significance of aeg-1 expression in correlation with vegf, microvessel density and...
TRANSCRIPT

Journal of Surgical Oncology 2011;103:184–192
Significance of AEG-1 Expression in Correlation With VEGF, Microvessel Density
and Clinicopathological Characteristics in Triple-Negative Breast Cancer
CONG LI, PhD,1 RUI LI, MD,2 HONGTAO SONG, PhD,1 DONG WANG, PhD,2 TIAN FENG, PhD,5
XIAOGUANG YU, PhD,5* YULAN ZHAO, PhD,1 JUNJUN LIU, PhD,1 XIAOYU YU, PhD,1 YANBO WANG, MD,4
AND JINGSHU GENG, PhD1,3**
1Department of Pathology, the Affiliated Tumor Hospital of Harbin Medical University, Harbin 150040, China2Department of Surgery, People’s Hospital, Peking University, Beijing 100044, China3Department of Medical Genetics, Harbin Medical University, Harbin 150086, China
4Department of Breast Surgery, the Affiliated Tumor Hospital of Harbin Medical University, Harbin 150040, China5Department of Biochemistry and Molecular Biology, College of Basic Medical Science, Harbin Medical University, Harbin 150081, China
Purpose: Our study is to examine astrocyte-elevated gene-1 (AEG-1) expression in triple-negative breast cancer and to determine whether it is
associated with vascular endothelial growth factor (VEGF), microvessel density (MVD), clinicopathological parameters and poor survival.
Methods: Specimens from 125 patients with triple-negative breast cancers were investigated by immunohistochemistry for MVD, AEG-1 and
VEGF expression. Correlations between the expression of AEG-1, VEGF, MVD, and various clinicopathological factors including survival status
were studied.
Results: AEG-1 and VEGF were highly expressed in 56.8% and 52.8% of triple-negative breast cancer patients, respectively. The intensity of
AEG-1 was gradually up-regulated from VEGF�MVD�low, VEGF�high, or MVD�high to VEGF�MVD�high tissues using Western blot
analysis. Statistically significant correlation was found among AEG-1 and VEGF, and MVD. Moreover, AEG-1 expression was correlated with
clinical stage, lymphatic venous invasion, lymph nodal metastasis, tumor size, Ki67, and recurrence. Patients with AEG-1 high-expression
showed far lower disease-free survival (DFS) and overall survival (OS) rates than those with AEG-1 low-expression. For VEGF and MVD, there
were similar results in these patients. Only AEG-1 expression and tumor size were independent prognostic factors for both DFS and OS by
multivariate analysis. However, the prognostic impact of tumor size was not as strong as that of AEG-1.
Conclusions: AEG-1 expression may be related with tumor angiogenesis and progression and is a valuable prognostic factor in patients with
triple-negative breast cancer.
J. Surg. Oncol. 2011;103:184–192. � 2010 Wiley-Liss, Inc.
KEY WORDS: triple-negative breast cancer; prognosis; angiogenesis; astrocyte-elevated gene-1; vascular endothelialgrowth factor
INTRODUCTION
Breast cancer is the second leading cause of cancer related death
among women in the Western world [1]. It is a heterogeneous disease
for which there is a variety of biology, natural history, and treatment
options. The triple-negative breast cancer, denoted by lack of
expression of all three protein receptors (ER-PR-HER2-), has recently
emerged as a distinct subtype [2]. This type of breast cancer, which
carries a poor prognosis, is insensitive to most available hormonal or
targeted therapeutic agents [3,4]. Therefore, it is important for the
prevention of triple-negative breast cancer to find reliable biomarkers
that may be used to individualize the patient prognosis.
In recent years, emphasis has increasingly been placed on pro-
and anti-angiogenic factors in malignant tumor, because unbalance
between them results in angiogenesis. Angiogenesis, the process of
forming neovascularization from existing vascular networks, is a
fundamental event in the development and maintenance of solid tumors
and their metastasis [5,6]. Current studies have demonstrated that the
remodeling for breast cancer to grow beyond a certain size requires
constant vascular growth [7]. Nowadays, a multitude of both pro- and
anti-angiogenic factors have been described [8–11], but there are no
studies investigating the expression of these factors in the triple-
negative breast cancer tissues.
Astrocyte-elevated gene-1 (AEG-1), also known as metadherin
(MTDH) [12], is initially identified as a human immunodeficiency
virus (HIV)-1 and tumor necrosis factor (TNF)-a-inducible gene in
primary human fetal astrocytes [13]. Ectopic expression of AEG-1 as a
prominent contributor to cancer progression can promote anchorage-
independent growth and invasion of non-tumorigenic melanocytes and
astrocytes [14]. Partly due to the phenomenon that the 8q22 gain
functions independently in poor prognosis in breast cancer, human
AEG-1 gene is located at chromosome 8q22 [12,15]. Its genomic
amplification has also been found in diverse cancers including breast
cancer in comparison with their normal counterparts [16,17]. AEG-1 is
Abbreviations: AEG-1, astrocyte-elevated gene-1; HIV-1, human immu-nodeficiency virus type-1; LVS, lymphatic and venous; MVD, microvesseldensity; PI3K, phosphoinositide 3-kinase; TNF-a, tumor necrosis factor-a;VEGF, vascular endothelial growth factor.
Grant sponsor: Natural Science Foundation of Heilongjiang ProvinceD2009–21; Grant sponsor: Innovation Fund for Excellent Graduates ofHarbin Medical University HCXB2010018; HCXS2010001.
*Correspondence to: Xiaoguang Yu, Department of Biochemistry andMolecular Biology, College of Basic Medical Science, Harbin MedicalUniversity, Harbin, 150081, China. E-mail: [email protected]
**Correspondence to: Jingshu Geng, Department of Pathology, theAffiliated Tumor Hospital of Harbin Medical University, Harbin 150040,China. Fax No.: 86-451-86298232. E-mail: [email protected]
Received 15 July 2010; Accepted 22 September 2010
DOI 10.1002/jso.21788
Published online 23 November 2010 in Wiley Online Library(wileyonlinelibrary.com).
� 2010 Wiley-Liss, Inc.

a downstream target of Harvey-Ras (Ha-ras) and plays an important
role in Ha-ras mediated oncogenesis and angiogenesis through the
phosphatidylinositol 3-kinase (PI3K)/Akt signaling pathway [18].
The other signaling pathway activated by AEG-1 is nuclear factor k-B
(NF-kB) via IkBa degradation and p65 translocation [19,20]. AEG-1
also enhances DNA binding and transcriptional activities of NF-kB in
Hela cells [19,20]. NF-kB regulates the expression of various
molecules such as matrix metalloproteinase (MMP), inflammatory
cytokines, chemokines, and cell adhesion proteins, all of which initiate
cancer cell invasion and angiogenesis [19,20]. Recent studies have
demonstrated that AEG-1 up-regulation in epithelial cells inhibits
apoptosis and increases the invasiveness of malignant cells, favoring
tumorigenesis, neovascularization, and metastasis [21]. The lung-
homing domain of AEG-1 can mediate breast cancer cells metastasis to
lung by tumor cell adhesion to lung vasculature both in vivo and
in vitro [12,15]. In addition, AEG-1 is frequently over-expressed in
highly proliferative breast cancer and high-grade lesions [22,23]. Its
expression status is strikingly correlated with the progression and poor
prognosis of various cancers, including breast cancer [23–26].
