south africa: mental health care plan
TRANSCRIPT

1
South Africa: Mental Health Care Plan
1. Summary Table of Mental Health Care Packages
2. Detailed description of packages.
3. Table of indicators
4. Toc map (Separate Attachment)
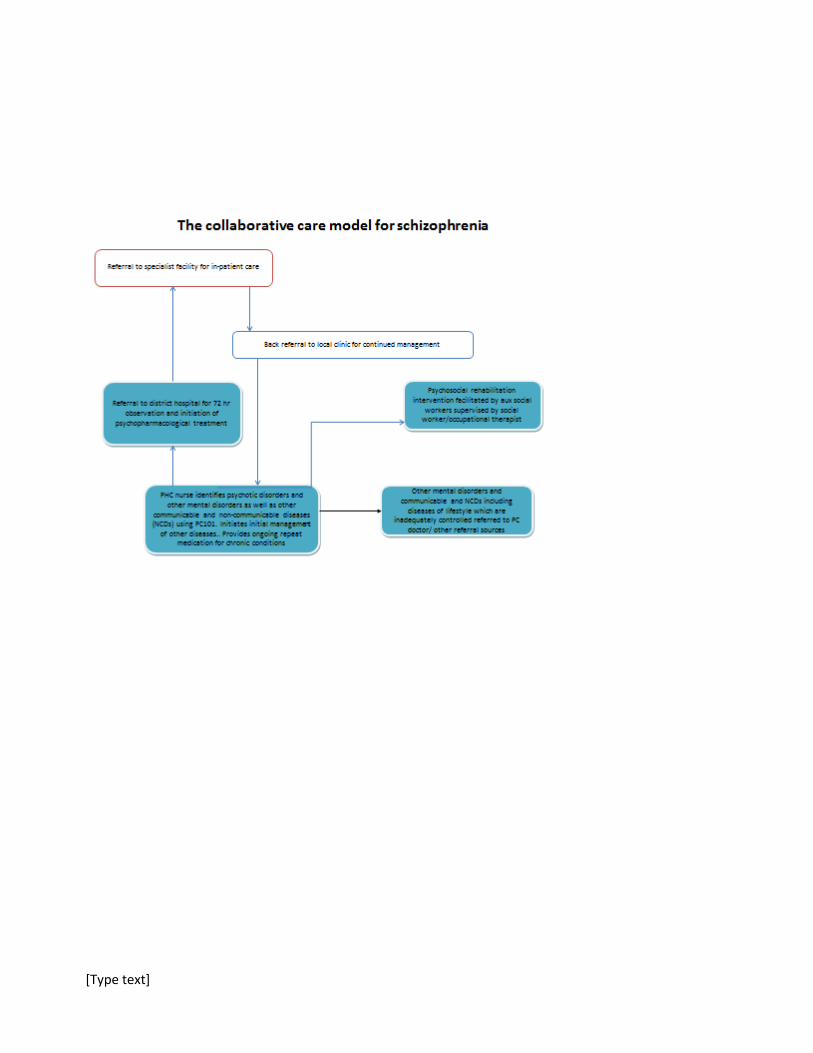
5. Collaborative care models for depression, alcohol misuse and schizophrenia
6. Framework for district mental health care within the re-engineered PHC service delivery platform in Dr Kenneth Kaunda District, NW
7. Table of human resource mix, services provided and tools available to assist in the provision of services
2
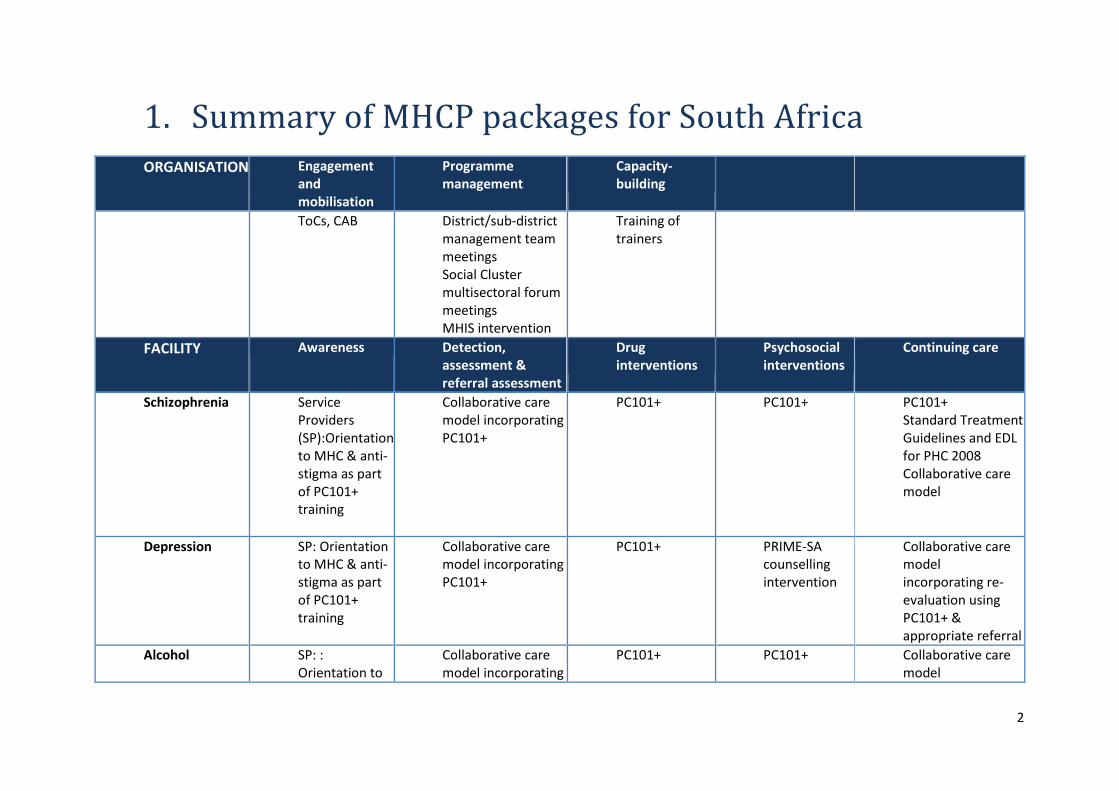
1. Summary of MHCP packages for South Africa
ORGANISATION Engagement and mobilisation
Programme management
Capacity-building
ToCs, CAB District/sub-district management team meetings Social Cluster multisectoral forum meetings MHIS intervention
Training of trainers
FACILITY Awareness Detection, assessment & referral assessment
Drug interventions
Psychosocial interventions
Continuing care
Schizophrenia Service Providers (SP):Orientation to MHC & anti-stigma as part of PC101+ training
Collaborative care model incorporating PC101+
PC101+ PC101+ PC101+ Standard Treatment Guidelines and EDL for PHC 2008 Collaborative care model
Depression SP: Orientation to MHC & anti-stigma as part of PC101+ training
Collaborative care model incorporating PC101+
PC101+ PRIME-SA counselling intervention
Collaborative care model incorporating re-evaluation using PC101+ & appropriate referral
Alcohol SP: : Orientation to
Collaborative care model incorporating
PC101+ PC101+ Collaborative care model

3
MHC & anti-stigma as part of PC101+ training
PC101+ incorporating re-evaluation using PC101+ & appropriate referral
COMMUNITY Awareness Case detection of SMD
Rehabilitation and recovery
User mobilisation
Outreach / adherence support
Psychosis 2nd phase DoH training of CCGs
2nd phase DoH training of CCGs Training of Traditional/faith healers/other lay community counsellors
Manualized community-based PRIME-SA psychosocial rehab (PSR) groups
Recovered service users will be trained as community care worker facilitators of the PSR groups
2nd phase DoH training for CCGs
Depression 2nd phase DoH training of CCGs
2nd phase DoH training of CCGs Training of Traditional/faith healers/other lay community counsellors
Alcohol 2nd phase DoH training of CCGs
2nd phase DoH training of CCGs Training of Traditional/faith healers/other lay community counsellors
4

[Type text]
2. Description of Packages
1.
Organizational Packages
1.1 Engagement & Advocacy Rationale Mental Health care receives some priority but inadequate funding
and prioritisation of other diseases translates into mental health being sidelined at some levels.
Goal and objectives
Sensitise service providers about integrating mental health packages into PC101
Provider PRIME-SA and DoH
Content TOC workshop; engagement with relevant stakeholders at national, provincial and district levels (Mental Health and Substance Abuse) within department and at community level
Source TOC; Advisory Group (CAB) Indicators Input indicators:
a) Costs of meetings / human resource time(CasStu: Res) Process indicators:
b) Number of ToC workshops / CAB meetings c) Participation in meetings [ __% of staff & community members
expected to participate who do participate in ___% of meetings.] (CasStu: DocRev, ToC)
Output indicators: d) No of staff & community representativesreached through this
engagement e) No of MH specialists aware of new system
configuration/diversification of roles (CasStu: Surv) f) No of PHC providers aware of new system and inclusion of
MHC as part of their roles g) Heightened awareness of the importance of the provision of
mental health care in PHC & reduced stigma (CasSt: Qual)
Outcome indicators: h) Increase in resources available to mental health (CasStu: Surv)

