setting the stage contextcontext - denver, colorado · first slide tracheoplasty on a baby with...
TRANSCRIPT

Acquired Subglottic StenosisAcquired Subglottic Stenosis
Michael J. Rutter, FRACSDepartment of Pediatric Otolaryngology-
Head & Neck SurgeryAerodigestive and Esophageal Center
Cincinnati Children’s Hospital Medical CenterCincinnati, Ohio
Michael J. Rutter, FRACSDepartment of Pediatric Otolaryngology-
Head & Neck SurgeryAerodigestive and Esophageal Center
Cincinnati Children’s Hospital Medical CenterCincinnati, Ohio
IPSADenver, CO
June 2nd 2016
Disclosure InformationDisclosure Information• Formerly scientific advisory board:
• Acclarent Medical• Airway balloon dilator
• Consultant / Patent holder• Bryan Medical – Aeris balloon dilator
• Consultant (no financial relationship)• Boston Medical Products
• Suprastomal stent
• And I also use many products off-label!
• Formerly scientific advisory board:• Acclarent Medical
• Airway balloon dilator
• Consultant / Patent holder• Bryan Medical – Aeris balloon dilator
• Consultant (no financial relationship)• Boston Medical Products
• Suprastomal stent
• And I also use many products off-label!
Setting the StageSetting the Stage
• Before the 1970s endoscopic surgery was the mainstay of airway surgery • Mainly bouginage dilation
• 1970s – 2000 open airway surgery predominated• Expansion grafting and resection
• 21st century a resurgence of interest in endoscopic surgery• Often complimenting open surgery
• Before the 1970s endoscopic surgery was the mainstay of airway surgery • Mainly bouginage dilation
• 1970s – 2000 open airway surgery predominated• Expansion grafting and resection
• 21st century a resurgence of interest in endoscopic surgery• Often complimenting open surgery
ContextContext
• I enjoy open airway surgery• In 2010:
• LTRs 28• CTRs 6• Clefts 4• Slides 20
• I enjoy open airway surgery• In 2010:
• LTRs 28• CTRs 6• Clefts 4• Slides 20
ContextContext
• I am also an endoscopic airway surgeon• Since 2001
• Balloon dilations > 2700
• Cleft > 25
• TEF > 18
• Glottic web > 8
• Posterior grafts > 10
• I am also an endoscopic airway surgeon• Since 2001
• Balloon dilations > 2700
• Cleft > 25
• TEF > 18
• Glottic web > 8
• Posterior grafts > 10
2016 - Trends2016 - Trends
• Evolution, both of operative techniques, and the patients themselves
• Collaboration
• Pre-operative evaluation and optimization
• New tools
• Endoscopic techniques compliment open reconstructive techniques
• Evolution, both of operative techniques, and the patients themselves
• Collaboration
• Pre-operative evaluation and optimization
• New tools
• Endoscopic techniques compliment open reconstructive techniques
Rutter, Michael, MD Acquired Subglottic Stenosis

Optimization and EvaluationOptimization and Evaluation
• Airway surgery may be challenging and risky• Revision surgery especially
• Pre-operative evaluation, patient optimization, and team collaboration improves outcomes• Not just airway, but voice,
aspiration, etc
• Airway surgery may be challenging and risky• Revision surgery especially
• Pre-operative evaluation, patient optimization, and team collaboration improves outcomes• Not just airway, but voice,
aspiration, etc
STATE OF THE ARTEvaluation, Collaboration, Optimization
STATE OF THE ARTEvaluation, Collaboration, Optimization
• Team Approach
• ADEC evaluation
• Triple scope• Pulmonary
• ORL
• GI• Reflux
• Eosinophilic Esophagitis
• Team Approach
• ADEC evaluation
• Triple scope• Pulmonary
• ORL
• GI• Reflux
• Eosinophilic Esophagitis
AERODIGESTIVE AND ESOPHAGEAL CENTERAERODIGESTIVE AND
ESOPHAGEAL CENTER
TEAM APPROACH
Reconstruction OptionsReconstruction Options
• Endoscopic techniques
• Expansion• Anterior cricoid split
• Anterior cartilage graft
• Posterior cartilage graft
• Anterior / posterior cartilage grafts
• Resection• Cricotracheal resection
• Endoscopic techniques
• Expansion• Anterior cricoid split
• Anterior cartilage graft
• Posterior cartilage graft
• Anterior / posterior cartilage grafts
• Resection• Cricotracheal resection
Graft MaterialsGraft Materials
• Costal Cartilage • The workhorse
• Thyroid alar cartilage• Auricular cartilage• Other
• Nasal septum• Hyoid• Clavicular periosteum• Buccal
• Costal Cartilage • The workhorse
• Thyroid alar cartilage• Auricular cartilage• Other
• Nasal septum• Hyoid• Clavicular periosteum• Buccal
Stenting OptionsStenting Options
• Nil
• Single stage - extubate on table
• Single stage - endotracheal tube
• T-Tube
• Suprastomal stent
• (Wired in full length stent)
• Nil
• Single stage - extubate on table
• Single stage - endotracheal tube
• T-Tube
• Suprastomal stent
• (Wired in full length stent)
Rutter, Michael, MD Acquired Subglottic Stenosis

What We have LearnedWhat We have Learned
• Risk factors for failure:• MRSA
• The “Active” larynx
• Causes of an active larynx• Reflux
• Eosinophilic esophagitis
• Unknown• Zithromax trial?