Immunohistochemical analysis has revealed that enhanced expression
of AEG-1 in tumor sections can augment expression of specific
angiogenesis molecules including angiopoietin-1 (Ang1), MMP-2, and
TNF-a, further supporting a potential role of AEG-1 in tumor
angiogenesis [20]. This study also identifies that AEG-1 is indeed an
oncogene and a direct regulator of angiogenesis by up-regulating key
components such as vascular endothelial growth factor (VEGF) in the
process of blood vessel formation [20,27]. VEGF is a specific
mitogenic factor for endothelial cells and promotes tumor angiogenesis
[28]. This glycoprotein facilities the permeability of the endothelium
of blood vessels, which in turn allows for cancerous cells to penetrate
the vessel walls and begin the process of metastasis, even in very
distant organs [29–31]. Previous studies have also indicated that
VEGF expression in tumors is a predictive factor of an increased risk of
metastatic diseases and poor survival in breast cancer [32–34]. An
enhanced understanding of AEG-1 and VEGF involved in angiogen-
esis of triple-negative breast cancer will pave the way for the
development of more potent and selective inhibitors of breast cancer.
To the best of our knowledge, our study is the first to immuno-
histochemically determine AEG-1 expression in triple-negative breast
cancer and to correlate its expression with VEGF, MVD, clinico-
pathological features, and survival in a large number of patients with
triple-negative breast cancer.
MATERIALS AND METHODS
Patients and Tissue Specimens
This study used archival material from the Department of Pathology
at the Affiliated Tumor Hospital of Harbin Medical University. The
invasive breast cancer tissue specimens were obtained from patients
undergoing primary mastectomies at our institution from December 1,
2003 to January 25, 2005. According to clinical requirement, our
department also routinely stained Ki67 and p53 for all invasive breast
cancer patients. In this study, the positive expression of Ki67 and p53
occurred in 110/125(88.0%) and 69/125(55.2%) patients with a
diagnosis of primary triple-negative breast cancer, respectively. In
addition, all three molecular markers (ER, PR, HER-2/neu) of these
patients were available. Excluded were patients who presented with
recurrent tumor, non triple-negative breast tumors, non-invasive tumor,
metastatic disease at presentation, bilateral tumors, other previous
tumor, or those who had previously received neo-adjuvant treatment.
Tumor size at the largest diameter of the invasive carcinoma was
measured in millimeters by the pathologist.
In all cases, the histological diagnosis was confirmed by
corresponding paraffin-embedded materials, and when necessary,
panels of immunohistochemical study were carried out, according to
the most recent World Health Organization (WHO) classification.
Breast cancers were routinely divided into ductal carcinoma, lobular
carcinoma and others (medullary carcinoma, mucinous carcinoma).
The tumor grade of invasive carcinoma was classified according to the
Scarff–Bloom–Richardson system [35]. Based on the frequency of
cell mitosis, tubule formation, and nuclear pleomorphism, invasive
carcinoma was graded as grade 1 (low), 2 (moderate) or 3 (high grade).
The presence of lymph node metastases was reviewed for each patient.
The tumor TNM (tumors, nodes, metastases) stage was done according
to the Handbook of Cancer Stages, Edition 6, AJCC: 25 patients (20%)
stage I, 71 patients (56.8%) at stage II, 29 patients (23.2%) at stage III
[36]. The median age of the patients was 52 years (range, 29–
72 years). WHO Criteria for determining menopause include any of
the following: prior bilateral oophorectomy; age 60 years; age
<60 years and amenorrhea for 12 or more months in the absence of
chemotherapy, Toremifene, tamoxifen, or ovarian suppression and
FSH and estradiol in the post-menopausal range (WHO 1996). Forty-
six cases were menopause and 79 cases were non-menopause. All
protocols were reviewed and approved by the Ethical Committee of
Harbin Medical University, Harbin, China. All patients gave informed
consent to the diagnostic procedures and the proposed treatment.
Follow-Up
Clinical and pathological records of all patients on the study were
reviewed periodically. Patients were followed regularly for 5 years at
the Affiliated Tumor Hospital of Harbin Medical University. Clinical
records were obtained from the departments providing follow-up care
to six patients on the study who moved to other parts of the country. All
patients were followed until death or the study closing date (April 25,
2010). Disease-free survival (DFS) and overall survival (OS) were the
two assessments used for prognostic analyses.
Triple-Negative Breast Carcinoma Tissues
The data on ER, PR, and HER-2/neu were obtained through
standard clinical testing. Immunohistochemical markers were assayed
in paraffin-embedded, formation-fixed tissue stained with hematoxylin
and eosin using antibodies to the proteins ER, PR, and HER-2/neu
(Dako, Glostrup, Denmark). For ER and PR, receptor positivity was
based on more than 10% of cells testing positive. HER-2/neu was
assessed through immunohistochemistry and scored on a qualitative
scale from 0 to 3þ, based on interpretation of staining, with 0 and 1þclassified as negative, and 3þ as positive [37]. HER-2/neu scores of 2þwere considered positive for the current study because this was the
accepted classification scheme at the time of clinical treatment. Each
case was analyzed by two independent scientists. It should be noted
that we only selected those with HER-2/neu scores of 0 as HER-2/neu
negative for accuracy in this study.
Immunohistochemical Staining
Immunohistochemical staining was performed in all tissue samples,
using UltrasensitiveTM S-P kit and diaminobenzidine (Maixin-Bio Co.,
Fuzhou, China), as recommended by the manufacturers. Briefly,
sections (4 mm, thickness) were deparaffinized with xylene, rehydrated
through graded alcohol and rinsed in phosphate-buffered saline (PBS).
Antigen retrieval was performed by placing the slides in boiling citric
acid buffer at pH 6.0 for 5 min. Endogenous peroxidase activity was
blocked with 3% hydrogen peroxide in methanol for 20 min.
Incubation with 10% normal goat serum in PBS was performed for
10 min to eliminate non-specific staining. Incubation with primary
antibody was carried out next, followed by incubation with secondary
antibody (according to the primary antibody). Sections were stained
Journal of Surgical Oncology
The Role of AEG-1 in Breast Cancer 185

with 0.02% DAB and 0.02% H2O2 in 0.05 M Tris–HCl buffer for
10 min. Finally, sections were lightly counterstained with 10% Mayer
hematoxylin, dehydrated, mounted, and observed. Immunostaining
was performed with a rabbit polyclonal immunoglobulin (Ig) G
specific for AEG-1 (dilution 1:400; Proteintech Group Inc., Carpin-
teria, CA), rabbit polyclonal IgG specific for VEGF (dilution 1:200;
Santa Cruz Biotechnology, Carpinteria, CA), and mouse monoclonal
IgG specific for CD34 (dilution 1:50; DakoCytomation, Carpinteria,
CA). Histofine Simple Stain Max PO (Multi, Tokyo, Japan) was used
as a secondary antibody (Nichirei, Tokyo, Japan). The negative
controls were substituting mouse (for mAb) or rabbit (for poly Ab)
non-immune IgG for the primary antibody and omitting the primary
antibody in the staining protocol. The positive controls were the
prostate cancer with positive expressions of AEG-1, VEGF, and CD34.
