social and community aspects of aging - the gateway...
TRANSCRIPT

SUCCESSFULLYgingA
SUCCESSFULLYgingA
A newsletter of the Division of Geriatric Medicine, Department of Internal Medicine, Saint Louis University School of Medicine; Geriatric Research,Education and Clinical Center, St. Louis Veterans Administration Medical Center; and the Gateway Geriatric Education Center of Missouri and Illinois
Summer 2005Vol. XV, No. 2
(continued on page 4)
looking insidethis issue....
Social and CommunityAspects of AgingBy Rodney M. Coe, John E. Morley, and Nina Tumosa
The interactions of social and community fac-tors and aging are extraordinarily complex (seeFigure 1 on page 4). It is important for the healthcare professional to be aware of the impact ofsocial and community factors on the health andwell-being of the older person.
Although the distinction is arbitrary, it is use-ful to try to separate the effects of the physicalprocesses affecting persons as they grow olderfrom the effects of the social consequences of at-taining an advanced chronological age. Three ofthese physical processes — aging, disease, anddisability — overlap with each other and with thesocial process which is often called growing old(see Figure 2 on page 14). Although it is morecommon for Aging Successfully to addressmedical issues about aging, disease, and dis-ability, in this issue we will consider the socialproblems that occur as a result of growingold.
phot
o co
urte
sy w
ww
.cli
part
.com
Social and Community Aspects of Aging..........................1Editorial..............................2US News and World Report Ranks SLU Geriatrics #8.....3Summer Institute.................5Best Docs in St. Louis..........6SLUGA Continues................6Nursing Education Program Set to Debut....................7News at SLU.......................8The Ride of Her Lifetime.......9Services and Products.........10“from the diary of a cynical missionary”..........11World Aging.....................12New Resident....................16SLU Goes International........21
Upcoming CME Programs.....23
Saint Louis

John E. Morley
E D I T O R I A L“She too looks over seventy, she’s arrived at the age where one must have feelings of respect for her.”
Ma Yan“The Diary of Ma Yan” 2002
The quote above is the logic usedby a starving Chinese peasant girl ofthirteen from Ningxia to spend her lastfive cents on buying a pear for anolder woman, rather than food forherself. To see this level of devotionto older persons expressed by MaYan in a remote corner of China cangive us all hope that globalization willeventually improve our positive atti-tudes to older persons.
Throughout the world, the mostvulnerable people remain those at theend of life. While CNN beams pic-tures of young children starving todeath in Dafur, Niger, or elsewhere intoour living rooms, we know that they areaccompanied by starving older people.Both groups are entitled to and needour support. For those aging in thedeveloping world, it is time that wepressured the United States governmentto increase aid to the level that starva-tion and lack of vaccines and medi-cines are no longer the major causesof death for older persons.
However, even in the United Stateswhere “seventy may be the newfifty,” ageism remains clearly evi-dent. There is a tendency to
glamorize the aging pro-cess and to focus onthose who have success-fully aged. This allows usto forget that both in theUnited States and the restof the world, there aremany old persons whoare aging less successfully.
There are several things we can doto improve elder care. Forexample, it is time to look atnew options for housing forseniors with disabilities. Onesuch option is group housing,such as is available for devel-opmentally disabled adults.This type of housing is beingdeveloped for rich seniors butshould become a viable op-tion for all seniors.
Also, we are coming close to be-ing able to slow the progression ofAlzheimer’s disease, if not totally curethis thief of the mind. It is time to re-consider incentives to encourage afull scale attack on this disease.Among these incentives should notonly be money, but also a recogni-tion that there is a need for a relax-ation of Institutional Review Boardrestrictions on human experimenta-tion in this area. Persons with cancerregularly consent to therapies that areas likely to kill as to save them. Wetend to be overprotective of persons
with Alzheimer’s disease because theyare a vulnerable population.Should I develop thisdreaded disease, I wouldwillingly be a human guineapig in the hopes that my ex-perience would lead to acure for others. I am surethat many older personswould join me in this senti-ment. Thus, I am proposingthat any person over sixty
years of age could sign a simple letteragreeing to be an experimental sub-ject in a trial for Alzheimer’s disease iftheir closest relative also acquiesces.This would be a true “Bill of Libera-tion” for all of those who suffer fromAlzheimer’s disease.
Finally, for good health care for allpersons, we need a Universal Com-puterized Medical Record. I join withSecretary Leavitt and the Bush Ad-ministration in suggesting that wemake this our number one health pri-ority and realize that if we utilized thehighly functional system developed
by the Veterans Administration,the conversion would be easilyaffordable.
With little effort and a modi-cum of expense, we can greatlyimprove the future for those ofus aging in the United States andalso for those in the rest of theworld.
phot
o co
urte
sy w
ww
.cli
part
.com
2 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]
SUCCESSFULLYgingA

U.S. News & World Report RanksSLU Geriatrics #8 in the U.S.
In geriatrics, in order to beranked by U.S. News and WorldReport, hospitals had to first meetat least one of three requirements:be a member of the Council ofTeaching Hospitals, be affiliatedwith a medical school, or makeavailable to patients at least 9 outof 18 technology-related servicesdeemed worthwhile (such aspositron emission tomography).This year, fewer than one-third ofall hospitals made it through thefirst gate.
Then, a hospital had to performa minimum number of specifiedprocedures on Medicare patientsin 2001, 2002, and 2003. Or thehospital had to have been recom-mended by at least one physicianin a U.S. News survey in 2003,2004, and 2005. The remaininghospitals got a numerical assess-ment (the U.S. News Score)made up of three equal parts:reputation, death rate, and care-related factors such as nursing andpatient services. Here’s how eachof the elements was ranked:
Reputation. For geriatrics, asampling of board-certified phy-sicians was randomly selectedfrom the American MedicalAssociation’s Masterf ile of all811,000 U.S. doctors and maileda survey form. The number of phy-sicians surveyed for geriatrics was
200 in 2005 and 150 in both2004 and 2003. All physicianswere asked to list the five hospi-tals they consider best in theirspecialty for difficult cases, with-out considering cost or location.The numbers in the “reputation”column are the percentages of re-sponding physicians who cited thehospi ta ls . SLU scored areputational score of 11.4%.
Mortality Ratio. This numberdefines a hospital’s ability to keeppatients alive. It is a ratio ofhow many Medicare pa-tients with certain condi-t ions d ied pr ior todischarge in 2001, 2002,and 2003 to how manydeaths would have beenexpected after factoringin severity. If the numberis below 1.00, the hos-pital did better than ex-pected; if above 1.00,worse than expected.SLU Hospital receiveda ratio of 0.76.
Other care-re-lated factors. Thisinformation comesfrom var ioussources , mostprominently theAmerican HospitalAssociation’s 2003 survey of its
By Susan Hakes, Director, Marketing and Public Relations, Saint Louis University
Just 176 hospitals scored high enough this year to rank ineven a single specialty out of all 6,007 U.S. medical centers.
members. This year, some factors,including “technology index” and“patient/community services,”were updated.
SLU Hospital provides 7 out of7 key technologies. SLU Hospi-tal received a U.S. News Scoreof 45.4 in geriatrics. This score isthe 8th best score in the country.
To make an appointment to seeone of SLU Hospital’s geriatri-cians, call 314-977-6505.
Aging Successfully, Vol. XV, No. 2 3Questions? FAX: (314) 771-8575 • email: [email protected]

