sliding osteotomy genioplasty for facial aesthetic … · transient, usually lasting for only a few...
TRANSCRIPT

Sliding Osteotomy Genioplasty for Facial Aesthetic Balance:
10 Years of Experience
Johannes Franz Hoenig, M.D., D.M.D., Ph.D.1
University Hospital and Medical School of Goettingen, Plastic Surgery Center, Paracelsus Clinic, Hannover, Germany
Abstract. The chin, one of the most obvious facial struc-tures, plays an important role in the perception of the faceas an instrument of communication. To alter the chin
contour in a reliable manner, horizontal sliding osteotomyof the mandibular symphysis with advancement of themobilized segment is the technique of choice for correctionof the anterior posterior deficiency. This study describes
surgical techniques used in aesthetic and functional surgeryof the chin as well as the outcomes. Over a 10-year period,474 patients underwent orthognathic surgery for correction
of their malocclusion. Of these 474 patients, 155 weretreated in combination with a sliding genioplasty (SGP)and 37 (29 women and 8 men; average age, 32 years; range,
18�47 years) had an isolated SGP. Of these patients, 33had chin advancement and 4 had chin reduction. The meanchin advancement was a modest 4.5 mm (range, 2�7 mm),and the mean chin vertical displacement was 3.9 mm
(range, 2.5�4.1 mm). All the patients in the mandibulardeficiency group had a residual sagittal disproportion of theprogonion relative to the subnasale (mean, �7.6 mm) and a
newly created vertical disproportion, with mean lower faceheights of 67.8 mm compared with mean midface heights of65.3 mm. The surgical outcome was evaluated by analysis
of pre- and postoperative photographs, analysis of pre- andpostoperative measurements, and patients� self judgment.All the patients healed uneventfully without any major
postoperative problems. Paraesthesia of the mental nervesoccurs to some degree in almost all patients measured bythe Simmon Weinstein diagnostic device. In the singlesliding chin osteotomy group, no major branches of the
mental nerves were transacted. Paraesthesia was only
transient, usually lasting for only a few weeks. At least 1year after the operation, normal sensitivity of the lower lipand both sides of the chin was reported by almost all of the
patients (93.1%). All who had only a single genioplastyrecovered totally from a neurosensory deficit. The level ofsatisfaction was significantly high for all the patients. Theresults were judged to be excellent in 73.2% and good in
23.6% of the cases. Only in 3.2% of the cases was it con-sidered to be poor (bimaxillary surgery combined withSGP). The current findings strongly suggest that SGP is a
reliable procedure for achieving harmony of the lower face.In addition, it permits a simplification of facial recon-struction and rejuvenation. The combination of chin
advancement and submental recontouring can have a po-sitive effect on facial appearance, provided the increasedchin projection is appropriate.
Key words: Facial balance—Facial harmony—Facial reju-
venation—Genioplasty
The chin, one of the most obvious facial structures, isthe basis for judging ‘‘human character.’’ A weakchin is associated with femininity, a strong chin withmasculinity. Because undesired characteristics areassociated with a weak chin, society seems to preferfacial forms with a least some chin prominence, morein men than in women [7,13,18].
Only within the last quarter century have surgicaltechniques been perfected to alter the chin contour ina reliable manner [1,2,6,8,9,10,12,13,16,21,24]. Avariety of surgical techniques for augmenting acontour-deficient chin have been described [5,8,10,15,16,17,21,23,24] since Hofer [11] introduced thehorizontal sliding osteotomy of the inferior anteriorborder of the mandible in 1942.
Correspondence to J.F. Hoenig, M.D., D.M.D., Ph.D.;
Georg-August-University Hospital and Medical School ofGoettingen, Robert-Koch-Street 40, 37075 Goettingen,Germany; email: [email protected]
Aesth. Plast. Surg. 31:384�391, 2007DOI: 10.1007/s00266-006-0177-6
Original Article

Currently, the horizontal sliding osteotomy of themandibular symphysis with advancement of themobilized segment is the technique of choice for cor-rection of anterior posterior deficiency, known as mi-crogenia (decrease of chin eminence with an essentiallynormal mandible). This technique achieves harmonyof the lower face because the results are predictableand stable [10,13,16,19,21,24]. This article describesthe surgical techniques used in aesthetic and functionalsurgery of the chin and discusses patient evaluation.
