sensation & perception. 17 – somatosensation touch heat/cold pain
Post on 18-Dec-2015
220 views
TRANSCRIPT

ΨΨSensation
&
Perception

ΨΨ17 – Somatosensation
Touch
Heat/Cold
Pain

Administrative stuff

The final
• Friday, December 10th, 10.30 am -12.30 pm
• In HGS 101
• Comprehensive, with an emphasis on things that haven’t been covered in previous exams.
• Like the midterms. Interpreting graphs, drawing diagrams, multiple choice and short written answers.

The early final
• For graduating seniors• Their grades have to be in by Dec the 3rd. • Format is similar as in regular final• This leaves only one day: Dec the 2nd. • But when on the 2nd? Someone has a mandatory
class from 11-12, someone else has another final from 2.30.
• What about really early (9 – 11 am) or really late (5-7 pm)?

The Review session
• When?
• Where?

Auditory system
PostScript

Young adults are most sensitive for frequencies corresponding to human speech

Range of audible frequencies of several species at 60 dB SPL. No species covers the whole range.

SomatosensationTouch
TemperaturePain

“Organ”: The skin

SomatosensationTouch
TemperaturePain

The skin receptors (transducers)

The skin receptors (transducers)
a) Merkel b) Meissner
c) Ruffini d) Pacinian

The skin receptors (transducers)
• Meissner corpuscle, shallow, stack of cells
• Merkel disk, shallow, disk-shaped
• Ruffini endings, deep, branched cylinder
• Pacinian corpuscle, very deep, onion-like

Spatiotemporal fiber properties
Time constants
short long
RF
structure
Small, Sharp
boundaries
Large, fuzzy
boundaries
Rapidly adapting, punctate
(RA-P)
Slowly adapting, punctate
(SA-P)
Rapidly adapting, diffuse
(RA-D)
Slowly adapting, diffuse
(SA-D)

The skin receptors (transducers)
• Meissner corpuscle: RA-P
• Merkel disk: SA-P
• Ruffini endings: SA-D
• Pacinian corpuscle: RA-D

Spatiotemporal fiber properties
Time constants
short long
RF
structure
Small, Sharp
boundaries
Large, fuzzy
boundaries
(RA-P) (SA-P)
(RA-D) (SA-D)
Meissner Corpuscle
Merkel Disk
Pacinian Corpuscle
Ruffini Ending

The skin receptors (transducers)
• Meissner corpuscle. Hooked up to RA-P fibers.• Optimal stimulus: Pressure. Perception: Flutter.
• Merkel disk. Hooked up to SA-P fibers.• Optimal stimulus: Light tapping. Perception: Pressure.
• Ruffini endings. Hooked up to SA-D fibers.• Optimal stimulus: Lateral Stretching. Perception: Stretch.
• Pacinian corpuscle. Hooked up to RA-D fibers.• Optimal stimulus: Vibration. Perception: Vibration.

One last word on skin receptors…
• Merkel disks = Merkel discs = Merkel receptors
• Ruffini endings = Ruffini cylinders
• SA-P = SA-1, SA-D = SA2
• RA-P = RA-1, RA-D = RA2

On receptive fields on the skin
• The vision analogy holds
• Somatosensory receptive fields have a antagonistic center-surround structure
• For the following experiment, have two sharp (but relatively blunt) objects like toothpicks or pen-points ready.
• If you hurt yourself, don’t sue anyone.

On receptive fields on the skin
Excitatory region
Inhibitory region

On receptive fields on the skin
1 stimulus in excitatory region:
Feels like 1 strong point

On receptive fields on the skin
2 stimuli in excitatory regions, far apart:
Feels like 2 separate strong points

On receptive fields on the skin
2 stimuli in excitatory regions, close together (both inhibiting and exciting each other)
Feels like 1 point

On receptive fields on the skin
2 stimuli in excitatory regions, intermediate distance (each inhibits the other)
Feels like 2 weak points

Relative sensitivity of body parts
• This rationale (measuring the two-point-threshold) was used to elicit the absolute sensitivity of different regions of skin.
• It allows to infer the spacing of receptive fields and – in turn the spatial resolution of a given skin region for a given body part.
• This was done very early (as early as 1880), using a compass.

