simultaneous, real-time measurement of nitric oxide and oxygen dynamics during cardiac...
TRANSCRIPT

Sds
SJa
Db
c
d
e
h
•
•
•
•
a
ARRAA
KNOSMS
0h
Analytica Chimica Acta 802 (2013) 74–81
Contents lists available at ScienceDirect
Analytica Chimica Acta
journa l homepage: www.e lsev ier .com/ locate /aca
imultaneous, real-time measurement of nitric oxide and oxygenynamics during cardiac ischemia–reperfusion of the rat utilizingol–gel-derived electrochemical microsensors
ung Wook Kanga,1, Ok Kyun Kimb,1, Bochan Seoc, Sung Ho Leed, Fu Shi Quane,ae Ho Shinc, Gi-Ja Leea,b,∗, Hun-Kuk Parka,b,∗
Department of Biomedical Engineering & Healthcare Industry Research Institute, College of Medicine, Kyung Hee University, Hoegi-dong,ongdaemun-gu, Seoul 130-701, Republic of KoreaDepartment of Medical Engineering, Kyung Hee University, Seoul 130-701, Republic of KoreaDepartment of Chemistry, College of Natural Science, Kwangwoon University, Seoul 139-701, Republic of KoreaDepartment of Neurosurgery, Kyung Hee University Hospital, Seoul 130-702, Republic of KoreaDepartment of Medical Zoology, College of Medicine, Kyung Hee University, Seoul 130-701, Republic of Korea
i g h l i g h t s
Sol–gel modified electrochem-ical nitric oxide (NO) and O2
microsensors.We successfully measured NO and O2
dynamics in the myocardium duringmyocardial IR.The endogenous NO production wascorrelated with reoxygenation inpost-ischemic myocardium.NO and O2 perm-selective microsen-sors could be utilized to evaluate theeffect of drug or treatment.
g r a p h i c a l a b s t r a c t
r t i c l e i n f o
rticle history:eceived 16 May 2013eceived in revised form 21 August 2013ccepted 16 September 2013vailable online 25 September 2013
a b s t r a c t
In this study, we simultaneously measured nitric oxide (NO) and oxygen (O2) dynamics in the myocardiumduring myocardial ischemia–reperfusion (IR) utilizing sol–gel modified electrochemical NO and O2
microsensors. In addition, we attempted to clarify the correlation between NO release in the ischemicperiod and O2 restoration in the myocardium after reperfusion, comparing a control heart with a remoteischemic preconditioning (RIPC)-treated heart as an attractive strategy for myocardial protection. Rat
vided into two groups: a control group (n = 5) and an RIPC group (n = 5, with
hearts were randomly di eywords:itric oxidexygenimultaneous monitoringyocardial ischemia–reperfusionol–gel modified microsensors
RIPC treatment). Myocardia that underwent RIPC treatment (182 ± 70 nM, p < 0.05) released more NOduring the ischemic period than those of the control group (63 ± 41 nM). The restoration value of oxy-gen tension (pO2) in the RIPC group significantly increased and was restored to pre-ischemic levels(92.6 ± 36.8%); however, the pO2 of the control group did not increase throughout the reperfusion period(5.7 ± 7.5%, p = 0.001). Myocardial infarct size measurements revealed a significant decrease in cell death
∗ Corresponding authors. Tel.: +82 2 961 2305; fax: +82 2 6008 5535.E-mail addresses: [email protected] (G.-J. Lee), [email protected] (H.-K. Park).
1 Sung Wook Kang and Ok Kyun Kim contributed equally to this paper.
003-2670/$ – see front matter © 2013 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.aca.2013.09.029

S.W. Kang et al. / Analytica Chimica Acta 802 (2013) 74–81 75
in the myocardium region of the RIPC group (41.44 ± 6.42%, p = 0.001) compared with the control group(60.05 ± 10.91%). As a result, we showed that the cardioprotective effect of RIPC could be attributed toendogenous NO production during the ischemic period, which subsequently promoted reoxygenation inpost-ischemic myocardia during early reperfusion. Our results suggest that the promotion of endoge-nous formation during an ischemic episode might be helpful as a therapeutic strategy for protecting themyocardium from IR injury. Additionally, our NO and O2 perm-selective microsensors could be utilizedto evaluate the effect of drug or treatment.
1
(saaetstdtdtpcf
puaomaosptfactNNtn
eiftsaatmeTcad
ilr
. Introduction
Myocardial ischemia is characterized by insufficient oxygenO2) and nutrient supply to the area at risk, which leads to tis-ue infarction [1]. After acute myocardial infarction (AMI), earlynd successful reperfusion utilizing pharmacological thrombolyticgents or mechanical revascularization is the most effective strat-gy for reducing damage to the myocardium [2,3]. Despite theimely application of reperfusion therapy, survivors of AMI are atignificant risk due to later myocardial remodeling, which leadso the development of heart failure and an elevated risk of deathuring the following five years [4]. Numerous studies have shownhat the generation of reactive oxygen species (ROS) in oxygen-eprived tissue plays a crucial role in the oxidative cellular damagehat occurs during ischemia–reperfusion (IR) [5,6]. A variety ofrotection strategies, including ischemic preconditioning and post-onditioning, have been developed for the protection of organsrom IR injury [7–9].
Nitric oxide (NO) is an important physiological mediator thatlays a major role in vascular biology, ischemia, and heart fail-re. It is generally accepted that NO is associated with protectiongainst ischemic cell death [10–12]. The administration of NOr its donors prior to ischemia attenuates the consequences ofyocardial ischemia/reperfusion; that is, it reduces infarct size
nd endothelial dysfunction [13–15]. In particular, the inhibitionf mitochondrial respiration by NO at low O2 levels has beenhown to result in the redistribution of oxygen toward nonres-iratory oxygen-dependent targets, including prolyl hydroxylases,hus modulating the response of tissues to hypoxia [16]. There-ore, NO might act as an endogenous regulator of the intracellularvailability of oxygen in mammalian cells [17]. Despite the closeorrelation between NO and O2, there have been no reported quan-itative analyses of the relationship between the concentration ofO and O2 in the heart during myocardial IR. Even the impact ofO on myocardial function has been controversial, as it is difficult
o accurately measure NO levels in vivo, because NO is present atanomolar concentrations in the body and has a half-life of 2–6 s.
