selecting & setting denture teeth rola m. shadid, bds, msc, m(aaid)
TRANSCRIPT
Selecting & Setting Denture Teeth
Rola M. Shadid, BDS, MSc, m(AAID)
The task of selecting teeth is the responsibility of the dentist and should not be left to others
All the teeth from a particular mode will have the same size & shape
Selection of tooth size
Selection of tooth shape
Selection of tooth shade
Selection of tooth material
Selection criteria for anterior teeth
Height (occluogingival)
Width (mesiodistal)
Thickness (faciolingual)
Selection of tooth size
Preextraction guides
Diagnostic guides are the most reliable guides in the selection of size & form
Extracted teeth
Previous dentures especially if they are immediate dentures
Postextraction methods
Selection of tooth size
Preextraction guide
Bizygomatic width
Cranial circumference
Corners of the mouth
Ala of nose
Determining Tooth Width
Bizygomatic width: the greatest bizygomatic width measured by facebow divided by 16= width of the central incisor; divided by 3.3 = approximate width of the six upper anterior teeth
Cranial circumference: the ratio of the cranial circumference to the combined upper anterior teeth width is 10 to 1.
Determining Tooth Width
Corners of mouth at rest coincide with distal of canines
Or ala of nose coincides with canine cusp tip
Determining Tooth Width
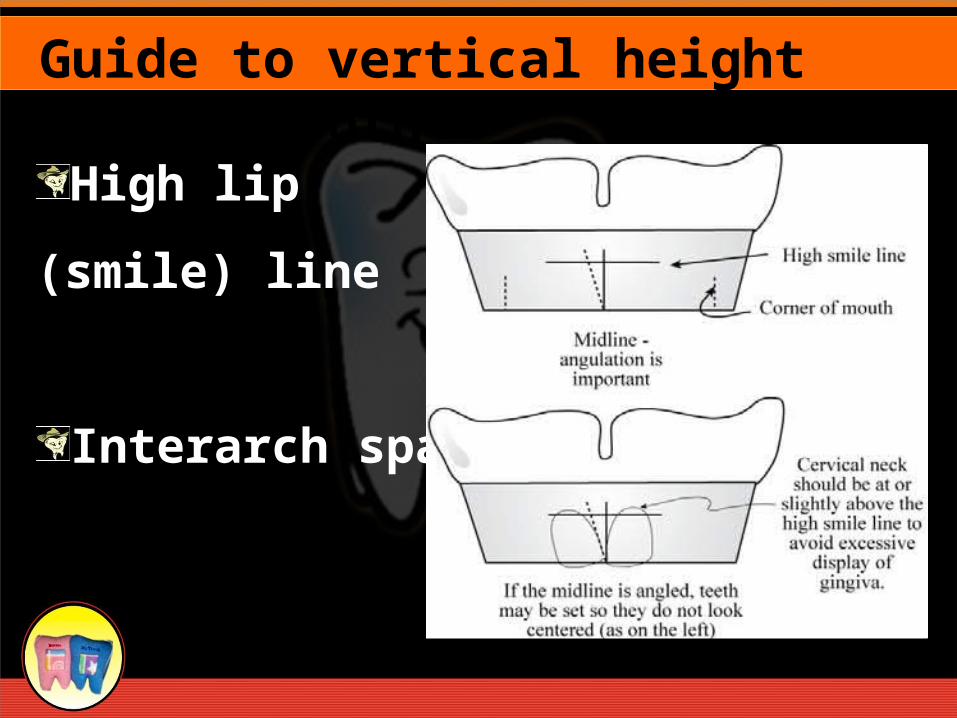
High lip
(smile) line
Interarch space *
Guide to vertical height of the tooth

Highest point of upper lip
when smiling
Cervical necks lie at
or above this line
If shorter teeth are selected,
esthetics compromised
Guide to vertical height of the tooth (High lip line)
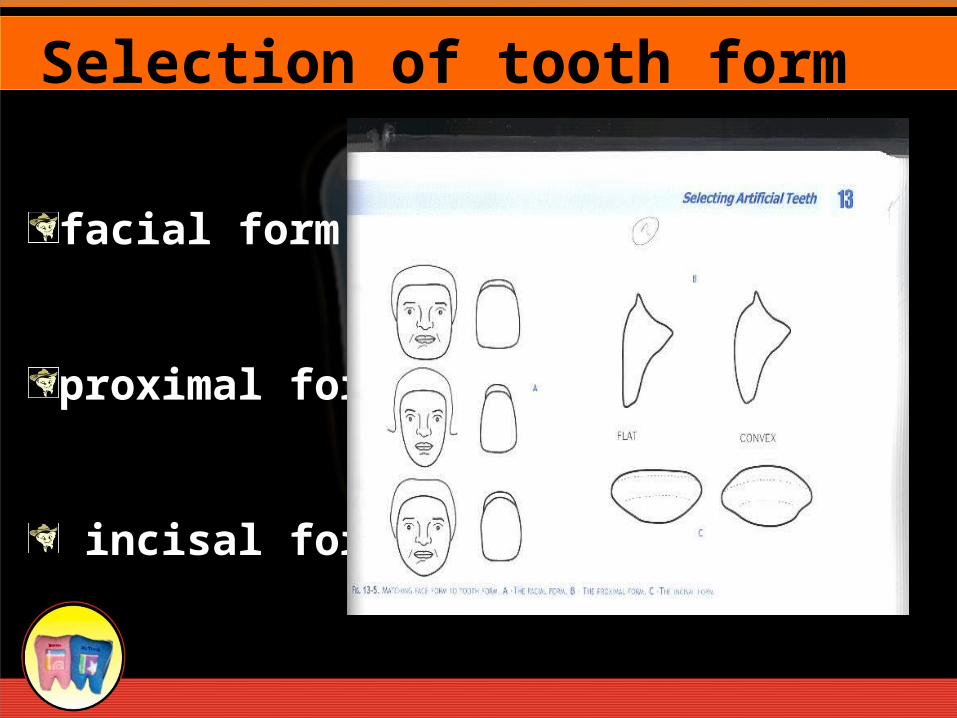
facial form
proximal form
incisal form
Selection of tooth form
Matching the tooth form to the face form (Leon Williams theory) *
The dentogenic concept in selecting teeth forms (proposed by Frush & Fisher) ¶
Teeth are selected according to sex then to personality & finally the age
Selection of tooth form
An appropriate color of artificial tooth is selected from a shade guide.