[Type text]
1.2
Programme Management 1.2.1 Development & approval of MHCP Rationale It is necessary to have a district MHCP adopted by the District DoH to
ensure implementation
Goal To have the MHCP adopted by the district/sub-district management Content ToC meetings
Provider DoH& PRIME-SA Source TOC workshop; engagement with relevant stakeholders at national,
provincial and district levels (Mental Health and Substance Abuse) within department and at community level
Supervision N/A Maternal Mental Health
N/A
Indicator Input indicators: a) Costs/humanresource costs associated with development of
MHCP(CasStu: Res) Process indicators:
a) ToC meetings leading to the development of the MHCP (CasStu: DocRev)
Output indicators: a) MHCP finalised b) Operational Guidelines finalised(CasStu: DocRev)
Outcome indicators: a) MHCP approved b) Operational Guidelines approved (CasStu: DocRev) c) Evidence of resource mobilisation for sustainability /
expansion of services (CasStu: Res)
1.2.2
Ongoing District/sub-district management of the implementation of the MHCP
Goal To plan, manage, monitor and evaluate the district/sub-district mental health services in conjunction with other programmes on an on-going basis
Content Management team meetings
Provider Chronic care coordinators Mental health coordinators PHC co-ordinators District/sub-district Information officer District/sub-district pharmacist Assistant Director for Community Health Services District/sub-district managers
Source District/sub-district management team meetings District Mental Health Plan
[Type text]
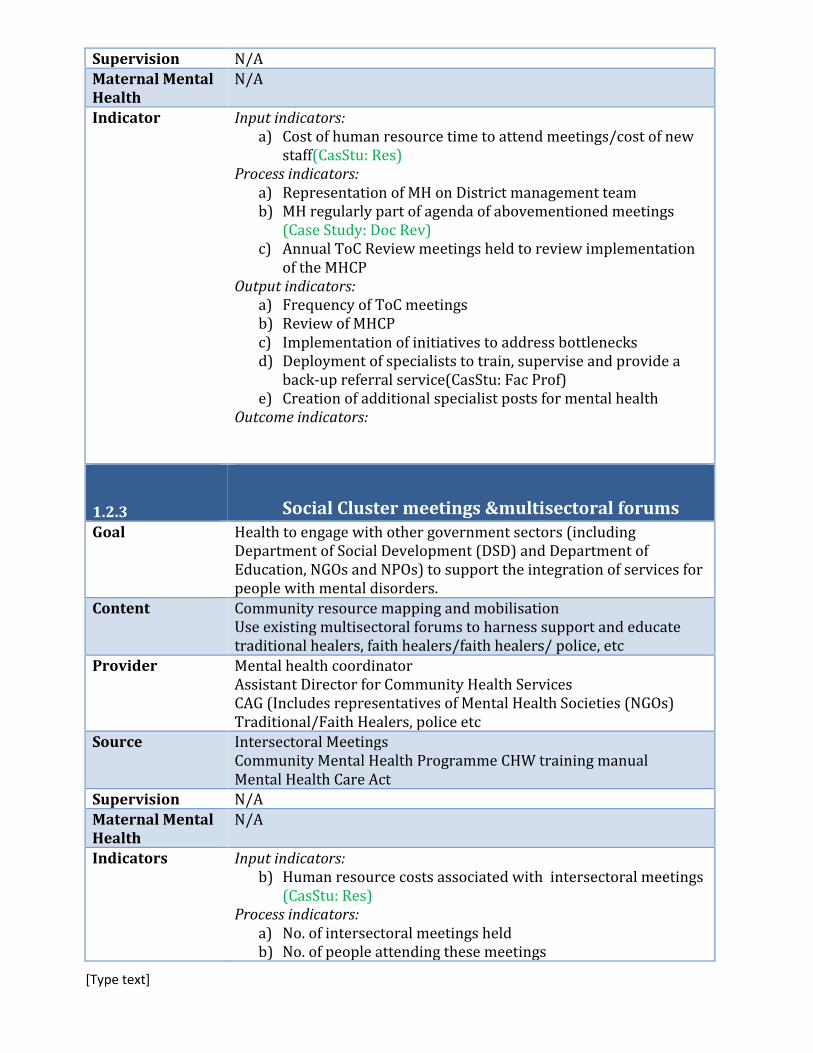
Supervision N/A
Maternal Mental Health
N/A
Indicator Input indicators: a) Cost of human resource time to attend meetings/cost of new
staff(CasStu: Res) Process indicators:
a) Representation of MH on District management team b) MH regularly part of agenda of abovementioned meetings
(Case Study: Doc Rev) c) Annual ToC Review meetings held to review implementation
of the MHCP Output indicators:
a) Frequency of ToC meetings b) Review of MHCP c) Implementation of initiatives to address bottlenecks d) Deployment of specialists to train, supervise and provide a
back-up referral service(CasStu: Fac Prof) e) Creation of additional specialist posts for mental health
Outcome indicators:
1.2.3 Social Cluster meetings &multisectoral forums Goal Health to engage with other government sectors (including
Department of Social Development (DSD) and Department of Education, NGOs and NPOs) to support the integration of services for people with mental disorders.
Content Community resource mapping and mobilisation Use existing multisectoral forums to harness support and educate traditional healers, faith healers/faith healers/ police, etc
Provider Mental health coordinator Assistant Director for Community Health Services CAG (Includes representatives of Mental Health Societies (NGOs) Traditional/Faith Healers, police etc
Source Intersectoral Meetings Community Mental Health Programme CHW training manual Mental Health Care Act
Supervision N/A
Maternal Mental Health
N/A
Indicators Input indicators: b) Human resource costs associated with intersectoral meetings
(CasStu: Res) Process indicators:
a) No. of intersectoral meetings held b) No. of people attending these meetings
[Type text]
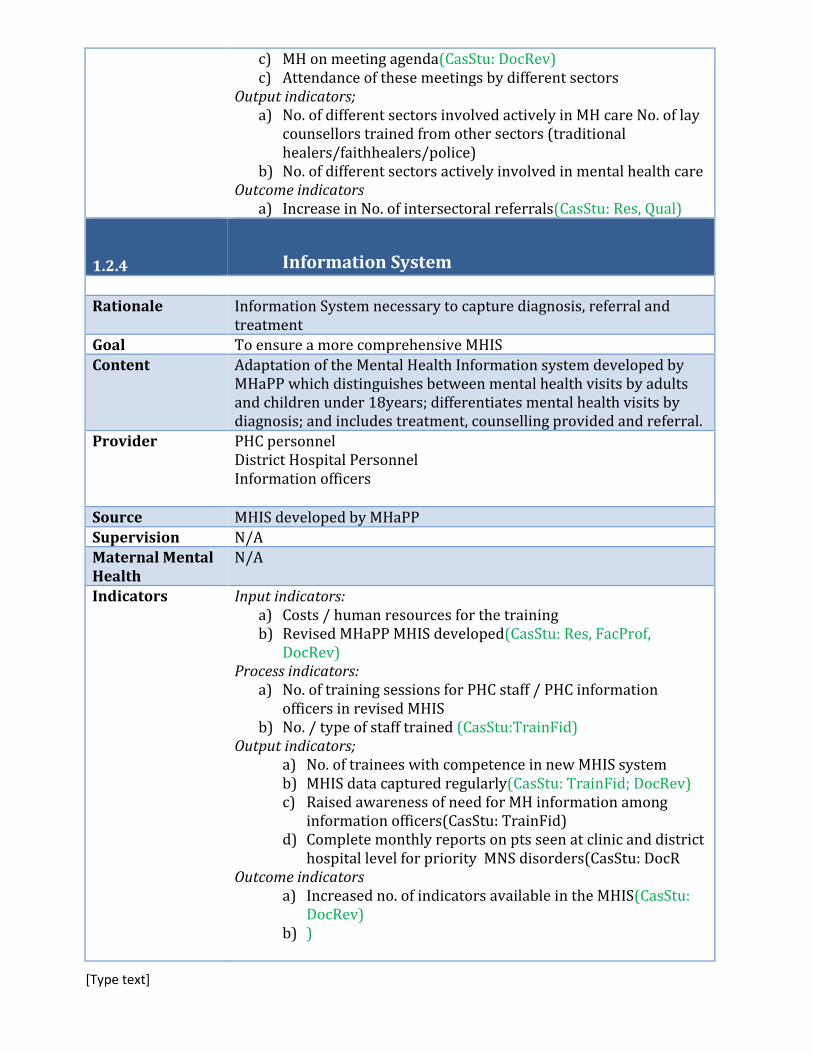
c) MH on meeting agenda(CasStu: DocRev) c) Attendance of these meetings by different sectors
Output indicators; a) No. of different sectors involved actively in MH care No. of lay
counsellors trained from other sectors (traditional healers/faithhealers/police)
b) No. of different sectors actively involved in mental health care Outcome indicators
a) Increase in No. of intersectoral referrals(CasStu: Res, Qual)
1.2.4 Information System Rationale Information System necessary to capture diagnosis, referral and
treatment
Goal To ensure a more comprehensive MHIS
Content Adaptation of the Mental Health Information system developed by MHaPP which distinguishes between mental health visits by adults and children under 18years; differentiates mental health visits by diagnosis; and includes treatment, counselling provided and referral.
Provider PHC personnel District Hospital Personnel Information officers
Source MHIS developed by MHaPP
Supervision N/A Maternal Mental Health
N/A
Indicators Input indicators: a) Costs / human resources for the training b) Revised MHaPP MHIS developed(CasStu: Res, FacProf,
DocRev) Process indicators:
a) No. of training sessions for PHC staff / PHC information officers in revised MHIS
b) No. / type of staff trained (CasStu:TrainFid) c) Output indicators;
a) No. of trainees with competence in new MHIS system b) MHIS data captured regularly(CasStu: TrainFid; DocRev) c) Raised awareness of need for MH information among
information officers(CasStu: TrainFid) d) Complete monthly reports on pts seen at clinic and district
hospital level for priority MNS disorders(CasStu: DocR Outcome indicators
a) Increased no. of indicators available in the MHIS(CasStu: DocRev)
b) )

[Type text]
1.2.5 Capacity Building Motivation There is a need to build capacity within the district to provide
ongoing training and supervision for task sharing interventions at the PHC Facility and Community levels of care
Goal To build capacity within the district to provide training and supervision to the PHC Facility and Community levels.
Content Training of district trainers & specialists to provide training Provision of manuals and support materials for training and supervision
Provider UCT Lung Institute PRIME SA National Department of Health
Source PC 101 PRIME counselling manuals for lay counsellors Community Mental Health Programme Manual for CHWs 1st& 2nd Phase of DoH training package for Community Caregivers Supervision guidelines
Supervision N/A
Maternal Mental Health
N/A
Indicators Input indicators: a) Costs and human resources to conduct ToT in training /
supervision(CasStu: Res) b) Availability of training manuals (CasStu:Surv)
Process indicators: a) No. of ToT courses run b) No. of trainers / specialists on the courses(CasStu:TrainFid)
Output indicators a) % of district trainers who are trained(CasStu:TrainFid) b) Adequacy of ToT training
Outcome indicators a) Competency of trainers to train (improved knowledge / skills
to conduct training / supportive supervision of PHC workers)(CasStu:TrainFid)
1.2.6 Supervision & support Motivation There is a need to ensure adequate clinical supervision is in place
Goal To build mechanisms to ensure supervision and support for general HCWs ongoing monitoring and evaluation of the MHCP.
Content Supervision tools Annual ToC review meetings
Provider PRIME SA National Department of Health

[Type text]
Source Supervision guidelines Supervision tools
Supervision N/A
Maternal Mental Health
N/A
Indicators Input indicators: a) Costs and human resources required for supervision (CasStu:
Res) b) Supervision tools (CasStu:Surv)
Process indicators: a) Supervision tools employed (CasStu:DocRev)
Output indicators a) Frequency of facility supervisions (CasStu- Fac Prof)
Outcome indicators
a) Structured supervision process in place and adequate supervision provided(CasStu: Surv; DocRev)

[Type text]
2. Primary Health Facility Packages for HIV+ and ante-natal/post-natal clinic population
2.1 Awareness 2.1.1 Service provider awareness Rationale Some negative attitudes from service providers towards treating people
with mental disorders exist at PHC level as well as inadequate education about mental disorders and appropriate interventions. These need to be changed.
Goal and objective
a) To increase sensitisation about the need to provide mental health care as part of comprehensive PHC
b) To reduce stigmatizing attitudes that facility staff may have towards people with mental disorders
Provider PHC doctors PHC nurses (Includes all levels) HIV Counsellors
Content and activities (components)
Enhanced PC101 training which will include an orientation to mental health care
Source and tools
PC101 training
Training required
PC101 training – 2 days
Supervision Existing PHC Supervisory structures Mental Health Co-ordinators
Maternal mental health
Enhanced PC101 to promote awareness of maternal depression
Indicator Input indicators a) Costs/human resources for training(CasStu: Res)
Process indicators

[Type text]
a) No. of PHC nurses/MH counsellors attending PC 101 training(CasStu:TrainFid)
Output indicators a) No. of PHC workers trained/ exposed to awareness training
materials(CasStu:TrainFid) Outcome indicators
a) Change in KAB in PHC staff over time (FacSur) b) Improved provider-patient interaction/ satisfaction by service
users(CasStu:Qual)
2.1.2 Service user awareness Goal and objectives
To sensitise service users about mental health and increase demand for services
Provider Health promoters, HIV Counsellors Primary Health Care nurses
Content and activities
Exposure to educational material on waiting room TVs Pamphlets
Source and tools
South African Mental Health Federation Perinatal Mental Health Project
Training required
Supervision Mental Health Co-ordinators
Maternal mental health
Educational material on maternal depression specifically to be shown in ante-natal and post-natal waiting rooms. Source: Perinatal Mental Health Project
Indicator Input indicators a) Costs & availability of awareness-raising resources & materials
(television sets in clinics,DVDs,pamphlets)(CasStu: Res; FacSurv) Process indicators
a) No. of airings of DVDs/plays on MH in waiting rooms b) No of pamphlets / posters in health facilities
distributed(CasStu:Surv) Output indicators
a) % of health facility attendees who read/watch materials(CasStu:Surv)
b) Service user perception of accessibility and acceptability(CasStu:Surv)
Outcome indicators a) Improved MH literacy b) Improved help-seeking / increased demand for MH care from HC
attendees(CasStu:Surv; MHIS) (FacSurv)
2.2.1 Identification and diagnosis Rationale In order to provide effective interventions for persons with mental
disorders, there needs to be identification and diagnosis first.

[Type text]
Provider PHC doctor Family physician PHC nurse B. Psych counsellor/psychologist
Goal Increase identification and diagnosis of PHC service users with priority mental disorders
Content Screening and assessment for Depression, MD, AUD& Psychotic Disorders. a) Assessment whether patient needs brief interventions for alcohol
misuse or referral using stepped care referral pathways b) Referral of depression using stepped care referral pathways c) Referral of acute psychotic conditions to next level of care following
the Mental Health Care Act (2002) guidelines Source PC101
PC 101+ to include SBI (AUDIT and brief educational material on hazardous drinking) PC101+ to include refined algorythms for stepped care referral for depression for medication and/or task shifted counselling intervention PC101 includes training in the Mental Health Care Act (2002)
Supervision Family Physicians
Maternal mental health
PC101 includes assessing for maternal depression
Indicator Input indicator: a) Training materials available b) Costs/human resources for training (CasStu: FacProf)
c) Process indicator: a) No. of training sessions / Numbers attending (CasStu: TraFid)
Output indicator: a) Improved knowledge about identification /
diagnosis(CasStu:TrainFid) Outcome indicator:
a) Increased no. of people correctly identified/diagnosed with DD/AUD in the facility (FacSur)
b) Increased no. of people correctly receiving evidence-based treatment (FacSur)
2.2.2 Psychotropic medication treatment Rationale Psychotropic drugs are essential to control and treat symptoms in persons
with psychotic disorders and moderate to severe major depression Goal and objectives
Prescribing antipsychotic and anti-depressant drugs for moderate to severe mental disorders
Provider PHC doctor Psychiatrist Pharmacy assistant Pharmacist Intern

