skin antisepsis for preventing … povidone -iodine or chlorhexidine are most suitable. nice 2008...
TRANSCRIPT

SKINANTISEPSIS FOR
PREVENTING INFECTION
Rabih O. Darouiche, M.D.VA Distinguished Service Professor
Director, Center for Prostheses InfectionBaylor College of Medicine
Houston, TexasUSA

Disclosure Statement
• Received research and educational funds from CareFusion/Cardinal Health
• Co-invented antimicrobial-impregnated devices
• I will quote data published only in peer-reviewed journals

Reasons to Optimize Prevention of SSI
• Unacceptably high incidence: the 30 million annual surgical procedures in the US result in 300,000-500,000 cases of SSI
• Difficult management: may require repeated surgical interventions
• Serious medical consequences: tremendous morbidity and occasional mortality
• Soaring economic burden: annual cost of treatment in the US, >$7 billions
Perioperative Approaches for Preventing SSI
• Non-antimicrobial approaches• Normothermia• Adequate oxygenation• Tight glucose control
• Antimicrobial approaches• Systemic antibiotic prophylaxis• Nasal application of mupirocin• Skin antisepsis

Impact of Timing of Systemic Antibiotic Prophylaxis on SSI
A Prospective Randomized Trial of Nasal Mupirocin Plus Chlorhexidine Wash
Rapid identification of nasal carriage by S. aureus followed by a 5-day course of nasal mupirocin plus chlorhexidine wash:• Reduces S. aureus infection (3.4% vs. 7.7%)• Decreases S. aureus SSI by almost 60%
Bode, et al. N Engl J Med 2010;362:9-17
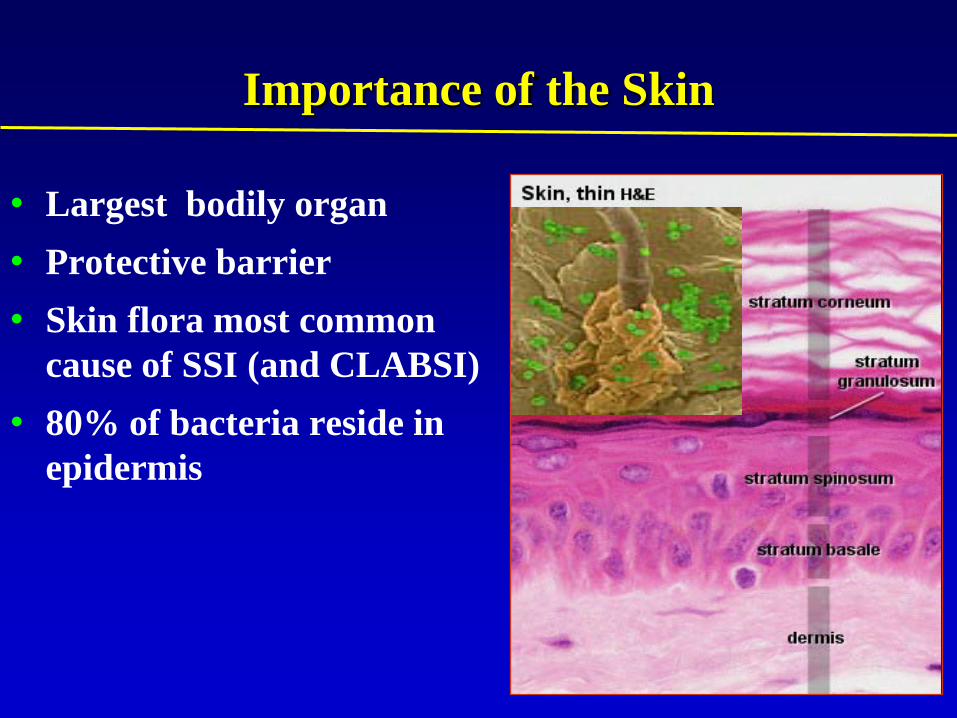
Importance of the Skin
• Largest bodily organ• Protective barrier • Skin flora most common
cause of SSI (and CLABSI)• 80% of bacteria reside in
epidermis

