service audit and review tool: opioid substitution ... · service audit and review tool: opioid...
TRANSCRIPT

2007
–
–
Service Audit andReview ToolOpioid substitution treatment in New Zealand

Service Audit and Review Tool Opioid Substitution Treatment in New Zealand

Citation: Ministry of Health. 2007. Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand. Wellington: Ministry of Health.
Published in April 2007 by the Ministry of Health
PO Box 5013, Wellington, New Zealand
ISBN 978-0-478-30769-6 (print) ISBN 978-0-478-30770-2 (online)
HP 4375
This document is available on the Ministry of Health website: http://www.moh.govt.nz
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand iii
Foreword The Ministry of Health is committed to better service delivery and actively promotes responsiveness and quality improvement. This update of the Opioid Substitution Treatment Audit and Review Tool accommodates the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003) and allows standardisation in the auditing and review of opioid substitution treatment services in New Zealand. The Audit and Review Tool can be used internally for self-evaluation or peer review purposes either in its entirety or in part. It supersedes the previous Ministry of Health Audit Tool as of November 2006. The key principles of safety, stabilisation, assessment and review, treatment planning, clinical case management and integrated treatment are stressed in the practice guidelines, as are the specialist skills and knowledge needed for opioid substitution treatment. The Audit and Review Tool is designed to evaluate how these principles are applied in service delivery and to offer services an opportunity to assess themselves against the Alcohol and Other Drug Treatment Sector Standard (NZS 8157:2003) or the National Mental Health Sector Standard (NZS 8143:2001). The National Addiction Centre of the University of Otago worked in collaboration with Ms Helen Mitchell Shand, representatives of the National Association of Opioid Treatment providers, and tāngata whaiora/consumers to develop this Audit and Review Tool. It has been trialled by a number of services and revised in minor ways since the initial work was carried out. The Ministry of Health acknowledges the efforts made by the sector to contribute to the provision of better, timely and fairer services for people with opioid dependence. Dr Janice Wilson Deputy Director-General Mental Health Directorate

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand v
Contents
Foreword iii
Introduction 1 Input to the development of the Audit and Review Tool 1
The External Audit Process 2 Guidance notes for the external audit process 3 Self-evaluation and peer review 5
Part A: Background and Statistical Information 7 A1 Basic service information 7 A2 Organisation documentation 8 A3 Opioid substitution treatment service-specific documentation 9 A4 Client statistics 11 A5 Staff statistics 12 A6 Key referrers and linkage services 14
Part B: Documentation Audit Tool 15 Guidance notes: documentation audit tool 15 B1 Documentation audit tool: organisation wide 16 B2 Documentation audit tool: service specific 17
Part C: Observation of Facility 25 Guidance notes: observation of facility 25 C1 Audit tool for observation of facility 25
Part D: Review of Incident Reports 27 Guidance notes: review of incident reports 27 D1 Audit tool for review of incident reports 28
Part E: Clinical Records Review 29 Guidance notes: clinical records review 29 E1 Opioid substitution treatment service, clinical records audit tool: intake assessment 30 E2 Opioid substitution service – clinical records audit tool: treatment planning and
progress notes 32 E3 Opioid substitution treatment service – clinical records audit tool: treatment monitoring
and reviews 33 E4 Opioid substitution treatment service – clinical records audit tool: summary 34 E5 Opioid substitution treatment service – audit tool for methadone or other medication
clinical records/files 35

vi Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Part F: Manager, Clinical Head/Team Leader and Staff Interviews 36 Guidance notes: manager, clinical head/team leader and staff interviews 36 F1 Audit tool for service interviews: service organisation, treatment environment and
culture, management/clinical leadership 37 F2 Audit tool for service interviews: policies, protocol and procedures 39 F3 Audit tool for service interviews: clinical case management 40 F4 Audit tool for service interviews: clinical practice procedures 42 F5 Audit tool for service interviews: therapeutic interventions 44 F6 Audit tool for service interviews: staff policies and practices 45 F7 Audit tool for service interviews: ethno-cultural safety and responsiveness 47 F8 Audit tool for service interviews: GP prescribing 48 F9 Audit tool for service interviews: pharmacy liaison 48 F10 Audit tool for service interviews: continuous quality improvement 49
Part G: Client/Tāngata Whaiora and Other Consumer Interviews 50 Guidance notes: client/tāngata whaiora and other consumer interviews 50 G1 Audit tool for consumer interviews 51
Part H: Interviews with Pharmacists, Authorised GPs and Other Key Interfaces/Linkages 55 Guidance notes: interviews with pharmacists, authorised GPs and other key interfaces/linkages 55 H1 Audit and review tool for interviews with pharmacists 56 H2 Audit tool for interviews with authorised GPs 58 H3 Audit tool for interviews with medicine control advisors, detoxification unit staff and
other key interfaces/linkages 61
References and Further Reading 63 Relevant legislation and guidelines 63
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 1
Introduction The purpose of audit is to ensure that the treatment and care provided are safe, effective and efficient and appropriate to the needs of the individual tāngata whaiora/client and their significant others/whānau. More specifically, audit identifies aspects of clinical care and service delivery that require change and improvement. Audits may be comprehensive, focus on particular aspects, or be issues focused. The content of this updated Audit and Review Tool is based on the Opioid Substitution Treatment New Zealand Practice Guidelines (OSTPG) (Ministry of Health 2003). Emphasised in the guidelines is a system of care approach to treatment and continuity of care that ranges from intensive intervention and active case management (stabilisation, integrated treatment) within a specialist alcohol and other drug treatment service to ongoing care within the primary health care sector. To this extent the Audit and Review Tool needs to take into account the:
1. different settings and geographical and cultural contexts within which treatment is provided
2. stage of service development
3. service organisation and mix of direct, indirect or linked service provision, for example, the mix of clients receiving shared care/attending general practitioners (GPs) under authority
4. range of interventions available or able to be accessed (which may vary, eg, for resource reasons or in relation to urban or rural setting).
It is expected that consumer advisors will be consulted and actively involved in all phases of an audit process or evaluation to ensure the most effective mix of input from tāngata whaiora/ consumer (including significant others/whānau) in relation to the specific service or programme being audited or reviewed. The National Association of Opioid Treatment Providers (NAOTP) offers consultation in relation to audit from the perspective of best practice. NAOTP also acts as an umbrella for the development of peer review processes.
Input to the development of the Audit and Review Tool The following representatives of NAOTP comprised a task group to provide input to the development of the audit tool: • Annemarie Wille, Manager, Auckland Regional Methadone Service • Dr Rod Bird, Medical Officer, Alcohol & Drug Services, Wairau Hospital, Blenheim • Dr Tony Farrell, FRNZCGP, MBChb, Mt Maunganui. Consumer input was provided through consumer consultation that was facilitated by: • Lynn Iti, South Island Alcohol and Drug Service Consumer Advisor • Sheridan Pooley, Auckland Regional Alcohol and Drug Service Consumer Advisor. Feedback on the draft Audit and Review Tool was provided by: • Lynn Iti, South Island Alcohol and Drug Service Consumer Advisor • members of NAOTP • Ministry of Health • Sheridan Pooley, Auckland Regional Alcohol and Drug Service Consumer Advisor.

2 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
The External Audit Process Organisation (eg, Ministry of Health or District Health Board) requests an audit or evaluation of the opioid substitution treatment service.
Organisation contracts with appropriate external auditors.
Service provider is made aware that it is subject to an audit using the Ministry of Health Opioid Substitution Treatment Audit and Review Tool.
Consumers/tāngata whaiora using the service are notified and voluntary participation in client interviews is elicited.
Background information is forwarded to the auditors prior to their visits (Parts A and B of tool).
Auditors arrange a time to conduct an on-site visit.
Auditors make observations regarding the physical environment of the service.
During the on-site visit, interviews are conducted with managers and clinical leaders, other staff, consumers/tāngata whaiora and key referrers/ linkages as relevant. Policies, administration and clinical procedures, protocols/guidelines and clinical records are reviewed.
Incident reports should be made available for review. These are not taken from the site.
Clinical record review: notes must not be taken from the service or used for any purpose other than the audit.
Auditors write a report based on the findings of the audit.
A draft of the report is made available to the service and to any individuals mentioned in the report, with opportunity for comment.
The report is made available to the organisation requesting the audit, the service and, in many instances, the clients/tāngata whaiora. If the audit is issues based, a copy must be forwarded to the Director of Mental Health for noting.
NoteCaution must be taken identifying who is able to have direct access to tāngata whaiora/client information. The Health Information Privacy Code 1994 allows for such information to be used for clinical and quality audits. However, where possible, client/tāngata whaiora permission should be sought for the use of their personal records, incident reports, etc. Such documents may not be taken from the site, and may be used only for auditing purposes. Efforts must be made to maintain privacy of client/tāngata whaiora as much as possible and, where files are viewed without the prior consent of the client/tāngata whaiora, notice must be left of the audit purpose and reason for viewing the file.
On-site audit visit

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 3
Guidance notes for the external audit process 1. The Ministry of Health or the purchaser/provider of the service (relevant District Health
Board) instigates the audit of an opioid substitution treatment service. The instigator of the audit must advise the service of the audit. The audit will include review of documentation (service policies and procedures including service provision frameworks/client pathway clinical processes (entry to discharge) and treatment protocols/guidelines). The audit will not evaluate or review treatment of an individual tāngata whaiora/client’s treatment although the auditors will review clinical records in order to audit administrative and clinical processes and to gain an overview of treatment provided.
2. The audit team comprises at least two people, one of whom has an in-depth clinical understanding of best practice opioid substitution treatment. The team also needs to have a clear understanding and knowledge of opioid substitution treatment in New Zealand and the Ministry of Health’s practice guidelines (Ministry of Health 2003).
3. Encouragement is given to consult with the National Association of Opioid Treatment Providers and relevant regional or service consumer advisors regarding relevant personnel to be involved with the audit process.
4. Documentation is sought prior to the on-site audit visit. Services will be given at least two working weeks to forward the required documentation. The information provided will be reviewed by the audit team prior to the on-site visit, and any questions raised will be clarified in advance where possible or addressed during the on-site visit.
5. The on-site audit will include interviews with the manager/clinical head/team leader(s) and other staff members, tāngata whaiora/clients and key referrers and representatives of key linkage services, including general practice staff and pharmacists. The number and range of external service representatives interviewed will depend on the individual service context. A timeframe will be worked out between the auditors and the service and this timeframe should also meet the needs of the organisation that instigated the audit.
6. Once a service has been notified that an audit of its service is to take place, the service manager/clinical head is required to notify staff and tāngata whaiora/clients of the upcoming audit. This notification is to be in a written form and, for the purpose of notifying tāngata whaiora/clients, a notice should be displayed in a public place. Where needed staff must communicate information about the audit verbally also. The notice needs to indicate that the auditors will carry out interviews and that volunteers for these interviews would be appreciated. A statement about confidentiality of the interviews and the independence of the auditors is also required.
7. A review of documentation is an important part of the audit. Certain aspects relating to policy and procedures and treatment protocols/guidelines will be covered in all interviews. As stated above, the audit will not evaluate or review cases of individual tāngata whaiora/ clients.
8. A draft report will be made available to the service, including consumer advisors, before the final report is submitted to the organisation that requested the audit. There will be opportunity at this stage for comments to be made to the auditors concerning the report.

4 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
9. Recommendations will be a major part of the report. These recommendations will refer to each of the areas defined in the Audit and Review Tool that the auditors consider need reviewing, changing or developing.
Obtaining information from clients/tāngata whaiora and access to their case records 10. The Health Information Privacy Code 1994 allows for the case records of a tāngata
whaiora/client to be used for clinical and quality audits. Such documents will not be taken from the site and they will only be used for auditing purposes. Efforts must be made to maintain the privacy of a tāngata whaiora/client as much as possible.
11. The service is to take reasonable steps to ensure all tāngata whaiora/clients are aware that an audit of the service is going to take place and, specifically, are aware of: • the fact that information is being collected • the purpose(s) for which it is being collected • the intended recipients of the information • contact details of the auditors • the possibility of individual client files being randomly selected by the auditors and the
purpose behind this.
12. A note will be placed in the file of each tāngata whaiora/client audited, at the time of audit. The relevant staff member will then provide information about the audit to the client at the next contact.
On-site audit visit 13. Checklist for auditors:
• Advise the service manager and clinical head in writing of your authorisation and intention to carry out the audit. Include an auditor profile and audit request acceptance.
• Enclose forms that need to be filled in by the service and a list of documentation (related to Parts A and B of the Audit and Review Tool) required prior to the on-site audit visit. This information enables the auditors to gain an overview of the service prior to the on-site visit. Enclose a copy of the full Audit and Review Tool.
• Request a date for an on-site audit visit by the auditors that fits within the timeframe required by the instigator of the audit. The on-site audit visit should be three days depending on the size of the service and the scope of the audit.
• Advise the service manager and clinical head that the following staff/personnel (as relevant to the specific service) will need to be interviewed and request that an interview schedule be organised by the manager and clinical head in consultation with consumer and cultural advisors and other relevant personnel: – clinical head and service manager – team leaders – staff members representing each discipline and staff group employed on the team,
including administration/reception staff

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 5
– tāngata whaiora/clients including those from the waiting list and interim-prescribing programme
– significant others/family/whānau members.
In addition, a list of key referrers and linkage services (which may be internal and external to the organisation) is required from the service manager and clinical head to enable the auditors to arrange interviews with representatives of these services.
14. An initial meeting with the manager and clinical head and other staff members should be arranged with the audit team at the commencement of the on-site audit. The purpose of this meeting is to make introductions and for the auditors to explain in person the reason for the audit and who has instigated it. Arrangements for interviews and review of documentation, including clinical records and the timetable, will also be confirmed at the initial meeting.
15. At the end of the on-site audit visit, the auditors will meet with the service manager and clinical head and other staff to provide general feedback, clarify any outstanding issues and respond to any queries that have arisen during the process. Also, at this meeting they will finalise the draft report timeframe.
Self-evaluation and peer review It is strongly encouraged that, in addition to formal external audit processes, the Audit and Review Tool is used for the purpose of quality improvement by individual opioid substitution service providers (self-evaluation) and/or peer review. For a clinical process evaluation framework and practical information on clinical audit/evaluation processes, including case-note and consumer audit, refer to Towards Clinical Excellence (Ministry of Health 2002) and the Guidelines for Clinical Process Self-Evaluation in Alcohol and Drug Treatment Agencies (Deering et al 1998). As noted by Deering et al (1998), requirements for successful self-evaluation or peer review include: • managers and clinical leaders who are committed to evaluation and quality improvement • staff autonomy to implement changes • an open, supportive, collegial and psychologically and culturally safe team environment
within which contributions are actively sought and valued from all team members • congruency between interests of staff and tāngata whaiora/clients • a commitment to work in partnership with tāngata whaiora/consumers, referrers, key
community groups and funders • a willingness to question and honestly reflect on clinical practice and processes, to actively
seek and consider critical feedback from clients/tāngata whaiora and their significant others/ whānau, referrers and key linkage personnel
• a commitment to adapt clinical processes in response to relevant feedback and monitor changes made
• the capability to collect basic information • adequate resources and access to consultation.

