selective brafv600e inhibition enhances t-cell recognition...
TRANSCRIPT
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
Priority Report
CancerResearch
Selective BRAFV600E Inhibition Enhances T-Cell Recognition ofMelanoma without Affecting Lymphocyte Function
Andrea Boni, Alexandria P. Cogdill, Ping Dang, Durga Udayakumar, Ching-Ni Jenny Njauw, Callum M. Sloss,Cristina R. Ferrone, Keith T. Flaherty, Donald P. Lawrence, David E. Fisher, Hensin Tsao, and Jennifer A. Wargo
Abstract
Authors' ADermatolog
Note: SuppOnline (http
CorresponMedical OnFruit Stree3895; E-ma
doi: 10.115
©2010 Am
www.aacr
Do
Targeted therapy against the BRAF/mitogen-activated protein kinase (MAPK) pathway is a promising newtherapeutic approach for the treatment of melanoma. Treatment with selective BRAF inhibitors results in ahigh initial response rate but limited duration of response. To counter this, investigators propose combiningthis therapy with other targeted agents, addressing the issue of redundancy and signaling through differentoncogenic pathways. An alternative approach is combining BRAF/MAPK-targeted agents with immunotherapy.Preliminary evidence suggests that oncogenic BRAF (BRAFV600E) contributes to immune escape and that block-ing its activity via MAPK pathway inhibition leads to increased expression of melanocyte differentiation anti-gens (MDA). Recognition of MDAs is a critical component of the immunologic response to melanoma, andseveral forms of immunotherapy capitalize on this recognition. Among the various approaches to inhibitingBRAF/MAPK, broad MAPK pathway inhibition may have deleterious effects on T lymphocyte function. Here,we corroborate the role of oncogenic BRAF in immune evasion by melanoma cells through suppression ofMDAs. We show that inhibition of the MAPK pathway with MAPK/extracellular signal-regulated kinase kinase(MEK) inhibitors or a specific inhibitor of BRAFV600E in melanoma cell lines and tumor digests results inincreased levels of MDAs, which is associated with improved recognition by antigen-specific T lymphocytes.However, treatment with MEK inhibitors impairs T lymphocyte function, whereas T-cell function is preservedafter treatment with a specific inhibitor of BRAFV600E. These findings suggest that immune evasion of melano-mas mediated by oncogenic BRAF may be reversed by targeted BRAF inhibition without compromising T-cellfunction. These findings have important implications for combined kinase-targeted therapy plus immunother-apy for melanoma. Cancer Res; 70(13); 5213–9. ©2010 AACR.
Introduction
Melanoma is a major world health problem with an inci-dence that is increasing at a rate faster than any other solidmalignancy. The overall survival for patients with metastaticmelanoma is poor (1, 2), and novel forms of treatment areneeded.Key genetic alterations have been identified in melanomas,
resulting in increased oncogenic potential (3). A better un-derstanding of these oncogenic signaling pathways has stim-ulated interest in therapeutic strategies targeting molecularmechanisms. Somatic mutations in the BRAF oncogene oc-cur in most melanomas, with >60% of melanomas harboringan activating point mutation in a specific codon of the BRAF
ffiliation: Division of Surgical Oncology, Medical Oncology, andy, Massachusetts General Hospital, Boston, Massachusetts
lementary data for this article are available at Cancer Research://cancerres.aacrjournals.org/).
ding Author: Jennifer A.Wargo, Division of Surgical Oncology,cology, and Dermatology, Massachusetts General Hospital, 55t, Boston, MA 02114. Phone: 617-643-6195; Fax: 617-724-il: [email protected].
8/0008-5472.CAN-10-0118
erican Association for Cancer Research.
