social care policy in québec
DESCRIPTION
A brief presentation on preliminary analysis of what should constitute the social criteria for public long-term care in Québec. Une analyse préliminaire de ce que peuvent être les critères sociaux d'une politique des soins de longue durée au Québec.TRANSCRIPT

Social Care Policy
“It is surely part of the evidence that the state doesn’t provide the cradle-to-grave care. It still depends fundamentally upon the family above all and to a lesser extent on friends, neighbours, and voluntary organizations to provide the routine day-to-day care of individuals who are dependent – infants, sick, disabled and the last stages of life.”
Hill, Michael, Bramley, G., (1986). Analysing Social Policy, Blackwell publishers

Agenda
Research focus: Comparative/evaluative research
Context:
Demography
Demography and health related issues
Financial considerations
Social Policy Criteria:
Values/Rights
Principles
Objectives
Existing/Proposed Systems/Regimes for long-term care
Quebec initiatives as outlined in public inquiry commissions
Other initiatives

Research Focus Comparative/Evaluative Inquiry into some aspects of a
potential Long-Term Care social policy for Québec
Potential inquiry Focus: Given some social desirable criteria – to be determined -, compare or evaluate different combinations of social services regimes to attain those goals taking into account constraints from the context.
-
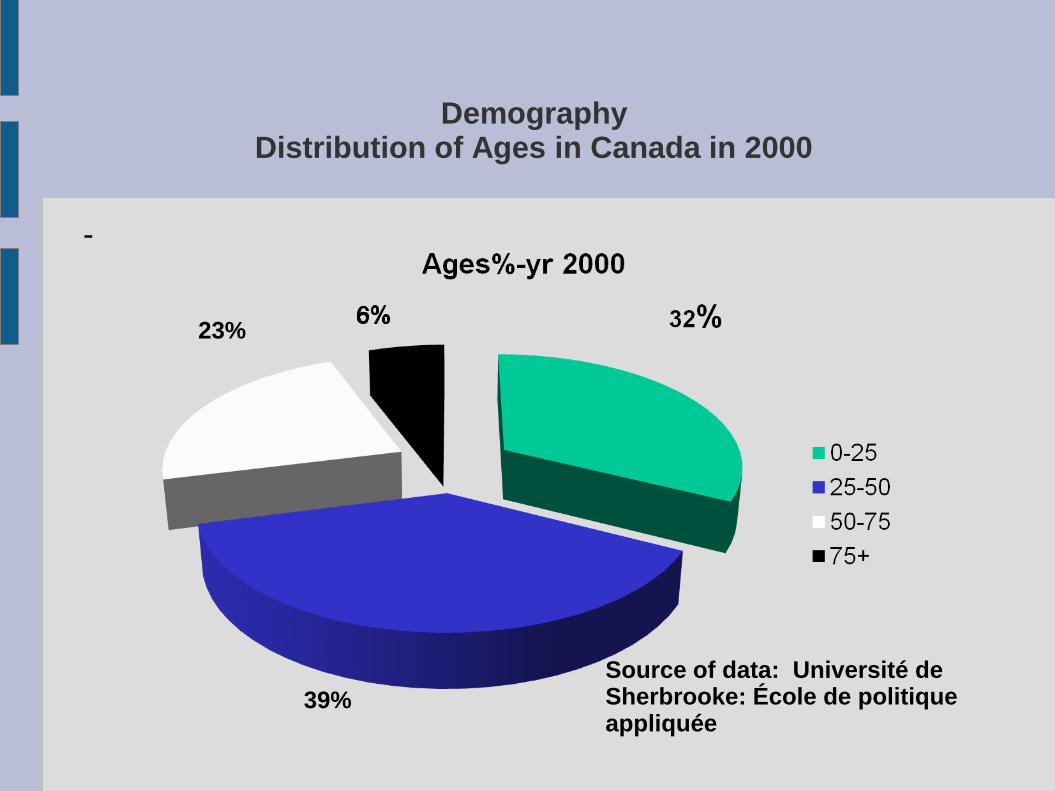
Demography Distribution of Ages in Canada in 2000
-
Source of data: Université de Sherbrooke: École de politique appliquée
23%
39%
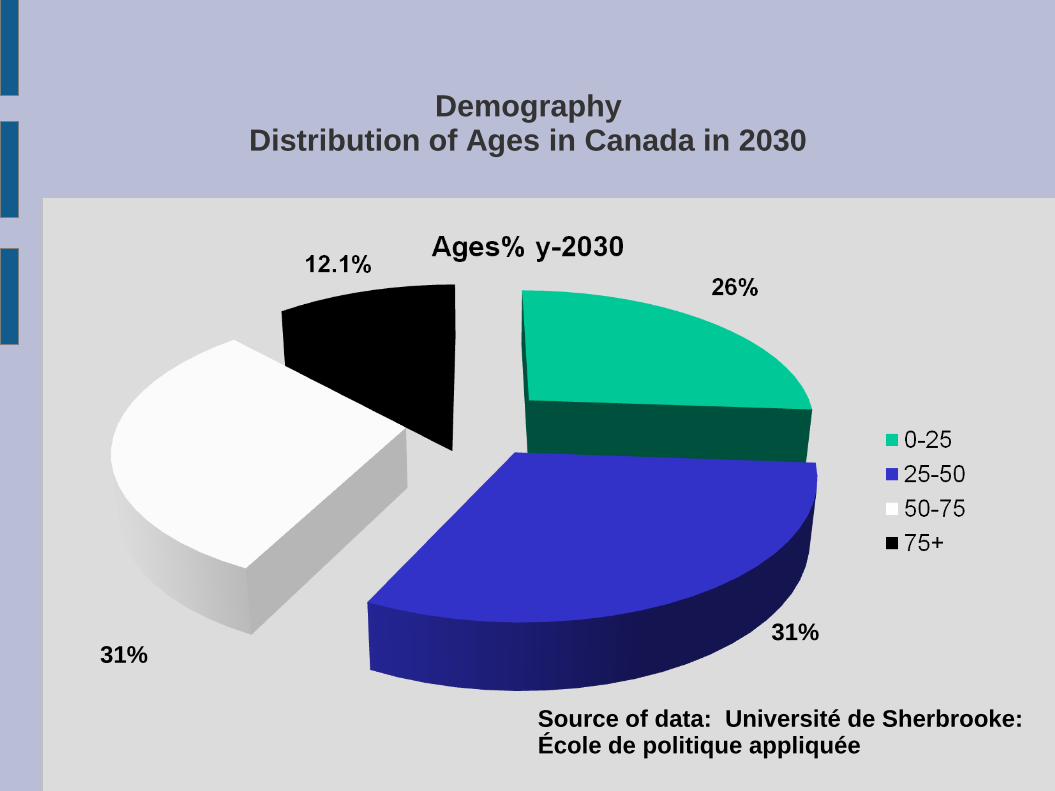
Demography Distribution of Ages in Canada in 2030
31% 31%
Source of data: Université de Sherbrooke: École de politique appliquée