[Type text]
Professional nurse
Content and activities (components)
Initiation of psychotropic medication (only medical doctors) including explanation of duration, time, side effects etc Provision of follow-up repeat medication (PHC nurses) Identification and referral of patients requiring adjustment to their medication to psychiatrist
Source and tools
Mini Drug Master Plan 2011/12-2012/13 Mini Drug Master Plan 2011/12-2013/14 Essential Drug List (EDL) Standard Treatment Guidelines and Essential Medicine List
forPrimary Health Care 2008 PC 101
Training required
PC 101
Supervision Family Physician Psychiatrist
Maternal mental health
Same procedure as above would apply
Indicator Input indicator: a) Training/human resource costs for training in PC101
b) b) Adequate stocks of medication available at PHC level (CasStu: FacProf)
c) Process indicator: a) No of nurses and PHC doctors in receipt of training(CasStu:
TrainFid) b) Regular orders of medication made to ensure adequate
stocks(CasStu: FacProf) Output indicator:
a) Improved knowledge about prescribing(CasStu: TrainFid) Outcome indicator:
a) % of patients with moderate to severe priority disorders who require medication who actually receive it(Correct dosage, frequency, duration of treatment, adherence to treatment (e.g. pill counts), loss to follow up, delivery of psychoeducation, screening for side effects, appropriateness of initiation and change of medications ins response to change in clinical status) (FacSur, Cohort)
b) Change in patient and family clinical, social and economic outcomes (Cohort) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis
c) Decrease in out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
2.2.3 Low intensity psychosocial support Rationale Comprehensive patient-centred PHC requires that PHC providers respond to
patients with mental health problems in a supportive manner before

[Type text]
onward referral for targeted high intensity psychosocial interventions
Goal and objectives
Provide low intensity psychosocial support to service users identified as having mental disorders during normal PHC consultation
Provider PHC nurse Content and activities (components)
Low intensity supportive counselling including psycho-education, problem solving and SBI for alcohol misuse
Source and tools
Perinatal MH Project manual for nurses/PC 101
Indicator Input indicator: a) Costs/ human resources for training (as part of PC 101
training(CasStu: Res) b) PC101 training includes low intensity supportive counselling
including psychoeducation, problem solving and SBI for alcohol misuse.
Process indicator: a) No of training sessions / No. attending(CasStu: TrainFid)
Output indicator: a) Improved skills to deliver low intensity psychosocial care(CasStu:
TrainFid) b) Outcome indicator:
a) Increased delivery of low intensity psychosocial interventions as part of routine care (FacSurv)
b) Improved patient experience of holistic care (FacSurv) 2.2.4 Targeted high intensity psychosocial/counselling
interventions Rationale Targeted high intensity psychosocial/counselling interventions for
depression co-morbid with HIV/maternal depression are required to address the large treatment gap for these disorders and to prevent the overuse of medication for these conditions, often associated with social problems, as well as promote mental health.
Provider Lay counsellors B.Psych counsellor (if available)
Goal and objectives
Provide targeted high intensity psychosocial/counselling interventions for depression/maternal depression
Content Structured manualized intervention drawing on evidence-based psychological treatments for depression (CBT/PST/IPT) delivered in groups/individually.
Source PRIME-SA lay counsellor training manual
Training required
4 day training following on from PC101 training
Supervision B.Psych counsellor (if available) Consultant intern psychologists from the sub-district hospital
Maternal mental health
Structured manualized intervention drawing on evidence-based psychological treatments for depression (CBT/PST/IPT) delivered in groups/individually delivered by lay counsellors/enrolled nurse.
[Type text]
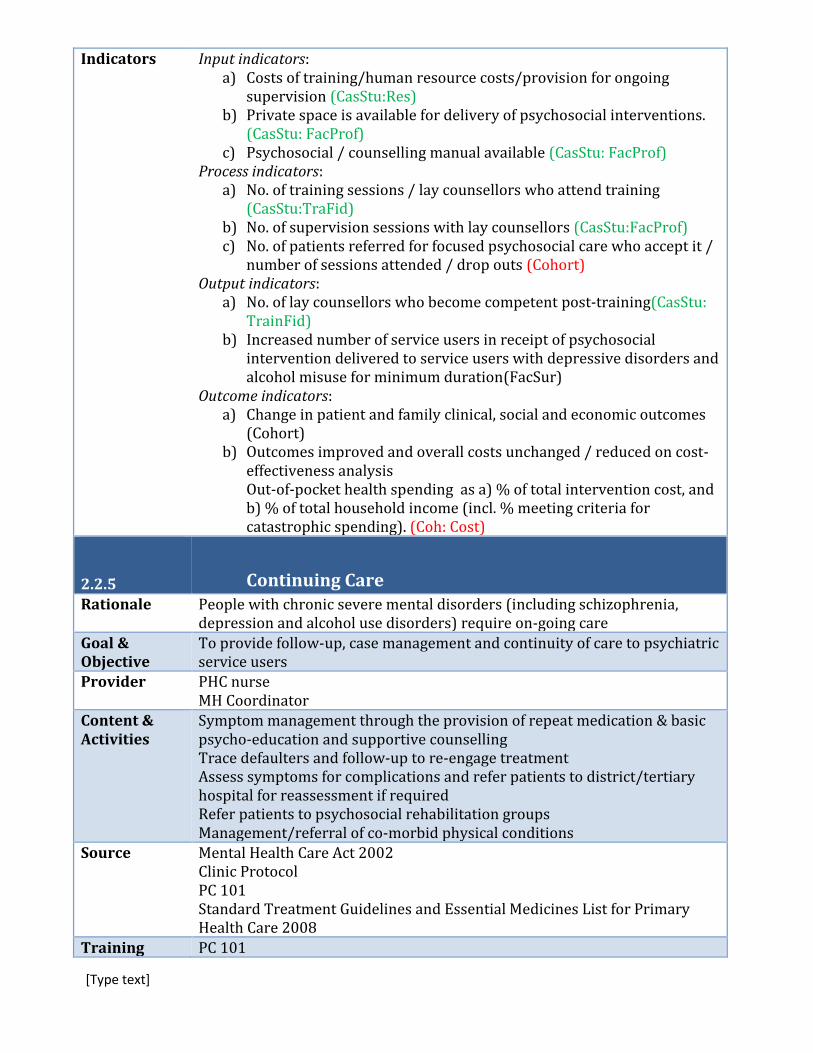
Indicators Input indicators: a) Costs of training/human resource costs/provision for ongoing
supervision (CasStu:Res) b) Private space is available for delivery of psychosocial interventions.
(CasStu: FacProf) c) Psychosocial / counselling manual available (CasStu: FacProf)
Process indicators: a) No. of training sessions / lay counsellors who attend training
(CasStu:TraFid) b) No. of supervision sessions with lay counsellors (CasStu:FacProf) c) No. of patients referred for focused psychosocial care who accept it /
number of sessions attended / drop outs (Cohort) Output indicators:
a) No. of lay counsellors who become competent post-training(CasStu: TrainFid)
b) Increased number of service users in receipt of psychosocial intervention delivered to service users with depressive disorders and alcohol misuse for minimum duration(FacSur)
Outcome indicators: a) Change in patient and family clinical, social and economic outcomes
(Cohort) b) Outcomes improved and overall costs unchanged / reduced on cost-
effectiveness analysis Out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
2.2.5 Continuing Care Rationale People with chronic severe mental disorders (including schizophrenia,
depression and alcohol use disorders) require on-going care
Goal & Objective
To provide follow-up, case management and continuity of care to psychiatric service users
Provider PHC nurse MH Coordinator
Content & Activities
Symptom management through the provision of repeat medication & basic psycho-education and supportive counselling Trace defaulters and follow-up to re-engage treatment Assess symptoms for complications and refer patients to district/tertiary hospital for reassessment if required Refer patients to psychosocial rehabilitation groups Management/referral of co-morbid physical conditions
Source Mental Health Care Act 2002 Clinic Protocol PC 101 Standard Treatment Guidelines and Essential Medicines List for Primary Health Care 2008
Training PC 101

[Type text]
Required
Maternal mental health
If applicable
Indicators Input indicator: a) MHIS system available which includes whether psychiatric patients
are in receipt of appropriate medication as per their diagnosis (CasStu: FacSur)
b) Costs of continuing care(CasStu: Res) Process indicators;
a) Data captured on MHIS system(CasStu: FacSur) b) Mechanism for following up defaulters operational
Output indicators: a) % of defaulters who are followed up / re-engaged b) % of persons in CC who are referred to psychosocial rehab groups c) % receiving psychoeducation d) % receiving regular physical check-ups (Cohort, CasStu: HMIS,
FacProf) Outcome indicators
a) Improvement in adherence rates (MHIS system) b) Reduction in relapse rates (MHIS system) c) Improved detection of co-morbid physical health problems(Cohort,
Coh: Qual) d) Change in patient and family clinical, social and economic outcomes
(Cohort, Coh: Qual)
2.3 Collaborative Care Rationale People identified as having mental disorders by PHC nurses at the PHC
facility level need to be referred onwards within a collaborative care model for diagnosis and treatment with psychotropic medication/specialist care and/or for counselling by lay health worker counsellors.
Goal & Objective
To provide a collaborative care referral system
Provider PHC nurse PHC doctor Lay mental health counsellors Mental health specialists
Content & Activities
Based on the severity of symptoms, PHC nurses need to refer service users to the appropriate provider for further treatment. Collaborative care referral/back-referral system for priority mental disorders needs to be in operational (see item no 6 of the Mental Health Care Plan).
Source Collaborative Care Referral systems (item 6 of the MHCP)
Training Required
PC 101
Maternal Collaborative care referral system for depression
[Type text]
mental health
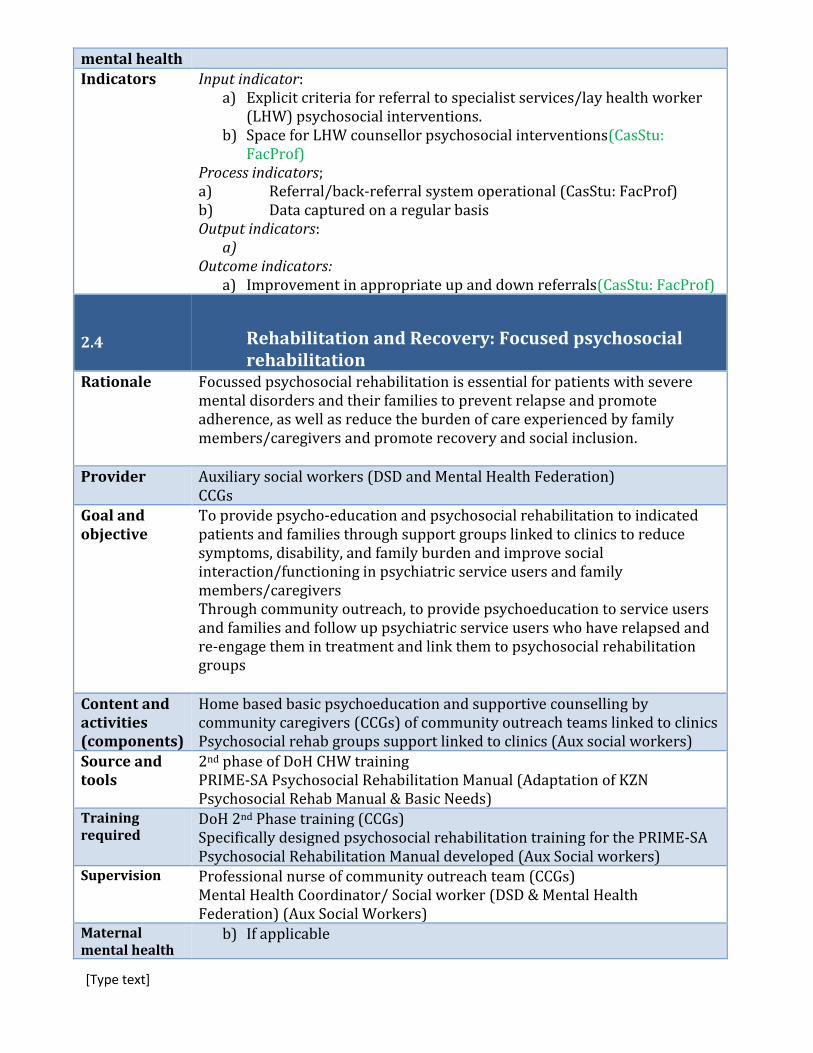
Indicators Input indicator: a) Explicit criteria for referral to specialist services/lay health worker
(LHW) psychosocial interventions. b) Space for LHW counsellor psychosocial interventions(CasStu:
FacProf) Process indicators; a) Referral/back-referral system operational (CasStu: FacProf) b) Data captured on a regular basis Output indicators:
a) Outcome indicators:
a) Improvement in appropriate up and down referrals(CasStu: FacProf) 2.4 Rehabilitation and Recovery: Focused psychosocial
rehabilitation Rationale Focussed psychosocial rehabilitation is essential for patients with severe
mental disorders and their families to prevent relapse and promote adherence, as well as reduce the burden of care experienced by family members/caregivers and promote recovery and social inclusion.
Provider Auxiliary social workers (DSD and Mental Health Federation) CCGs
Goal and objective
To provide psycho-education and psychosocial rehabilitation to indicated patients and families through support groups linked to clinics to reduce symptoms, disability, and family burden and improve social interaction/functioning in psychiatric service users and family members/caregivers Through community outreach, to provide psychoeducation to service users and families and follow up psychiatric service users who have relapsed and re-engage them in treatment and link them to psychosocial rehabilitation groups
Content and activities (components)
Home based basic psychoeducation and supportive counselling by community caregivers (CCGs) of community outreach teams linked to clinics Psychosocial rehab groups support linked to clinics (Aux social workers)
Source and tools
2nd phase of DoH CHW training PRIME-SA Psychosocial Rehabilitation Manual (Adaptation of KZN Psychosocial Rehab Manual & Basic Needs)
Training required
DoH 2nd Phase training (CCGs) Specifically designed psychosocial rehabilitation training for the PRIME-SA Psychosocial Rehabilitation Manual developed (Aux Social workers)
Supervision Professional nurse of community outreach team (CCGs) Mental Health Coordinator/ Social worker (DSD & Mental Health Federation) (Aux Social Workers)
Maternal mental health
b) If applicable
[Type text]
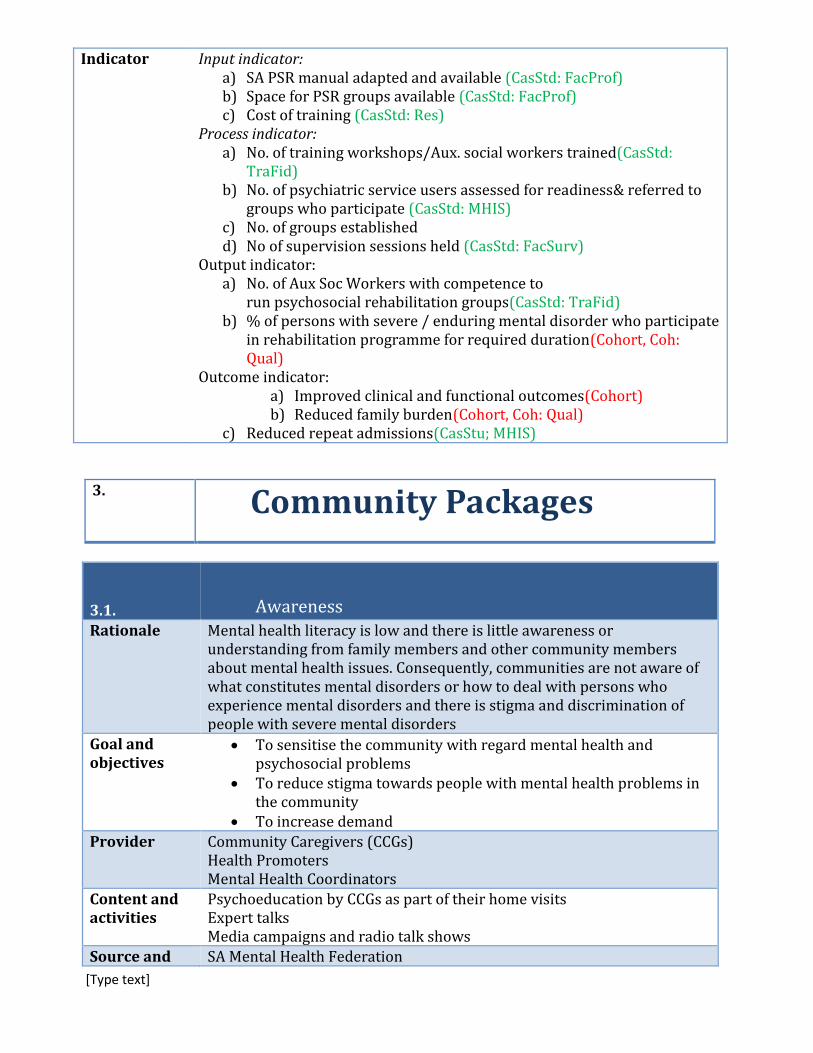
Indicator Input indicator: a) SA PSR manual adapted and available (CasStd: FacProf) b) Space for PSR groups available (CasStd: FacProf) c) Cost of training (CasStd: Res)
Process indicator: a) No. of training workshops/Aux. social workers trained(CasStd:
TraFid) b) No. of psychiatric service users assessed for readiness& referred to
groups who participate (CasStd: MHIS) c) No. of groups established d) No of supervision sessions held (CasStd: FacSurv)
Output indicator: a) No. of Aux Soc Workers with competence to
run psychosocial rehabilitation groups(CasStd: TraFid) b) % of persons with severe / enduring mental disorder who participate
in rehabilitation programme for required duration(Cohort, Coh: Qual)
Outcome indicator: a) Improved clinical and functional outcomes(Cohort) b) Reduced family burden(Cohort, Coh: Qual)
c) Reduced repeat admissions(CasStu; MHIS)
3. Community Packages
3.1. Awareness Rationale Mental health literacy is low and there is little awareness or
understanding from family members and other community members about mental health issues. Consequently, communities are not aware of what constitutes mental disorders or how to deal with persons who experience mental disorders and there is stigma and discrimination of people with severe mental disorders
Goal and objectives
To sensitise the community with regard mental health and psychosocial problems
To reduce stigma towards people with mental health problems in the community
To increase demand
Provider Community Caregivers (CCGs) Health Promoters Mental Health Coordinators
Content and activities
Psychoeducation by CCGs as part of their home visits Expert talks Media campaigns and radio talk shows
Source and SA Mental Health Federation

