: 18
FDG and PET-CT imaging is sophisticated nuclear medicine technique in assessing
oncological diagnosis, staging/restaging and therapy plan.

117
List of Presenters:
Name E-mail Address
Abir, Raihan [email protected]
Ahmad, Maruf [email protected]
Ahmed, Sayed Parvez [email protected]
Ahmed, Zisun [email protected]
Ahmmed, Kazi Tanvir
Ahsan, Sania [email protected]
Akhanda, Sabbir [email protected]
Akhter, Khaleda
Ali, Mohammad Hanif [email protected]
Anwar, Bhuiyan Md.Muktashif
Azam, Mosiul
Azam, Sakibul
Azim, Mohammad Anwar-Ul [email protected]
Bala, Mousumi [email protected]
Banergee, Biplob
Banu, Selina H. [email protected]
Barkat, Zubair [email protected]
Begum, A. [email protected]
Bhuiyan, Md Anisuzzman [email protected]
Chowdhury, A.M. Mahmud
Chowdhury, Ehsan Alam [email protected]
Chowdhury, Mahmud Ahmed
Dey, Hirak Kumar [email protected]
Gony, Md.Osman
Hassan, Mahmud [email protected]
Hernández, Erick [email protected]
Hossain, Md. Nahid [email protected]
Hossain, Md.Rabiul
Humaira, Rafiqa
Hussain, K M A [email protected]
Hussain, Md. Kamrul [email protected]
Hussain, Rezwan bin [email protected],
Islam, Ariful [email protected]
Islam, Shekh Md Mahmudul [email protected]
Kadir, Muhammad Abdul [email protected]
Kadir, Nazimul [email protected]
Kanta, Shayla Imam
Khan, Naila Z
Khan, R.K. [email protected]
Kiber, Md. Adnan [email protected]
Mahbub, Mustafa [email protected]
Mahbub, Zaid Bin [email protected]

118
Name E-mail Address
Majumder, Suraj Chandra
Malik, Sadiq R. [email protected]
Mamun, Khondaker Abdullah [email protected]
Masud, Md.Mehedi
Mollah, Abdus Satta [email protected]
Monika, A. N. [email protected]
Musa, Abu Saleh
Nabi, Naheed
Nahar, Meherun [email protected]
Nisa, Lutfun [email protected]
Qaderi, Humaira Rafiqua
Quadir, Kamila Afroj [email protected]
Rabbani, Khondkar [email protected]
Rahman, Khadiza
Rahman, M Obaidur [email protected]
Rahman, M.S. [email protected]
Rahman, Md. Shakilur [email protected]
Rana, Muhammad Masud [email protected]
Rani, Shipra
Roksana, Ismat Ara [email protected]
Roshid, Md. Harun Or [email protected]
Sabur, M.A. [email protected]
Salam, Abdus [email protected]
Salam, Abdus [email protected]
Sarker, Sopan
Shahidunnahar, Sumana [email protected]
Sharmin, M.N. [email protected]
Siraz, M.M.M. [email protected]
Sultana, Nasreen [email protected]
Talukder, Mohammad Abu Yousuf [email protected]
Uddin, Md. Jamal [email protected]
Yasmeen,Shanta
Yeasmin, Selina [email protected]
Yousuf, Abu [email protected]
Zerin, Tasnim [email protected]
Zubair, Kazi Abu
119
A Brief Introduction to the Organizing Bodies
Bangladesh Medical Physics Association (BMPA)
Website: <www.bmpaweb.org>
Understanding the importance of Medical Physics in the modern healthcare a conference was
organized at the Bangladesh University of Engineering & Technology (BUET) in 1996 at the
initiatives of Professor Gias Uddin Ahmed, then at BUET, Dr. Syed Reza Hussain Ex Director,
Institute of Nuclear Medicine, Bangladesh Atomic Energy Commission (BAEC), Dr. A Sattar Mollah
of BAEC, Dr. M A Hai, Ex. Director of National Cancer Hospital, and an expatriate Bangladeshi in
Germany, Dr. G A Zakaria. This initiative was supported by Professor Uri Quest and Professor Hover
from Heidelberg University, Germany, and through a resolution in a meeting held during that
Conference, Bangladesh Medical Physics Association (BMPA) was born. Professor Gias Uddin
Ahmed, presently Vice Chancellor of the Primeasia University, was elected the first President of
BMPA, and Dr. Sattar Mollah as the first General Secretary. Through this leadership, continuing till
2009, the executive committee organized several International Conferences and Seminars, published a
scientific Journal with the name ‗Bangladesh Journal of Medical Physics‘, and got BMPA recognized
as the representative National member of International Organisation of Medical Physics (IOMP) and
Asia-Oceania Federation of Organizations for Medical Physics (AFOMP). BMPA also actively
supported a proposal to the Government by the National Institute of Cancer Research & Hospital in
creating 64 posts of Medical Physicists in all major hospitals. However, this still remains to be
addressed. In 2010 a new Executive Committee was formed with Professor K Siddique-e Rabbani as
its President and he is still continuing, at the request of the members. This Committee has been
continuing publication of the journal each year since 2011, which has recently been made online and
open source. Through this conference, the Association hopes to go forward in the mission with which
it was initiated.
Bangladesh Clinical Neuroelectrophysiologist Society
(BCNEPS)
BCNEPS was registered on 23
rd November, 2009. It started its regular activities in 2006 with aim to
produce recognized, well formatted training protocol and to establish a platform for the experts, i.e.,
technologists, physicists, biotechnical engineers and the clinical neurophysiologists of the country.
Clinical neurophysiology includes a) EEG (electro encephalography), that measures cerebral electrical
activity and currently the only available clinical laboratory test of brain physiology, b) NCS (nerve
conduction study) and EMG (electromyography) that measures the electrical activities of peripheral
nerves and muscle action potentials and c) SEPs (sensory evoked potential) to test the integrity of the
sensory pathway.
Through our society we provide training to technicians, physicians and set up electrophysiology labs
in different health facilities. We have monthly teaching classes for the society members and we share
knowledge and recent advancements. Our society has trained technicians and physicians from other
countries. We arrange short workshops for young doctors.

