selecting paths and setting priorities in ... -...
TRANSCRIPT

SELECTING PATHS AND SETTING PRIORITIES IN A MAZE OF
CARE AND PAYMENT REFORMS
HMM, CPAs LLP Healthcare 360 December 1, 2016
ZIMMET HEALTHCARE SERVICES GROUP, LLC www.zhealthcare.com
Reimbursement, Compliance & Planning Solutions for Post-Acute Care

www.zhealthcare.com
10,000 new people added to Social Security and Medicare daily The number of persons aged >65 years is
expected to increase from approximately 35 million in 2000
To an estimated 71 million in 2030 The number of persons aged >80 years is
expected to increase from 9.3 million in 2000 to 19.5 million in 2030
Boomer’s have different expectations for care delivery and changes in settings
2

www.zhealthcare.com
70% of “Baby Boomers” can expect to use some form of long-term care during their lives
The population that is most likely to need LTSS – individuals aged 85 and over – is expected to increase by almost 70% in the next 20 years
3
www.zhealthcare.com
Approximately 80% of all persons aged >65 years have at least one chronic condition, and 50% have at least two Diabetes which causes excess morbidity and increased
health-care costs, affects approximately one in five (18.7%) persons aged >65 years, and as the population ages, the impact of diabetes will intensify
The largest increases in diabetes are expected amongst adults aged >75 years, from 1.2 million women and 0.8 million men in 2000 to 4.4 million women and 4.2 million men in 2050
As U.S. adults live longer, the prevalence of Alzheimer's disease, which doubles every 5 years after age 65, also is expected to increase
Approximately 10% of adults aged >65 years and 47% of adults aged >85 years suffer from this degenerative and debilitating disease
4
www.zhealthcare.com 5

www.zhealthcare.com
IMPACT, VBP, QRP QM, Five Star, OIG, PAC Facilities must Conduct SWOT analysis
‒ Strengths ‒ Weakness ‒ Opportunities ‒ Threats
Review standards of practice, policies and procedures ‒ SOM identifies Rules of Participation and Dates of
Enforcement ‒ Ensure accuracy of clinical documentation and compliance;
train and educate staff Facility specific Data requires strong Investigative
technology platforms that help quantity performance, improve quality of care, improve quality of life and reduce re-hospitalizations
QAPI, data analysis, internal and external auditing of core components on a routine basis
6

www.zhealthcare.com 7
Reducing & Preventing Health Care Associated Infections Reducing & Preventing Adverse Drug Events Community Living Council Multiple Chronic Conditions National Alzheimer’s Project Act Partnership for Patients Million Hearts National Quality Strategy Data.gov
Accountable Care Organizations Community Based Transitions Care Program Dual Eligible Coordination Care Model Demonstrations & Projects 1115 Waivers
Fraud & Abuse Enforcement
National & Local decisions Mechanisms To Support Innovation (CED, parallel review, other)
Hospital Inpatient Quality Hospital Outpatient In-patient Psychiatric Hospitals Cancer Hospitals Nursing Homes Home Health Agencies Long-term Care Acute Hospitals In-patient Rehabilitation Facilities Hospices
Hospitals, Home Health Agencies, Hospices, ESRD facilities
QIOs ESRD Networks
ESRD QIP Hospital VBP
Physician Value Modifier Plans for Skilled Nursing
Facility and Home Health Agencies
Coverage of services Physician Feedback report
Quality Resource Utilization Report Hospital Readmissions
Reduction Program Health Care Associated
Conditions Program
Target Surveys Quality Assurance Performance
Improvement
CMS Authorized Programs & Activities

www.zhealthcare.com
Deficit Reduction Act (DRA) of 2005 Required the standardization of assessment
items used at discharge From an acute care setting and at admission to a
PAC setting Established the Post-Acute Care Payment
Reform Demonstration (PAC-PRD) to harmonize payments for similar settings in PAC settings
Resulted in the Continuity Assessment Record and Evaluation (CARE) tool, a component to test the reliability of standardized items when used in each Medicare setting
8
www.zhealthcare.com
PAC Reform Demonstration requirement of 2006 Interoperability Standards
Nursing Home Compare 2008 Developed Star Ratings To Identify Quality Homes
Affordable Care Act 2010 Government Performance and Results
Modernization Required CMS To Develop Strategies Specific To
Better Care, Lower Costs, Education/Prevention Expansion of Care Coverage, Enterprise Excellence
Enhancement and Expansion of Nursing Home Compare adding MDS 3.0, Survey Findings and PEPPER 2012
9