[Type text]
tools 2nd Phase DoH training manual for CCG
Training required
First and second phase DoH training of CCGs
Supervision Professional nurse of community outreach teams Mental Health Coordinators
Maternal mental health
Promote awareness of maternal depression in above activities
Indicator Input indicators: a) Community caregiver (CCG) training material available(CasStd:
FacProf) b) Costs of developing awareness-raising material/cost of delivery of
activities (CasStu: Res) c) Process indicators:
a) No. of training sessions / No. of CCGs attending (CasStd:TraFid) b) No. of media campaigns(CasStd: FacProf)
Output indicators: Outcome indicator:
a) Increase in no of people who self-referred or were referred by community for treatment. (CasStd:MHIS)FacSurv) b) Decreased delay to help-seeking(CasStu: HMIS; FacSurv) c) Decreased discrimination / abuse (FacSurv)
3.2 Community Informant Case Detection Rationale Detection at community level will increase access to care
Goal and objective
Increase case detection in the community
Provider CCGs South African police services Auxiliary social workers Traditional healers Community lay counsellors e.g., spiritual leaders
Content and activities (components)
Pro-active community case finding by trained community outreach team,South African Police Service, (auxiliary)social workers, traditional healers and lay counsellors e.g., spiritual leaders
Referral of MHCUs in need of facility (clinic or hospital) care
Source and tools
2nd Phase training manual for CCGs (Incl screening tool for AUD and depression)
Community Mental Health Programme training manual for community health workers (for traditional healers and spiritual leaders)
Training required
5 day training for traditional healers 2nd Phase DoH training of CCGs
Supervision Professional nurse of community outreach team MHCo-ordinators

[Type text]
Maternal mental health
Community outreach teams will be able to screen and refer women suspected of suffering maternal depression
Indicator Input indicator: a) Training manuals with detection protocols available(CasStu:
FacProf) b) Training costs (CasStu: Res)
Process indicator: a) No. of sessions / No. of relevant persons attending training(CasStd:
TraFid) b) No. of supervision sessions (CasStd: FacProf)
Output indicators: a) Competence to detect / refer post-training(CasStd: TraFid)
Outcome indicators: a) Increased number of detected cases / appropriate
referrals(CasStd: MHIS, FacSurv) b) Decreased delay before accessing care(CasStd: MHIS, Fac Survey)

[Type text]

[Type text]
3. INDICATOR TABLE
1. INDICATORS FOR ORGANIZATIONAL LEVEL
MHCP Function ToC Outcome
1.1 Engage, mobilise and sensitise district level stakeholders e. Health care organisation staff informed and committed to mental health programme, have reduced stigma and are willing to engage with programme
Cross-country South Africa
Input Costs of meetings / human resources (CasStu: Res) Costs of meetings / human resource time(CasStu: Res)
Process Depends on package e.g. No of meetings and participation in meetings [ __% of staff participate in ___% of meetings.] (CasStu: DocRev, ToC)
Number of ToC workshops / CAB meetings Participation in meetings [ __% of staff, categories & community members participating to participate who do participate in ___% of meetings.] (CasStu: DocRev, ToC)
Output Mental health in reports of HSO MH in approved work plan Representation of MH on HSO Level of MH activity / inclusion in work plans MH regularly (define) on agenda of HSO meetings
No. of staff & community representatives reached through this engagement No. of MH specialists aware of new system configuration/diversification of roles (CasStu: Surv) No. of PHC providers aware of new system and inclusion of MHC as part of their roles Heightened awareness of the importance of providing mental health in PHC & reduced stigma(CasStu: Qual
Outcome Heightened awareness of the importance of providing mental health in PHC and level of engagement with programme (CasStu: Qual)
)Increase in resources allocated to mental health (% increase in budget allocation for mental health) (CasStu: FacProf) Increased outreach support ) (CasStu: FacProf) % increase of human resources for mental health in line with the norms. (CasStu: FacProf)
EVALUATION
Case study may include: Qualitative: qualitative interviews (to look at awareness / stigmatising attitudes / evidence of advocacy for MH) Resources: recording of costs / programme resources Document review: documentary analysis (e.g. for monitoring what is included on agenda of meetings) ToC:ToC workshops
MHCP Function ToC Outcome
1.2 Programme management 1.2.1 Development & Approval of MHCP
a. MHCP approved/accepted

[Type text]
Cross-country South Africa
Input Costs associated with management meetings (CasStu: Res) Costs/humanresource costs associated with development of MHCP (CasStu: Res)
Process No finance meetings with MH on the agenda (CasStu: DocRev)
ToC meetings leading to the development of the MHCP (CasStu: DocRev)
Output MHCP finalised Operational Guidelines finalised Budget finalised (CasStu: DocRev) Budget sanctioned for MHCP(CasStu: Res)
MHCP finalised Operational Guidelines finalised(CasStu: DocRev)
Outcome MHCP approved Operational Guidelines approved(CasStu: DocRev) MHCP budget approved at district level (CasStu: Res) Evidence of resource mobilisation for sustainability / expansion of services compared to needs-based resource modelling tool (CasStu: Res)
MHCP approved Operational Guidelines approved(CasStu: DocRev Evidence of resource mobilisation for sustainability / expansion of services (CasStu: Res)
EVALUATION Case study may include:
Document review: review of meeting agendas and minutes, final MCHP and budget required Resources: data from HSO on budget available (not just in writing), costing tool
MHCP Function ToC Outcome
1.2 Programme management 1.2.2 Ongoing District/sub-district management of the implementation of the MHCP
(b) MH Programme Co-ordinator functioning adequately (c). Specialist, primary and community level service providers are in place to: 1. Train, 2. Supervise 3. Deliver services
Cross-country South Africa
Input Costs associated with recruiting and paying staff (CasStu: Res) Cost of human resource time to attend meetings/costs of new staff(CasStu: Res)
Process Time taken to recruit posts, unfilled posts (CasStu: DocRev)
Representation of MH on District management teamMH regularly part of agenda of above mentioned meetings (CasStu: DocRev) Annual ToC review meetings held
Output Mental health integrated into the District Health Plan. (CasStu: DocRev)
Outcome Programme co-ordinator in post [100% of programme co-ordinator function fulfilled by the start of programme roll-out] (CasStu: DocRev) MH co-ordinator functioning adequately (CasStu: Qual) No. of service providers available to provide: 1. Training, 2. Supervision, 3. Service delivery (CasStu: FacProf)
Frequency of ToC meetings to review MHCP Implementation of initiatives to address bottlenecks Creation of additional specialist posts for mental health Deployment of specialists to train, supervise and provide a back-up referral service (Outreach support for mental health training supervision and support)(CasStu: FacProf)

