skin integrity in the older person - care inspectorate...
TRANSCRIPT
Workbook to record your training and personal development in assessment and management of the older skin
SKIN INTEGRITYFOCUS
Skin integrity in the older personassessment and management to optimise skin health
SKIN INTEGRITYFOCUS
Published November 2015
© Skin Integrity Focus 2015
Authors: Janice Bianchi MSc, BSc, RGN, RMN, PGCE Barbara Page MBE, RGN BN, DipN, ENB25 Sheila Robertson RGN
Contact: [email protected] [email protected]
The views expressed in this publication represent those of Skin Integrity Focus.
Skin integrity in the older person: assessment and management to optimise skin health 1
Contents
Introduction 2
Section 1: Skin changes in the older person 4
Section 2: Possible consequences of skin changes in the older person 8
Section 3: Skin Tears 12
Section 4: Pressure Ulcers 16
Section 5: Moisture Lesions 20
Section 6: Sun damage 22
Section 7: Keeping the skin in optimal condition with emollient therapy 24
Section 8: Common skin conditions seen in the older person 28
Assessment: Multiple choice questions 30
Assessment: Multiple choice answers 32
Statement of completion 34
Further reading 35
Acknowledgements 36
2 Skin integrity in the older person: assessment and management to optimise skin health
Introduction
The skin is the largest organ of the body and the most visible. It is a complex structure with the unique capacity to renew itself. The structure of the skin allows it to carry out its functions to maximum effect by providing an effective barrier. It is the barrier which holds us together “keeps the outside out and the inside in”. To keep healthy the skin must be intact i.e. its barrier function must not be compromised. In older people, the barrier becomes less effective. This impacts on the integrity of the skin, resulting in physical changes and numerous possible assaults such as wounds and sun damage.
Skin changes can also have a negative impact on the person’s quality of life. Changes in the skin’s appearance can profoundly impact on psychosocial well-being. We all make judgements about others by looking at their skin and as such the skin is a major organ for communication. Additionally, damage to the skin’s integrity can lead to debilitating wounds or sun damage, which can result in social isolation.
This workbook has been developed to enhance your knowledge and understanding of the older person’s skin.
The workbook is divided into Sections:Sections 1 & 2 examines changes in the skin in older people and possible consequences of these changes. Sections 3-6 gives information on best practice in relation to prevention and management of breaches in the skin’s integrity. Section 7 advises on treatments to keep the skin in optimum health. Section 8 explores common skin conditions in the older person.
Finally the effect age related skin changes have on an individual’s quality of life should not be underestimated. Potential quality of life issues are discussed throughout the workbook.
Skin integrity in the older person: assessment and management to optimise skin health 3
Target audienceThis workbook is suitable for any practitioner or carer working in health and social care. Before completing the workbook it is recommended that you attend the Skin integrity in the older person workshop. As you go through the activities in the workbook, you may wish to revisit the presentation. You can do this by going to the Scottish Dermatological Nursing Society (SDNS) website www.sdns.co.uk.
Completing the workbook The purpose of this workbook is to support your learning around maintaining skin integrity in the older person. It is a resource where you and your line manager/mentor can assess your current level of knowledge of skin and agree with your line manager/mentor your developmental needs. There are learning activities within the workbook where you can reflect on current practice and compare it to the new recommendations for practice. These reflective activities are for your own record and will not be assessed.
On completion of the workbook there are 10 multiple choice questions to demonstrate you have achieved the learning outcomes. These questions will be assessed by your line manager/mentor.
Once you have successfully completed the learning activities and assessment then your line manager/mentor will review your assessment answers and sign your workbook as completed, using the Statement of completion on page 34 to record your achievement and your development needs. You can use the Statement of completion to evidence achievement of the learning outcomes.
There is a further reading section on page 35. This includes details on where to find relevant best practice statements.
NHS staff can scan and upload a copy into e-KSF or in your own evidence of learning folder. Non NHS staff can record in their practice training and learning record or in your own evidence of learning folder. Registered nurses can use their learning towards NMC revalidation by completing a reflective account. The reflective account template is available from www.nmc.org.uk. On completion of the workbook you will have achieved 4 hours of learning.
Learning outcomes
By the end of this workbook you will be able to:• List the main layers and describe the key functions of the skin.• Demonstrate an understanding of age related skin changes.• Demonstrate an understanding of key principles in relation to prevention of skin damage including: skin tears;
pressure ulcers; moisture lesions and sun damage.• Identify how emollients help keep the skin in optimal condition.• Identify the key components of complete emollient therapy.• Recognise how changes in the skin can affect the individuals quality of life.
Your details
Name: .....................................................................................Job Title: ..............................................................................
Line manager/mentor: ..........................................................................................................................................................
Organisation: ........................................................................................................................................................................
Department: ..........................................................................................................................................................................
Date workbook commenced: .................................................
Date workbook completed: ....................................................
4 Skin integrity in the older person: assessment and management to optimise skin health
Section 1: Skin changes in the older person
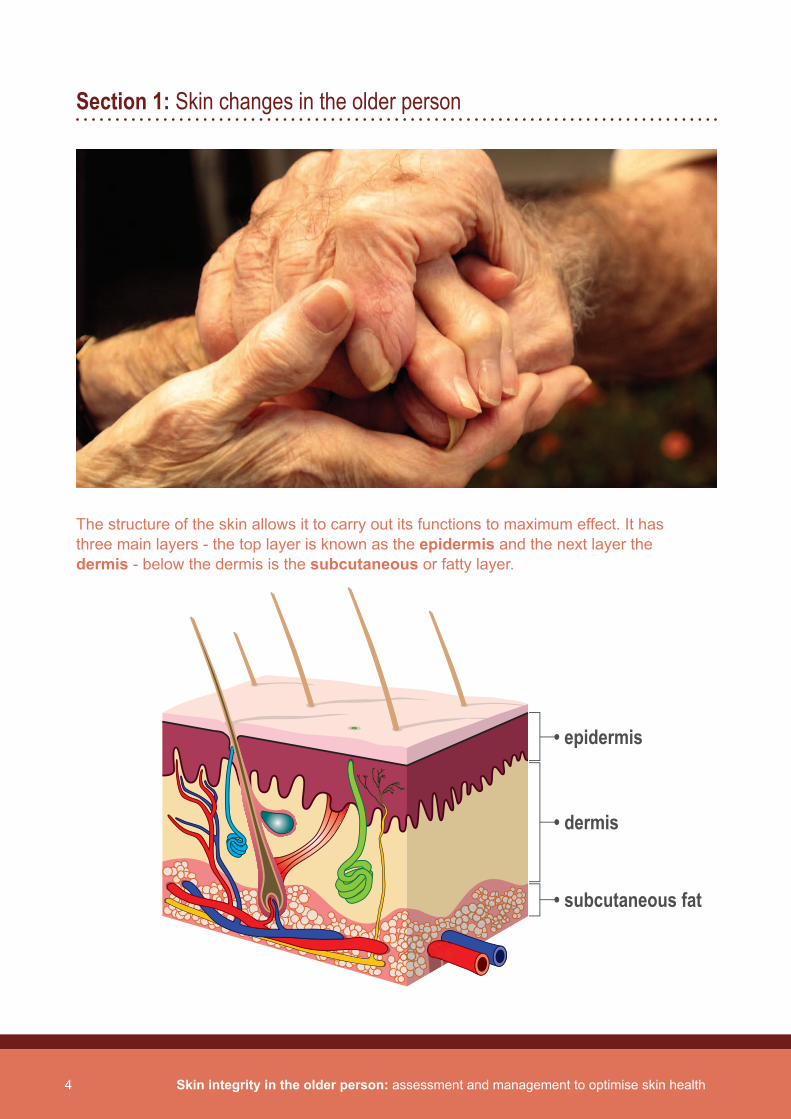
The structure of the skin allows it to carry out its functions to maximum effect. It has three main layers - the top layer is known as the epidermis and the next layer the dermis - below the dermis is the subcutaneous or fatty layer.
• epidermis
• dermis
• subcutaneous fat