2-point Thresholds on skin

Pathways for touch
• Afferent touch fibers enter the spinal cord in the dorsal root.
• Some of the fibers synapse onto local inter-neurons which in turn synapse onto motor neurons, implementing a spinal reflex arc (like a withdrawal reflex)

Ascending pathways for touch
• Other fibers travel upward to the brain, carrying touch-information to the brain-stem.
• They are in the lemniscal pathway
• After synapsing in the brainstem, fibers cross to the opposite side of the brain.
• After synapsing in the thalamus, these neurons project to cortical areas.

Cortical processing of touch
• The projection area is the somatosensory cortex (S1, S2)
• It is situated immediately posterior of the central sulcus.
• Both S1 and S2 contain a full sensory MAP of the body.

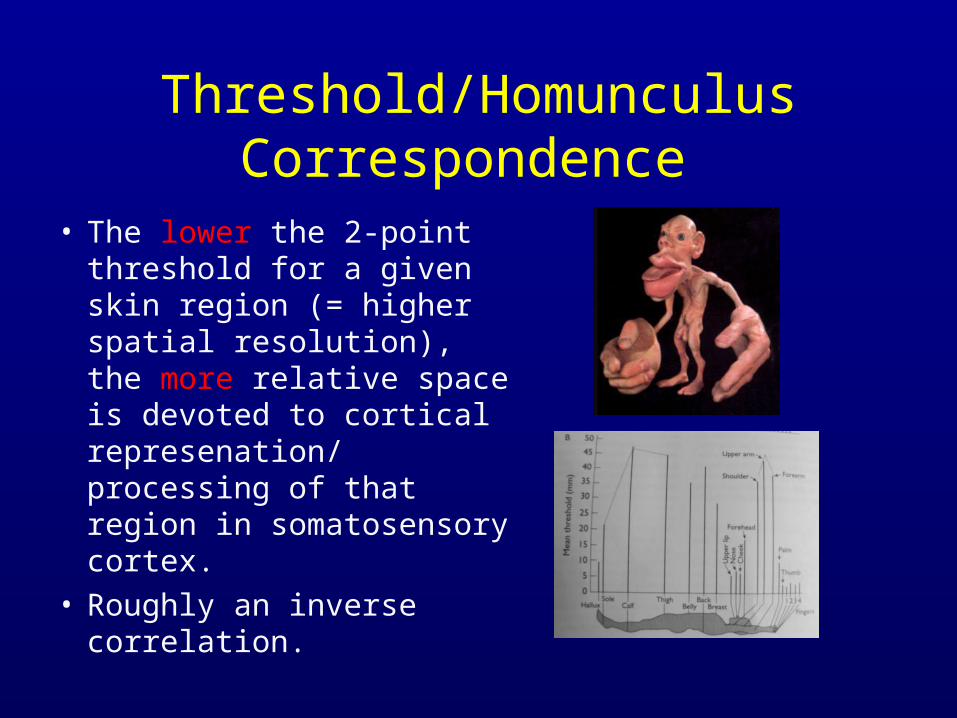
Threshold/Homunculus Correspondence
• The lower the 2-point threshold for a given skin region (= higher spatial resolution), the more relative space is devoted to cortical represenation/ processing of that region in somatosensory cortex.
• Roughly an inverse correlation.

Sidenote
• Recently, the analogy between retinotopic mapping in vision and somatotopic mapping in somatosensation has come under fire.
• Critics of this model argue that there are many more body maps in the somatosensory cortices
• They also argue that the mapping is much more distributed and not somatotopic.
Homunculus model too nice to be true.

Another analogy to vision
• Just like in the case of eye movements, where the brain needs to know if the eyes moved or the world moved, an efference copy is sent from the motor system to the sensory system.
• In the case of the somatosensory system, this is the somatosensory cortex.
• This is the reason why one can’t tickle oneself. The body knows that it’s not an external stimulus and takes it into account (dismissing it).