There has been growing interest in the development oflectrochemically-based sensors for direct and real-time monitor-ng of NO and/or O2. Electrochemical methods provide simplicity,ast response times, good sensitivity, high selectivity, and long-erm calibration stability [18–20]. A previous study reported thatol–gel derived electrochemical sensors showed good sensitivitynd selectivity for NO detection in vitro [21] and ex vivo [22]. Inddition, we reported that quantitative measurement of oxygenension dynamics utilizing the sol–gel derived oxygen sensor in the
yocardium would be helpful for evaluating the cardioprotectiveffects of therapeutic treatments such as drug administration [23].he accurate detection of physiological NO concentration is cru-ial to understanding NO signaling and its biological role, as wells the quantitative analysis of the correlation between NO and O2ynamics and the mechanisms of various therapies.
Ischemic preconditioning is an adaptive response of briefly
schemic tissues that serves to protect against subsequent pro-onged ischemic insults and reperfusion injury [24]. In particular,emote ischemic preconditioning (RIPC) is a novel method where© 2013 Elsevier B.V. All rights reserved.
ischemia followed by reperfusion of one organ is believed to pro-tect remote organs either by the release of biochemical messengersinto circulation or by the activation of nerve pathways, resulting inthe release of messengers that have a protective effect [25–28].This protects the target tissue without trauma to major vessels ordirect stress to the target organ [26]. Although some studies havedemonstrated that endothelial NO is one of the major contribu-tors to the candidate mechanism of RIPC [24,29], the mechanismof RIPC-induced cardioprotection has not yet been fully eluci-dated.
In this study, we simultaneously measured NO and O2 dynamicsin the myocardium during myocardial IR utilizing sol–gel modifiedelectrochemical NO and O2 microsensors. By comparing controland RIPC-treated hearts, we attempted to clarify the correlationbetween NO release in the ischemic period and O2 restoration inthe myocardium after reperfusion.
2. Experimental
2.1. Materials
Platinum wire (127 �m in diameter), chloroplatinic acidhexahydrate, and lead(II) acetate trihydrate were purchasedfrom Sigma (St. Louis, MO). Silver wire (250 �m in diame-ter) was purchased from Alfa Aesar (Ward Hill, MA). Tung-sten rod (250 �m in diameter) was purchased from FHC(Bowdoin, ME). Methyltrimethoxysilane (MTMOS) was pur-chased from Fluka (Buchs, Switzerland). (Heptadecafluoro-1,1,2,2-tetrahydrodecyl)trimethoxysilane (17FTMS) was purchased fromGelest (Tullytown, PA). A silver conducting epoxy paste was pur-chased from ASAHI (Tokyo, Japan). Gases for preparing standardsolutions of oxygen (5%, 10%, and 20% O2, balance N2) and nitricoxide (99.99%) were purchased from Dong-A Scientific (Seoul,South Korea) and Sung-Kang Special Gas (Seoul, South Korea). Othersolvents and chemicals were analytical-reagent grade and used asreceived. All aqueous solutions were prepared using distilled waterof 18.2 M� cm resistivity.
2.2. Animal preparation
Male Sprague-Dawley rats (Orient Bio., Inc., Seoul, Korea)weighing 250–350 g were kept under a 12-h light/12-h dark cycle(lights on at 0800 h) at 24 ± 0.5 ◦C in a central animal care facility.Food and water were provided ad libitum, but the animals werefasted for 1 day before the surgical procedure. All animal experi-ments were approved by the Committee of Animal Experiments ofthe College of Medicine, Kyung Hee University (KHUASP(SE)-11-017), and were in strict accordance with the National Institutes ofHealth Guide for the Care and Use of Laboratory Animals.
2.3. Preparation of sol–gel derived microsensors
The nitric oxide (NO) and oxygen (O2) microsensors (two-electrode configuration) consisted of a platinum working electrodeand an Ag/AgCl reference electrode. Platinum wire (127 �m in
76 S.W. Kang et al. / Analytica Chimica Acta 802 (2013) 74–81
F of ana
ddcTTwweTPat2Uao
amftd
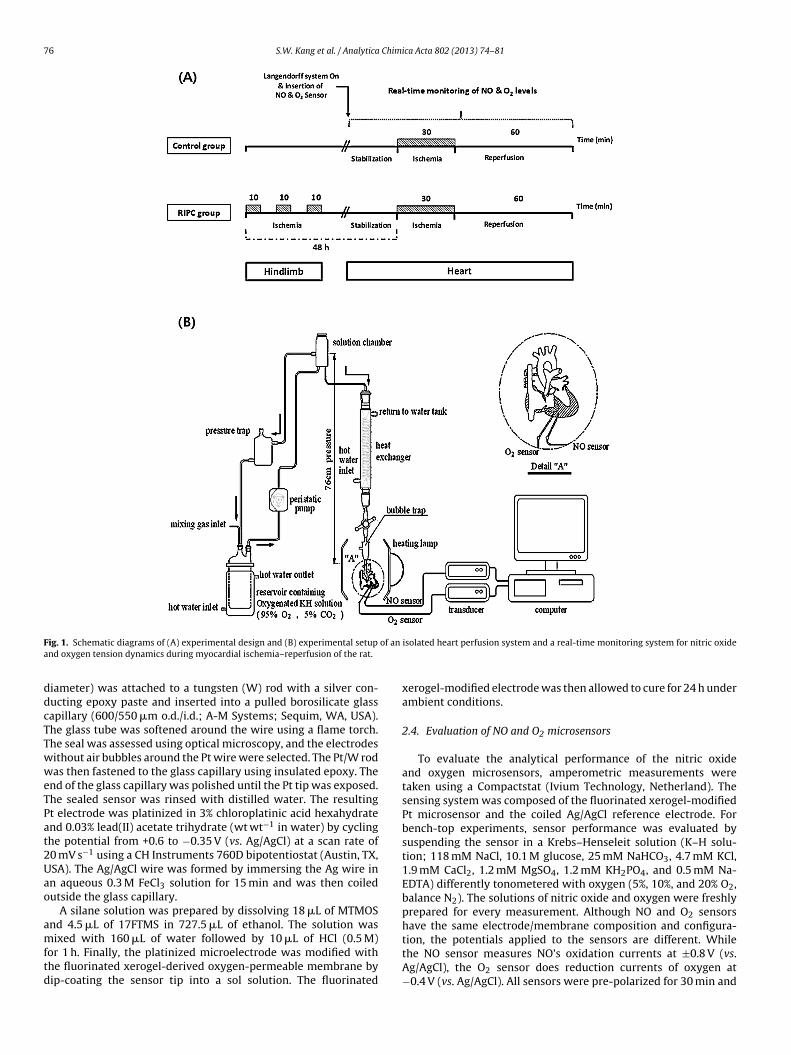
ig. 1. Schematic diagrams of (A) experimental design and (B) experimental setupnd oxygen tension dynamics during myocardial ischemia–reperfusion of the rat.