Skin integrity in the older person: assessment and management to optimise skin health 5
Functions of the skinThe skin has 5 key functions. These require to be maintained to promote healthy skin and act as a protective barrier.
1. Temperature control is regulated in the skin either by dilating or constricting the blood vessels, or by increased sweating.
2. The skin enables the synthesis of vitamin D when Ultra Violet Light (sunlight) is present.3. The skin acts to protect us from harmful Ultra Violet Light and has a complex immune response.4. The skin is an important sense organ to touch, heat, pain and cold.5. The skin is an organ of display and communication.
Think of the skin as a cell factory producing plump cells, surrounded by fats and oils (sebum), which hold the skin cells together. This process of cell development usually takes around 28 days, after which the cells are lost or shed from the epidermis. The structure of the epidermis is often likened to a brick wall: the bricks being the skin cells and the oils surrounding the cells being the cement. This brick wall illustrates how the skin acts as a barrier to the external environment.
The process of ageing results in skin changes. You may notice in an older person the skin is not as smooth, dries out more quickly and is not as firm as it was. The structure and function of an older person’s skin reflects the cumulative effects of “natural” ageing and “environmental” ageing. Natural ageing is the true biological process, whereas environmental refers to the damage caused from exposure to the environment. This will be explained further in Section 2.
In ageing skin, the process of cell renewal is slowed down considerably, making it less healthy than younger skin. The water and fat levels reduce as we age. Emollient is the cornerstone to help lubricate the skin surface making it more flexible and strong. This will be explained further in Section 7.
Let’s take a moment to consider each layer of the skin, what it does and how it changes as we age.
The epidermisThe epidermis (or outer layer) contains no blood vessels and is divided into 5 layers. Cells move from the base of the epidermis up to the surface, changing shape and structure as they go. The outer layer of the epidermis plays a role in the skin’s protective function. The epidermis gets thinner as we age.
The dermisThe main function of the dermis is to provide physical support and nutrients to the epidermis. Key substances found in the dermis include collagen and elastin. Collagen is an important substance which helps give support and protection within the skin. The amount of collagen we have decreases as we age.
6 Skin integrity in the older person: assessment and management to optimise skin health
The dermis also contains nerve endings, sweat glands, hair follicles, sebaceous glands and blood vessels. The papillary dermis contains smaller blood vessels which supply oxygen, elastic fibers and nutrients to the lower epidermis. These vessels also assist in the removal of waste products from the skin into the general circulation.
As we age, the skin becomes less elastic, due to the decrease in collagen, gravity takes over resulting in sagging skin, not returning to its original shape. This can make the skin more vulnerable to tearing or shearing.
The subcutaneous layerThe subcutaneous layer provides support for the dermis and is made up largely of fatty and connective tissue. It is essential to protect the internal structures and also provides insulation. The subcutaneous layer gets thinner as we age.
Older people’s skin may also bruise more easily and be susceptible to traumatic wounds such as skin tears, as the support structure deteriorates. See Section 3.
Quality of lifeIt is important to recognise that the older person’s quality of life can be significantly affected by age related skin changes. We must not underestimate the importance of the skin as the organ through which we interact with the outside world. Our psychological and social wellbeing are affected by what our skin looks like and how we feel about it. Some grow old graciously and for others the ageing process can be viewed negatively.
Key Points
• Skin changes as we age are inevitable.• An understanding of the age related changes that are affecting the skin will have an impact on how we recognise
problems and provide practical solutions to the everyday skin care changes experienced by the older population.