When making the choice, it is advisable to moisten the teeth with water and hold them just inside the patient’s open mouth.
Selection of the color (shade)
Care should be taken to avoid letting the patient view the teeth against a light background such as the dentist’s white coat as this can be positively misleading. Under such conditions the shade will appear darker than it will when the denture is eventually in the mouth. As a result, the patient is likely to choose a shade that is too light.
Selection of the color (shade)
• Natural teeth tend to become darker with increasing age. It is, therefore, appropriate to choose a shade of denture tooth which is in keeping with the patient’s age.
• Correlation with skin and hair color is suspect
Selection of the color
Don’t show a patient all shades in the shade guide outside of the mouth – patients will almost always pick the whitest shade
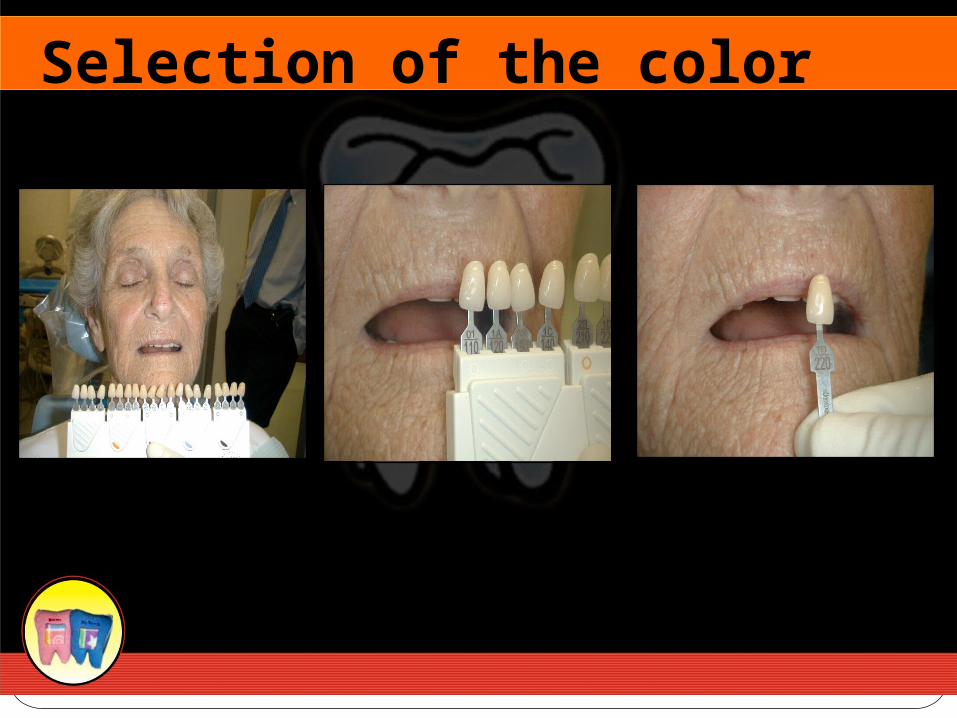
Instead show patient 2 or 3 shades under lip and ask their opinion
Anterior and posterior tooth shades are the same (e.g. anterior shade P3.5 corresponds with posterior shade P3.5)
Selection of the color
Selection of the color
•Patient owns the dentureswill look at them every day
•Offer your opinion, don’t persuade
Patient Chooses Shade with Input from Dentist

Requirements of posterior teeth:
Chew food efficiently
Contribute to denture stability