Evaluation of AEG-1 Immunohistochemistry
AEG-1 and VEGF staining were mainly localized in the cytoplasm
in the vast majority of cancer tissues. Staining for AEG-1 and VEGF
was assessed in a series of randomly selected 10 high-power fields, and
they were believed to be representative of the average in tumors at
400� magnification. The sections were scored by combining the
proportion and intensity of positively stained tumor cells [23,24,38].
The proportion of positively stained tumor cells was scored as follows:
0 (no positive tumor cells), 1 (<10% positive tumor cells), 2 (10–50%
positive tumor cells), and 3 (>50% positive tumor cells). Staining
intensity was classified according to the following criteria: 0 (no
staining); 1 (weak staining¼ light yellow), 2 (moderate staining¼yellow brown), and 3 (strong staining¼ brown).
Staining index (SI) was calculated as the staining intensity
score� the proportion score. Using this method, we evaluated the
expressions of AEG-1 and VEGF in triple-negative breast cancer
specimens by determining the SI, with scores 0, 1, 2, 3, 4, 6, or 9. AEG-
1 and VEGF cut-off values were based on measuring heterogeneity by
the log-rank test with regard to OS. The SI score of 4 (a cut-off point)
was used to distinguish between low and high expression of AEG-1
and VEGF.
Assessment of the staining was scored independently by two
investigators (Q.J.X: Qiuju Xu; J.B.: Jing Bai) without knowledge of
the clinicopathological findings. The scoring staining and allocation of
tumors by the two investigators were similar. Cases with discrepancies
were re-reviewed simultaneously by the original two pathologists and a
senior pathologist until a consensus was reached.
Western Blotting
Total tissue proteins from frozen triple-negative breast cancer
tissues that had different expression levels of VEGF and MVD were
extracted by suspending in a lysis buffer consisting of 20 mM Tris–
HCl (pH 7.5), 2 mM EDTA, 150 mM NaCl, 1% Triton X-100, and
protease inhibitors. These tissues were from tissue sample reservoir in
our department, which was established this year. The selection of these
tissues was similar to the criterion of selected specimens from 125
patients with triple-negative breast cancers. Total tissue proteins from
frozen triple-negative breast cancer tissues (n¼ 12) that had different
expression levels of VEGF and MVD were harvested from patients
with triple-negative breast cancer. These frozen tissues were from
tissue sample reservoir in our department. The selection of these
tissues was similar to the criterion of selected specimens from 125
patients with triple-negative breast cancers. Then, we classified
VEGF�MVD�low tissues (n¼ 3), VEGF�high tissues (n¼ 3),
MVD�high tissues (n¼ 3) and VEGF�MVD�high tissues (n¼ 3)
for our further Western blot analysis. Using the bicinchoninic acid
protein assay kit, protein concentrations were quantified, and 30 mg of
protein per sample was separated onto a denaturing polyacrylamide gel
containing SDS and transferred to a methanol-activated nitrocellulose
filter membrane (Bio-Rad, Carpinteria, CA). Before immunodetection,
membranes were blocked within 5% non-fat dry milk. Primary
antibodies, anti-AEG-1 (1:400; rabbit polyclonal; Proteintech Group),
anti-VEGF (1:200; Santa Cruz Biotechnology), and anti-CD34 (1:50;
DakoCytomation), were diluted in the buffer and incubated at 48Covernight. After being subsequently washed with TBST, membranes
were incubated with secondary antibody (horseradish peroxidase
conjugated anti-rabbit) for 1 h at room temperature. The experiment
was repeated in triplicate. The bands were detected by enhanced
chemiluminescence detection reagents (Applygen Technologies Inc.,
Beijing, China).
Quantification of Microvasculature Density
Microvascular profiles identified by CD34 staining were performed
as described by Weidner et al. [39][40]. Any brown stained cells or cell
clusters that had been clearly separated from adjacent microvessels
were considered a single, countable microvessel. Undefined endothe-
lial cells that appeared to be fragments were not counted as micro-
vessels. Branching structures were counted as single vessel unless there
was a break in continuity of the structure. A visible vascular lumen was
not required to count as a microvessel [41]. Subsequent to immuno-
staining, the entire section was scanned at low power (40� and 100�)
to identify the hot spots, which represented the highest vascular density
(so called ‘‘hot spot’’). The microvessel count was determined by
counting the number of CD34-positive vessels in three separate hot
spots at a still higher magnification (200�, 0.4-mm2 per field area).
The mean value of the CD34-positive vessel counts in the three
selected hot spots per section was then calculated. They were then
taken as the MVD of the tumor. The median MVD (value 76) of all
patients was used to classify patients in high and low MVD groups. All
counts were performed by a pathologist who did not know the clinical
data. Figure 2E showed a representative field of high MVD in triple-
negative breast cancers. For comparison, Figure 2F depicted a
representative field of triple-negative breast cancers with low MVD.
Statistical Analysis
All data were analyzed by statistics software (SPSS 13.0 for
Windows; SPSS, Inc., Chicago, IL). Analyzed variables included age,
tumor size, histological type, depth of invasion, lymph node status,
venous and lymphatic invasion, TNM stage, and expressions of Ki67,
p53, AEG-1, VEGF, and CD34. The correlation between expressions
of Ki67, p53, AEG-1, VEGF, and CD34, and the other variables was
assessed with the chi-square and Fisher exact tests. Bivariate
correlations between two independent variables were analyzed by
calculating the Spearman’s correlation coefficients. Survival analysis
was performed using the Kaplan–Meier method and compared by the
log-rank test. Prognostic relevance was evaluated by multivariate Cox
regression analysis. P< 0.05 was considered as significant.