Skin integrity in the older person: assessment and management to optimise skin health 7

8 Skin integrity in the older person: assessment and management to optimise skin health
Section 2: Possible consequences of skin changes in the older person
Assessing the skin is an ongoing process which requires great sensitivity. It is helpful to give careful consideration to the environment. Is the room warm enough, are unwanted interruptions guarded against? When you carry out the assessment be sure to check the entire skin - this may be most appropriately carried out when helping the individual to bathe.
The table below describes changes you may see in elderly skin and the consequences of these changes.
Changes in the skin Consequence
Epidermal turnover slows Thinner skin
Less effective barrier function More prone to infection and dryness
Less flexible and softer collagen More prone to wrinkles and shearing
Less evenly distributed melanin More prone to sun damage
Fewer sweat glands Less effective temperature control
Less sebum production Increased skin dryness
Skin integrity in the older person: assessment and management to optimise skin health 9
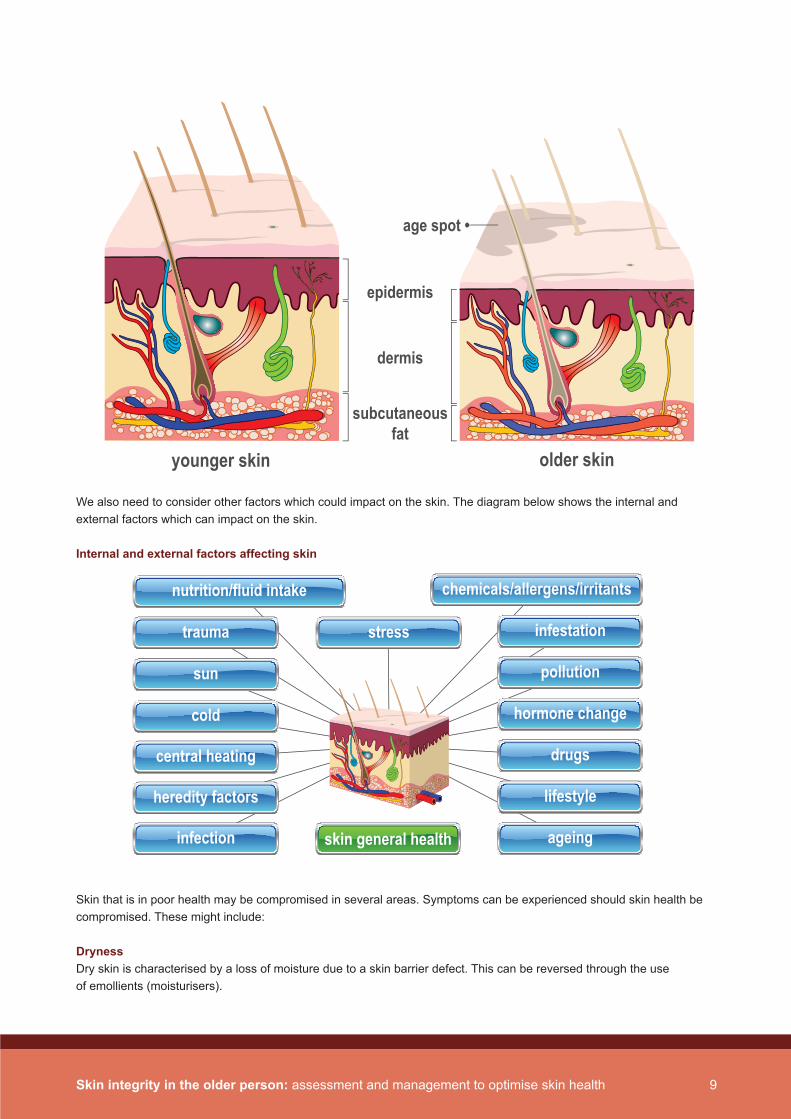
We also need to consider other factors which could impact on the skin. The diagram below shows the internal and external factors which can impact on the skin.
Internal and external factors affecting skin
Skin that is in poor health may be compromised in several areas. Symptoms can be experienced should skin health be compromised. These might include:
DrynessDry skin is characterised by a loss of moisture due to a skin barrier defect. This can be reversed through the use of emollients (moisturisers).
age spot •
younger skin older skin
epidermis
dermis
subcutaneousfat
skin general health
stress
drugs
ageing
chemicals/allergens/irritants
lifestyle
hormone change
pollution
infestation
central heating
cold
heredity factors
infection
sun
trauma
nutrition/fluid intake

10 Skin integrity in the older person: assessment and management to optimise skin health
Itch (also known as pruritus) Itching is a symptom, not a diagnosis or a disease, but can plague older people. As the skin ages and becomes drier it may well itch for no particular or obvious reason. Itch is a sensation which triggers the urge to scratch, is unpleasant and poses a threat to skin integrity.
It is useful to understand the possible cause of itch which, in the elderly, is not always easy to identify, for instance when there is no evidence of a rash.
Itching may be triggered by:• Environmental causes - heat, sweating, clothing.• Physical/psychological causes - fatigue or emotional distress. • Medical conditions - renal failure, iron deficiency or diabetes. • Infestation - If there is a sudden onset of itching, investigate for scabies, especially in a care setting.
Management of itch should include prevention, identification and treatment of the underlying problem wherever possible.
Learning activity 1
Think about a time when you have had itchy skin such as an insect bite or a nettle rash. Describe how your skin felt at that time and how you would feel if this lasted for weeks or months.
Skin integrity in the older person: assessment and management to optimise skin health 11
CrackingCracked skin is a classic symptom of dry skin but it can also occur in response to scratches and trauma. As the skin dries it can become rough and flaky, with small tears that can lead to deeper cracks.
ScalingScaling skin is the loss of the outer layer of the epidermis in large, scale-like flakes. The skin appears dry and cracked, although skin dryness is not always to blame.
InfectionMost skin infections are relatively minor and only affect the skin or underlying tissue, some may result in deeper tissue involvement (cellulitis). Infection may be caused by bacterial, fungal or viral organisms.
PainSkin is very sensitive to touch due to the high proportion of nerve endings situated in the skin. Depending on the cause, skin pain may occur in a specific location, or in a number of locations. This may be accompanied by redness, itching or swelling. Any painful symptom should be investigated.
Quality of life The consequences of skin changes in the older person can have a significant effect on their quality of life. The changes can lead to, amongst other things, sleep deprivation and fatigue which can also result in low mood.
Key Points
• Internal and external factors contribute to age related skin change.• Ongoing assessment and management of the factors will optimise skin health.