6 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Peer review The National Association of Opioid Treatment Providers has a commitment to best practice in the provision of opioid substitution treatment in New Zealand. This group is willing to provide consultation to individual treatment providers and also to act as the umbrella group in the development of peer review processes with a particular focus on clinical processes, treatment interventions and improving treatment outcomes for clients/tāngata whaiora receiving methadone or other opioid substitution treatment, and their significant others/whānau.
Consumer input For advice on consumer input to audit and evaluation processes, it is expected that services will consult with consumer advisors (including family/whānau advisors).
Cultural consultation and input It is expected that all services will be:
• culturally competent, meaning practitioners and services are aware of the impact of their own cultural frameworks or kawa on the ‘therapeutic’ relationship and take these factors into account when planning and delivering programmes, activities and interventions
• culturally safe, meaning people feel fully able to use a health service provided by people of another culture without risk to their own culture (Ramsden 1993).
Therefore it is expected that services may need to seek advice and input from appropriate Māori and other relevant cultural advisors in relation to audit and evaluation processes.
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 7
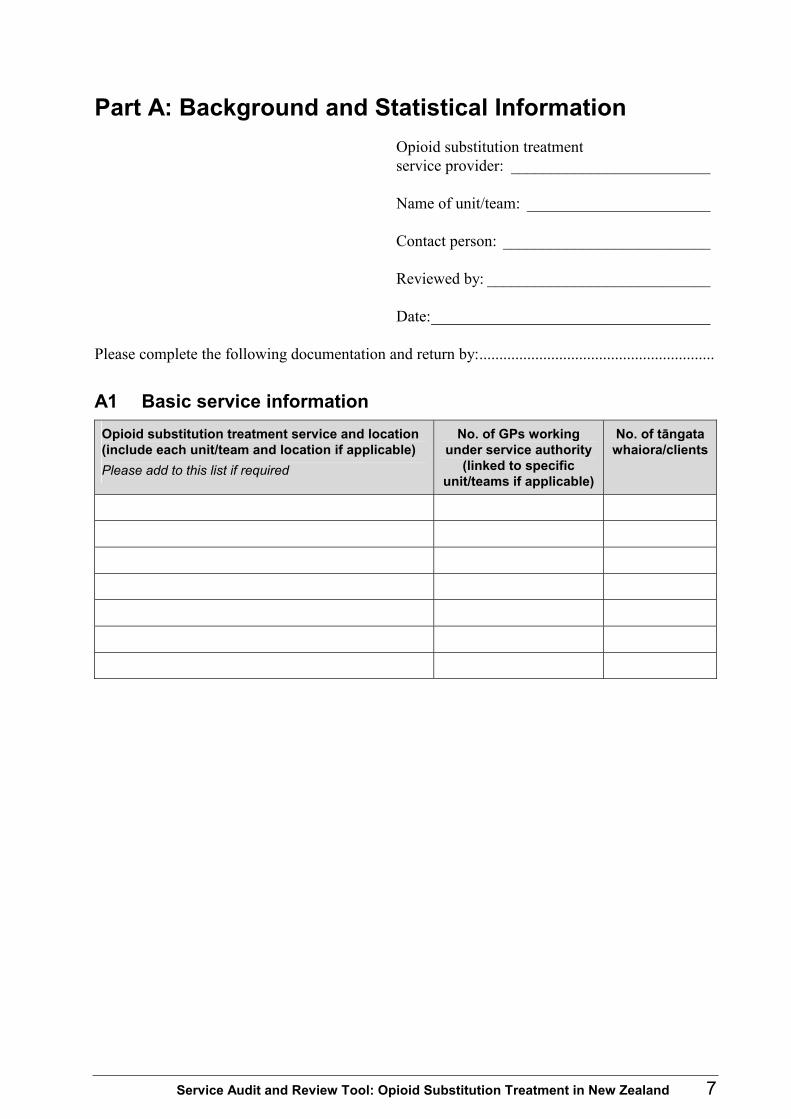
Part A: Background and Statistical Information Opioid substitution treatment service provider: _________________________ Name of unit/team: _______________________ Contact person: __________________________ Reviewed by: ____________________________ Date:___________________________________
Please complete the following documentation and return by:...........................................................
A1 Basic service information Opioid substitution treatment service and location (include each unit/team and location if applicable) Please add to this list if required
No. of GPs working under service authority
(linked to specific unit/teams if applicable)
No. of tāngata whaiora/clients

8 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
A2 Organisation documentation Please provide a copy of the index of your organisation’s Policy and Procedures
Manual that includes the polices identified in the checklist below. Ref: OSTPG page(s) or section(s) reference to the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003). Ref: OSTPG Documentation Comments (auditor use only) Yes No
Page 2 Statement of commitment to the principles of Treaty of Waitangi
2.13 Privacy
2.13 Client rights
2.17 Complaints
2.22–2.25 4.23 8.25
Incident reporting/ risk management
2.2–2.8 Staff training/education
2.2–2.8 Clinical supervision
2.2–2.8 Performance management
2.2–2.8 Workforce development
2.10 Clinical record/documentation
1.13 1.15 1.46
Informed consent

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 9
A3 Opioid substitution treatment service-specific documentation The following documentation (policies, administration and clinical processes/procedures, protocols and, guidelines) is likely to be gathered from a number of sources in your service and organisation. Ref: OSTPG, in the first column, gives the relevant page(s) or section(s) in the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003).
Please place documents you provide in the same order as this checklist, taking into account that some documentation you provide may cover more than one checklist item.
Please tick either the YES or NO box to indicate the presence or absence of each requested
document. Ref: OSTPG Documentation Yes No 1.0–1.5 Service philosophy/kaupapa, principles and description (include
brochure)
Organisational chart showing lines of reporting and accountability within your service and organisation
Page 3 Objectives for opioid substitution treatment that reflect national OSTPG objectives
1.15 2.13–2.17 3.20
Client information package/booklet (information provided to tāngata whaiora/clients and their significant others/whānau about the service and opioid substitution treatment)
1.22–1.23 2.13–2.17
Waiting list information package/booklet for tāngata whaiora/clients and their significant others/whānau Waiting list management protocol; interim prescribing protocol; other interventions offered to waiting list tāngata whaiora/clients and their significant others/whānau
8.0–8.29 Approval to offer opioid substitution treatment
1.45 2.25 4.0 8.19 8.25 App. 8
Memoranda of understanding/interface protocols with key linkage services/agencies
Page 3 2.0–2.1 2.27 8.0–8.20
Current service plan and goals/quality improvement strategies
1.4–1.7 1.16
Entry/eligibility criteria for entry to opioid substitution treatment services
1.8–1.14 Assessment
1.15 Informed consent
1.18–1.21 Treatment plan
1.24–1.44 Stabilisation
1.45–1.47 2.18–2.21
Case management
10 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
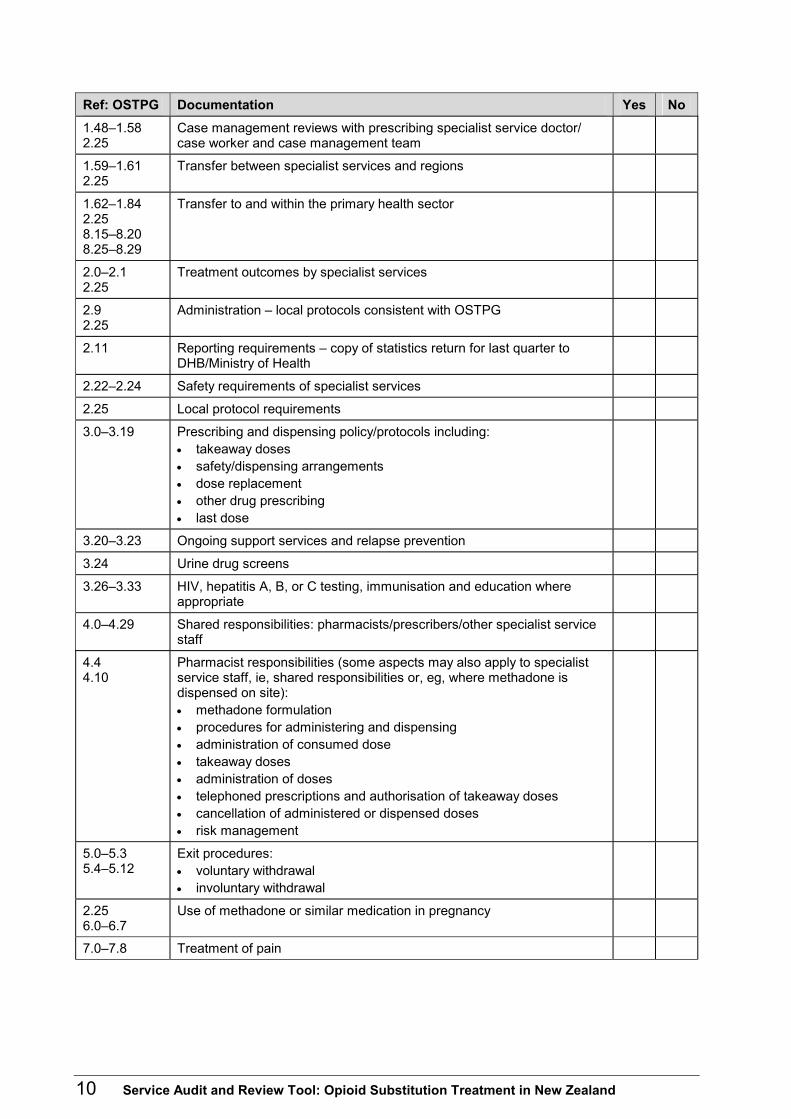
Ref: OSTPG Documentation Yes No 1.48–1.58 2.25
Case management reviews with prescribing specialist service doctor/ case worker and case management team
1.59–1.61 2.25
Transfer between specialist services and regions
1.62–1.84 2.25 8.15–8.20 8.25–8.29
Transfer to and within the primary health sector
2.0–2.1 2.25
Treatment outcomes by specialist services
2.9 2.25
Administration – local protocols consistent with OSTPG
2.11 Reporting requirements – copy of statistics return for last quarter to DHB/Ministry of Health
2.22–2.24 Safety requirements of specialist services
2.25 Local protocol requirements
3.0–3.19 Prescribing and dispensing policy/protocols including: • takeaway doses • safety/dispensing arrangements • dose replacement • other drug prescribing • last dose
3.20–3.23 Ongoing support services and relapse prevention
3.24 Urine drug screens
3.26–3.33 HIV, hepatitis A, B, or C testing, immunisation and education where appropriate
4.0–4.29 Shared responsibilities: pharmacists/prescribers/other specialist service staff
4.4 4.10
Pharmacist responsibilities (some aspects may also apply to specialist service staff, ie, shared responsibilities or, eg, where methadone is dispensed on site): • methadone formulation • procedures for administering and dispensing • administration of consumed dose • takeaway doses • administration of doses • telephoned prescriptions and authorisation of takeaway doses • cancellation of administered or dispensed doses • risk management
5.0–5.3 5.4–5.12
Exit procedures: • voluntary withdrawal • involuntary withdrawal
2.25 6.0–6.7
Use of methadone or similar medication in pregnancy
7.0–7.8 Treatment of pain
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 11
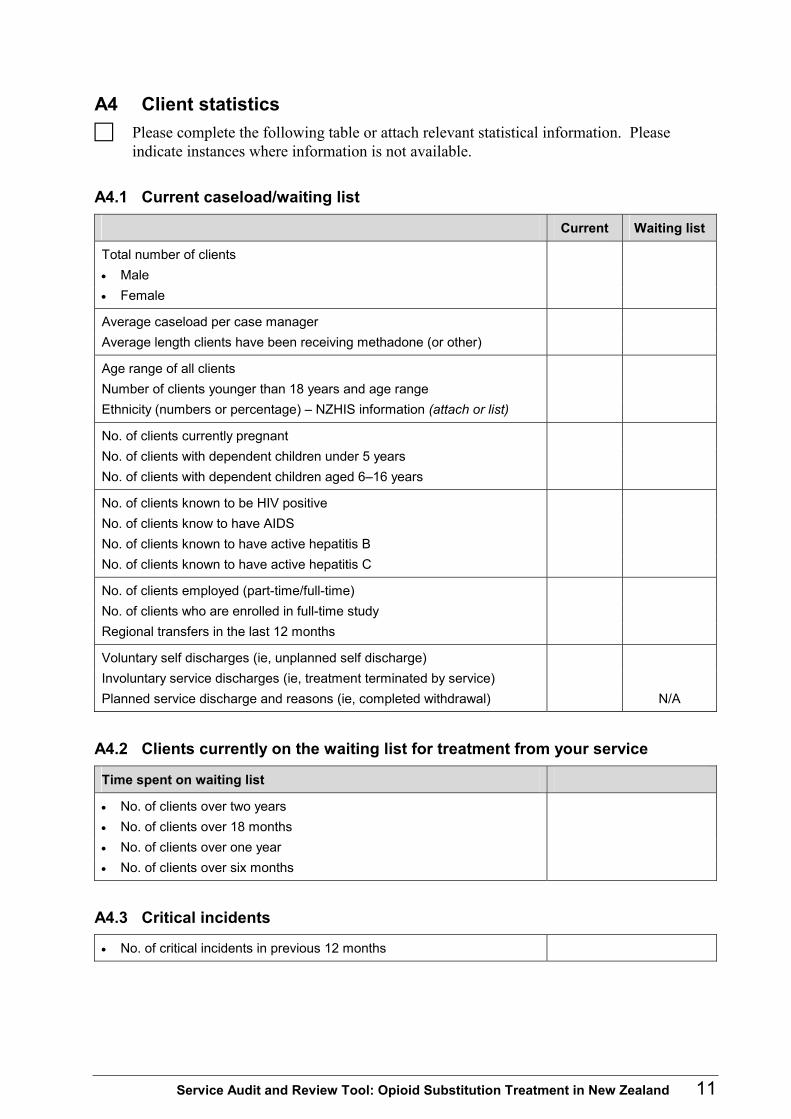
A4 Client statistics Please complete the following table or attach relevant statistical information. Please
indicate instances where information is not available.
A4.1 Current caseload/waiting list
Current Waiting list
Total number of clients • Male • Female
Average caseload per case manager Average length clients have been receiving methadone (or other)
Age range of all clients Number of clients younger than 18 years and age range Ethnicity (numbers or percentage) – NZHIS information (attach or list)
No. of clients currently pregnant No. of clients with dependent children under 5 years No. of clients with dependent children aged 6–16 years
No. of clients known to be HIV positive No. of clients know to have AIDS No. of clients known to have active hepatitis B No. of clients known to have active hepatitis C
No. of clients employed (part-time/full-time) No. of clients who are enrolled in full-time study Regional transfers in the last 12 months
Voluntary self discharges (ie, unplanned self discharge) Involuntary service discharges (ie, treatment terminated by service) Planned service discharge and reasons (ie, completed withdrawal) N/A
A4.2 Clients currently on the waiting list for treatment from your service
Time spent on waiting list
• No. of clients over two years • No. of clients over 18 months • No. of clients over one year • No. of clients over six months
A4.3 Critical incidents
• No. of critical incidents in previous 12 months