A Life Course Perspective on AgeInfancy, childhood and adolescence involve preparation
for a job while living at home as a dependent. Adulthoodand middle age bring with them increasing involvement inwork, marriage, and creating a family in an independent set-ting. Persons in old age, however, will have experiencedretirement, death of loved ones, and increasing dependencyfrom functional health limitations. From a psychosocial perspec-tive the transition from youth to adulthood may be seen as in-creasing attachmentto one’s socialgroups throughmeaningful and pro-ductive roles. Thetransition fromadulthood to oldage may be seen asdetachment fromone’s social groupsas these meaningfuland productiveroles are given up.This may help ac-count for the re-ports that the veryold are, or at leastperceive them-selves to be, isolated, a ‘burden to society’ and have feel-ings of unworthiness. In fact, clinical depression is a commonproblem for older people, which could be exacerbated bythese perceptions.
Social ProblemsCommon social problems of elderly people include cer-
tain practical problems that occur more frequently amongolder people, such as housing problems, difficulties with trans-portation, and isolation. The reasons why older people suf-fer from these types of social problems more frequently than
Social and Community Aspects of Aging(continued from page 1)
younger people include:Poverty: The inability to purchase needed services
to maintain an acceptable quality of life.Immobility: Due to the high prevalence of disabling
disease combined with the difficulties with public trans-port, compounded by restricted use of cars and taxis.
Attitudes: Older people are generally not asser-tive because many were brought up in a culture inwhich the individual had fewer rights than s/he has to-day. Hence, few appeal against official decisions, seek
help from elected representatives, or try to overcomebureaucratic inertia.
PovertyPoverty threshold is defined by comparing a
household’s income with the level of prices of the basiccommodities necessary for life—the subsistence level,sometimes called the ‘poverty line.’ Those with incomesbelow the minimum level necessary for subsistence are
deemed to be living in poverty. Relative poverty isdefined by comparing a household’s income with theaverage level of incomes in society. J.K. Galbraithhas described the condition of relative poverty elo-quently: “People are poverty stricken when their in-come, even if it is adequate for survival, falls markedlybelow that of the community. Then they cannot havewhat the larger community regards as the minimumnecessary for decency and they cannot wholly escape,therefore, the judgment of the larger community thatthey are indecent. They are degraded, for in the lit-eral sense they live outside the grades or categorieswhich the community regards as acceptable.”
In the United States, older persons now have similarpoverty rates to those seen in working persons. SocialSecurity provides 90% of income for one-third of Ameri-cans over 65. Other sources of income for retirees areassets (55% of Americans), private pensions (29%), gov-ernment pensions (14%), and earnings (22%).
There is a wide range of wealth within the group ofretiree households. In general, the older a person is,
(continued on page 14)
Community Supports
Environment
Genome
PsychosocialRelationships
Disease
DepressionAnxiety
CopingSkills
SpiritualityReligion
Disability
Disasters
Death
Figure 1. An illustration of the complex inter-relationships between the community/social aspects of aging,the genome, and the progression of disease and disability towards death in the older person.
4 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Max K. Horwitt and James Flood Awards Presented
The 16th Annual
Summer Geriatric Instituteat Saint Louis University
R o n n i C h e r n o f f , P h D ,R D , FA DA , is the Directorof the Arkan-sas GeriatricE d u c a t i o nCenter, Di-rector of Edu-cation at theDonald W.Reynolds In-stitute on Ag-ing, UAMS;and AssociateDirector, Edu-cation at theGeriatric Re-search, Edu-ca t ion , andClinical Center at the CentralArkansas Veterans HealthcareSystem. A professor at theDonald W. Reynolds Depart-ment of Geriatrics, she is a pastpresident of the American Di-etetic Association. She received
the Max K. Horwitt Award for herlifetime achievement in geriatric
nutrition. Following thepresentation of heraward, she shared herwisdom about how hy-dration care haschanged for eldersacross the continuum ofcare at the 16th AnnualSaint LouisU n i v e r s i t ySummer Geri-atric Institute.
Ke i t h W.K e l l e y ,
P h D , Professor ofImmunophysiology in theDepartment of Animal Sci-ences at the University ofIllinois at Urbana-Champaign, received theJames Flood Award for
Left to right: Nina Tumosa, RonniChernoff, John Morley
his remarkable contributions tothe understanding of how healthis affected by hormones and im-munology. He spoke to the au-dience on how the brain and theimmune system interact, with par-ticular emphasis on intracellularsignaling molecules that are ac-tivated by the insulin-like growthfac tor ( IGF)-I receptor in
promyeloidcel l s andneurons andon the roleof pro- in-flammatorycytokines ascommunica-t ion mol-e c u l e sbetween theimmune andcentral ner-vous sys-tems.
Over 300 participants from 22 statesplus Puerto Rico attended the 16th Annual Saint LouisUniversity Summer Geriatric Institute. Conferenceattendees enjoyed plenary sessions and workshops onthe medical, social, and spiritual aspects of aging. Topicsof discussion included incontinence, religion andspirituality, mental health, the genetics of aging, chronicdisease management, nusring home care, quality of care,and geriatric assessment. A series of workshops onemergency preparedness for the elderly across thecontinuum of care completed a two-year initiativesupported by the Bureau of Health Professions.
Workshop participants watch carefully as one of theircolleagues learns why gait and balance are essentialwhen using a computer program that measures threedimensional space.
Left to right: William Banks, JohnMorley, Keith Kelley
Aging Successfully, Vol. XV, No. 2 5Questions? FAX: (314) 771-8575 • email: [email protected]

SLUGA Continuescountry due to the extensive nature ofwounds suffered in the Middle East,an entire afternoon was devoted to twoworkshops on Clinical Assessment ofGait and Balance and on Prosthetic andOrthotic Care.
Five physicians have now completedthe 160-hour Geriatric Leadershiptraining program. Three of them areVeterans Administration physicians:Asif Ali from the Hollidaysburg,Pennsylvania VA Medical Center(VAMC), James Stauffer
from the Lebanon,P e n n s y l v a n i aVAMC, and RafiKevorkian fromthe St. Louis,M i s s o u r iVAMC. Theother two are
Maria Hansberry from
Rush Medical Center in Chicago, Illi-nois, and Julie Gammack from SaintLouis University in St. Louis, Missouri.
The next SLUGA is scheduled forJanuary 9-13, 2006. We are currently ac-cepting registrations. Contact NinaTumosa, PhD, at 314-894-6560 formore details.
Saint Louis University Geriatricians
Of all the doctors in St. Louis, only those at Saint Louis University were named in St.Louis Magazine’s ranking of Best Doctors in Geriatric Medicine.
The August 2005 issue of St.Louis Magazine’s cover storylists 592 physicians in 39 special-ties. These physicians are consid-ered the best in their field.
Joseph H. Flaherty, MD, JohnE. Morley, MB, BCh, and DavidR. Thomas, MD, comprised theentire list of Geriatricians in the St.Louis region. They join 101SLUCare physicians from otherspecialties chosen for the 2005 list.
Best in St. Louis
The list is based on the annual“Best Doctors in America” data-base, which considers more thanone million peer evaluations tocreate a directory of approxi-mately 30,000 doctors.
To see one of these physicians,call 314-977-6055 for an ap-pointment at Saint Louis Univer-sity or 314-966-9313 for anappointment at Des Peres Hos-pital.
July 11-15,2005 marked the fourth meeting of theSaint Louis University (SLU) GeriatricLeadership Academy in the SLU Divi-sion of Geriatrics. Thirty-two physi-cians, pharmacists, and nurses met with15 faculty members to discuss geriat-rics, literature, business, education,and leadership skills. Guest lecturesincluded Strategic Planning by Dr.Timothy Hickman, Capacity Buildingwith Janet Frank, DrPH, SupportingClinical Geriatric Programs and Howto Write an Introduction with Dr. JamesGoodwin, Cardiovascular Ag-ing by Dr. Michael Rich,and Infectious Diseases andGeriatric Leadership withDr. Stefan Gravenstein.
In light of the recent in-creased workload at VeteransAffairs Hospitals around the
Dear Dr. Morley,
I would like to register my congratu-
lations to you and your organizing
committee for an excellent course!
And a special note of appreciation
for your generosity in making this
course possible....
Thanks and best regards,
Wee Shiong
Pictured (left to right) are new SLUGeriatrics Academy Graduates RafiKevorkian, MD, James Stauffer, MD,and Julie Gammack, MD
6 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Thistrainingcoursewill beoffered
at the2006
SummerGeriatricInstitute
phot
o co
urte
sy w
ww
.cli
part
.com
phot
o co
urte
sy w
ww
.cli
part
.com
New Nursing Education ProgramSet to Debut
Dr. Julie K. Gammack is thePrincipal Investigator of a Depart-ment of Health and Human Ser-vices, Health Resources andSer vices Adminis t ra t ion(HRSA), Comprehensive Geriat-ric Education Program Award. Thisone-year award suppor ts thedevelopment and implementation ofnew programs that provide train-ing for nurses who provide geriatriccare for the elderly. In partnershipwith the Saint Louis University(SLU) School of Nursing and Co-investigator Dr. Helen Lach, threenew nursing educational activitieswill be implemented in 2005-6.
Faculty and Staff DevelopmentA four-hour train-the-trainer
course will be offered for nursesand nursing faculty who plan toteach geriatric assessment skills tonursing trainees. Detailed instruc-tion and classroom demonstrationswill prepare course participants toimplement geriatric skills work-shop sessions at their home insti-tutions. Workshop topics includedin the curriculum include: SensoryImpairment, Gait and BalanceTraining, Wound Care Manage-ment, Therapy and Dietary Sup-
port, History and Examination ofthe Elderly, Mental Status Evalua-tion, Breaking Bad News, andChallenging Communication Sce-narios. Participants will be providedwith the Geriatric Skills Workshopcurriculum and materials needed toimplement this course at a hospital,academic pro-gram, nursing fa-c i l i ty or o therorganization. Thistraining coursewill be offered atthe June 6-8 ,2006 Ger ia t r icSummer Institutehosted by SLU’sDivision of Geri-atric Medicine in St.Louis, Missouri.Course fees arecovered throughSummer Instituteregistration. Con-tinuing NursingEducation creditswill be available for the training.
Nursing Trainee EducationDuring the 2005-6 academic
year, all SLU nursing students willreceive a four-hour orientation to
geriatrics. As an introduction toclinical training, this modulewill cover geriatric syndromes,geriatric assessment, and com-mon disorders in the older adult.
After completing the f irstyear of training, undergraduateand graduate level nursing stu-
dents at SLU willbe e l ig ible toe lec t a two-credit GeriatricSkills WorkshopCourse. A seriesof eight hands-onworkshops intro-duces students tothe common clini-cal screening andassessment toolsused in evaluatingthe older adult.S tudents wi l lpract ice theseskills on volun-teer elders.
For more in-formation on these opportu-nities, contact Dr. Gammack at314-977-8457; or by email [email protected] or Dr.Helen Lach at 314-977-8939;[email protected].
Aging Successfully, Vol. XV, No. 2 7Questions? FAX: (314) 771-8575 • email: [email protected]