12 Skin integrity in the older person: assessment and management to optimise skin health
Section 3: Skin Tears
Definition: A wound caused by shear, friction and/or blunt force resulting in separation of skin layers. A skin tear can be partial-thickness (separation of the epidermis from the dermis) or full thickness separation of both the epidermis and dermis from underlying structures.
Skin tears are an increasing problem for all healthcare practitioners. If appropriate treatment is not given, these injuries may become chronic wounds, causing unnecessary pain and distress. This type of injury usually occurs in very young infants and in the older person due to skin fragility. As our population changes and the number of older people increases, whether we are caring for that person in their own home, a care home or hospital, we need to be aware of how to prevent skin tears. If a skin tear does happen, we need to understand how to assess and manage appropriately.
Age related skin changes associated with skin tearsThinning of the layers of the skin was described in Section 1. These changes will make the skin more vulnerable to damage such as skin tears. Additionally, other factors may also impact on fragility of the skin.
These would include:• Immunological status.• Malnutrition.• Poor circulation.• Oxygen intake.
Prevention of skin tearsPrevention of skin tears starts with early identification and assessment of individuals who are at risk. Based on available evidence the consensus statement of an international panel suggests the following strategies should be part of prevention.

Skin integrity in the older person: assessment and management to optimise skin health 13
These are: • Risk assessment on admission to healthcare service or if the individual’s condition changes and document findings in
care plan.• Have individuals at risk wear long sleeves, long trousers or knee high socks.• Provide shin guards/leg protectors for those individuals who experience repeat skin tears on shins.• Ensure safe patient handling techniques and equipment/environment.• Educate all staff and care givers on safe patient handling technique.• Involve individuals and families in prevention strategies.• Ensure adequate nutrition and hydration and if necessary consult a dietician.• Keep skin well hydrated with emollient (moisturiser) therapy.• Encourage the patient or their carers to apply emollient.• Protect individuals at high risk of trauma during routine care from self-injury.
Practical advice on maintaining a safe environment to minimise the risk of skin tears:• Ensure adequate lighting and position small furniture (night tables, chairs) to avoid bumps or knocks. Remove rugs
and excessive furniture.• Upholster or pad sharp borders of furniture or bed surroundings with padding and soft material.• Use appropriate aids when transferring patients and adopt good moving and handling techniques according to
local policy.• Never use bed sheets to move patients as this can contribute to damage by causing a dragging effect on the skin.
Always use lifting device or slide sheet.• Where possible reduce or eliminate pressure, shear and friction using pressure relieving devices and positioning
techniques.• Continence management if relevant.
Include this practical advice in the patient care plan where relevant
Assessing a skin tearThe most important aspect of assessment and management is to minimise further trauma and preserve viable tissue.It is important to classify the type of skin tear, as this will determine the severity and aid in planning appropriate treatment. The STAR Skin Tear Classification System (Carville et al, 2007) is a validated classification tool. It is important for the practitioner to be aware of the classification system which is being used in their clinical setting.
Managing a skin tear • Control bleeding.• Assess the wound, skin flap or pedicle and determine the type or category of skin tear using a validated documentation
system (STAR classification system).• Cleanse the skin tear following assessment using warm saline or water to remove debris and any residual haematoma. • Depending on healthcare setting a tetanus immunoglobulin may be administered.• Approximate the skin flap by gently easing the flap back into place using dampened cotton bud or gloved finger.• If the skin flap is difficult to align, consider applying a sterile moistened non-woven swab for 5-10 minutes first to
rehydrate the skin flap.• Moist wound healing should be encouraged by the application of appropriate dressings. You will find information on
dressing options in your local wound care formulary.• Avoid the use of adhesive strips.• If possible dressing should be left in place for several days to avoid disturbing the flap.• If an opaque dressing is used mark an arrow to indicate the preferred direction of removal and document in care plan.• Dressings should be held in place with a tubular retention bandage. • Pain assessment should be carried out and appropriate analgesia administered.• Complete a wound assessment form and document in care plan.• Complete accident/incident documentation and discuss with family or next of kin if relevant.

14 Skin integrity in the older person: assessment and management to optimise skin health
When to refer to specialistsIf the skin tear is extensive, or with uncontrolled bleeding or haematoma, consider emergency department referral. If the skin tear is on the lower leg and fails to progress, consider early referral to local leg ulcer service or tissue viability services.
Learning activity 2
From the information you have read in this section how could this change the prevention and management of skin tears in your workplace?
Ongoing management At each dressing change the dressing should be gently removed in the direction indicated by the arrow. If it does not remove easily, consider the use of saline soaks or silicone-based adhesive removers. The skin tear may be friable so care should be taken to prevent disturbing it. The wound should be observed for signs of infection and any changes in colour of the skin flap, which may indicate that it is becoming non-viable.
Quality of lifeAn individual’s quality of life may be affected by any of the following: Pain, infection, loss of function and reduced mobility. The skin tear can become a chronic wound producing odour and exudate.
Skin integrity in the older person: assessment and management to optimise skin health 15
Key Points
• Skin tears are common wounds, particularly at the extremes of age. • We should be aware of the risk factors associated with skin tears and minimise wherever possible. • When an individual develops a skin tear, the use of a skin tear classification system will aid our decision making,
and ensure we are all using the same language to describe wounds. • Treatment regimens should be structured on best available evidence.