RESULTS
Expression of AEG-1, VEGF, and MVD in
Triple-Negative Breast Cancer
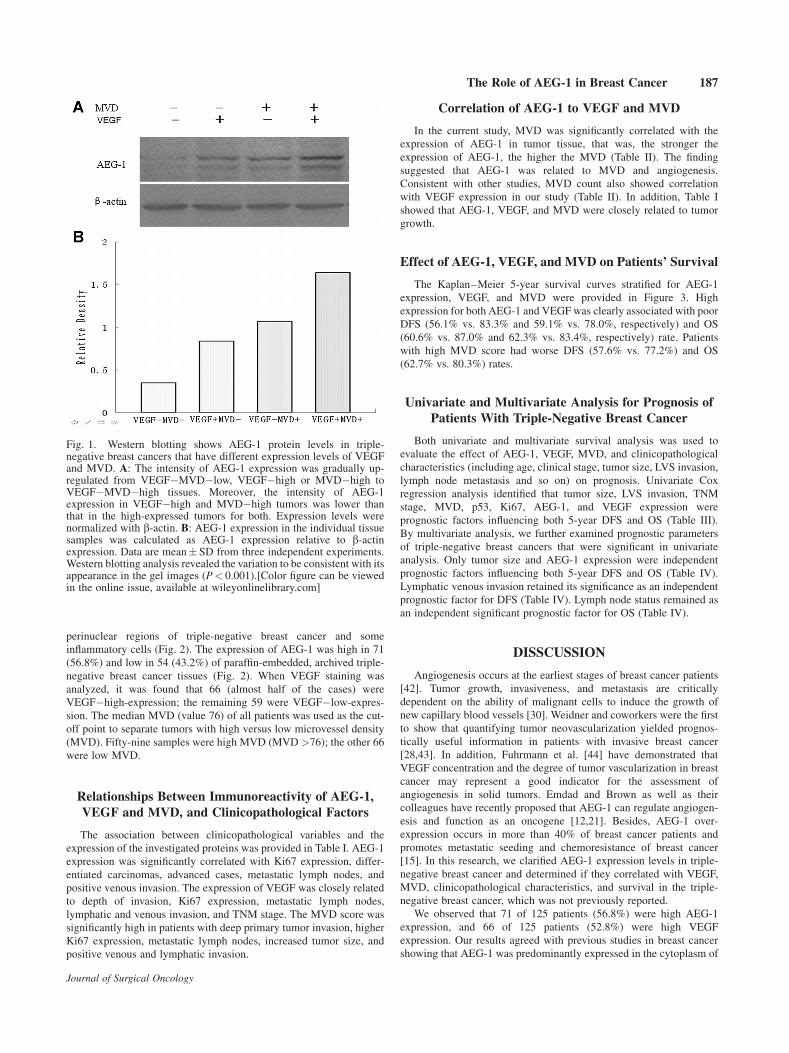
The intensity of AEG-1 expression was gradually elevated from
VEGF�MVD�low tissues to VEGF�high or MVD�high tissues
using Western blot analysis. In addition, AEG-1 expression in
VEGF�high and MVD�high tumors was lower than that in the
high-expressed tumors for both (Fig. 1).
Immunoreactivity for both AEG-1 and VEGF proteins was shown
as brown color and presented diffusely or focally in the cytosolic and
Journal of Surgical Oncology
186 Li et al.
perinuclear regions of triple-negative breast cancer and some
inflammatory cells (Fig. 2). The expression of AEG-1 was high in 71
(56.8%) and low in 54 (43.2%) of paraffin-embedded, archived triple-
negative breast cancer tissues (Fig. 2). When VEGF staining was
analyzed, it was found that 66 (almost half of the cases) were
VEGF�high-expression; the remaining 59 were VEGF�low-expres-
sion. The median MVD (value 76) of all patients was used as the cut-
off point to separate tumors with high versus low microvessel density
(MVD). Fifty-nine samples were high MVD (MVD >76); the other 66
were low MVD.
Relationships Between Immunoreactivity of AEG-1,
VEGF and MVD, and Clinicopathological Factors
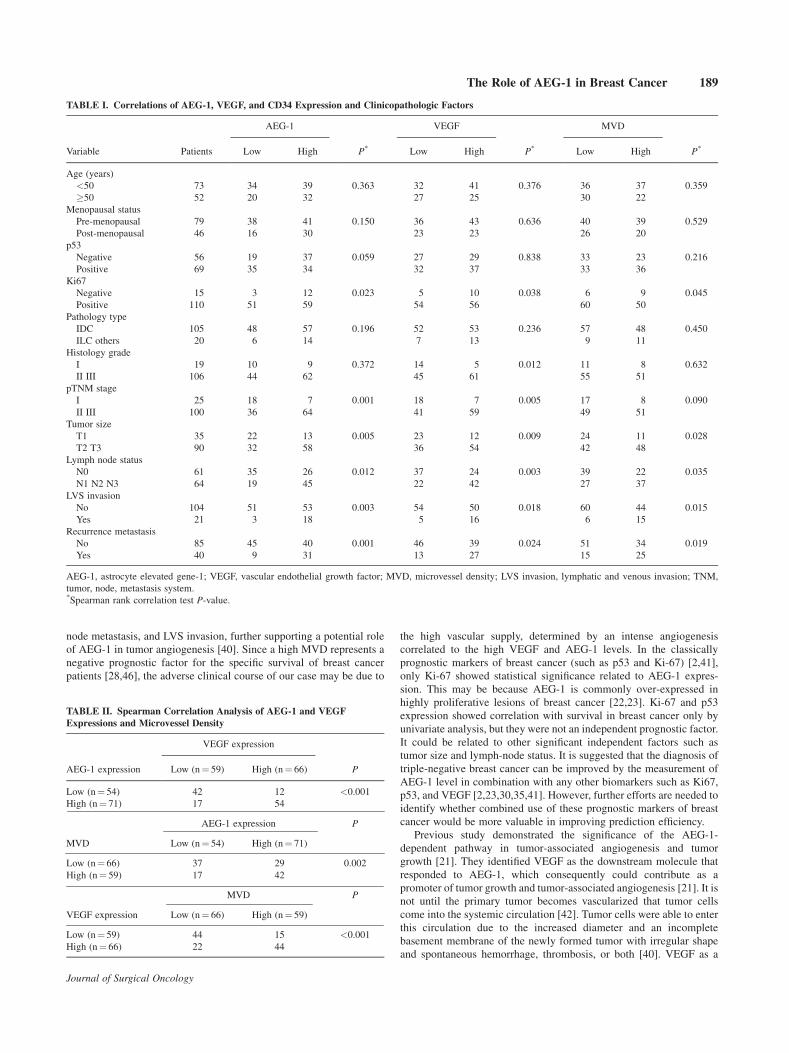
The association between clinicopathological variables and the
expression of the investigated proteins was provided in Table I. AEG-1
expression was significantly correlated with Ki67 expression, differ-
entiated carcinomas, advanced cases, metastatic lymph nodes, and
positive venous invasion. The expression of VEGF was closely related
to depth of invasion, Ki67 expression, metastatic lymph nodes,
lymphatic and venous invasion, and TNM stage. The MVD score was
significantly high in patients with deep primary tumor invasion, higher
Ki67 expression, metastatic lymph nodes, increased tumor size, and
positive venous and lymphatic invasion.
Correlation of AEG-1 to VEGF and MVD
In the current study, MVD was significantly correlated with the
expression of AEG-1 in tumor tissue, that was, the stronger the
expression of AEG-1, the higher the MVD (Table II). The finding
suggested that AEG-1 was related to MVD and angiogenesis.
Consistent with other studies, MVD count also showed correlation
with VEGF expression in our study (Table II). In addition, Table I
showed that AEG-1, VEGF, and MVD were closely related to tumor
growth.