12 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
A5 Staff statistics Please provide a copy of range of role/job descriptions employed in your service. Please
fill in a separate page for each service unit/team described in section 1.0.
Please provide details as indicated below (expand the table as required). Job designation (eg, specific health professionals, counsellors/ therapists, administration/reception staff, consumer/tāngata whaiora, family/ whānau, cultural appointed roles and voluntary roles)
Number of full-time
equivalent staff
Gender Ethnicity Alcohol and other drug qualification/health
professional registration/DAPAANZ
registration/other
How many staff have left the unit/team or opioid substitution treatment service in the last
year? (Number and designation.) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________
How many vacant positions do you currently have? _______________________________
How long has each position been vacant? (Include total number of vacancies plus
designation and, if appropriate, length of vacancy.) ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 13
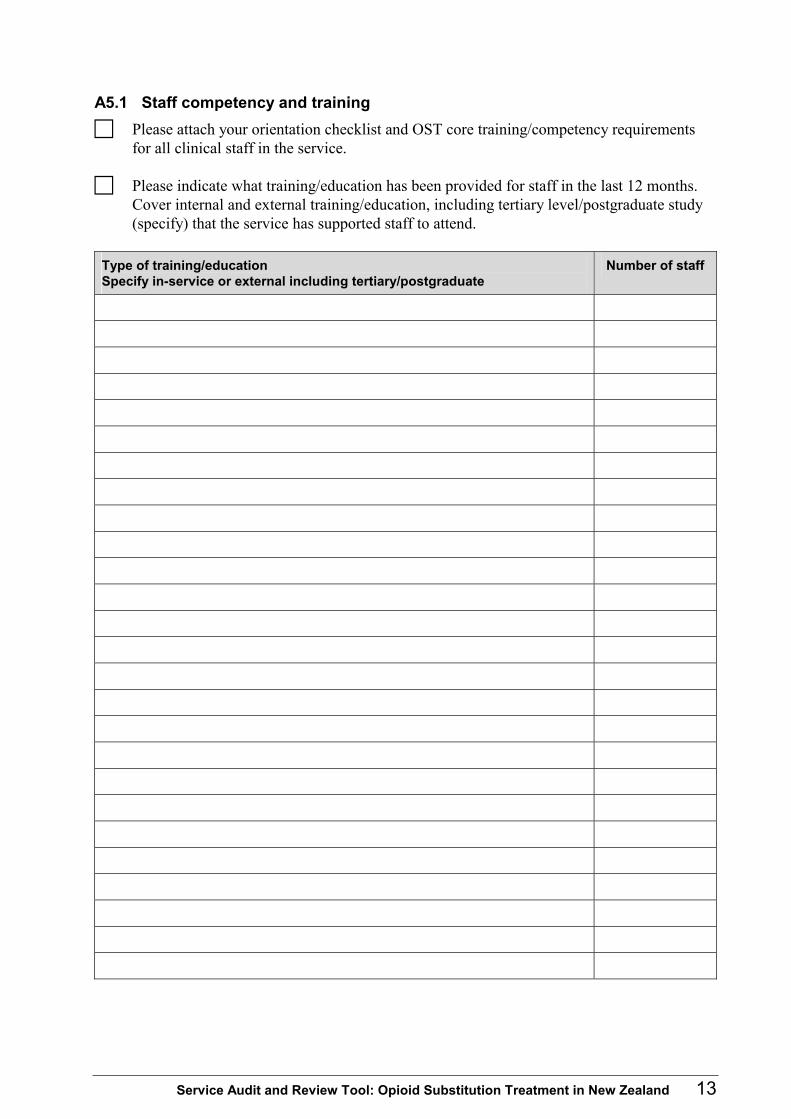
A5.1 Staff competency and training Please attach your orientation checklist and OST core training/competency requirements
for all clinical staff in the service.
Please indicate what training/education has been provided for staff in the last 12 months. Cover internal and external training/education, including tertiary level/postgraduate study (specify) that the service has supported staff to attend.
Type of training/education Specify in-service or external including tertiary/postgraduate
Number of staff

14 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
A6 Key referrers and linkage services Please list below the contact details and names of key referrers and service linkages/personnel (eg, Corrections, Work and Income, Child, Youth and Family, other alcohol and other drug agencies and GPs). Name of organisation/service Contact person, telephone number and email if known

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 15
Part B: Documentation Audit Tool Opioid substitution treatment service provider: _________________________ Name of unit/team: _______________________ Contact person: __________________________ Reviewed by: ____________________________ Date:___________________________________
Guidance notes: documentation audit tool • Where possible documentation should be reviewed prior to the on-site audit visit.
• The audit team will rate the adequacy of documentation (policies, administrative and clinical procedures/processes, protocols and guidelines) as: – SA Substantially achieved – PA Partially achieved – MA Minimally achieved.
• Ratings will take into account how documentation reflects: – the requirements of relevant sector standards which will satisfy the provisions of the Health
and Disability Services (Safety) Act 2001 – the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health
2003) – processes for ensuring clinical and cultural safety for staff and clients, as well as
effectiveness of service delivery – day-to-day practice (evaluated in conjunction with interviews, clinical records audit, etc).
Suggested indicators are provided as a guide in relation to documentation audit.

16 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
B1 Documentation audit tool: organisation wide Please tick either YES or NO to indicate the presence or absence of each document in the index. Ref: OSTPG, in the first column, gives the relevant page(s) or section(s) in the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003). Ref: OSTPG Yes No
Page 2 Statement of commitment to the principles of Treaty of Waitangi
2.13 Privacy
2.13 Client rights
2.17 Complaints
2.22–2.25 4.23 8.25
Incident reporting/risk management
2.2–2.8 Staff training/education
2.2–2.8 Clinical supervision
2.2–2.8 Performance management
2.2–2.8 Workforce development
2.10 Clinical record/documentation
1.13 1.15 1.46
Informed consent
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 17
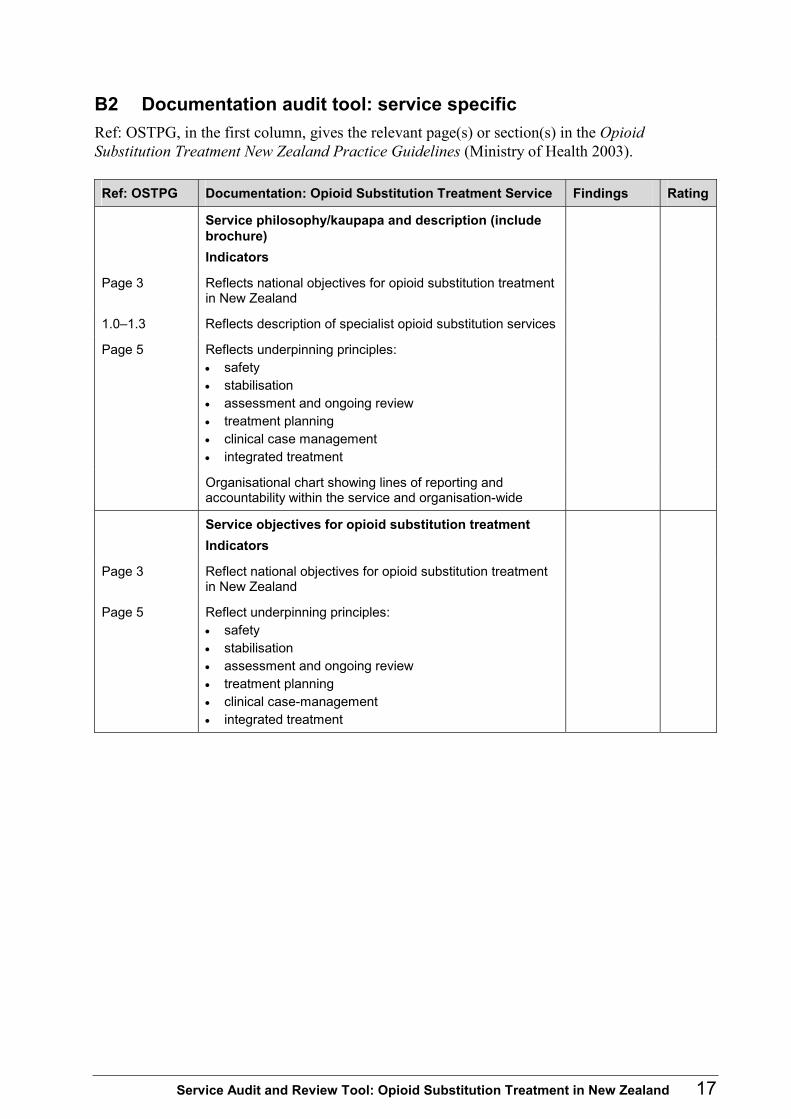
B2 Documentation audit tool: service specific Ref: OSTPG, in the first column, gives the relevant page(s) or section(s) in the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003). Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Service philosophy/kaupapa and description (include brochure) Indicators
Page 3 Reflects national objectives for opioid substitution treatment in New Zealand
1.0–1.3 Reflects description of specialist opioid substitution services
Page 5 Reflects underpinning principles: • safety • stabilisation • assessment and ongoing review • treatment planning • clinical case management • integrated treatment
Organisational chart showing lines of reporting and accountability within the service and organisation-wide
Service objectives for opioid substitution treatment Indicators
Page 3 Reflect national objectives for opioid substitution treatment in New Zealand
Page 5 Reflect underpinning principles: • safety • stabilisation • assessment and ongoing review • treatment planning • clinical case-management • integrated treatment

18 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Client information package/booklet Indicators
1.15 2.13–2.17 3.20 5.0–5.12
Includes information on: • opioid substitution treatment including potential side-
effects of this medication • range of treatment options available and offered by the
service provider or access facilitated by provider including after hours, crisis and respite
• use of psychosocial interventions (best practice would indicate medication is not enough)
• expected responsibilities/obligations as a service user including active participation in all aspects of their treatment
• client/tāngata whaiora rights and advocacy • privacy • the service’s complaints procedure (particularly in
relation to individuals seeking a review of their situation) • relevant advocacy contacts • opportunities for involvement in service planning/
evaluation • voluntary and involuntary withdrawal processes
Waiting list for clients/tāngata whaiora and their significant others/whānau information package/booklet
Indicators
1.22–1.23 2.13–2.17 2.25 3.20
Includes information on: • waiting time for admission to opioid substitution
treatment • opioid substitution treatment, the various medications
and potential side-effects • range of other interventions available including crisis,
respite, detoxification, day and residential and self-help, interim prescribing
• reviews and ongoing contact and service expectations • client/tāngata whaiora rights including privacy • advocacy contacts
Approval to offer opioid substitution treatment Indicators
8.0–8.29 Copy of approval

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 19
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Memoranda of Understanding/interface protocols with key linkage services/agencies
Indicators
1.45 2.25 4.0 8.19 8.25 App 8
MoUs/interface protocols are in place and current
Reflect partnership/multi-systemic approach and include: • roles and expectations of each service, shared care
arrangements and re-engagement into specialist service arrangements
• MoU/protocol review mechanisms
Current service plan and goals/quality improvement strategies Indicators
Page 3 2.0–2.1 2.27 8.0–8.20
Current
Reflects continuous quality improvement approach
Entry/eligibility criteria for entry to opioid substitution treatment services Indicators
1.4–1.7 1.16–1.17
Includes: • emphasis on accessibility and prompt entry • criteria for acceptance and eligibility restrictions • acceptance decision based on team decision • criteria for any interim programme, bring up system or
interaction with other providers
Assessment Indicators
1.8–1.14 Tools/guidelines reflect comprehensive assessment process including involvement of significant others/whānau and consultation/involvement with GP and other relevant providers involved in assisting the client/tāngata whaiora All key areas covered including co-existing medical, psychiatric and behavioural problems or disorders (eg, problem gambling or hepatitis)
Informed consent Indicators
1.15 1.46
Adequate information is provided before clients/tāngata whaiora consent to treatment and an initial treatment plan Informed consent is an ongoing part of the programme of care

20 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Waiting list management protocol; interim treatment protocol (aligns with client information provided for clients/tāngata whaiora and their significant others on the waiting list) Indicators
1.22–1.23 2.25
Consistent with the principles of safety and stabilisation Specifies interventions offered to clients/tāngata whaiora and their significant others/whānau including crisis and interim prescribing and other interventions Frequency of reviews and contact is specified
Treatment plan Indicators
1.18–1.21 Standard comprehensive document Indicates collaborative development with client/tāngata whaiora and where possible significant others/whānau, GP and other relevant treatment providers Review date specified
Stabilisation Indicators
1.24–1.44 Includes: • identified case manager for each client/tāngata whaiora • specified frequency of contact with the prescribing
specialist service doctor or GP, case manager and other team members
• realistic short-term treatment objectives incorporating attention to acute/immediate needs including needs of children
• adequate dose and reflects principles of safety in relation to initial and subsequent doses
• realistic indicators of stability
Case management Indicators
1.45–1.47 2.18–2.21 3.20
Each client/tāngata whaiora is allocated a case manager to co-ordinate their treatment and care Role reflected in job descriptions individualised, holistic, multi-systemic approach Key component is establishing and maintaining therapeutic relationships over time with clients/tāngata whaiora and where possible their significant others/whānau Involves screening, assessment and therapeutic interventions, linking and referral, health education/ promotion and discharge planning, consultation and liaison