[Type text]
MH co-ordinator functioning adequately (CasStu: Qual) . (CasStu: FacProf)
EVALUATION Case study may include:
Document review/facility survey: Data from HSO/facilities on number of personnel in post, staff turnover, successful implementation of mechanisms to ensure workers appropriately trained and supported Resources: Costing of additional human resources (WHO costing tool) Qualitative: exploration of role of co-ordinator – whether side-tracked by other issues, given sufficient time and support, effective in their post
MHCP Function ToC Outcome
1.2 Programme management 1.2.3 Plan and co-ordinate inter-sectoral collaboration for MHCP
d. Health care organisation staff and staff from other sectors are aware of mental illness, have reduced stigma and are willing to engage with programme
Cross-country South Africa
Input Costs associated with intersectoral meetings (CasStu: Res) Human resource costs associated with attending intersectoral meetings(CasStu: Res)
Process No of intersectoral meetings with MH on the agenda (CasStu: DocRev)
No. of intersectoral meetings held No. of people attending these meetings MH on meeting agenda (CasStu: DocRev) Attendance of these meetings by different sectors
Output No. of different sectors involved actively in MH care No of lay counsellors trained from other sectors (traditional healers/faithhealers/police) No. of different sectors actively involved in mental health care
Outcome Increased No. of different sectors involved actively in mental health care(CasStu: DocRev, Qual)
Increase in number of intersectoral referrals(CasStu: DocRev, Qual)
EVALUATION Case study may include:
Document review: review of meeting agendas and minutes of intersectoral meetings Resources: resources allocated and costs for other sectors involved in MH care Qualitative: exploration of interaction between MH care and other sectors
MHCP Function ToC Outcome
1.2 Programme management e. Health information System includes key mental health indicators which are routinely
[Type text]
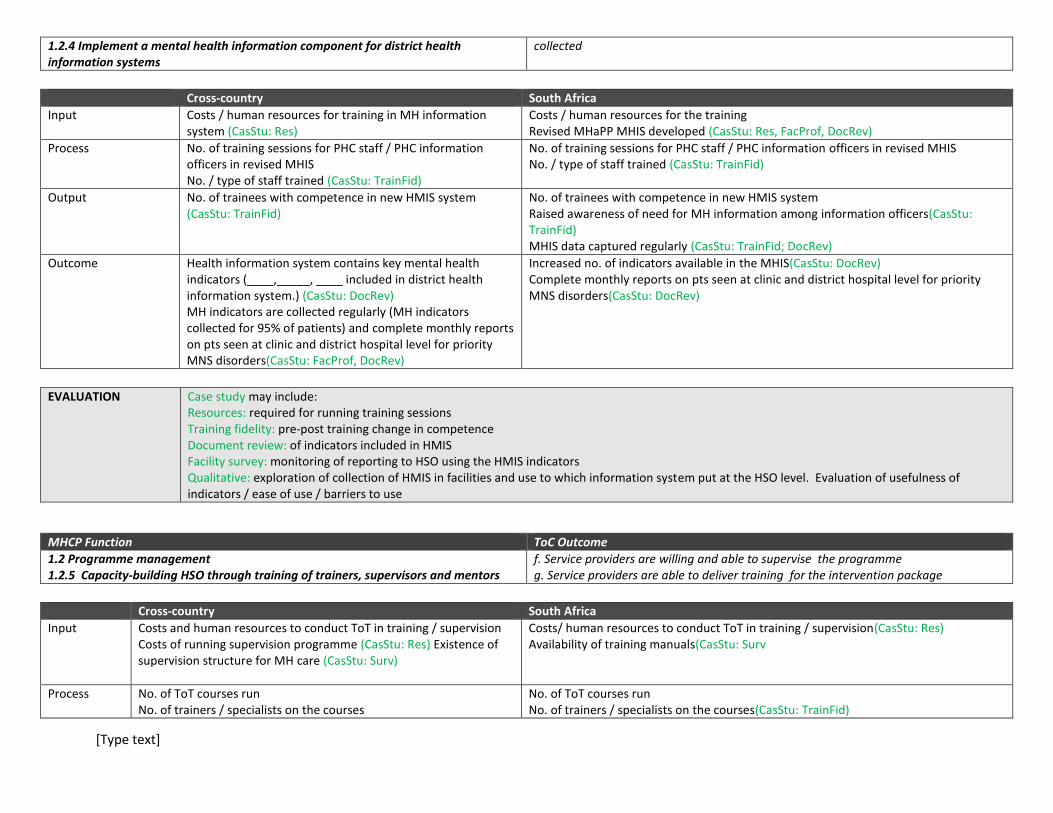
1.2.4 Implement a mental health information component for district health information systems
collected
Cross-country South Africa
Input Costs / human resources for training in MH information system (CasStu: Res)
Costs / human resources for the training Revised MHaPP MHIS developed (CasStu: Res, FacProf, DocRev)
Process No. of training sessions for PHC staff / PHC information officers in revised MHIS No. / type of staff trained (CasStu: TrainFid)
No. of training sessions for PHC staff / PHC information officers in revised MHIS No. / type of staff trained (CasStu: TrainFid)
Output No. of trainees with competence in new HMIS system (CasStu: TrainFid)
No. of trainees with competence in new HMIS system Raised awareness of need for MH information among information officers(CasStu: TrainFid) MHIS data captured regularly (CasStu: TrainFid; DocRev)
Outcome Health information system contains key mental health indicators (____,_____, ____ included in district health information system.) (CasStu: DocRev) MH indicators are collected regularly (MH indicators collected for 95% of patients) and complete monthly reports on pts seen at clinic and district hospital level for priority MNS disorders(CasStu: FacProf, DocRev)
Increased no. of indicators available in the MHIS(CasStu: DocRev) Complete monthly reports on pts seen at clinic and district hospital level for priority MNS disorders(CasStu: DocRev)
EVALUATION
Case study may include: Resources: required for running training sessions Training fidelity: pre-post training change in competence Document review: of indicators included in HMIS Facility survey: monitoring of reporting to HSO using the HMIS indicators Qualitative: exploration of collection of HMIS in facilities and use to which information system put at the HSO level. Evaluation of usefulness of indicators / ease of use / barriers to use
MHCP Function ToC Outcome
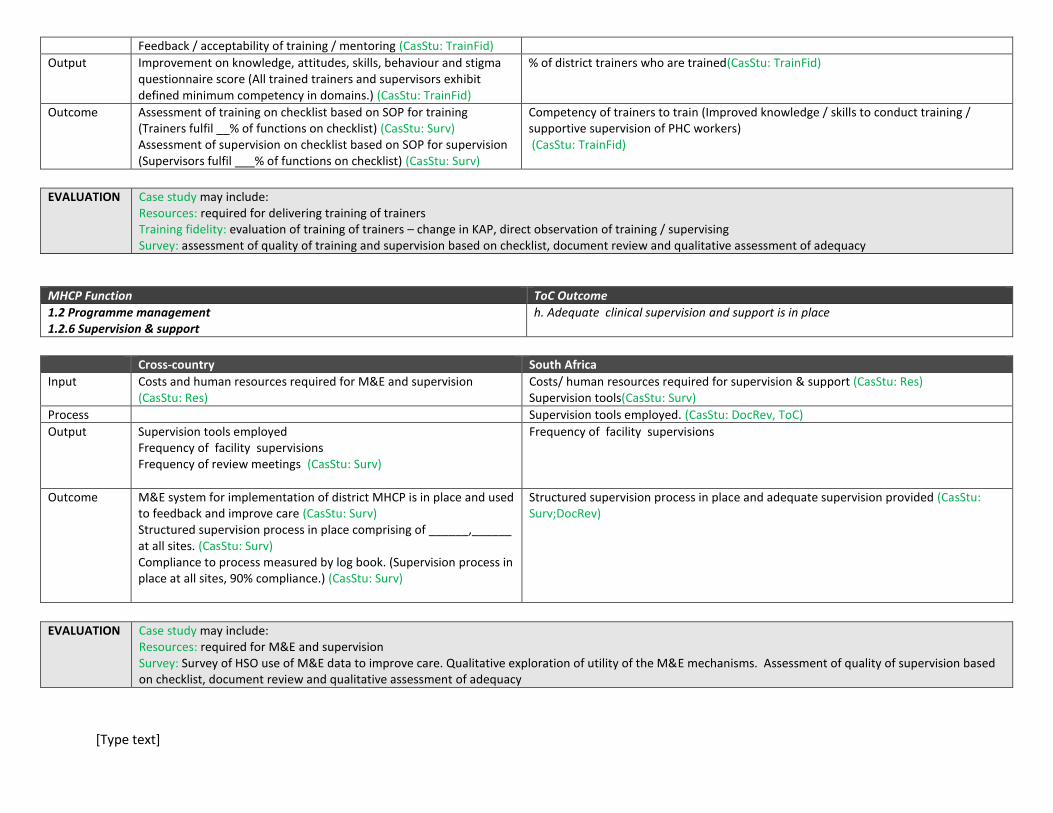
1.2 Programme management 1.2.5 Capacity-building HSO through training of trainers, supervisors and mentors
f. Service providers are willing and able to supervise the programme g. Service providers are able to deliver training for the intervention package
Cross-country South Africa
Input Costs and human resources to conduct ToT in training / supervision Costs of running supervision programme (CasStu: Res) Existence of supervision structure for MH care (CasStu: Surv)
Costs/ human resources to conduct ToT in training / supervision(CasStu: Res) Availability of training manuals(CasStu: Surv
Process No. of ToT courses run No. of trainers / specialists on the courses
No. of ToT courses run No. of trainers / specialists on the courses(CasStu: TrainFid)
[Type text]
Feedback / acceptability of training / mentoring (CasStu: TrainFid)
Output Improvement on knowledge, attitudes, skills, behaviour and stigma questionnaire score (All trained trainers and supervisors exhibit defined minimum competency in domains.) (CasStu: TrainFid)
% of district trainers who are trained(CasStu: TrainFid)
Outcome Assessment of training on checklist based on SOP for training (Trainers fulfil __% of functions on checklist) (CasStu: Surv) Assessment of supervision on checklist based on SOP for supervision (Supervisors fulfil ___% of functions on checklist) (CasStu: Surv)
Competency of trainers to train (Improved knowledge / skills to conduct training / supportive supervision of PHC workers) (CasStu: TrainFid)
EVALUATION
Case study may include: Resources: required for delivering training of trainers Training fidelity: evaluation of training of trainers – change in KAP, direct observation of training / supervising Survey: assessment of quality of training and supervision based on checklist, document review and qualitative assessment of adequacy
MHCP Function ToC Outcome
1.2 Programme management 1.2.6 Supervision & support
h. Adequate clinical supervision and support is in place
Cross-country South Africa
Input Costs and human resources required for M&E and supervision (CasStu: Res)
Costs/ human resources required for supervision & support (CasStu: Res) Supervision tools(CasStu: Surv)
Process Supervision tools employed. (CasStu: DocRev, ToC)
Output Supervision tools employed Frequency of facility supervisions Frequency of review meetings (CasStu: Surv)
Frequency of facility supervisions
Outcome M&E system for implementation of district MHCP is in place and used to feedback and improve care (CasStu: Surv) Structured supervision process in place comprising of ______,______ at all sites. (CasStu: Surv) Compliance to process measured by log book. (Supervision process in place at all sites, 90% compliance.) (CasStu: Surv)
Structured supervision process in place and adequate supervision provided (CasStu: Surv;DocRev)
EVALUATION
Case study may include: Resources: required for M&E and supervision Survey: Survey of HSO use of M&E data to improve care. Qualitative exploration of utility of the M&E mechanisms. Assessment of quality of supervision based on checklist, document review and qualitative assessment of adequacy
[Type text]
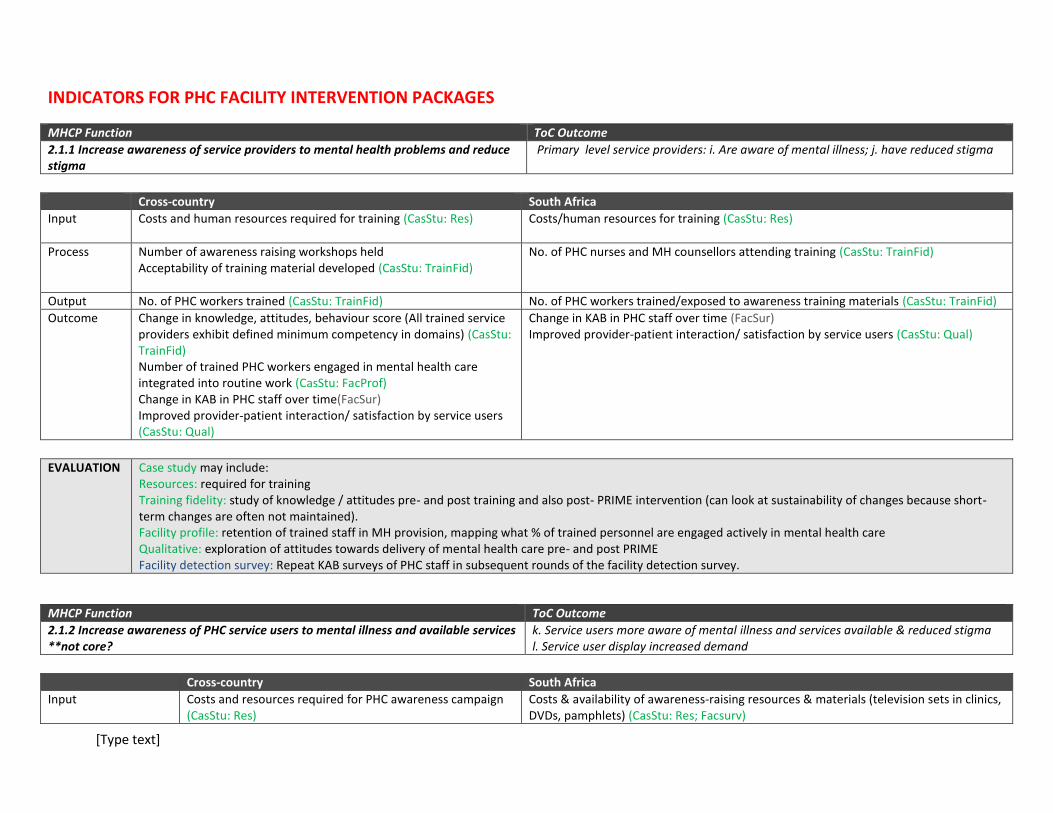
INDICATORS FOR PHC FACILITY INTERVENTION PACKAGES
MHCP Function ToC Outcome
2.1.1 Increase awareness of service providers to mental health problems and reduce stigma
Primary level service providers: i. Are aware of mental illness; j. have reduced stigma
Cross-country South Africa
Input Costs and human resources required for training (CasStu: Res) Costs/human resources for training (CasStu: Res)
Process Number of awareness raising workshops held Acceptability of training material developed (CasStu: TrainFid)
No. of PHC nurses and MH counsellors attending training (CasStu: TrainFid)
Output No. of PHC workers trained (CasStu: TrainFid) No. of PHC workers trained/exposed to awareness training materials (CasStu: TrainFid)
Outcome Change in knowledge, attitudes, behaviour score (All trained service providers exhibit defined minimum competency in domains) (CasStu: TrainFid) Number of trained PHC workers engaged in mental health care integrated into routine work (CasStu: FacProf) Change in KAB in PHC staff over time(FacSur) Improved provider-patient interaction/ satisfaction by service users (CasStu: Qual)
Change in KAB in PHC staff over time (FacSur) Improved provider-patient interaction/ satisfaction by service users (CasStu: Qual)
EVALUATION
Case study may include: Resources: required for training Training fidelity: study of knowledge / attitudes pre- and post training and also post- PRIME intervention (can look at sustainability of changes because short-term changes are often not maintained). Facility profile: retention of trained staff in MH provision, mapping what % of trained personnel are engaged actively in mental health care Qualitative: exploration of attitudes towards delivery of mental health care pre- and post PRIME Facility detection survey: Repeat KAB surveys of PHC staff in subsequent rounds of the facility detection survey.
MHCP Function ToC Outcome
2.1.2 Increase awareness of PHC service users to mental illness and available services **not core?
k. Service users more aware of mental illness and services available & reduced stigma l. Service user display increased demand
Cross-country South Africa
Input Costs and resources required for PHC awareness campaign (CasStu: Res)
Costs & availability of awareness-raising resources & materials (television sets in clinics, DVDs, pamphlets) (CasStu: Res; Facsurv)
[Type text]
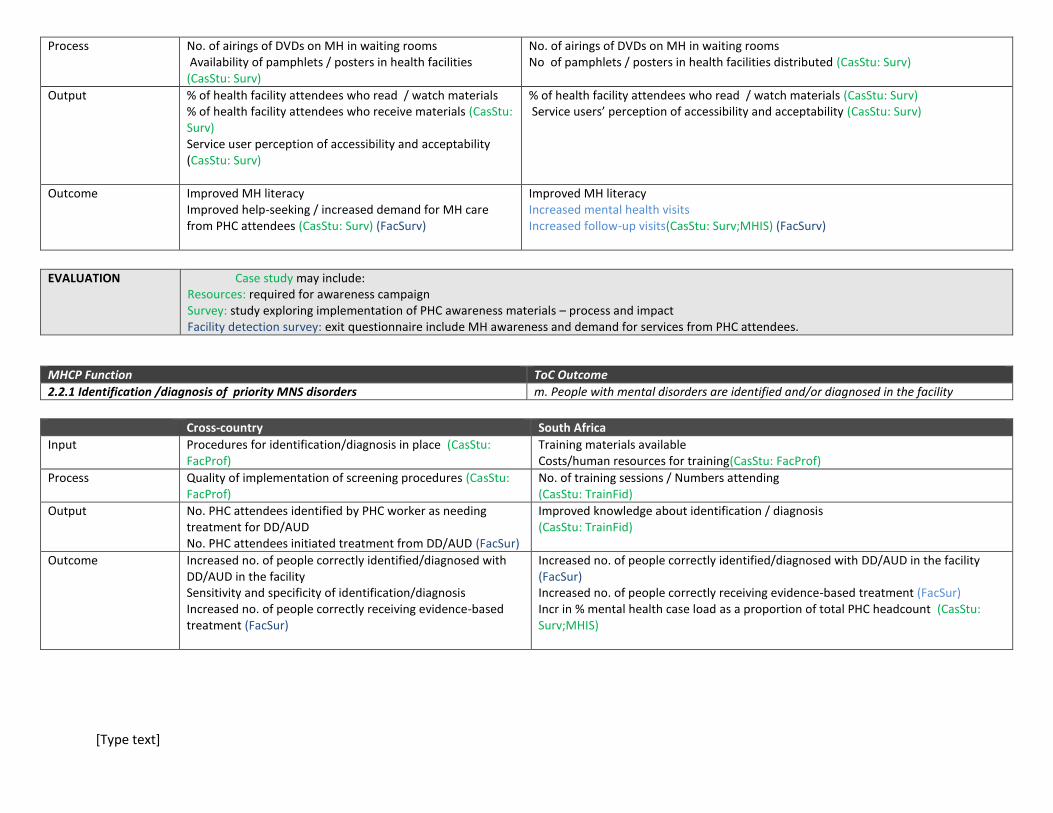
Process No. of airings of DVDs on MH in waiting rooms Availability of pamphlets / posters in health facilities (CasStu: Surv)
No. of airings of DVDs on MH in waiting rooms No of pamphlets / posters in health facilities distributed (CasStu: Surv)
Output % of health facility attendees who read / watch materials % of health facility attendees who receive materials (CasStu: Surv) Service user perception of accessibility and acceptability (CasStu: Surv)
% of health facility attendees who read / watch materials (CasStu: Surv) Service users’ perception of accessibility and acceptability (CasStu: Surv)
Outcome Improved MH literacy Improved help-seeking / increased demand for MH care from PHC attendees (CasStu: Surv) (FacSurv)
Improved MH literacy Increased mental health visits Increased follow-up visits(CasStu: Surv;MHIS) (FacSurv)
EVALUATION Case study may include:
Resources: required for awareness campaign Survey: study exploring implementation of PHC awareness materials – process and impact Facility detection survey: exit questionnaire include MH awareness and demand for services from PHC attendees.
MHCP Function ToC Outcome
2.2.1 Identification /diagnosis of priority MNS disorders m. People with mental disorders are identified and/or diagnosed in the facility
Cross-country South Africa
Input Procedures for identification/diagnosis in place (CasStu: FacProf)
Training materials available Costs/human resources for training(CasStu: FacProf)
Process Quality of implementation of screening procedures (CasStu: FacProf)
No. of training sessions / Numbers attending (CasStu: TrainFid)
Output No. PHC attendees identified by PHC worker as needing treatment for DD/AUD No. PHC attendees initiated treatment from DD/AUD (FacSur)
Improved knowledge about identification / diagnosis (CasStu: TrainFid)
Outcome Increased no. of people correctly identified/diagnosed with DD/AUD in the facility Sensitivity and specificity of identification/diagnosis Increased no. of people correctly receiving evidence-based treatment (FacSur)
Increased no. of people correctly identified/diagnosed with DD/AUD in the facility (FacSur) Increased no. of people correctly receiving evidence-based treatment (FacSur) Incr in % mental health case load as a proportion of total PHC headcount (CasStu: Surv;MHIS)
[Type text]
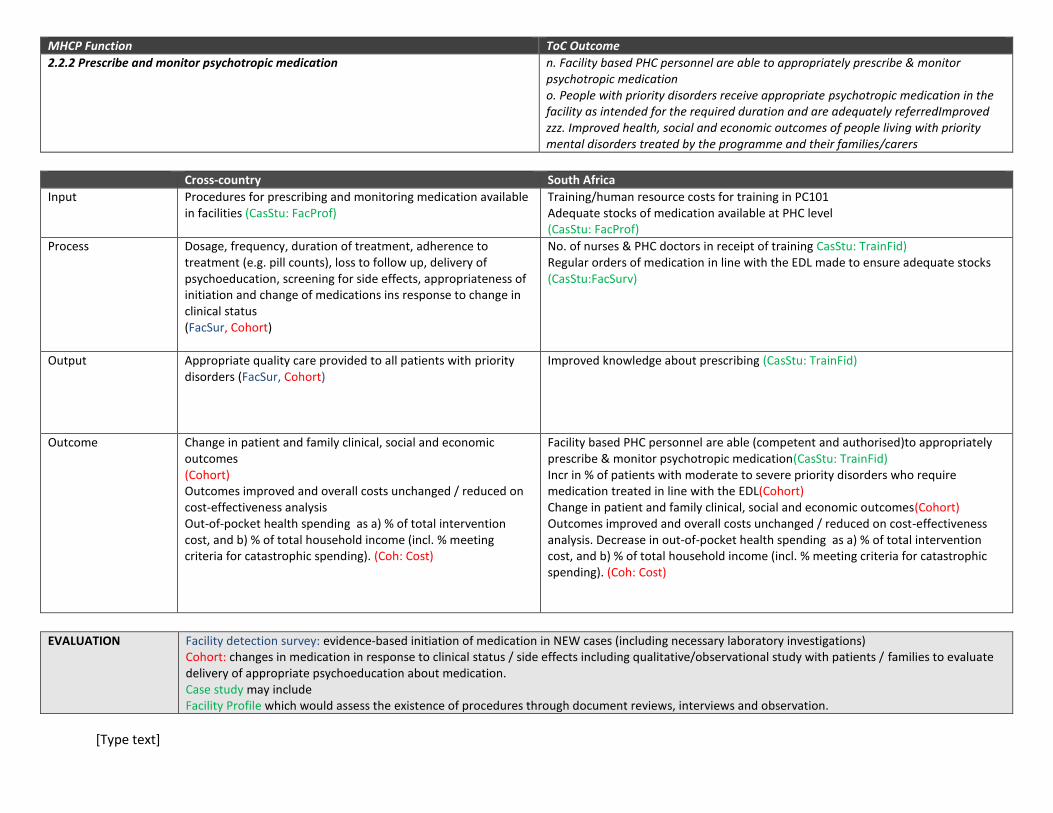
MHCP Function ToC Outcome
2.2.2 Prescribe and monitor psychotropic medication n. Facility based PHC personnel are able to appropriately prescribe & monitor psychotropic medication o. People with priority disorders receive appropriate psychotropic medication in the facility as intended for the required duration and are adequately referredImproved zzz. Improved health, social and economic outcomes of people living with priority mental disorders treated by the programme and their families/carers
Cross-country South Africa
Input Procedures for prescribing and monitoring medication available in facilities (CasStu: FacProf)
Training/human resource costs for training in PC101 Adequate stocks of medication available at PHC level (CasStu: FacProf)
Process Dosage, frequency, duration of treatment, adherence to treatment (e.g. pill counts), loss to follow up, delivery of psychoeducation, screening for side effects, appropriateness of initiation and change of medications ins response to change in clinical status (FacSur, Cohort)
No. of nurses & PHC doctors in receipt of training CasStu: TrainFid) Regular orders of medication in line with the EDL made to ensure adequate stocks (CasStu:FacSurv)
Output Appropriate quality care provided to all patients with priority disorders (FacSur, Cohort)
Improved knowledge about prescribing (CasStu: TrainFid)
Outcome Change in patient and family clinical, social and economic outcomes (Cohort) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis Out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
Facility based PHC personnel are able (competent and authorised)to appropriately prescribe & monitor psychotropic medication(CasStu: TrainFid) Incr in % of patients with moderate to severe priority disorders who require medication treated in line with the EDL(Cohort) Change in patient and family clinical, social and economic outcomes(Cohort) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis. Decrease in out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
EVALUATION
Facility detection survey: evidence-based initiation of medication in NEW cases (including necessary laboratory investigations) Cohort: changes in medication in response to clinical status / side effects including qualitative/observational study with patients / families to evaluate delivery of appropriate psychoeducation about medication. Case study may include Facility Profile which would assess the existence of procedures through document reviews, interviews and observation.