News at SLU
Two Awards for Dr. Gammack
Dr. Flaherty Administers OathDr. Joseph Flaherty was granted the honor ofadministering the Hippocratic Oath at the 2005Sa in t Lou is Un ivers i ty Schoo l o f Medic inegraduation ceremony.
Dr. Julie K. Gammack received a 2005 Pfizer QualityImprovement Award. The award is designed toencourage the development of innovative projects
Dr. Wilson Awarded TenureMargaret-Mary Wilson, M.B.B.S, has been awardedtenure as an Associate Professor of Medicine in theDivision of Geriatric Medicine at Saint Louis University.
John Morley Winner of Awardfor ExcellenceDr. John E. Morley has been selected from a group ofoutstanding nominees as the first winner of the MarshaGoodwin-Beck Excellence in Geriatric LeadershipAward. Dr. Morley contributes significantly to clinicalcare of the patients in the VA and he has pioneered themedication reduction approach of the GRECC clinics.Dr. Morley received the award at the NationalLeadership Board Meeting in June 2005.
Seema Joshi, MD, Joins FacultyDr. Seema Josh i jo ined thedivision of Geriatric Medicineat Saint Louis University as anAss i s tant P r o fessor o fMedicine in August 2005. Sherecent ly completed herfellowship training in GeriatricMedic ine a t Sa in t Lou isUn ivers i ty . She a t tendedmedical school at King George’s Medical Collegein Lucknow, India and completed her residencyin internal medicine at St. Luke’s Hospital in St.Louis, Missouri. She will be pursuing her interestsin memory impairment, dementia, and associatedcaregiver burden.
Dr. Joshi is married with two children, ages 4 and4 months. In her free time, she likes to work inher garden, read a good novel, or attempt theoccasional home improvement project. Welcome,Dr. Joshi!
that will help to make a distinct impact on the qualityof long term care. This $7000 award supportsresearch, education, health literacy, and qualityimprovement to enhance patient care in the nursinghome setting. Dr. Gammack’s project is titled “Effectsof Natural Light Therapy on Sleep in the Elderly.”
Additionally, Dr. Gammack is one of two recipientsof the 2005 Saint Louis University Department ofInternal Medicine Faculty Career DevelopmentAward. This $2500 award supports junior faculty whoparticipate in accredited educational programs toenhance career competency in teaching, clinical care,biomedical research, or community service. Dr.Gammack will attend the European Academy forMedicine and Ageing (EAMA). The aim of EAMA isto improve knowledge and ski l ls in geriatr icmedicine. The course was developed in 1995 by theGroup of European Professors in MedicalGerontology and is held each year at the Institut KurtBösch in Sion, Switzerland.
News at SLU
8 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

The Ride of Her LifetimeThe Ride of Her LifetimeThe Ride of Her LifetimeThe Ride of Her LifetimeThe Ride of Her LifetimeTwenty years ago, I drove a cab
for a living. When I arrived at 2:30a.m., the building was dark exceptfor a single light in a ground floorwindow. Under these circum-stances, many drivers would justhonk once or twice, wait a minute,then drive away. But, I had seentoo many impoverished people whodepended on taxis as their onlymeans of transportation. Unless asituation smelled of danger, I alwayswent to the door. This passengermight be someone who needs myassistance, I reasoned to myself. SoI walked to the door and knocked.
“Just a minute,” answered a frail,elderly voice. I could hear some-thing being dragged across the floor.After a long pause, the dooropened. A small woman in her 80’sstood before me. She was wearinga print dress and a pillbox hat witha veil pinned on it, like somebodyout of a 1940s movie. By her sidewas a small nylon suitcase.
The house looked as if no onehad lived in it for years. All the fur-niture was covered with sheets.
There were noclocks on the walls,no knickknacks orutensils on thecounters. In the cor-ner was a cardboardbox filled with pho-tos and glassware.
“Would you carrymy bag out to thecar?” she said. Itook the suitcase tothe cab, then re-turned to assist thewoman. She tookmy arm and wewalked slowly to-ward the curb. Shekept thanking me formy kindness. “It’snothing,” I told her.“I just try to treat mypassengers the wayI would want mymother treated.”“Oh, you’re such a
good boy,” shesaid.
When wegot in the cab, she gave me anaddress, then asked, “Couldyou drive through downtown?”“It’s not the shortest way,” Ianswered quickly. “Oh, I don’tmind,” she said. “I’m in nohurry. I’m on my way to a hos-pice.”
I looked in the rear-viewmirror. Her eyes were glis-tening. “I don’t have anyfamily left,” she continued.“The doctor says I don’thave very long.”
I quietly reached over and shutoff the meter. “What route wouldyou like me to take?” I asked. For
the next twohours , wed r o v ethrough thec i ty. Sheshowed methe buildingwhere shehad onceworked asan elevatoro p e r a t o r .We drovethrough then e i g h b o r -hood whereshe and herhusband hadlived whenthey werenewlyweds.She had mepull up infront of a fur-niture ware-house thathad oncebeen a ball-room where
she had gone dancing as a girl.Sometimes she’d ask me to slowin front of a particular building orcorner and would sit staring intothe darkness, saying nothing.
As the first hint of sun was creas-ing the horizon, she suddenly said,“I’m tired. Let’s go now.” Wedrove in silence to the addressshe had given me. It was a lowbuilding, like a small convales-cent home, with a drivewaythat passed under a portico.
Two orderlies came out to thecab as soon as we pulled up.They were solicitous and intent,
(continued on page 16)
phot
o co
urte
sy w
ww
.cli
part
.com
Aging Successfully, Vol. XV, No. 2 9Questions? FAX: (314) 771-8575 • email: [email protected]