Factors that Support the Need for Optimal Skin Antisepsis
• Most Pathogens that cause SSI are skin flora
• At least 2/3 of cases of SSI are incisional
• Most SSI are considered preventable
• Other preventive measures reduce but do not eliminate SSI

Commonly used Preoperative Antiseptics
• Povidone-iodine (Iodophor)• Chlorhexidine gluconate• Alcohol • Combination products: >2 active agents
Comparison of Antimicrobial Activity of Antiseptic Preparations
Chlorhexidine-based preparations are better than alcohol or iodine-based products in:
• Reducing colonization of vascular catheters
• Preventing contamination of blood cultures
• Decreasing contamination of surgical tissues

Prospective Randomized Clinical Trial of 2% Chlorhexidine Gluconate in 70% IPA vs. 70% IPA for Disinfection of Skin
Prior to Peripheral Venous Cannulation
19.8
33.1
0
5
10
15
20
25
30
35
2% CHG/70% IPA 70% IPA
PV
C ti
ps c
olon
ized
(%)
91 PVC tips evaluated 79 PVC tips evaluated
P=0.05
• There was a statistically significant reduction in the number of PVC tips colonized with coagulase-negative staphylococci in the 2% CHG/70% IPA group vs. 70% IPA group
Small, et al. Infect Control Hosp Epidemiol, 2008.

Impact of Skin Antisepsis on Blood Culture Contamination
Contamination rate
Study 2% CHG/70% IPA Iodine Tincture
Barenfanger* 2.9% 2.7%
Smith 3.1% 6.8%
Tepus 2.2% 3.5%
Trautner* 0.5% 1.4%
*No statistically significant differenceBarenfaner J, et al. Journal of Clinical Microbiology. 2004;42(5):2216-2217.
Smith SM, et al. 28th Annual Meeting of APIC 2001; Publication #11-89.
Tepus D, et al. 2005. J Emerg Nurs. 31:133. Abstract 402-C.
Trautner BW, et al. Infect Control Hosp Epidemiol. 2002;23:397-401.

Culligan, et al. Am J Obstet Gynecol. 2005;192:422-5.
Comparison of Povidone-Iodine vs. Chlorhexidine for Skin Antisepsis before Vaginal Hysterectomy
Pressing Need to Compare Clinical Efficacy of Antiseptic Preparations in Preventing SSI
• CDC guidelines for prevention of infections related to vascular catheters recommend antiseptic cleansing of the skin with 2% chlorhexidine-containing productsO’Grady, et al. Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep 2002;51(RR-10): 1-29
• CDC has not previously issued a preference as to type of preoperative skin antiseptics
Intraoperative phase• Prepare the skin at the surgical site immediately before incision using an antiseptic (aqueous or alcohol-based) preparation: povidone-iodine or chlorhexidine are most suitable.
NICE 2008 Guidelines for Prevention of Surgical Site Infection
www//:nice.org.uk/guidance
How to convince surgeons to study SSI?They do not have a problemThey do not observe any wound infectionsThey do not need any help