Comfortable to underlying soft tissues
Should not cause any bone resorption
Should contribute to esthetics & not create any sound on impact
Selection of posterior teeth
Color
Mesiodistal width
Buccolingual width
Occlusogingival length
Cuspal inclination
Material
Selection criteria for posterior teeth
Selecting Posterior Tooth
Form
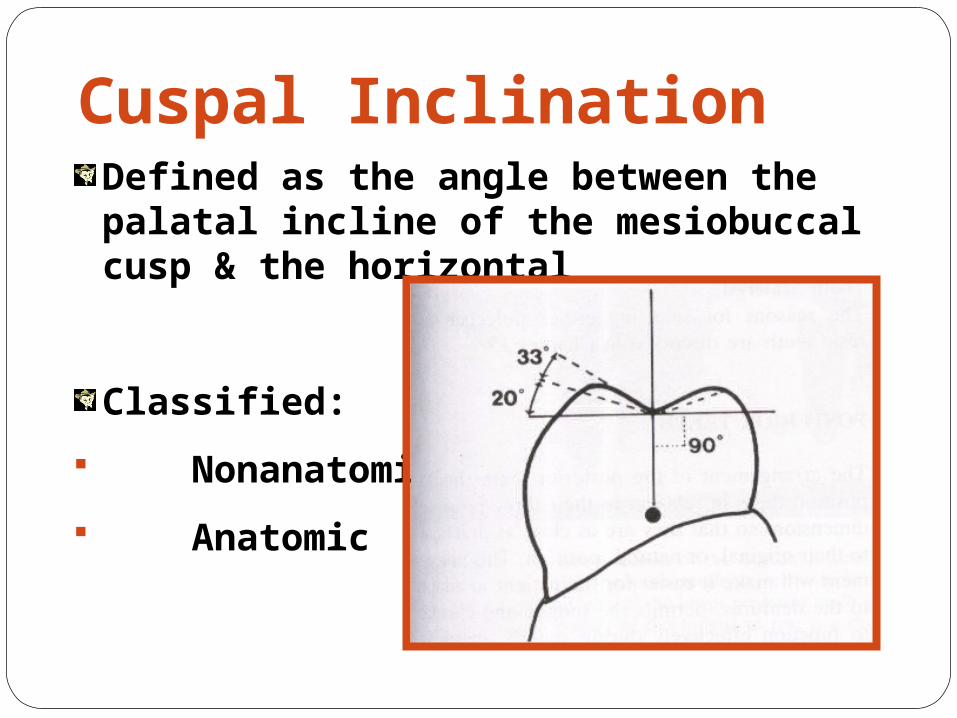
Cuspal InclinationDefined as the angle between the palatal incline of the mesiobuccal cusp & the horizontal
Classified:
Nonanatomic
Anatomic
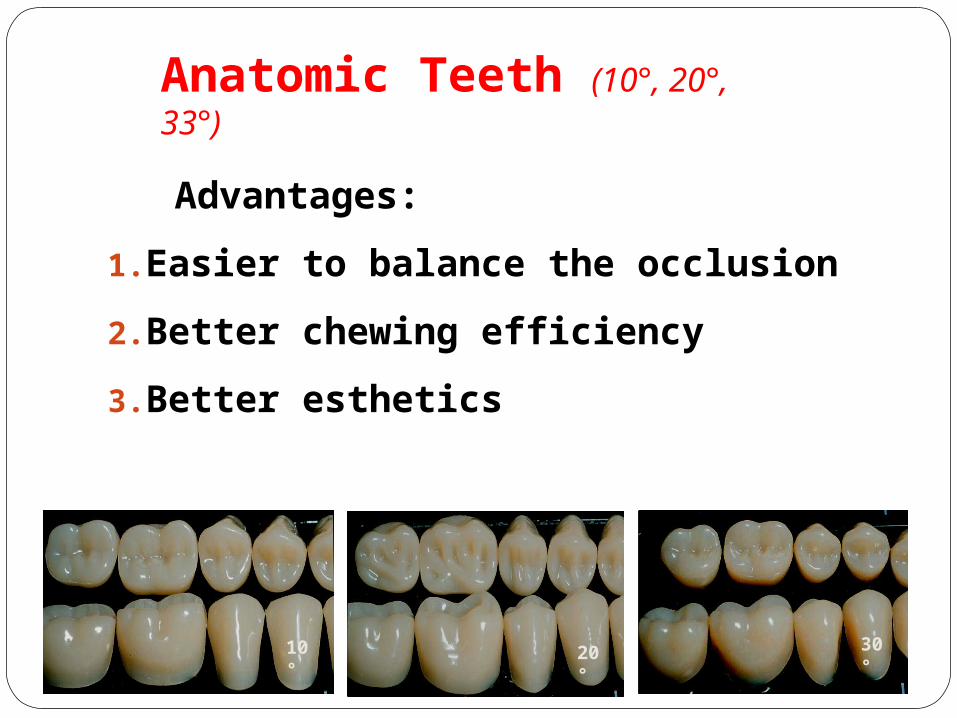
Anatomic Teeth (10°, 20°, 33°)
Advantages:
1.Easier to balance the occlusion
2.Better chewing efficiency
3.Better esthetics
20°
10°
30°
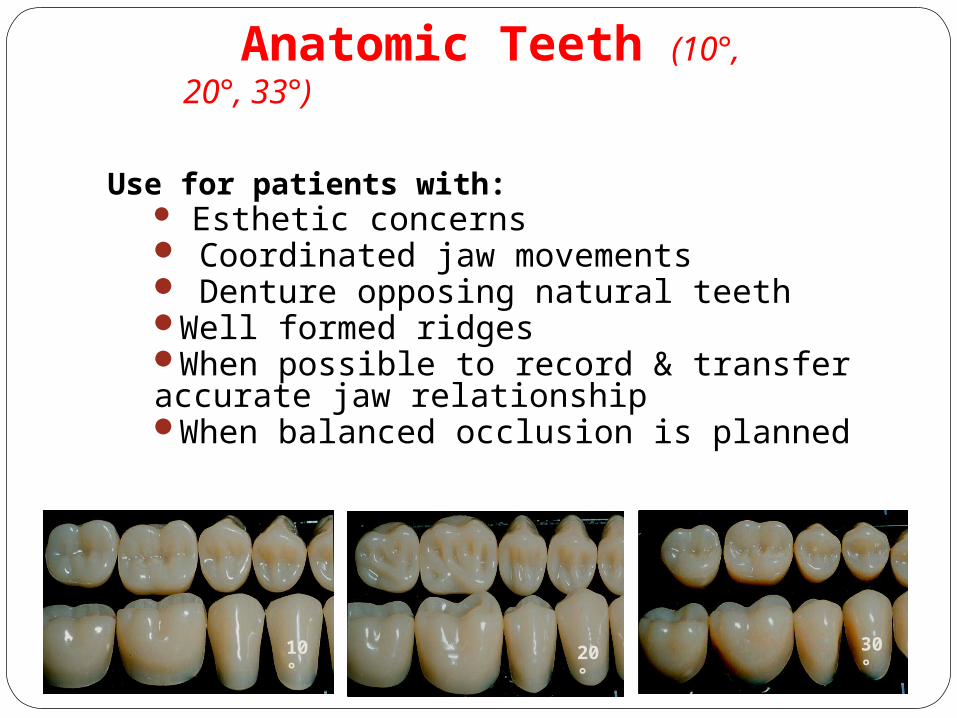
Anatomic Teeth (10°, 20°, 33°)
Use for patients with: Esthetic concerns Coordinated jaw movements Denture opposing natural teethWell formed ridgesWhen possible to record & transfer accurate jaw relationshipWhen balanced occlusion is planned
20°
10°
30°
Non-Anatomic Teeth(0°, Rational, Monoline, etc.)
Advantages:
1.Freedom of occlusal movement
2.Elimination of lateral forces
3.Lack of interferences & better able to accommodate positional changes of the dentures relative to the supporting tissues brought about by resorption of alveolar bone
Disadvantages:
Not esthetic looking, lower shearing efficiency & difficult to balance
Non-Anatomic Teeth(0°, Rational, Monoline, etc.)