PRODUCTS from the Gateway GECGEROPADY
ACE Unit VideoCrossword Puzzle BookChallenges and Choices
Aging Successfully NewsletterSLU GEMS
Emergency Preparedness CDBooks
Call 314-977-8848 for moreinformation about these products.
AGING SUCCESSFULLYIS ON THE WEB!
THIS ISSUE AND EVERY ISSUE IS AVAILABLE AT OUR WEBSITE:http://medschool.slu.edu/agingsuccessfully/
Also, there, you will findscreening tools, links to otheruseful sites, and information
about our upcomingconferences.
Check it out!
If you need additional copies of this or a previous issue ofAging Successfully,
please contact [email protected].
SERVICESServices of the Division ofGeriatric Medicine, Saint LouisUniversity Health SciencesCenter include clinics at twolocations in the following areas:
Aging and DevelopmentalDisabilities
Bone MetabolismFalls: Assessment and
PreventionGeneral Geriatric
AssessmentGeriatric Diabetes
Medication ReductionMenopause
NutritionPodiatry
RheumatologySexual Dysfunction
Urinary Incontinence
For an appointment,call
314-977-6055(at Saint Louis University)
or314-966-9313
(at Des Peres Hospital)
10 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

‘…from the diary of a cynical missionary…’By Margaret-Mary Georgiana Wilson, MD
“…those who live long shall tell of many disasters…”Anonymous
Efik proverb from South-Eastern Nigeria
“Those the godslove die young” is anoften quoted cliché,presumably intendedto convince the gull-ible that the only al-ternative to aging isthe frightening con-cept of death. In theWestern world, ideal-istic notions of aginglull us into forgettingthat in poor coun-tries, aging is a cyni-cal game in which‘survival of the fittest’is frequently re-warded by death. Asa Nigerian-born geri-atrician, trained and practicing in theUnited States, I have often won-dered what becomes of the frail eld-erly in Nigeria, a country wheregeriatric medicine is a little knownspecialty. How do the elderly sur-vive in a country where national andinternational healthcare assistance isdirected almost exclusively towardchildren and young adults?
Perhaps, “the village that raisesa family” that widely publicizedClintonian African health insurancesystem also caters to the frail andlonely elder; or perhaps, as por-trayed in countless televised char-ity appeals, the only starving victimsin Africa are the same familiar chil-dren who never seem to age and aretraipsed out each year to prod ourWestern conscience. Although myexperience as a prototypical Nige-rian is limited, I do know that oldNigerians exist. My father died at82 and my mother is still living at
age 76. I am still haunted by myearly childhood memories of very an-cient tobacco-reeking grandparentsand a smattering of really old peopleof dubious genealogical origins whoall claimed to be great-aunts, great-uncles or complex relatives of onesort or the other. I also know thathealthcare for the sick Nigerian is an“all or nothing approach”…all for therich and nothing for the poor. Thus,over the years, thoughts of the poorand frail Nigerian elder shamefullyneglected by a country that propa-gates the traditional myth of respectand care for the aged, has quietlygnawed away at my Catholic con-science. I had gradually been trans-formed into a missionary, albeit areluctant and cynical one. I was de-termined to seek out and help the frailNigerian elder. I was not prepared forwhat I found.
Bordering the Gulf of Guinea, Ni-geria has a population of 130 mil-
lion and yet is onlytwice the size of Cali-fornia. Both the cli-mate and terrain arevariable, with southernlowlands merging intocentral hills and pla-teaus; mountains in thesoutheast and plains inthe north. A countryrich in natural re-sources such as natu-ral gas, petroleum, tin,iron ore, and coal, yetdevastated by politicalcorruption and a crimerate that has earned itthe distinction of beingamong the most dan-
gerous countries in the world. As-sembling a team willing to brave theunknown and the daunting crimestatistics was the first challenge.Janice Della Hicks, a disillusionedand happily retired registered nurse,now a part-time medical educationconsultant, volunteered her services.Brenda McCrimon, an administra-tive assistant, was coerced into ac-companying us. We set off toNigeria.
Catholicism is one of the oldestreligions in Nigeria with century-oldparishes, schools, and missionhospitals extending far into therural areas. Other than thechurches, which have an at-tendance paralleled only byevangelical revival meetings inthe United States, the schoolsand hospitals have been re-duced to pathetic vestiges oftheir former selves. Father
(continued on page 17)
Aging Successfully, Vol. XV, No. 2 11Questions? FAX: (314) 771-8575 • email: [email protected]
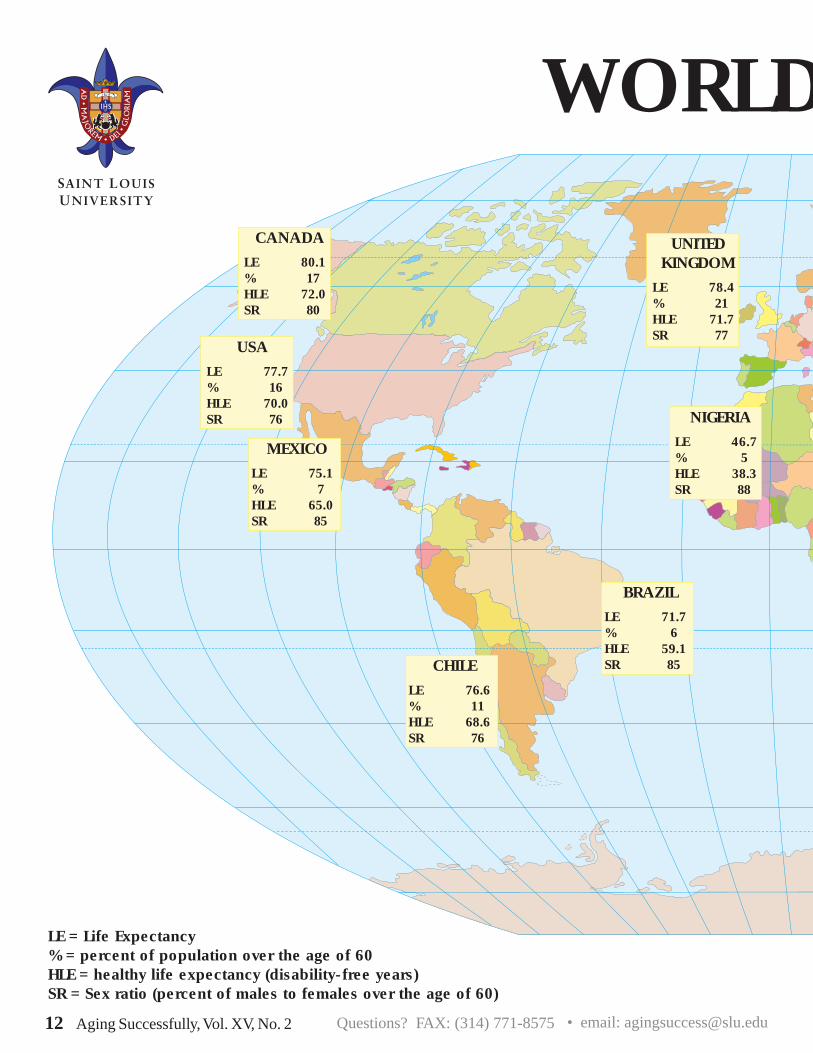
WORLD
LE = Life Expectancy% = percent of population over the age of 60HLE = healthy life expectancy (disability-free years)SR = Sex ratio (percent of males to females over the age of 60)
CANADA
LE 80.1% 17HLE 72.0SR 80
USA
LE 77.7% 16HLE 70.0SR 76
MEXICO
LE 75.1% 7HLE 65.0SR 85
BRAZIL
LE 71.7% 6HLE 59.1SR 85CHILE
LE 76.6% 11HLE 68.6SR 76
UNITEDKINGDOM
LE 78.4% 21HLE 71.7SR 77
NIGERIA
LE 46.7% 5HLE 38.3SR 88
12 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

D AGING
FRANCE
LE 79.6% 21HLE 73.1SR 73
GERMANY
LE 78.6% 24HLE 70.4SR 72
ITALY
LE 79.6% 25HLE 72.7SR 74
KENYA
LE 48% 4HLE 29.3SR 87
SOUTHAFRICA
LE 43.3% 6HLE 39.8SR 66
RUSSIA
LE 67.1% 10HLE 61.3SR 53
CHINA
LE 72.3% 10HLE 62.3SR 91
PAKISTAN
LE 63.0% 6HLE 55.9SR 100
SAUDIARABIA
LE 75.5% 5HLE 64.5SR 83
INDIA
LE 64.3% 8HLE 53.2SR 94
AUSTRALIA
LE 80.4% 17HLE 73.2SR 84
JAPAN
LE 81.1% 24HLE 74.5SR 72
Aging Successfully, Vol. XV, No. 2 13Questions? FAX: (314) 771-8575 • email: [email protected]