journals.org
Researcon Februarycancerres.aacrjournals.org wnloaded from
gene (V600E; ref. 4). This leads to constitutive activation ofthe mitogen-activated protein kinase (MAPK) signaling path-way and increased oncogenic potential through a variety ofmechanisms, including reduced apoptosis, increased inva-siveness, and increased metastatic behavior (3).Various inhibitors of BRAF and the MAPK signaling path-
way have been tested in clinical trials. Treatment with a se-lective MAPK/extracellular signal-regulated kinase (ERK)kinase (MEK) inhibitor yielded modest response rates(12%) among patients with a known BRAF mutation in aphase II trial involving melanoma (5). Preliminary results ofa phase I/II trial with a selective BRAF inhibitor suggest thatobjective responses are seen in the majority of patientswhose tumors harbor BRAFV600E (6). However, even the mostencouraging of these agents yielded a median duration ofresponse of only 8 months.Functional redundancy and compensatory activity through
alternate signaling pathways might explain the low responserates to MEK inhibitors and the emergence of resistance seenin patients treated with selective BRAF inhibitors (7, 8). Toaddress these issues, combination of BRAF/MAPK-targetedtherapy with other signal transduction inhibitors or withconventional chemotherapy has been proposed (9).Another potential approach involves combining BRAF/
MAPK-targeted therapy with immunotherapy. To date,
5213
h. 7, 2019. © 2010 American Association for Cancer

Boni et al.
5214
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
one of the most successful forms of immunotherapy incor-porates adoptive transfer of autologous T lymphocytes af-ter a lymphodepleting preconditioning regimen (10).However, this type of therapy is limited by the ability togenerate tumor-reactive T cells and by the technical andfinancial resources required (11). An important variant in-volves the genetic modification of patient's peripheralblood lymphocytes (PBL) to express T-cell receptors(TCR) targeting melanocyte differentiation antigens(MDA) for use in adoptive transfer. This strategy hasshown promise in generating antitumor responses in clin-ical trials of patients with melanoma (12) but requiresantigen expression by the tumor cells. Other immune-mediated approaches such as vaccines, monoclonal antibo-dies, and cytokines are also available but are associatedwith lower response rates (13, 14).The rationale for combination targeted therapy–immu-
notherapy is based on evidence that MAPK pathway in-hibition leads to increased expression of MDAs (15).Recognition of antigens (including MDAs) is central tomelanoma immunotherapy. This is supported by findingsthat loss of antigen expression can lead to relapse afterimmunotherapy (16).We sought to test the hypothesis that treatment of mel-
anoma cell lines with MEK inhibitors or a specific BRAFinhibitor would increase the expression of MDAs, resultingin improved recognition by MART-1–specific and gp100-specific T lymphocytes. We analyzed the effect of severaldifferent MAPK pathway inhibitors on T-cell function toprovide a basis for rational combinations of systemic tar-geted therapy and immunotherapy for melanoma.
Materials and Methods
Cell lines and tumor digestsMelanoma cell lines 888 MEL, 624 MEL, and 1300 MEL
were provided by the Surgery Branch, National Cancer Insti-tute (NCI). Melanoma cell lines SKMEL28, UACC903, andMel-Juso were provided by Dr. Hensin Tsao (MassachusettsGeneral Hospital, Boston, MA). Fresh tumor digests wereisolated from patients with metastatic melanoma enrolledon a tissue procurement protocol. All cell lines/digests weregenotyped for BRAF mutation. Melanoma lines/digests werecultured in RPMI 1640 containing 10% fetal bovine serum at37°C in 5% CO2.
ChemicalsMEK inhibitors U0126 and PD0325901 were obtained from
Cell Signaling Technology. The BRAF-V600E inhibitorPLX4720 was obtained from Symansis.
Quantitative PCRDifferential expression of MDAs in melanoma lines was
validated using Taqman Gene Expression Assays (AppliedBiosystems) with glyceraldehyde-3-phosphate dehydrogenaseas control. Total RNA (250 ng) was used as template, and Su-perScript III Platinum kit (Invitrogen) was used for one-stepquantitative reverse transcription-PCR in a 25 μL reaction.
Cancer Res; 70(13) July 1, 2010
Researcon Februarycancerres.aacrjournals.org Downloaded from
TCR transduction of PBLsRetroviral vectors with TCR specific for the MART-1 and
gp100 antigens were provided by the Surgery Branch, NCI.A green fluorescent protein (GFP)–encoding vector servedas negative control. PBLs were obtained from melanomapatients on protocol and stimulated in vitro and trans-duced with TCR-encoding retroviral vectors as previouslydescribed (12).
Flow cytometric analysisMelanoma cell lines were stained with intracellular stains
for MART-1 using a phycoerythrin-conjugated antibody(Santa Cruz Biotechnology) and for surface staining ofHLA class I expression using β2-microglobulin. TransducedPBLs were stained for MART-1 and gp100 tetramer, CD3,CD4, and CD8. Intracellular staining was also performedfor IFN-γ. Cells were analyzed on a FACSCalibur instrument(BD Biosciences), and data were analyzed using FlowJo soft-ware (Tree Star).