Demography Distribution of Ages in Cameroun
1.5%
Source of data: Université de Sherbrooke: École de politique appliquée
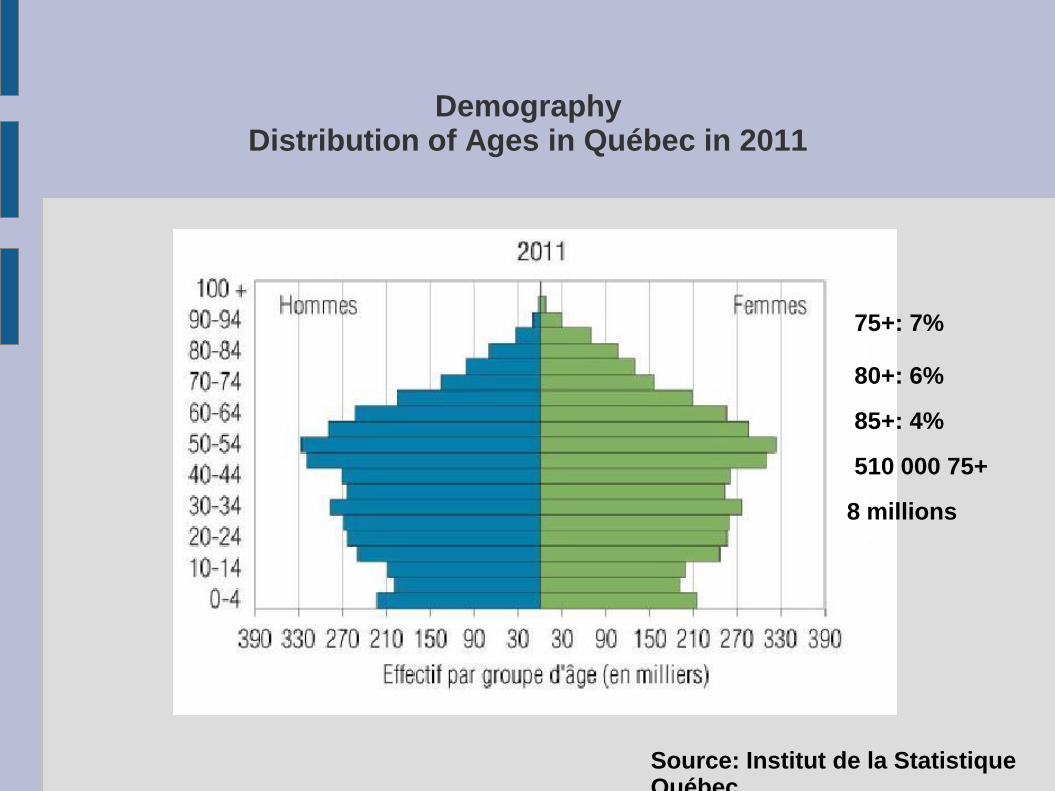
Demography Distribution of Ages in Québec in 2011
Source: Institut de la Statistique Québec
75+: 7%
80+: 6%
85+: 4%
510 000 75+
8 millions

Demography Distribution of Ages in Québec in 2031
Source: Institut de la Statistique Québec
75+13%
80+: 7% 85+: 4%
1 168 000 75+
9 200 000
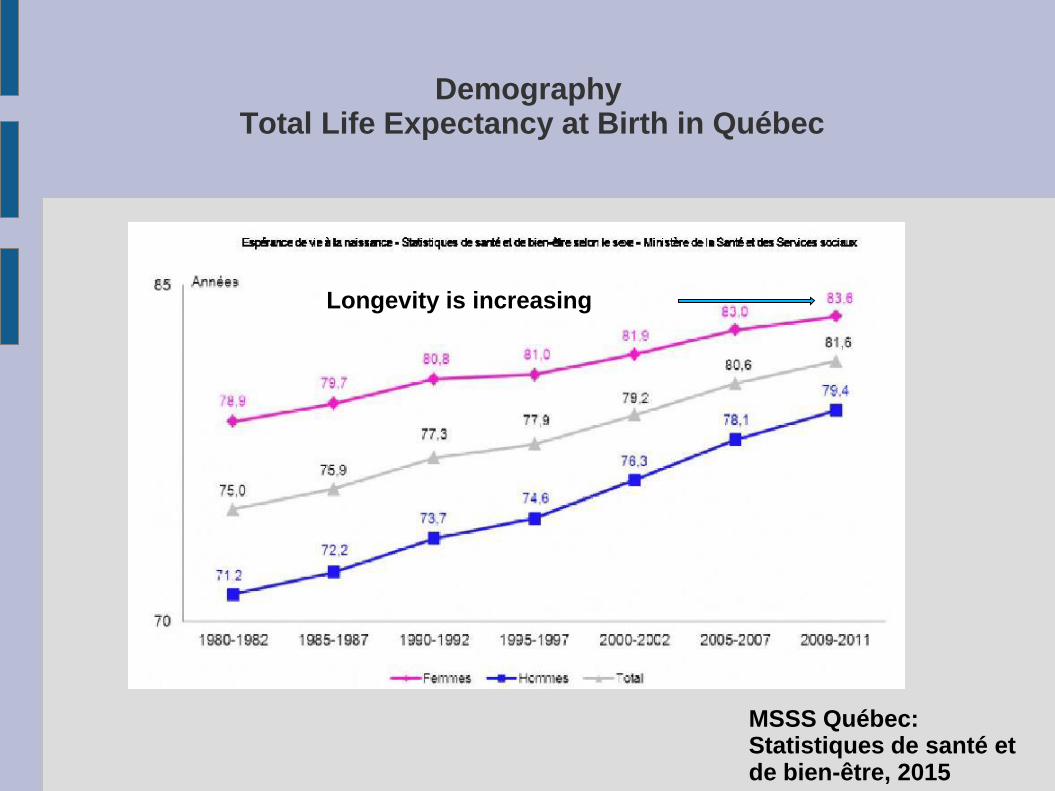
Demography Total Life Expectancy at Birth in Québec
MSSS Québec: Statistiques de santé et de bien-être, 2015
Longevity is increasing