16 Skin integrity in the older person: assessment and management to optimise skin health
Section 4: Pressure Ulcers
Definition: A pressure ulcer is an area of skin damage caused by pressure or shear, or a combination of both.
Most pressure ulcers are preventable, and appropriate clinical care can help to prevent their occurrence. Understanding how pressure ulcers develop provides us with the know-how to avoid them forming in the first place.
Prevention of pressure ulcersSome people may be more vulnerable to developing pressure ulcers than others. When you are caring for an individual, it is important to be aware of the factors that might cause them to become vulnerable to pressure damage. These factors may be internal, innate (intrinsic) or external, environmental (extrinsic). Internal factors include the person’s age, health status, mobility, body weight. External factors may include pressure, shear or moisture. Often the person will have several of these factors which impact on skin integrity. Some important steps can be taken to reduce the risk to individuals who are vulnerable to skin damage.
These include:• Inspecting the skin regularly.• Making sure all surfaces, such as the bed and chair, are appropriate to the individual.• Assisting the individual to reposition on a regular basis.• Using moving and handling aids to minimise shear and friction injury.
A structured formal risk assessment tool should be used in all health and social care settings. Although there are several pressure ulcer risk assessment tools available, the most commonly used are the Braden Risk Assessment Tool and the Waterlow Risk Assessment Tool.
These tools were developed to enable early detection of individuals at risk of developing pressure ulcers. Strategies can then be put in place to reduce risk, such as repositioning more frequently and, in some cases, the use of pressure-redistributing devices.
Skin integrity in the older person: assessment and management to optimise skin health 17
When should risk assessment be carried out?A registered nurse or a health care worker normally carries out pressure ulcer risk assessment. The Healthcare Improvement Scotland best practice statement for Scotland states that:
“All patients should be assessed using both formal and informal risk assessment to ensure that the correct preventative strategies are initiated and maintained.
If a patient is admitted to hospital the risk assessment should be carried out within six hours of admission.
In other health care settings this may not be possible but the risk assessment should be carried out as soon as is reasonably possible.”
Reassessment should be carried out regularly, but the frequency depends on individual needs. Informal reassessment should take place every time you care for the at risk person. This will help determine the frequency of structured formal reassessment.
Reassessment should be carried out if there is any significant change in the individual’s condition.
Skin inspection helps us to identify any early changes in the skin that may lead to a pressure ulcer.
We are looking for areas of redness (erythema) when we inspect the skin. When you see such an area, compare it to the skin nearby. If nearby skin appears normal in colour, the area of redness may be an early warning sign of pressure damage. You should also conduct a blanching test, which involves applying light pressure with your finger to the area. If the area of skin turns white on pressure then quickly becomes red again after the pressure is removed, this indicates that the microcirculation is intact. If the skin remains red on finger pressure, it indicates damage to the microcirculation. It is extremely important to identify, report and record early changes in the skin. If we intervene quickly and appropriately to stop further damage, we can prevent tissue loss.
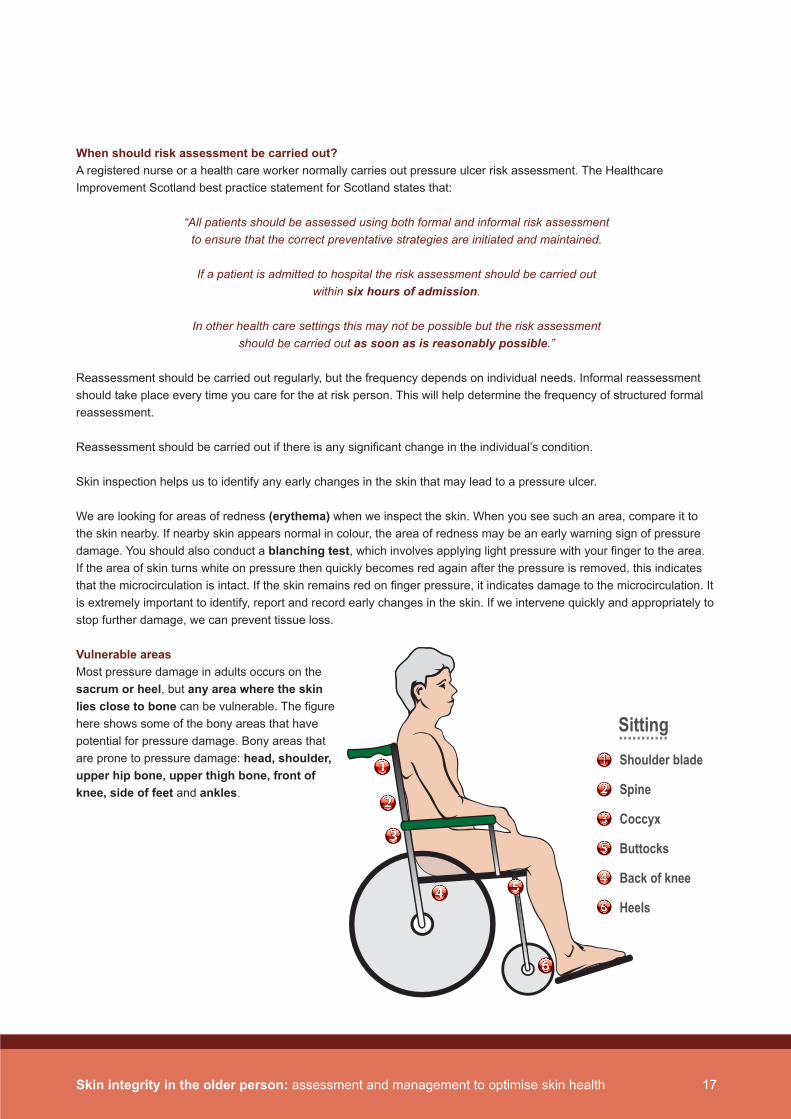
Vulnerable areas Most pressure damage in adults occurs on the sacrum or heel, but any area where the skin lies close to bone can be vulnerable. The figure here shows some of the bony areas that have potential for pressure damage. Bony areas that are prone to pressure damage: head, shoulder, upper hip bone, upper thigh bone, front of knee, side of feet and ankles.
Shoulder blade
Spine
Coccyx
Buttocks
Back of knee
Heels
Sitting...........
18 Skin integrity in the older person: assessment and management to optimise skin health
Management of pressure ulcersIf a pressure ulcer occurs, we aim to heal the wound and prevent further damage. The pressure ulcer should be graded. The European Pressure Ulcer Advisory Panel (EPUAP) have devised a grading tool. You may have a locally adapted version of the grading tool. Contact your tissue viability services for advice.
Strategies to reduce further damage are similar to those used to reduce risk, such as repositioning more frequently and, in some cases, the use of pressure-redistributing devices.
Appropriate dressings should be used. The type of dressing will depend on several factors.
These include:• Position of the wound.• Size of the wound.• Tissue type in the wound bed.• Amount of exudates.• Condition of the surrounding skin.• Known sensitivity or allergy to a dressing.
There are many available dressings and your local wound formulary will help you determine which is best for each individual and their wound.