• Risk factors for failure:• MRSA
• The “Active” larynx
• Causes of an active larynx• Reflux
• Eosinophilic esophagitis
• Unknown• Zithromax trial?
2 Year Old Boy2 Year Old Boy
• 8.5kg, tracheotomy dependent, ex-25 weeker
• LTP declined due to weight
• Mother (a urologist) seeking a second opinion
• 8.5kg, tracheotomy dependent, ex-25 weeker
• LTP declined due to weight
• Mother (a urologist) seeking a second opinion
MLB – Active LarynxMLB – Active Larynx Other Investigations?Other Investigations?
• Impedance probe – NEGATIVE
• Esophagoscopy + biopsies – NEGATIVE
• No reflux, no eosinophilic esophagitis
• What next?
• Impedance probe – NEGATIVE
• Esophagoscopy + biopsies – NEGATIVE
• No reflux, no eosinophilic esophagitis
• What next?
WAITWAIT
• Didn’t work
• Zithromax• Azithromycin, macrolide antibiotic
• Suggested by pulmonology
• Used as an anti-inflammatory drug in cystic fibrosis
• 5 mls (200mg) Monday, Wednesday, Friday
• Didn’t work
• Zithromax• Azithromycin, macrolide antibiotic
• Suggested by pulmonology
• Used as an anti-inflammatory drug in cystic fibrosis
• 5 mls (200mg) Monday, Wednesday, Friday
2 Months Zithromax2 Months Zithromax
Rutter, Michael, MD Acquired Subglottic Stenosis
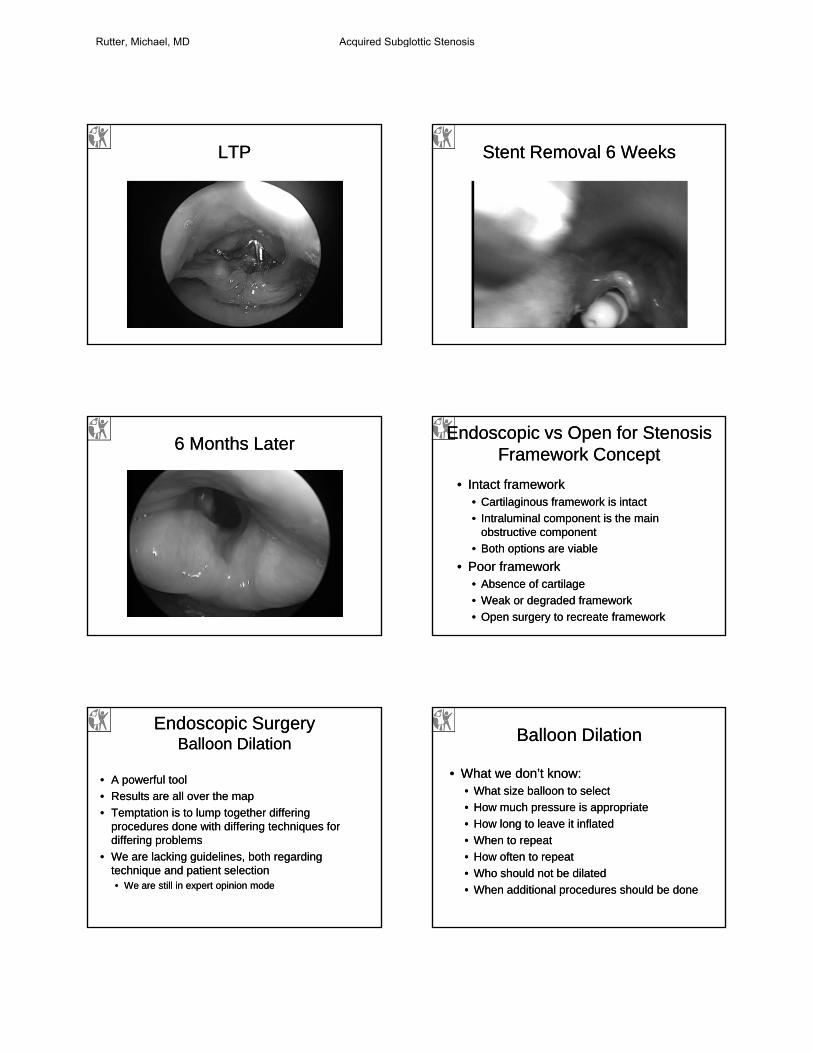
LTPLTP Stent Removal 6 WeeksStent Removal 6 Weeks
6 Months Later6 Months LaterEndoscopic vs Open for Stenosis
Framework ConceptEndoscopic vs Open for Stenosis
Framework Concept
• Intact framework• Cartilaginous framework is intact
• Intraluminal component is the main obstructive component
• Both options are viable
• Poor framework• Absence of cartilage
• Weak or degraded framework
• Open surgery to recreate framework
• Intact framework• Cartilaginous framework is intact
• Intraluminal component is the main obstructive component
• Both options are viable
• Poor framework• Absence of cartilage
• Weak or degraded framework