Methods
Assessment
A face is balanced when the upper middle and lowerthirds are approximately equal in size and the struc-tures within each segment are proportional in sizeand prominence [1,3,10], especially when the lengthof the nose and the height of the lower face are inbalance [3,9]. Therefore, the chin should also be inharmony with the jaw as well as with the structures inthe middle third of the face.Anatomically, the chin is the area below the labio-
mental fold. The vertical portion of the deep point ofthe labiomental fold has considerable effect on theappearance of the chin. For good balance, it should belocated near the midpoint between the superior borderof the lip and the inferior border of the chin. This pointcorresponds to the juncture between the lower and themiddle thirds of the lower third of the face.The shape of the labiomental fold is influenced by
all the factors that control lower lip contour, espe-cially bony chin proportion and length, mentalmuscle thickness, and soft tissue chin thickness [3,4].A consistent relationship of 1:75 between bone and
soft tissue change has been confirmed [14,19,20]. Thisis supported by our results indicating that minimalsoft tissue detachment allows closer correlation ofbone and soft tissue movement.The general contour, depth, and height of the
submental fold determines the aesthetic appeal.Many landmarks are recommended for determin-
ing a normal prominence of the chin. In a cephalicradiography, according to Gonzalez-Ulloa and Ste-vens, a vertical reference line perpendicular toFrankfurt�s plane beginning at the nasion provides aconvenient reproducible mechanism for determiningthe relationship of the chin to the remainder of thefacial profile. With a normal chin prominence, thisline should lie tangential to the progonion.A more common measurement for assessing ade-
quate chin projection is its relationship to the lowerlip. A man�s chin should approach, but not exceed, aline from the lower vermillion border in repose.A woman� chin, however, is ideally situated 2 to 3 mmbehind this line [10]. However, analysis of facialaesthetics is more complex than simply using a single
profile reference line. A multitude of complex inter-relationships among other facial structures must beconsidered when the position for any part of the faceis altered. Consequently, the final decision as to theposition for the chin must be made by evaluating thepatient in a clinical setting.
Surgical Technique
The surgical treatment of the skeletal malformationwas carried out under aseptic conditions in a sterilefield and with perioperative antibiotic cover. Systolicblood pressure was maintained below 100 mm ofmercury, thus minimizing bleeding.
After temporary intermaxillary fixation, a vestibu-lar stair step incision of the mucosa was performed5 to 8 mm labial to the depth of the vestibulum at aright angle to the surface only. Then it was directedhorizontally to the alveolar process from one cuspidto the other. The periosteum was incised from beneaththe mental foramen as far back as necessary fromcuspid to cuspid. The superficial branches of themental nerve were exposed. The chin prominence wasminimally degloved subperiosteally to maximizeattachments of the integument to the anterior andinferior border of the mandible while providingaccessibility for the planned bone incision withoutdetaching the soft tissue pedicle from the mid sym-physis.
The planned osteotomy was marked, and themidline vertical reference line was etched into themidsagittal plane of the chin across the osteotomyline. The chin repositioning clamp was applied to thechin and fixed with two 6-mm-long screws parasag-ittally beneath the planned osteotomy line (Fig. 1aand b). The mental nerve and continuous soft tissueflaps were retracted and protected while osteotomy ofthe chin was extended laterally and posteriorly with areciprocating saw blade (Fig. 2a and b). Once thehorizontal osteotomy was started, the bone was sec-tioned completely as soon as possible with a recip-rocating saw.
After meticulous control of the bleeders, theosteotomized segment was fixed with two miniplates(2 whole plates) applied in the paramedian withmonocortical mini screws in the new position (Fig. 3aand b). The chin reposition tool was removed. Thenew profile was checked, and wound closure wasperformed with 2 · 0 nonabsorbable interrupted su-tures (Fig. 4). The temporary intermaxillary fixationwas released, and a pressure dressing was applied forapproximately 3 days.