Prospective, Randomized, 6-Center Clinical Trial of 849 Patients
• Population: adult patients scheduled for abdominal or non-abdominal clean-contaminated surgery
• Randomization: hospital-stratified• Intervention: preoperative skin cleansing with:
• ChloraPrep® (2% chlorhexidine gluconate-70% isopropyl alcohol = CA) 26-ml applicators; OR
• 10% povidone-iodine (PI) scrub and paint• Evaluation: SSI was assessed by blinded evaluators
Darouiche, et al. NEJM 2010;362:18-26
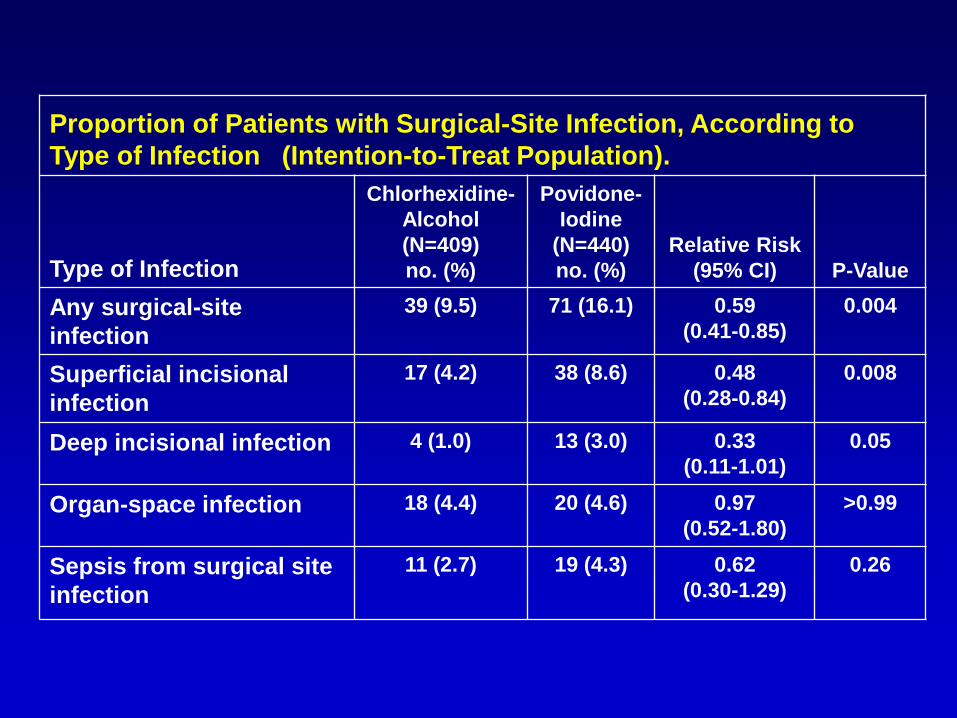
Proportion of Patients with Surgical-Site Infection, According to Type of Infection (Intention-to-Treat Population).
Type of Infection
Chlorhexidine-Alcohol (N=409)no. (%)
Povidone-Iodine
(N=440)no. (%)
Relative Risk(95% CI) P-Value
Any surgical-site infection
39 (9.5) 71 (16.1) 0.59 (0.41-0.85)
0.004
Superficial incisional infection
17 (4.2) 38 (8.6) 0.48 (0.28-0.84)
0.008
Deep incisional infection 4 (1.0) 13 (3.0) 0.33 (0.11-1.01)
0.05
Organ-space infection 18 (4.4) 20 (4.6) 0.97 (0.52-1.80)
>0.99
Sepsis from surgical site infection
11 (2.7) 19 (4.3) 0.62 (0.30-1.29)
0.26

Kaplan-Meier Curves for Freedom from Surgical-Site Infection (Intention-to-Treat Population)

