section for child care regulation
TRANSCRIPT

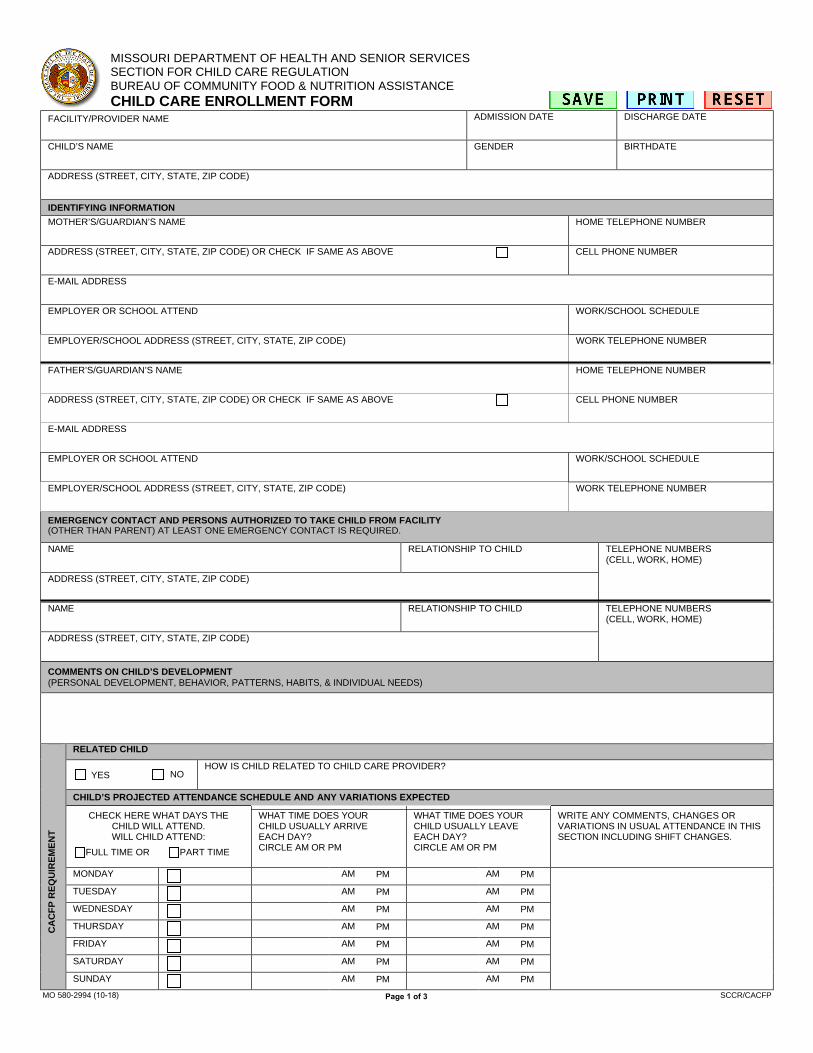
MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES SECTION FOR CHILD CARE REGULATION BUREAU OF COMMUNITY FOOD & NUTRITION ASSISTANCE CHILD CARE ENROLLMENT FORM
FACILITY/PROVIDER NAME ADMISSION DATE DISCHARGE DATE
CHILD’S NAME GENDER BIRTHDATE
ADDRESS (STREET, CITY, STATE, ZIP CODE)
IDENTIFYING INFORMATION MOTHER’S/GUARDIAN’S NAME HOME TELEPHONE NUMBER
ADDRESS (STREET, CITY, STATE, ZIP CODE) OR CHECK IF SAME AS ABOVE CELL PHONE NUMBER
E-MAIL ADDRESS
EMPLOYER OR SCHOOL ATTEND WORK/SCHOOL SCHEDULE
EMPLOYER/SCHOOL ADDRESS (STREET, CITY, STATE, ZIP CODE) WORK TELEPHONE NUMBER
FATHER’S/GUARDIAN’S NAME HOME TELEPHONE NUMBER
ADDRESS (STREET, CITY, STATE, ZIP CODE) OR CHECK IF SAME AS ABOVE CELL PHONE NUMBER
E-MAIL ADDRESS
EMPLOYER OR SCHOOL ATTEND WORK/SCHOOL SCHEDULE
EMPLOYER/SCHOOL ADDRESS (STREET, CITY, STATE, ZIP CODE) WORK TELEPHONE NUMBER
EMERGENCY CONTACT AND PERSONS AUTHORIZED TO TAKE CHILD FROM FACILITY (OTHER THAN PARENT) AT LEAST ONE EMERGENCY CONTACT IS REQUIRED.