ImmunofluorescenceMelanoma cell lines were cultured on glass slides and trea-
ted as described. Cells were fixed and stained with a mono-clonal antibody targeting MART-1 and a FITC-conjugatedsecondary antibody (Abcam). Images were acquired using aNikon Eclipse-80i fluorescence microscope.
Cytokine release assayIFN-γ release was measured using commercially available
ELISA kits (IFN-γ; Endogen).
Cell viability assay for T cells treated with MEK orBRAF inhibitorsPBLs were treated for 3 days with either U0126 or
PLX4720. Each cell sample was then collected and assayedfor viability using CellTiter-Glo Luminescent Cell ViabilityAssay from Promega.
Results
MAPK pathway inhibition increases expression ofMDAs in melanoma cell lines and fresh tumor digestsGiven the critical role of the MAPK signaling pathway in
melanoma, we sought to investigate the role of oncogenicBRAF in modulating expression of MDAs. We expanded onprior literature by increasing the number of antigens assayedand also by testing the effects of treatment with a specificinhibitor of BRAFV600E. Melanoma cell lines were treatedwith two specific MEK inhibitors (U0126 and PD0325901),and mRNA levels of gp100, MART-1, Tyrp-1, and Tyrp-2 wereanalyzed. We observed a significant increase in mRNA levelsfor all four genes after treatment with MEK inhibitors,regardless of BRAF mutational status. In contrast, treatmentof melanoma cell lines with a selective inhibitor of BRAFV600E
(PLX4720; ref. 17) increased antigen expression only in BRAF-mutant lines (Fig. 1A). Fresh tumor digests were also treatedwith these agents, showing similar results (Fig. 1B). Westernblot analysis showed that suppression of phospho-ERK
Cancer Research
h. 7, 2019. © 2010 American Association for Cancer

BRAF Inhibition Enhances Recognition of Melanoma
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
Figure 1. MAPK pathway inhibition increases mRNA expression of MDAs. mRNA levels of gp100, MART-1, Tyrp-1, and Tyrp-2 in melanoma cell lines(A) and fresh tumor digest (B) treated with MEK inhibitors U0126 (10 μmol/L) and PD0325901 (0.2 μmol/L) or with the selective BRAFV600E inhibitorPLX4720 (1 μmol/L). Expression levels are shown as fold increase over the untreated control (X axis). Experiments were repeated at least three timeswith similar results.
Cancer Res; 70(13) July 1, 2010www.aacrjournals.org 5215
Research. on February 7, 2019. © 2010 American Association for Cancercancerres.aacrjournals.org Downloaded from
Boni et al.
5216
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
correlated with upregulation of MDAs (Supplementary Fig. S1).There was no change in HLA class I expression (Supplemen-tary Fig. S2). Expression of MDAs was proportionally upregu-lated in each cell line, although the level of induction variedsignificantly between different melanoma cell lines (e.g.,2-fold induction in 888 MEL versus 100-fold induction inUACC903), a point that will be discussed further later.