Proportion of Patients with Surgical-Site Infection, According to Type of Surgery (Intention-to-Treat Population).
Chlorhexidine-Alcohol Povidone-Iodine
Type of Surgery Nno.
Infected(%)
Infected Nno.
Infected(%)
Infected Abdominal 297 37 (12.5) 308 63 (20.5)
Colorectal 186 28 (15.1) 191 42 (22.0)Biliary 44 2 (4.6) 54 5 (9.3)Small intestinal 41 4 (9.8) 34 10 (29.4)Gastroesophageal 26 3 (11.5) 29 6 (20.7)
Non-abdominal 112 2 (1.8) 132 8 (6.1)
Thoracic 44 2 (4.5) 57 4 (7.0)Gynecologic 42 0 (0.0) 40 1 (2.5)Urologic 26 0 (0.0) 35 3 (8.6)
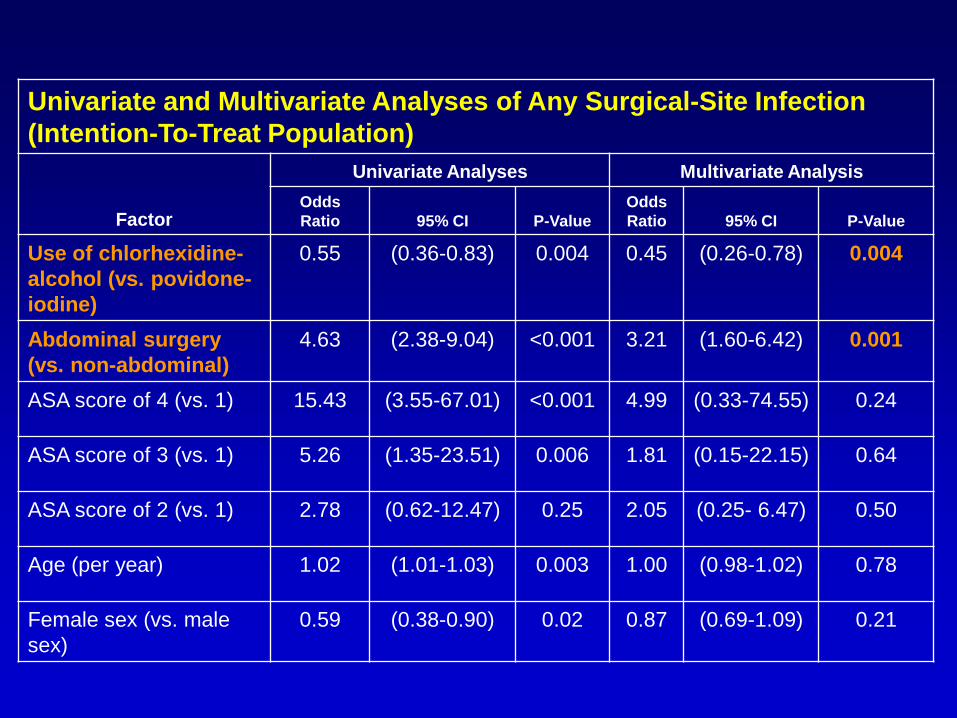
Univariate and Multivariate Analyses of Any Surgical-Site Infection (Intention-To-Treat Population)
Factor
Univariate Analyses Multivariate AnalysisOdds Ratio 95% CI P-Value
Odds Ratio 95% CI P-Value
Use of chlorhexidine-alcohol (vs. povidone-iodine)
0.55 (0.36-0.83) 0.004 0.45 (0.26-0.78) 0.004
Abdominal surgery (vs. non-abdominal)
4.63 (2.38-9.04) <0.001 3.21 (1.60-6.42) 0.001
ASA score of 4 (vs. 1) 15.43 (3.55-67.01) <0.001 4.99 (0.33-74.55) 0.24
ASA score of 3 (vs. 1) 5.26 (1.35-23.51) 0.006 1.81 (0.15-22.15) 0.64
ASA score of 2 (vs. 1) 2.78 (0.62-12.47) 0.25 2.05 (0.25- 6.47) 0.50
Age (per year) 1.02 (1.01-1.03) 0.003 1.00 (0.98-1.02) 0.78
Female sex (vs. male sex)
0.59 (0.38-0.90) 0.02 0.87 (0.69-1.09) 0.21