NAME RELATIONSHIP TO CHILD TELEPHONE NUMBERS (CELL, WORK, HOME)
ADDRESS (STREET, CITY, STATE, ZIP CODE)
NAME RELATIONSHIP TO CHILD TELEPHONE NUMBERS (CELL, WORK, HOME)
ADDRESS (STREET, CITY, STATE, ZIP CODE)
COMMENTS ON CHILD’S DEVELOPMENT (PERSONAL DEVELOPMENT, BEHAVIOR, PATTERNS, HABITS, & INDIVIDUAL NEEDS)
CA
CFP
REQ
UIR
EMEN
T
RELATED CHILD
YES NO HOW IS CHILD RELATED TO CHILD CARE PROVIDER?
CHILD’S PROJECTED ATTENDANCE SCHEDULE AND ANY VARIATIONS EXPECTED
CHECK HERE WHAT DAYS THE CHILD WILL ATTEND. WILL CHILD ATTEND:
FULL TIME OR PART TIME
WHAT TIME DOES YOUR CHILD USUALLY ARRIVE EACH DAY? CIRCLE AM OR PM
WHAT TIME DOES YOUR CHILD USUALLY LEAVE EACH DAY? CIRCLE AM OR PM
WRITE ANY COMMENTS, CHANGES OR VARIATIONS IN USUAL ATTENDANCE IN THIS SECTION INCLUDING SHIFT CHANGES.
MONDAY AM PM AM PM
TUESDAY AM PM AM PM
WEDNESDAY AM PM AM PM
THURSDAY AM PM AM PM
FRIDAY AM PM AM PM
SATURDAY AM PM AM PM
SUNDAY AM PM AM PM
MO 580-2994 (10-18) Page 1 of 3 SCCR/CACFP

CA
CFP
REQ
UIR
EMEN
T CHECK THE MEALS YOUR CHILD IS USUALLY GIVEN AT THIS FACILITY
BREAKFAST MORNING SNACK LUNCH AFTERNOON SNACK SUPPER EVENING SNACK NONE
CHECK THE HOLIDAYS YOUR CHILD IS IN CARE AT THIS FACILITY
NEW YEARS’S DAY (JANUARY) MARTIN LUTHER KING JR.’S BIRTHDAY (JANUARY)
PRESIDENT’S DAY (FEBRUARY) EASTER (MARCH/APRIL)
MEMORIAL DAY (MAY) INDEPENDENCE DAY (JULY) LABOR DAY (SEPTEMBER) COLUMBUS DAY (OCTOBER)
VETERANS DAY (NOVEMBER) ELECTION DAY (NOVEMBER) THANKSGIVING (NOVEMBER) CHRISTMAS DAY (DECEMBER)
AUTHORIZATION FOR EMERGENCY MEDICAL CARE
I UNDERSTAND THAT I WILL BE NOTIFIED AT ONCE IN CASE OF AN EMERGENCY WITH MY CHILD, AND I WILL MAKE ARRANGEMENTS FOR MEDICAL CARE OF MY CHILD WITH THE PHYSICIAN OR HOSPITAL OF MY CHOICE.
IF I CANNOT BE REACHED TO MAKE NECESSARY ARRANGEMENTS, OR IN A CRITICAL EMERGENCY REQUIRING MEDICAL CARE, I AUTHORIZE
DAY CARE PROVIDER OR HOME PROVIDER TO CONTACT THE FOLLOWING:
PHYSICIAN OR CLINIC NAME TELEPHONE NUMBER
PREFERRED HOSPITAL NAME TELEPHONE NUMBER
ACKNOWLEDGEMENTS
A I HAVE RECEIVED A COPY OF THIS FACILITY’S POLICIES PERTAINING TO THE ADMISSION, CARE AND DISCHARGE OF CHILDREN.