iameter) was attached to a tungsten (W) rod with a silver con-ucting epoxy paste and inserted into a pulled borosilicate glassapillary (600/550 �m o.d./i.d.; A-M Systems; Sequim, WA, USA).he glass tube was softened around the wire using a flame torch.he seal was assessed using optical microscopy, and the electrodesithout air bubbles around the Pt wire were selected. The Pt/W rodas then fastened to the glass capillary using insulated epoxy. The
nd of the glass capillary was polished until the Pt tip was exposed.he sealed sensor was rinsed with distilled water. The resultingt electrode was platinized in 3% chloroplatinic acid hexahydratend 0.03% lead(II) acetate trihydrate (wt wt−1 in water) by cyclinghe potential from +0.6 to −0.35 V (vs. Ag/AgCl) at a scan rate of0 mV s−1 using a CH Instruments 760D bipotentiostat (Austin, TX,SA). The Ag/AgCl wire was formed by immersing the Ag wire inn aqueous 0.3 M FeCl3 solution for 15 min and was then coiledutside the glass capillary.
A silane solution was prepared by dissolving 18 �L of MTMOSnd 4.5 �L of 17FTMS in 727.5 �L of ethanol. The solution was
ixed with 160 �L of water followed by 10 �L of HCl (0.5 M)or 1 h. Finally, the platinized microelectrode was modified withhe fluorinated xerogel-derived oxygen-permeable membrane byip-coating the sensor tip into a sol solution. The fluorinated
isolated heart perfusion system and a real-time monitoring system for nitric oxide
xerogel-modified electrode was then allowed to cure for 24 h underambient conditions.
2.4. Evaluation of NO and O2 microsensors
To evaluate the analytical performance of the nitric oxideand oxygen microsensors, amperometric measurements weretaken using a Compactstat (Ivium Technology, Netherland). Thesensing system was composed of the fluorinated xerogel-modifiedPt microsensor and the coiled Ag/AgCl reference electrode. Forbench-top experiments, sensor performance was evaluated bysuspending the sensor in a Krebs–Henseleit solution (K–H solu-tion; 118 mM NaCl, 10.1 M glucose, 25 mM NaHCO3, 4.7 mM KCl,1.9 mM CaCl2, 1.2 mM MgSO4, 1.2 mM KH2PO4, and 0.5 mM Na-EDTA) differently tonometered with oxygen (5%, 10%, and 20% O2,balance N2). The solutions of nitric oxide and oxygen were freshlyprepared for every measurement. Although NO and O2 sensorshave the same electrode/membrane composition and configura-
tion, the potentials applied to the sensors are different. Whilethe NO sensor measures NO’s oxidation currents at ±0.8 V (vs.Ag/AgCl), the O2 sensor does reduction currents of oxygen at−0.4 V (vs. Ag/AgCl). All sensors were pre-polarized for 30 min and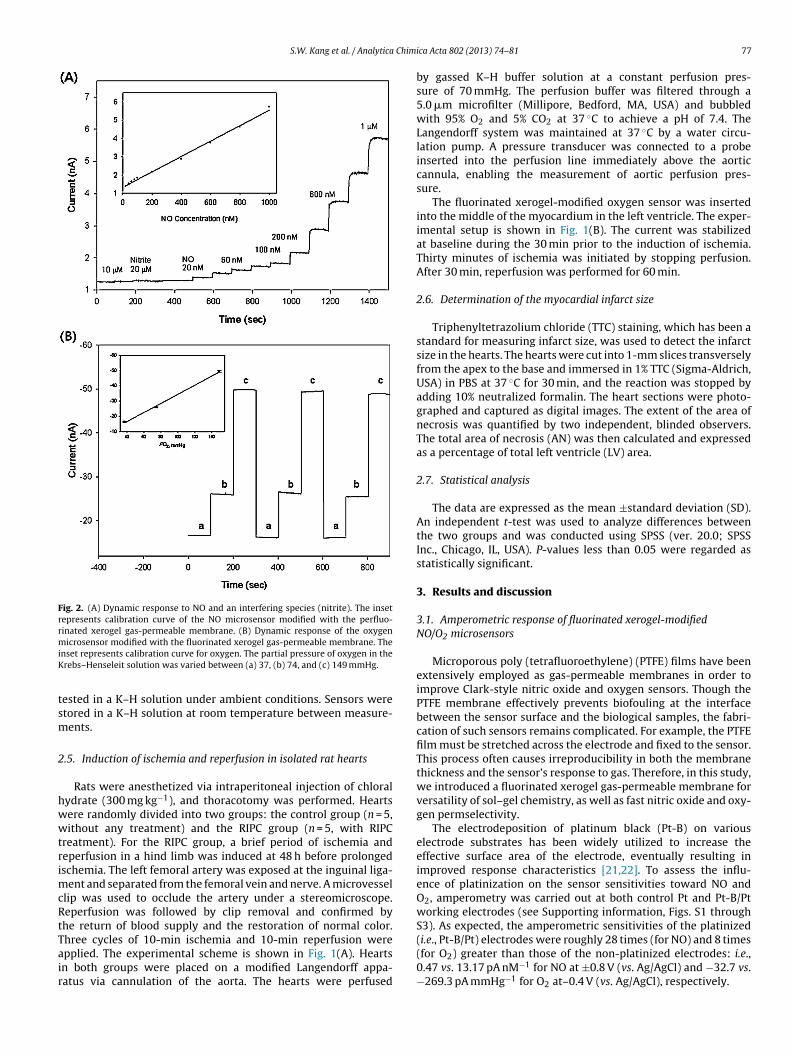
S.W. Kang et al. / Analytica Chimi
Fig. 2. (A) Dynamic response to NO and an interfering species (nitrite). The insetrepresents calibration curve of the NO microsensor modified with the perfluo-rinated xerogel gas-permeable membrane. (B) Dynamic response of the oxygenmiK
tsm
2
hwwtrimcRtTair
icrosensor modified with the fluorinated xerogel gas-permeable membrane. Thenset represents calibration curve for oxygen. The partial pressure of oxygen in therebs–Henseleit solution was varied between (a) 37, (b) 74, and (c) 149 mmHg.
ested in a K–H solution under ambient conditions. Sensors weretored in a K–H solution at room temperature between measure-ents.