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 21
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Case reviews Indicators
1.20 1.23 1.48–1.58 1.64 2.25
Protocol specifies: • timeframes as specified in OSTPG in relation to reviews
by specialist service prescribing doctor, caseworker and case-management team
• client/tāngata whaiora and opportunity for support person involvement in formal case reviews
Transfer between specialist services and regions Indicators
1.59–1.61 2.25
Protocol specifies: • responsibility for prescribing and dispensing
arrangements • case management review and assessment requirements • transfer documentation and consultation requirements
Transfer to and within the primary health sector Indicators
1.62–1.84 2.25 8.15–8.20 8.25–8.29
Protocols in accordance with legislative requirements and OSTPG and specify: • transfer conditions, assessment and review processes
and acceptance criteria • ongoing support and service provision/access to
interventions • consultation and liaison requirements including with
pharmacists and other providers • prescribing, dispensing arrangements and other drug
prescribing • criteria/processes for re-stabilisation/referral back to
specialist service provider
Treatment outcomes by specialist services Indicators
2.0–2.1 2.25
Protocol exists that reflects Alcohol and Other Drug/National Mental Health Sector Standard Activities reflect commitment to quality improvement of treatment and care through the use of the Audit and Review Tool, or other approved indices/measures and evaluation processes
Reporting requirements Indicators
2.11–2.12 Copy of statistical data return includes data related to waiting lists and retention in treatment

22 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Safety requirements Indicators
2.22–2.24 Reflect Alcohol and Other Drug Sector Standard and National Mental Health Sector Standard and balance needs of clients/tāngata whaiora with safety requirements Cover areas of: • personal safety for clients/tāngata whaiora and staff • prescribing • dispensing • takeaway medications
Local protocol requirements Indicators
2.25 Protocols exist in relation to: • access to services • management of pregnant women • people suspected of being intoxicated • people suspected of diverting medication • transfer of people to primary health care • transfer of people between specialist services • review of progress of client/tāngata whaiora • aggressive/violent behaviour • use of alcohol and/or other drugs • measurement of client/tāngata whaiora outcomes • review of safety issues
Prescribing and dispensing policy/protocols Indicators (general)
3.0–3.19 Cover legal requirements and reflect OSTPG and underpinned by principle of safety in relation to limiting potential to overdose, diversion, intoxication, safe storage practices Reflect need for adequate client/tāngata whaiora information and understanding on safe storage practices etc; specify dose replacement, other drug prescribing, last dose policy/procedures
Indicators (takeaway doses)
Based on clinical decision making by case management team in consultation with clients/tāngata whaiora and significant others/whānau (particularly where children are in household); pharmacist, primary care team, other providers as appropriate Reviewed regularly

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 23
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Urine drug screens Indicators
3.24 Reflect: • clear understanding of what urine drug screens can and
cannot provide • client/tāngata whaiora rights, particularly of informed
consent, respect and dignity
HIV, hepatitis A ,B ,C testing, immunisation and education where appropriate Indicators
3.26–3.33 Include reference to: • access to testing, education, immunisation and
treatment for clients/tāngata whaiora and families/ whānau/significant others
• confidentiality of test results • liaison/referral arrangements with infectious diseases
specialist referral protocol attached
Shared responsibilities: pharmacists/prescribers (and other specialist team staff) Indicators
4.0 Protocol or equivalent exists that: • reflects pharmacists as members of multidisciplinary
team • refers to shared responsibilities, liaison and support
mechanisms
Voluntary withdrawal Indicators
5.0–5.3 Refer to: • documented discharge plan with emphasis on
collaborative decision-making, flexibility and development of a network of support
• evidence that case managers actively pursue withdrawal rather than maintenance
• facilitation of access back to treatment as required
24 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
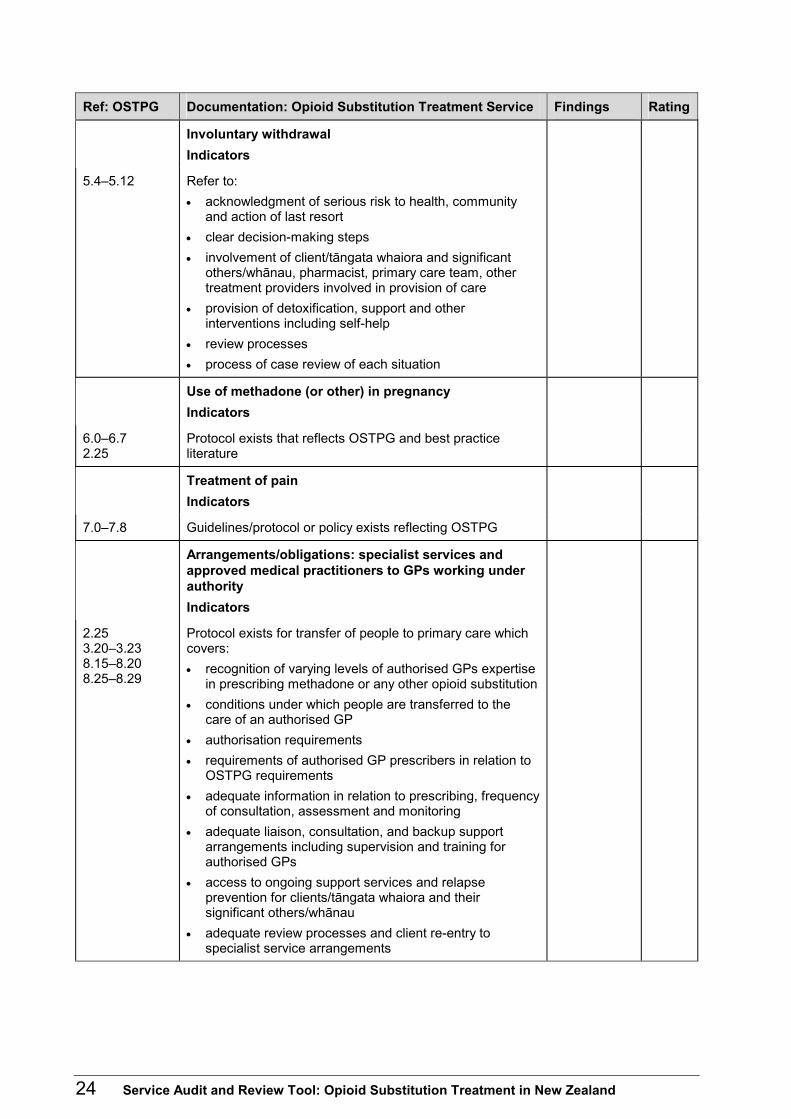
Ref: OSTPG Documentation: Opioid Substitution Treatment Service Findings Rating
Involuntary withdrawal Indicators
5.4–5.12 Refer to: • acknowledgment of serious risk to health, community
and action of last resort • clear decision-making steps • involvement of client/tāngata whaiora and significant
others/whānau, pharmacist, primary care team, other treatment providers involved in provision of care
• provision of detoxification, support and other interventions including self-help
• review processes • process of case review of each situation
Use of methadone (or other) in pregnancy Indicators
6.0–6.7 2.25
Protocol exists that reflects OSTPG and best practice literature
Treatment of pain Indicators
7.0–7.8 Guidelines/protocol or policy exists reflecting OSTPG
Arrangements/obligations: specialist services and approved medical practitioners to GPs working under authority Indicators
2.25 3.20–3.23 8.15–8.20 8.25–8.29
Protocol exists for transfer of people to primary care which covers: • recognition of varying levels of authorised GPs expertise
in prescribing methadone or any other opioid substitution • conditions under which people are transferred to the
care of an authorised GP • authorisation requirements • requirements of authorised GP prescribers in relation to
OSTPG requirements • adequate information in relation to prescribing, frequency
of consultation, assessment and monitoring • adequate liaison, consultation, and backup support
arrangements including supervision and training for authorised GPs
• access to ongoing support services and relapse prevention for clients/tāngata whaiora and their significant others/whānau
• adequate review processes and client re-entry to specialist service arrangements

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 25
Part C: Observation of Facility Opioid substitution treatment service provider: _________________________ Name of unit/team: _______________________ Contact person: __________________________ Reviewed by: ____________________________ Date:___________________________________
Guidance notes: observation of facility It is recommended that observation of the facility occur as part of the Manager and Clinical Head/Team Leader interview during the on-site audit visit. An observation guide outlining the key environmental features has been provided. The observation visit provides an opportunity to elicit additional information about the service’s treatment provision and service delivery. Familiarisation with provisions within the relevant sector standards is recommended. Any additional observations relevant to the audit should also be recorded.
C1 Audit tool for observation of facility Rating Comments
1. Facility appropriateness and environment
Description of facility
Appropriate reception facilities (consider physical attractiveness, welcoming nature, therapeutic environment, adequate number of reception staff and space)
Appropriate waiting area (consider physical attractiveness, adequate space, relevant reading material, prompt access to welcoming reception staff) Client rights/advocacy information visible
Clinic area: • adequate and appropriate equipment • adequate space • drug safe attached to building – appropriate staff (only)
access, appropriately secure and locked when not in use • appropriate key handling • adequate observation of medication administration

26 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Rating Comments
Safety features of facilities: • evacuation procedure in the event of fire or other emergency • safety mechanisms for staff and clients (eg, alarm buttons in
relevant places) • adequate interviewing facilities (including space, setting,
sound-proofing) • safety features balanced with a treatment ethos (ie, promoting
client engagement and maintaining a therapeutic relationship)
Toilet facilities: • adequate access • if observation is required, staff of relevant gender can
observe • infection control information available
Security of facilities: • all external doors have adequate locks • public areas are clearly marked (distinguished from private
areas) • adequate security lighting • attended by security personnel after hours and as required
2. Filing systems/privacy of information
• Only appropriate staff have access to the filing system • Clinical records are not accessible to the public • Cabinets holding clinical records are able to be appropriately
secured • Adequate privacy of tāngata whaiora/client information (eg,
computer screens, clinical records) in reception and other public areas

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 27
Part D: Review of Incident Reports Opioid substitution treatment service provider: _________________________ Name of unit/team: _______________________ Contact person: __________________________ Reviewed by: ____________________________ Date:___________________________________
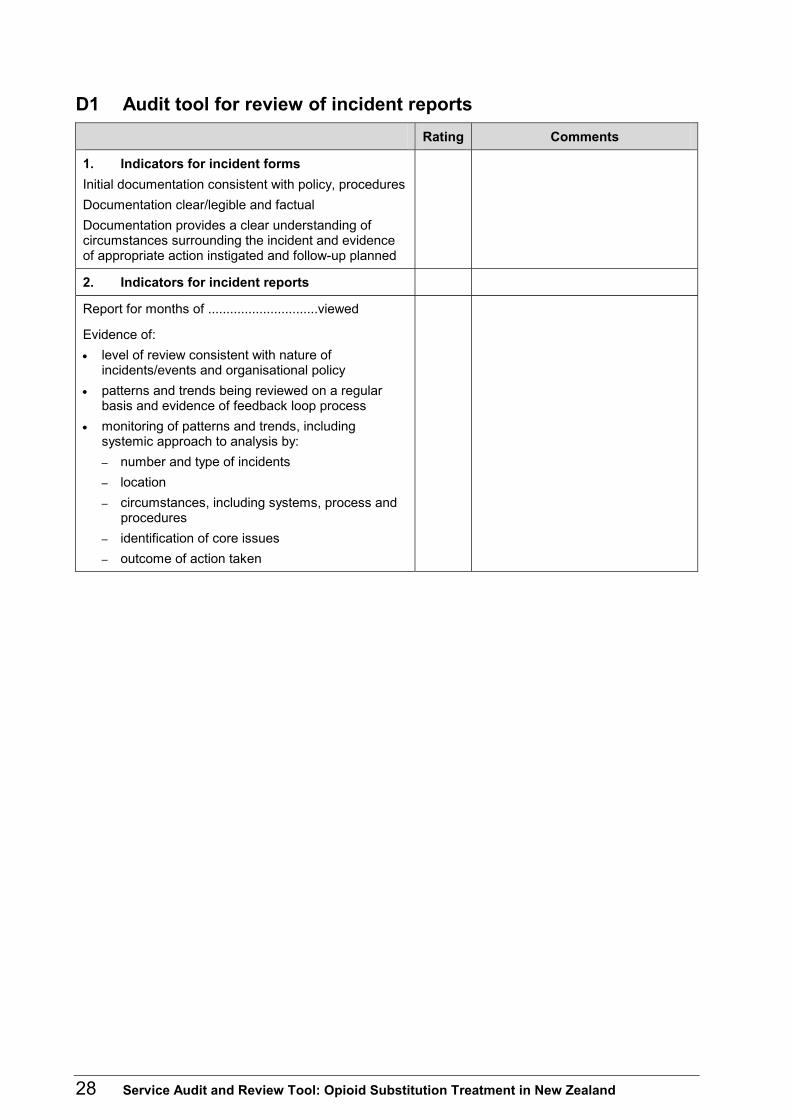
Guidance notes: review of incident reports Statistics on numbers of critical incidents (adverse, unplanned or untoward events) will be gathered as part of the background material sought prior to the audit visit. A description of incident reporting policy and procedures will be sought during management interviews. During the on-site audit visit, a review of incident reports should include a review of:
• a sample of incident forms, with audit objectives of (a) complete and comprehensive records to enable an understanding of the circumstances surrounding the incident and (b) evidence that appropriate action and review have been completed at the appropriate organisational level
• a summary of incident report data.
28 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
D1 Audit tool for review of incident reports Rating Comments
1. Indicators for incident forms Initial documentation consistent with policy, procedures Documentation clear/legible and factual Documentation provides a clear understanding of circumstances surrounding the incident and evidence of appropriate action instigated and follow-up planned
2. Indicators for incident reports
Report for months of ..............................viewed
Evidence of: • level of review consistent with nature of
incidents/events and organisational policy • patterns and trends being reviewed on a regular
basis and evidence of feedback loop process • monitoring of patterns and trends, including
systemic approach to analysis by: – number and type of incidents – location – circumstances, including systems, process and
procedures – identification of core issues – outcome of action taken

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 29
Part E: Clinical Records Review Opioid substitution treatment service provider: _________________________ Name of unit/team: _______________________ Contact person: __________________________ Reviewed by: ____________________________ Date:___________________________________
Guidance notes: clinical records review A minimum sample of 25–30 cases will be selected by the auditors for review using a randomised method. If more than one site is being audited, then the case review should take the minimum sample from each site. Systematic sampling uses every nth case (eg, every 10th case). Choose the starting point at random (eg, based on a random number between 1 and 10 (use a calculator or computer)). Then review only the cases identified in the sampling. It may also be important to specify certain conditions for the sample. For example, to represent Māori appropriately, you can separate the cases into two groups, Māori and non-Māori, and sample from each group at random. (Note: If the selection does not include at least one file of each staff member then add files using the same randomised process from the list till this are achieved.) Access to clinical records raises privacy issues. The service’s code of practice (policy) covers the use and disclosure of personal health information. (Refer also to the Health Information Privacy Code 1994.) Under the terms of that code, clinical and quality audits are deemed to be a legitimate use of personal health information. Good practice includes informing tāngata whaiora/clients of the audit and the purpose for reviewing clinical records. In addition, in each case file reviewed, the auditors will insert a note advising of the clinical record audit. At the next contact with the client/tāngata whaiora concerned, a staff member will provide information on the purpose of the audit. In addition, the audit team should observe the following:
• No case files to be taken from the service.
• No personal health information obtained from clinical record reviews is to be used for any purpose other than the purpose of the audit.