Increased expression of MDAs is associated withincreased antigen-specific T-cell recognitionNext, we performed studies to test the ability of MAPK
pathway inhibition to induce protein expression of MDAsand to improve antigen-specific recognition by T cells target-
Cancer Res; 70(13) July 1, 2010
Researcon Februarycancerres.aacrjournals.org Downloaded from
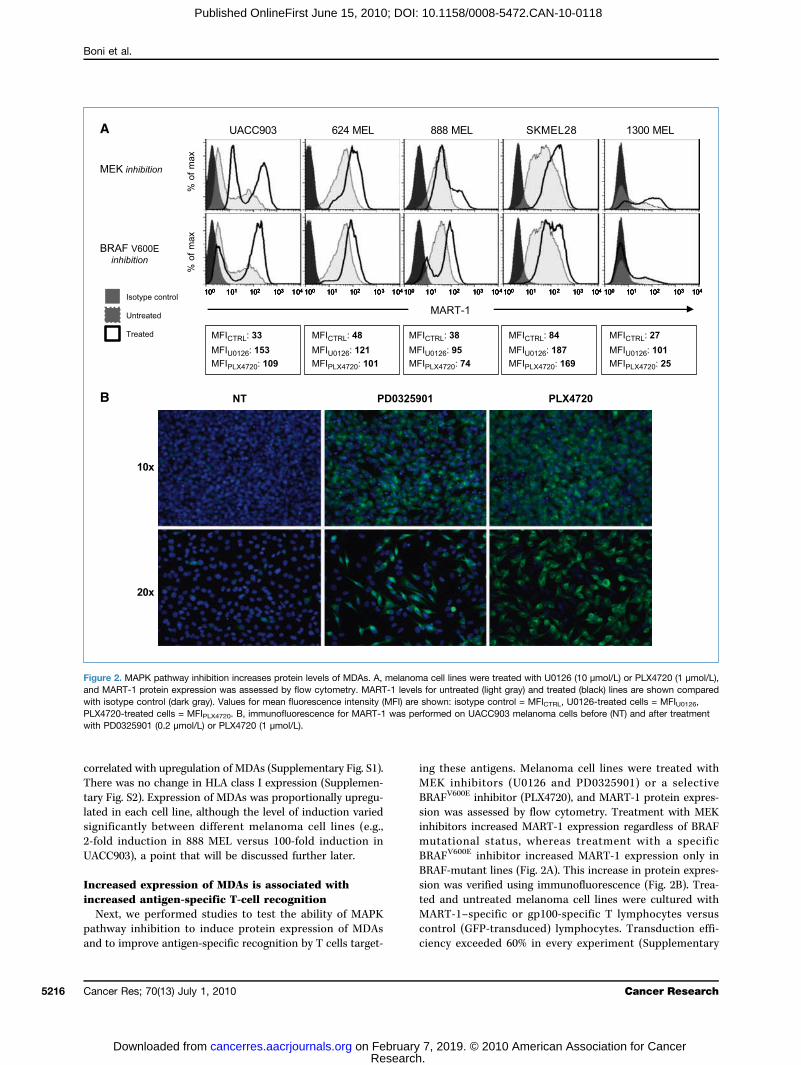
ing these antigens. Melanoma cell lines were treated withMEK inhibitors (U0126 and PD0325901) or a selectiveBRAFV600E inhibitor (PLX4720), and MART-1 protein expres-sion was assessed by flow cytometry. Treatment with MEKinhibitors increased MART-1 expression regardless of BRAFmutational status, whereas treatment with a specificBRAFV600E inhibitor increased MART-1 expression only inBRAF-mutant lines (Fig. 2A). This increase in protein expres-sion was verified using immunofluorescence (Fig. 2B). Trea-ted and untreated melanoma cell lines were cultured withMART-1–specific or gp100-specific T lymphocytes versuscontrol (GFP-transduced) lymphocytes. Transduction effi-ciency exceeded 60% in every experiment (Supplementary
Figure 2. MAPK pathway inhibition increases protein levels of MDAs. A, melanoma cell lines were treated with U0126 (10 μmol/L) or PLX4720 (1 μmol/L),and MART-1 protein expression was assessed by flow cytometry. MART-1 levels for untreated (light gray) and treated (black) lines are shown comparedwith isotype control (dark gray). Values for mean fluorescence intensity (MFI) are shown: isotype control = MFICTRL, U0126-treated cells = MFIU0126,PLX4720-treated cells = MFIPLX4720. B, immunofluorescence for MART-1 was performed on UACC903 melanoma cells before (NT) and after treatmentwith PD0325901 (0.2 μmol/L) or PLX4720 (1 μmol/L).