.5. Induction of ischemia and reperfusion in isolated rat hearts
Rats were anesthetized via intraperitoneal injection of chloralydrate (300 mg kg−1), and thoracotomy was performed. Heartsere randomly divided into two groups: the control group (n = 5,ithout any treatment) and the RIPC group (n = 5, with RIPC
reatment). For the RIPC group, a brief period of ischemia andeperfusion in a hind limb was induced at 48 h before prolongedschemia. The left femoral artery was exposed at the inguinal liga-
ent and separated from the femoral vein and nerve. A microvessellip was used to occlude the artery under a stereomicroscope.eperfusion was followed by clip removal and confirmed byhe return of blood supply and the restoration of normal color.
hree cycles of 10-min ischemia and 10-min reperfusion werepplied. The experimental scheme is shown in Fig. 1(A). Heartsn both groups were placed on a modified Langendorff appa-atus via cannulation of the aorta. The hearts were perfusedca Acta 802 (2013) 74–81 77
by gassed K–H buffer solution at a constant perfusion pres-sure of 70 mmHg. The perfusion buffer was filtered through a5.0 �m microfilter (Millipore, Bedford, MA, USA) and bubbledwith 95% O2 and 5% CO2 at 37 ◦C to achieve a pH of 7.4. TheLangendorff system was maintained at 37 ◦C by a water circu-lation pump. A pressure transducer was connected to a probeinserted into the perfusion line immediately above the aorticcannula, enabling the measurement of aortic perfusion pres-sure.
The fluorinated xerogel-modified oxygen sensor was insertedinto the middle of the myocardium in the left ventricle. The exper-imental setup is shown in Fig. 1(B). The current was stabilizedat baseline during the 30 min prior to the induction of ischemia.Thirty minutes of ischemia was initiated by stopping perfusion.After 30 min, reperfusion was performed for 60 min.
2.6. Determination of the myocardial infarct size
Triphenyltetrazolium chloride (TTC) staining, which has been astandard for measuring infarct size, was used to detect the infarctsize in the hearts. The hearts were cut into 1-mm slices transverselyfrom the apex to the base and immersed in 1% TTC (Sigma-Aldrich,USA) in PBS at 37 ◦C for 30 min, and the reaction was stopped byadding 10% neutralized formalin. The heart sections were photo-graphed and captured as digital images. The extent of the area ofnecrosis was quantified by two independent, blinded observers.The total area of necrosis (AN) was then calculated and expressedas a percentage of total left ventricle (LV) area.
2.7. Statistical analysis
The data are expressed as the mean ±standard deviation (SD).An independent t-test was used to analyze differences betweenthe two groups and was conducted using SPSS (ver. 20.0; SPSSInc., Chicago, IL, USA). P-values less than 0.05 were regarded asstatistically significant.
3. Results and discussion
3.1. Amperometric response of fluorinated xerogel-modifiedNO/O2 microsensors
Microporous poly (tetrafluoroethylene) (PTFE) films have beenextensively employed as gas-permeable membranes in order toimprove Clark-style nitric oxide and oxygen sensors. Though thePTFE membrane effectively prevents biofouling at the interfacebetween the sensor surface and the biological samples, the fabri-cation of such sensors remains complicated. For example, the PTFEfilm must be stretched across the electrode and fixed to the sensor.This process often causes irreproducibility in both the membranethickness and the sensor’s response to gas. Therefore, in this study,we introduced a fluorinated xerogel gas-permeable membrane forversatility of sol–gel chemistry, as well as fast nitric oxide and oxy-gen permselectivity.
The electrodeposition of platinum black (Pt-B) on variouselectrode substrates has been widely utilized to increase theeffective surface area of the electrode, eventually resulting inimproved response characteristics [21,22]. To assess the influ-ence of platinization on the sensor sensitivities toward NO andO2, amperometry was carried out at both control Pt and Pt-B/Ptworking electrodes (see Supporting information, Figs. S1 throughS3). As expected, the amperometric sensitivities of the platinized
(i.e., Pt-B/Pt) electrodes were roughly 28 times (for NO) and 8 times(for O2) greater than those of the non-platinized electrodes: i.e.,0.47 vs. 13.17 pA nM−1 for NO at ±0.8 V (vs. Ag/AgCl) and −32.7 vs.−269.3 pA mmHg−1 for O2 at–0.4 V (vs. Ag/AgCl), respectively.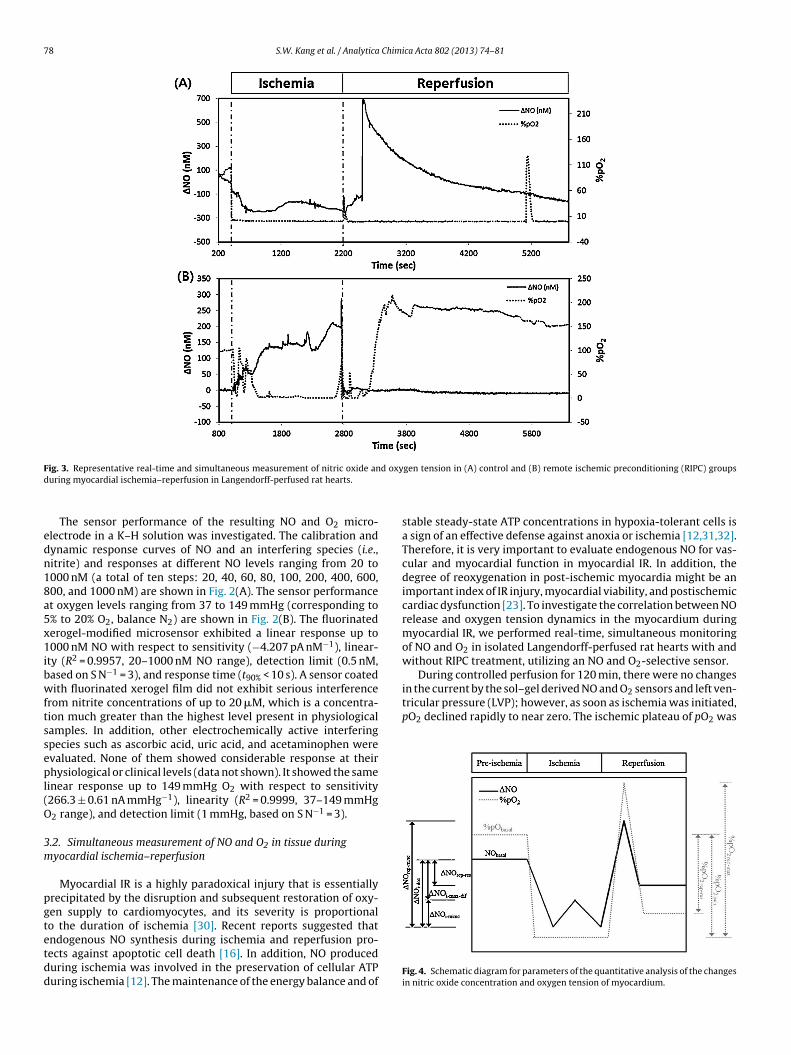
78 S.W. Kang et al. / Analytica Chimica Acta 802 (2013) 74–81
F d oxyd
edn18a5x1ibwftssepl(O
3m
pgtetdd
in the current by the sol–gel derived NO and O2 sensors and left ven-tricular pressure (LVP); however, as soon as ischemia was initiated,pO2 declined rapidly to near zero. The ischemic plateau of pO2 was
ig. 3. Representative real-time and simultaneous measurement of nitric oxide anuring myocardial ischemia–reperfusion in Langendorff-perfused rat hearts.