Univariate and Multivariate Analyses of Any Surgical-Site Infection (Intention-To-Treat Population)
FactorUnivariate Analyses Multivariate Analysis
Odds Ratio 95% CI P-Value Odds Ratio 95% CI P-Value
Alcohol abuse 1.11 (0.67-1.83) 0.69 1.12 (1.05-1.19) <0.001
Liver cirrhosis 3.28 (1.31-8.24) 0.02 2.14 (1.15-3.99) 0.02
Immunologic disease
2.72 (1.32-5.62) 0.01 1.79 (1.00-3.22) 0.05
Cancer 2.05 (1.31-3.21) 0.002 1.65 (1.04-2.64) 0.03
Diabetes mellitus 1.90 (1.16-3.11) 0.01 1.75 (1.05-2.92) 0.03
Malnutrition 3.02 (1.57-5.84) 0.003 2.62 (1.23-5.55) 0.01
Gastrointestinal disease
2.96 (1.75-5.01) <0.001 1. 27 (1.00-1.61) 0.05

Univariate and Multivariate Analyses of Any Surgical Site Infection (Intention-To-Treat Population)
Univariate Analyses Multivariate Analysis
Odds Ratio 95% CI P-Value Odds Ratio 95% CI P-Value
Infection at another bodily site (vs. no infection)
0.92 (0.32-2.68) 1.00 0.89 (0.50-1.58) 0.68
Duration of surgery(per hour)
1.33 (1.17-1.51) <0.001 1.11 (1.02-1.21) 0.01
Days that surgical drain was in place (per day)
1.03 (1.00-1.06) 0.02 1.04 (1.02-1.05) <0.001
Preop shower withChlorhexidine (vs. no shower)
1.56 (0.57-4.25) 0.38 0.95 (0.78 -1.15) 0.19
Preop shower withpovidone-iodine(vs. no shower)
0.13 (0.02-0.92) 0.01 0.36 (0.32-0.39) <0.001
Preop shower with soap (vs. no shower)
1.08 (0.65-1.82) 0.79 0.96 (0.75-1.21) 0.72