PARENT/GUARDIAN INITIALS
B I HAVE BEEN INFORMED THAT A COPY OF THE LICENSING RULES FOR CHILD CARE HOMES OR THE LICENSING RULES FOR GROUP CHILD CARE HOMES AND CENTERS IS AVAILABLE AT THIS FACILITY FOR REVIEW.
PARENT/GUARDIAN INITIALS
C THE PROVIDER AND I HAVE AGREED ON A PLAN FOR CONTINUING COMMUNICATION REGARDING MY CHILD’S DEVELOPMENT, BEHAVIOR, AND INDIVIDUAL NEEDS.
PARENT/GUARDIAN INITIALS
D WHEN MY CHILD IS ILL, I UNDERSTAND AND AGREE THAT S/HE MAY NOT BE ACCEPTED FOR CARE OR REMAIN IN CARE.
PARENT/GUARDIAN INITIALS
E I UNDERSTAND THAT, BEFORE THE FIRST DAY OF ATTENDANCE BY MY CHILD, I WILL PROVIDE PROOF OF COMPLETED AGE-APPROPRIATE IMMUNIZATIONS OR EXEMPTION FROM IMMUNIZATIONS.
PARENT/GUARDIAN INITIALS
F I DO DO NOT GIVE PERMISSION FOR FIELD TRIPS/EXCURSIONS.
I UNDERSTAND I WILL BE NOTIFIED IN ADVANCE WHEN THEY ARE PLANNED.
PARENT/GUARDIAN INITIALS
G I DO
DO NOT GIVE PERMISSION FOR THE FACILITY TO TRANSPORT MY CHILD.
PARENT/GUARDIAN INITIALS
H I HAVE BEEN INFORMED AND HAVE RECEIVED A COPY OF THE FACILITY’S SAFE SLEEP POLICY WHEN ENROLLING A CHILD LESS THAN ONE (1) YEAR OF AGE.
PARENT/GUARDIAN INITIALS
I I HAVE BEEN NOTIFIED THAT I MAY REQUEST NOTICE AT INITIAL ENROLLMENT OR ANY TIME THERE AFTER WHETHER THERE ARE CHILDREN CURRENTLY ENROLLED IN OR ATTENDING THE FACILITY FOR WHOM AN IMMUNIZATION EXEMPTION HAS BEEN FILED.
PARENT/GUARDIAN INITIALS
PARENT’S/GUARDIAN’S SIGNATURE DATE
CA
CFP
R
EQU
IREM
ENT
FIRST ANNUAL UPDATE PARENT/GUARDIAN SIGNATURE DATE
SECOND ANNUAL UPDATE PARENT/GUARDIAN SIGNATURE DATE
THIRD ANNUAL UPDATE PARENT/GUARDIAN SIGNATURE DATE
MO 580-2994 (10-18) Page 2 of 3 SCCR/CACFP

MO 580-2851 (6-14) TO BE FILED IN CHILD’S RECORD AT CHILD CARE FACILITY. BCC-6B
MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICESSECTION FOR CHILD CARE REGULATIONPARENT’S HEALTH STATEMENT FOR SCHOOL-AGE CHILD
IDENTIFYING INFORMATIONCHILD’S NAME BIRTHDATE
HEALTH STATEMENT (CHECK ONE)
My child is in good health, is able to participate in group care, has no special health or medical requirements.
My child is able to participate in group care but has special health or medical requirements as listed below.
SCHOOL-AGE CHILD’S SPECIAL HEALTH OR MEDICAL REQUIREMENTSPLEASE LIST ANY ALLERGIES, SPECIAL MEDICAL CONDITIONS, INCLUDING CHRONIC HEALTH PROBLEMS (SUCH AS ASTHMA, SEIZURES), BEHAVIORAL DISORDERS,SPECIAL NEEDS, ETC.