30 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
E1 Opioid substitution treatment service, clinical records audit tool: intake assessment
Service/team:.......................................................... Total number of case files audited: .........................Audit carried out by: ................................................ Date:........................................................................Clinical record number – enter NHI number: ..........
Criteria 1 2 3 4 5 6 7 8 9 10
Completion of a comprehensive assessment including; reason why tāngata whaiora/client is seeking help; expectations of treatment; perceived level of motivation and readiness to change; adequate involvement of significant others/whānau; adequate consultation/input from other service providers and GP
Completion of alcohol and other drug use history including current use and: screening of current use of nicotine, alcohol, sedative/hypnotic, cannabis, stimulants and other drug use in addition to opioid use; signs of intoxication, withdrawal, evidence of past/current drug use; previous treatments
Completion of mental health/psychological history, including; previous assessments and treatment. Screening for current problems/disorders (eg, mood/anxiety disorder, conduct disorder/anti social personality disorder) and problem gambling
Completion of medical history and investigations, including: current physical health status, history of significant illnesses, head injuries, accidents, overdose hospitalisations; GP, current medications, complementary therapies; key investigations – full blood count, liver function tests and hepatitis serology, urine drug screen
Completion of relevant legal/criminal offending history and current legal status
Completion of risk assessment, including assessment of high-risk behaviours and level of risk to self (including suicidality), to others and from others
Completion of family/whānau history, including: family history of alcohol and other drug use problems/disorders and treatment, significant medical and mental health problems/disorders and treatment
Mental status examination/observation of current mental state

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 31
Criteria 1 2 3 4 5 6 7 8 9 10
Completion of a personal/developmental history from birth through to current social circumstances, including: details of family/whānau upbringing and cultural context; enduring friendships and key relationships; education/work history and role functioning (employment/parenting); particular strengths
Presence of a comprehensive diagnostic statement that includes: opioid and other drug diagnoses; psychiatric and medical diagnoses
Presence of an individualised list of problems and strengths of client/tāngata whaiora
Identification of further information needed, record of treatment options discussed and assessed to be appropriate/inappropriate or declined

32 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
E2 Opioid substitution service – clinical records audit tool: treatment planning and progress notes
Criteria 1 2 3 4 5 6 7 8 9 10
Completion of a comprehensive treatment plan following the intake assessment which indicates development in collaboration with the client/ tāngata whaiora and involvement of significant others/whānau and relevant others (including the GP) involved with the treatment
The treatment plan and progress notes document indicate the following:
Initial informed consent for treatment (discussion of its risks, limitations and benefits) has been obtained
Education about the disorder(s) and medications prescribed including methadone or other substitution medication provided to: 1) the client/tāngata whaiora 2) their significant other/whānau (as relevant)
Evidence that the client/tāngata whaiora has received adequate information regarding their rights and responsibilities related to the treatment offered
Initial opioid agonist dose and expected dose required
Individualised treatment goals (short and long-term) in relation to identified treatment needs – and suggested timeframes
Family/whānau/social interventions (including consideration of children)
Treatment of co-existing problems
Psychological interventions
Work/education plan
Self-help/consumer group linkages
Progress notes document actual treatment being undertaken – evidence of contact with clinical case manager and medical staff, and linkages with other agencies
Record of current medications prescribed; and prescription and dispensing arrangements
Ongoing treatment plans are easily accessible in case notes and include treatment objectives and timeframe – up to date

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 33
E3 Opioid substitution treatment service – clinical records audit tool: treatment monitoring and reviews
Criteria 1 2 3 4 5 6 7 8 9 10
Record of reviews by the prescribing specialist in accordance with OSTPG
Record of regular monitoring of progress by the case worker in relation to short and longer-term treatment plans and updated assessments of risk, in accordance with OSTPG
Progress notes record ongoing contact with the client/tāngata whaiora and where possible significant others/whānau and other providers (including GP and pharmacist) and interventions implemented in keeping with the current treatment plan
Progress notes indicate when withdrawal is considered and clinical reasons why maintenance may be the treatment of choice
Case notes and progress notes indicate how medication complements the psychosocial treatment
Records of case management team reviews exist, and the treatment plan is updated where necessary – last review occurred at the time indicated
Evidence that the client/tāngata whaiora and where possible significant others/whānau and other providers involved in the treatment plan (including the GP and pharmacist) are involved in each review of treatment progress
Evidence of discharge planning as relevant
34 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
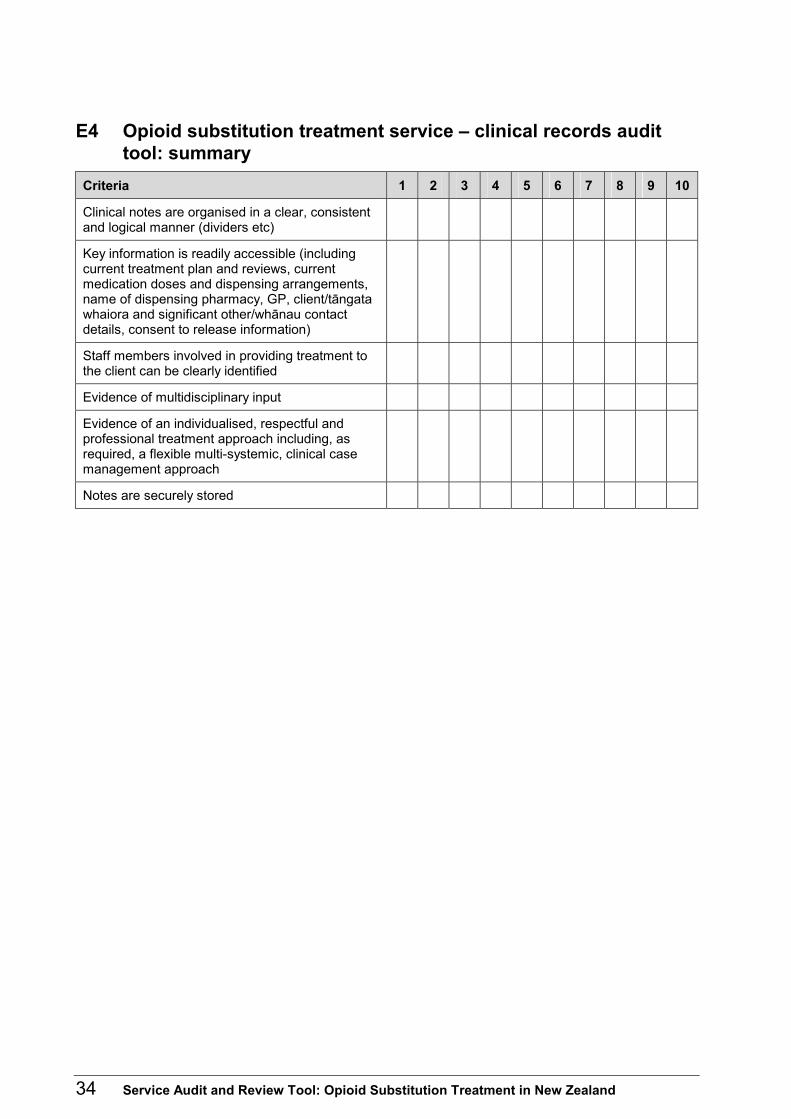
E4 Opioid substitution treatment service – clinical records audit tool: summary
Criteria 1 2 3 4 5 6 7 8 9 10
Clinical notes are organised in a clear, consistent and logical manner (dividers etc)
Key information is readily accessible (including current treatment plan and reviews, current medication doses and dispensing arrangements, name of dispensing pharmacy, GP, client/tāngata whaiora and significant other/whānau contact details, consent to release information)
Staff members involved in providing treatment to the client can be clearly identified
Evidence of multidisciplinary input
Evidence of an individualised, respectful and professional treatment approach including, as required, a flexible multi-systemic, clinical case management approach
Notes are securely stored

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 35
E5 Opioid substitution treatment service – audit tool for methadone or other medication clinical records/files
Record key comments/findings for each file audited on this page. Record/ file number
Notes/comments Total records audited
Clinical record numbers
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.

36 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Part F: Manager, Clinical Head/Team Leader and Staff Interviews
Interviewee and designation: ________________ Opioid substitution treatment service provider: __________________________ Name of unit/team:________________________ Contact person:___________________________ Date: ___________________________________
Guidance notes: manager, clinical head/team leader and staff interviews The mix of staff members interviewed will reflect the particular context of each service provider. The purpose of the interviews is to obtain an overview of service philosophy and objectives, the treatment environment and culture, treatment provided, service delivery practices and clinical pathways, policies and procedures, service directions and any key issues. In other words, they are concerned with establishing whether the treatment is of a high standard with demonstrated commitment within the service to ongoing improvement of the quality of treatment and care. Note: Questions are provided as a guide to interviews. Interviews will need to be flexible to suit the context and the interviewee.
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 37
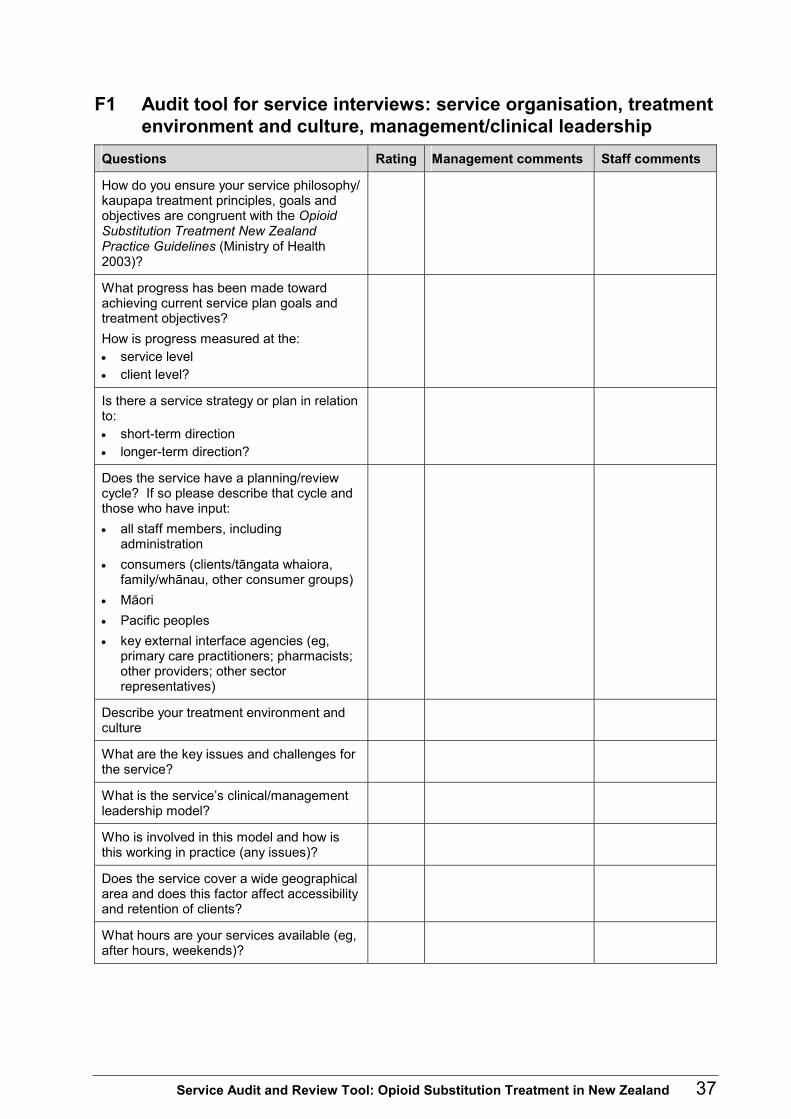
F1 Audit tool for service interviews: service organisation, treatment environment and culture, management/clinical leadership
Questions Rating Management comments Staff comments
How do you ensure your service philosophy/ kaupapa treatment principles, goals and objectives are congruent with the Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003)?
What progress has been made toward achieving current service plan goals and treatment objectives? How is progress measured at the: • service level • client level?
Is there a service strategy or plan in relation to: • short-term direction • longer-term direction?
Does the service have a planning/review cycle? If so please describe that cycle and those who have input: • all staff members, including
administration • consumers (clients/tāngata whaiora,
family/whānau, other consumer groups) • Māori • Pacific peoples • key external interface agencies (eg,
primary care practitioners; pharmacists; other providers; other sector representatives)
Describe your treatment environment and culture
What are the key issues and challenges for the service?
What is the service’s clinical/management leadership model?
Who is involved in this model and how is this working in practice (any issues)?
Does the service cover a wide geographical area and does this factor affect accessibility and retention of clients?
What hours are your services available (eg, after hours, weekends)?