Cancer Research
h. 7, 2019. © 2010 American Association for Cancer
BRAF Inhibition Enhances Recognition of Melanoma
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
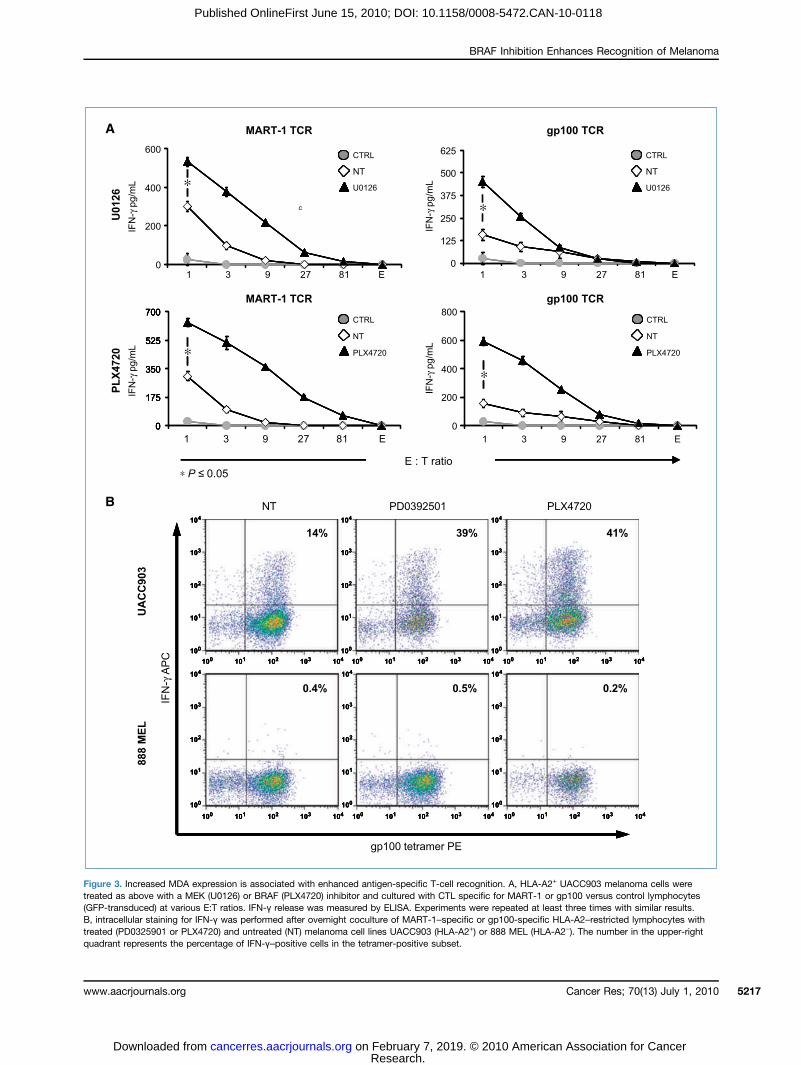
Figure 3. Increased MDA expression is associated with enhanced antigen-specific T-cell recognition. A, HLA-A2+ UACC903 melanoma cells weretreated as above with a MEK (U0126) or BRAF (PLX4720) inhibitor and cultured with CTL specific for MART-1 or gp100 versus control lymphocytes(GFP-transduced) at various E:T ratios. IFN-γ release was measured by ELISA. Experiments were repeated at least three times with similar results.B, intracellular staining for IFN-γ was performed after overnight coculture of MART-1–specific or gp100-specific HLA-A2–restricted lymphocytes withtreated (PD0325901 or PLX4720) and untreated (NT) melanoma cell lines UACC903 (HLA-A2+) or 888 MEL (HLA-A2−). The number in the upper-rightquadrant represents the percentage of IFN-γ–positive cells in the tetramer-positive subset.
Cancer Res; 70(13) July 1, 2010www.aacrjournals.org 5217
Research. on February 7, 2019. © 2010 American Association for Cancercancerres.aacrjournals.org Downloaded from
Boni et al.
5218
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
Fig. S3). IFN-γ release was used to assess T-cell recognitionof tumor cells. Significant increases in IFN-γ were observedwhen MART-1–specific and gp100-specific T cells were cul-tured with melanoma cell lines treated with the MEK inhib-itor or the selective BRAFV600E inhibitor PLX4720 (Fig. 3A)but not with control lymphocytes (P < 0.05). These findingswere verified with intracellular staining for IFN-γ (Fig. 3B)and cytotoxicity assay (Supplementary Fig. S4).These data suggest that MAPK pathway inhibition triggers
upregulation of melanocyte antigen expression, which con-fers improved recognition by antigen-specific T cells.