Demography and Health
(MSSS: no limitations in daily activities nor incapacities)
MSSSQuébec: Statistiques de santé et de bien-être, 2015
∆:10 years for both men and women but starting at a different age →
Women live longer and more than often will be the one providing the informal care

Demographic and Health Different perspectives
Bourbeau, Robert, (2006), Évolution de l’espérance de vie au Québec: tendances récentes et perspectives, UdM Démographie

Demographic and Health Different perspectives
Bourbeau, Robert, (2006), Évolution de l’espérance de vie au Québec: tendances récentes et perspectives, UdM Démographie

Demography and Health Factors that impact longevity
Source: Centers for Medicare and Medicaid Services. (2012), Dpt of health and human services USA

Demography and Health Factors that impact longevity
Source: Centers for Medicare and Medicaid Services. (2012), Dpt of health and human services USA

Demography and Health Factors that impact longevity
Source: Centers for Medicare and Medicaid Services. (2012), Dpt of health and human services USA

Demography and Health Impact: Limitations in activities
Statistiques Canada, Enquête sur la santé dans les collectivités canadiennes (ESCC) 2009-2010, in Plan commun de surveillance produit par l’Infocentre de santé publique de l’Institut nationale de santé publique du Québec(2012)
1:limitation in activities: home, work, school, or other impacts resulting from a health, mental, or other circumstances.
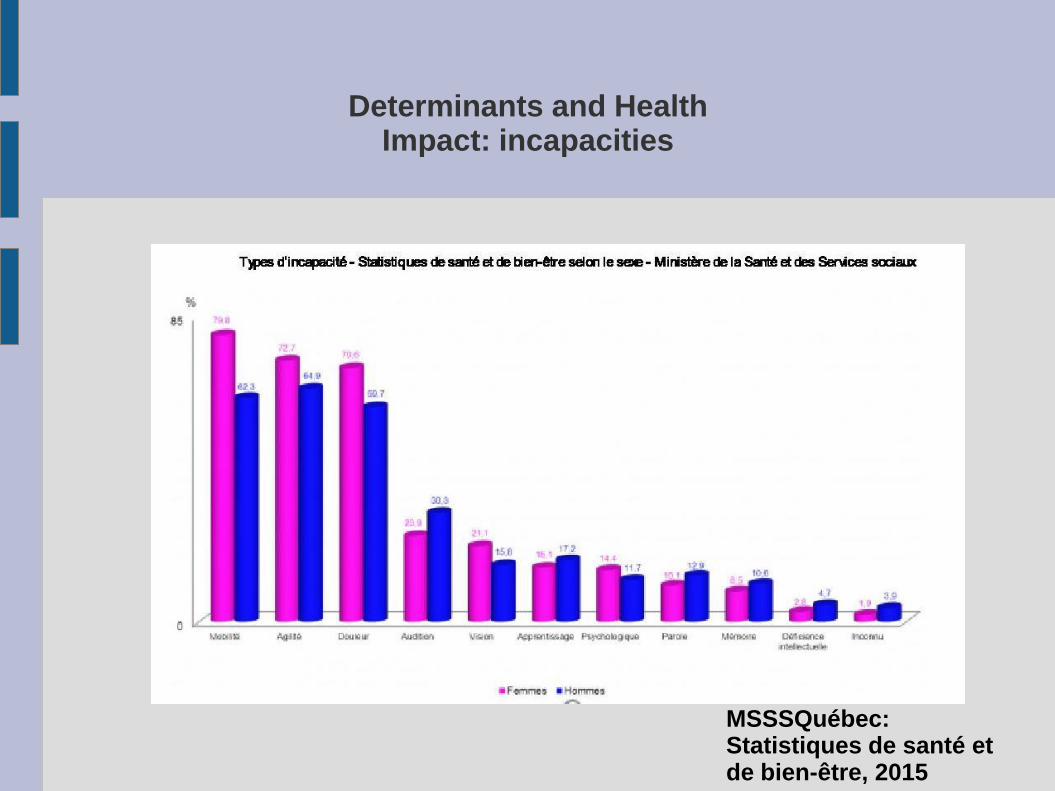
Determinants and Health Impact: incapacities
MSSSQuébec: Statistiques de santé et de bien-être, 2015

Financial Considerations
Cirano (2015). Le Québec économique
Around 5%

Social Policy Criteria
• “If we wish to study welfare states, we must begin with a set of criteria that define their role in society” (Esping-Andersen,
(1990). The Three Worlds of Welfare, Princeton University Press)
• Social rights as: “the whole range from the right to a modicum of economic welfare and security to the right to share to the full in the social heritage and to live the life of a civilized being according to the standards prevailing in the society.” (Marshall, T.H. (1992). Citizenship and Social Class, p.74).
Social Policy Criteria
• Policy Values/Rights
• Policy Principles
• Policy Objectives