• Open surgery to recreate framework
Endoscopic SurgeryBalloon Dilation
Endoscopic SurgeryBalloon Dilation
• A powerful tool
• Results are all over the map
• Temptation is to lump together differing procedures done with differing techniques for differing problems
• We are lacking guidelines, both regarding technique and patient selection• We are still in expert opinion mode
• A powerful tool
• Results are all over the map
• Temptation is to lump together differing procedures done with differing techniques for differing problems
• We are lacking guidelines, both regarding technique and patient selection• We are still in expert opinion mode
Balloon DilationBalloon Dilation
• What we don’t know:• What size balloon to select
• How much pressure is appropriate
• How long to leave it inflated
• When to repeat
• How often to repeat
• Who should not be dilated
• When additional procedures should be done
• What we don’t know:• What size balloon to select
• How much pressure is appropriate
• How long to leave it inflated
• When to repeat
• How often to repeat
• Who should not be dilated
• When additional procedures should be done
Rutter, Michael, MD Acquired Subglottic Stenosis

Airway Balloon DilationAirway Balloon Dilation
• This is not new• Resurgence of
interest
• High pressure balloon dilation• Primary
intervention
• Complimentary procedure
• Adjunctive procedure
• This is not new• Resurgence of
interest
• High pressure balloon dilation• Primary
intervention
• Complimentary procedure
• Adjunctive procedure
Current ExperienceCurrent Experience
• Since 2001, over 2700 balloon dilations performed• 1 complication
• Even my more cynical colleagues are converting!
• As with standard dilation techniques, not effective for everything
• Since 2001, over 2700 balloon dilations performed• 1 complication
• Even my more cynical colleagues are converting!