MEK inhibition, but not BRAFV600E inhibition, impairsT lymphocyte functionOne critical question in planning combined targeted mo-
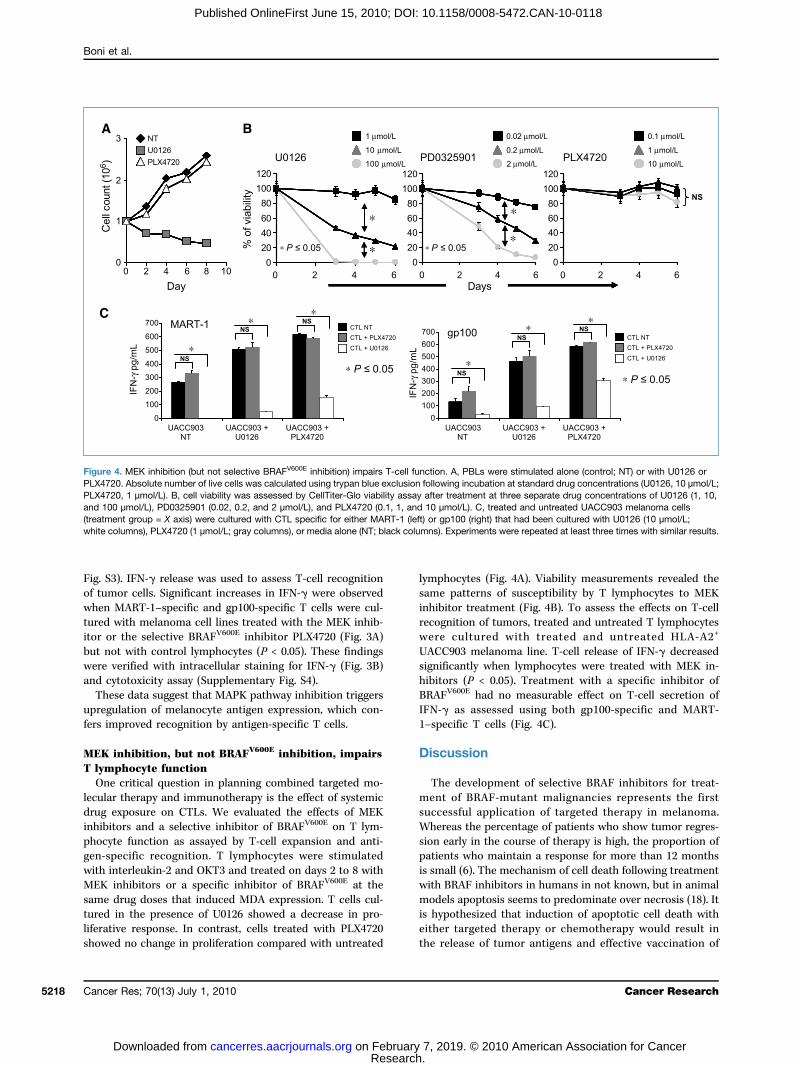
lecular therapy and immunotherapy is the effect of systemicdrug exposure on CTLs. We evaluated the effects of MEKinhibitors and a selective inhibitor of BRAFV600E on T lym-phocyte function as assayed by T-cell expansion and anti-gen-specific recognition. T lymphocytes were stimulatedwith interleukin-2 and OKT3 and treated on days 2 to 8 withMEK inhibitors or a specific inhibitor of BRAFV600E at thesame drug doses that induced MDA expression. T cells cul-tured in the presence of U0126 showed a decrease in pro-liferative response. In contrast, cells treated with PLX4720showed no change in proliferation compared with untreated
Cancer Res; 70(13) July 1, 2010
Researcon Februarycancerres.aacrjournals.org Downloaded from
lymphocytes (Fig. 4A). Viability measurements revealed thesame patterns of susceptibility by T lymphocytes to MEKinhibitor treatment (Fig. 4B). To assess the effects on T-cellrecognition of tumors, treated and untreated T lymphocyteswere cultured with treated and untreated HLA-A2+
UACC903 melanoma line. T-cell release of IFN-γ decreasedsignificantly when lymphocytes were treated with MEK in-hibitors (P < 0.05). Treatment with a specific inhibitor ofBRAFV600E had no measurable effect on T-cell secretion ofIFN-γ as assessed using both gp100-specific and MART-1–specific T cells (Fig. 4C).