Social Policy Criteria Source: existing social actors
Bourque, Mélanie, Leruste, G., (2010). La transformation des idées sur la privatisation du système de santé québécois depuis 1970 : le passage à un nouveau référentiel sectoriel ?, Politiques et Sociétés, vol 29. no2, p.105-129
Principles Values Objectives
Social Policy Criteria: Values Source: theoretical researchers
• Value: According to (Hick, Steven (2004), Social Welfare in Canada: Understanding Income Security):
• Deserving vs under-deserving
• economic security/disincentive to work
• amount of assistance lower than lowest job pay
• basic subsistence (means-tested) vs Adequate living standards ( needs test)
• fact-of-need (notion of risk) vs cause-of-need(personal cause of one’s problem
• Right: Council of Europe(European Social Charter (ESC): social and economic rights…including « the right to social welfare services, the right to social and medical assistance. »
Social Policy Criteria: Values Source: proponents of new paradigm
Values from the Social Investment Welfare State paradigm
• modernization of welfare systems in order to address the issue of growing poverty and social exclusion
• better respond to the new needs and new social risk structures of contemporary society
• make welfare systems sustainable
• make them ‘productive’ in the sense that they should promote and support employment and economic growth.
• Central to this modernisation of welfare systems is the idea that social policy should aim at ‘preparing’ the population to prevent certain social and economic risks associated with changing employment conditions and family patterns, and to minimise the intergenerational transfer of poverty, rather than at ‘repairing’ through passive income maintenance schemes after the risk has occurred.
• Source:
Bruno, Palier, Palme, J., Morel, N., (2012), Towards a Social Investment Welfare State? : Ideas, Policies and Challenges, Bristol Policy Press
Social Policy Criteria: Values Source: Rights movement
• Evolution from a gift to a right: « Bonapartist welfare » to a broader collectivisation of social risks.
• Bismark(1880s): right, per contingency, limited to workers, based on the « equivalence principle » : contributions, benefits, risks - « Assurance part »
• Beveridge(1942) : « Protect citizens from proverty. », more universal right, comprehensive but basic, the « solidarity principle. »
• UN 1948 convention, article 22 « Everyone, as a member of society, has a right to social security. »
• International Convenant on Economic, Social and Cultural Rights (1966) – Article 9 -: right to social security.
• International Labour Conference ( 1944): Broad view of social security…for the provision of ‘a basic income to all in need of such protection’.
• European Code of Social Security(1964)
• France, Code de la sécurité sociale: 5th risk of old-age
• Canada. We don’t seem to have taken this view. Maybe we should?
Social Policy Criteria: Values Source: social security field
Social Policy Criteria: Principles Source: existing laws
• Principle of subsidiarity:
• « This concept has a long standing tradition in Roman Catholic ethics and came to be incorporated into German social law some 30 years ago. According to the Subsidiaritätsprinzip,an individual’s well-being is first his or her own responsibility,then an issue of family solidarity or community support and only then a concern of public entities such as municipalities or regional states (Schneider, Ulrick,1999 « Germany's social long-term care insurance: Design, implementation, evaluation », International Social Security Review, vol. 52)
• Principles as found originally in the Canadian Health Act relevant to long-term care? « Most participants support the Canada Health Act, but there is no real
agreement on what it means or stands for.” (Summary of Input on the Conversation on Health:Canadian Health Act and its Principles, British Columbia Government)
• Public Administration
• Comprehensiveness, Universality and Portability
• Accessibility and Medically Necessary
• Sustainability, Patient-Centered (proposed new ones!)
Social Policy Criteria: Principles Source: social security
• Adequacy of benefits to ensure that as much insecurity as possible can be prevented and more still significantly reduced in extent and time;
• Optimum coverage to ensure that as many as possible are eligible for protection;
• Maximum takeup of benefits to ensure that as many as possible of those covered are in fact protected when they are vulnerable;
• Regular upgrading to ensure that benefits remain adequate to protect beneficiaries and any dependants from insecurity and poverty.
Source: Sinfield, Adrian. (2012) Strengntening the prevention of social insecurity,
International social security review, no 66