[Type text]
MHCP Function ToC Outcome
2.2.3 Provide low intensity psychosocial interventions p. PHC providers are able to provide low intensityc psychosocial support as part of routine care q. People with priority disorders receive low intensity psychosocial support as part of routine care
Cross-country South Africa
Input Private space is available for delivery of psychosocial interventions. Referral systems in place for psychosocial interventions. (CasStu: FacProf)
Costs/ human resources for training (CasStu: Res) PC101 training includes low intensity supportive counselling including psychoeducation, & problem solving and SBI for alcohol misuse. (CasStu: FacProf)
Process Dosage, frequency, duration of psychosocial interventions (Cohort,FacSur)
No. of training sessions / No. attending (CasStu: TrainFid)
Output Appropriate and quality care provided to all patients with priority disorders (FacSur, Cohort) Increased delivery of basic psychosocial interventions as part of routine care
Improved skills to deliver low intensity psychosocial care (CasStu: TrainFid)
Outcome Change in patient and family clinical, social and economic outcomes (Cohort)Improved patient experience of holistic care (Coh: Qual) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis Out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
Increased delivery of low intensity psychosocial interventions as part of routine care (Fac Sur) Improved patient experience of holistic care (Fac Sur)
EVALUATION
Cohort: would assess factors related to the process of medication prescription delivery and outcomes– may need observational methods / patient feedback / evaluation using case vignettes / documentary analysis of case notes where likely to be informative Facility detection survey: evidence-based initiation of psychosocial interventions in new patients Case Study may include Facility Profile would assess the existence of procedures for treatments as well as space through document reviews, interviews and observation as well