Effect of AEG-1, VEGF, and MVD on Patients’ Survival
The Kaplan–Meier 5-year survival curves stratified for AEG-1
expression, VEGF, and MVD were provided in Figure 3. High
expression for both AEG-1 and VEGF was clearly associated with poor
DFS (56.1% vs. 83.3% and 59.1% vs. 78.0%, respectively) and OS
(60.6% vs. 87.0% and 62.3% vs. 83.4%, respectively) rate. Patients
with high MVD score had worse DFS (57.6% vs. 77.2%) and OS
(62.7% vs. 80.3%) rates.
Univariate and Multivariate Analysis for Prognosis of
Patients With Triple-Negative Breast Cancer
Both univariate and multivariate survival analysis was used to
evaluate the effect of AEG-1, VEGF, MVD, and clinicopathological
characteristics (including age, clinical stage, tumor size, LVS invasion,
lymph node metastasis and so on) on prognosis. Univariate Cox
regression analysis identified that tumor size, LVS invasion, TNM
stage, MVD, p53, Ki67, AEG-1, and VEGF expression were
prognostic factors influencing both 5-year DFS and OS (Table III).
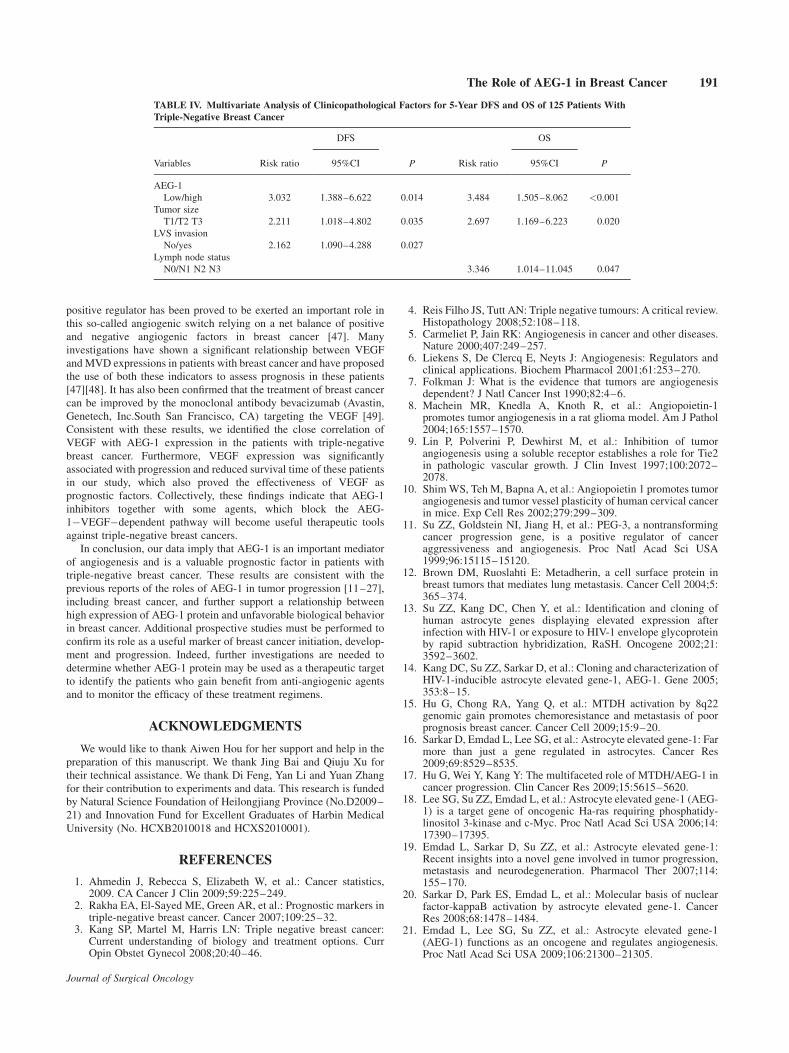
By multivariate analysis, we further examined prognostic parameters
of triple-negative breast cancers that were significant in univariate
analysis. Only tumor size and AEG-1 expression were independent
prognostic factors influencing both 5-year DFS and OS (Table IV).
Lymphatic venous invasion retained its significance as an independent
prognostic factor for DFS (Table IV). Lymph node status remained as
an independent significant prognostic factor for OS (Table IV).
DISSCUSSION
Angiogenesis occurs at the earliest stages of breast cancer patients
[42]. Tumor growth, invasiveness, and metastasis are critically
dependent on the ability of malignant cells to induce the growth of
new capillary blood vessels [30]. Weidner and coworkers were the first
to show that quantifying tumor neovascularization yielded prognos-
tically useful information in patients with invasive breast cancer
[28,43]. In addition, Fuhrmann et al. [44] have demonstrated that
VEGF concentration and the degree of tumor vascularization in breast
cancer may represent a good indicator for the assessment of
angiogenesis in solid tumors. Emdad and Brown as well as their
colleagues have recently proposed that AEG-1 can regulate angiogen-
esis and function as an oncogene [12,21]. Besides, AEG-1 over-
expression occurs in more than 40% of breast cancer patients and
promotes metastatic seeding and chemoresistance of breast cancer
[15]. In this research, we clarified AEG-1 expression levels in triple-
negative breast cancer and determined if they correlated with VEGF,
MVD, clinicopathological characteristics, and survival in the triple-
negative breast cancer, which was not previously reported.
We observed that 71 of 125 patients (56.8%) were high AEG-1
expression, and 66 of 125 patients (52.8%) were high VEGF
expression. Our results agreed with previous studies in breast cancer
showing that AEG-1 was predominantly expressed in the cytoplasm of
Journal of Surgical Oncology
Fig. 1. Western blotting shows AEG-1 protein levels in triple-negative breast cancers that have different expression levels of VEGFand MVD. A: The intensity of AEG-1 expression was gradually up-regulated from VEGF�MVD�low, VEGF�high or MVD�high toVEGF�MVD�high tissues. Moreover, the intensity of AEG-1expression in VEGF�high and MVD�high tumors was lower thanthat in the high-expressed tumors for both. Expression levels werenormalized with b-actin. B: AEG-1 expression in the individual tissuesamples was calculated as AEG-1 expression relative to b-actinexpression. Data are mean� SD from three independent experiments.Western blotting analysis revealed the variation to be consistent with itsappearance in the gel images (P< 0.001).[Color figure can be viewedin the online issue, available at wileyonlinelibrary.com]
The Role of AEG-1 in Breast Cancer 187

breast cancer cells [15,23,24]. Employing Western blot, we found that
the intensity of AEG-1 expression is significantly higher in
VEGF�MVD�high cases than that in VEGF�MVD�low cases.
The AEG-1 protein levels of VEGF�high and MVD�high tumors
were higher than those of VEGF�MVD�low tumors. A statistically
significant correlation was found between high AEG-1 expression and
tumor size in our research. A similar relationship was found between
the number of newly formed vessels and the size of triple-negative
breast cancers, confirming Folkman’s theory that tumor size was
restricted to a few cubic millimeters in the absence of neovasculariza-
tion [40]. With clinical experience, the size of a malignant tumor
represented a classic prognostic indicator in breast cancer patients [45].