Social Policy Objective Source: top-bottom/bottom-up Objectives
• « vieillesse »: being/feeling old, a social construction
• « vieillessement: » natural process of loosing one’s physical and adaptability capacities
• Dependencies:
• Dr Jean-Pierre Aquino, rappelait que " la dépendance n'est pas liée à l'âge, mais à des situations pathogènes de nature médicales, psychologiques ou sociales.
• Autonomy: capacity to manage/live with one’s multiple dependencies.
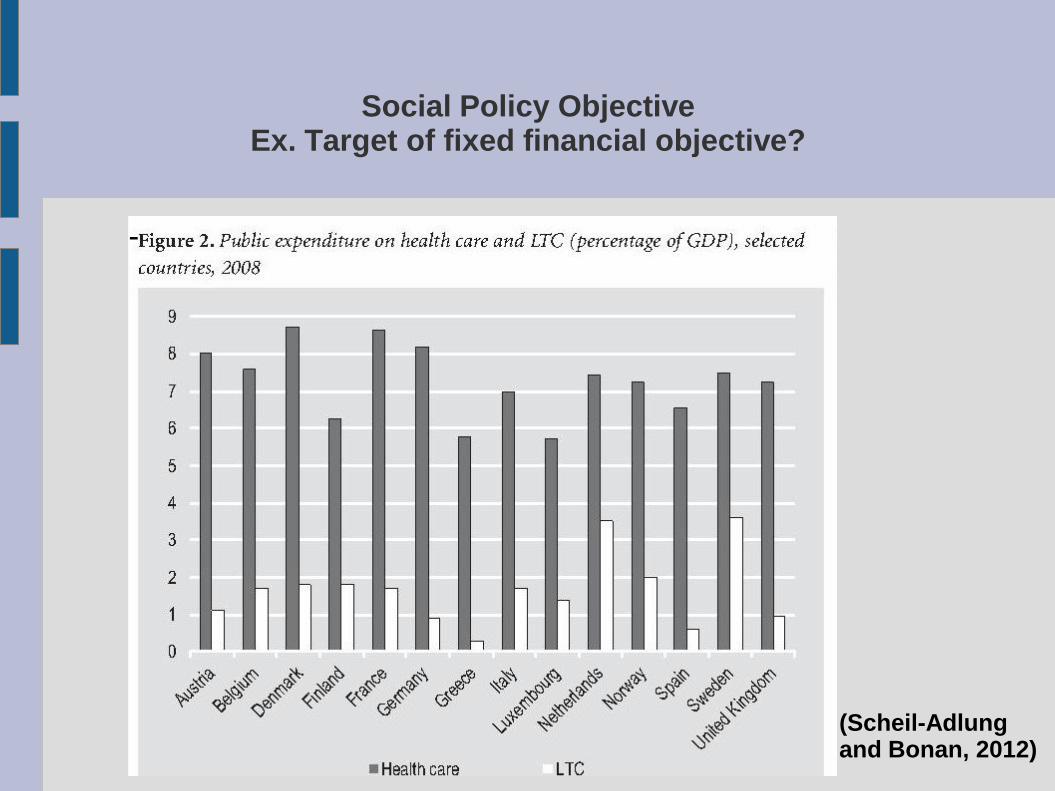
Social Policy Objective Ex. Target of fixed financial objective?
-
(Scheil-Adlung and Bonan, 2012)
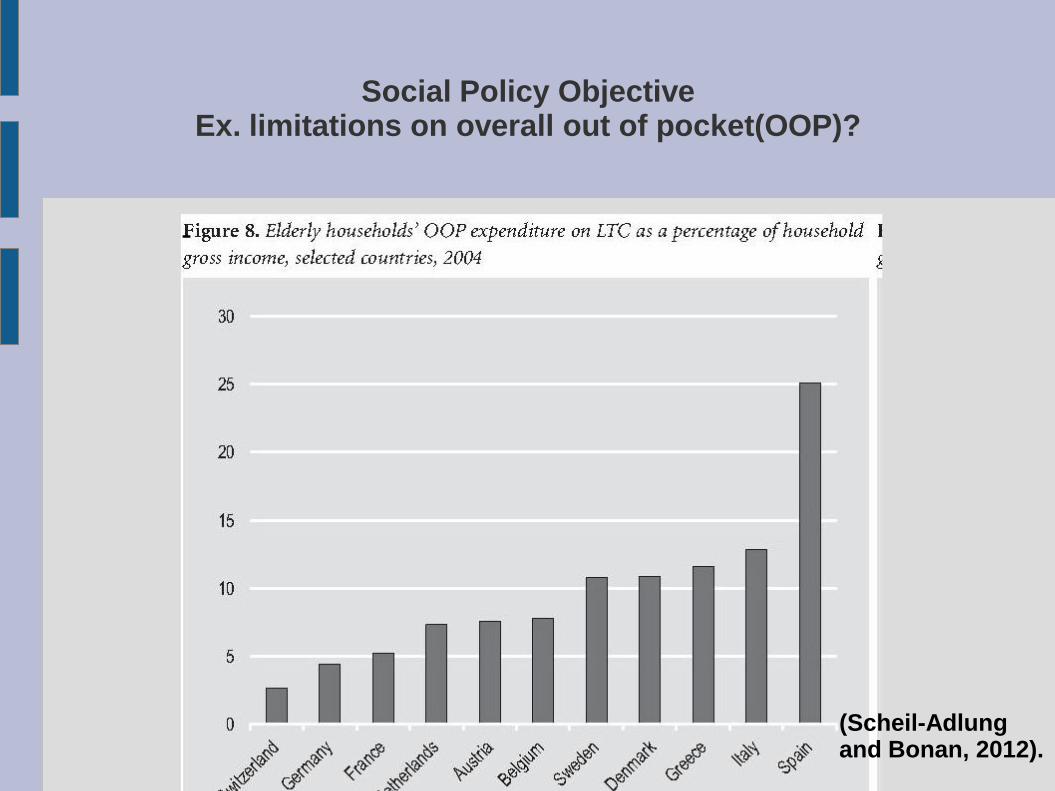
Social Policy Objective Ex. limitations on overall out of pocket(OOP)?
-
(Scheil-Adlung and Bonan, 2012).
Social Policy Objective Type of situation protected against
-Katz' Index of Independence in Activities of daily living (ADL)
-Institut de la santé publique : functional limitations
-Proposed Assurance-autonomie du Québec : autonomy
-Europe: dependency
Ex. Germany Dependency care social insurance: « illness basically can be treated and will lead to recovery, whereas a “state of dependency on care” is irreversible, cannot be cured and ultimately excludes the client from the labour market. » (Sceiner, 1999)
-Other potential definitions:
• incapacity/chronically illness
• invalidity/infirmity/handicapped
• deficiency in physical/cognitive. Federal tax system

Social Policy Objective Type of situation protected against
• Disability: "the ... result of complex relationships between an individual's health condition and personal factors, and of the external factors that represent the circumstances in which the individual lives“ (WHO (2001). The
International Classification of Functioning, Disability and Health)
• Disability: restrictions in the ability to perform activities of daily living (ADL), or, the inability to function independently in terms of basic ADL or instrumental ADL (WHO. 2003)
• In gerontology: 'the disablement process’: a dynamic interaction intimately tied to cultural norms and socioeconomic status encompassing attitudes, emotions, stigma, accessibility or lack thereof of various services, wheelchair accessible buildings, etc.

Social Policy Objective Type of situation protected against
Kathz’ Index of ADL

Social Policy Objective Type of incapacity protected against

Social Policy Objective Type of incapacity protected against

Existing/Proposed Systems/Regimes for Long-Term Care Potential sources of data
• Quebec public commissions
• Canada royal commissions
• « Les commissions d’enquête, d’étude et les groupes de travail constituent des lieux importants de débats liés aux politiques publiques et à l’intervention de l’État (Denis, 2001) »
• « Il ne fait aucun doute qu’ils constituent des laboratoires d’idées pour les gouvernements »(Firbank, 2008)
• Canadian public/private advocacy groups
• International groups: World Bank, OECD
• Other countries’ system of long-term care: France, Scotland, UK, Netherlands, Japan, Singapore, US
Main Quebec Public Inquiry Commissions
• Commission Montpetit, 1933
• Commission d’enquête sur l’assurance-hospitalisation, (Favreau) 1960
• Commission Castonguay-Nepveu, 1969-1972
• Commission Rochon, 1988
• Groupe de travail sur la complémentarité du secteur privé dans la poursuite des objectifs fondamentaux du système de santé au Québec (Arpin) 1999
• Commission Clair, 2001
• La politique de soutien à domicile Chez soi : le premier. MSSS, 2003
• Comité de travail sur la pérennité du système de santé et de services sociaux du Québec (Ménard) 2005
• Groupe de travail sur le financement du système de santé (Castonguay) 2008
• Rapport du comité d'experts sur l'avenir du système de retraite québécois (d’Amours), 2013
• Projet d’assurance-autonomie, 2013