Somatosensory efference copy and tickling
• If one is instructed to push oneself and then push another person with the same force, the other person experiences this as a much stronger push (escalation)
• Blakemore et al. (1998):

By the way
• Brodmann Areas 1,2,3
• = Somatosensory cortex
• = S1, S2
• =Postcentral gyrus
• =Postcentral cortex

SomatosensationTouch
TemperaturePain

Thermoreceptors

Thermoreceptors
• Free nerve endings act as thermoreceptors• There are separate classes of thermoreceptors:
“Cold fibers” and “Warm fibers” • Cold fibers respond to a decrease in
temperature, while warm fibers respond to an increase in temperature.
• An individual fiber has a preferred temperature (exhibits a temperature tuning curve just like V1 neurons are tuned for orientation)

Thermoreceptors
• Both cold and warm fibers don’t respond to mechanical pressure.
• Preferred temperatures of cold fibers range from 20º C to 45º C, while preferred temperatures of warm fibers range from 30º C to 48º C.
• This response to a preferred temperature is a sustained response, it doesn’t adapt like the additional increase/decrease response discussed previously.

Thermoreceptor tuning curves
• Explains “paradoxical cold”• Jumping into a very hot bath transiently activates
both hot and cold fibers.• For a short time, the bath feels both hot and cold
Cold
Hot

Higher temperature processing
• Temperature information reaches the brain via the spinothalamic tract in the spinal cord.
• It’s target in the brain is both Somatosensory cortex, but also Insular cortex.

SomatosensationTouch
TemperaturePain

Pain as a special perceptual quality
• A quality that has complex phenomenological facets (behavioral, sensory, emotional)
• Pain perception can be modulated by all kinds of factors, including behavioral states (stress, sex), cognitive states (hypnosis), mental states (“trance”), social norms and drugs.
• It’s significance for society is enormous. E.g.: Should fishing be legal?
• Evolutionary significance to organism obvious.

Pain is not a purely sensory experience
• It shares components of an emotion (distress that is associated with pain).
• But it also shares sensory characteristics. It signals the presence of stimuli that are harmful to the organism.

Pain receptors• Free nerve endings in the skin
• They are connected to various fibers:
• Aδ – small, myelinated. High conductance speed
• C – small, unmyelinated. Slow conductance speed

Pain receptors
• Aδ – fast, sensitive to mechanical noxious stimuli.• C – slow, sensitive to many noxious stimuli
(chemical, etc.)• This distinction has been used to explain the
phenomenon of double-pain:• One noxious stimulus causes first a quick, sharp
pain (mediated by Aδ fibers) and is followed by a dull and burning pain (mediated by C fibers)

Pain pathways
• Pain information also reaches the brain via the spino-thalamic tract.
• There are projections to the Somatosensory cortex and the Anterior cingulate cortex

Cortical pain processing• Sensory aspects of pain seem to be processed in the
Somatosensory cortex.
• Emotional distress associated with pain seems to be processed in the Anterior Cingulate Cortex (ACC).
• Subjects with lesions in ACC could still accurately judge the intensity of pain. But they were not in the least bothered by it.
• On the other hand, subjects empathy for the pain of others only elicits activity in ACC, not Somatosensory cortex.

The Gate control theory
• Devised by Melzack & Wall (1965)• Tries to explain the fact that pain intensity can be
cognitively (top-down) controlled.• Components of the model: • Large fibers (involved in touch)• Small fibers (involved in Pain perception)• Substantia gelatinosa (the gate)• T-cells (Transmission cells, sending pain signals to
the brain)• If T-cells are sufficiently active, we experience pain.

The Gate control theory
•The large fibers are under cognitive control. If they are active, they activate the substantia gelatonisa (sg) in the spinal cord.
•If the sg is active, the activity of T-cells is diminished.
•If the T-cells don’t reach their activity threshold, no pain is experienced.
•If small fibers are active first, sg is inhibited, both fibers increase T-activity

Explanatory power of the theory
• Cognitive factors can diminish pain experience. Large fibers have descending tracts.
• Chemical Analgesics act to inhibit small fibers, disinhibiting the sg reducing pain.
• Rubbing the skin around a hurting area reduces pain by activating large (touch-sensitive) fibers, activating sg reducing pain.
• This effectively implements a peripheral pain control

Central control of pain
• There is a system of endogenous opiates and corresponding receptors in the brain.
• Endogenous opiates are particularly enkephalins and endorphins.
• In situations of stress, release of endorphins reduces the expected pain centrally.
• Morphine also acts on these endogenous opiate receptors.