The sensor performance of the resulting NO and O2 micro-lectrode in a K–H solution was investigated. The calibration andynamic response curves of NO and an interfering species (i.e.,itrite) and responses at different NO levels ranging from 20 to000 nM (a total of ten steps: 20, 40, 60, 80, 100, 200, 400, 600,00, and 1000 nM) are shown in Fig. 2(A). The sensor performancet oxygen levels ranging from 37 to 149 mmHg (corresponding to% to 20% O2, balance N2) are shown in Fig. 2(B). The fluorinatederogel-modified microsensor exhibited a linear response up to000 nM NO with respect to sensitivity (−4.207 pA nM−1), linear-
ty (R2 = 0.9957, 20–1000 nM NO range), detection limit (0.5 nM,ased on S N−1 = 3), and response time (t90% < 10 s). A sensor coatedith fluorinated xerogel film did not exhibit serious interference
rom nitrite concentrations of up to 20 �M, which is a concentra-ion much greater than the highest level present in physiologicalamples. In addition, other electrochemically active interferingpecies such as ascorbic acid, uric acid, and acetaminophen werevaluated. None of them showed considerable response at theirhysiological or clinical levels (data not shown). It showed the same
inear response up to 149 mmHg O2 with respect to sensitivity266.3 ± 0.61 nA mmHg−1), linearity (R2 = 0.9999, 37–149 mmHg2 range), and detection limit (1 mmHg, based on S N−1 = 3).
.2. Simultaneous measurement of NO and O2 in tissue duringyocardial ischemia–reperfusion
Myocardial IR is a highly paradoxical injury that is essentiallyrecipitated by the disruption and subsequent restoration of oxy-en supply to cardiomyocytes, and its severity is proportionalo the duration of ischemia [30]. Recent reports suggested that
ndogenous NO synthesis during ischemia and reperfusion pro-ects against apoptotic cell death [16]. In addition, NO produceduring ischemia was involved in the preservation of cellular ATPuring ischemia [12]. The maintenance of the energy balance and ofgen tension in (A) control and (B) remote ischemic preconditioning (RIPC) groups
stable steady-state ATP concentrations in hypoxia-tolerant cells isa sign of an effective defense against anoxia or ischemia [12,31,32].Therefore, it is very important to evaluate endogenous NO for vas-cular and myocardial function in myocardial IR. In addition, thedegree of reoxygenation in post-ischemic myocardia might be animportant index of IR injury, myocardial viability, and postischemiccardiac dysfunction [23]. To investigate the correlation between NOrelease and oxygen tension dynamics in the myocardium duringmyocardial IR, we performed real-time, simultaneous monitoringof NO and O2 in isolated Langendorff-perfused rat hearts with andwithout RIPC treatment, utilizing an NO and O2-selective sensor.
During controlled perfusion for 120 min, there were no changes
Fig. 4. Schematic diagram for parameters of the quantitative analysis of the changesin nitric oxide concentration and oxygen tension of myocardium.

S.W. Kang et al. / Analytica Chimica Acta 802 (2013) 74–81 79
Table 1Parameters of the quantitative analysis of changes in nitric oxide concentration and oxygen tension in myocardia during myocardial ischemia–reperfusion.
Parameter Description
Changes in NO and O2
concentrationIschemic period NObasal Baseline NO concentration during pre-ischemic period
�NOi-idec Initial decrement of NO after the onset of ischemia�NOi-minc Maximum increment of NO during the ischemic period�NOi-max-dif Difference between maximum level of NO (NOmax) during ischemic period and
NObasal (positive): NOmax > NObasal, (negative): NOmax < NObasal
%pO2 basal Normalized pO2 during the pre-ischemic period (pO2 basal/pO2basal) × 100%pO2 isch Normalized pO2 in an ischemic plateau (pO2 isch/pO2 basal) × 100
Reperfusion period �NOrep-minc Maximum increment of NO during the reperfusion period�NOrep-res Difference between restoration level of NO (NOres) after reperfusion and NObasal
(positive): NOres > NObasal, (negative): NOres < NObasal
%pO2rep-max Maximum level of pO2 during the reperfusion period (pO2 rep-max/pO2 basal) × 100%pO2 rep-res Restoration level of pO2 after 60 min of reperfusion (pO2 rep-res/pO2basal) × 100
Table 2Changes in nitric oxide concentration and oxygen tension during myocardial ischemia–reperfusion of control and remote ischemic preconditioning (RIPC) treated groups inan isolated heart perfusion system.