Clinical Experience
Over a 10-year period, 474 patients with an averageage of 21.5 ± 3.7 years underwent orthognathicsurgery to correct their malocclusion. Of these pa-
J. F. Hoenig 385

tients, 134 underwent bimaxillary surgery, and 41also underwent a sliding genioplasty (SGP). A totalof 128 patients underwent isolated mandibleadvancement to improve malocclusion and mandibleretrusion. Of these patients, 61 were treated in com-bination with SGP advancement. A total of 57 pa-tients underwent correction of their mandibularprotrusion by a setback of the mandible. In thisgroup, the mandibular setback was combined withSGP and chin advancement in 16 cases. Single SGPwith chin advancement to harmonize the profile
(microgenia) was performed for 37 patients (29women and 8 men) with an average age of 32.3 years(range, 18�47 years). In this group, 33 patientshad chin advancement and 4 had chin reduction(Table 1). All the patients underwent a thorough,individualized preoperative evaluation for a correctdiagnosis and evaluation of the malocclusion.
The surgical outcome was evaluated by analysis ofpre- and postoperative photographs, analysis of pre-and postoperative measurements, and patients� self-judgment.
Fig. 3. (a) Schematic drawing of thesliding genioplasty (SGP). The inferiorsegment has been advanced. It is fixedin the new planned position with twoparamedially applied osteosynthesisplates. The chin repositioning clamp isstill in place. (b) Intraoperative situs ofthe SGP. The chin has been advanced5 mm anteriorly and 2 mm downward.The resulting gap will reossify duringthe next 3 months.
Fig. 1. (a) Schematic drawing of the sliding genioplasty (SGP). The osteotomy is performed with a reciprocating saw 3 to4 mm beneath the mental foramen. Note the temporary intermaxillary fixation to ensure a stable position for a preciseosteotomy. The chin repositioning clamp is fixed to the chin segment with two 6-mm screws beneath the osteotomy line.(b) Intraoperative view of the SGP. The mental nerves are protected while the osteotomy is performed.
Fig. 2. (a) Schematic drawing of the sliding genioplasty (SGP). The inferior bone segment has been displaced downward. Thegenioglossus and mylohyoid muscles come into view. (b) Intraoperative view of the SGP. The inferior segment, which is fixedto the chin repositioning clamp, is displaced downward. Note the protruding genioglossus muscles along with some fat in themiddle of the osteotomy gap.
386 Sliding Osteotomy Genioplasty

Results
The median follow-up time was 5.4 years. Immediatehealing was achieved without complications or ad-verse reactions. The mean chin advancement was amodest 4.5 mm (range, 2�7 mm), and the mean chinvertical displacement was 3.9 mm (range, 2.5�4.1mm). All the patients in the mandibular deficiencygroup had residual sagittal disproportion of theprogonion relative to the subnasale (mean, �7.6mm). The newly created vertical disproportion in-volved mean lower face heights of 67.8 mm comparedwith mean midface heights of 65.3 mm.All the patients healed uneventfully without any
major postoperative problems. Infection after hori-zontal sliding osteotomy was uncommon. As mayoccur with any ‘‘degloving’’ exposure of the mandi-ble, superficial dehiscence of the mucosal incisionwith exposure of the underlying bone occurred in 15of the 474 patients. Four of these patients hadundergone SGP with more than a 5-mm advancementof the chin. Two of them also had Beta-Tri calciumphosphate (ß-TCP) augmentation above the slidingosteotomy for correction of the stair step. The sur-gical wound was irrigated daily through the mucosalwound margins, and antibiotics were prescribed for 5days.Paraesthesia of the mental nerves occurs to some
degree in almost all patients measured with the Sim-mon Weinstein diagnostic device. In the group thatunderwent single sliding chin osteotomy, no majorbranches of the mental nerves were transacted, andparaesthesia was only transient (usually a matter offew weeks) (Table 1). Of all 155 patients whounderwent SGP, 131 (84.52%) showed disturbancesof the mental nerve 1 month postoperatively(Table 2). At least by 1 year after the operation,normal sensitivity of the lower lip and both sides ofthe chin was reported by almost all except 15.48% of
these patients. In particular, all the patients whounderwent only an isolated SGP recovered totallyfrom any neurosensory deficit (Table 3).