www.zhealthcare.com
2014 Medicare Transformation Act: Changes to Quality Measures; Changes to CASPER, CMS finalizes Quality Policies
2015 Implementation of Increased Civil Monetary Penalties For Inadequate Staffing Patterns, Training and Supervision of Staff, Resident Outcomes; Finalizes Five Star
2015 ICD 10 Implementation 2016 Federal release of 2013 PUF Data Revision to CMS SOM incorporating ACA
and more
10

www.zhealthcare.com
2017 - 2020 Post Acute Payment Reform Re-hospitalization Penalties Standardized PAC Assessment Episodic Payments Bundled Payment Risk Sharing Census Concerns Transitions of Care Managed Care Resident Rights Discharges Community-Based Care Incentives Outcomes
11

www.zhealthcare.com
Transform Medicare from a passive payer of claims to an active purchaser of quality healthcare
Interoperability across all Providers Hospitals Value Based Program Hospital Readmission Reduction Programs Hospital Acquired Conditions Reduction Program End Stage Renal Disease Incentive Program Physician value Based Payments
SNF Value Based Program
Reward better value, outcomes & innovation in shorter LOS
Leverage purchasing power in the LTC sector to incentivize SNFs to improve quality
Align incentives & improve care coordination
12
www.zhealthcare.com 13
www.zhealthcare.com 14
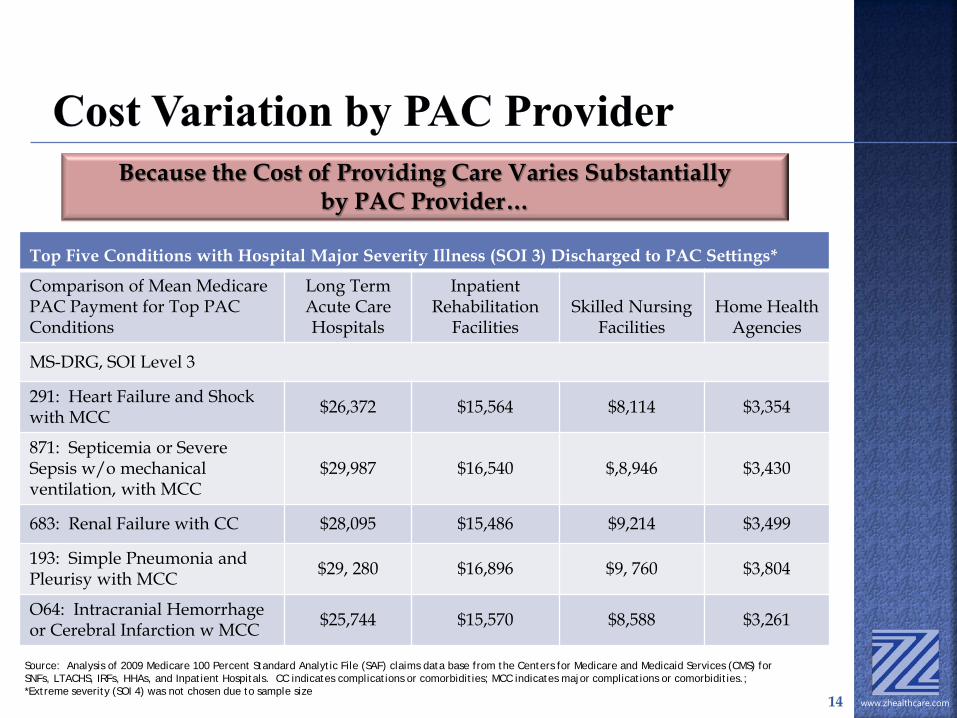
Top Five Conditions with Hospital Major Severity Illness (SOI 3) Discharged to PAC Settings*
Comparison of Mean Medicare PAC Payment for Top PAC Conditions
Long Term Acute Care Hospitals
Inpatient Rehabilitation
Facilities Skilled Nursing
Facilities Home Health
Agencies
MS-DRG, SOI Level 3
291: Heart Failure and Shock with MCC $26,372 $15,564 $8,114 $3,354
871: Septicemia or Severe Sepsis w/o mechanical ventilation, with MCC
$29,987 $16,540 $,8,946 $3,430
683: Renal Failure with CC $28,095 $15,486 $9,214 $3,499
193: Simple Pneumonia and Pleurisy with MCC $29, 280 $16,896 $9, 760 $3,804
O64: Intracranial Hemorrhage or Cerebral Infarction w MCC $25,744 $15,570 $8,588 $3,261
Because the Cost of Providing Care Varies Substantially by PAC Provider…
Source: Analysis of 2009 Medicare 100 Percent Standard Analytic File (SAF) claims data base from the Centers for Medicare and Medicaid Services (CMS) for SNFs, LTACHS, IRFs, HHAs, and Inpatient Hospitals. CC indicates complications or comorbidities; MCC indicates major complications or comorbidities.; *Extreme severity (SOI 4) was not chosen due to sample size