Clinical Adverse Events (Intention-to-Treat Population)
Clinical Adverse Event
Chlorhexidine-Alcohol (N=409)no. (%)
Povidone-Iodine
(N=440)no. (%)
Absolute Difference(95% CI) P-Value
Adverse events in >5% of patients in either group
228 (55.7) 256 (58.2) -2.4(-9.1 to 4.2)
0.49
Type of event- Abnormal cardiac rhythm or rate
25 (6.1) 25 (5.7) 0.4 (-2.7 to 3.6)
0.88
- Nausea 30 (7.3) 34 (7.7) -0.4(-3.9 to 3.2)
0.90
- Urinary tract infection 23 (5.6) 28 (6.4) -0.7 (-3.9 to 2.5)
0.67
- Abdominal pain 25 (5.1) 29 (6.6) -1.5(-4.6 to 1.7)
0.39
- Ileus 19 (4.6) 24 (5.5) -0.8(-3.8 to 2.1)
0.64
Drug-related adverse events 3 (0.7) 3 (0.7) 0.1(-1.1 to 1.2)
>0.99
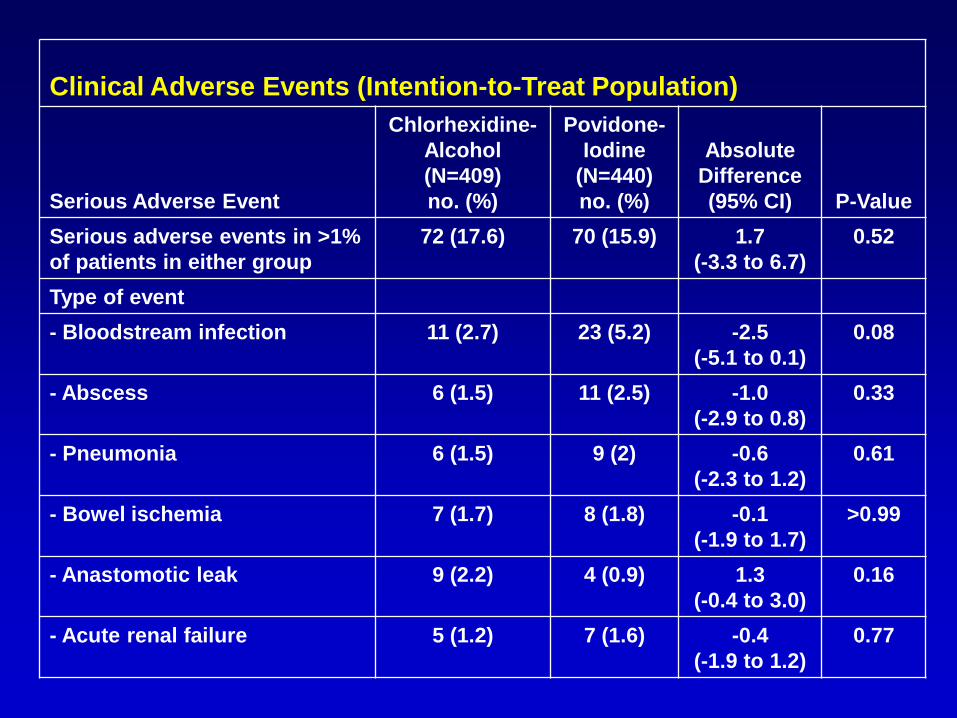
Clinical Adverse Events (Intention-to-Treat Population)
Serious Adverse Event
Chlorhexidine-Alcohol (N=409)no. (%)
Povidone-Iodine
(N=440)no. (%)
Absolute Difference(95% CI) P-Value
Serious adverse events in >1% of patients in either group
72 (17.6) 70 (15.9) 1.7(-3.3 to 6.7)
0.52
Type of event- Bloodstream infection 11 (2.7) 23 (5.2) -2.5
(-5.1 to 0.1)0.08
- Abscess 6 (1.5) 11 (2.5) -1.0(-2.9 to 0.8)
0.33
- Pneumonia 6 (1.5) 9 (2) -0.6 (-2.3 to 1.2)
0.61
- Bowel ischemia 7 (1.7) 8 (1.8) -0.1(-1.9 to 1.7)
>0.99
- Anastomotic leak 9 (2.2) 4 (0.9) 1.3(-0.4 to 3.0)
0.16
- Acute renal failure 5 (1.2) 7 (1.6) -0.4(-1.9 to 1.2)
0.77