Skin integrity in the older person: assessment and management to optimise skin health 19
Learning activity 3
From the information you have read in this section how could this change the prevention and management of pressure ulcers in your workplace?
Quality of lifePressure ulcers can be devastating for the individual, causing pain and distress and reducing the person’s ability to get on with their day-to-day lives. They may also require long and arduous courses of treatment and make the individual vulnerable to potentially life-threatening infections.
Key Points
• Pressure ulcers are wounds which can have serious consequences and are often seen at the extremes of age.• We should be aware of the risk factors associated with pressure ulcers and minimise risk wherever possible by
applying prevention strategies.• If an individual develops a pressure ulcer, follow guidelines on management of pressure ulcers.• Treatment regimens should be structured on best available evidence.

20 Skin integrity in the older person: assessment and management to optimise skin health
Section 5: Moisture Lesions
Definition: Moisture Lesions and incontinence dermatitis are both terms used to describe areas of skin damage caused by urinary and/or faecal incontinence.
Moisture lesions are often associated with increased age and decreased mobility and the presence of incontinence. In addition to these factors, the individual’s overall health, cognitive impairment and concurrent medications are also involved. Once urine and faeces come into contact with the skin, fluid containing bacteria can penetrate the skin, potentially leading to infection. The pattern of skin damage is reflective of the flow of urine and faeces around the perineal area, the effect on the skin often appears like a superficial burn. Ongoing assessment will highlight early changes in the skin or deterioration.
A continence advisor should be part of the interdisciplinary team.
Prevention and management of moisture lesions• Prevention begins with regular inspection of the skin of individuals with incontinence. • Skin inspection should include all the areas affected by urine and faeces, the perineal area, anal cleft, between the
thighs, skin folds and the buttocks.• Using pH balanced skin cleansers is another important step in managing the skin of the incontinent individual. Avoid
the use of soap and water. • Skin should be cleansed after each episode of loose stool, using the non-rinse skin cleansers and soft wipes. This
will help prevent excessive friction on the skin. • Barrier creams should also be used to help form a protective layer on the skin, between episodes of incontinence. It
is important to avoid build-up of these products on the skin, therefore the area should be cleansed at each episode of incontinence.
• Liquid barrier films are available containing a solvent which dries on the skin - some cannot be used on broken skin.• The use of appropriate incontinence pads is an important part of caring for individuals with moisture related skin
damage. High quality, super-absorbent, breathable pads should be used. These minimise moisture contact with the skin, locking away incontinence.
Skin integrity in the older person: assessment and management to optimise skin health 21
Learning activity 4
From the information you have read in this section how could this change the prevention and management of moisture lesions in your workplace?
Quality of LifeSkin damage is often associated with significant pain and discomfort caused by the changes in the affected area.
Key Points
• Moisture lesions occur as a result of incontinence.• They can be extremely painful.• We should be aware of the risk factors associated with moisture lesions and minimise risk wherever possible
by applying prevention strategies.• If an individual develops a moisture lesion, follow guidelines on management of moisture lesions.• Treatment regimens should be structured on best available evidence.

22 Skin integrity in the older person: assessment and management to optimise skin health
Section 6: Sun damage
Definition: Older people who have had a lifetime of exposure to sun may have damaged skin known as photodamage.
It is important to remember the benefits to health and wellbeing of safe sun exposure. The reaction of sunlight on the skin enables the synthesis of vitamin D. Limited exposure to sunlight can also be beneficial to wellbeing and help lift mood.
We do however need to be aware of early changes to the skin which may be a result of sun damage. Before discussing suspicious lesions, it is worth noting that older people have a tendency to develop numerous lumps and bumps which are completely harmless – a skin tag is a good example of this.
However, lifetime sun exposure and the fact that older skin is less able to protect from harmful sun rays, makes them more at risk of developing benign or malignant skin cancer. The amount of photodamage will be influenced by factors such as the person’s occupation, outdoor pursuits or geographic location (such as living in countries which have sunny climates)
Skin cancers are most commonly seen in sun exposed sites so vigilance is important when checking these areas. Areas include bald scalps, tops of ears, bridge of nose, temples, backs of hands and forearms. It is worth checking the back of men if they have been an outdoor worker.
Actinic Keratoses (AK)Presents most commonly on backs of hands, bald scalp and temples as a persistent scaly patch.
Basal Cell Carcinoma (BCC)This is the commonest type of skin cancer. A slow growing flesh-coloured lump may develop into a sore that will not heal. It is often found on the forehead or side of the nose. On the trunk it often takes the form of a slowly enlarging red dry patch.
Skin integrity in the older person: assessment and management to optimise skin health 23
Bowens DiseasePresents as multiple red, slowly growing, crusted, scaly patches most often on the lower legs.
Squamous Cell Carcinoma (SCC)May grow rapidly, forming a tender crusting lump. They are also found on exposed areas, especially the ears, lips, hands and lower legs.
Malignant Melanoma (MM) This is the least common skin cancer but the most dangerous. This can occur in young adults as well as the elderly. It takes the form of a changing mole with an unusual appearance. A useful rule to follow when checking for suspicious lesions is the ABCD guide from the British Association of Dermatologists. It helps to distinguish between the innocent mole and a possible Malignant Melanoma.
ABCD Guide:A - ASYMMETRY of an MM
the two halves of the area may differ in their shapeB - BORDER of an MM
the outside edges of the area may be irregular or blurred, and sometimes show notches or look raggedC - COLOUR of an MM
may be uneven and patchy: different shades of black, brown and pink may be seenD - DIAMETER of an MM
most, but not all, melanomas are at least 6mm in diameter
A sudden change in any mole should be checked by a GP as soon as possible.
Quality of LifeIf an individual develops skin changes/lesions they may be extremely anxious. Early referral to the GP and reassurance is important. It is important for wellbeing that individuals are able to be out in the sun, therefore it is the responsibility of the carer to facilitate safe sun exposure.
Key Points
• The skin’s ability to protect itself from Ultra Violet Light reduces as it gets older. • If an individual has any abnormal changes to the skin they should be referred to their GP for further assessment.