Aspects of Aging(continued from page 4)
the poorer that person is. The disparity is due to the fact thatthe proportion of people in each age group who have anoccupational pension decreases the older the age group con-sidered. The difference between the income of differentage groups of retired people is accentuated because mendie younger than women, on average, so that the older groupsconsist of relatively more women, many of whom are ineli-gible for national insurance or occupational pensions anddepend on a supplementary pension which is set at the low-est social security rate. Poverty is most common, therefore,among elderly women, particularly those who never mar-ried.
Housing ProblemsEnvironmental Problems:For some older people the cause of their housing prob-
lem is not their dwelling but its environment. Many eithercannot afford to, or do not wish to, move even when newneighbors do not share their cultural or social values.
(continued on next page)
Figure 2. The social consequences of growing old
Aging Disease
Disability
TheSocial
Consequencesof Growing
Old
Structural Problems:Often the dwelling has deteriorated. Common prob-
lems and their solutions are presented in Table 1. The ser-vices listed are not universally available and where suchservices exist older people often have difficulty accessingthem. Every health professional can help by being awareof the range of services available, suggesting ways to im-prove the dwelling and helping the person to contact theappropriate services.
Difficulties Caused by Disability:Sometimes the dwelling is unsuitable after the onset of
disability. Disabilities can affect the person’s ability to climbthe stairs, access the bathroom, do the laundry, or enterthe dwelling. Sometimes the circulation space within thehouse is too small to allow easy movement for a personusing a wheelchair or walking aid.
One solution is adaptation of the dwelling, and domiciliaryoccupational therapists have the skill to do this. Solutionsinclude the installation of ramps and indoor elevators. Adap-tation of the kitchen and bathroom and addition of handrailscan dramatically increase the safety of the house.
Making a Move:The decision about when to move into a less indepen-
dent environment represents one of the hardest decisionsassociated with aging for both the older person and thecaregiver. The development of “smart homes,” lifelinealarms, etc. are delaying the time to when that decisionhas to be made. Each case is unique but possible guide-lines for decision-making are listed in Table 2 on page 15.photo courtesy www.clipart.com
Table 1. Solutions to Housing Problems
14 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Table 2. Good Reasons for Movingn To move nearer a son, daughter, or other
relative who is willing and able to offer care
n To move away from a dwelling that is impossibleto repair, improve, or adapt
n To move away from an environment that is caus-ing severe depression or anxiety
n To move to sheltered housing if living alone is nolonger safe
“...notsmoking,exercise,
not drinkingalcohol to
excess,avoidingobesity,
and astable
marriagewere
the factorsthat
predictedsuccessful
aging.”
(continued on page 18)
Senior apartment buildings or assisted living facilities arethe types of housing which most people think of when newhousing for elderly people is mentioned, although manymove to independent flats or villas. Such congregate hous-ing offers security and reassurance to elderly people andthus meets the needs of many frail elderly people, particu-larly those who are:n Nervous about living alonen Anxious that they could not call anyone if they
should fall illn At risk of hypothermia or hyperthermian Isolated (although some people feel just as isolated
in congregate housing as in an independent dwelling).
Assisted living is not always suitable forantisocial or very confused persons becausestaff members are often not trained to copewith excessively dependent people. Peoplerequiring individual attention by dedicated staffmay require the level of assistance best pro-vided by nursing homes. However, it is im-portant to remember that the majority ofdisabled elderly people live, and will continueto live, in independent dwellings.
RetirementRetirement became a reality for older
Americans with the introduction of Social Se-curity. For many, pensions from employ-ers and personal investments supplement thatretirement. At present, insecurity about theability of the government to fund Social Se-curity and health plans for the old (Medicare)and the poor (Medicaid) is creating fear, es-pecially among the poor elderly.
The ‘Golden Age’ MythThe ‘Golden Age’ myth states
that there used to be a time whenit was good to be old because allelderly people were loved and re-spected. Some believe that theGolden Age was destroyed by theindustrial revolution when the tra-ditional skills of elderly men andwomen, which they passed on tothe younger generations by the fire-side, were rendered irrelevant.However, that myth is false. Al-
though rich elderlypeople weretreated respect-fully, poor elderlypeople usually fin-ished up in a work-house. Theproportion of eld-erly people living inthis situation washigher in times pastthan today. Thequality of care inmodern institutions far surpasses that seen
even a quarter of a century ago. Ifever there was a ‘Golden Age’ forolder persons, it is now.
Ageism‘Ageism,’ like ‘racism’ and ‘sex-
ism,’ is a prejudice. People whohold ageist views believe that allpeople over the age of 65 are ofdeclining intelligence, rigid, conser-vative, dull, and unable to changeor learn. They assume that physi-cal or mental changes are due tothe aging process and areuntreatable. They also have ex-pectations about the way olderpeople should behave, e.g., that itis not normal for older people todrink to excess, show an interestin sex, or even to argue forcibly
Aspects of Aging(continued from page 14)
phot
o co
urte
sy w
ww
.cli
part
.com
phot
o co
urte
sy w
ww
.cli
part
.com
Aging Successfully, Vol. XV, No. 2 15Questions? FAX: (314) 771-8575 • email: [email protected]