The results of our study revealed that, along with the size of the tumor,
increased AEG-1 expression was an independent prognostic factor
influencing both 5-year DFS and OS. Though tumor size was an
additional predictor of DFS and OS, the prognostic impact was
statistically inferior to AEG-1 expression in the univariate and
multivariate analysis. Moreover, we demonstrated that AEG-1-high
patients had lower OS and DFS rates as compared with AEG-1-low
patients. From these results, it can be seen that AEG-1 may become a
valuable predictor for prognosis and survival among triple-negative
breast cancer patients.
Our clinical studies demonstrated positive correlation of AEG-1
expression with increased MVD, greater metastatic potential and a
poor outcome in triple-negative breast cancer patients. High AEG-1
expression was also previously found in patients with breast cancer
[24]. However, the relationship between AEG-1 expression and MVD
in breast cancer has not been previously characterized. Tumor
angiogenesis in invasive breast cancer was quantitated by MVD,
which was also a crucial factor for the assessment of this tumor
prognosis [28]. There was confirmed evidence that antibody against
CD34 in the assessment of MVD was particularly reliable, so we
adopted CD34 immunostaining to assess MVD in our study [39,40].
High MVD was associated with elevated risk of metastasis and shorter
survival in solid tumors including breast cancer [28]. Based on these
reports, we investigated the association of AEG-1 expression with
MVD and looked at its correlation with prognosis in breast cancer. We
revealed that AEG-1 expression was significantly correlated with
MVD and disease prognosis. On the basis of above studies, we indicate
that AEG-1 may play a crucial part in angiogenesis, which is an
essential component in breast cancer development, growth, and
progression to metastasis. Statistic analysis of the relationship between
AEG-1 staining and the clinical characteristics of patients presented a
significant correlation of AEG-1 expression with clinical stage, lymph
Journal of Surgical Oncology
Fig. 2. Immunohistochemical staining of AEG-1, VEGF, and CD34 in triple-negative breast cancer tissues. A: high AEG-1 expression (B) lowAEG-1 expression (C) high VEGF expression (D) low VEGF expression (E) CD34-positive endothelial cells of blood vessels in high MVD area,the mean MVD was 84.25 in this sample (F) CD34-positive endothelial cells of blood vessels in low MVD area, the mean MVD was 45.66 in thissample. Original magnification, 200� (A–F).[Color figure can be viewed in the online issue, available at wileyonlinelibrary.com]
188 Li et al.
node metastasis, and LVS invasion, further supporting a potential role
of AEG-1 in tumor angiogenesis [40]. Since a high MVD represents a
negative prognostic factor for the specific survival of breast cancer
patients [28,46], the adverse clinical course of our case may be due to
the high vascular supply, determined by an intense angiogenesis
correlated to the high VEGF and AEG-1 levels. In the classically
prognostic markers of breast cancer (such as p53 and Ki-67) [2,41],
only Ki-67 showed statistical significance related to AEG-1 expres-
sion. This may be because AEG-1 is commonly over-expressed in
highly proliferative lesions of breast cancer [22,23]. Ki-67 and p53
expression showed correlation with survival in breast cancer only by
univariate analysis, but they were not an independent prognostic factor.
It could be related to other significant independent factors such as
tumor size and lymph-node status. It is suggested that the diagnosis of
triple-negative breast cancer can be improved by the measurement of
AEG-1 level in combination with any other biomarkers such as Ki67,
p53, and VEGF [2,23,30,35,41]. However, further efforts are needed to
identify whether combined use of these prognostic markers of breast
cancer would be more valuable in improving prediction efficiency.
Previous study demonstrated the significance of the AEG-1-
dependent pathway in tumor-associated angiogenesis and tumor
growth [21]. They identified VEGF as the downstream molecule that
responded to AEG-1, which consequently could contribute as a
promoter of tumor growth and tumor-associated angiogenesis [21]. It is
not until the primary tumor becomes vascularized that tumor cells
come into the systemic circulation [42]. Tumor cells were able to enter
this circulation due to the increased diameter and an incomplete
basement membrane of the newly formed tumor with irregular shape
and spontaneous hemorrhage, thrombosis, or both [40]. VEGF as a
Journal of Surgical Oncology
TABLE I. Correlations of AEG-1, VEGF, and CD34 Expression and Clinicopathologic Factors
Variable Patients
AEG-1
P*
VEGF
P*
MVD
P*Low High Low High Low High
Age (years)
<50 73 34 39 0.363 32 41 0.376 36 37 0.359
�50 52 20 32 27 25 30 22
Menopausal status
Pre-menopausal 79 38 41 0.150 36 43 0.636 40 39 0.529
Post-menopausal 46 16 30 23 23 26 20
p53
Negative 56 19 37 0.059 27 29 0.838 33 23 0.216
Positive 69 35 34 32 37 33 36
Ki67
Negative 15 3 12 0.023 5 10 0.038 6 9 0.045
Positive 110 51 59 54 56 60 50
Pathology type
IDC 105 48 57 0.196 52 53 0.236 57 48 0.450
ILC others 20 6 14 7 13 9 11
Histology grade
I 19 10 9 0.372 14 5 0.012 11 8 0.632
II III 106 44 62 45 61 55 51
pTNM stage
I 25 18 7 0.001 18 7 0.005 17 8 0.090
II III 100 36 64 41 59 49 51
Tumor size
T1 35 22 13 0.005 23 12 0.009 24 11 0.028
T2 T3 90 32 58 36 54 42 48
Lymph node status
N0 61 35 26 0.012 37 24 0.003 39 22 0.035
N1 N2 N3 64 19 45 22 42 27 37
LVS invasion
No 104 51 53 0.003 54 50 0.018 60 44 0.015
Yes 21 3 18 5 16 6 15
Recurrence metastasis
No 85 45 40 0.001 46 39 0.024 51 34 0.019
Yes 40 9 31 13 27 15 25
AEG-1, astrocyte elevated gene-1; VEGF, vascular endothelial growth factor; MVD, microvessel density; LVS invasion, lymphatic and venous invasion; TNM,
tumor, node, metastasis system.*Spearman rank correlation test P-value.