PARENT OR LEGAL GUARDIAN SIGNATURE DATE

MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICESSECTION FOR CHILD CARE REGULATION
MEDICATION AUTHORIZATION
MO 580-1875 (6-14) FORM TO BE RETAINED IN CHILD’S RECORD BCC-11
MEDICATION REQUIREMENT
RECORD OF ADMINISTRATION
PRESCRIPTION MEDICATION SHALL BE IN THE ORIGINAL CONTAINER AND LABELED WITH THE CHILD’S NAME, INSTRUCTIONS,INCLUDING TIMES AND AMOUNTS FOR DOSAGES, AND THE PHYSICIAN’S NAME. ALL NON-PRESCRIPTION MEDICATION SHALLBE IN THE ORIGINAL CONTAINER AND LABELED BY THE PARENT(S) WITH THE CHILD’S NAME AND INSTRUCTIONS FORADMINISTRATION, INCLUDING TIMES AND AMOUNTS FOR DOSAGES. A SEPARATE FORM IS NEEDED FOR EACH MEDICATION.THIS FORM IS VALID ONLY FOR THE DATES INDICATED BELOW.
I AUTHORIZE CHILD CARE PERSONNEL TO ADMINISTER THE FOLLOWING MEDICATION TO MY CHILD:
(PROPER NAME OF MEDICATION)
CHILD’S FULL NAME DATE MEDICATION TAKEN FROM UNTIL
DOSAGE TIME(S) OF DAY
POSSIBLE SIDE EFFECTS
SIGNATURE OF PARENT(S) OR GUARDIAN DATE
STAFF NAME DATE MEDICATION NAME DOSAGE TIME

COVID-19 Screening Questions
Date: _________________________
Child’s Name (first and last name):______________________________________________________________________________
Date of Birth (mmddyy): __________________________________
COVID-19 Screening
Questions
YES NO
Does child or anyone in your
household have any of the
following?
□ Fever or feeling feverish
(chills, sweating) □ Shortness
of breath (not severe) □ Cough
In the past 14 days, has your
child or any household member
traveled outside the four
state? If so, where:
______________________________________
In the past 14 days, has your
child or any household member
had any contact with a person
who has tested positive for
COVID-19?
Has your child or any
household member have a
history of exposure to
COVID19 biologic material?
__________________________________ _______________________________________
PRINT NAME PARENT/GUARDIAN SIGNATURE

Assumption of the Risk and Waiver of Liability Relating to Coronavirus/COVID-19
The novel coronavirus, COVID-19, has been declared a worldwide pandemic by the World Health Organization.
COVID-19 is extremely contagious and is believed to spread mainly from person-to-person contact. The Joplin
Family YMCA (JFY) has put in place preventative measures to reduce the spread of COVID-19; however, the JFY
cannot guarantee that you will not become infected with COVID-19. Further, participation could increase your risk
of contracting COVID-19.
READ CAREFULLY BEFORE SIGNING – INITIAL EACH PARAGRAPH
____ INITIALS By signing this agreement, I acknowledge the contagious nature of COVID-19 and voluntarily assume the risk that I may be exposed to or infected by COVID-19 by participation; and that such exposure or infection may result in personal injury, illness, permanent
disability, and death. I understand that the risk of becoming exposed to or infected by COVID-19 at the JFY may result from the actions,
omissions, or negligence of myself and others, including, but not limited to, the JFY’s employees, volunteers, and program participants
and their families.
____ INITIALS I voluntarily agree to assume all of the foregoing risks and accept sole responsibility for any injury to myself (including, but not limited to, personal injury, disability, and death), illness, damage, loss, claim, liability, or expense, of any kind, that I may experience or incur
in connection with my participation at the JFY. On my behalf, I hereby release, covenant not to sue, discharge, and hold harmless the JFY,
its employees, agents, and representatives, of and from the Claims, including all liabilities, claims, actions, damages, costs or expenses
of any kind arising out of or relating thereto. I understand and agree that this release includes any Claims based on the actions,
omissions, or negligence of the JFY, its employees, agents, and representatives, whether a COVID-19 infection occurs before, during,
or after participation at the JFY.