Commission Montpetit
Commission Montpetit(1933):Commission des assurances sociales
Mostly focused on income security Mandate:
Faire une étude aussi complète que possible des questions suivantes et de la manière dont les
problèmes qu'elles comportent peu-être réglés dans la Province de Québec: assurance du vieil
âge; assurance contre le chômage; assurance contre la maladie; assurance contre l'invalidité;
assistance aux mères nécessiteuses; placement familial; mode d'adoption et placement des enfants
adoptés; assistance aux familles nombreuses; conditions sanitaires des établissements industriels
et des travailleurs dans ces établissements; maladies professionnelles; inspection médicale des
ouvriers employés aux travaux dangereux; secours médicaux à l'atelier; éducation sanitaire de
l'ouvrier et tous autres problèmes d'assurances sociales. Étudier la législation des pays étrangers
sur ces différents sujets et l'application qu'ils en ont faite. Se rendre compte sur place, si
nécessaire, de cette application, en vue de l'adaptation de telle législation à notre population, en
tenant compte des conditions spéciales à la Province de Québec. Faire comparaître toute personne
intéressée à ces questions afin d'entendre leurs témoignages et de requérir des rapports de toute
autre personne qu'elle jugera à propos. Faire rapport de temps à autre, au Lieutenant-Gouverneur
en Conseil, des progrès de son travail et de ses recommandations.

Commission Montpetit 5th report on old-age
Mostly focused on the concept of public insurance against old-age

Commission Montpetit 5th report on old-age
P.148
Loi 1927 where federal gov. shared 50% of the cost old-age assistance program.
Other Quebec Public Inquiry Commissions
Commission d'enquête sur la santé et le bien-être social (Castonguay-Nepveu, 1969-1972)
Martin, Jean-Marie, 1970. Pour une politique de la vieillesse (to do)
Commission d'enquête sur les services de santé et les services sociaux (Rochon, 1988)
• Mandate :« Évaluer le fonctionnement et le financement du système des services de santé et des services sociaux connexes. »
• 6000 individuals consulted, 400 experts, own research

Commission Rochon
Persons above 65, only 8.8% of population but 37.4% of all health exp.
Society must encourage autonomy so as to reduce potential “handicap”
Takes the position that family must care for its older citizens, so the State has a residual role.
Notes a difference between anglophones and francophones
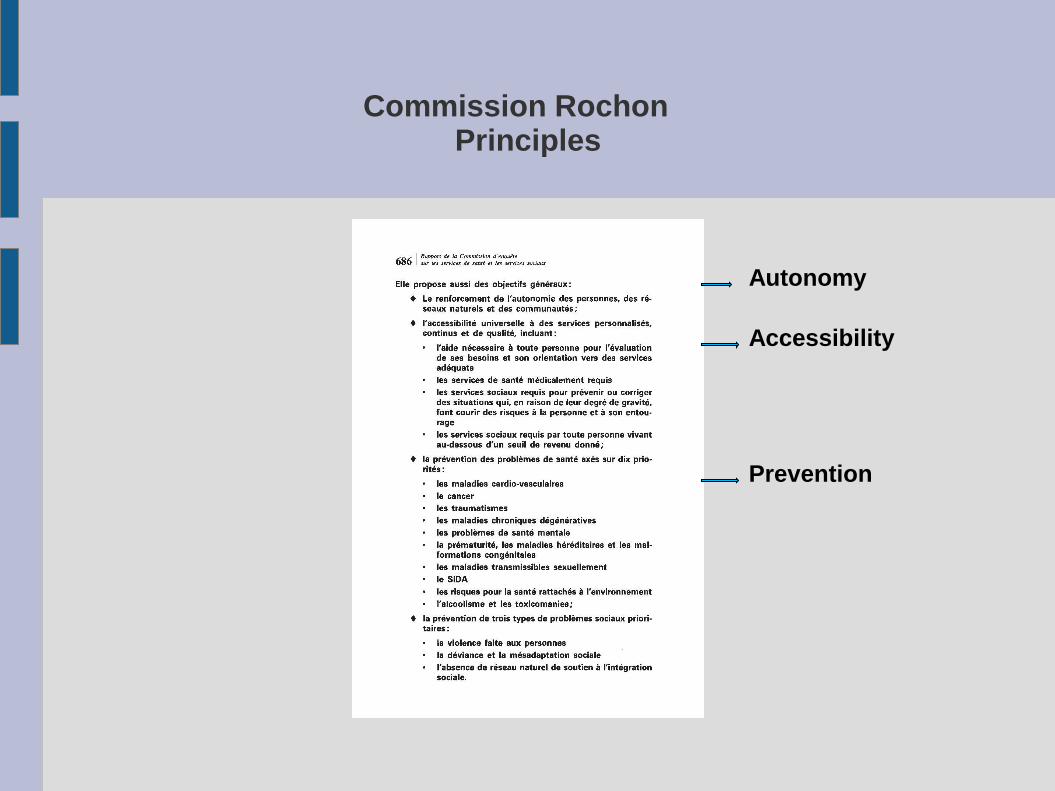
Commission Rochon Principles
Autonomy
Accessibility
Prevention

Commission Rochon Principles
Develop autonomy not just maintain autonomy/compensate the loss of autonomy
Input by potential beneficiaries
Supporting natural networks/communities Adapting environment: residual state

Commission Rochon Principles
Public financing for covered services and through the tax system
The 50% cost sharing with federal government is eroding for the health covered services
Negotiates a new agreement with federal government for universal access to social services
Commission Clair(2000)
Mandate : « tenir un débat public sur les enjeux auxquels fait face le système de santé et de services sociaux et proposer des avenues de solution pour l’avenir. …. le financement et l’organisation des services. »

Commission Clair
Proposes the same concept as was proposed by Commission Montpetit in 1933!