120
Department of Biomedical Physics & Technology
University of Dhaka
Website: <www.bmpt.du.ac.bd>
This multidisciplinary post graduate department started its journey with Professor K Siddique-e
Rabbani joining as its first Chairperson on 3 November, 2008. This department, emphasizing R&D at
Ph.D. and M.Phil levels, stands on 30 years of work carried out by the group while in the Department
of Physics, the mother department. There, late Professor M Shamsul Islam initiated and organized
research and education programmes in Biophysics and Medical Physics, visualising their far reaching
importance in 1978. A ten-year academic link with Universities in UK under a British ODA
sponsorship later gave a significant boost to these activities.
About 80% of Global population living in the Third World is deprived of the benefits of modern
healthcare technology, and this failure forms the key motivation of this department‘s research
programmes. This group has already achieved significant innovations in several areas: i) A novel
Focused Impedance Method (FIM) with potential in the detection and diagnosis of disorders and
diseases. This idea has received international acclaim and Universities in UK and Korea have already
started working in FIM, ii) Distribution of F-latency (DFL), a new physiological parameter giving a
velocity profile of motor nerves, having potential in the detection and diagnosis of peripheral
neuropathy. Researchers in UK and Singapore have already started working on this innovation. iii)
Design and development of low cost medical instruments for dissemination in the Third World
including telemedicine, and finally iv) Destruction of diarrhoeal germs in water at low cost by solar
energy using simple and easily available materials, which also provides an indirect means of solving
the Arsenic problem.
The department takes in students from all branches of science, engineering and medicine for its PhD
and MPhil programmes, and has already created an excitement among young scientists. At present 9
students are working for PhD and 2 for MPhil degrees. The department has initiated Masters courses
recently. The third batch has recently started and 27 students joined, 12 for specialization in Medical
Physics and 15 in Biomedical Engineering. Of course only students with backgrounds in Physics,
Applied Physics, Electrical and Electronic Engineering, Mechatronics and Biomedical Physics and/or
Engineering are taken in for the Masters course.
Through creation of a research environment that targets the needs of the deprived human beings in the
low resource countries, the department has been able to attract talented young researchers and has
already made its name known in the international arena. The department has already started to deliver
the results of its research to real life and hopes to add newer devices and techniques with further
research activities.