Clinical Adverse Events (Intention-to-Treat Population)
Serious Adverse Event
Chlorhexidine-Alcohol (N=409)no. (%)
Povidone-Iodine
(N=440)no. (%)
Absolute Difference(95% CI) P-Value
Patients with serious adverse events
72 (17.6) 70 (15.9) 1.7(-3.3 to 6.7)
0.52
Type of event- Respiratory failure 4 (1) 8 (1.8) -0.8
(-2.4 to 0.7)0.39
- Bowel obstruction 3 (0.7) 5 (1.1) -0.4(-1.7 to 0.9)
0.73
Serious drug-related adverse events
0 0 --- ---
Death 4 (1) 3 (0.7) 0.3(-0.9 to 1.5)
0.72

ConclusionEfficacy and safety of CA vs. PI
• Significantly reduces SSI• Number of patients needed to receive CA
instead of PI to prevent one case of SSI: 17 • Delays onset of SSI • Its superior protection is largely due to
significant reduction in rates of superficial and deep incisional infections
• As safe as PI
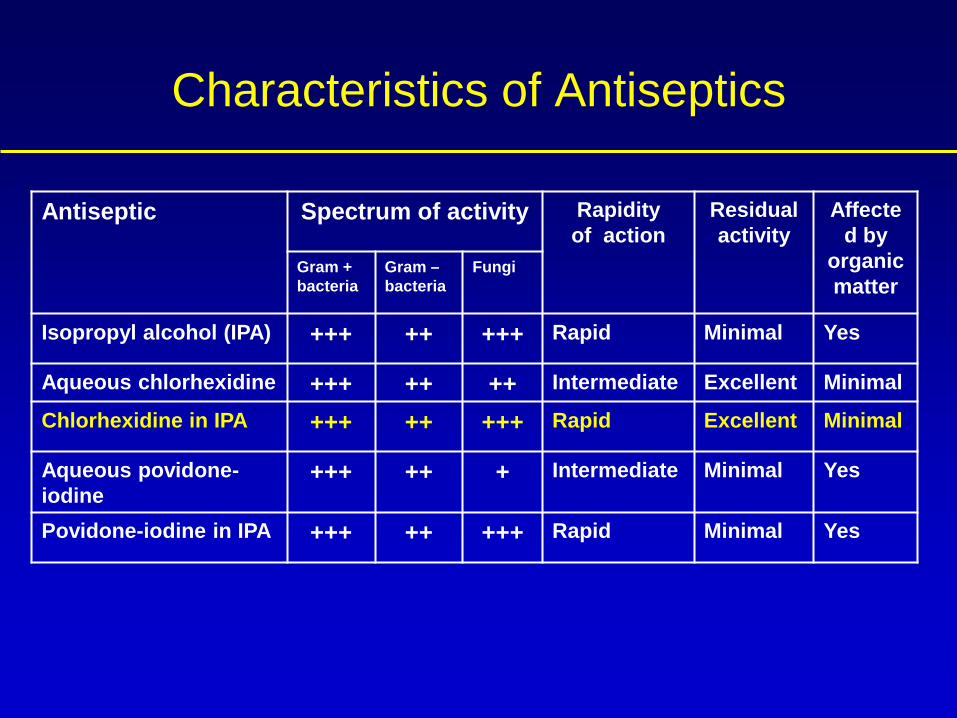
Antiseptic Spectrum of activity Rapidity of action
Residual activity
Affected by
organic matter
Gram +bacteria
Gram –bacteria
Fungi
Isopropyl alcohol (IPA) +++ ++ +++ Rapid Minimal Yes
Aqueous chlorhexidine +++ ++ ++ Intermediate Excellent Minimal
Chlorhexidine in IPA +++ ++ +++ Rapid Excellent Minimal
Aqueous povidone-iodine
+++ ++ + Intermediate Minimal Yes
Povidone-iodine in IPA +++ ++ +++ Rapid Minimal Yes
Characteristics of Antiseptics

Cost of Antiseptic Products in the US
• Mean cost of PI prep tray per patient: ~$3• Mean cost of one CA applicator: ~$7• Mean no. of CA applicators/patient: 2 • Mean cost of CA applicators per patient: $14• Extra cost of CA vs. PI/1,000 patients: $11,000

Cost of Superficial SSI
($500/case)
Cost of Deep SSI
($20,000/case)
Cost of 80:20 mix SSI($4,400/case)
CA group $49,50099 SSI cases
$1,980,00099 SSI cases
$435,60099 SSI cases
PI group $83,500167 SSI cases
$3,340,000167 SSI cases
$734,800167 SSI cases
Savings(CA vs. PI)
$34,000 $1,360,000 $299,200
Cost Savings(CA vs. PI)
$23,000 $1,349,000 $288,200
Potential Cost-SavingsPer 1,000 Surgeries in the US

Perspective on the CA applicatorCPSI
• Cost-saving• Practical• Safe• Infection-reducing

Quality Management
Patient1. Surveillance
2. Analysis
3. Intervention 4. Evaluation

Future Considerations
• Investigate the efficacy of 2% chlorhexidine-70% isopropyl alcohol in other types of surgery
• Assess the actual cost-savings associated with use of different antiseptic preparations
• Examine the potential role of complementing preoperative use of 2% chlorhexidine-70% isopropyl alcohol with other approaches

Too much skin
antisepsis
Similarities Between CRBSI and SSI• Both infections are caused mostly by skin
organisms• Both infections result primarily from
breaking skin integrity • Both infections occur at unacceptably high
rates, can be difficult to manage, may require future interventions, and are costly to treat