Commission Clair Values
Both a personal and collective benefit and responsibility
Maintain health but assume collectively some risks.

Commission Clair Principles
Health system based on the notion of insurance and risk
Notion of risk has disappeared to be replaced by a notion of right
Il y donc a à la base une nécessité évidente de revenir au concept original d’un « système d’assurance collective » administré par l’État et financé par nos taxes et nos impôts. Il faut revoir et préciser quels sont les services assurés, dans quel délai raisonnable sont-ils offerts, pour qui, auprès de qui et où. Il faut définir l’organisation de services la plus pertinente et comment en assurer une gestion efficace. P. 136
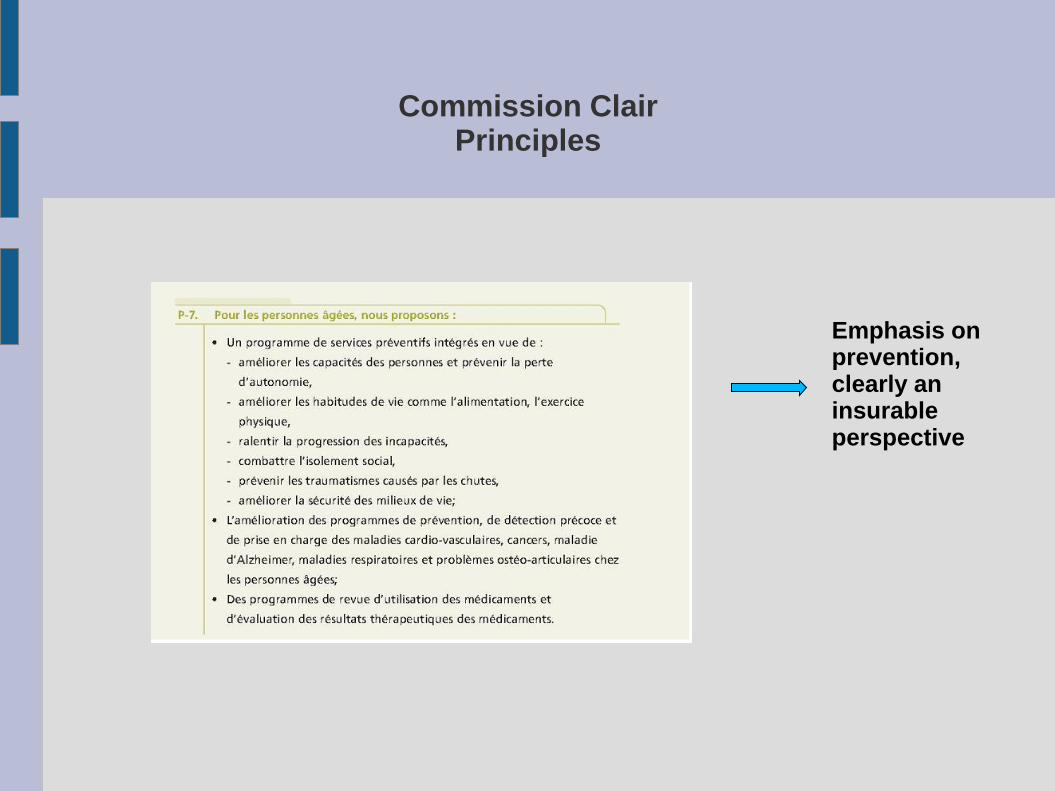
Commission Clair Principles
Emphasis on prevention, clearly an insurable perspective

Commission Clair Objectives
To care
To cure
To prevent
« l’amélioration de la capacité à composer avec le problème, à vivre une vie satisfaisante malgré celui-ci.” p. 11
Commission Clair Objectives
Focused on home services

Commission Clair Objectives
Main characteristics of public insurance regime, funded. Again, no comment on actual funding/financing
Assurance-Autonomie proposal(livre blanc 2013)
Assurance-Autonomie
Architecte : Ministre Dr. Réjean Hébert, founder du Centre du Viellissement de l'université de Sherbrooke, and now professor à l'École de santé publique de l'UdM.
Being old is not a sickness, it is a step in one’s life

Assurance-Autonomie
MSSS actual policy :
Soutien à l'autonomie des personnes âgées(SAPA)
Le programme « Soutien à l’autonomie des personnes âgées » regroupe tous les services destinés aux personnes en perte d’autonomie et à leur entourage, que ces services soient dispensés dans un établissement, à domicile ou ailleurs. Il s’adresse à toutes les personnes qui sont en perte d’autonomie, principalement due à l’avancement en âge, et ce, peu importe la cause : perte d’autonomie fonctionnelle, problèmes cognitifs (ex. : maladie d’Alzheimer) ou maladies chroniques.
Total MSSS budget: 33 billion $ -48% of total Quebec Budget -Cirano projects 75% in 15-20 years from now. -17% in home care compared to 43% in France, Danemark, 73%
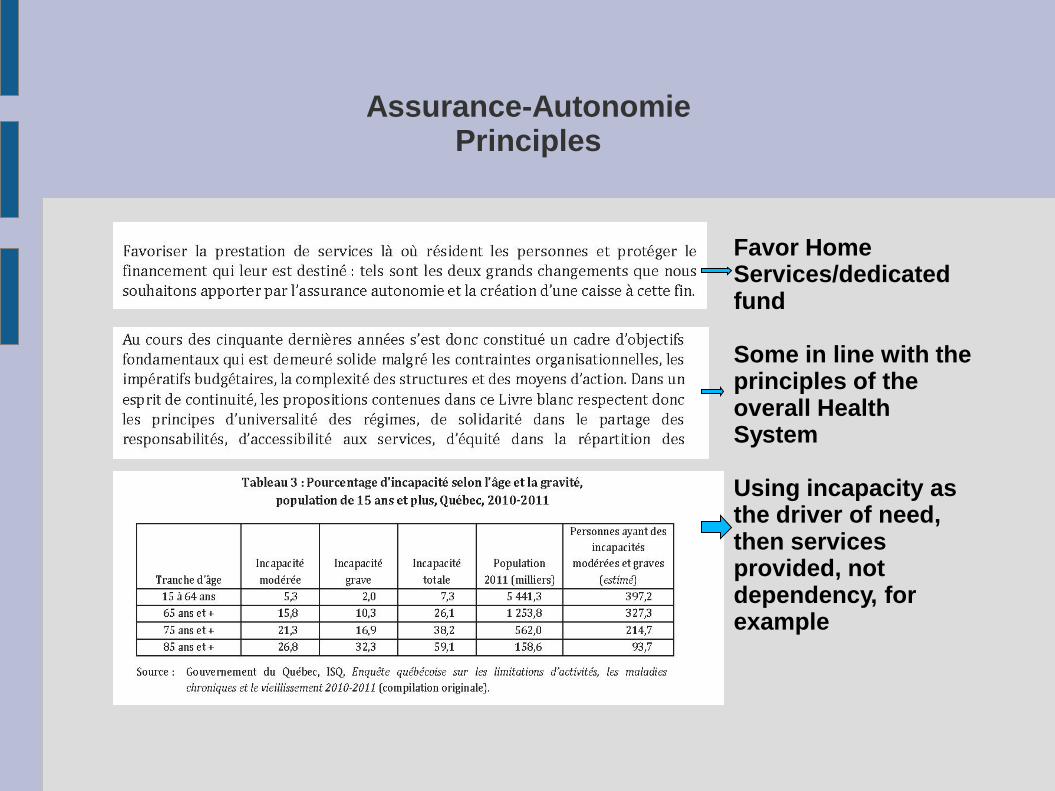
Assurance-Autonomie Principles
Favor Home Services/dedicated fund Some in line with the principles of the overall Health System Using incapacity as the driver of need, then services provided, not dependency, for example