Parameter Control group RIPC group p value
Ischemicperiod
�NOi-idec (nM) 107 ± 47 8 ± 4 0.001�NOi-minc (nM) 63 ± 41 182 ± 70 0.011�NOi-max-dif (nM) −46 ± 23 199 ± 80 0.002%pO2-ischemic 0.8 ± 0.6 1.5 ± 1.3 0.339
Reperfusionperiod
�NOrep-minc (nM) 70 ± 28 87 ± 35 0.415�NOrep-res (nM) 109 ± 45 14 ± 10 0.008%pO2-rep-max 11.9 ± 9.1 159.9 ± 78.5 0.013%pO2-rep-res 5.7 ± 2.5 92.6 ± 36.8 0.001
mtwgdgtwgtmospiwdF
(bwithbgnTei
aioe
aintained during the ischemic period in both groups. In contrast,he NO dynamics in the RIPC group during the ischemic episodeere different from those in the control group. In the control
roup, the NO level initially decreased but then gradually increaseduring the ischemic period. In contrast, the NO level in the RIPCroup rapidly increased after the onset of ischemia and continuedo rise throughout the entire ischemic period. When reperfusionas initiated, the pattern of both NO level and pO2 in the RIPC
roup was different from that of the control group. Fig. 3 showshe representative pattern of NO release and pO2 response during
yocardial IR in the control (A) and RIPC (B) groups. After 30 minf ischemia followed by 60 min of reperfusion, the two groupshowed different NO and pO2 dynamics. For efficient analysis, weroposed a total of ten parameters, including six parameters for the
schemic period and four parameters for the reperfusion episode,hich represented the NO and pO2 dynamics in both groups. Theefinitions of these parameters are summarized in Table 1 andig. 4.
During the ischemic period, the pO2 of the ischemic plateau%pO2ische) did not show statistically significant differencesetween the two groups, but the NO dynamics in the RIPC groupere different from those in the control group. The initial decrease
n NO level (�NOi-idec) in the control group was 107 ± 47 nM, andhe maximum increase in NO level (�NOi-minc) was 63 ± 41 nM;owever, this NO concentration did not exceed the pre-ischemicasal NO concentration (�NOi-max-dif: (−) 46 ± 23 nM). In the RIPCroup, the �NOi-idec after the onset of ischemia (8 ± 4 nM) wasegligible, but the �NOi-minc was 182 ± 70 nM (p < 0.005, n = 5).he maximum change in NO level during the ischemic episodexceeded the pre-ischemic level by 199 ± 80 nM (�NOi-max-dif: pos-tive).
During the reperfusion episode, the changes in both NO level
nd pO2 in the RIPC group were significantly different from thosen the control group. NO level sharply increased after the onsetf reperfusion and gradually declined to below pre-ischemic lev-ls in both groups; however, the �NOrep-res (14 ± 10 nM) of theRIPC group was similar to that of the pre-ischemic period, and wassignificantly lower than that of the control group (109 ± 45 nM,p < 0.008, n = 5). Additionally, as soon as reperfusion was induced,the pO2 of the RIPC group significantly increased and was restoredto pre-ischemic levels (%pO2rep-res: 92.6 ± 36.8); however, as shownin Table 2, the pO2 of the control group did not increase throughoutthe reperfusion period (%pO2rep-res: 5.7 ± 2.5) except for the tran-sient reoxygenation peak in 5200 s. As a result, the NO level andthe pO2 of the myocardium in the RIPC group were restored topre-ischemic levels, unlike those in the control group that did notrecover to their pre-ischemic state (Fig. 5).
In summary, the endogenous production of NO during theischemic period appears to be correlated with the restoration ofNO and pO2 in post-ischemic myocardium after early reperfusion.Additionally, we inferred that RIPC would promote endogenous NOrelease against ischemic stimuli and subsequently facilitate reoxy-genation in post-ischemic myocardia after reperfusion.
3.3. Changes in myocardial infarct size
RIPC is a physiological mechanism whereby brief IR episodesattenuate damage from subsequent prolonged ischemic insults[33]. It can provide either early preconditioning protection if donejust prior to an operative procedure (<4 h) or late preconditioningif done 24 to 72 h before a cardiac procedure [8,34,35]. To confirmthe cardioprotective effect of RIPC in the late phase (48 h), we mea-sured myocardial infarct size by TTC staining. As shown in Fig. 6,the mean infarct size in the control group (60.05 ± 10.91%) was sig-nificantly larger than in the RIPC group (41.44 ± 6.42%, p = 0.001).These results were similar to those of previous studies regardingRIPC [36–38].
Though several encouraging trials of RIPC have suggested clin-
ical benefit, the mechanism of RIPC-induced protection is unclear.It has been assumed that autocoids such as adenosine, bradykinin,and nitric oxide may stimulate a neural pathway and be carriedinto the bloodstream to the target organ via a humoral pathway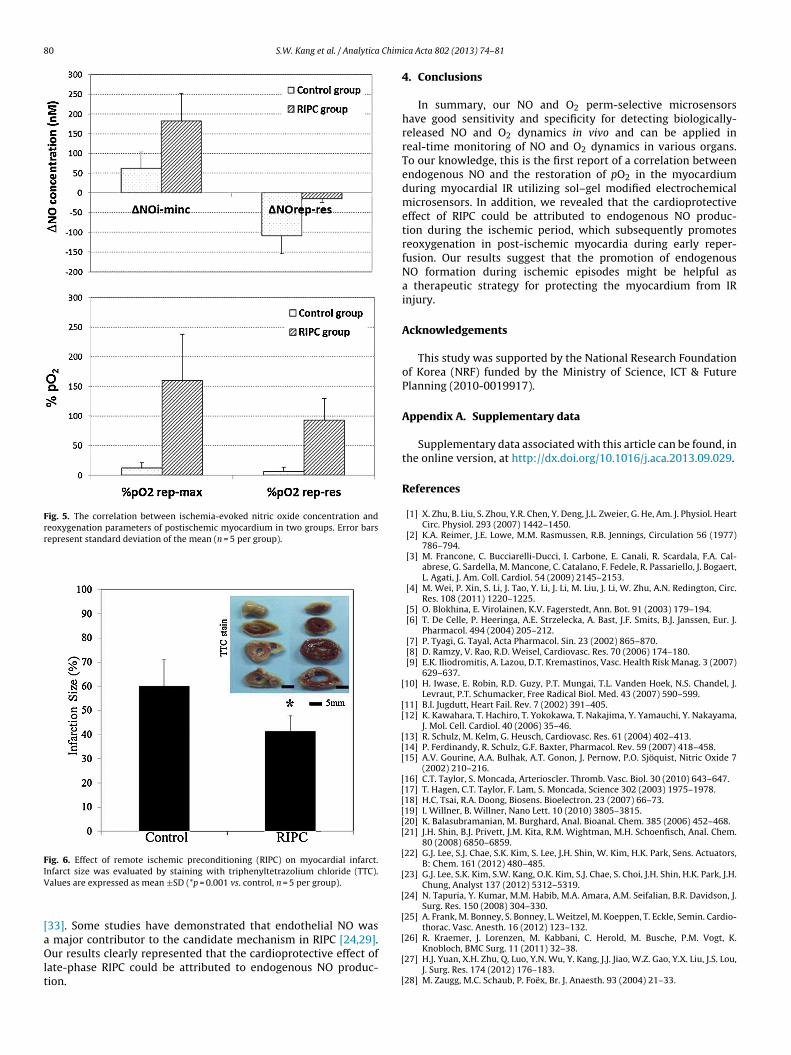
80 S.W. Kang et al. / Analytica Chim
Fig. 5. The correlation between ischemia-evoked nitric oxide concentration andreoxygenation parameters of postischemic myocardium in two groups. Error barsrepresent standard deviation of the mean (n = 5 per group).