Use for patients with:Jaw size discrepancies (Class III)Severe ridge resorptionUncoordinated jaw movementsFor elderly patients because an
increased variation in occlusal contact positions is characteristic of this groupso it is difficult to record & transfer accurate jaw relationship
Selection Of Denture Tooth
Material
Denture Tooth Material
Acrylic resin
Porcelain teeth
Porcelain acrylic combination
Acrylic teeth with amalgam inserts or with cast gold occlusal surfaces
Denture Tooth Material
Porcelain teeth less common now
Acrylic easier to set and adjustLast life of denture (5-7 years)
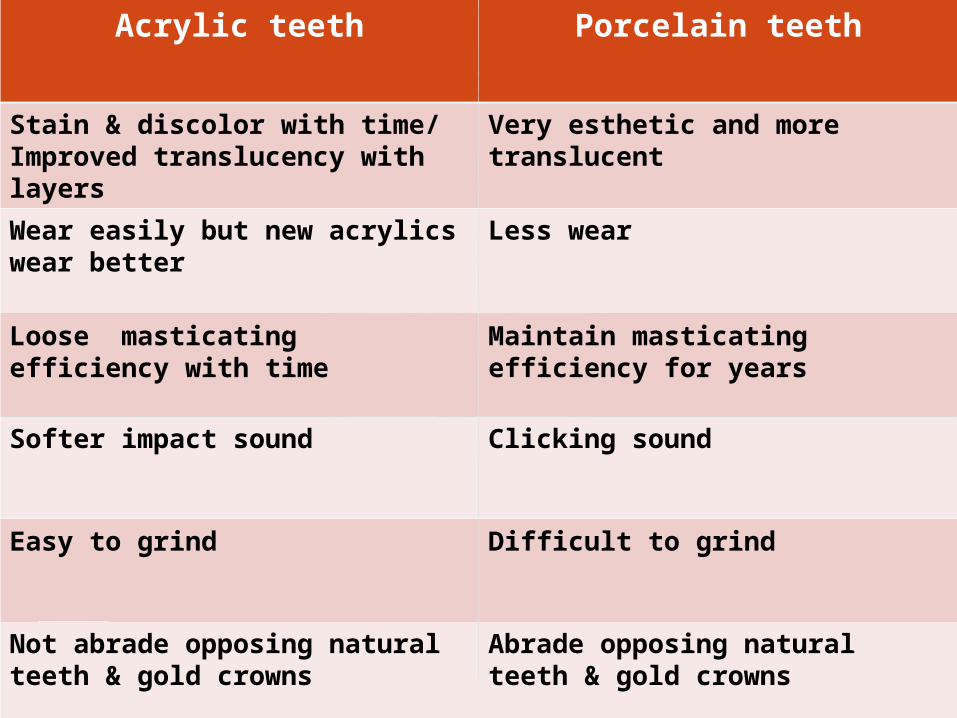
Selection of tooth materialAcrylic teeth Porcelain teeth
Stain & discolor with time/Improved translucency with layers
Very esthetic and more translucent
Wear easily but new acrylics wear better
Less wear
Loose masticating efficiency with time
Maintain masticating efficiency for years
Softer impact sound Clicking sound
Easy to grind Difficult to grind
Not abrade opposing natural teeth & gold crowns
Abrade opposing natural teeth & gold crowns
Selection of tooth materialAcrylic teeth Porcelain teeth
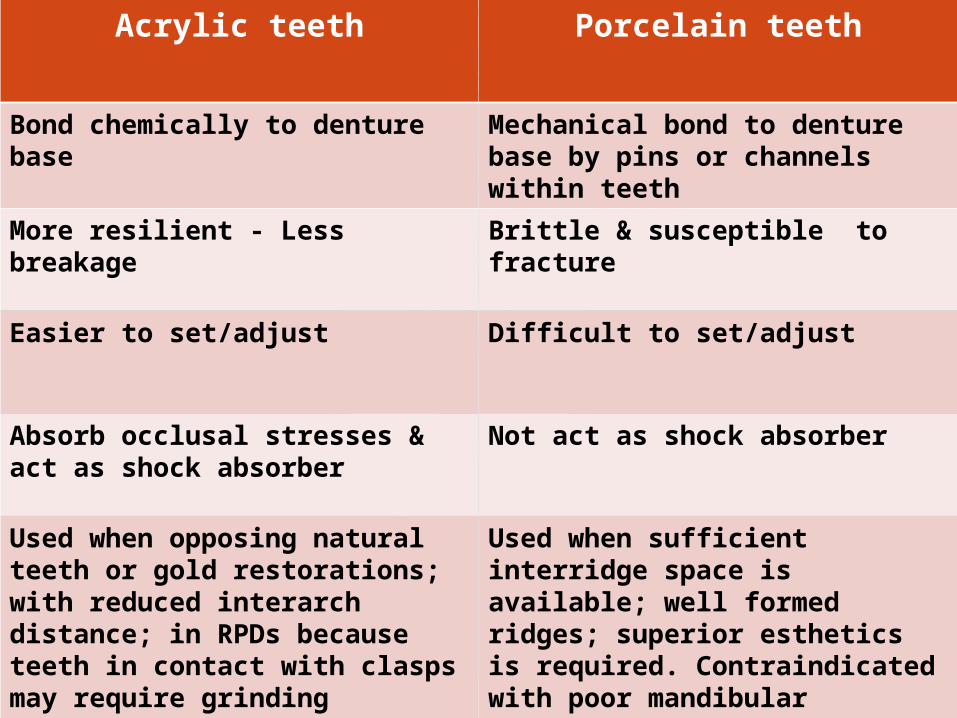
Bond chemically to denture base
Mechanical bond to denture base by pins or channels within teeth
More resilient - Less breakage Brittle & susceptible to fracture
Easier to set/adjust Difficult to set/adjust
Absorb occlusal stresses & act as shock absorber
Not act as shock absorber
Used when opposing natural teeth or gold restorations; with reduced interarch distance; in RPDs because teeth in contact with clasps may require grinding
Used when sufficient interridge space is available; well formed ridges; superior esthetics is required. Contraindicated with poor mandibular ridges ; when opposing natural teeth or gold restorations
Porcelain-Acrylic Combination
Resin posteriors oppose porcelain posteriors *
Porcelain anteriors & resin
posteriors Х
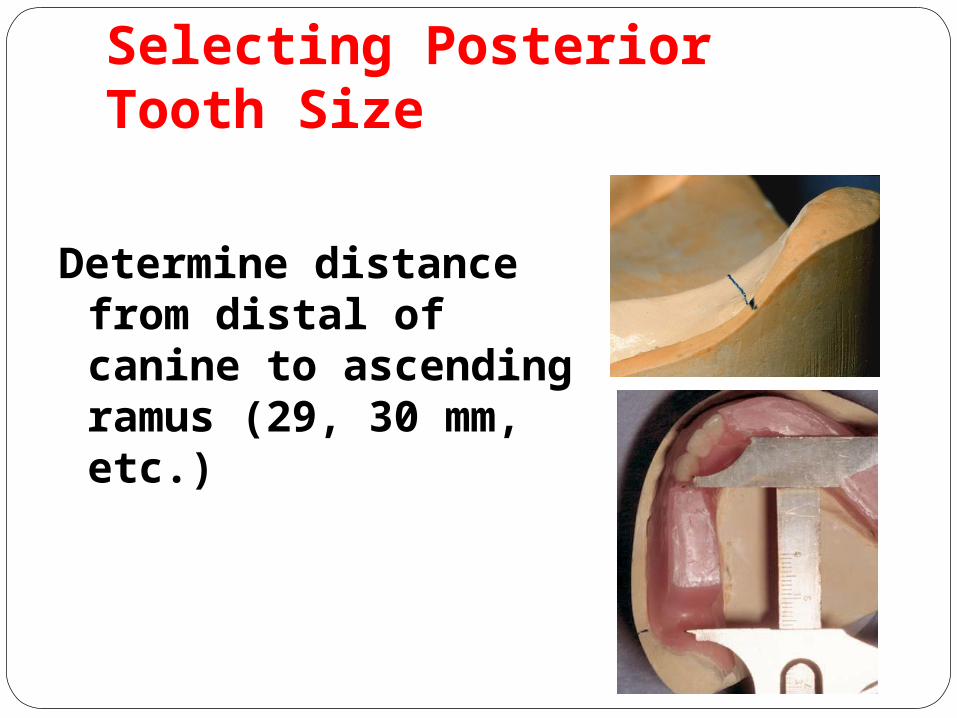
Selecting Posterior Tooth Size
Determine distance from distal of canine to ascending ramus (29, 30 mm, etc.)