Assurance-Autonomie Objectives
-
Pretty broad coverage based on autonomy – not incapacity? -, organic deficiency?, social roles... Pretty broad, maybe too broad?
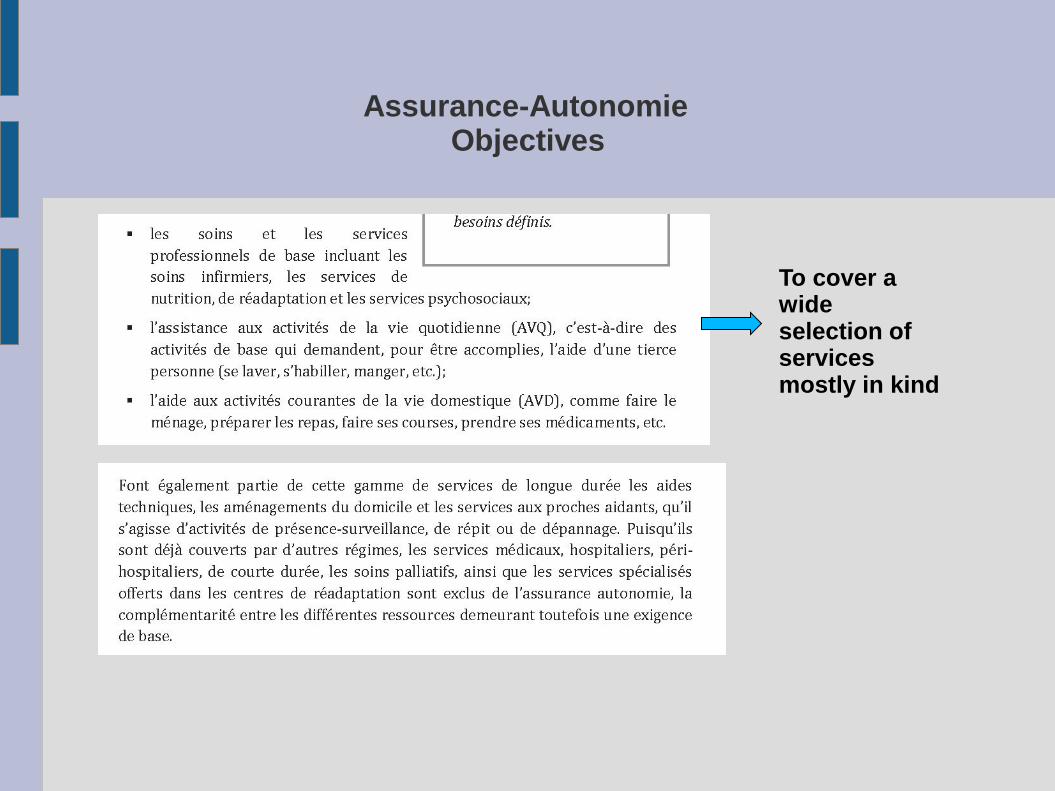
Assurance-Autonomie Objectives
To cover a wide selection of services mostly in kind
Assurance-Autonomie Objectives
Proposed to use an indicator –SMAF – aligned with WHO definition SMAF developed by Dr. Hébert.

Assurance-Autonomie Objectives
Provided some financial projections but no explicit plan to pay for it! Not really sustainable in the long term.

Other Groups/Actors/Initiatives
Québec: tax credits+ SHQ+Ministère Transport(Subsidized transportation), soins palliatifs
Other provinces. Ontario
Federal: Tax credits + Unemployment Insurance Fund
Municipal level: local housing policies
International level : OECD comparativestudies
Other public systems: US Medicaid

Other Groups/Actors/Initiatives
Social Economy : Home care, benevolent
Private insurance companies: Long-term Care policies
Private residences. Ex. Résidences Soleil
Coop de services de santé

Feedback? Where should I focus my inquiry efforts?
Where should I focus my research questions?
Comparison of overall principles/objectives for different types of existing regimes? Ex. A tax-based approach vs a social insurance/assistance approach?
Compare/evaluate different types of status covered? Ex. Incapacity vs dependency vs autonomy vis-à-vis a potential social criteria? Ex. principles of the Canadian Health Act, accessibility, financial?
Compare/evaluate different types of indicators used? AdLs vs SMAF(proposed Quebec) vs Somos(France) for a specific goal? Ex. accessibility
Should I focus on one type of regime? Compare a system based on the principles/objectives of a social security and one based on social need/right like the Canadian system?