24 Skin integrity in the older person: assessment and management to optimise skin health
Section 7: Keeping skin in optimal condition with emollient therapy
Emollient is the medical term for a moisturiser. Emollients are oils that spread easily on the skin, providing partial occlusion to hydrate and improve the outer layer of the skin.
Emollients are the cornerstone to maintaining skin integrity in the older person’s skin. This is best achieved by the use of complete emollient therapy. This takes the form of a three stage approach:
• Emollient soap substitute.• Emollient lotion, cream or ointment.• Emollient bath/shower product.*
* Due to the oily nature of some of these products a risk assessment should be undertaken to avoid slipping or falls and only use bath/shower products if it is safe to do so. Talcum powder should be avoided on the older person’s skin.
The objective of complete emollient therapy is to correct some of the factors contributing to dry skin, by restoring the skin barrier and reducing the likelihood of further damage. Emollient products can be enhanced with additional ingredients such as humectants which attract and hold water in the outer layer of the skin. It is important to recognise that emollients are not all the same and that advice should be guided by clinical need and informed individual choice.
Using emollients is a key way of helping to maintain healthy skin. They help to promote the barrier function of the skin, lubricate, soften and make the skin less likely to be itchy and scaly. This section looks at how health care workers can help individuals to choose and use emollients in all aspects of their personal care.
Complete emollient therapy is a useful way of thinking how emollients can be incorporated into all elements of the skin care process. Emollients work in two ways:
Skin integrity in the older person: assessment and management to optimise skin health 25
Occlusive emollients work by:• Sealing in the moisture so that water loss is prevented from the stratum corneum.
Humectant emollients work by:• Drawing and retaining water from below into the stratum corneum increasing the amount of moisture there.
Emollient bath/shower products and soap substitutes The purpose of washing/bathing is twofold. It maintains skin hygiene and also ensures a feeling of wellbeing for the individual. Washing the skin is something carers spend a lot of time doing. This provides an opportunity to assess and advise on best practice. It would be appropriate to mention the importance of allowing individuals to have choice about when they wash, how they wash and with what products. The information given here is so that individuals can be informed of ways of looking after their own skin most effectively.
As already mentioned the skin is a complex environment with a unique balance of natural organisms and an acidic pH. Washing using soap or bubble bath will alter the skin pH and can disturb the balance of natural organisms, which may result in skin damage or making the skin more vulnerable to fungal or bacterial infection. These products may also strip the skin of natural oils (sebum) which help maintain flexibility and limit dryness.
To maintain skin health, there are various emollient wash products such as bath additives, shower products and soap substitutes. The advantage these products have is that they do not strip the skin of natural oils. Washing should always be gentle followed by a thorough rinsing and meticulous drying. Areas that are left damp are prone to breaking down and attracting fungal infections. Particular attention should be paid to skin folds and finger/toe webs. Whilst thorough drying is important, it should be carried out gently, rather than vigorous rubbing.
Emollient gel, lotion, cream or ointment Emollients are put into categories: • Gels have the highest water content and are best used on hairy areas.• Lotions have a low oil content and are cosmetically acceptable.• Creams have a moderate oil content, are effective and also cosmetically acceptable.• Ointments are mostly grease and consequently very effective but not always popular.
Choosing an emollient is a very personal selection and what will suit one person will not suit another. There is no point insisting that an individual uses what you know will work, if they dislike it and avoid applying it. It is true that the least effective moisturiser is the one that stays in the pot.
Application of emollientEmollients should be applied in a downwards direction following the line of hair growth. Vigorous rubbing with an emollient can cause irritation and inflammation. It is best to apply emollient after a warm bath or shower when the skin is most receptive, but they can be applied at any time. Should the individual be having another treatment applied to their skin, e.g. a steroid, it is best applied after the emollient. It is important that the emollient has been allowed to absorb into the skin. This can take around 20 minutes, depending on how dry the skin is and how greasy the moisturiser.
26 Skin integrity in the older person: assessment and management to optimise skin health
Learning activity 5
From the information you have read in this section how could this change the choice and application of emollient in your workplace?
Key Points
• Emollient therapy is the cornerstone to maintaining skin integrity and patient/client choice is essential.• Knowledge on different types of emollient and how they work with correct application will help restore and maintain
the skin’s integrity and reduce the likelihood of further damage.

Skin integrity in the older person: assessment and management to optimise skin health 27
28 Skin integrity in the older person: assessment and management to optimise skin health
Section 8: Common skin conditions seen in the older person
In addition to the skin changes in the older person we have discussed in this workbook, there are a number of skin conditions we need to be aware of.
The following are types of eczema which are found almost exclusively in the older person. Emollient therapy will help reduce dryness in the skin, but other treatments may be required to treat the skin condition. It is important to identify if the individual has a skin condition and refer to the GP for further assessment.
Asteototic eczemaDry and red skin, with cracking due to the loss of the skin’s natural oils giving a crazy paving appearance.
Venous DermatitisAlso known as gravitational or stasis eczema. This is associated with poor venous circulation of the lower limbs.
Seborrhoeic EczemaRed and scaling where the sebaceous glands are most active. Immunocompromised and nutrition deficient individuals are more at risk.
Lichen SimplexAlso known as neurodermatitis. It can be associated with stress and habit forming behaviour such as the itch scratch cycle. This results in thickened (lichenified) skin following persistent rubbing/scratching of areas such as the neck or lower limbs.
Discoid EczemaPresents as coin shaped lesions. The onset is usually sudden and may display as one well defined patch, or many affecting the trunk and extensor surfaces (e.g. elbows or knees ).
Irritant Contact DermatitisCommonly seen in incontinence See Section 4.

Skin integrity in the older person: assessment and management to optimise skin health 29
You have now completed the workbook.
Please now complete the workbook assessment.