[Type text]
MHCP Function ToC Outcome
2.2.4 Provide high intensity targeted counselling r. Lay Health Worker counsellors are able to provide high intensity effective targeted counselling for depression in PLWHAs and maternal depression s. Lay Health Worker counsellors are able to provide high intensity effective targeted counselling for maternal depression t. People with these priority disorders receive targeted effective interventions in the facility as intended for the required duration u. People with priority disorders are adequately referred. zzz. Improved health, social and economic outcomes of people living with priority mental disorders treated by the programme and their families/carers
Cross-country South Africa
Input Private space is available for delivery of psychosocial interventions. (CasStu: FacProf)
Costs of training/human resource costs/provision for ongoing supervision (CasStu:Res) Private space is available for delivery of psychosocial interventions. (CasStu: FacProf) Psychosocial / counselling manual available (CasStu: FacProf)
Process Dosage, frequency, duration of psychosocial interventions (Cohort, FacSur)
No. of training sessions / lay counsellors who attend training (CasStu:TraFid) No. of supervision sessions with lay counsellors (CasStu:FacProf) No. of patients referred for focused psychosocial care who accept it / number of sessions attended / drop outs (Cohort)
Output Appropriate and quality care provided to all patients with priority disorders (FacSur, Cohort) Increased delivery of basic psychosocial interventions as part of routine care (Cohort, FacSur)
No. of lay counsellors who become competent post-training (CasStu:TraFid) Increased number of service users in receipt of psychosocial intervention delivered to service users with depressive disorders and alcohol misuse for minimum duration (CasStu:FacProf)
Outcome Improved patient experience of holistic care (Coh: Qual) Change in patient and family clinical, social and economic outcomes (Cohort) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis Out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
Change in patient and family clinical, social and economic outcomes (Cohort) Outcomes improved and overall costs unchanged / reduced on cost-effectiveness analysis Out-of-pocket health spending as a) % of total intervention cost, and b) % of total household income (incl. % meeting criteria for catastrophic spending). (Coh: Cost)
EVALUATION
Cohort: – may need observational methods / patient feedback / evaluation using case vignettes / documentary analysis of case notes where likely to be informative Facility detection survey: evidence-based initiation of psychosocial interventions in new patients Facility Profile: would assess the availability of space for psychosocial interventions.

[Type text]
MHCP Function ToC Outcome
2.2.5 Ensure continuing care through monitoring of treatment, adherence / loss to follow up and recovery in psychiatric patients with schizophrenia
t. People with chronic schizophrenia receive appropriate follow-up care. zzz. Improved health, social and economic outcomes of people living with priority mental disorders treated by the programme and their families/carers.
Cross-country South Africa
Input Costs of continuing care intervention (CasStu: Res) MHIS system available which includes whether psychiatric patients are in receipt of appropriate medication as per their diagnosis (CasStu: FacSur) Costs of continuing care(CasStu: Res)
Process Mechanism for following up defaulters operational CasStu: FacProf)
Data captured on HMIS system(CasStu: FacSur) Mechanism for following up defaulters operational(CasStu: FacSur)
Output % of defaulters who are followed up / re-engaged % of persons in CC who are referred appropriately for specialist input % receiving psychoeducation % receiving regular physical check-ups (Cohort, CasStu: HMIS, FacProf)
% of defaulters who are followed up / re-engaged % of persons with chronic schizophrenia who are referred to psychosocial rehab groups % receiving psycho-education % receiving regular physical check-ups (Cohort, CasStu: HMIS, FacProf)
Outcome Improvement in adherence rates Reduction in relapse rates Improved detection of co-morbid physical health problems Reduced repeat readmissions Change in patient and family clinical, social and economic outcomes (Cohort, Coh: Qual)
Improvement in adherence rates (MHIS system) Reduction in relapse rates (MHIS system) Improved detection of co-morbid physical health problems (Cohort, Coh: Qual) Change in patient and family clinical, social and economic outcomes (Cohort, Coh: Qual)
EVALUATION
Cohort to look at adherence / clinical and social outcomes Coh: Qual: Qualitative work with patients / family members in relation to quality / acceptability of care / any challenges due to outreach (increased stigma / perceived intrusiveness / coerciveness)? CasStu: FacProffor evaluation of the system for delivering continuing care .
MHCP Function ToC Outcome
2.3 Ensure specialist mental health care interfaces with PHC u.Collaborative care referral system to ensure a seamless service between PHC and specialist services
Cross-country South Africa

[Type text]
Input Programme costs Service providers who are trained are available to deliver interventions. Private space is available for delivery of psychosocial interventions. Referral systems in place for psychosocial interventions. (CasStu: FacProf)
Stepped care referral system developed for referral to specialist services/lay health worker (LHW) psychosocial interventions. Space for LHW counsellor psychosocial interventions. (CasStu: FacProf)
Process
Output Referral / back-referral consultation system operational Satisfaction from PHC and specialist MH services (CasStu: FacProf, Qual)
Referral/back-referral system operational (CasStu: FacProf) Data captured on regular basis
Outcome Seamless service across interface between PHC and specialist MH care (CasStu: FacProf)
Improvement in % of service users with appropriate up and down referrals (CasStu: FacProf)
EVALUATION Case study may include:
Facility profile: surveys / qualitative exploration of specialist mental health care / PHC facilities to evaluate functioning of the interface.
MHCP Function ToC Outcome
2.4 Promote rehabilitation and recovery through multi-sectoral approaches and livelihood interventions
z. Interventions for people with chronic schizophrenia receive PSR (incl. livelihoods interventions, peer support, adherence support and psychosocial interventions) are linked to the clinics. People with chronic schizophrenia receive PSR (above) as intended for the required duration and are adequately referred Improved health, social and economic outcomes of people living with priority mental disorders treated by the programme and their families/carers
Cross-country South Africa
Input Community rehabilitation service and SOPs established in the community (CasStu: FacProf)
SA PSR manual adapted and available(CasStu: FacProf) Space for PSR groups available(CasStu: FacProf) Costs of training (CasStu: Res)
Process Community rehabilitation service functioning (CasStu: FacProf)
No. of training courses / Aux. social workers trained (CasStu; TraFid) No. of psychiatric service users assessed for readiness & referred to group who participate(CasStu; MHIS) No. of groups established No. of supervision sessions held (CasStu; FacSurv)
Output % of persons with severe / enduring mental disorder who are employed / engaged in rehabilitation programme / linked with livelihoods initiative (CasStu: FacProf, HMIS)
No. of Aux Soc Workers with competence to run psychosocial rehabilitation groups(CasStu; TraFid) % of persons with severe / enduring mental disorder who participate in rehabilitation programme for required duration (Cohort, Coh: Qual)

[Type text]
Outcome Reduced family burden Change in patient and family clinical, social and economic outcomes (Cohort, Coh: Qual)
Improved clinical and functional outcomes(Cohort) Reduced family burden(Cohort, Coh: Qual) Reduced relapse/repeat admissions(CasStu; MHIS)
EVALUATION
Cohort study of persons with psychosis / severe mental disorders Qualitative exploration with families / persons with SMD / relevant community members Case Study includes Facility profile of services, and collaboration with NGOs, CBOs
INDICATORS FOR COMMUNITY PACKAGES
MHCP Function ToC Outcome
3.1. Improve community awareness and decrease stigma v. Community is aware of mental illness and local availability of treatment. Stigma is reduced and demand for mental health services increased w. People with mental disorders are willing to seek treatment x. Services in the community are perceived to be accessible, affordable and acceptable to people with mental disorders so they are willing to receive intervention
Cross-country South Africa
Input Costs of awareness-raising activities (CasStu: Res) Community caregiver (CCG) training material available(CasStd: FacProf) Costs of developing awareness-raising material/cost of delivery of activities (CasStu: Res)
Process Depends on package(CasStd: FacProf) No. of training sessions / No. of CCGs attending (CasStd:TraFid) No. of media campaigns(CasStd: FacProf)
Output Improved knowledge, attitudes and stigma questionnaire Improved mental health literacy Decreased stigma(ComSurCoh: Qual) Reduced discrimination / abuses (ComSurCoh: Qual)
Outcome No of people who self-referred or were referred by community for treatment. (CasStu: HMIS, FacSurv)
Incr. in no of people who self-referred or were referred by community for treatment. (CasStd:MHIS)FacSurv) Decreased delay inhelp-seeking(CasStu: HMIS)FacSurv Decreased stigma/ discrimination / abuse(FacSurv)

[Type text]
EVALUATION
Community survey of mental health literacy and attitudes Case Study will include: MHIS/ facility survey: referral pathways for new patients attending Cohort: repeated measures of experiences of stigma / discrimination / abuse, Qualitative exploration of experience of living with mental illness
MHCP Function ToC Outcome
3.2 Improve case detection in the community y. People with mental disorders are identified in the community
Cross-country South Africa
Input Detection protocols in place (CasStu: FacProf) Training manuals with detection protocols available(CasStu: FacProf) Training costs (CasStu: Res)
Process No. of sessions / No. of relevant persons attending training(CasStd:TraFid) No. of supervision sessionsCasStu: FacProf)
Output No. of people identified in community by CHW (CasStu: HMIS, FacSurv)
Competence to detect / refer post-training(CasStd:TraFid)
Outcome At aggregate level, relate the total of these Ns from facilities and communities to estimated prevalence of disorders to get measure of coverage of identified and treated cases, respectively Decreased delay before accessing care (ComSur,CasStu: MHIS, Gap)
Increased number of detected cases & appropriate referrals(CasStu: HMIS, FacSurv) Decreased delay before accessing care (CasStu: HMIS, FacSurv) Incr in % follow-up care for mental health by CHWs(CasStu: HMIS, FacSurv
EVALUATION
Community Surveys – delay in seeking care pre- and post- intervention Facility surveys, HMIS - % of referrals deemed appropriate? / No. of referrals coming from the community Estimation of treatment gap: Number of detected and/or treated cases/prevalence of disorder
4. ToC Map (attachment)

