single points of entry robert mollica march 2006 [email protected]
TRANSCRIPT


Overview
• Balancing long term supports systems
• Single points of entry
• Considerations

The SPE context
• SPEs are one of several key components of long term support systems that affect choice & balance
• Others:– Funding streams
– Budget mechanisms
– Eligibility process
– Nursing home supply strategies
– Full array of services

Medicaid spending balance (billions) FY 2004
$57.6
$31.7
$15.3
$45.8
$0
$10
$20
$30
$40
$50
$60
$70
Institutions Community
All groups Elderly & Disabled
All groups = Elderly, adults with disabilities, MR/DD

Percent by population group
36%
64%
58%
42%
75%
25%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Institutions Community
All groups MR/DD Elderly and disabled

Medicaid Spending Balance 2004: Elders and adults with disabilities
51% 50%
39% 38%
29%26%
22%
11% 9%
55%
36%
0%
10%
20%
30%
40%
50%
60%
NM
, OR
AK
WA
CA
ID, N
C
MN
CO
WI
MA
AL
, FL
IN
2004
Includes HCBS waiver, state plan personal care and home health. Does not include some state plan services, state general revenue, OAA and other programs
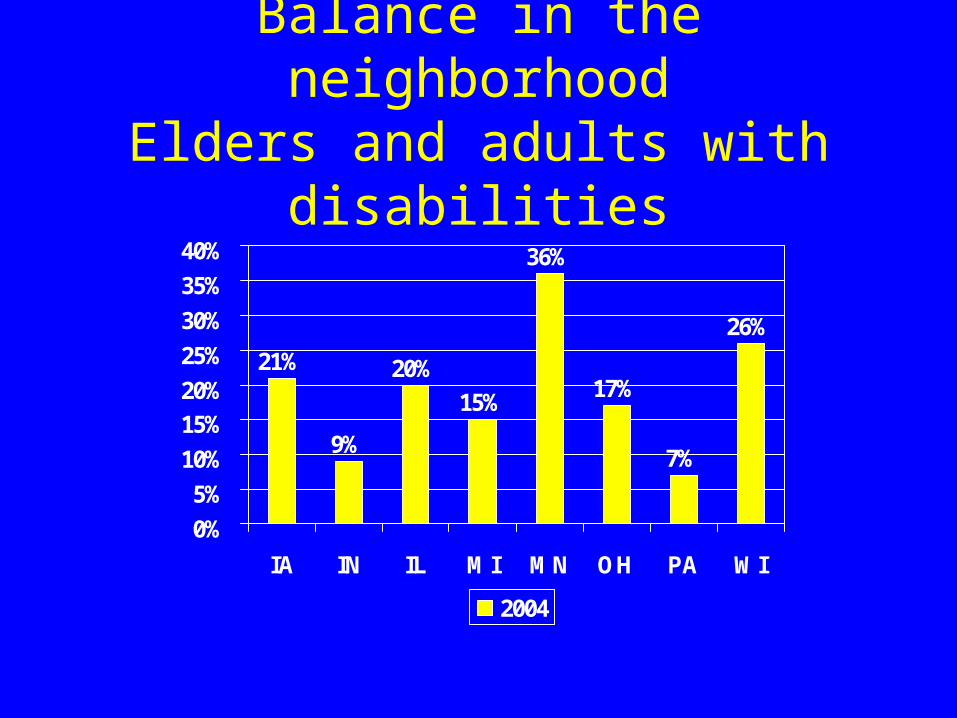
Balance in the neighborhoodElders and adults with disabilities
21%
9%
20%
15%
36%
17%
7%
26%
0%
5%
10%
15%
20%
25%
30%
35%
40%
IA IN IL MI MN OH PA WI
2004

Improving the balance in Michigan: How long will it take?
0
10
20
30
40
50
60
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
1% per year 2% per year 3% per year

Measures of balance
• Percentage spending on HCBS, NF
• Percentage of people served in community settings
• Participants days or days of coverage