www.zhealthcare.com
Increase of $920 M (2.4%) to Skilled Nursing Facilities for 2017 Staying with the same RUG classifications and MDS assessments
completed in compliance with MDS Manual Specifies potentially preventable all-cause 30-day readmission
measure for the Skilled Nursing Facility Value Based Purchasing Program (SNF VBP) Implements requirements including performance standards, scoring
methodology Includes review/correction policies and measures for the Skilled
Nursing Quality Performance Program (SNF QRP) Quarterly confidential feedback reports specific to CASPER Public reporting on NH Compare of SNFs receiving value-based
incentive payments for high quality; SNFs will be listed by ranking Adds new Quality and Resource Measures as part of
requirements for IMPACT All cause all condition hospital readmission measure A resource use measure An all condition risk adjusted potentially preventable hospital
readmission measure 15

www.zhealthcare.com
Revisions to Five Star Quality Rating System New measures Survey & certification issues CASPER
Value-Based Purchasing Re-hospitalizations Incentives & penalties
Electronic Submission of Payroll Based Journals Nurse staffing
Revisions to Nursing Home Action Plan CMS response to Congressional action and implementation
Revisions to Medicare Intermediary Manuals RAC and MAC review SNF PUF data
OIG Work Plan Compliance
16

www.zhealthcare.com
SNF Level of Care –Administrative Presumption Administrative Presumption utilizes the beneficiary’s initial
classification in one of the upper 52 SNF level RUGs on the Medicare 5 day initial assessment and meeting a SNF level of care
Beneficiary in the lower 14 RUG levels is not automatically disqualified, however it is incumbent upon the SNF to ensure the level of care is appropriate, includes monitoring of condition and documentation
Consolidated Billing rules and exclusions continue with no changes
Impact Act Medicare claim based Measure Discharges to Community based on PAC-SNF-QRP
IMPACT Act SNF QRP Quality Measure Potential or Actual clinically significant medications identified on
admission Timely review to include medication accuracy and impact on function
& safety SOM to include guidelines for management and review
17

www.zhealthcare.com
As part of IMPACT 2014 and Final Rule 2016, beginning with payments in 2018, Secretary shall reduce annual market basket updates by 2% for any SNF that does not comply with quality submission requirements FY 2018 reporting year is based on data collected and
submitted for admissions on/after October 1, 2016 and discharged from SNF by December 31, 2016
80% compliance with Medicare Part A MDS submissions required to calculate SNF QRP measures
90% of Medicare payments tied to quality/value in 2018
18