38 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Questions Rating Management comments Staff comments
Are funding and other resources adequate? • Are there any particular issues? • Are clients required to meet any costs?
MoU/protocols. Describe the service’s key interfaces/linkages and quality of relationships with, eg: • primary care teams • alcohol and other drug services • mental health services • Child, Youth and Family • Work and Income • other
How are these relationships maintained, monitored and reviewed (eg, last review)? Are there any issues/planned developments in this area?
How does the service maintain demographic information about the client groups?
What information is provided for individual clinicians?
How is this information used? Give examples.
Are there processes in place for regular monitoring of: • access • waiting times/list and management • client retention in treatment • shared care (with primary sector) • outcome evaluation (client progress) • changing client profiles and needs?
How does this information contribute to service delivery and treatment provision?
What is the quality of the service relationship with consumers? How are areas of conflict managed? Are there any planned developments in this area?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 39
F2 Audit tool for service interviews: policies, protocol and procedures
This section includes service provision frameworks, clinical pathway processes (entry to discharge) and treatment protocols/guidelines. Questions Rating Management comments Staff comments
How are policies, procedures and treatment protocols/ guidelines for your service developed and reviewed?
Who is involved in developing, reviewing and updating policies and procedures?
How do you gain participation from: • consumers/tāngata whaiora including
significant others/whānau • Māori • Pacific peoples • external stakeholders (eg, pharmacists,
GPs)?
How do you ensure policies and procedures reflect current day-to-day practice, OSTPG, National Alcohol and Other Drug Sector Standards, Mental Health Sector Standards and other legislative/key standards? How are they used?
Identify any policy questions (eg, matters not included in prior documentation provided)
How is the tension between individualisation of care and treatment consistency managed?
How are staff members, clients, key interface/linkage providers kept up to date and familiar with changes?
40 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
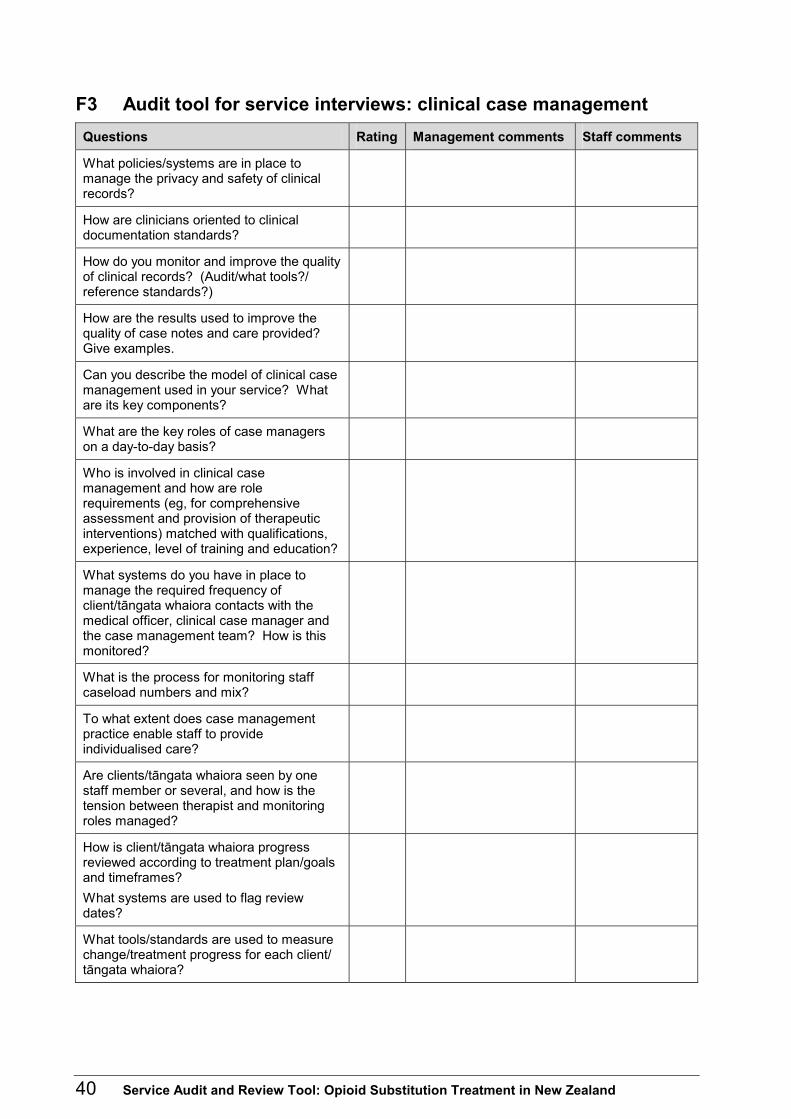
F3 Audit tool for service interviews: clinical case management Questions Rating Management comments Staff comments
What policies/systems are in place to manage the privacy and safety of clinical records?
How are clinicians oriented to clinical documentation standards?
How do you monitor and improve the quality of clinical records? (Audit/what tools?/ reference standards?)
How are the results used to improve the quality of case notes and care provided? Give examples.
Can you describe the model of clinical case management used in your service? What are its key components?
What are the key roles of case managers on a day-to-day basis?
Who is involved in clinical case management and how are role requirements (eg, for comprehensive assessment and provision of therapeutic interventions) matched with qualifications, experience, level of training and education?
What systems do you have in place to manage the required frequency of client/tāngata whaiora contacts with the medical officer, clinical case manager and the case management team? How is this monitored?
What is the process for monitoring staff caseload numbers and mix?
To what extent does case management practice enable staff to provide individualised care?
Are clients/tāngata whaiora seen by one staff member or several, and how is the tension between therapist and monitoring roles managed?
How is client/tāngata whaiora progress reviewed according to treatment plan/goals and timeframes? What systems are used to flag review dates?
What tools/standards are used to measure change/treatment progress for each client/ tāngata whaiora?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 41
Questions Rating Management comments Staff comments
How is outcome information collated/ analysed to provide service planning information? Give trends etc.
How is the involvement of significant others/ whānau actively promoted?
How is the quality of case management evaluated?
Are there regular clinical staff meetings to review and discuss clinical issues/case management? Who co-ordinates these meetings and who attends?
How is discharge planning carried out? Who is involved in planning, who undertakes discharge and who monitors to ensure that the required linkages are in place?
What information is provided to clients/ tāngata whaiora regarding relapse/ re-accessing the service?
42 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
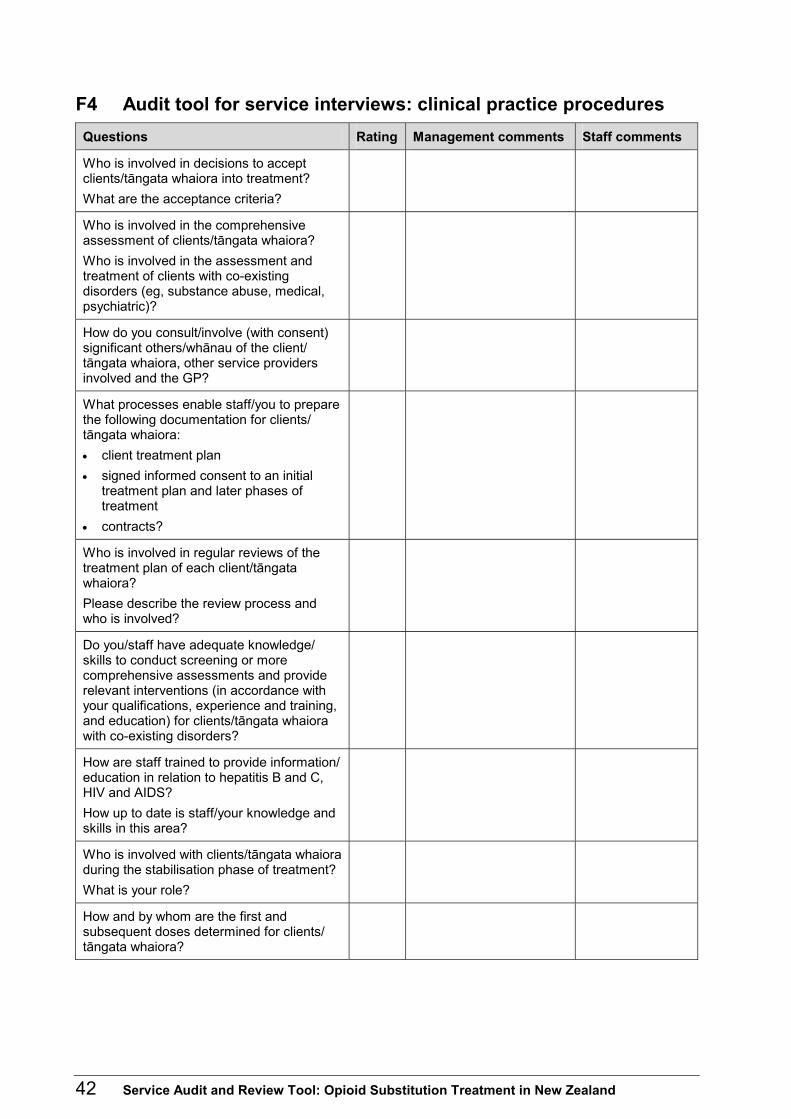
F4 Audit tool for service interviews: clinical practice procedures Questions Rating Management comments Staff comments
Who is involved in decisions to accept clients/tāngata whaiora into treatment? What are the acceptance criteria?
Who is involved in the comprehensive assessment of clients/tāngata whaiora? Who is involved in the assessment and treatment of clients with co-existing disorders (eg, substance abuse, medical, psychiatric)?
How do you consult/involve (with consent) significant others/whānau of the client/ tāngata whaiora, other service providers involved and the GP?
What processes enable staff/you to prepare the following documentation for clients/ tāngata whaiora: • client treatment plan • signed informed consent to an initial
treatment plan and later phases of treatment
• contracts?
Who is involved in regular reviews of the treatment plan of each client/tāngata whaiora? Please describe the review process and who is involved?
Do you/staff have adequate knowledge/ skills to conduct screening or more comprehensive assessments and provide relevant interventions (in accordance with your qualifications, experience and training, and education) for clients/tāngata whaiora with co-existing disorders?
How are staff trained to provide information/ education in relation to hepatitis B and C, HIV and AIDS? How up to date is staff/your knowledge and skills in this area?
Who is involved with clients/tāngata whaiora during the stabilisation phase of treatment? What is your role?
How and by whom are the first and subsequent doses determined for clients/ tāngata whaiora?
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 43
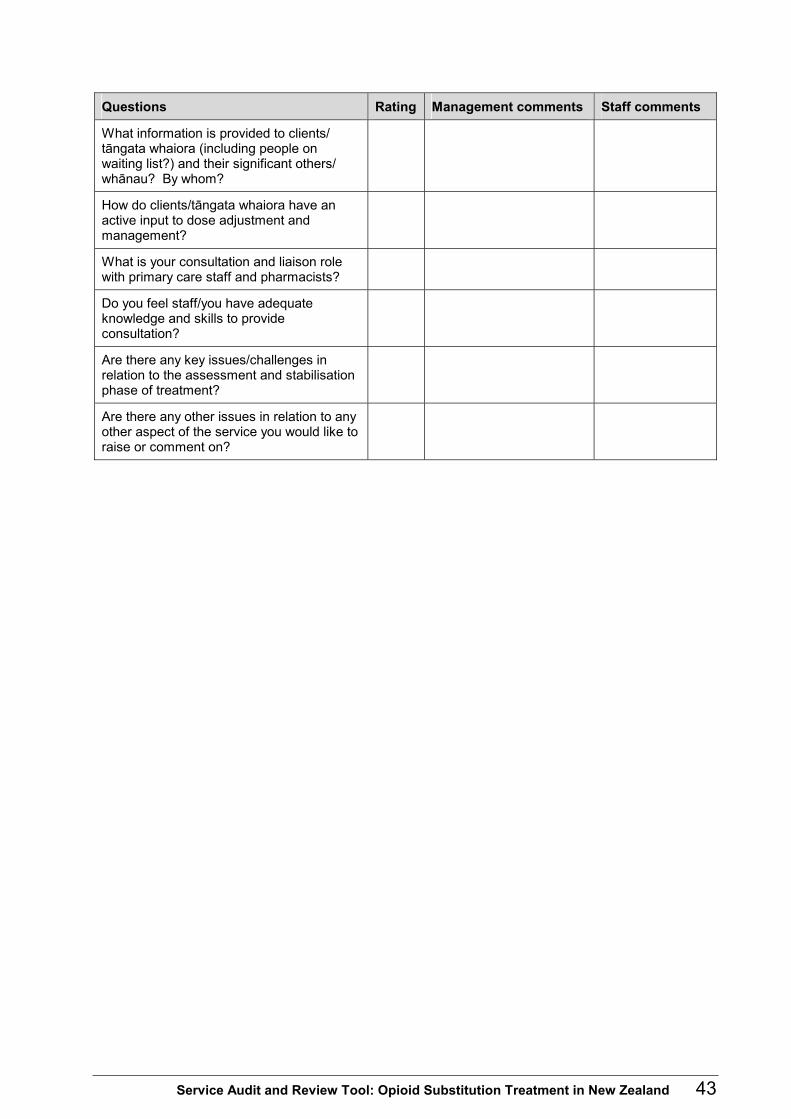
Questions Rating Management comments Staff comments
What information is provided to clients/ tāngata whaiora (including people on waiting list?) and their significant others/ whānau? By whom?
How do clients/tāngata whaiora have an active input to dose adjustment and management?
What is your consultation and liaison role with primary care staff and pharmacists?
Do you feel staff/you have adequate knowledge and skills to provide consultation?
Are there any key issues/challenges in relation to the assessment and stabilisation phase of treatment?
Are there any other issues in relation to any other aspect of the service you would like to raise or comment on?