30 Skin integrity in the older person: assessment and management to optimise skin health
Assessment: Multiple choice questions
Choose the correct response to all the questions below by circling the one correct answer. Read each question, instructions and all possible answers carefully before you choose the correct answer.
There are 10 questions.
1. Starting with the top layer and in the correct order the main layers of the skin are:
A. Epidermis and dermis
B. Dermis and subcutaneous layer
C. Epidermis, dermis, subcutaneous layer
D. Dermis, epidermis, subcutaneous layer 2. The skin has key functions. Which of the following is not a function of the skin?
A. Protection from harmful Ultra Violet Light
B. Temperature control
C. Metabolism of fat
D. A barrier to harmful bacteria
3. Which of the following can happen to the skin as we get older?
A. Skin gets more oily
B. Skin gets thicker
C. Skin gets tougher
D. Skin gets drier 4. If individuals experience repeat skin tears on shins:
A. Make sure legs are shaved to decrease the risk of infection
B. Provide limb protectors
C. Advise to wear short socks
D. Apply moisturiser once a day
5. Which of the following practical advice can be given to minimise the risk for individuals who are vulnerable to developing pressure ulcers?
A. Use bed sheets rather than anything else to move patients
B. Advise the individual not to change position too much
C. Only inspect the skin on the sacral area
D. Use moving and handling aids to minimise shear injury
Skin integrity in the older person: assessment and management to optimise skin health 31
6. Which of the following is not part of the guidance on the prevention of moisture lesions?
A. Regular inspection of the skin
B. Use a pH balanced skin cleanser after episodes of incontinence
C. Avoid the use of incontinence pads
D. Apply a barrier cream to affected areas
7. Photodamage will be determined by:
A. The person’s occupation
B. Outdoor pursuits
C. Geographical location
D. All of the above
8. Complete emollient therapy consists of:
A. Soap; lotion, cream or ointment; bath or shower product
B. Soap substitute; lotion, cream or ointment; bath or shower product
C. Lotion, cream or ointment;
D. Soap; lotion, cream or ointment;
9. Emollients help keep the skin in optimal condition by:
A. Allowing water to evaporate from the stratum corneum
B. Hydrating the outer layer of the skin and restoring the skin barrier
C. Allowing the skin to dry out
D. Penetrating deep into the subcutaneous layer
10. Age related skin changes and skin damage can affect the individuals quality of life by:
A. Causing stress and distress
B. Causing pain
C. Causing sleep deprivation and fatigue
D. Any of the above
32 Skin integrity in the older person: assessment and management to optimise skin health
Assessment: Multiple choice answers
Check your answers against the answers below. Allocate one mark for each correct answer. If your answer is incorrect, revisit the section of the workbook indicated below the correct answer.
1. Starting with the top layer and in the correct order the main layers of the skin are:
A. Epidermis and dermis
B. Dermis and subcutaneous layer
C. Epidermis, dermis, subcutaneous layer (workbook Section 1)
D. Dermis, epidermis, subcutaneous layer 2. The skin has key functions. Which of the following is not a function of the skin?
A. Protection from harmful Ultra Violet Light
B. Temperature control
C. Metabolism of fat (workbook Section 1)
D. A barrier to harmful bacteria
3. Which of the following can happen to the skin as we get older?
A. Skin gets more oily
B. Skin gets thicker
C. Skin gets tougher
D. Skin gets drier (workbook Section 2) 4. If individuals experience repeat skin tears on shins:
A. Make sure legs are shaved to decrease the risk of infection
B. Provide limb protectors (workbook Section 3)
C. Advise to wear short socks
D. Apply moisturiser once a day
5. Which of the following practical advice can be given to minimise the risk for individuals who are vulnerable to developing pressure ulcers?
A. Use bed sheets rather than anything else to move patients
B. Advise the individual not to change position too much
C. Only inspect the skin on the sacral area
D. Use moving and handling aids to minimise shear injury (workbook Section 4)
Skin integrity in the older person: assessment and management to optimise skin health 33
6. Which of the following is not part of the guidance on the prevention of moisture lesions?
A. Regular inspection of the skin
B. Use a pH balanced skin cleanser after episodes of incontinence
C. Avoid the use of incontinence pads (workbook Section 5)
D. Apply a barrier cream to affected areas
7. Photodamage will be determined by:
A. The person’s occupation
B. Outdoor pursuits
C. Geographical location
D. All of the above (workbook Section 6)
8. Complete emollient therapy consists of:
A. Soap; lotion, cream or ointment; bath or shower product
B. Soap substitute; lotion, cream or ointment; bath or shower product (workbook Section 7)
C. Lotion, cream or ointment;
D. Soap; lotion, cream or ointment;
9. Emollients help keep the skin in optimal condition by:
A. Allowing water to evaporate from the stratum corneum
B. Hydrating the outer layer of the skin and restoring the skin barrier (workbook Section 7)
C. Allowing the skin to dry out
D. Penetrating deep into the subcutaneous layer
10. Age related skin changes and skin damage can affect the individuals quality of life by:
A. Causing stress and distress
B. Causing pain
C. Causing sleep deprivation and fatigue
D. Any of the above (workbook Section 8)
34 Skin integrity in the older person: assessment and management to optimise skin health
Statement of completion of the Skin integrity in the older person workbook
Name of organisation: .........................................................................................................................................................
Name of person who completed the learning outcomes and 4 hours learning time: ................................................................................................................
Job title: ................................................................................................................................................................................
Ward/unit/department: ........................................................................................................................................................
Date of completion: ....................................................
Signature of line manager/mentor: ....................................................
Agreed development needs:

Skin integrity in the older person: assessment and management to optimise skin health 35
Further reading
Emollient Best Practice Guideline
www.bdng.org.uk/document/emollientbpg.pdf
Pressure Ulcer Best Practice Guideline
www.npuap.org
Skin Tears Best Practice Guideline
www.tissueviabilityscotland.org
36 Skin integrity in the older person: assessment and management to optimise skin health
Acknowledgements
The Almirall pharmaceutical company supplied an educational grant to facilitate the development of this resource.
The Scottish Dermatological Nursing Society (SDNS) have kindly agreed to host this resource on their website: www.sdns.co.uk

Skin integrity in the older person: assessment and management to optimise skin health 37

SKIN INTEGRITYFOCUS