The Ride of Her Lifetime(continued from page 9)
Erin Thomas, PharmD is the2005-2006 Geriatric PharmacyPractice Resident at the St. LouisVA Medical Center GRECC, un-der the direction of Myra Belgeri,PharmD, CGP, BCPS, FASCP.Dr. Thomas graduated from St.Louis College of Pharmacy withher BS in Pharmacy in2004 and her PharmD in2005. As part of her 12-month ASHP-AccreditedResidency, Dr. Thomas willspend the majority of hertime providing clinical phar-macy services in theGRECC and Hypertensionclinics and participating ininterdisciplinary teamrounds on the GEMU at theVA. She will also gainclinical pharmacy experi-ence at the PACE program,
Myra Belgeri, PharmD (left), and Erin Thomas, PharmD(right)
New Pharmacy Resident Joins Saint Louis VA GRECCthe ACE unit at Des Peres Hospital,VA geropsychia t r y, and VAnursing home. Her residency re-search project will involve evalu-ating outcomes in GEMU patientswith anemia. She will participatein St. Louis College of Pharmacy’sresident teaching workshops, in
which she will learn the principlesof abilities-based education andwill have the opportunity to ap-ply these principles in severalspring College of Pharmacycourses. Dr. Thomas will also beconducting presentations at mul-tiple medical and pharmacy con-
ferences, including St. Louisarea pharmacy residentsseminar series this fall, SaintLouis University GeriatricMedicine Grand Rounds inthe spring, Midwest Phar-macy Residents Conferencein May 2006, and the SummerGeriatric Institute in June2006. St. Louis College ofPharmacy and St. Louis VAMedical Center are proud tohave Dr. Thomas as a part ofour team – Welcome, Erin!
watching her every move. They musthave been expecting her. I openedthe trunk and took the small suitcaseto the door. The woman was alreadyseated in a wheelchair. “How muchdo I owe you?” she asked, reachinginto her purse. “Nothing,” I said. “Youhave to make a living,” she answered.
“There are other passengers,” Iresponded. Almost without thinking,
I bent and gave her a hug. Sheheld onto me tightly. “You gavean old woman a little momentof joy,” she said. “Thank you.”I squeezed her hand, thenwalked into the dim morninglight. Behind me, a door shut.It was the sound of the closingof a life. I didn’t pick up anymore passengers that shift. I
drove aimlessly, lost in thought. For therest of that day, I could hardly talk.What if that woman had gotten anangry driver, or one who was impatientto end hisshift? What ifI had refusedto take therun, or hadhonked once,then drivenaway? On aquick review,I don’t thinkthat I havedone anythingmore impor-tant in my life.We’re condi-tioned to think
that our lives revolve around greatmoments. But great moments oftencatch us unaware-beautifullywrapped in what others may consider
a small one.
This article isreprinted with thepermission of TheHumor Network.Submitted by one oftheir readers, theauthor is unknown.While many of thearticles on TheHumor Network arelight-hearted andhumorous, others,like this one, arep o i g n a n t ,bittersweet, andthought-provoking.
photo courtesy www.clipart.com
16 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Boniko, the spiritual director of theDivine Mercy Prayer Group of thePort-Harcourt Catholic Diocese inEastern Nigeria, offered to guide
us on our tour. He is also the par-ish priest of St. Patrick’s Parish inBodo, a nearby village. Our firstencounter with life on the other sideof the geriatric divide was at thePort Harcourt “Home for the Eld-erly.” This is one of only two longterm care facilities in Nigeria. Thisfacility, run by the Catholic dio-cese, was established to care forsick, poor, abandoned, and re-jected elders. The facility housestwenty-nine residents, only one ofwhom is a man. Incidentally healso doubles as the facility gardener.On arrival, we were met by the en-tire workforce, Pauline themiddle-aged supervisor and fiveteenage girls. Attempting to definethe specific responsibilities of eachemployee soon proved impossible.There were no departments or dis-ciplines. Care plans and standardsof care did not exist. Apparently,the only qualifications necessary
residents were hypertensive, sevenof them had dementia, several hadmajor depression, and one ladywho roamed freely through thefacility had full blown tuberculo-sis. Most of the residents were justlonely. A really withdrawn womanwas so malnourished and wastedthat I thought at first glance she musthave cancer. Examination revealedseveral decaying teeth and amouth full of pus making it almostimpossible for her to eat. After wehad finished with the residents, thestaff demanded an examination!One young teenage employee hada nasopharyngeal tumor, anotherteenager had severe hypertension.With all the ‘patients’ seen and allthe prescriptions written, the onlything left to do was order the medi-cation. At this point we realized theobvious-someone had to pay for the
medicines. Peter-Anthony, the lay-diocesan leader of the DivineMercy Group, and our three-per-son team pooled funds to buy the
(continued from page 11)
‘…from the diary of a cynical missionary…’
(continued on page 22)
Janice Della Hicks interviews the elderly patient as BrendaMcCrimon creates the patient’s medical chart.
were a cheerful disposition, theability to work hard, and a crucifixworn around the neck. The homeis comprised of three buildings
that could easilybe mistaken forw a r e h o u s e s .Residents arehoused in a dor-mitory-like style,with beds ar-ranged alongeach wall in aFlorence Night-ingale fashion.Faded and well-worn bed linensstood in starkcontrast to thecold concretefloors. Besideeach bed was a
small cabinet that housed eachres ident ’s en t i reworldly possessions.
Shouts of jubila-tion erupted whenthe residents weretold that a medicalteam from the UnitedStates was here tovisit. We suddenly re-alized that we wereexpected to provideeach resident with acomprehensive medi-cal examination. Thiswas not an unreason-able expectation con-sidering a doctor hadnot visited the facil-ity for at least fifteenyears. We got to work; there wereno laboratories, no X-ray facilities,no CAT scans, or ultrasounds. I hadto rely on the Livingstone approach:“My little black bag and I!” All the
Dr. Wilson discusses the need for medications with aNigerian woman.
Aging Successfully, Vol. XV, No. 2 17Questions? FAX: (314) 771-8575 • email: [email protected]

Aspects of Aging(continued from page 14)
with people with whose views they disagree. Both oldand young people hold ageist views and may assume that allphysical and mental changes are due to the aging process,rather than to disease. The two main effects of ageist beliefsamong older persons are:
1. Failure to seek help for treatable medical problems—“What else can you expect at my age,” and
2. Failure to comply with medical advice—“It was kindof the doctor to give me tablets but there’s no point in tak-ing them; it’s just old age that’s the problem.”
Ageist beliefs lead to undervaluing the contributions ofolder persons and providing inadequate societal resources forthem. Political activism is needed to combat ageism. Per-sons at all levels of the community and health professionsoften pay lip service to the aging demographic imperative,but fail to provide the financial and social supportsneeded to overcome ageist policies.
The Effect of Social Factors on the AgingProcess
George Valiant (2003) studied aging in Harvard gradu-ates and inner city persons living in Boston and found thatnot smoking, exercise, not drinking alcohol to excess, avoid-ing obesity, and a stable marriage were the factors that pre-dicted successful aging. Social connection and perceivedsocial support have an effect on health in persons facingcrises, stressors and/or adversity (Johnson and Krueger,2005) while social isolation or perceived lack of social sup-
port leads to more diseases and a higher mortality rate.When volunteers sat with recipients of home-delivered mealswhile they ate, the elders experienced decreased risk forpoor nutrition and dysphoria (Suda et al. 2001). Allostaticload, an index of wear and tear on the physiological sys-tems of the body that is related to heart disease, physicalfunction, cognitive function and death can be significantlymodulated in men, but not women, with strong emotionalsupports (Karlamangla et al, 2002).
The effect of social relationships on an older person de-veloping and coping with disability depends not only on thestrength of the relationship but also on the ability of theperson to accept the relationship (e.g., are they depressedor did they have a lifelong inability to bond with others?)and their innate coping skills, as well as their economic sta-tus and the inherent severity of the disease process (Figure 3).
Endurance and resistance exercise can modulate dis-ease processes and slow the development of frailty, dis-ability and death. Exercise enhances frontal lobe cognitivefunction and may slow cerebral atrophy. Yet, over half ofmen and women over 65 years of age do not engage inphysical activities. It is important that simple ways to im-prove physical fitness, e.g., climbing stairs rather than tak-ing the elevator, can be as effective as organized activities.The importance of balance exercises, such as Tai Chi, toreduce falls needs also to be stressed.
Lifestyle, Nutrition and Healthy Aging: Lessonsfrom the SenecaStudy
The Survey in Europe onNutrition and The Elderly:A Concerned Action(SENECA) examined howsocial factors modulate dis-ability and mortality in 19towns throughout Europe.The participants, born be-tween 1913 and 1918, hada large variation in lifestylefactors such as alcoholconsumption, smoking,and activity in sports (DeGroot et al., 2004).Physical activity and smok-ing habits both predicteddeath and dependency.
(continued on page 19)
Social Relationships
Strength ofRelationship(i.e., Number ofcontacts/week
Quality ofRelationship
Depression Innate Abilityto Bond
EconomicStrength
InnateCoping Skills
DisabilityAgingand
DiseasePotency
Figure 3. Factors modulating the ability of social relationships to affect the aging process.
18 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Another study examined the effects of social factors onaging in centenarians in Okinawa, Japan. This populationhas changed its diet from a calorie restricted, sweet po-tato base to a higher calorie, rice and meat base and, atthe same time, has decreased its energy expenditure. Earlyreports suggest that these lifestyle changes may be delete-rious as males in Okinawa now have a lifespan that hassunk from 1st to 26th among the prefectures in Japan.
Religion andSpirituality
An emerging litera-ture recognizes the roleof religion and spiritual-ity in the preservation ofpsychological andphysical health of olderpersons. Overall, reli-gion and spirituality im-prove psychologicalhealth with a lesser ef-fect on physical health,although not all forms ofreligion are positive. Therole of religion and spiri-tuality in health may be
that it increases coping skills and enhances access to sup-port groups. Health care professionals need to be awareof the religious and spiritual affiliations of their patients and,in appropriate cases, be prepared to incorporate them intoa holistic model of health care. Prayer is a commonly usedcoping strategy for many older persons dealing with dis-ability or life-threatening illnesses. Involvement of a person’sreligious leader as part of the team approach to health careis important.
Anti-Aging MedicinePeople have long sought the mythical fountain of youth
(Fisher and Morley, 2002). This has lead to unscrupulouspeople selling their version of “snake oil” to vulnerable olderpersons. Within recent times, pseudoscientific claims as-sociated with the growth hormone anddehydroepiandrosterone as agents that will “reverse theaging process” regularly appear in newspapers, magazinesand books. Many of these claims are based on flawedstudies originally published in mainstream medical jour-nals. Others are based on hypotheses developed by sci-entists and published in mainstream literature and then
translated as fact by the lay press. For example, the claimby Linus Pauling that megavitamins will protect cellsfrom free radical damage remains alive today, despite stud-ies suggesting that instead of prolonging life, they mayshorten it.
Stem cells are a promising therapy that might reverseaging of muscle and cure Alzheimer’s disease. This researchis accruing in Israel and South Korea, while under em-bargo in the United States. Such social factors will limit therigor of scientific exploration into the role of stem cells andmay eventually limit their use to the very rich.
The Environment and the GenomePharmacogenomics has shown that the efficacy and side
effects of drugs are associated with specific alleles. Forexample, persons with the apolipoprotein E (APOE) allelehave different responses to the antidepressant, paroxetine,depending on the allele (Shanahan and Hofer, 2005). Sideeffects from paroxetine are related to the number of Calleles of the HTR2A gene which codes for the serotoninreceptor 2A.
The environment can modulate gene expression. Twoexamples have been found with the APOE4 gene: (i) Headinjury accelerates Alzheimer’s disease in persons who havethe APOE4 allele (Mayeux et al., 1995); (ii) APOE4 is arisk factor for ischemic heart disease predominantly insmokers (Humphries et al., 2001). The interaction of amajor life event with a genetic predisposition increases thelikelihood of major depression. Physical exercise producesdifferent responses depending on the person’s angiotensinconverting enzyme insertion deletion genotype.
These simple examples represent only the start of theexploration of gene/environment interactions. It is both the
(continued on page 20)
phot
o co
urte
sy w
ww
.cli
part
.com
phot
o co
urte
sy w
ww
.cli
part
.com
Aspects of Aging(continued from page 18)
Aging Successfully, Vol. XV, No. 2 19Questions? FAX: (314) 771-8575 • email: [email protected]