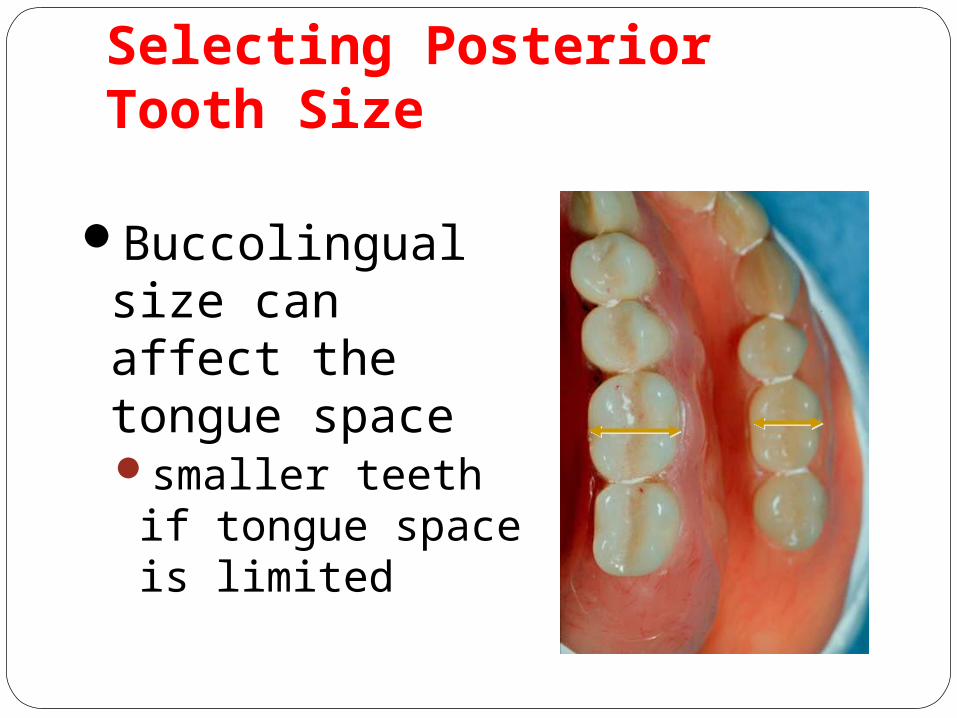
Selecting Posterior Tooth Size
Buccolingual size can affect the tongue spacesmaller teeth if tongue space is limited
Summary
Selecting denture teeth advise patient don’t persuade an art, minimal science use common sense use old denture as a starting point look at dentate patient esthetics

Setting of Denture Teeth at Balanced Occlusion
The goals of proper teeth selection and arranging are to construct complete dentures that:
1.Function well
2.Allow the patient to speak normally
3.Are esthetically pleasing
4.Will not abuse the tissues over residual ridges
5.Offer health & comfort to TMJ
Arranging Prosthetic Teeth
1.The artificial teeth should be placed as near as possible to the position occupied by natural teeth, with being compatible with surrounding musculature.
2.The preliminary position of both anterior & posterior teeth is determined during jaw relation appointment (Refer to the lecture)
Some guidelines for arranging artificial teeth
3.Regarding anteroposterior position of upper anterior teeth: fullness of the lips, phonetics (f & v sounds) as a guide, distance from incisive papilla, and relation to the residual alvealar ridge as to be placed anterior to it according to the amount of resorption; all guide their position.
4. Regarding superoinferior position of upper anterior teeth: preextraction records, former dentures, and visibility of the upper incisors are used as a guide.
Some guidelines for arranging artificial teeth
5.Inclination of the anterior teeth; there is an obtuse angle between the labial surface of bone & the labial surface of anterior teeth
6.Mediolateral position; midline & ala of nose are used as aguide
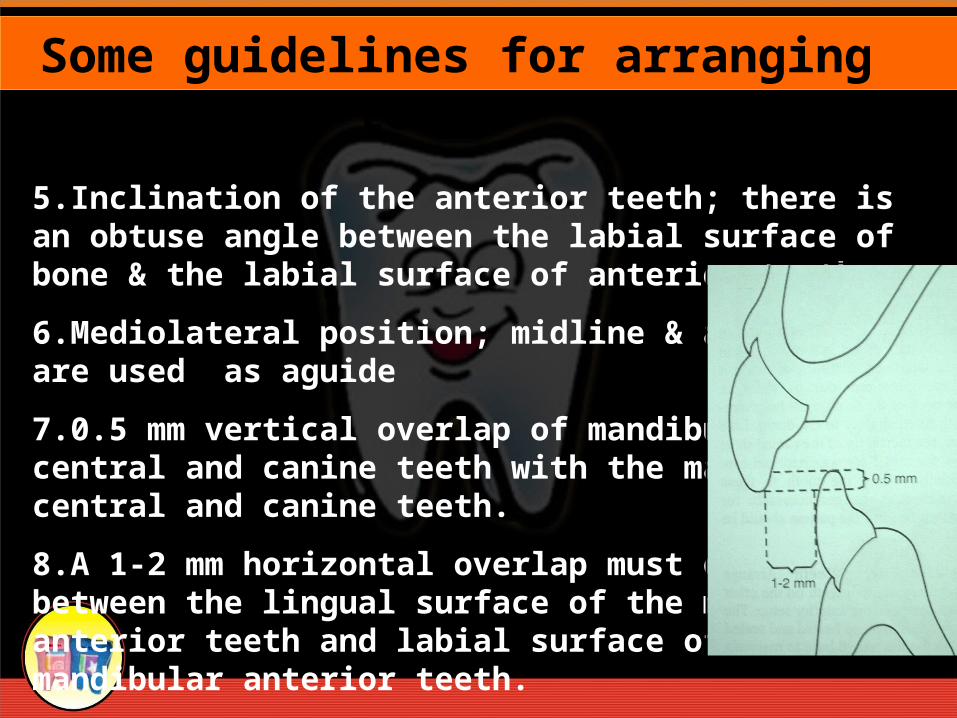
7.0.5 mm vertical overlap of mandibular central and canine teeth with the maxillary central and canine teeth.