• As with standard dilation techniques, not effective for everything
The Index CaseThe Index Case
• In February 2001, Peter Manning and I performed our first slide tracheoplasty on a baby with complete tracheal rings and a Grade 1 subglottic stenosis
• Post operatively she developed a “Figure 8” trachea
• Wished to dilate, but was limited by the subglottic stenosis
• An angioplasty balloon dilator was the solution
• In February 2001, Peter Manning and I performed our first slide tracheoplasty on a baby with complete tracheal rings and a Grade 1 subglottic stenosis
• Post operatively she developed a “Figure 8” trachea
• Wished to dilate, but was limited by the subglottic stenosis
• An angioplasty balloon dilator was the solution
Advantages / DisadvantagesAdvantages / Disadvantages
• Advantages• Radial dilation - no
shear forces
• Precise high pressure dilation
• Low risk
• Disadvantages• Cost
• Balloon “slips” easily
• Single use device
• Advantages• Radial dilation - no
shear forces
• Precise high pressure dilation
• Low risk
• Disadvantages• Cost
• Balloon “slips” easily
• Single use device
GuidelinesGuidelines
• Formula:• Take the outer diameter
of an age appropriate endotracheal tube
• Add 1mm for laryngeal dilation
• Add 2mm for tracheal dilation
• Formula:• Take the outer diameter
of an age appropriate endotracheal tube
• Add 1mm for laryngeal dilation
• Add 2mm for tracheal dilation
Example: A 4 year old child should take a 5.0 ETT, with an outer diameter of 6.8mm, therefore I would choose a 8mm balloon to dilate the larynx, and a
9mm balloon to dilate the trachea
TechniqueTechnique• Endoscopically guided balloon
placement• Usually direct placement into the
trachea• Occasionally through the suction port
of a ventilating bronchoscope or tracheoscope
• Patient is pre-oxygenated, then Propofol bolus
• Balloon is inflated to rated burst pressure• Pressure is maintained for either 2
minutes, or until the oxygen saturation drops to 90%
• Balloon is then deflated and removed
• Endoscopically guided balloon placement• Usually direct placement into the
trachea• Occasionally through the suction port
of a ventilating bronchoscope or tracheoscope
• Patient is pre-oxygenated, then Propofol bolus
• Balloon is inflated to rated burst pressure• Pressure is maintained for either 2
minutes, or until the oxygen saturation drops to 90%
• Balloon is then deflated and removed
Rutter, Michael, MD Acquired Subglottic Stenosis

Complimentary Procedure 6 Week Old Girl
Complimentary Procedure 6 Week Old Girl
• Transferred with stridor
• Term delivery
• Apnea at home at 2 weeks – intubated by the ambulance crew, transferred to local hospital. 4.5ETT
• Extubated 3 days later
• Home day 7
• Increasing stridor
• Transferred with stridor
• Term delivery
• Apnea at home at 2 weeks – intubated by the ambulance crew, transferred to local hospital. 4.5ETT
• Extubated 3 days later
• Home day 7
• Increasing stridor
6 Week Old Girl6 Week Old Girl
• Balloon dilation with a 5mm balloon at 20 atmospheres for 30 seconds
• Now leaking around a 3.0 ETT
• 5 days later “elective” LTR