genome and the environment that eventually deter-mines the successful aging potential of a person. Thenew social science of aging in the 21st century willrequire the inclusion of the person’s genetic back-ground to allow full interpretation of environmentalaffects.
Elder AbuseApproximately 5% of older persons suffer elder
abuse. In most cases this is due to neglect. Overall,persons who abuse older persons are more likely tohave been abused when they were young and to havea mental illness. The solutions to elder abuse are com-plex, ranging from criminal prosecution and separa-tion of the elder from the abuser to psychosocialtherapies including such options as daycare, respitefor the caregiver and increased home care.
The InternetAlthough older persons are much less likely to
use the Internet than are younger adults or children, manynursing homes offer Internet facilities for older per-
sons to communicate with family, as well as to accessthe news. Older persons are also using the Internet toobtain healthcare information. With the movement ofthe “Baby Boomers” into the young-old cohort overthe next decade, these uses are expected to increaseexponentially. There will be increased communica-tion between physicians and their patients via the
Internet. We can expect to see an increase in telemedicine asa more technologically adept group of persons join the oldcohorts.
Cultural CompetencyShifts in populations require that health professionals ac-
quire cultural competency and that social policy adapts tocreate more health professionals from ethnic minorities.Throughout the United States, immigration of religiously andpolitically persecuted persons, many with war-time experi-ences of torture and displacement, are presenting healthcareprofessionals not only with new medical, but also with newsocial and cultural, challenges. Changes such as these requiretraining programs for health professionals in the beliefs of dif-ferent cultures and how they impact the interactions betweenolder persons and their healthcare providers.
Emergencies and DisastersIn all emergencies and disasters, whether human-made or
natural, older persons are disproportionately affected. Socialinterventions that healthcare professionals can use to improvethe survival of elders were discussed in an earlier Aging Suc-
cessfully (Vol. XIII (2), 2003). Itis the responsibility of all to seethat older persons are properlyprepared for disasters, cared forduring disasters, and returned totheir homes after disasters.
Referencesde Groot LCPMG, et al. J Gerontol Med
Sci 2004;59A: 1277-1284.
Fisher A, Morley JE. J Gerontol Med
Sci 2002;57A:M636-M639.
Humphries SE, et al. Lancet.
2001;358:115-119.
Johnson W, Kreuger RF. J Gerontol
Soc Sci. 2005;60B (Spec Issue I):65-78.
Karlamangla A et al. J Clin Epid.
2002;55:699-710.
Mayeux R, et al. Neurology.
1995;45:555-557.
Shanahan MJ, Hofer SM. J Gerontol Soc Sci 2005; 60B(Spec Issue
I):65-78.
Suda Y et al. J Nutr Hlth Aging. 2001;5:118-123.
Valiant GE. Aging well. New York: Little, Brown & Co. 2003.
Aspects of Aging(continued from page 19)
phot
o co
urte
sy w
ww
.cli
part
.com
This article is exerpted from Principles and Practice of GeriatricMedicine, Fourth Edition, Vol. 1-2, Editors: MS John Pathy, Alan J.Sinclair, and John E. Morley.
20 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Saint Louis UniversityGoes InternationalInternational Aging and Nutrition Meeting Held in St. Louis
Professor Bruno Vellas and SaintLouis University faculty organizedthe 3rd International Aging andNutrition Meeting in St. Louis inMay. Over 300 attendees heardpresentations from 60 faculty. Ple-nary sessions, including talks onNutrition and Alzheimer’s Diseaseby Professor Vellas, CardiacCachexia by Professor StefanAnker, Nutrition in Europe by Pro-fessor Wija van Stavaren, Exercisein the Older Person by ProfessorWilliam Evans, and Anorexia of Ag-ing by Professor Ian Chapman.
Among the symposia, the prob-lem of weight loss was highlighted.There were discussions on comple-
mentary medicine and nutritioneducation for older persons.The nutritional aspects of dia-betes and osteoporosis werecovered in detail. The role offree radicals and fruits andvegetables in dementia werehighlighted. The InChianti
group led by Luigi Ferrucci gavean outstanding series of presen-tations on the nutritional findingsof this Italian Aging Study.
A highlight of the conferencewas an evening on a paddle
steamer on the Mis-sissippi River. Thejazz band included anumber of membersover 80 years of age.
The next Interna-tional Meeting willbe held in Adelaide,Australia, under theorganizational skillsof Ian Chapman inSeptember, 2007.
Saint Louis University Jointly Sponsors Aging Meeting in BogotaTogether with
F u n d a c i o nCardio-Infantil,Saint Louis Uni-versity jointlysponsored the2nd InternationalGeriatric meet-ing in Bogota,Colombia. Themeeting was at-tended by over600 social work-ers, nurses, andphysicians. Themeeting was opened by the Minister of Healthfrom Colombia, Dr. Diego Palacios, who high-lighted the rapidly increasing older population
Saint Louis UniversityGoes International
Professor Cabrera proudly shows his guests the heartfountain which depicts blood flow through the heart.
Saint Louis University’s Dr.David Thomas is interviewed inSpanish by a local televisioncrew in Colombia.
Aging Successfully, Vol. XV, No. 2 21Questions? FAX: (314) 771-8575 • email: [email protected]
in Colombia and the need for increasing the servicesavailable for the elderly. The organizers in Bogotawere Professor Cabrera, Professor Dennis, and Dr.Silvia Cuenca. Presentations were made by Dr. DavidThomas, Dr. John E. Morley, and Dr. Oscar Cepedafrom Saint Louis University.
medication. We had a farewell partywith meat patties and sodas. Pass-ersby gawked as music blared and thesound of festivities emanated fromthe old peoples home.
Next, we traveled to Bodo tovisit the old rural Nigerians in theirnatural habitat. We arrived at St.
Patrick’s church on a Monday. Fa-ther Boniko had announced at Sun-day mass that we would be arriving.We set up shop in the only avail-
able space, the church. As Isat facing the crucifix, pre-paring to minister to sick el-ders, I f inally grasped thesignif icance of the Jesuitministry at Saint Louis Uni-versity. I thought of Father JimBaker and Father Boniko,worlds apart, so different andyet so alike. My philosophi-
cal musings were rudely inter-rupted by a flood of elders fromvillages far and near. The wordhad spread and they had madetheir way, walking several miles,some suppor ted by youngadults, others with canes; all ea-ger to be seen by a physician,
some for the first time ever. Wesaw one hundred and fifty-fourelders on that day. I diagnosedhypertension, cardiac failure,syphilitic heart disease, chronicbronchitis, diabetes, malnutri-tion, possible tuberculosis, evencancer. Yet, in the midst of somuch poverty and disease theywere all very grateful, courteous,and optimistic. Father Bonikodonated one of his bedrooms forpatients who needed to be fullyundressed for examinations.
(continued from page 17)
‘…from the diary of a cynical missionary…’
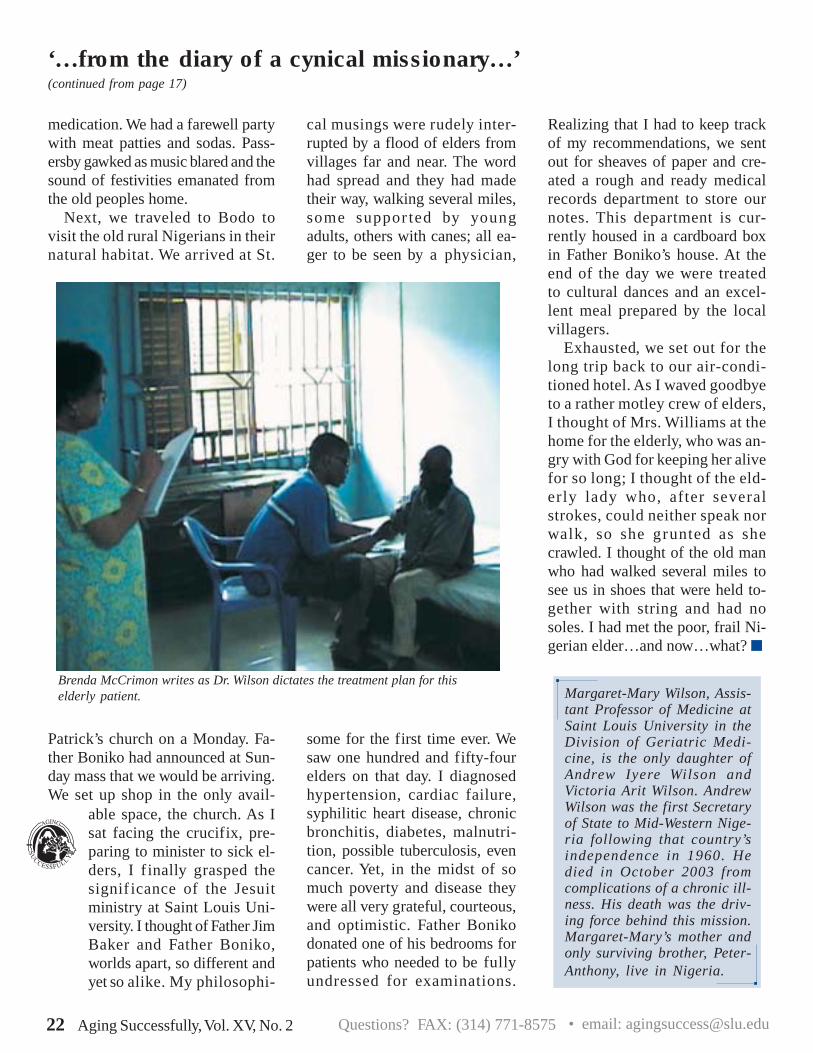
Brenda McCrimon writes as Dr. Wilson dictates the treatment plan for thiselderly patient.
Realizing that I had to keep trackof my recommendations, we sentout for sheaves of paper and cre-ated a rough and ready medicalrecords department to store ournotes. This department is cur-rently housed in a cardboard boxin Father Boniko’s house. At theend of the day we were treatedto cultural dances and an excel-lent meal prepared by the localvillagers.
Exhausted, we set out for thelong trip back to our air-condi-tioned hotel. As I waved goodbyeto a rather motley crew of elders,I thought of Mrs. Williams at thehome for the elderly, who was an-gry with God for keeping her alivefor so long; I thought of the eld-erly lady who, after severalstrokes, could neither speak norwalk, so she grunted as shecrawled. I thought of the old manwho had walked several miles tosee us in shoes that were held to-gether with string and had nosoles. I had met the poor, frail Ni-gerian elder…and now…what?
Margaret-Mary Wilson, Assis-tant Professor of Medicine atSaint Louis University in theDivision of Geriatric Medi-cine, is the only daughter ofAndrew Iyere Wilson andVictoria Arit Wilson. AndrewWilson was the first Secretaryof State to Mid-Western Nige-ria following that country’sindependence in 1960. Hedied in October 2003 fromcomplications of a chronic ill-ness. His death was the driv-ing force behind this mission.Margaret-Mary’s mother andonly surviving brother, Peter-Anthony, live in Nigeria.
22 Aging Successfully, Vol. XV, No. 2 Questions? FAX: (314) 771-8575 • email: [email protected]