Discussion
The development of selective BRAF inhibitors for treat-ment of BRAF-mutant malignancies represents the firstsuccessful application of targeted therapy in melanoma.Whereas the percentage of patients who show tumor regres-sion early in the course of therapy is high, the proportion ofpatients who maintain a response for more than 12 monthsis small (6). The mechanism of cell death following treatmentwith BRAF inhibitors in humans in not known, but in animalmodels apoptosis seems to predominate over necrosis (18). Itis hypothesized that induction of apoptotic cell death witheither targeted therapy or chemotherapy would result inthe release of tumor antigens and effective vaccination of
Figure 4. MEK inhibition (but not selective BRAFV600E inhibition) impairs T-cell function. A, PBLs were stimulated alone (control; NT) or with U0126 orPLX4720. Absolute number of live cells was calculated using trypan blue exclusion following incubation at standard drug concentrations (U0126, 10 μmol/L;PLX4720, 1 μmol/L). B, cell viability was assessed by CellTiter-Glo viability assay after treatment at three separate drug concentrations of U0126 (1, 10,and 100 μmol/L), PD0325901 (0.02, 0.2, and 2 μmol/L), and PLX4720 (0.1, 1, and 10 μmol/L). C, treated and untreated UACC903 melanoma cells(treatment group = X axis) were cultured with CTL specific for either MART-1 (left) or gp100 (right) that had been cultured with U0126 (10 μmol/L;white columns), PLX4720 (1 μmol/L; gray columns), or media alone (NT; black columns). Experiments were repeated at least three times with similar results.
Cancer Research
h. 7, 2019. © 2010 American Association for Cancer

BRAF Inhibition Enhances Recognition of Melanoma
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118
the host. This might set the stage for more effective treat-ment with active immunotherapy, such as cytokines orimmune checkpoint inhibitors.Cytokine-based immunotherapy is associated with durable
complete responses in a subset of patients with metastaticmelanoma. Monoclonal antibodies blocking CTLA-4 are as-sociated with an objective response rate 10% to 15% of pa-tients, and the majority of these responses are durable (19).Thus, the longevity of clinical response is well established forthis approach, whereas the percentage of responding pa-tients remains low.In the present study, we provide preclinical evidence sup-
porting the use of combination BRAF-targeted therapy andimmunotherapy for melanoma. We show that MAPK path-way inhibition using a selective inhibitor of BRAFV600E leadsto increased expression of MDAs, conferring enhanced anti-gen-specific recognition by CTL without compromising lym-phocyte function. In contrast, MEK inhibition has a similareffect on MDAs but deleterious effects on T cells. Clinicalin vivo validation of these findings in patients being treatedwith these agents is a critical next step, and these studies arecurrently under way.Further investigation is also required to uncover the mech-
anism underlying the effect of oncogenic BRAF on antigenexpression in melanoma. Preliminary data suggest that onco-genic BRAF suppresses MDA expression through micro-phthalmia-associated transcription factor, as suggested byWellbrock and colleagues (Supplementary Fig. S5; ref. 20).However, additional signaling pathways are important tomelanoma pathophysiology and may account for the vari-ability in MDA induction we observed across different mela-
www.aacrjournals.org
Researcon Februarycancerres.aacrjournals.org Downloaded from
noma cell lines. In clinical trials, it will be critical to assaygenetic alterations and status of pathway activation in thenetwork of pathways beyond MAPK and correlate this withexpression of MDAs, as significant heterogeneity may existeven among BRAF-mutant tumors. Variability in MDA ex-pression changes with BRAF-targeted therapy will likely iden-tify those patients for whom the addition of immunotherapywill be most effective. In those for whom MDA expression isminimally altered, additional signaling inhibitors might beused to achieve maximal antigen expression. Our data pro-vide a clear rationale for the combination of targeted therapyand immunotherapy for melanoma and provide candidatepharmacodynamic markers to investigate in clinical trials.
Disclosure of Potential Conflicts of Interest
K.T. Flaherty: advisory board, Roche Pharmaceuticals. The other authorsdisclosed no potential conflicts of interest.
Acknowledgments
We thank the Surgery Branch, NCI, for providing technical support, celllines, and retroviral vectors.
Grant Support
Intramural funds from Massachusetts General Hospital and philanthropicsupport of the Schlesinger family.
The costs of publication of this article were defrayed in part by the paymentof page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received 01/12/2010; revised 04/15/2010; accepted 04/29/2010; publishedOnlineFirst 06/15/2010.
References
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics,2009. CA Cancer J Clin 2009;59:225–49.2. Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009
AJCC melanoma staging and classification. J Clin Oncol 2009;27:6199–206.
3. Singh M, Lin J, Hocker TL, Tsao H. Genetics of melanoma tumori-genesis. Br J Dermatol 2008;158:15–21.
4. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene inhuman cancer. Nature 2002;417:949–54.