• Today I would have tried to avoid the LTR!
• Balloon dilation with a 5mm balloon at 20 atmospheres for 30 seconds
• Now leaking around a 3.0 ETT
• 5 days later “elective” LTR
• Today I would have tried to avoid the LTR!
6 Year Old Girl6 Year Old Girl
• Ex-premmie, prolonged intubation, past cricoid split
• Past “bouginage” dilation
• Stridor at rest, exercise intolerance, 3.0 ETT airway
• Sickle knife division, kenalog injection, dilation
• Ex-premmie, prolonged intubation, past cricoid split
• Past “bouginage” dilation
• Stridor at rest, exercise intolerance, 3.0 ETT airway
• Sickle knife division, kenalog injection, dilation
Tools – Blitzer KnifeTools – Blitzer Knife
Tools – Oral Tracheal InjectorTools – Oral Tracheal Injector 6 Year Old Girl6 Year Old Girl
• Returns 2 weeks later
• Now 4.5 ETT airway
• Asymptomatic
• Re-dilation 10mm balloon
• Age appropriate airway at 1 year
• Returns 2 weeks later
• Now 4.5 ETT airway
• Asymptomatic
• Re-dilation 10mm balloon
• Age appropriate airway at 1 year
Rutter, Michael, MD Acquired Subglottic Stenosis
Open Airway SurgeryOpen Airway Surgery
• There are only 3 open airway operations for laryngotracheal stenosis:• Augmentation grafting
• Resection
• Slide
• There are only 3 open airway operations for laryngotracheal stenosis:• Augmentation grafting
• Resection
• Slide
Open Airway Surgery21st Century
Open Airway Surgery21st Century
• LTR• Anterior vs posterior vs anterior and posterior• Posterior grafting without sutures• Infant LTR
• CTR• With combined posterior grafting
• Slide tracheoplasty• Congenital tracheal stenosis (transthoracic)• Acquired tracheal stenosis (transcervical)
• LTR• Anterior vs posterior vs anterior and posterior• Posterior grafting without sutures• Infant LTR
• CTR• With combined posterior grafting
• Slide tracheoplasty• Congenital tracheal stenosis (transthoracic)• Acquired tracheal stenosis (transcervical)
Augmentation GraftingAugmentation Grafting
• Aim is to expand the laryngotracheal exoskeleton
• Grafts may include costal cartilage, thyroid cartilage, pericardium, even homograft
• Operations include anterior graft LTP, posterior graft LTP, A/P grafts, pericardial patches etc
• Aim is to expand the laryngotracheal exoskeleton
• Grafts may include costal cartilage, thyroid cartilage, pericardium, even homograft
• Operations include anterior graft LTP, posterior graft LTP, A/P grafts, pericardial patches etc
Augmentation GraftingAugmentation Grafting
• A 2 dimensional operation• Less surgeon specific
• Outcomes relate to Grade of stenosis
• Negative predictors of success include• Active larynx
• GER, EoE
• MRSA colonization
• Revision surgery
• 50 - 90% success
• A 2 dimensional operation• Less surgeon specific
• Outcomes relate to Grade of stenosis
• Negative predictors of success include• Active larynx
• GER, EoE
• MRSA colonization
• Revision surgery
• 50 - 90% success
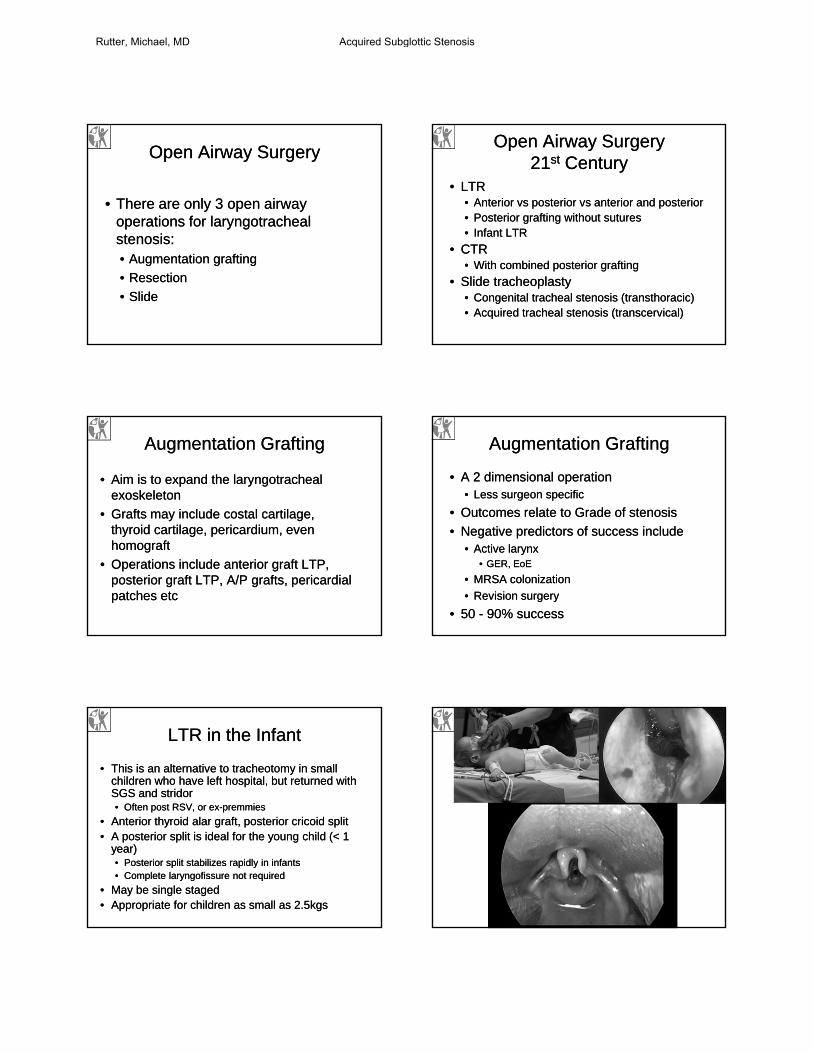
LTR in the InfantLTR in the Infant
• This is an alternative to tracheotomy in small children who have left hospital, but returned with SGS and stridor• Often post RSV, or ex-premmies