www.zhealthcare.com
Reward SNFs with incentive payments for the delivery of Quality of Care
It begins in Fiscal Year 2019 (October 2018) Collection of Data October 2016 utilized in Standards to be published
2017 Promotes better clinical outcomes and intended to improve care
in the facility Will pay SNFs for their services based on Quality of Care, not
just Quantity Part of 2014 Protecting Access Medicare Act (PAMA)
Utilizes Quality Measures Establishes Performance Standards Scores reported publically
Most important Measures include 30 Day All Cause Readmission Measure (included in the SNF Final
Rule 2016) Potentially Preventable Readmission
19

www.zhealthcare.com
Implementation of new quality measures based on hospital readmissions, ED visits and quality outcomes
Establish performance standards for achievement and improvement
Rank SNFs from low to high Issue bonus payments and penalties
beginning FY 2019 Specify an all cause, all condition readmission
measure
20
www.zhealthcare.com
Readmissions within 30 days of discharge from hospital regardless of whether the beneficiary is readmitted
directly from SNF or had been discharged from SNF Impact on both in-house and discharged
residents Risk-adjusted adjusted based on patient demographics, principal
diagnosis in prior hospitalization, comorbidities, and other health status variables that affect probability of readmission
Excludes planned readmissions Similar to hospital readmission measures
21

www.zhealthcare.com
17% to 20% of Medicare beneficiaries discharged from hospital are readmitted within 30 days
84% of 7 day readmissions were potentially preventable
75% of 15- and 30-day readmissions were potentially preventable
Potential savings: $12B (30-day), $8B (15-day), and $5B (7-day)
22

www.zhealthcare.com
Requires SNFs to report standardized data (VBP & IMPACT) for measures in specified Quality and Resource use domains Information collected in October 2016 will be utilized for facility rates
in October 2018
SNF QRP Measures will also affect payment in 2018 Percent of Residents with Pressure Ulcers that are new or worsened
(SS)
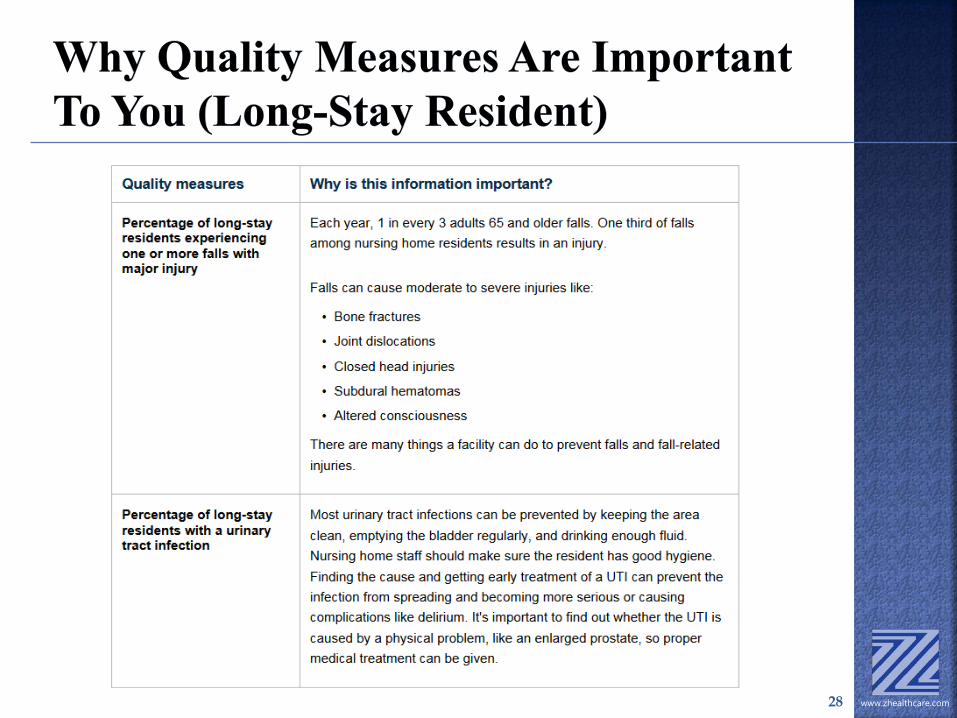
Percent of Residents experiencing one or more Falls with major injury
Percent of Patients with an Admission and Discharge Functional Assessment and a Care Plan that addresses function
Incorporates SNF VBP and Performance Improvement awards for 2019 payments January 1, 2017 thru December 31, 2017 will be the Collection Year for
2019
Will use a 0 to 100 point score with 25%, 50% and 75% thresholds and benchmarks
23
www.zhealthcare.com
SNFs will have an opportunity to review and provide corrections to their performance information that will be made public
CMS adopted a process by which one of the quarterly reports would be used to provide SNFs with A count of readmissions The number of eligible stays at the SNF The SNF’s risk-standardized readmissions ratio,
and The national SNF measure performance rate 24
www.zhealthcare.com
3 types of performance measures, each of which has its own individual rating system Health Inspections
‒ Measured on the 3 most recent annual surveys ‒ Higher weighting for more recent surveys ‒ Compared to rest of the state
Staffing ‒ Adjusted based on RUG-53 case-mix ‒ Payroll-based journal
25
National Average Hours Per Resident Per Day Total Nursing Staff 4.0309 Registered Nurses 0.7472