5. Dummer RRC, Chapman PB, Sosman JA, et al. AZD6244 (ARRY-142886) vs temozolomide (TMZ) in patients with advanced melano-ma: an open-label, randomized, phase II study. J Clin Oncol 2008;26.
6. Flaherty KT, Puzanov I, Sosman J, et al. Phase I study of PLX4032:proof of concept for V600E BRAF mutation as a therapeutic target inhuman cancer [Suppl; abstract 9000]. J Clin Oncol 2009;27:15s.
7. Emery CM, Vijayendran KG, Zipser MC, et al. MEK1 mutations conferresistance to MEK and B-RAF inhibition. Proc Natl Acad Sci U S A2009;106:20411–6.
8. Smalley KS, Nathanson KL, Flaherty KT. Genetic subgrouping ofmelanoma reveals new opportunities for targeted therapy. CancerRes 2009;69:3241–4.
9. Smalley KS, Flaherty KT. Integrating BRAF/MEK inhibitors intocombination therapy for melanoma. Br J Cancer 2009;100:431–5.
10. Rosenberg SA, Restifo NP, Yang JC, Morgan RA, Dudley ME. Adop-tive cell transfer: a clinical path to effective cancer immunotherapy.Nat Rev 2008;8:299–308.
11. Klapper JA, Thomasian AA, Smith DM, et al. Single-pass, closed-system rapid expansion of lymphocyte cultures for adoptive celltherapy. J Immunol Methods 2009;345:90–9.
12. Johnson LA, Morgan RA, Dudley ME, et al. Gene therapy withhuman and mouse T-cell receptors mediates cancer regressionand targets normal tissues expressing cognate antigen. Blood2009;114:535–46.
13. Wang E, Monaco A, Monsurro V, et al. Antitumor vaccines, immu-notherapy and the immunological constant of rejection. IDrugs2009;12:297–301.
14. Eggermont AM, Schadendorf D. Melanoma and immunotherapy.Hematol Oncol Clin North Am 2009;23:547–64.
15. Kono M, Dunn IS, Durda PJ, et al. Role of the mitogen-activatedprotein kinase signaling pathway in the regulation of human melano-cytic antigen expression. Mol Cancer Res 2006;4:779–92.
16. Khong HT, Wang QJ, Rosenberg SA. Identification of multiple anti-gens recognized by tumor-infiltrating lymphocytes from a singlepatient: tumor escape by antigen loss and loss of MHC expression.J Immunother 2004;27:184–90.
17. Tsai J, Lee JT, Wang W, et al. Discovery of a selective inhibitor ofoncogenic B-Raf kinase with potent antimelanoma activity. Proc NatlAcad Sci U S A 2008;105:3041–6.
18. Cartlidge RA, Thomas GR, Cagnol S, et al. Oncogenic BRAF(V600E)inhibits BIM expression to promote melanoma cell survival. PigmentCell Melanoma Res 2008;21:534–44.
19. Weber J. Overcoming immunologic tolerance to melanoma: target-ing CTLA-4 with ipilimumab (MDX-010). Oncologist 2008;13 Suppl4:16–25.
20. Wellbrock C, Rana S, Paterson H, Pickersgill H, Brummelkamp T,Marais R. Oncogenic BRAF regulates melanoma proliferationthrough the lineage specific factor MITF. PLoS One 2008;3:e2734.
Cancer Res; 70(13) July 1, 2010 5219
h. 7, 2019. © 2010 American Association for Cancer
2010;70:5213-5219. Published OnlineFirst June 15, 2010.Cancer Res Andrea Boni, Alexandria P. Cogdill, Ping Dang, et al. of Melanoma without Affecting Lymphocyte Function
Inhibition Enhances T-Cell RecognitionV600ESelective BRAF
Updated version
10.1158/0008-5472.CAN-10-0118doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2010/06/14/0008-5472.CAN-10-0118.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/70/13/5213.full#ref-list-1
This article cites 19 articles, 6 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/70/13/5213.full#related-urls
This article has been cited by 80 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/70/13/5213To request permission to re-use all or part of this article, use this link
Research. on February 7, 2019. © 2010 American Association for Cancercancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 15, 2010; DOI: 10.1158/0008-5472.CAN-10-0118