Been Here? Done This ?Offering regular updates on geriatrics, Cyberounds, an internet-basededucational program for physicians and other health providers, is editedby Dr. John E. Morley. The internet address for Cyberounds is:
www.cyberounds.comA cybersite for seniors has been developed in collaboration with SaintLouis University and the Gateway Geriatric Education Center. Besidesarticles written by geriatric experts, this site provides health updates andan interactive question and answer section. The address for this site iswww.thedoctorwillseeyounow. See you in cyberspace!
Upcoming CME Programs
17th Annual Saint LouisUniversity Summer GeriatricInstitute
Caring for theVulnerableJune 6-8, 2006
All of the conferences will be held at Saint Louis University, except as noted. For moreinformation about any of these conferences, please call
314-977-8848.
SaintLouisUniversityGeriatric Academy(SLUGA)January 9-13, 2006 on theSaint Louis University Campus
Caringfor theVulnerable
17th Annual Saint LouisUniversity Summer GeriatricInstitute
14th Annual Multi-DisciplinaryCertificate Program in Geriatrics for
Non-PhysiciansIn Downers Grove, Illinois onFridays, Sept. 9, 23, Oct. 7, 21,Nov. 4, and 18, 2005.In Bloomington, Illinois onFridays, Sept. 16, 30, Oct. 14,28, Nov. 11, and Dec. 2, 2005
AnnualMulti-DisciplinaryCertificateProgram inLong-TermCareAdministrationand ManagementIn Oak Brook, Illinois onWednesdays, Sept. 28, Oct. 12,26, Nov. 9, 23, and Dec. 7, 2005.
17th AnnualSLU School ofMedicineSymposium forMedicalDirectors
NURSINGHOMEISSUESSaturday, Dec.10, 2005
Universityof the Third
AgeConference
November 5,2005
University ofthe Third
Age
Fall 2005
Aging Successfully, Vol. XV, No. 2 23Questions? FAX: (314) 771-8575 • email: [email protected]

Non-Profit Org.U. S. Postage
PAIDSt. Louis, MOPermit No. 6
This newsletter is a publication of:
Division of Geriatric Medicine
Department of Internal Medicine
Saint Louis University School of Medicine
Geriatric Research, Education, andClinical Center (GRECC)
St. Louis Veterans Affairs Medical Center
Gateway Geriatric Education Center of Missouri andIllinois (Gateway GEC)(supported by a grant from the Bureau of HealthProfessions, Health Resources and Services Administration)
John E. Morley, M.B., B.Ch.Dammert Professor of Gerontology andDirector, Division of Geriatric MedicineDirector, Gateway Geriatric Education CenterDepartment of Internal MedicineSaint Louis University School of Medicineand Director, GRECC, St. Louis VeteransAffairs Medical Center
Nina Tumosa, Ph.D.EditorHealth Education Specialist, GRECCSt. Louis VAMC-Jefferson Barracksand Executive Director, Gateway GECProfessorDivision of Geriatric MedicineDepartment of Internal MedicineSaint Louis University School of Medicine
Carolyn E. PhelpsAssistant Editor
Please direct inquiries to:Saint Louis University School of MedicineDivision of Geriatric Medicine1402 S. Grand, Room M238St. Louis, Missouri 63104e-mail: [email protected]
Please fax the mailing label below along withyour new address to 314-771-8575 so you won’tmiss an issue! If you prefer, you may email usat [email protected]. Be sure to type theaddress exactly as it appears.
Division of Geriatric MedicineSaint Louis University School of Medicine1402 South Grand BoulevardSt. Louis, Missouri 63104
SUCCESSFULLYgingA