The level of satisfaction was significantly high forall the patients. The result was judged to be excellentby 73.2% of the patients and good by 23.6% of thepatients. Only 3.2% of the patients judged it to bepoor. Nearly 90% of the patients who underwentisolated SGP estimated the results to excellent. Inlight of the experience gained to date, the long-lastingresults seem to be excellent. Figures 5 to 12 illustratethe indications and results.
Discussion
Genioplasty has gained popularity as a means ofenhancing chin projection [10,12,21,24]. It is a useful
Table 1. Surgical correction of the facial profile with orwithout a sliding genioplasty (SGP)
Surgery Without SGP With SGP
Single bimaxillary surgery 134Bimaxillary surgery plusSGP advancement
41
Single mandibularadvancement
128
Single mandibular advancementplus SGP advancement
61
Single mandibular setback 57Single mandibular setbackplus SGP advancement
16
Single SGP with chinadvancement
33
Single SGP with chin setback 4Total number of patients: 474 319 155
Fig. 4. Schematic drawing of the sliding genioplasty (SGP).The chin repositioning clamp has been removed. Themucoperiosteumis sutured while the intermaxillary fixationis still maintained.
Table 2. Nerve disturbances of 155 patients 1 and 12months after sliding genioplasty (SGP) in combination withjaw surgery
Patients with nervedisturbances afterSGP (n)
Patients withnerve disturbancesafter SGP (%)
Follow-up period(months)
131 84.52 124 15.48 12
Table 3. Nerve disturbances of 37 patients 1 and 12 monthsafter isolated sliding genioplasty (SGP)
Patients with nervedisturbances afterisolated SGP (n)
Patients with nervedisturbances afterisolated SGP (%)
Follow-up period(months)
14 37.83 10 0 12
J. F. Hoenig 387
and frequently applied technique in the armamen-tarium of the aesthetic facial surgeon [22]. It can alterthe position of the chin in a three-dimensional man-ner. The goal of surgery is to create a stable, pleasingchin contour that provides an anatomically correctskeletal shape.Many variations of the horizontal sliding osteoto-
my may be adopted to meet the individual�s aestheticsneeds. But the fact that the inferior alveolar canalcurves superiorly as it approaches the mental fora-men makes it mandatory that the horizontal osteot-omy be positioned 2 to 3 mm below the inferior edgeof the mental foramen to prevent injury to the neu-rovascular bundle.Therefore, a moderate decrease in the vertical
dimension of the chin can be achieved by obliquesliding osteotomy. By angling the bone cut superi-orly, the inferior segment can be transposed forwardand upward to reduce the chin height approximately5 mm. When larger height reductions are indicated, ahorizontal wedge of bone is removed above the hor-izontal sliding osteotomy.The anterior height of the osteotomy is dictated
by the direction that the segment must move toproduce the desired chin contour and prominence.If only horizontal augmentation is desired, theosteotomy should be performed parallel to thenatural horizontal plane. Horizontal and verticalaugmentation may be accomplished by directing theanterior part of the osteotomy below the naturalhorizontal. Shortening is produced by directingthe anterior base cut incision above the naturalhorizontal.When it is not feasible to direct the osteotomy at
the necessary angle and still maintain the desiredthickness of the segment, a wedge osteotomy may beused to shorten the chin and alter the direction offorward movement. An interposition bone graft
likewise permits lengthening the chin while segmentthickness is maintained.
Bone substitutes such as ß-TCP above the slidingosteotomy segment may be indicated to prevent for-mation of a deep angular labiomental fold [10]. Themore extensive the advancement performed, thegreater is the tendency to produce a deep angularlabiomental fold because of the larger step createdabove the advanced segment. By sculpting ß-TCPfrom cuspid to cuspid to achieve this step, theresulting soft tissue fold may be corrected to the de-sired form (Fig. 11b and e).