[Type text]
5. Collaborative Care models
Back referral to local clinic for continued management
PHC nurse identifies depression and other mental disorders as well as other non-
communicable diseases (NCDs) using PC101. Initiates initial management of other NCDs.
Other mental disorders and NCDs including diseases of lifestyle which are inadequately controlled referred to PC
doctor/ other referral sources
If severe depression with suicide risk refer for out patient/ specialist care
9 to 10 weeks re-assessment by PHC nurse using PC101 post
the psychosocial interventions
Referral to psychosocial group
intervention sessions facilitated by lay counselors and supervised by mental
health coordinator
Referral to PC doctor for assessment & diagnosis and initiation of
psychopharmacological treatment and/ or referral to group intervention
or upward referral if suicide risk
Mild-moderate/severe depression
Severe/moderate depression
The collaborative care intervention for depression
[Type text]
[Type text]
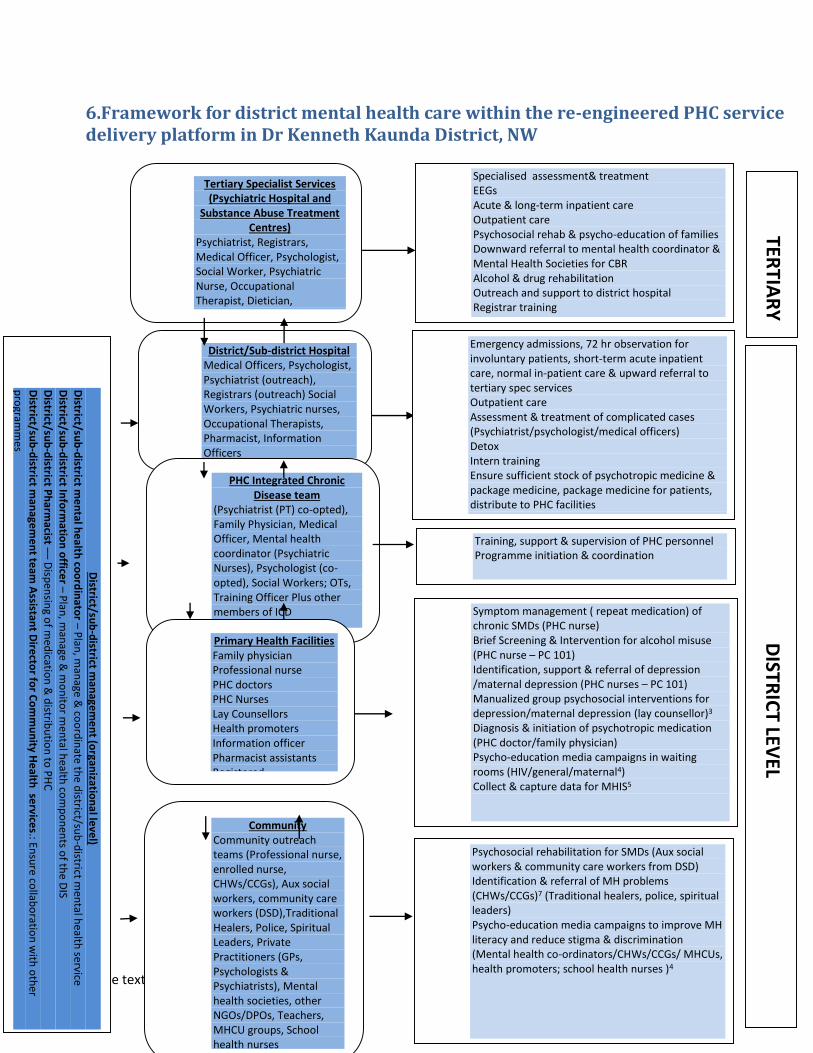
6.Framework for district mental health care within the re-engineered PHC service delivery platform in Dr Kenneth Kaunda District, NW
Tertiary Specialist Services (Psychiatric Hospital and
Substance Abuse Treatment Centres)
Psychiatrist, Registrars, Medical Officer, Psychologist, Social Worker, Psychiatric Nurse, Occupational Therapist, Dietician, biokinetecist, pharmacist, neurologist (P/T), EEG technician , Information Officers
District/Sub-district Hospital Medical Officers, Psychologist, Psychiatrist (outreach), Registrars (outreach) Social Workers, Psychiatric nurses, Occupational Therapists, Pharmacist, Information Officers
PHC Integrated Chronic
Disease team (Psychiatrist (PT) co-opted), Family Physician, Medical Officer, Mental health coordinator (Psychiatric Nurses), Psychologist (co-opted), Social Workers; OTs, Training Officer Plus other members of ICD
Primary Health Facilities Family physician Professional nurse PHC doctors PHC Nurses Lay Counsellors Health promoters Information officer Pharmacist assistants Registered B.Psychcounsellors ?? Intern Clinical Psychologist
Community Community outreach teams (Professional nurse, enrolled nurse, CHWs/CCGs), Aux social workers, community care workers (DSD),Traditional Healers, Police, Spiritual Leaders, Private Practitioners (GPs, Psychologists & Psychiatrists), Mental health societies, other NGOs/DPOs, Teachers, MHCU groups, School health nurses
Specialised assessment& treatment EEGs Acute & long-term inpatient care Outpatient care Psychosocial rehab & psycho-education of families Downward referral to mental health coordinator & Mental Health Societies for CBR Alcohol & drug rehabilitation Outreach and support to district hospital Registrar training
Training, support & supervision of PHC personnel Programme initiation & coordination
Symptom management ( repeat medication) of chronic SMDs (PHC nurse) Brief Screening & Intervention for alcohol misuse (PHC nurse – PC 101)
Identification, support & referral of depression /maternal depression (PHC nurses – PC 101)
Manualized group psychosocial interventions for depression/maternal depression (lay counsellor)3
Diagnosis & initiation of psychotropic medication (PHC doctor/family physician) Psycho-education media campaigns in waiting rooms (HIV/general/maternal4) Collect & capture data for MHIS5
Psychosocial rehabilitation for SMDs (Aux social workers & community care workers from DSD) Identification & referral of MH problems (CHWs/CCGs)7 (Traditional healers, police, spiritual leaders)
Psycho-education media campaigns to improve MH literacy and reduce stigma & discrimination (Mental health co-ordinators/CHWs/CCGs/ MHCUs, health promoters; school health nurses )4
TERTIA
RY
DISTR
ICT LEV
EL
District/su
b-d
istrict man
agem
en
t (organ
ization
al le
vel)
District/su
b-d
istrict me
ntal h
ea
lth co
ord
inato
r – Plan
, man
age & co
ord
inate th
e district/su
b-d
istrict men
tal health
service
District/su
b-d
istrict Info
rmatio
n o
fficer – P
lan, m
anage &
mo
nito
r men
tal health
com
po
nen
ts of th
e DIS
District/su
b-d
istrict Ph
armacist –– D
ispen
sing o
f med
ication
& d
istribu
tion
to P
HC
D
istrict/sub
-district m
anage
me
nt te
am A
ssistant D
irecto
r for C
om
mu
nity H
ealth
service
s.: Ensu
re collab
oratio
n w
ith o
ther
pro
gramm
es
Social C
luste
r Me
etin
gs: Intersecto
ral collab
oratio
n
Emergency admissions, 72 hr observation for involuntary patients, short-term acute inpatient care, normal in-patient care & upward referral to tertiary spec services Outpatient care Assessment & treatment of complicated cases (Psychiatrist/psychologist/medical officers) Detox Intern training Ensure sufficient stock of psychotropic medicine & package medicine, package medicine for patients, distribute to PHC facilities

[Type text]
7. Table of human resource mix, services provided and tools available to assist in the provision of services Health provider Services Tools
DISTRICT MANAGEMENT (ORGANIZATIONAL) TIER
District Management Team (MH represented by Assistant Director: Community Health Services)
Management of programmes e.g., maternal health, HAST (HIV/AIDS/STIs/TB).
Ensure collaboration with other services
District/sub-district meetings of programmes
District/sub-district PHC coordinator
Attend social cluster meetings to promote intersectoral collaboration
Collaborative meetings
Information officer Plan, manage and monitor the mental health components of the district information system.
MHIS (to be negotiated)
Provincial Indicator Data Set, DHIS
Patient Register in terms of section 39 of the Regulations to the Mental Health Care Act No 17 of 2002 for health establishments that render mental health services
District/sub-district Pharmacist
Ensuring sufficient stock of psychotropic medication
Dispensing of medication & distribution to PHC
Packaging of psychotropic medication for patients
Standard Treatment Guidelines and Essential Drug List – Hospital level Adults 2006
Standard Treatment Guidelines and Essential Medicines List for Primary Health Care 2008
District/sub-district MH coordinators
Plan, manage & monitor the district/sub-district mental health services
Attending sub-district management meetings
District/sub-district mental health care plan
Health provider Services Tools
TERTIARY HOSPITAL TIER
Psychiatrist
Assessment, diagnosis and holistic treatment (including psychiatric treatment) of in-patients/out-patients
Consultation-liaison service for PHC doctors and other mental health specialists (outreach & support)
Hospital protocol
Standard Treatment Guidelines and Essential Drug List – Hospital level Adults 2006

[Type text]
Training & supervision of registrars
Clinical Psychologist
Assessment, diagnosis and psychological treatments for in-patients and outpatients
Psycho-education of patients/families
Training of intern psychologists
Hospital protocol
Psychiatric nurse In-patient care/out-patient nursing care
Psycho-social rehabilitation
Psycho-education of families
Hospital protocol
Clinical Social Worker
Family assessment and psycho-education
Psych-education of families
Placement in alternative accommodation and/or sheltered workshops on discharge
Assist psychiatric patients with applications for disability grants
Hospital protocol
Occupational Therapist
Assessment and psycho-social rehabilitation Hospital protocol
Pharmacist Orders & dispenses medication Hospital protocol and EDL
Dietician Prepares menus Hospital protocol
Neurologist (P/T) Assesses EEGs Hospital protocol
Information officer Capture, and manage patient records District Information system
Health provider Services Tools
DISTRICT HOSPITAL TIER
Clinical Psychologist
Assessment, diagnosis and psychological treatments for in-patients (emergency admissions, 72 hr observation of involuntary patients, short-term acute inpatient care, normal in-patients & upward referral to tertiary spec services
Psychological referral service for complicated cases and more severe mental disorders
Training of intern psychologists
Support to PHC level
MH Care Act
Hospital protocol
Medical Officers Assessment, diagnosis and medical treatments for MH Care Act

[Type text]
mental disorders and other co-morbid medical conditions for in-patients/outpatients
Detox of substance abuse cases
Hospital protocol Standard Treatment Guidelines and Essential Drug List for Hospital level Adults 2006
Psychiatrist (P/T) Assessment, diagnosis and psychiatric treatment for in-patients (emergency admissions, 72 hr observation of involuntary patients, short-term acute inpatient care, normal in-patients & upward referral to tertiary spec services
Psychiatric referral service for confirmation and adjustment of diagnoses and treatment regimes for more complex psychiatric cases.
MH Care Act
Hospital protocol
Standard Treatment Guidelines and Essential Drug List for Hospital level Adults 2006
Psychiatric nurses In-patient care/out-patient nursing care
Hospital protocol
Pharmacist Ensure sufficient stock of medicine, package medicine for patients, distribute to PHC facilities
EDL
Hospital protocol
Health Provider Services Tools
PHC SPECIALIST TEAM
District/sub-district Chronic care co-ordinators (PHC Specialist team)
Training and support of PHC nurses in the emergency management and ongoing psychopharmacological treatment of psychiatric patients
Linking discharged psychiatric patients with community-based psychosocial rehab programme
Training of traditional healers, spiritual leaders, police in identification and referral of mental disorders
Media campaigns to increase mental health literacy and reduce stigma and discrimination in the clinics & community
MH Care Act & DoH training materials
Hospital protocol
Collaborative care model for schizophrenia
Existing training protocol
SAFM material

[Type text]
Psychiatrist (P/T) Psychiatric referral service for confirmation and adjustment of diagnoses and treatment regimes for more complex psychiatric cases.
Standard Treatment Guidelines and Essential Drug List for Hospital level Adults 2006
Psychologist /Intern Psychologist
Referral psychological service for patients requiring more complex psychological treatments.
Training, supervision and support for mental health coordinators & lay counsellors.
Attending district mental health management meetings
Hospital protocol
Manualized psychosocial interventions developed by PRIME-SA
Family Physician Training, supervision and support for PHC doctors and nurses in identification and management of mental disorders
PC 101+
Health Provider Services Tools
PHC FACILITY TIER
PHC doctors Diagnosis of mental disorders & other co-morbid medical conditions
Management of comorbid medical conditions.
Initiation of psychotropic medication
Referral of mild-moderate/severe depression cases to lay counselors for the provision of manualized group/individual psychosocial interventions for depression co-morbid with chronic conditions/maternal depression
Onward referral of complex and severe cases to district outpatients services/psychiatric hospital
Brief Screening & Intervention for alcohol misuse
Emergency management and referral of patients
PC 101+
PC 101+
PC 101+
Collaborative care model using referral protocol
PC 101+, Mini Drug Master Plan 2011/12-2012/13
PC 101+ & Clinic protocol
Standard Treatment Guidelines and Essential Medicines List for Primary Health Care 2008

[Type text]
with acute psychiatric conditions to the district hospital
Primary health care nurse (incl. at general, ante-natal, post-natal and chronic care)
Emergency management and transfer of acute psychiatric conditions to the district hospital
Ongoing symptom management of chronic psychiatric conditions - repeat medication
Identification of depression using PC 101 and referral
Brief Screening & Intervention for alcohol misuse (PC 101)
Record information on service users with mental disorders
Management/referral of co-morbid medical conditions
PC 101+ & Clinic protocol
Clinic protocol
PC 101+ & referral protocols using collaborative care model
PC 101+
MHIS
PC101+
Standard Treatment Guidelines and Essential Medicines List for Primary Health Care 2008
B. Psych Counsellor/ PHC Psychologist/Intern Psychologist
Training and support of HIV counselors in the provision of manualized group/individual psychosocial interventions for depression
Individual counseling referral service
Manualized counselling intervention developed by PRIME-SA
HIV counselor Facilitation of manualized individual and structured group-based psychosocial interventions for depression.
Pre- and post HCT counselling
Manualized counselling intervention developed by PRIME-SA
Information officer Capture, and manage mental health components of the information system
MHIS developed by PRIME & clinic protocols
District Health Information System
Health Provider Services Tools
COMMUNITY TIER
Community health workers
Identification & referral of people with mental disorders
Psycho-education on mental illness and stigma and discrimination
2nd Phase DoH training manual for CHWs
2nd Phase DoH training manual for CHWs
2nd Phase DoH training manual for CHWs

[Type text]
Follow-up and adherence counseling for patients who default on their medication
Mental health promotion
Conduct household visits inclusive of mental health care.
Referral of MHCUs in need of facility (clinic or hospital) care
1st Phase DoH training manual for CHWs
2nd Phase training manual for CHWs (referral document)
Social workers Assisting psychiatric patients in their applications for disability grants
Training and supervision of auxiliary social workers in the delivery of community-based psychosocial rehabilitation
DSD protocol
PSR training manual
Auxiliary social workers
Group-based psychosocial rehabilitation for MHCUs with severe chronic mental disorders
PRIME-SA psychosocial rehab manual
User Groups NGOs
Psycho-educational campaigns to improve MH literacy and reduce stigma and discriminations
Material from Federation for Mental Health