soapping case study
TRANSCRIPT

University of sulaimaniaCollege of pharmacy
Pharmacy practice experience II
Case SOAPing
Muhammad Kokash Sdiq
B.Sc. In pharmacy
1

case• T…M is 60 year old male who is gainer and have chronic
hypertension for 10 years ago who presents to the medical clinic at 3 a.m. With complaints for his sever chest pain for 3 hr. Radiated to both shoulders , nausea but no vomiting , abdominal pain , but he is conscious his blood pressure is 110/70 , troponin test is positive , ST segment elevated in v1 ,v2 . PR= 86 bpm , spo2 = 96% , R.B.S= 155 mg/ dl .
• The patient has HTN and Hyperlipidemia and two days ago undergo dental extraction . Echo show that there is no blood supply to part of myocardium by occlusion of coronary artery .
• The ECG indicates ST segment elevation. • Family history: his father died because of HTN and MI. His sister
also has Hyperlipidemia.• Social history: no smoking , past- IBS . Second attack .• Drug history: no drug allergy, on anti-hypertensive drug ( unknown) • They agreed for thromboembolic agent just for one time . • Diagnosis indicate ST segment elevated MI.
2
Subjective
• Name : T…M• Sex : male • Age :60• Chief compliance : sever chest pain for 3 hr. radiated to both
shoulders , nausea but no vomiting , abdominal pain , and sever head ache but he is conscious .
• past medical history: no drug allergy, on anti-hypertensive drug ( unkown but take diuretic for 4 month ) .
• Social history: no smoking , HTN and Hyperlipidemia. past- IBS (now he are not taking any medication for this condition ) . Secondary rise of BP , two days ago undergo dental extraction ).
• Family history: his father died because of HTN and MI. His sister also has Hyperlipidemia.
3
Objective
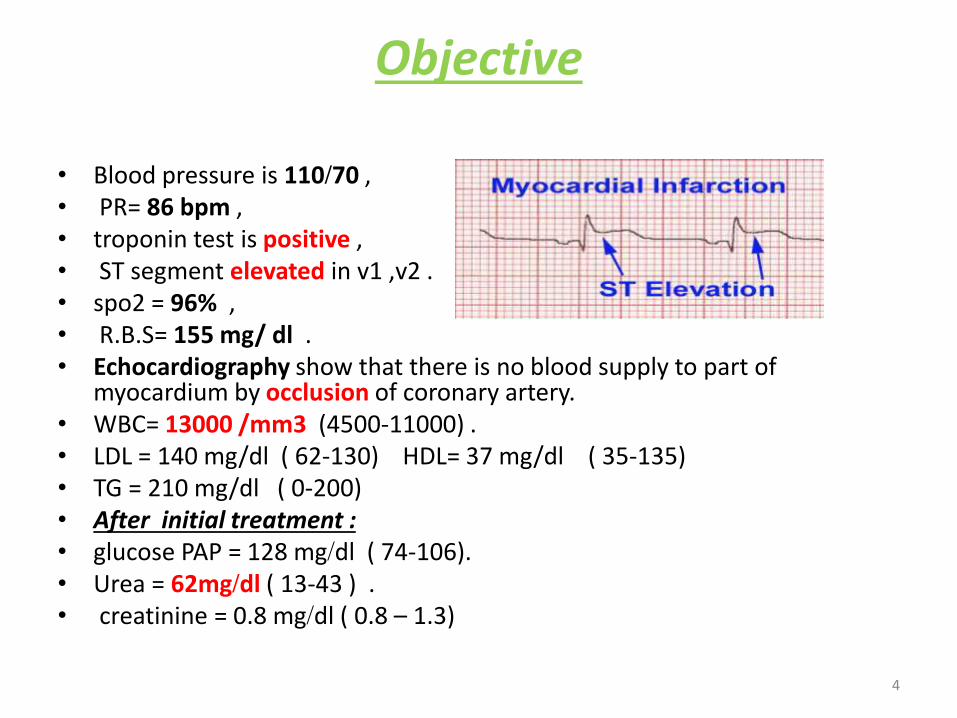
• Blood pressure is 110/70 ,• PR= 86 bpm , • troponin test is positive ,• ST segment elevated in v1 ,v2 .• spo2 = 96% ,• R.B.S= 155 mg/ dl .• Echocardiography show that there is no blood supply to part of
myocardium by occlusion of coronary artery. • WBC= 13000 /mm3 (4500-11000) . • LDL = 140 mg/dl ( 62-130) HDL= 37 mg/dl ( 35-135) • TG = 210 mg/dl ( 0-200) • After initial treatment : • glucose PAP = 128 mg/dl ( 74-106). • Urea = 62mg/dl ( 13-43 ) .• creatinine = 0.8 mg/dl ( 0.8 – 1.3)
4

Assessment
• Sudden sever chest pain radiated to the shoulder with nausea and troponin test positive and ST segment elevation is diagnosis of ST segment elevated MI. high level of WBC may indicate necrosis .
• Resulted from either :
• non-compliance to antihypertensive drug .
• does not take medication for his hyperlipidemia .
• dose not control his salt and fat intake .
5