In cases of chin setback, small posterior move-ments have a minimal effect on the contour of themandible�s inferior border, and gradual remodelingof the repositioned segment restores the contour ofthe mandible�s inferior border to normal. Only whenthe amount of correction exceeds 3 to 4 mm are the
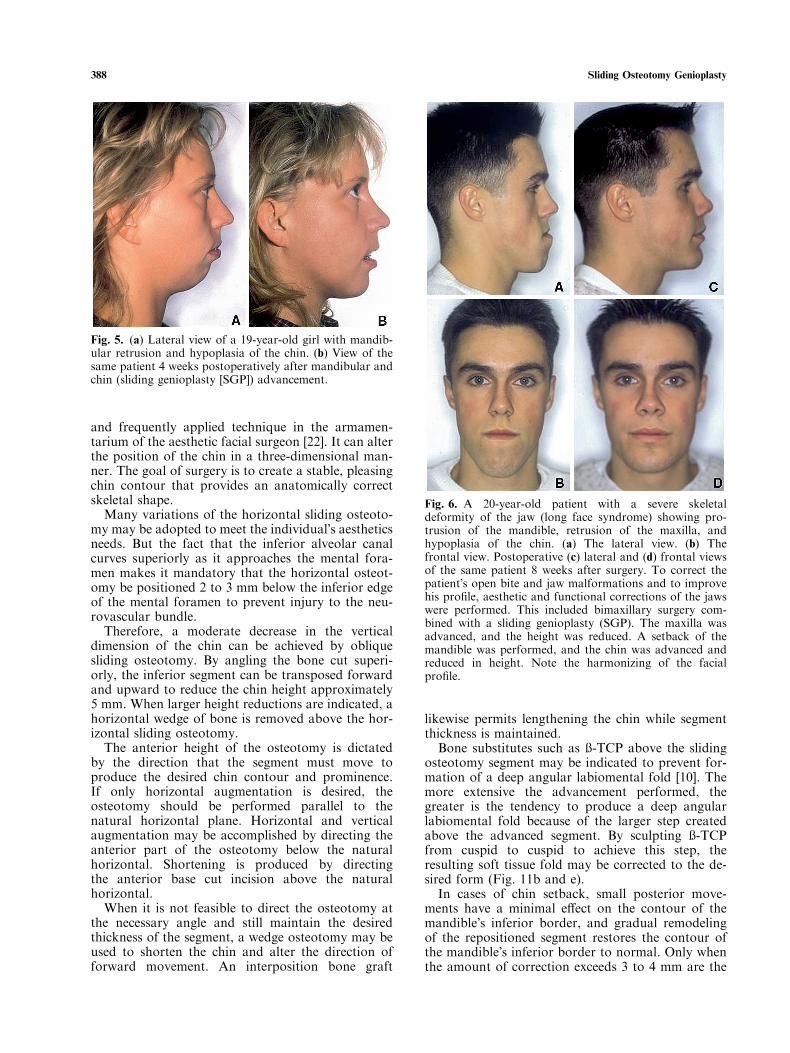
Fig. 5. (a) Lateral view of a 19-year-old girl with mandib-ular retrusion and hypoplasia of the chin. (b) View of thesame patient 4 weeks postoperatively after mandibular andchin (sliding genioplasty [SGP]) advancement.
Fig. 6. A 20-year-old patient with a severe skeletaldeformity of the jaw (long face syndrome) showing pro-trusion of the mandible, retrusion of the maxilla, andhypoplasia of the chin. (a) The lateral view. (b) Thefrontal view. Postoperative (c) lateral and (d) frontal viewsof the same patient 8 weeks after surgery. To correct thepatient�s open bite and jaw malformations and to improvehis profile, aesthetic and functional corrections of the jawswere performed. This included bimaxillary surgery com-bined with a sliding genioplasty (SGP). The maxilla wasadvanced, and the height was reduced. A setback of themandible was performed, and the chin was advanced andreduced in height. Note the harmonizing of the facialprofile.
388 Sliding Osteotomy Genioplasty

posterior portions of the mobilized segments usuallyshortened to maintain the desired contour of the skinat the inferior border of the mandible.
In cases of chin advancement, studies have shownthat the edges of the advanced segment are remod-eled and rounded off after 6 to 12 months. Theanterior projection of the segment remains stable[15].