• Anterior thyroid alar graft, posterior cricoid split• A posterior split is ideal for the young child (< 1
year)• Posterior split stabilizes rapidly in infants• Complete laryngofissure not required
• May be single staged• Appropriate for children as small as 2.5kgs
• This is an alternative to tracheotomy in small children who have left hospital, but returned with SGS and stridor• Often post RSV, or ex-premmies
• Anterior thyroid alar graft, posterior cricoid split• A posterior split is ideal for the young child (< 1
year)• Posterior split stabilizes rapidly in infants• Complete laryngofissure not required
• May be single staged• Appropriate for children as small as 2.5kgs
Rutter, Michael, MD Acquired Subglottic Stenosis
Posterior Cricoid GraftingPosterior Cricoid Grafting
• Technique evolution• Non-sutured posterior
costal cartilage grafts
• Shorter stenting periods
• Attempting to preserve the anterior commissure
• LTR number 1000!• 1998
• Our first sutureless posterior graft
• Technique evolution• Non-sutured posterior
costal cartilage grafts
• Shorter stenting periods
• Attempting to preserve the anterior commissure
• LTR number 1000!• 1998
• Our first sutureless posterior graft
The cricoid, cricothyroid membrane and lower 1/3rd of the thyroid cartilage are incised in the midline, preserving the anterior commissure, and the integrity of the thyroid cartilage
The cricoid, cricothyroid membrane and lower 1/3rd of the thyroid cartilage are incised in the midline, preserving the anterior commissure, and the integrity of the thyroid cartilage
The posterior cricoid is infiltrated with 1:100 000 epinephrine and lidocaineThe posterior cricoid is infiltrated with 1:100 000 epinephrine and lidocaine
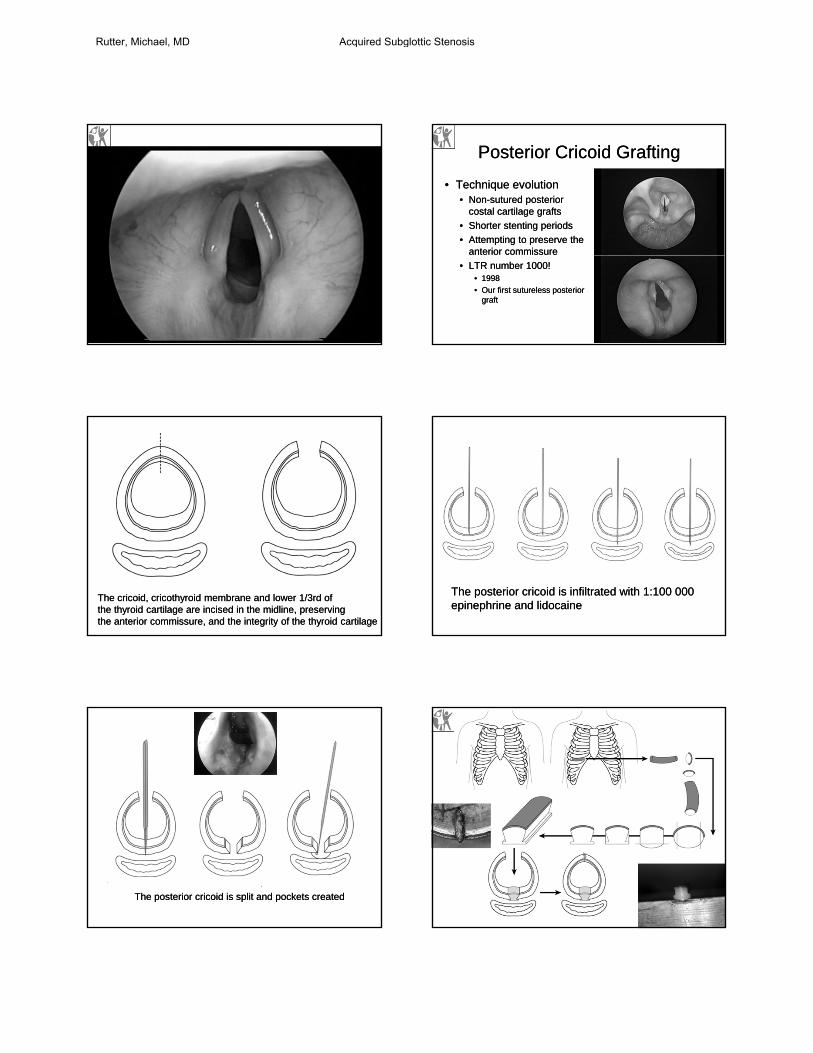
The posterior cricoid is split and pockets createdThe posterior cricoid is split and pockets created
Rutter, Michael, MD Acquired Subglottic Stenosis

AdvantagesAdvantages
• Avoiding a complete laryngofissure stabilizes the larynx
• LA infiltration posterior to the cricoid provides hemostasis and protects the esophagus
• Keeping the anterior commissure intact is desirable• Voice• Laryngeal cartilage stability
• The flanged graft is rapidly carved
• The technique is faster
• Avoiding a complete laryngofissure stabilizes the larynx
• LA infiltration posterior to the cricoid provides hemostasis and protects the esophagus
• Keeping the anterior commissure intact is desirable• Voice• Laryngeal cartilage stability
• The flanged graft is rapidly carved
• The technique is faster
Anterior / Posterior GraftAnterior / Posterior Graft
• Gd III and IV subglottic stenosis
• Especially if lateral shelves
• Especially if close to the cords
• Gd III and IV subglottic stenosis
• Especially if lateral shelves
• Especially if close to the cords
Rutter, Michael, MD Acquired Subglottic Stenosis

LTP OutcomesLTP Outcomes
• LTR has been established as a mainstay for treatment of laryngotracheostenosis
• Success is highly correlated with the degree of stenosis• (increasing stenosis and decreasing success
rate)