44 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
F5 Audit tool for service interviews: therapeutic interventions Questions Rating Management comments Staff comments
What is the service/clinician approach and personal philosophy/values related to working with clients/tāngata whaiora of the service?
Please describe the range of therapeutic interventions that are available for tāngata whaiora/clients – provided directly by your service/via referral/shared care etc. Please list and describe in more detail: (check: are these evident in consumer information?)
How do you match interventions to the needs of the client/tāngata whaiora and their significant others/whānau (including needs of children) and ensure the interventions are accessed?
Does the service provide levels of intervention? If so, what are these and how are they monitored and evaluated?
Please identify the support/linkages provided to other agencies that are regularly involved in referral of clients/tāngata whaiora.
What therapeutic approaches/models do clinicians use routinely in day-to-day work with clients/tāngata whaiora?
What treatment protocols/guidelines are available to guide staff members in their interventions?
How do you or your service evaluate the quality of interventions provided?
How do you or your service gain an overview of the quality of service provision of agencies you refer clients/tāngata whaiora to?
Are there any therapeutic intervention gaps or planned developments in this area?
Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 45
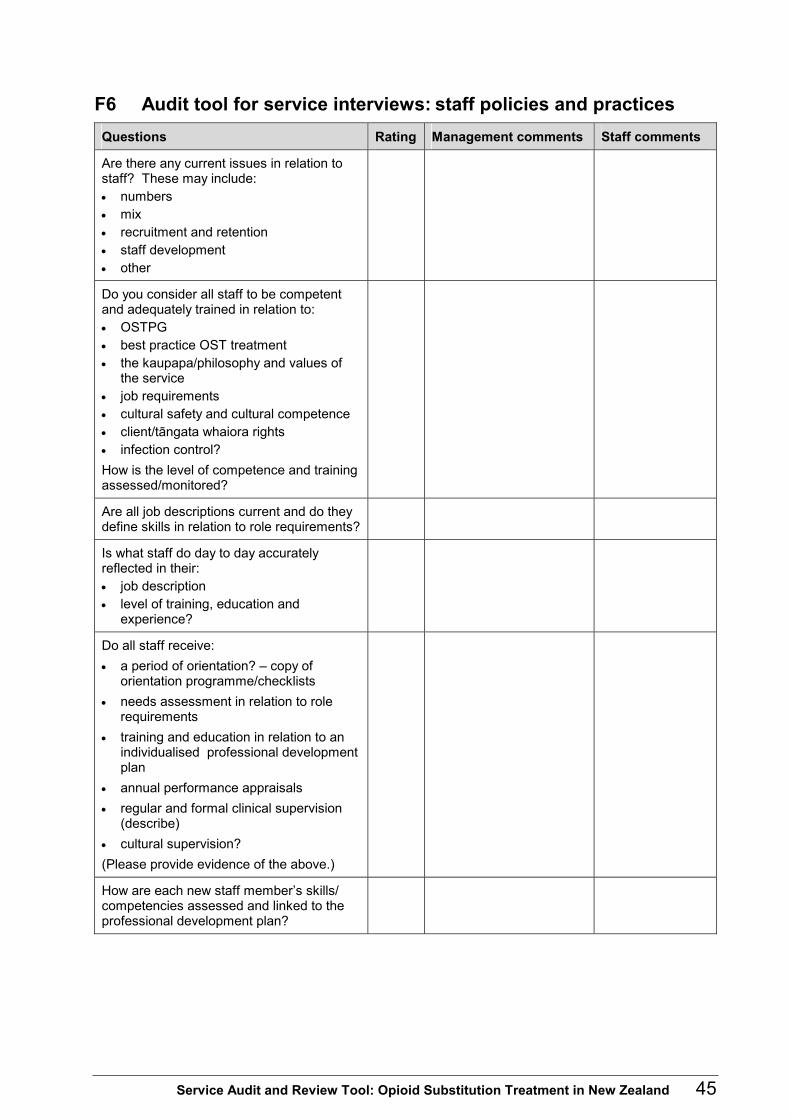
F6 Audit tool for service interviews: staff policies and practices Questions Rating Management comments Staff comments
Are there any current issues in relation to staff? These may include: • numbers • mix • recruitment and retention • staff development • other
Do you consider all staff to be competent and adequately trained in relation to: • OSTPG • best practice OST treatment • the kaupapa/philosophy and values of
the service • job requirements • cultural safety and cultural competence • client/tāngata whaiora rights • infection control? How is the level of competence and training assessed/monitored?
Are all job descriptions current and do they define skills in relation to role requirements?
Is what staff do day to day accurately reflected in their: • job description • level of training, education and
experience?
Do all staff receive: • a period of orientation? – copy of
orientation programme/checklists • needs assessment in relation to role
requirements • training and education in relation to an
individualised professional development plan
• annual performance appraisals • regular and formal clinical supervision
(describe) • cultural supervision? (Please provide evidence of the above.)
How are each new staff member’s skills/ competencies assessed and linked to the professional development plan?

46 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Questions Rating Management comments Staff comments
How is staff development organised, managed and evaluated in relation to transfer of skills to practice? Comment on: • inservice • access to external training, education • any current priorities?
What support mechanisms are available to staff?
What is in place to manage staff safety? Following an incident how can debriefing/ support be accessed?
How are staff issues/conflicts managed? Are there any such issues including philosophical ones, apparent at present?
What liaison links do staff have with workers elsewhere in the alcohol and other drug sector, in primary care, mental health or in other areas?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 47
F7 Audit tool for service interviews: ethno-cultural safety and responsiveness
Questions Rating Management comments Staff comments
What steps are taken to ensure the ethno-cultural needs of clients/tāngata whaiora (eg, women, youth, gay, lesbian) are met?
How do you assess/gain feedback about any barriers that may discourage some people, in particular Māori, from accessing your service? What about feedback on barriers for: • Pacific peoples • other client groups with specific needs?
From your understanding and experience, do you think that the number of Māori clients attending your service or on the waiting list is representative of the number of opioid dependent Māori people in your service’s catchment area?
How do you access the situation for: • Pacific clients • other ethnic/cultural groups with specific
needs?
Are Māori staff employed by your service? Does your service employ: • Pacific staff • staff to meet the needs of specific client
groups?
What systems are in place to ensure tāngata whaiora can access Māori support/ clinical staff?
How are local iwi, kaumatua, etc, involved in any aspects of the treatment programme?
How are representatives of Pacific peoples employed in your service, and what key relationships with Pacific peoples enable cultural input to service development, delivery and evaluation? What are other key ethnic linkages and linkages with representatives of specific client groups?
Are trained interpreters available for assessment and treatment of clients?

48 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
F8 Audit tool for service interviews: GP prescribing Questions Rating Management comments Staff comments
Does your service authorise GPs who do not work in the service to prescribe for particular clients/tāngata whaiora?
What are the criteria for GP prescribing for clients/tāngata whaiora?
What review mechanisms are in place?
What percentage of clients/tāngata whaiora is prescribed for by GPs?
What protocols are in place including for: incident management, consultation and back-up support; and re-entry for clients/ tāngata whaiora to the specialist service when required?
What training/education or supervision arrangements are in place for GPs in your area?
What regular consultation/liaison with GPs occurs?
Are there any particular issues or concerns (eg, issues related to quality of relationship or quality of care)?
F9 Audit tool for service interviews: pharmacy liaison Questions Rating Management comments Staff comments
What consultation/liaison with pharmacists occurs?
Are there specific policies, procedures or treatment protocols in place? What do these cover?
What about incidents that occur – how are these managed?
Are there any training/education or supervision activities in place for pharmacists in your area?
How do you evaluate the quality of the relationship between the service and pharmacists, and the quality of the service provided by pharmacists (eg, last evaluation)?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 49
F10 Audit tool for service interviews: continuous quality improvement
Questions Rating Management comments Staff comments
Who is responsible for quality improvement?
How are staff introduced to/and involved in quality improvement projects internal to the service and/or special projects/staff that are externally provided to the service, eg, consultants?
Does the service have a quality improvement plan or undertake regular quality improvement projects/activities? (Describe.) Are current projects/activities being undertaken?
Does the service set quality indicators? What are these?
What auditing/evaluation mechanisms are in place to ensure policies, procedures and treatment protocols/guidelines reflect the OSTPG, and the Alcohol and Other Drug Sector Standards, the Mental Health Sector Standards and best practice?

50 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Part G: Client/Tāngata Whaiora and Other Consumer Interviews
Interview(s) with: _________________________ Opioid substitution treatment programme/service provider: ________________ Reviewed by: ____________________________ Contact person who arranged interview participants: _____________________ Date: ___________________________________
Guidance notes: client/tāngata whaiora and other consumer interviews Considerable flexibility in approach is required when interviewing clients/tāngata whaiora so that the interview is appropriate for their circumstances. Consideration must be given to the setting of the interviews, number of clients/tāngata whaiora required to be interviewed (as percentage of total clients/tāngata whaiora) and an appropriate cross-section (relating to gender, long-term/ short-term clients/tāngata whaiora, Māori, non-Māori, clients/tāngata whaiora with co-existing disorders, those prescribed by GP and those on the waiting list). Consideration should also be given to the mix of methods that best suits the particular audit. Possible methods include individual interviews, interviews with significant others/whānau, focus groups and interviews/focus groups with wider consumer networks. It is expected that consultation will occur with relevant consumer advisors in relation to gaining client and consumer group perspectives and that a consumer advisor or representative will be actively involved in all phases of the audit process. When inviting clients to participate it is important to emphasise that the interview is about aspects of daily life and what the service is like from the perspective of clients. Interviews do not cover matters relating to the details of the client’s background or the events leading up to entry into the programme. The following questions have been provided as a checklist only to guide discussion. The appropriateness of taking notes will need to be gauged in each individual situation and consent sought from each client/tāngata whaiora. A separate interview form should be used for each interview or focus group involving clients/ tāngata whaiora or other consumers.

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 51
G1 Audit tool for consumer interviews Ref OSTPG Questions (guide only) Check Comments
A Information from client Gender: Ethnicity: Māori/non-Māori Age: Is this your first time on methadone? How long have you been on the programme this time? Is your methadone prescribed by your GP or from the clinic/service? Are you on a waiting list? Y/N (May need to be tailored by the auditors if the client/ tāngata whaiora is now on buprenorphine.)
1.9–1.11
2.14
B Assessment (Note: the initial assessment may be difficult for some interviewees to remember.) At your initial assessment were you asked about: • your expectations of treatment • your alcohol/drug history and your current alcohol/drug
use • your general health and medical history • your mental health (including suicidality) • your legal situation • family/whānau history and current relationships?
Did you undergo urine and blood testing for liver function, hepatitis etc?
Did you receive a description of the opioid substitution treatment programme?
1.14–1.16
2.13
C Decisions about treatment
Before you entered the programme were you made aware of: • your rights and responsibilities • the side effects, limitations, interactions with other
drugs (including alcohol) • eventual transfer to a GP Were your requests for information listened to and responded to appropriately? Did you sign a consent form for treatment? Do you have a copy of the consent form?
1.22–1.24 1.23
D Admission to the programme How long did you have to wait to get on the programme? Were you told how long you would have to wait? Did the service provide you with information, advice and support while you were on the waiting list?
1.18–1.19
2.13
1.54
E Treatment plan Did you develop your treatment plan with your case manager? Did you write it together? Do you have a copy of it? How often do you and your case manager review your treatment plan?

52 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref OSTPG Questions (guide only) Check Comments
Page 7
F Family/whānau and significant other involvement Is the involvement of your family/whānau and others actively encouraged by the clinic/service?
1.45–1.47
3.24
G Case management Do you see your case worker as often you feel you need? Too much/too little? Do you see the doctor as often as you feel you need to? Too much/too little? Do you feel fully involved in decision-making about your treatment? When you meet with your case manager what do you discuss? (Use as prompts:) • Your physical and mental health? • Current drug/alcohol use? • Your dose and takeaway arrangements? How often do you have to do urinalysis tests? Do you have any comments regarding urinalysis tests? Do you have a copy of the service’s policies? Have you ever been offered this information?
2.13–2.17
H Clients rights and complaints Do you feel that your privacy and confidentiality are respected? Would you know how to go about making a formal complaint? If you’ve ever laid a formal complaint, how did the clinical service respond? What action did staff take in response to your complaints? Do you feel that there are barriers to clients/tāngata whaiora making complaints? What are they? Would you know how to access a client advocate if you needed one? Does the clinic/service encourage you to give feedback? Are there opportunities to do so, like suggestion boxes or satisfaction surveys?
I Cultural safety (Begin by explaining that this topic doesn’t refer solely to ethnicity but includes sexual orientation, disability, age, gender.) Do you personally require certain cultural needs to be met? Does the clinic/service meet those needs?
1.15–1.54
1.56
3.7
3.5–3.14
J Dose and dispensing How well does your dose meet your individual needs? Have significant changes been made to your dose (not the usual titration for stabilisation purposes)? If yes, did you or your case manager initiate the change? Was the reason for the change discussed with you so you felt part of the decision-making process? Do you get takeaways? If not, do you know why not? How often are your takeaway arrangements reviewed?
5.0
5.6
K Exit procedures Have you ever been discharged from the programme? Were you given written or verbal warnings prior to your

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 53
Ref OSTPG Questions (guide only) Check Comments
5.7
5.8
5.12
discharge? (Were you offered a supported detoxification?)
(Who made the decision to discharge you?)
Have you felt/did you feel encouraged by the clinic/service to re-enter treatment?
5.0–5.3
L Withdrawal from programme Have you withdrawn from the programme? How long ago? Did you develop a discharge plan with your case manager? Were you able to control how often and at what rate your dose was reduced? Did the service provide support while you withdrew? Did you have a ‘window period’ where you could re-enter the programme if you needed to? If so, who determined this window period?
3.20
M Counselling Has the service/clinic made you aware of opportunities for counselling should you require it?
1.64–1.68
N Transfer to authorised GP How did the clinic/service support your transition to a GP? Were you given information about the expected roles and responsibilities of the GP, the service and yourself? Have you been informed of the conditions under which you can return to or utilise the specialist service?
1.59–1.61
O Transfer between services and regions Have you transferred to this clinic/service from another one in New Zealand? If so were you reassessed by this clinic/service? How long did you have to wait to get onto this programme? Is the clinic/service you transferred to different in any way from the clinic/service you were with before?
1.14
P Prescribing (For clients/tāngata whaiora receiving their treatment from the specialist service) Has the clinic/service discussed having your methadone (or other clinic/service prescribed medication) prescribed by your GP? (For clients/tāngata whaiora with a GP) How long have you been under GP care/receiving your prescription from a GP? Has this arrangement been satisfactory to you?
6.0–6.7
Q Pregnancy When you started on the programme, were you informed about the effects of your medication, alcohol, nicotine and other drug use on the foetus? Have you received that information since? Was there satisfactory liaison between the clinic/service, your GP, midwife, obstetrician etc while you were pregnant?

54 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref OSTPG Questions (guide only) Check Comments
Page 3
R General Are you aware of the goals and objectives of the opioid substitution treatment programme? Are clients/tāngata whaiora involved in the planning, implementation and evaluation of the clinic/service? Are the staff non-judgemental in their attitudes and behaviour towards clients/tāngata whaiora? Give examples?
Do you have any other comments to make about the clinic/ service?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 55
Part H: Interviews with Pharmacists, Authorised GPs and Other Key Interfaces/Linkages
Interviewee and designation: ________________ Opioid substitution treatment service provider: _________________________ Name of unit/service provider:________________________________ Reviewed by: ____________________________ Contact person: __________________________ Date:___________________________________
Guidance notes: interviews with pharmacists, authorised GPs and other key interfaces/linkages The Opioid Substitution Treatment New Zealand Practice Guidelines (Ministry of Health 2003) emphasise a multidisciplinary team approach to working with clients/tāngata whaiora in the process of delivering methadone or other opioid substitution treatment. Those involved in this approach include pharmacists, prescribers and other specialist service and primary health care team members. The OSTPG stress the continuity of care that ranges from intensive intervention and active case management (stabilisation) to ongoing care in the primary health system through appropriately trained and authorised GPs. This part provides a guide to interviews with pharmacists and authorised GPs/primary care teams. It is important that interviews are flexible and reflect the areas of emphasis given in the OSTPG. It is also important to consider the information gained from interviews with authorised GPs/ primary care teams and pharmacists together with information gathered from interviews with clients/tāngata whaiora and other consumers (Part G), specialist service staff (Part F) and the review of documentation (Part B). Such an approach will allow the evaluation of the quality of treatment across the system of care for clients/tāngata whaiora and their significant others/ whānau and the identification of key issues or areas for development and improvement that can inform audit recommendations.