8.A 1-2 mm horizontal overlap must exist between the lingual surface of the maxillary anterior teeth and labial surface of the mandibular anterior teeth.
Some guidelines for arranging artificial teeth
9.The upper & lower posterior teeth are centered over the crest of the ridge whenever possible
10. Placing maxillary teeth over maxillary tuberosity should be avoided
11.Placing mandibular teeth over retromolar pad or over steep slopes should be avoided.
12.Placing posterior teeth too far buccally should be avoided
Some guidelines for arranging artificial teeth
13.Placing posterior teeth too far lingually should be avoided
14.The lingual cusps of mandibular posterior should be in alignment with mylohyoid ridge & never lingual to it
15. Regarding occlusal plane: oInterpupillary line & ala-tragus line
oCorners of the mouth ( anterior occlusal plane is placed at or slightly below corners) & level with one-half to two-thirds of retromolar pad
oTongue (lateral borders of tongue should be just superior to occlusal plane)
Some guidelines for arranging artificial teeth

16.The lower posterior teeth are placed buccolingualy along a line extending from the tip of the canine to the middle of the retromolar pad. This line should pass through the central fossae of the premolars and molars.
Some guidelines for arranging artificial teeth
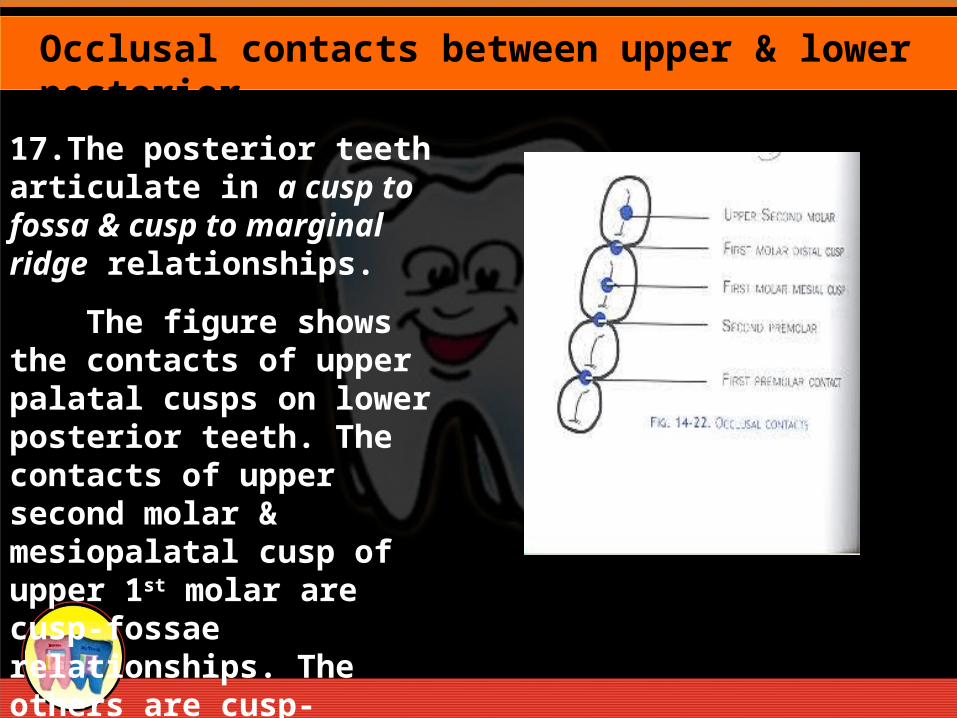
17.The posterior teeth articulate in a cusp to fossa & cusp to marginal ridge relationships.
The figure shows the contacts of upper palatal cusps on lower posterior teeth. The contacts of upper second molar & mesiopalatal cusp of upper 1st molar are cusp-fossae relationships. The others are cusp-marginal ridges contacts.
Occlusal contacts between upper & lower posterior
a #7Midline of the maxillary rim: score a line demarcating the position of the midline of philtrum of the lip. This is one of the most critical references to record. Ensure the mark is a line, not just a dot, which parallels the patients overall facial midline. Otherwise the incisors can be set at an angle, making the set up look off center. The mandibular midline can be marked at the same time.