• LTR has been established as a mainstay for treatment of laryngotracheostenosis
• Success is highly correlated with the degree of stenosis• (increasing stenosis and decreasing success
rate)
Cricotracheal ResectionCricotracheal Resection
• CONCEPT:• Remove the
“Diseased” or damaged segment of the laryngotracheal airway
• Connect the “Healthy” superior and inferior airway segments
• Achieve decannulation
• CONCEPT:• Remove the
“Diseased” or damaged segment of the laryngotracheal airway
• Connect the “Healthy” superior and inferior airway segments
• Achieve decannulation
Best Candidates for CTRBest Candidates for CTR
• Grade IV or Severe Grade III Subglottic Stenosis with a Clear Margin (> 3 mm) Between the Stenosis and the Vocal Folds
• Grade IV or Severe Grade III Subglottic Stenosis with a Clear Margin (> 3 mm) Between the Stenosis and the Vocal Folds
Rutter, Michael, MD Acquired Subglottic Stenosis

The Future Role of CTRThe Future Role of CTR
• Ideal for severe SGS and salvage SGS
• Complementary to LTR• Very useful to have both
tools available
• CTR is a technically challenging operation in children (compared to LTR)
• There is a significant learning curve
• When it goes wrong, it can really go wrong
• Ideal for severe SGS and salvage SGS
• Complementary to LTR• Very useful to have both
tools available
• CTR is a technically challenging operation in children (compared to LTR)
• There is a significant learning curve
• When it goes wrong, it can really go wrong
Subglottic Stenosis - CTRSubglottic Stenosis - CTR
• This is a difficult operation• Demands 3 dimensional thinking
• A distinct learning curve
• Certain operative risks• Is CTR the right procedure?
• Hug the tracheal perichondrium to avoid recurrent laryngeal nerves
• Very vunerable close to the cricothyroid joints
• This is a difficult operation• Demands 3 dimensional thinking
• A distinct learning curve
• Certain operative risks• Is CTR the right procedure?
• Hug the tracheal perichondrium to avoid recurrent laryngeal nerves
• Very vunerable close to the cricothyroid joints
Tracheal Stenosis -Slide TracheoplastyTracheal Stenosis -Slide Tracheoplasty
• The 3rd alternative
• Introduced by Tsang and Goldstraw in 1989
• Popularized by Grillo in the 1990s
• Introduced at Cincinnati Children’s in 2001
• Conceived as an intrathoracic technique for managing complete tracheal rings
• The 3rd alternative
• Introduced by Tsang and Goldstraw in 1989
• Popularized by Grillo in the 1990s
• Introduced at Cincinnati Children’s in 2001
• Conceived as an intrathoracic technique for managing complete tracheal rings
Cervical Slide - EvolutionCervical Slide - Evolution
• Acquired tracheal stenosis • Initially long segment
• Increasingly as a replacement for tracheal resection even for short segment
• Salvage
• Acquired tracheal stenosis • Initially long segment
• Increasingly as a replacement for tracheal resection even for short segment
• Salvage
Rutter, Michael, MD Acquired Subglottic Stenosis

Mike Rutter
Catherine Hart
Robin Cotton
Alessandro deAlarcon
Rutter, Michael, MD Acquired Subglottic Stenosis