Planning
• Initial medication for emergency care :• Put Cannula for patient • Aspirin tablet 300 mg 1X1 in first day than maintained
on tablet 100 mg 1X1for two day .• Plavix ( clopidogrel) tablet 300mg 1X1 in first time
than maintained on tablet 75 mg 1X1 for two day ..• Motalase vial 1X1 just for one time . • Metoprolol tablet 50 mg 1X2for two day . .• Atorvastatin tablet 80 mg 1X1 for two day ...• Lisinopril tablet 5 mg 1X1 for two day ..• Zantac ( ranitidine ) tablet 150 mg 1X2 for two day ..
6

Planning . continue
On need medication :
• Morphine ampule 2.5 mg 1X1 at time of attack .
• Plasil ampule 1X1 for vomiting .
• Angesid( glyceryl trinitrate ) tablet 1X1 at time of chest pain .
7

Planning . continue
Recommendation :
• Patient should continue on his initial medication until weeks and monitor .
• Motalase should not given more than once .
• Taking of zantac tab 150mg 1x2 for qday.
8

Aspirin dose should be monitordbecause of:
Significant intraction - Monitor Closely : • aspirin decreases effects of metoprolol by
pharmacodynamic antagonism. • aspirin, clopidogrel. Either increases toxicity of the other by
pharmacodynamic synergism. • lisinopril, aspirin. Either increases toxicity of the other by
Other. May result in renal function deterioration, particularly in elderly or volume depleted individuals.
• aspirin decreases effects of lisinopril by pharmacodynamicantagonism. NSAIDs decrease synthesis of vasodilatingrenal prostaglandins, and thus affect fluid homeostasis and may diminish antihypertensive effect.
• metoprolol and aspirin both increase serum potassium.
9

Follow up • In 24 hours to assess drug therapy changes and record outcomes.
• Arrange for follow-up within 2 weeks of discharge. Arrange for cardiac rehabilitation.
• Good controlling of coagulation state by regular taking of aspirin 75mg 1x1 and clopidogrel 75mg 1x1 but if clopidogrel used along is better to prevent drug intraction of aspirin or clopidogril used if patient not tolerate aspirin , according to regular test for 6 month by PT , PTT , BT , CT .
• Good control of HTN by lisinopril 5 mg 1x1 for 6 weeks and/or metoprolol 50mg 1x2 for 5 weeks then monitoring and follow up required .
• Good control of lipid profile by atorvastatin 10-20 mg 1x1 for years and monitor .
• Monitor renal and liver function because many drug excretd through urine .
• Regular follow up of ECG .
• Good monitoring of Vital signs .
• Good adherence to medication to prevent recurrent attack and complication .
• Take zantac for reducing risk of GI bleeding through out the course of antiplatelet drugs .
10
Follow up continue
• Change in life style and diet intake
• Initially, (NPO)
• Following the patient’s initial therapy and admission, A low-salt, low-fat, and low-cholesterol diet is generally recommended.
• Confine patients to bed rest
• Call on call with doctor .
11
Thank you
12

• Statins: In addition to cholesterol- lowering properties, statin has antithrombatic & antiproliferative properties.• ACE-Inhibitors :Useful in patients with signs of heart failure, tachycardia or a history of previous infarction. It should be started with 24 hrs. of diagnosis. Initial doses should be low then titrated as quickly as the patient tolerated.• Zantac : To prevent stress ulceration .
• Morphine ; ( Narcotic analgesic): It is important because pain & anxiety associated with MI will contribute to increase myocardial O2 demand . There is no benefit in leaving a patient in pain while the diagnosis is considered . Morphine as a pain killer ,should administrated rapidly with an antiemetic drug such as plasil .• Angesid : Nitrates These agents may help to relieve pain , especially if coronary spasm produce the MI. This is because the pain of MI can trigger the release of catecholamine which can produce a coronary spasm.
13

Drug information and monitoring
• AntiplatelatLow doses are as effective as higher doses & have a lower risk of GI hemorrhage .Advice the patient to take it with food .C/I in bronchospasm &a history of GI bleeding.Clopidogrel: Useful as an alternative to aspirin in patients who are allergic or cannot tolerate aspirin .• Thrombolytic agents :It is indicated for suspected MI with chest pain of less than 6 hrs. Also for patient with ST-segment elevation unrespond to NG . • Metoprololuse to reduce mortality in patient with MI to prevent recurrent MI and complication . Is selective b-blocker, consider that its block-ing properties (usually at higher doses) may contribute to SOB due to bronchoconstriction, negative inotropic effects, or both.
14

According to Guide line ACC /AHA
• The long-term use of aspirin results in significant reduction in subsequent mortality rate. The prescription of 75-162 mg/d of aspirin indefinitely is a class I recommendation for patients with STEMI.
• Beta-blocker therapy has confirmed therapeutic benefit in survivors of acute myocardial infarction.
• The use of ACE inhibitors in patients with known coronary artery disease has been shown to reduce mortality rate.
• patients should achieve a low-density a lipoprotein (LDL) level of less than 100 mg/dL, a high-density lipoprotein (HDL) level of greater than 40 mg/dL, and a triglyceride level of less than 200 mg/dL.
• Atorvastatin significantly reduced the frequency of the combined end point of death, recurrent death, myocardial infarction, or worsening unstable angina requiring hospitalization.
• Clopidogrel should be prescribed for a year following discharge if the patient has no contraindications and cost is not prohibitive. To reduce the risk of bleeding, the aspirin dose can be reduced to 75 mg.
15