seizures - norwichsimulation.orgnorwichsimulation.org/images/pdfs/seizurespresentation.pdf ·...
TRANSCRIPT

Seizures
Overview
• 5% of paeds a+endances to ED

Status Epilepticus
‘’generalised convulsions las7ng 30 minutes or longer’’ • or ‘’failed to regain consciousness between fits over 30 minutes’’
Why is SE important?
• 4% mortality
• Significant morbidity: • Epilepsy • Learning difficul7es • Behavioural problems • Motor deficits
Why is it important?
• Cerebral autoregula7on is impaired • Compromises blood flow
• Vicious cycle of anaerobic metabolism and lac7c acidosis • Neuronal cell oedema/ death • Increased intracranial presssure à further reduced perfusion
• Systemic: Leucocytosis, acidosis, DIC, Rhabdomyolysis, cardiac dysfunc7on-‐ pulmonary oedema


Neonates
• Subtle • Motor or behavioural or autonomic
• Hypoglycemia <2mmol/L • Feeding difficul7es, sepsis or metabolic disorders • ℞ 2 ml/kg of 10% Glucose iv
• NAI
Febrile seizures
• 6 months to 6 years • Self-‐limi7ng <15 min • 5% with status
CNS infection
• Febrile CSE • Local an7bio7c policy
• Epilepsy • Not everyone with seizures has epilepsy • h/o AED-‐ compliance, change or withdrawal
• Poisoning
• Non-‐convulsive or par7al

Hx and examination
• Focused clinical history • Simultaneously assessing/managing ABC • Drug/allergy hx
• Directed examina7on: Meningism, rash, fever, trauma • Thorough examina7on a]er stabilisa7on-‐ infec7on screen, neuro, fundoscopy, etc

Mx
• Airway manoeuvres • NP airway (cau7on: Head injury)
• Reduced LOC à intubate
• Simultaneous-‐ iv or IO access/ samples • VBG-‐ glucose, electrolytes, mixed metabolic and resp acidosis • Bedside BM



Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
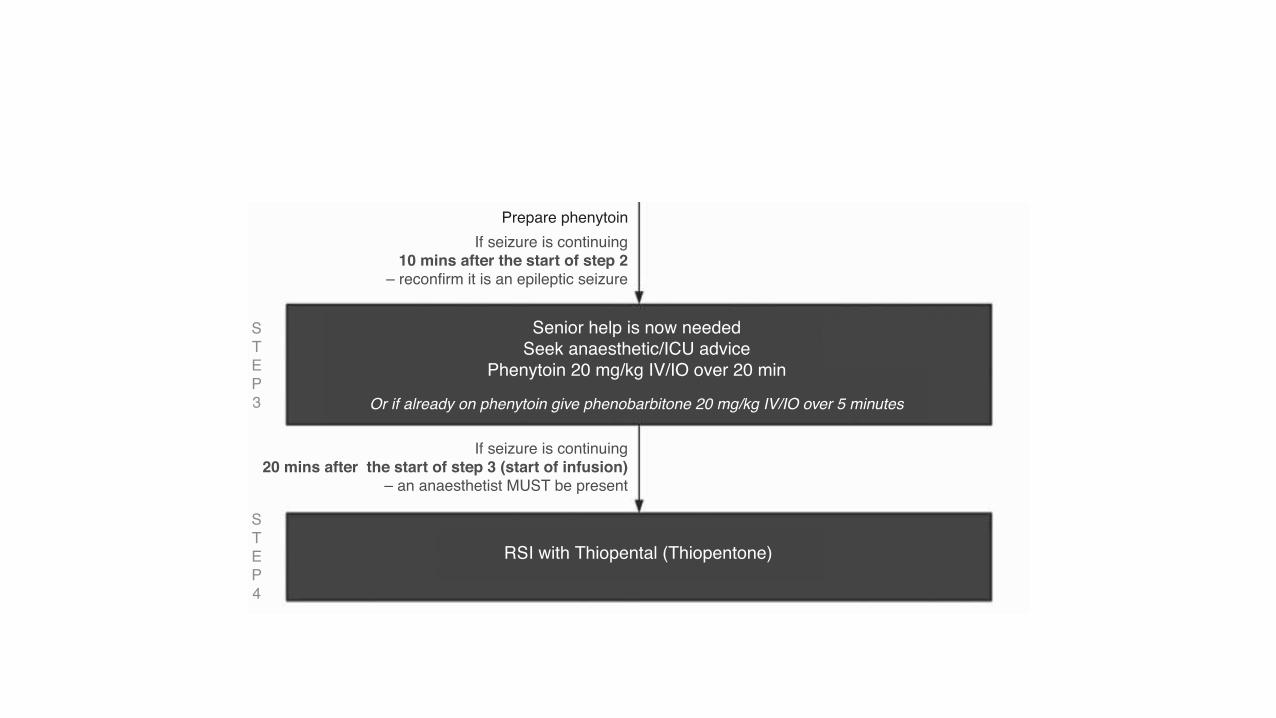
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions

Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions

Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions

• Or Diazepam 0.25 mg/kg iv
Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions

Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions
Lorazepam0.1 mg/kg IV/IO
Vascular Access?
STEP1
STEP2
STEP3
STEP4
5 minutes after convulsion started
Yes or canbe established quickly
If seizure is continuing 10 mins after start of step 1
Or if already on phenytoin give phenobarbitone 20 mg/kg IV/IO over 5 minutes
Prepare phenytoin
If seizure is continuing20 mins after the start of step 3 (start of infusion)
– an anaesthetist MUST be present
If seizure is continuing10 mins after the start of step 2
– reconfirm it is an epileptic seizure
AirwayHigh-flow oxygen
Don’t ever forget glucose
Lorazepam0.1 mg/kg IV/IO
Call for senior help
RSI with Thiopental (Thiopentone)
Senior help is now neededSeek anaesthetic/ICU advice
Phenytoin 20 mg/kg IV/IO over 20 min
Midazolam (buccal)0.5 mg/kg or
Diazepam (rectal)0.5 mg/kg
A charity dedicated to saving lifeby providing training
AdvancedLifeSupportGroup
No
Figure 10.1. Status epilepticus treatment algorithm (reproduced with kind permission of the Advanced LifeSupport Group).
100 Section 2: Clinical Conditions

CSE
• Longer a fit con7nues, more difficult it can be to terminate • More likely to intubate • Think ahead and have essen7al drugs • Senior anaesthe7c help sooner
• Phenytoin alternate: • Phenobarbitone • Leve7racetam • Valproate

Intubation and sedation
• RSI-‐ thiopentone • Morphine and Midazolam infusion • Short ac7ng relaxant • D/w PICU • Further seizures-‐ further AED; midaz bolus; double M+M rate
• Reassess; review blood reports; CT; NGT • Normothermia/carbia/glycaemia/30’headup

Further after I&V
• Seizure controlled and cause corrected • Extubate or transfer • d/w ter7ary centre • Depending on age, cause, ward and medical cover • Minimise delay of transfer
Summary
• Management is highly protocolised • Early VBG and don’t forget glucose • Decisive and 7mely interven7on could prevent long-‐term injury.