Excessive subperiosteal dissection of the inferiormental symphysis area to facilitate the bony surgeryproduces unpredictable changes in the soft tissuedrape, and chin ptosis may occur as a consequence.Avoiding this complication, a more predictablechange in the soft tissue is achieved by keeping thesoft tissue attached to the inferior anterior border ofthe repositioned segment [10,13]. Preserving the soft
Fig. 7. A 22-year-old patient with hemifacial microsomiaof the face. The maxilla and the mandible are tilted to theleft (a) with a hanging occlusion line (b). (c,d) Postoperativeviews after bimaxillary surgery that involved removal of atriangle bone segment on the right side of the maxilla incombination with a Le Fort I osteotomy, a sagittal splitosteotomy of the mandible, and an oblique SGP. Note thethe chin midpoint brought back to the midsagittal plane,the corrected hemifacial microsomia, and the harmonyachieved in the facial proportion. Fig. 10. Lateral view of a 38-year-old woman with hypo-
plasia of the chin (a) before and (b) after SGP. To achieve aharmonized profile, a sliding genioplasty (SGP) was per-formed, bringing the chin 6 mm forward and shortening theheight by 3 mm.
Fig. 8. (a) Lateral view of a 20-year-old patient with severemandibular retrusion and sublabial fold. (b) Lateral view ofthe same patient 3 months after a 13-mm mandibularadvancement in combination with a sliding genioplasty(SGP).
Fig. 9. Lateral view of a 53-year-old woman with hypo-plasia of the chin and a fatty neck (a) before and (b) 4 weeksafter surgery. Liposuction in combination with chinadvancement (sliding genioplasty [SGP]) resulted in ayouthful neck contour and facial profile harmony.
J. F. Hoenig 389

tissue attachments to the anterior aspect of themobilized segment maximizes the soft tissue changein the vertical facial dimension and provides pre-dictable treatment planning [1,13]. If the chin isnarrow transversely, advancement will tend to makethe face appear even more tapered.
Conclusion
The lower jaw, especially the mentum, plays animportant role in the perception of the face as aninstrument of communication [7]. Horizontal slidinggenioplasty is a reasonable option, but should beconsidered only when the surgeon is well trained inthe technique and the deformity merits its use. Slid-ing genioplasty results in aesthetic and functionalchanges to the chin and perioral areas [19,21].The procedure combines osseous and soft tissuereconstruction to produce a superior result, whichis especially important for individuals with bila-bial incompetence [19]. The combination of chinadvancement and submental recontouring can have apositive effect on facial appearance, provided theincreased chin projection is appropriate.
Genioplasty is considered to be an easy and reliableprocedure for achieving harmony of the lower face[24]. Together with other authors, we recommendthe sliding genioplasty as a practical alternative toalloplastic chin augmentation [1,10,21,24].
Fig. 11. (a) Lateral view of a 19-year-old patient with an obtuse neck and asevere chin retrusion. (b) Intraoperativeview showing that sliding genioplasty(SGP) with chin advancement of 8 mmresulted in a stair step deformity, whichwas corrected by augmenting of bonesubstitutes. The bone substitutes werefixed paramedially with small osteo-synthesis screws. Allowing better accessto the operation field, the chin reposi-tioning clamp is still in place holding thelip away. (c) Lateral view of the patient4 weeks after chin advancement (SGP).Note the harmony of the profile and theimprovement in neck contour. Lateralplane radiograms (d) before and (e)after surgery. Note the advancement ofthe lower chin segment as well as thefixation and the correction of the stairstep deformity by augmenting bonesubstitutes placed on the inferior chinsegment.
Fig. 12. (a) Lateral view of a 48-year-old patient with asevere protrusion of the chin and hump deformity of thenose before and after surgery. The nasal hump was re-moved; the tip of the nose was reduced and elevated; andthe inferior chin segment was osteotomized and set backseveral millimeters. (b) Lateral postoperative view 12 weeksafter surgery. (c) The intraoperative situs. The inferior chinsegment is fixed in the new posterior position with twoparamedially applied osteosynthesis plates. For betteraccess, the chin reposition clamp is still in place.