TABLE II. Spearman Correlation Analysis of AEG-1 and VEGF
Expressions and Microvessel Density
AEG-1 expression
VEGF expression
PLow (n¼ 59) High (n¼ 66)
Low (n¼ 54) 42 12 <0.001
High (n¼ 71) 17 54
MVD
AEG-1 expression P
Low (n¼ 54) High (n¼ 71)
Low (n¼ 66) 37 29 0.002
High (n¼ 59) 17 42
VEGF expression
MVD P
Low (n¼ 66) High (n¼ 59)
Low (n¼ 59) 44 15 <0.001
High (n¼ 66) 22 44
The Role of AEG-1 in Breast Cancer 189

Journal of Surgical Oncology
TABLE III. Univariate Analysis of Clinicopathological Factors for 5-Year DFS and OS of 125 Patients With Triple-Negative Breast Cancer
Variables Risk ratio
DFS
P Risk ratio
OS
P95%CI 95%CI
Age (years)
<50/�50 1.054 0.563–1.972 0.870 1.354 0.698–2.628 0.370
Menopausal status
Pre-menopausal/post-menopausal 0.938 0.490–1.797 0.847 1.167 0.593–2.295 0.654
p53
Negative/positive 2.527 1.281–0.987 0.015 3.539 1.275–8.051 0.020
Ki67
Negative/positive 2.318 1.432–7.987 0.026 3.156 2.485–6.531 0.038
Pathology type
IDC/ILC others 0.926 0.389–2.205 0.862 0.875 0.339–2.255 0.782
Histology grade
I/II III 2.652 0.818–8.606 0.104 3.498 0.839–14.584 0.086
pTNM stage
I/II III 3.810 1.174–12.364 0.026 4.972 1.193–20.730 0.028
Tumor size
T1/T2 T3 4.441 1.579–12.487 0.005 5.128 1.569–16.759 0.007
Lymph node status
N0/N1 N2 N3 4.308 2.048–9.064 0.0263 4.800 2.094–11.003 0.013
LVS invasion
No/yes 3.872 2.036–7.363 0.015 3.184 1.583–6.407 0.001
AEG-1
Low/high 3.299 1.569–6.935 0.002 3.761 1.642–8.617 <0.001
VEGF
Low/high 2.148 1.108–4.166 0.024 2.525 1.212–5.258 0.013
MVD
Low/high 2.090 1.101–3.966 0.024 2.052 1.034–4.075 0.040
Fig. 3. A–C: Five-year DFS, and (D–F) OS curves of patients with triple-negative breast cancer according to the AEG-1, VEGF, and CD34immunostaining.[Color figure can be viewed in the online issue, available at wileyonlinelibrary.com]
190 Li et al.
positive regulator has been proved to be exerted an important role in
this so-called angiogenic switch relying on a net balance of positive
and negative angiogenic factors in breast cancer [47]. Many
investigations have shown a significant relationship between VEGF
and MVD expressions in patients with breast cancer and have proposed
the use of both these indicators to assess prognosis in these patients
[47][48]. It has also been confirmed that the treatment of breast cancer
can be improved by the monoclonal antibody bevacizumab (Avastin,
Genetech, Inc.South San Francisco, CA) targeting the VEGF [49].
Consistent with these results, we identified the close correlation of
VEGF with AEG-1 expression in the patients with triple-negative
breast cancer. Furthermore, VEGF expression was significantly
associated with progression and reduced survival time of these patients
in our study, which also proved the effectiveness of VEGF as
prognostic factors. Collectively, these findings indicate that AEG-1
inhibitors together with some agents, which block the AEG-
1�VEGF�dependent pathway will become useful therapeutic tools
against triple-negative breast cancers.
In conclusion, our data imply that AEG-1 is an important mediator
of angiogenesis and is a valuable prognostic factor in patients with
triple-negative breast cancer. These results are consistent with the
previous reports of the roles of AEG-1 in tumor progression [11–27],
including breast cancer, and further support a relationship between
high expression of AEG-1 protein and unfavorable biological behavior
in breast cancer. Additional prospective studies must be performed to
confirm its role as a useful marker of breast cancer initiation, develop-
ment and progression. Indeed, further investigations are needed to
determine whether AEG-1 protein may be used as a therapeutic target
to identify the patients who gain benefit from anti-angiogenic agents
and to monitor the efficacy of these treatment regimens.
ACKNOWLEDGMENTS
We would like to thank Aiwen Hou for her support and help in the
preparation of this manuscript. We thank Jing Bai and Qiuju Xu for
their technical assistance. We thank Di Feng, Yan Li and Yuan Zhang
for their contribution to experiments and data. This research is funded
by Natural Science Foundation of Heilongjiang Province (No.D2009–
21) and Innovation Fund for Excellent Graduates of Harbin Medical
University (No. HCXB2010018 and HCXS2010001).
REFERENCES
1. Ahmedin J, Rebecca S, Elizabeth W, et al.: Cancer statistics,2009. CA Cancer J Clin 2009;59:225–249.
2. Rakha EA, El-Sayed ME, Green AR, et al.: Prognostic markers intriple-negative breast cancer. Cancer 2007;109:25–32.
3. Kang SP, Martel M, Harris LN: Triple negative breast cancer:Current understanding of biology and treatment options. CurrOpin Obstet Gynecol 2008;20:40–46.
4. Reis Filho JS, Tutt AN: Triple negative tumours: A critical review.Histopathology 2008;52:108–118.
5. Carmeliet P, Jain RK: Angiogenesis in cancer and other diseases.Nature 2000;407:249–257.
6. Liekens S, De Clercq E, Neyts J: Angiogenesis: Regulators andclinical applications. Biochem Pharmacol 2001;61:253–270.
7. Folkman J: What is the evidence that tumors are angiogenesisdependent? J Natl Cancer Inst 1990;82:4–6.
8. Machein MR, Knedla A, Knoth R, et al.: Angiopoietin-1promotes tumor angiogenesis in a rat glioma model. Am J Pathol2004;165:1557–1570.
9. Lin P, Polverini P, Dewhirst M, et al.: Inhibition of tumorangiogenesis using a soluble receptor establishes a role for Tie2in pathologic vascular growth. J Clin Invest 1997;100:2072–2078.
10. Shim WS, Teh M, Bapna A, et al.: Angiopoietin 1 promotes tumorangiogenesis and tumor vessel plasticity of human cervical cancerin mice. Exp Cell Res 2002;279:299–309.
11. Su ZZ, Goldstein NI, Jiang H, et al.: PEG-3, a nontransformingcancer progression gene, is a positive regulator of canceraggressiveness and angiogenesis. Proc Natl Acad Sci USA1999;96:15115–15120.
12. Brown DM, Ruoslahti E: Metadherin, a cell surface protein inbreast tumors that mediates lung metastasis. Cancer Cell 2004;5:365–374.
13. Su ZZ, Kang DC, Chen Y, et al.: Identification and cloning ofhuman astrocyte genes displaying elevated expression afterinfection with HIV-1 or exposure to HIV-1 envelope glycoproteinby rapid subtraction hybridization, RaSH. Oncogene 2002;21:3592–3602.
14. Kang DC, Su ZZ, Sarkar D, et al.: Cloning and characterization ofHIV-1-inducible astrocyte elevated gene-1, AEG-1. Gene 2005;353:8–15.
15. Hu G, Chong RA, Yang Q, et al.: MTDH activation by 8q22genomic gain promotes chemoresistance and metastasis of poorprognosis breast cancer. Cancer Cell 2009;15:9–20.
16. Sarkar D, Emdad L, Lee SG, et al.: Astrocyte elevated gene-1: Farmore than just a gene regulated in astrocytes. Cancer Res2009;69:8529–8535.
17. Hu G, Wei Y, Kang Y: The multifaceted role of MTDH/AEG-1 incancer progression. Clin Cancer Res 2009;15:5615–5620.
18. Lee SG, Su ZZ, Emdad L, et al.: Astrocyte elevated gene-1 (AEG-1) is a target gene of oncogenic Ha-ras requiring phosphatidy-linositol 3-kinase and c-Myc. Proc Natl Acad Sci USA 2006;14:17390–17395.