56 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Interviews with other key interfaces/linkages services/personnel (internal or external to the organisation) should be included in the audit. These agencies and referrers include primary care workers/services, other alcohol and other drug services, Child, Youth and Family, Work and Income, Corrections etc, and Medicine Control Advisors. Key linkages/interfaces will vary according to the context (eg, rural, urban or provincial town). The auditor/s should arrange these interviews and keep the discussion fairly general, focusing on accessibility, co-ordination, continuity and integration of care for clients/tāngata whaiora and their significant others/whānau. Areas that could be covered are outlined in the following.
H1 Audit and review tool for interviews with pharmacists Ref OSTPG Questions Check Comments
4.0
4.4–4.28
How many clients/tāngata whaiora do you administer and dispense methadone or other opioid substitution medication to? How would you describe your role and relationship with these clients/tāngata whaiora and their significant others/ whānau? What training/education have you been provided with or undertaken in relation to opioid substitution treatment? Was it: • informal • formal? Was this training/education adequate? Do you see training in this area as important? If so, what aspects of training would be helpful? What peer support or supervision arrangements do you have in relation to your treatment role? How familiar are you with Section 4.0 of the OSTPG on pharmacist administering and dispensing? Do you have procedures in place to minimise the risk of dispensing errors, such as administering a dose that is lower or higher than prescribed or an overdose dose? Do you have any concerns regarding administering or dispensing methadone or other medications? Examples are: • formulation • administering/dispensing instructions • takeaway doses • telephoned prescriptions and authorisation of takeaway
doses • cancellation of administered/dispensed doses • managing risk.

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 57
Ref OSTPG Questions Check Comments
4.23–4.29
4.0
4.1
What policies or procedures do you have in place for if and when clients/tāngata whaiora: • fail to present for their dose • present intoxicated • exhibit abusive or threatening behaviour/disruptive
incidents • attempt to divert medication • are believed to inject dose • exhibit withdrawal symptoms • deteriorate physically, emotionally or mentally? Do you report to the service on incidents that occur with its clients/tāngata whaiora?
What is the quality of your working relationship with: • the opioid substitution treatment service? • authorised GP prescribers/primary care teams? Are there any policies/protocols in place regarding your liaison with the service? Do you have regular communication/liaison meetings with specialist service staff and GP prescribers? What is working well? What are the areas for improvement? Are there any key issues, gaps from your perspective? Is there a satisfactory level of support and timeliness of consultation (eg, regarding client concerns) from the opioid substitution treatment service staff? Does the service have a protocol with pharmacists that relates to takeaway doses? Do you have any other comments about the specialist service or GPs/primary care teams in terms of organisation, treatment provision and service delivery? Any needed developments? Are there any gaps apparent, or any developments or changes needed, in your view, in relation to treatment provided? Are there any other comments you would like to make?

58 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
H2 Audit tool for interviews with authorised GPs Ref OSTPG Questions Check Comments
1.62–1.78 8.25–9.0
1.78
1.0–1.3
3.26–3.33
How long have you been authorised to prescribe methadone by the methadone/opioid substitution treatment service? How many clients/tāngata whaiora do you prescribe for? What is the quality of the working relationship with the specialist service? • What is working well? • What are the areas for improvement? • Are there any key issues/gaps? • Do you have any other comments in relation to this
working relationship? Are other staff members of your practice (eg, receptionist, practice nurse) involved with the clients/tāngata whaiora and their significant others/whānau? What training/education and supervision is provided for these staff members? Do you involve significant others/whānau of the client/ tāngata whaiora? What training/education have you undertaken in relation to opioid substitution treatment and prescribing? Was it: • informal • formal Was this training/education adequate? What peer or other supervision arrangements do you have in relation to your treatment role? How familiar are you with: • Opioid Substitution Treatment New Zealand Practice
Guidelines? • the legal implications of the authorisation? (for named
patients, specified period of time, and in accordance with conditions specified by the authorising medical practitioner)
• the treatment aims of the opioid substitution treatment service
• service policies, philosophy and procedures and protocols/guidelines
• appropriate record keeping • current opioid substitution treatment issues • HIV/AIDS, hepatitis B and C and prevention issues Do you have regular contact with staff from the specialist service?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 59
Ref OSTPG Questions Check Comments
1.62–1.66
1.80
1.66
How often are liaison meetings held? Are they regular? • Who attends? • Are they useful? Is there a documented formal process/protocol for transferring clients/tāngata whaiora from the specialist service to your care? If so does it cover: • prescribing methadone and other drugs • prescribing in general • needed interventions and ongoing contact with the staff
of the specialist service • consultation and liaison (back-up) • monitoring and reviews • process for clients/tāngata whaiora who become
‘unstable’ or who have complex needs • urine testing • management of incidents • discharge planning and discharge itself? If not, what is the understanding you have with the specialist service in relation to: • prescribing opioid substitution and other drugs • needed interventions and ongoing contact with the staff
of the specialist service • consultation and liaison (back-up) • monitoring and reviews • clients/tāngata whaiora who become unstable or have
complex needs • urine testing • management of incidents • discharge planning • other Is there a satisfactory level of support and timely consultation (eg, regarding client management issues) from the opioid substitution treatment service? What client review processes are in place? • Who is involved? • How often are clients/tāngata whaiora reviewed? • Are there any issues in relation to these processes? Are there any major concerns/issues eg, related to attitudes, training, client/tāngata whaiora, service delivery or other? What contact do you or your team have with pharmacists? • Are there any issues in this regard? • Are there areas for development/improvement?
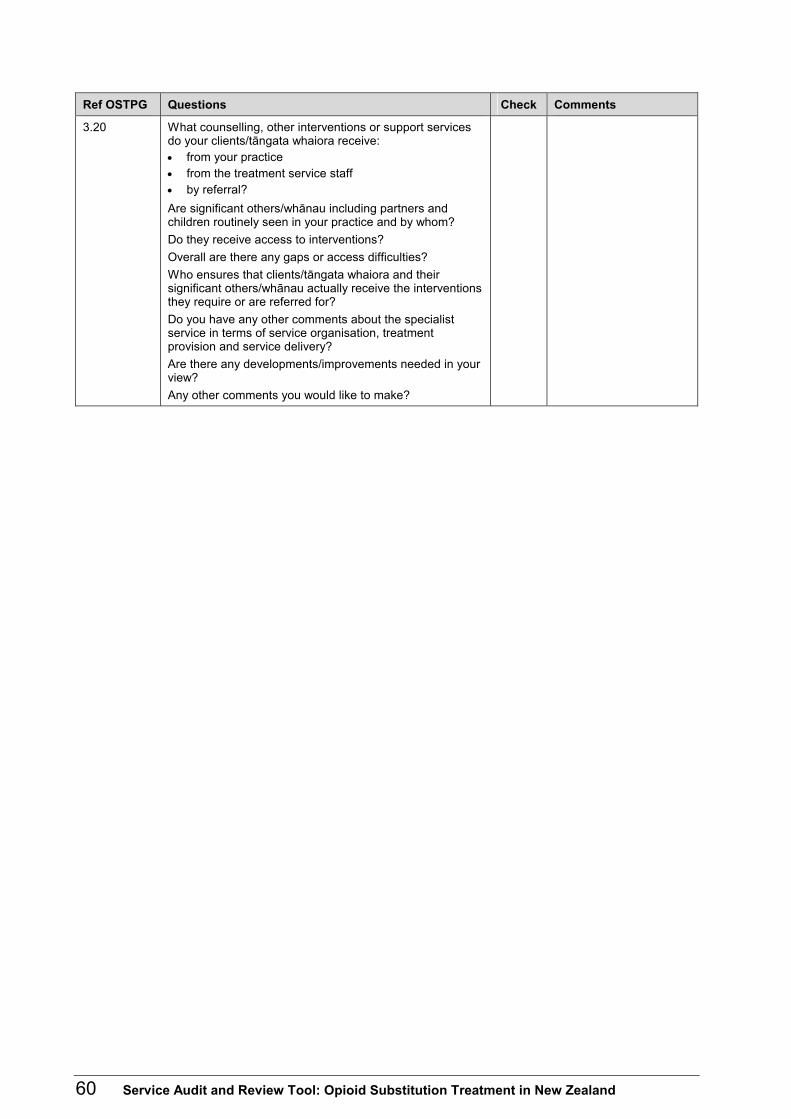
60 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref OSTPG Questions Check Comments
3.20 What counselling, other interventions or support services do your clients/tāngata whaiora receive: • from your practice • from the treatment service staff • by referral? Are significant others/whānau including partners and children routinely seen in your practice and by whom? Do they receive access to interventions? Overall are there any gaps or access difficulties? Who ensures that clients/tāngata whaiora and their significant others/whānau actually receive the interventions they require or are referred for? Do you have any other comments about the specialist service in terms of service organisation, treatment provision and service delivery? Are there any developments/improvements needed in your view? Any other comments you would like to make?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 61
H3 Audit tool for interviews with medicine control advisors, detoxification unit staff and other key interfaces/linkages
Ref OSTPG Questions Check Comments
Medicine control advisors General prescribing practices within the specialist service/other provider • Are there any particular concerns? Authorisation of GPs • Are there any quality issues related to
training/education, supervision or treatment? Liaison with pharmacists • Are there any quality issues regarding
training/education in relation to treatment? Meetings with opioid substitution treatment services/other providers • What is working well? • What could be improved? • Are there any particular issues/concerns/critical
incidents? • Are there areas for joint development or review? • Other comments? Overall delivery of treatment • Do you have any comments on the quality of
treatment/care provided? • What is working well? • What could be improved? • Are there any gaps? • Do you have any particular issues, concerns or critical
incidents that you wish to raise? • Are there any areas for development or review? • Are there any other matters that you wish to raise?
Staff at detoxification units • What is the quality of your working relationship with the
opioid substitution treatment service or other providers of opioid substitution treatment?
• What consultation/liaison mechanisms are in place? • What is the quality of your relationship with clients/
tāngata whaiora? • What is the unit’s role in treatment provision? • What training/education have staff undertaken in
relation to competencies and role requirements of alcohol and other drug practitioners?
• What is working well? • Have there been any critical incidents? • What could be improved? • Are there areas for joint development or review? • Do you have any other comments or concerns?

62 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
Ref OSTPG Questions Check Comments
Other key interfaces/linkages • What is the quality of your working relationship with the
opioid substitution treatment service? • Adequacy of policies and procedures, protocols
/guidelines etc? • What is working well? • What could be improved? • Are MOU/interface protocols or understandings with the
service adequate? • What consultation/liaison mechanisms are in place? • Do you have any comments on the quality of
treatment/care provided? • Are there any gaps? • Have there been any critical incidents? • Are there areas for joint development or review? • Do you have any particular issues/concerns?

Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand 63
References and Further Reading Amato L, Davoli M, Ferri M, et al. 2002. Methadone at tapered doses for the management of opioid withdrawal (Cochrane Review). Cochrane Database Syst Rev (1): CD003409.
Deering D, Huriwai T, Sellman JD. 1998. Guidelines for Clinical Process Self-Evaluation in Alcohol and Drug Treatment Agencies. Wellington: Alcohol Advisory Council of New Zealand.
Lenne M, Lintzeris N, Breen C, et al. 2001. Withdrawal from methadone maintenance treatment: prognosis and participant perspectives. Aust NZ J Public Health 25(2): 121.5.
Lilly R, et al. 1999. Juggling multiple roles: staff and client perceptions of key worker roles and the constraints on delivering counselling and support services in methadone treatment. Addiction Research 7(4): 267–89.
Magura S, et al. 1999. Program quality effects on patient outcomes during methadone maintenance: a study of 17 clinics. Substance Use and Misuse 34(9): 1299–324.
McLellan AT, et al. 1998. Supplemental social services improve outcomes in public addiction treatment. Addiction 93(10): 1489–99.
Ministry of Health. 2002. Towards Clinical Excellence: An introduction to clinical audit, peer review and other clinical practice improvement activities. Wellington: Ministry of Health.
Ministry of Health. 2003. Opioid Substitution Treatment New Zealand Practice Guidelines. Wellington: Ministry of Health.
National Treatment Agency For Substance Misuse. 2004. Methadone Dose and Methadone Maintenance. United Kingdom: National Treatment Agency for Substance Misuse.
National Treatment Agency For Substance Misuse. 2004. More Than Just Dose: Enhancing treatment outcomes for methadone maintenance. United Kingdom: National Treatment Agency for Substance Misuse.
Ramsden I. 1997. Cultural Safety: Implementing the concept. In: Te Whaiti P, McCarthy M, Durie A (eds) Mai I Rangi Atea: Māori wellbeing and development. Auckland University Press, Auckland.
Sievewright N. 2000. Community Treatment of Drug Misuse: More than methadone. United Kingdom: Cambridge University Press.
Relevant legislation and guidelines The audit team should be aware of the following legislation and relevant guidelines:
• ALAC. 2001. Practitioner Competencies for Alcohol and Drug Workers. Wellington: Alcohol Advisory Council of New Zealand.
• Code of Health and Disability Services Consumers Rights, 1996.
• Community Liaison Committee, Royal Australian and New Zealand College of Psychiatrists. 2000. Involving Families: Guidance notes. Guidance for involving families and whanau of mental health consumers/tangata whaiora in care, assessment and treatment processes. Wellington: Ministry of Health.
• Deering D, Huriwai T, Sellman JD. 1998. Guidelines for Clinical Process Self-Evaluation in Alcohol and Drug Treatment Agencies. Wellington: Alcohol Advisory Council of New Zealand.

64 Service Audit and Review Tool: Opioid Substitution Treatment in New Zealand
• Health Information Privacy Code 1994. • Ministry of Health. 1995. A Guide to Effective Consumer Participation in Mental Health Services.
Wellington.
• Ministry of Health in partnership with Health Funding Authority. 1998. Guideline for Clinical Risk Assessment and Management in Mental Health Services. Wellington: Ministry of Health.
• Ministry of Health. 2002. Towards Clinical Excellence: An introduction to clinical audit, peer review and other clinical practice improvement activities. Wellington: Ministry of Health.
• Misuse of Drugs Act 1975.
• National Service Framework for Mental Health Services. (The Operational Policy Framework – 2004. Available only to District Health Boards via email [email protected])
• O’Hagan M. 2001. Recovery Competencies for New Zealand Mental Health Workers. Wellington: Mental Health Commission.
• Todd F, Sellman JD, Robertson PJ. 1999. The Assessment and Management of People with Co-existing Substance Use and Mental Health Disorders. Wellington: Alcohol Advisory Council, Ministry of Health and Mental Health Commission.