Reference marks in maxilla
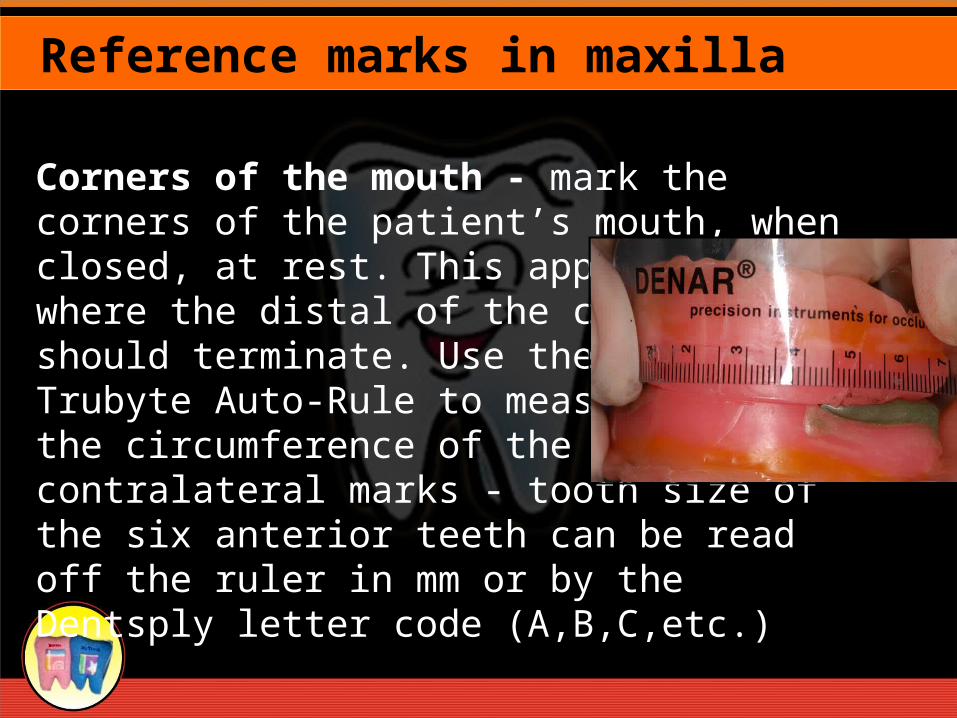
Corners of the mouth - mark the corners of the patient’s mouth, when closed, at rest. This approximates where the distal of the canine teeth should terminate. Use the flexible Trubyte Auto-Rule to measure around the circumference of the rim between contralateral marks - tooth size of the six anterior teeth can be read off the ruler in mm or by the Dentsply letter code (A,B,C,etc.)
Reference marks in maxilla
High Lip line - mark the highest point the upper lip reaches when the patient smiles. The maxillary anterior teeth should be selected so the cervical necks lie at or above this line. If shorter teeth are selected, the esthetic result will be compromised.
Reference marks in maxilla
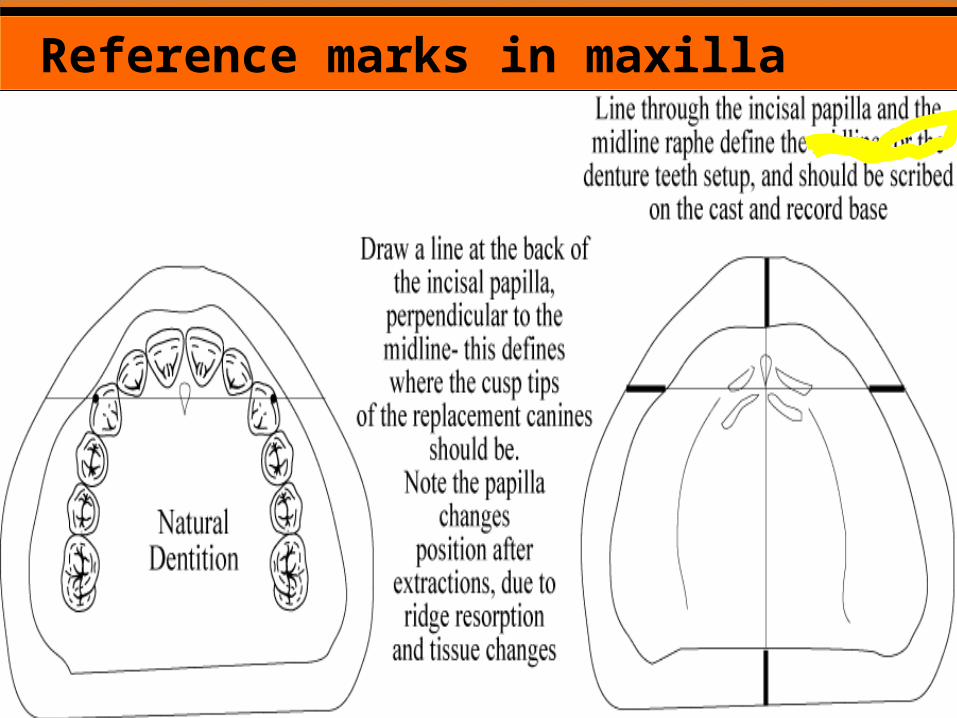
Palatal Midline - With a pencil and a straight edge, draw a line through the middle of the incisive papilla and the mid-palatal raphe, extending it onto the land area of the cast. Check your occlusal rim for symmetry about this important midline. If it is not symmetrical, adjust the rim prior to sending it to the lab for placement of teeth.
Reference marks in maxilla
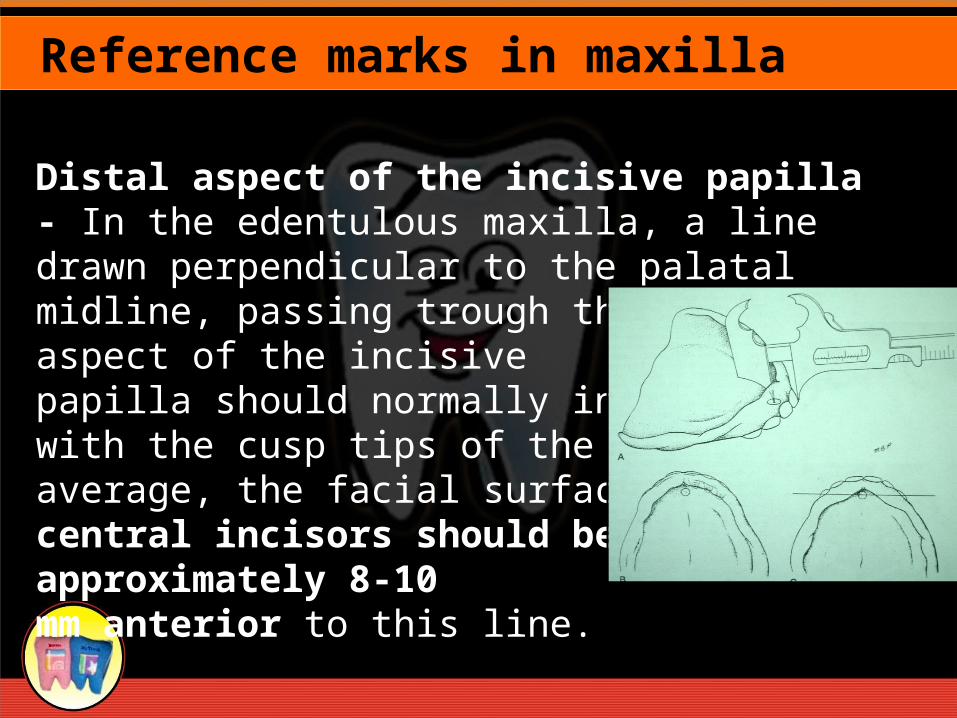
Distal aspect of the incisive papilla - In the edentulous maxilla, a line drawn perpendicular to the palatal midline, passing trough the distal aspect of the incisivepapilla should normally intersect with the cusp tips of the canines. On average, the facial surface of the central incisors should be approximately 8-10mm anterior to this line.