Balancing strategies
• Single long term care budget (OR, MD, WA)
• Access – PA Community Choices
• Money Follows the Person (TX, MD, IN)
• Options counseling (NJ)
• Nursing home transition (NJ, WA, MA)

PA: Community Choices
• Access to assessment 24/7
• Services within 12 to 72 hours
• Reduce financial application (12 to 5 pages) and functional assessment (27 to 5 pages)
• Disregard $6,000 in assets
• Self-declaration of income and assets
• Presumptive eligibility

Washington: NF caseload trends
10000
11000
12000
13000
14000
15000
16000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
NF caseloadFigures for July each year

Washington: HCBS trends
22000
24000
26000
28000
30000
32000
34000
36000
38000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
HCBS caseload
Figures for July each year

Washington LTC Spending trends (millions)
0
200
400
600
800
1000
1200
NF spending HCBS NF @ 3% growth
Based on data from the Washington Aging and Disability Services Administration
Key SPE questions
• What is SPE? One stop? No wrong door?• A place, a web based process or both?• For whom?• For what? • Who does it? • How much does one organization offer?• Aging and Disability Resource Centers• Full or split functions?

ADRC role
• Provide information and assistance to public and private-pay individuals
• “Entry” point to publicly administered long term supports
• Target individuals at imminent risk of admission to an institution by creating linkages with the pathways to long-term care
Greg Case, AoA, 3/3/04

Key access features
• “Planting the seed” - awareness of resources• Information readily available when the
need arises• Access vs referrals• Streamlined assessment, clinical and financial
eligibility• Virtual gateway – using the internet

Comprehensive system – selected features
• Philosophy, leadership
• Comprehensive entry points/one stop
• Financing that supports access and choice
• Full array of services
• Nursing home case management and relocation assistance
• Streamlined access

Comprehensive entry points
• What is “entry”?
• A system that enables consumers to access long term and supportive services through one agency or organization
• 42 CEPs in 32 states and DC
NASHP 2003

CEP functions
• Information & referral• Assistance• Web based I&A• Initial screening• NF screening or
options counseling• Assessment
• Financial eligibility• Functional eligibility• Develop care plan • Authorize service • Monitor services • Reassessment • Protective services
Michigan SPE functions
• Planning and collaboration
• Outreach, education and advocacy
• Information and assistance
• Person centered planning (care plan)
• Facilitator
• Options counseling

Michigan SPE
• Program or service transitions
• Supports coordination (authorization)
• Function/medical eligibility determination
• Facilitate financial eligibility decision
• Ongoing coordination

SPE examples
• Colorado • Connecticut (CBOs)• Illinois (CCUs)• Indiana (AAAs)• Kansas (AAAs)• Maine (split)• Massachusetts
(ASAPs/AAAs)
• Minnesota (Counties)• Oregon (County AAA,
state field offices)• Pennsylvania (AAAs)• Vermont (split)• Washington (split)• Wisconsin (Counties)

Populations served
20
6 63
7
13
2224
0
5
10
15
20
25
30
Population NASHP 2003

Funding sources
35
26
1513
9
4
42
0
5
10
15
20
25
30
35
40
45
HCBS GR Stateplan
SSBG OAA County Other
NASHP 2003

Organizations
16
8
10
3
1
1313
0
2
4
6
8
10
12
14
16
18
Stateoffices
CBOs AAAs County Other CILs HHA
NASHP 2003

Split system - Vermont
• DAIL (state agency) reviews referral information and determines clinical eligibility– May make a home visit– Decides level of need (highest, high, moderate)– Reviews service options with the applicant
• Sends information to selected CMA (AAA or HHA)
• CMA completes assessment, develops care plan• DAIL reviews the plan of care

Split system - Washington
• Aging and Disability Services Administration staff complete all assessments
• Determine clinical and financial eligibility• Review service options• Develop initial care plan• Provide CM for consumers in nursing homes and
residential settings• AAAs provide ongoing CM for in-home clients

Discussion
• What does SPE mean to you?
• What functions should an SPE perform?
• What components of the current system should be kept in a SPE system?
• What linkages will be needed between community providers, physicians and SPEs?