www.zhealthcare.com
Quality measures with scores/percentages/calculations available 16 total measures 4 most recent quarters Minimum sample size for inclusion in
calculations is 20 (across 4 quarters) for both long- and short-stay measures
Both MDS and claim-based measures
26

www.zhealthcare.com
Phased into 5 Star between July 2016 and January 2017
New measures will only count for half of the weighting through December 31, 2016
100% weight effective January 2017 Using national cut points for the new ADL
QM, as opposed to state-specific thresholds Recalculating all QM cut points to reflect
current national averages
27
www.zhealthcare.com 28

www.zhealthcare.com 29

www.zhealthcare.com 30
www.zhealthcare.com 31
www.zhealthcare.com 32
www.zhealthcare.com 33
www.zhealthcare.com 34
www.zhealthcare.com 35

www.zhealthcare.com 36

www.zhealthcare.com 37
www.zhealthcare.com 38
www.zhealthcare.com
Quality measures used across all PAC providers
Used to gauge outcomes, cost, and quality Focus on residents, self-care, mobility, and
function across the continuum Incorporates assessment and care planning Requires interdisciplinary documentation
that coordinates between therapy and nursing
Identify real function at different points in time
39
www.zhealthcare.com
Achievement Score: Points awarded by comparing the facility’s rate during the performance period (CY 2017) with the performance of all facilities nationally during the baseline period (CY 2015) Rate better or equal to benchmark: 100 points Rate Worse than achievement threshold: 0 points Rate between 1-99: Awarded points as per the
final rule
40

www.zhealthcare.com
Improvement Score: Points awarded by comparing the facility’s rate during the performance period (CY 2017) with its previous performance during the baseline period (CY 2015) Rate better than or equal to benchmark: 90 points Rate worse than improvement threshold; 0 points Rate between 1-89 points: awarded according to
the formula in the Final Rule
41

www.zhealthcare.com
What are your Metrics? What and How is it Tracked? Measured? Analyzed? Translates
into Financial terms?
Are you functioning with Clinical and Financial Silos? How to utilize Clinical/Quality and Cost equations? Identify areas for clinical and cost improvement
Are you gathering/using outdated or complex reporting
information? Develop a healthcare analytics strategy
Are you able to implement Data Driven Changes?
Are you implementing QAPI as detailed in the SOM
Rules of Participation?
42
www.zhealthcare.com
Creating a learning environment to create healthy clinical and financial collaborations using data to drive improvement Admission process Treatment plans Cost of Care LOS Discharge Planning Documentation Resident Satisfaction Coordination of care
QAPI Where do you want to be as an Organization in 2020?
Working together for sustainable improvement and good outcomes
43
www.zhealthcare.com
Implementation of the SOM Phase 1 Rules for Participation “New” Survey Process begins November 28, 2016 Revisions of policies and care delivery
Official collection period begins for PBJ The deadline for the first required submission is
February 14, 2017 Not utilized until 2018
Section GG & other changes (MDS) for new admissions Facilities will be able to review first Q in January
Hospital readmissions Now
CMS will issue reports for SNF review & identification of errors
44

www.zhealthcare.com 45