Reference marks in maxilla

Reference marks in maxilla
Reference marks in maxilla
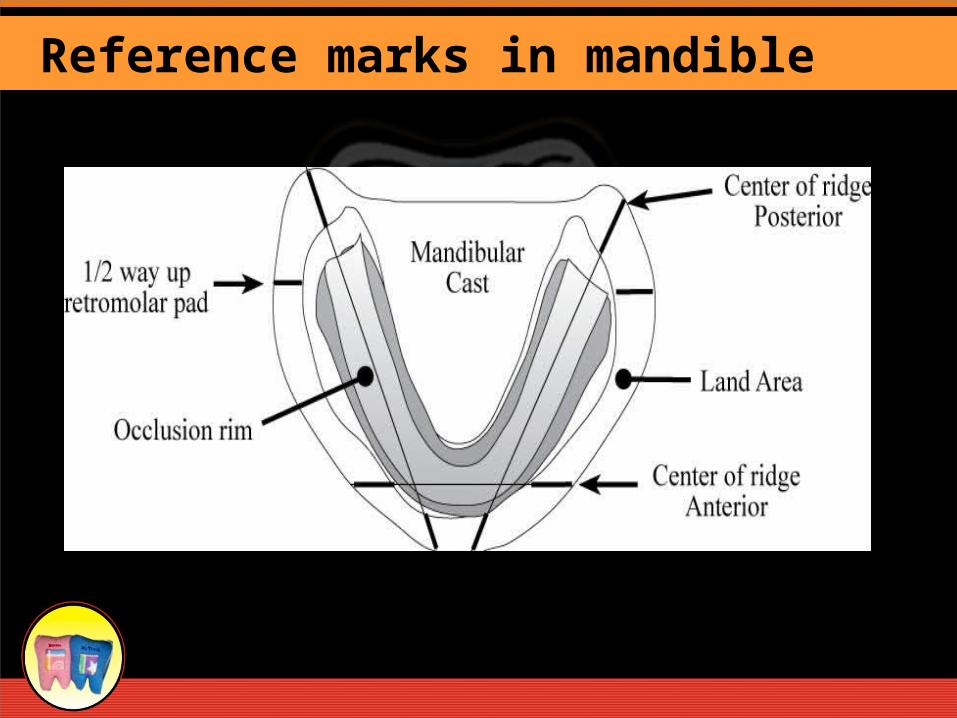
1) Half way to two thirds up the retromolar pad - the posterior aspect of the occlusal plane should intersect the half to two thirds of the retromolar pad, to ensure the occlusal plane is not set too low (can cause tongue biting) or too high (can cause instability & strain as tongue struggles to place the food bolus back on occlusal table)
Reference marks in mandible
2) Center of the posterior mandibular ridge - Draw this line with a pencil and a straight edge, on the cast, extending out to the land area. The lingual cusp of the maxillary posterior teeth should be centered over this line to ensure denture stability, by reducing fulcruming forces during function
Reference marks in mandible
3) Center of the anterior mandibular ridge - Draw this line with a pencil and a straight edge, on the cast, extending out to the land area. If the anterior teeth are set too far anterior to this line, heavy fulcruming forces can cause tilting and dislodging of the mandibular denture, particularly when the mandibular ridge is severely resorbed.
Reference marks in mandible
Reference marks in mandible
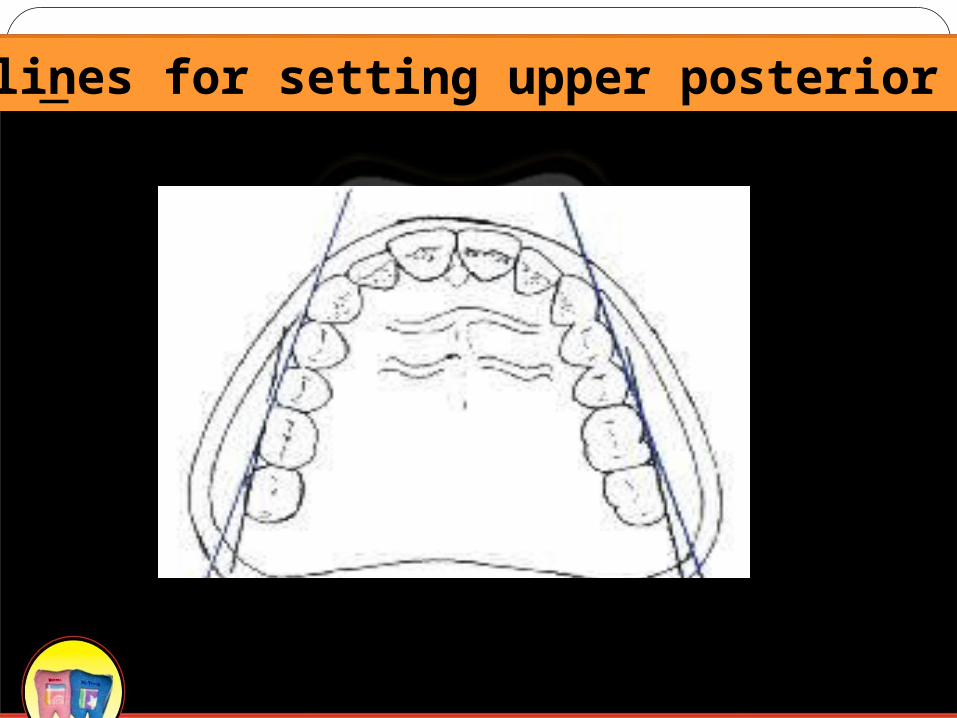
Guidelines for setting upper posterior teeth
References :
1. Basker’s Prosthetic treatment of the edentulous patient. Fourth edition Ch. 11.
2. G. Zarb, Prosthodontic Treatment for Edentulous Patients 2004, Ch. 17
3. Complete Denture Prosthodontics, 1st Edition, 2006 by John Joy Manappallil, Ch. 13 & 14