19. Emdad L, Sarkar D, Su ZZ, et al.: Astrocyte elevated gene-1:Recent insights into a novel gene involved in tumor progression,metastasis and neurodegeneration. Pharmacol Ther 2007;114:155–170.
20. Sarkar D, Park ES, Emdad L, et al.: Molecular basis of nuclearfactor-kappaB activation by astrocyte elevated gene-1. CancerRes 2008;68:1478–1484.
21. Emdad L, Lee SG, Su ZZ, et al.: Astrocyte elevated gene-1(AEG-1) functions as an oncogene and regulates angiogenesis.Proc Natl Acad Sci USA 2009;106:21300–21305.
Journal of Surgical Oncology
TABLE IV. Multivariate Analysis of Clinicopathological Factors for 5-Year DFS and OS of 125 Patients With
Triple-Negative Breast Cancer
Variables Risk ratio
DFS
P Risk ratio
OS
P95%CI 95%CI
AEG-1
Low/high 3.032 1.388–6.622 0.014 3.484 1.505–8.062 <0.001
Tumor size
T1/T2 T3 2.211 1.018–4.802 0.035 2.697 1.169–6.223 0.020
LVS invasion
No/yes 2.162 1.090–4.288 0.027
Lymph node status
N0/N1 N2 N3 3.346 1.014–11.045 0.047
The Role of AEG-1 in Breast Cancer 191

22. Li J, Yang L, Song L, et al.: Astrocyte elevated gene-1 is aproliferation promoter in breast cancer via suppressing transcrip-tional factor FOXO1. Oncogene 2009;28:3188–3196.
23. Su P, Zhang Q, Yang Q: Immunohistochemical analysis ofmetadherin in proliferative and cancerous breast tissue. DiagnPathol 2010;5:38.
24. Li J, Zhang N, Song LB, et al.: Astrocyte elevated gene-1is a novel prognostic marker for breast cancer progressionand overall patient survival. Clin Cancer Res 2008;14:3319–3326.
25. Yoo BK, Emdad L, Su ZZ, et al.: Astrocyte elevated gene-1regulates hepatocellular carcinoma development and progression.J Clin Invest 2009;119:465–477.
26. Yu C, Chen K, Zheng H, et al.: Overexpression of astrocyteelevated gene-1 (aeg-1) is associated with esophageal squamouscell carcinoma (ESCC) progression and pathogenesis. Carcino-genesis 2009;30:894–901.
27. Toi M, Hoshina S, Takayanagi T, et al.: Association of vascularendothelial growth factor expression with tumor angiogenesis andearly response in primary breast cancer. Jpn J Cancer Res 1994;85:1045–1049.
28. Hansen S, Grabau DA, Sorensen FB, et al.: Vascular grading ofangiogenesis: Prognostic significance in breast cancer. Br JCancer 2000;82:339–347.
29. Breier G: Functions of the VEGF/VEGF receptor system inthe vascular system. Semin Thromb Hemost 2000;26:553–559.
30. Esteva FJ, Hortobagyi GN: Prognostic molecular markers in earlybreast cancer. Breast Cancer Res 2004;6:109–118.
31. Ferrara N: Molecular and biological properties of vascularendothelial growth factor. J Mol Med 1999;77:527–543.
32. Hoeben A, Landuyt B, Highley MS, et al.: Vascular endothelialgrowth factor and angiogenesis. Pharmacol Rev 2004;56:549–580.
33. Morabito A, Sarmiento R, Bonginelli P, et al.: Antiangiogenicstrategies, compounds, and early clinical results in breast cancer.Crit Rev Oncol Hematol 2004;49:91–107.
34. Nagy JA, Vasile E, Feng D, et al.: Vascular permeability factor/vascular endothelial growth factor induces lymphangiogenesis aswell as angiogenesis. J Exp Med 2002;96:1497–1506.
35. Le Doussal V, Tubiana-Hulin M, Friedman S, et al.: Prognosticvalue of histologic grade nuclear components of Scarff-Bloom-Richardson (SBR): An improved score modification based on amultivariate analysis of 1262 invasive ductal breast carcinomas.Cancer 1989;64:1914–1921.
36. Greene FI, Page DI, Fleming ID: AJCC cancer staging manual,6th edn. New York: Springer; 2002.
37. Birner P, Oberhuber G, Stani J, et al.: Evaluation of the UnitedStates Food and Drug Administration-approved scoring and testsystem of HER-2 protein expression in breast cancer. Clin CancerRes 2001;7:1669–1975.
38. Song H, Li C, Li R, et al.: Prognostic significance of AEG-1expression in colorectal carcinoma. Int J Colorectal Dis 2010;25:1201–1209.
39. Vermeulen PB, Gasparini G, Fox SB, et al.: Quantification ofangiogenesis in solid human tumors: An international consensuson the methodology and criteria of evaluation. Eur J Cancer1996;32:2474–2484.
40. Weidner N, Semple JP, Welch WR, et al.: Tumor angiogenesis andmetastasis—correlation in invasive breast carcinoma. N Engl JMed 1991;324:1–8.
41. Tas F, Yavuz E, Aydiner A, et al.: Angiogenesis and p53 proteinexpression in breast cancer: Prognostic roles and interrelation-ships. Am J Clin Oncol 2000;23:546–553.
42. Schneider BP, Miller KD: Angiogenesis of breast cancer. J ClinOncol 2005;23:1782–1790.
43. Guidi AJ, Berry DA, Broadwater G, et al.: Association ofangiogenesis and disease outcome in node-positive breast cancerpatients treated with adjuvant cyclophosphamide, doxorubicin,and fluorouracil: A Cancer and Leukemia Group B correlativescience study from protocols 8541/8869. J Clin Oncol 2002;20:732–742.
44. Fuhrmann-Benzakein H, Ma HN, Rubba-Brandt L: Elevatedlevels of angiogenic cytokines in the plasma of cancer patients. IntJ Cancer 2000;1:40–45.
45. Ogawa Y, Chung YS, Nakata B, et al.: Microvessel quantitation ininvasive breast cancer by staining for factor VIII related antigen.Br J Cancer 1995;71:1297–1301.
46. Heimann R, Ferguson D, Powers C, et al.: Angiogenesis as apredictor of long-term survival for patients with node-negativebreast cancer. J Natl Cancer Inst 1996;88:1764–1769.
47. Toi M, Inada K, Suzuki H, et al.: Tumor angiogenesis in breastcancer: Its importance as a prognostic indicator and theassociation with vascular endothelial growth factor expression.Breast Cancer Res Treat 1995;36:193–204.
48. Li J, Song ST, Jiang ZF, et al.: Significance of microvasculardensity and vascular endothelial growth factor in breast cancer.Anticancer Res 2002;22:1925–1928.
49. Kerr DG: Targeting angiogenesis in cancer: Clinical developmentof bevacizumab. Nat Clin Pract Oncol 2004;1:39–43.
Journal of Surgical Oncology
192 Li et al.