New CMS Regulations (effective 10/08) Changes to Inpatient Prospective Payment System
10 non-reimbursable conditions met these criteria:• High cost• High volume• Triggers a high-paying MS-DRG• May be considered reasonably preventable through
application of evidence-based guidelinesFederal Register, Volume 73, No. 161; 08/19/08

Non-reimbursable Infectious Conditions
• Catheter-associated urinary tract infection• Vascular catheter-associated infection• Surgical site infection-mediastinitis after CABG• Surgery on various joints, including shoulder,
elbow, and spine
Differences Between CRBSI and SSI• CRBSI manifests while the catheter is still in
place, whereas SSI can manifest at any time after surgery, usually by 30 days post-op
• Microbiologic cause of CRBSI is almost always identified, whereas the microbiologic cause of SSI is unknown in many patients
• Occurrence of CRBSI can be attributed to various healthcare providers, whereas SSI is typically linked to the surgeon

Nosocomial Infections in the ICU
PNEU27%
OTHER6%LRI
4%EENT
4%CVS4%
GI5%
BSI19%
UTI31%
National Nosocomial Infections Surveillance (NNIS) (97 hospitals)
87% central lines
86% Mechanical Ventilation95% Urinary Catheters
N= 14,177
< 55 = 33%55 – 70 = 32%>70 = 35%

Impact of CRBSI
• Incidence: of the 6 million CVC inserted annually in the US, 250,000 result in BSI
• Management: cure often requires removal of the infected catheter and long antibiotic therapy
• Medical sequelae: attributable mortality 5-25%• Economic burden: cost of treatment is $10-56
thousand; annual cost in US, $3–$16.8 billions

Annual Death Rates in the US for Selected Infectious Diseases
0
5,000
10,000
15,000
20,000
25,000
30,000
CRBSI MRSA AIDS Hep B Tbc Measles
Dea
ths p
er Y
ear

Comprehensive Protective StrategyInfection Control Bundle
• Hand washing• Maximal barrier precautions• 2% chlorhexidine-based skin antisepsis• Avoiding femoral site if possible• Removing unnecessary catheters

Although very essential, they: • Are not easily enforceable• Are not very durable• Do not completely prevent infection• Saves some, but not enough, lives
Potential Limitations of Traditional Infection Control Measures

Perspective
Optimal prevention of SSI and CRBSI can:• Improve patient care• Incur cost-savings• Enhance infection control measures

Screening, Randomization, and Follow-up of Study Participants

Systemic Prophylactic Antibiotics for Colorectal Surgery (Intention-to-Treat Population).
Chlorhexidine-Alcohol Povidone-Iodine(n=186) (n=191) P-Value
Cephalosporin - % 64.5 67.5 0.59
Glycopeptide - % 10.2 11.0 0.87
Nitroimidazole - % 16.1 14.7 0.78
Aminoglycoside - % 14.5 17.3 0.48
Carbapenem - % 15.1 13.6 0.77
Penicillin - % 3.8 3.7 >0.99
Macrolide - % 3.2 4.2 0.79
Fluroquinolone - % 2.7 1.6 0.50
Monobactam - % 1.1 0 0.24
Tetracycline - % 0.5 0.5 >0.99

Microbiology of Infection
• 60/110 (55%) infections had identifiable cause(s)
• 23 infections in CA group vs. 37 in PI group
• 14 more superficial or deep incisional infections by Staphylococcus aureus and streptococci in PI group
• 43% of cases were polymicrobial (total, 107 isolates)
• GP bacteria outnumbered GN bacteria by 2.5 fold
• Most common organism: S. aureus (24/60=40%)
• No significant differences in frequency of organisms, except streptococci (3% in CA vs. 16% in PI; P=0.02)
• All 4 Candida infections were in PI group (P=NS)

Clinical Manifestations of infected CVC
• Exit site infection• Tunnel infection• Thrombophlebitis• BSI