Fig. 6. Effect of remote ischemic preconditioning (RIPC) on myocardial infarct.IV
[aOlt
[
[[
[[[
[[[[[[
[
[
[
[
nfarct size was evaluated by staining with triphenyltetrazolium chloride (TTC).alues are expressed as mean ±SD (*p = 0.001 vs. control, n = 5 per group).
33]. Some studies have demonstrated that endothelial NO was
major contributor to the candidate mechanism in RIPC [24,29].ur results clearly represented that the cardioprotective effect ofate-phase RIPC could be attributed to endogenous NO produc-ion.
[
[
[
ica Acta 802 (2013) 74–81
4. Conclusions
In summary, our NO and O2 perm-selective microsensorshave good sensitivity and specificity for detecting biologically-released NO and O2 dynamics in vivo and can be applied inreal-time monitoring of NO and O2 dynamics in various organs.To our knowledge, this is the first report of a correlation betweenendogenous NO and the restoration of pO2 in the myocardiumduring myocardial IR utilizing sol–gel modified electrochemicalmicrosensors. In addition, we revealed that the cardioprotectiveeffect of RIPC could be attributed to endogenous NO produc-tion during the ischemic period, which subsequently promotesreoxygenation in post-ischemic myocardia during early reper-fusion. Our results suggest that the promotion of endogenousNO formation during ischemic episodes might be helpful asa therapeutic strategy for protecting the myocardium from IRinjury.
Acknowledgements
This study was supported by the National Research Foundationof Korea (NRF) funded by the Ministry of Science, ICT & FuturePlanning (2010-0019917).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.aca.2013.09.029.
References
[1] X. Zhu, B. Liu, S. Zhou, Y.R. Chen, Y. Deng, J.L. Zweier, G. He, Am. J. Physiol. HeartCirc. Physiol. 293 (2007) 1442–1450.
[2] K.A. Reimer, J.E. Lowe, M.M. Rasmussen, R.B. Jennings, Circulation 56 (1977)786–794.
[3] M. Francone, C. Bucciarelli-Ducci, I. Carbone, E. Canali, R. Scardala, F.A. Cal-abrese, G. Sardella, M. Mancone, C. Catalano, F. Fedele, R. Passariello, J. Bogaert,L. Agati, J. Am. Coll. Cardiol. 54 (2009) 2145–2153.
[4] M. Wei, P. Xin, S. Li, J. Tao, Y. Li, J. Li, M. Liu, J. Li, W. Zhu, A.N. Redington, Circ.Res. 108 (2011) 1220–1225.
[5] O. Blokhina, E. Virolainen, K.V. Fagerstedt, Ann. Bot. 91 (2003) 179–194.[6] T. De Celle, P. Heeringa, A.E. Strzelecka, A. Bast, J.F. Smits, B.J. Janssen, Eur. J.
Pharmacol. 494 (2004) 205–212.[7] P. Tyagi, G. Tayal, Acta Pharmacol. Sin. 23 (2002) 865–870.[8] D. Ramzy, V. Rao, R.D. Weisel, Cardiovasc. Res. 70 (2006) 174–180.[9] E.K. Iliodromitis, A. Lazou, D.T. Kremastinos, Vasc. Health Risk Manag. 3 (2007)
629–637.10] H. Iwase, E. Robin, R.D. Guzy, P.T. Mungai, T.L. Vanden Hoek, N.S. Chandel, J.
Levraut, P.T. Schumacker, Free Radical Biol. Med. 43 (2007) 590–599.11] B.I. Jugdutt, Heart Fail. Rev. 7 (2002) 391–405.12] K. Kawahara, T. Hachiro, T. Yokokawa, T. Nakajima, Y. Yamauchi, Y. Nakayama,
J. Mol. Cell. Cardiol. 40 (2006) 35–46.13] R. Schulz, M. Kelm, G. Heusch, Cardiovasc. Res. 61 (2004) 402–413.14] P. Ferdinandy, R. Schulz, G.F. Baxter, Pharmacol. Rev. 59 (2007) 418–458.15] A.V. Gourine, A.A. Bulhak, A.T. Gonon, J. Pernow, P.O. Sjöquist, Nitric Oxide 7
(2002) 210–216.16] C.T. Taylor, S. Moncada, Arterioscler. Thromb. Vasc. Biol. 30 (2010) 643–647.17] T. Hagen, C.T. Taylor, F. Lam, S. Moncada, Science 302 (2003) 1975–1978.18] H.C. Tsai, R.A. Doong, Biosens. Bioelectron. 23 (2007) 66–73.19] I. Willner, B. Willner, Nano Lett. 10 (2010) 3805–3815.20] K. Balasubramanian, M. Burghard, Anal. Bioanal. Chem. 385 (2006) 452–468.21] J.H. Shin, B.J. Privett, J.M. Kita, R.M. Wightman, M.H. Schoenfisch, Anal. Chem.
80 (2008) 6850–6859.22] G.J. Lee, S.J. Chae, S.K. Kim, S. Lee, J.H. Shin, W. Kim, H.K. Park, Sens. Actuators,
B: Chem. 161 (2012) 480–485.23] G.J. Lee, S.K. Kim, S.W. Kang, O.K. Kim, S.J. Chae, S. Choi, J.H. Shin, H.K. Park, J.H.
Chung, Analyst 137 (2012) 5312–5319.24] N. Tapuria, Y. Kumar, M.M. Habib, M.A. Amara, A.M. Seifalian, B.R. Davidson, J.
Surg. Res. 150 (2008) 304–330.25] A. Frank, M. Bonney, S. Bonney, L. Weitzel, M. Koeppen, T. Eckle, Semin. Cardio-
thorac. Vasc. Anesth. 16 (2012) 123–132.