390 Sliding Osteotomy Genioplasty

References
1. Bell WH, Dann JJ: Correction of dentofacial defor-mities by surgery in the anterior part of the jaws. Am JOrthod 64:162�1187, 1973
2. Brusati R, Gianni AB: Anterior mandibular apical baseaugmentation in the surgical orthodontic treatment ofmandibular retrusion. Int J Oral Maxillofac Surg34:846�850, 2005
3. Burstone CJ: Lip posture and its significance in treat-ment planning. Am J Orthod 53:262�284, 1967
4. Burstone J: Integumental contour and extension pat-terns. Am J Orthod 29:93�104, 1959
5. Converse JM, Horowitz SL, Wood-Smith D: Defor-mities of the jaws In: Converse JM (ed) Reconstructiveplastic surgery. 2nd ed. WB Saunders: Philadelphia, pp1386�1456, 1977
6. Converse JM, Wood-Smith D: Horizontal osteotomyof the mandible. Plast Reconstr Surg 34:464�471, 1964
7. Driemel O, Kloss F, Roth B, Wurzler KK, Pistner H:Genioplasty alone and in combination: Long-term re-sults with emphasis on sensitivity and photoanalysis.Mund Kiefer Gesichtschir 8:289�295, 2004
8. Fitzpatrick BN: Genioplasty with reference to resorp-tion and the hinge sliding osteotomy. Int J Oral Surg3:247�251, 1974
9. Hoenig JF: Asthetische Chirurgie. Steinkopff Verlag:Darmstadt, pp 134�137, 2000
10. Hoenig JF: Maxillomandibulare Umstellungsosteotom-ien. Steinkopff Verlag: Darmstadt, pp 59�64, 2002
11. Hofer O: Operation der Prognathie und Microgenie.Dtsch Zahn Kieferheilk 9:121�133, 1942
12. Hohl TH, Epker BN: Macrogenia: A study of treat-ment results, with surgical recommendations. Oral SurgOral Med Oral Pathol 41:545�567, 1976
13. Luhr HG: Significance of the chin for the aestheticsof the face. Fortschr Kiefer Gesichtschir 34:23�27,1989
14. McDonnell J, McNeil W, West R: Advancement gen-ioplasty: A retrospective cephalometric analysis of
osseous and soft tissue changes. J Oral Surg35:640�647, 1977
15. Neuner O: Correction of mandibular deformities. OralSurg Oral Med Oral Pathol 36:779�789, 1973
16. Obwegeser H, Trauner R, Obwegeser H: The surgicalcorrection of mandibular prognathism and retrogna-thia with consideration of genioplasty: I. Surgicalprocedures to correct mandibular prognathism andreshaping of the chin. Oral Surg Oral Med Oral Pathol10:677�689, 1957
17. Rabey GP: Current principles of morphanalysis andtheir implications in oral surgical practice. Br J OralSurg 15:97�109, 1977
18. Rosen HM: Aesthetic guidelines in genioplasty: Therole of facial disproportion. Plast Reconstr Surg95:463�469, discussion 470�472, 1995
19. Schendel SA: Genioplasty: A physiological approach.Ann Plast Surg 14:506�514, 1985
20. Shaughnessy S, Mobarak KA, Hogevold HE, EspelandL: Long-term skeletal and soft tissue responses afteradvancement genioplasty. Am J Orthod DentofacialOrthop 130:8�17, 2006
21. Spear SL, Mausner ME, Kawamoto HK Jr: Slidinggenioplasty as a local anesthetic outpatient procedure:A prospective two-center trial. Plast Reconstr Surg80:55�67, 1987
22. Stanton DC: Genioplasty. Facial Plast Surg 19:75�86,2003
23. Trauner R, Obwegeser H: The surgical correction ofmandibular prognathism and retrognathia with con-sideration of genioplasty: II. Operating methods formicrogenia and distoclusion. Oral Surg Oral Med OralPathol 10:899�909, 1957
24. Wolfe SA, Rivas-Torres MT, Marshall D: The geni-oplasty and beyond: An end-game strategy forthe multiply operated chin. Plast Reconstr Surg117:1435�1446, 2006
25. Gonzalez-Ulloa, Stevens: The role of chin correction inPlastic and Reconstr Surg 41:477�486, 1968
J. F. Hoenig 391