26] R. Kraemer, J. Lorenzen, M. Kabbani, C. Herold, M. Busche, P.M. Vogt, K.Knobloch, BMC Surg. 11 (2011) 32–38.27] H.J. Yuan, X.H. Zhu, Q. Luo, Y.N. Wu, Y. Kang, J.J. Jiao, W.Z. Gao, Y.X. Liu, J.S. Lou,
J. Surg. Res. 174 (2012) 176–183.28] M. Zaugg, M.C. Schaub, P. Foëx, Br. J. Anaesth. 93 (2004) 21–33.

Chimi
[[
[[
[
[
[
[[[
SsoImo
OSPSm
BSorm
SUYKNo
S.W. Kang et al. / Analytica
29] L.S. Burwell, P.S. Brookes, Antioxid. Redox Signal. 10 (2008) 579–599.30] X. Li, F. Arslan, Y. Ren, S.S. Adav, K.K. Poh, V. Sorokin, C.N. Lee, D. de Kleijn, S.K.
Lim, S.K. Sze, J. Proteome Res. 11 (2012) 2331–2346.31] R.G. Boutilier, J. Exp. Biol. 204 (2001) 3171–3181.32] P.W. Hochachka, P.L. Lutz, Comp. Biochem. Physiol. Part B: Biochem. Mol. Biol.
130 (2001) 435–459.33] S.R. Walsh, S.A. Nouraei, T.Y. Tang, U. Sadat, R.H. Carpenter, M.E. Gaunt, Vasc.
Endovasc. Surg. 44 (2010) 434–439.34] S. Kanoria, R. Jalan, A.M. Seifalian, R. Williams, B.R. Davidson, Transplantation
84 (2007) 445–458.35] S.P. Loukogeorgakis, A.T. Panagiotidou, M.W. Broadhead, A. Donald, J.E. Dean-
field, R.J. MacAllister, J. Am. Coll. Cardiol. 46 (2005) 450–456.36] S.Y. Lim, D.M. Yellon, D.J. Hausenloy, Basic Res. Cardiol. 105 (2010) 651–655.37] G.T. Wong, Y. Lu, B. Mei, Z. Xia, M.G. Irwin, Life Sci. 91 (2012) 860–865.38] J. Gao, Y. Kang, J. Lou, J. Surg. Res. 174 (2012) e47–e54.
ung Wook Kang received his M.S. degree in Pharmacology at Kyung Hee Univer-ity, South Korea in 2009. Since 2009, he is a Ph.D. candidate under the supervisionf Prof. Hun-Kuk Park in Department of Biomedical Engineering and Healthcarendustry Research Institute at Kyung Hee University, South Korea. Currently, His
ain research interest includes neuroscience, biosensors and medical applicationsf electrotaxis.
k Kyun Kim received his M.S. in Biomedical Engineering from Nambu University,outh Korea in 2011. Since 2011, he is a Ph.D. candidate under the supervision ofrof. Hun-Kuk Park in Department of Medical Engineering at Kyung Hee University,outh Korea. His main research interest includes biosensors, ultrasonography andyocardial infarction.
ochan Seo received his B.S. degree in Chemistry from Kwangwoon University ineoul, South Korea in 2012. Currently, he is a MS candidate under the supervisionf Prof. Jae Ho Shin in the Department of Chemistry at Kwangwoon University. Hisesearch interest is in the development of amperometric nitric oxide and oxygenicrosensors equipped with a sol–gel-derived gas permselective membrane.
ung Ho Lee received his M.D. and B.M. from the School of Medicine at Kyung Hee
niversity, South Korea in 2005. He is a Ph.D. candidate under the supervision of Prof.oung Jin Lim in the Department of Neurosurgery at Kyung Hee University, Southorea. From 2006 to 2009, he served as an intership and residency at Department ofeurosurgery, Kyung Hee University Hospital, South Korea. Currently, he is a fellowf Department of Neurosurgery, Kyung Hee University Hospital, South Korea. Hisca Acta 802 (2013) 74–81 81
main interests include neurovascular surgery, cerebral endovascular intervention,and vascular neuroscience.
Fu Shi Quan received her Ph.D. degree at Korea University Seoul, Korea and had post-doctoral training in the laboratory of professor Richard W. Compans (Department ofMicrobiology & Immunology, School of Medicine, Emory University, GA USA). Shehas spent most of her scientific career in Dr. Compans’ lab studying virus-like particlevaccines. Currently, she is an Assistant Professor in Department of Medical Zoologyat Kyung Hee University School of Medicine, where her focus is the development ofVLP protective vaccines against influenza and a respiratory syncytial virus (RSV). Sheis recognized as an expert in influenza VLP vaccine research and the developmentof related mouse models.
Jae Ho Shin is an Associate Professor in the Department of Chemistry at Kwang-woon University in Seoul, South Korea, where he received his BS and MS degrees inChemistry. He earned his Ph.D. in Chemistry from the University of North Carolina atChapel Hill in 2006. He was then a Carolina Center of Cancer Nanotechnology Excel-lence Postdoctoral Fellow at UNC at Chapel Hill for one year. His research interestsinclude chemical and biosensors based on sol–gel-derived materials, electrochem-ical immunosensing platforms, and nitric oxide-releasing silica scaffolds.
Gi-Ja Lee received her M.S. and Ph.D. in Physical Chemistry from Yonsei Universityin Seoul, South Korea in 1997 and 2000, respectively. Since 2006, she has worked asa Principal Researcher in the Department of Biomedical Engineering and HealthcareIndustry Research Institute at Kyung Hee University, South Korea. Currently, sheis an Assistant Professor in Department of Biomedical Engineering at Kyung HeeUniversity. Her main research interests include amperometric biosensors, biochips,CNT-FET sensors, and medical applications of AFM.
Hun-Kuk Park received his M.D. and B.M. from the School of Medicine at KyungHee University, South Korea in 1982. He received a Ph.D. in Biomedical Engineeringat Rutgers University and the University of Medicine and Dentistry of New Jersey,USA in 1993. From 1997 to 2003, he served as an Assistant Professor in the Depart-ment of Neurosurgery at Wayne State University, MI, USA. He also was a facultymember of the Department of Biomedical Engineering, School of Medicine at KyungHee University, South Korea from 2003 to 2008. Since 2008, he has been a Profes-
sor in the Department of Biomedical Engineering, School of Medicine at Kyung HeeUniversity, South Korea. Dr. Park’s main research interests include neuroscience,biomechanics, cranioplasty, endovasculartherapy, nano-biosensors, pain analysis,nano-acupunture techniques, bioinformatics/pharmacogenomics, and AFM appli-cations for medical science.