____ INITIALS I represent that I have adequate insurance to cover any injury or illness I may suffer or cause while participating in this
activity, or else I agree to bear the costs of such injury or illness myself. I further represent that I have no medical or physical condition
which could interfere with my safety in this activity, or else I am willing to assume – and bear the costs of – all risks that may be
created, directly or indirectly, by any such condition.
____ INITIALS In the event that I file a lawsuit, I agree to do so in the state where the JFY is located, and I further agree that the
substantive law of that state shall apply. I agree that if any portion of this agreement is found to be void or unenforceable, the
remaining portions shall remain in full force and effect.
____ INITIALS By signing this document, I agree that if I am exposed or infected by COVID-19 during my participation in this activity, then I may be found by a court of law to have waived my right to maintain a lawsuit against the parties being released on the basis of any claim for negligence.
____ INITIALS I have had sufficient time to read this entire document and, should I choose to do so, consult with legal counsel prior to signing.
Also, I understand that this activity might not be made available to me or that the cost to engage in this activity would be significantly
greater if I were to choose not to sign this release, and agree that the opportunity to participate at the stated cost in return for the
execution of this release is a reasonable bargain. I have read and understood this document and I agree to be bound by its terms.
____ INITIALS If I have signed a separate general waiver of liability connected to my participation at the JFY, I agree that the terms of
that waiver are wholly incorporated into this document and that the terms of this document are incorporated into the separate general
waiver.
____ INITIALS I agree that I will practice safe social distancing and clean hygiene during my participation at the JFY.
Signature Print Name
Address City State Zip
Telephone ( ) Date
Emergency Contact__________________________________ Emergency Contact Number______________________________________
PARENT OR GUARDIAN ADDITIONAL AGREEMENT (Must be completed for participants under the age of 18)
In consideration of _________________________________ (PRINT minor’s names) being permitted to participate in this activity, I further agree to
indemnify and hold harmless Releasees from any claims alleging negligence which are brought by or on behalf of minor or are in any
way connected with such participation by minor.
Parent or Guardian Print Name Date

JOPLIN FAMILY YMCA
3404 W. McIntosh Circle Dr., Joplin, MO 64804 P 417 781 9622 F 417 625 2503
School Age Services Enrollment and Handbook Acknowledgements
Child Name: ______________________________________ Date of Birth:____________________________
Program Participating In (Circle One): After School Summer Day Camp Winter/Spring Activity Days
School your child is attending:_________________________________________________________
I, _______________________________________________________ acknowledge that I have been provided with a copy of the parent
handbook outlining the following policies, releases, and program information:
Media Release- I am giving my child permission to be a part of YMCA’s advertising, photo promotions highlighting
our child care programs: YES of NO (please circle one)
Please Initial ____________________
Authorization for Release of Information- I am giving my child’s attending school authorization to release
information that will assist with completing enrollment and assist with any program concerns: YES or NO
(please circle one) Please initial ______________________
Behavior Management Procedures and Discharge Policy- Children who attend our program are expected to interact
appropriately and follow behavior guidelines outlined in parent handbook.
Foster/Adoptive Parent Child Care Subsidy- Children must use our program every day and not miss more than 5
days in a month. Children are checked in upon arrival that day and must stay a minimum of 30 minutes that day, if
not the state will not authorize payment. See more information in the parent handbook.
Late Fee and Pick-up Policy- Normal business hours for are 2:30 p.m. 6:00 p.m. Monday thru Friday. A fee of
$10.00 will be assessed after a 10 minute grace period and assessed $10.00 every 10 minutes thereafter. Please
note we do not provide services at school locations when school is not in section and earlier outs.
Release and Waiver of Liability and Indemnity Agreement- In consideration for being permitted to utilize the
facilities, services and programs of the YMCA an expressed agreement that foregoing information has been
outlined in the parent handbook regarding this matter.
_________________________________________________________ ________________________
Print Name Date
_________________________________________________________
Parent/Guardian Signature

FOR YOUTH DEVELOPMENT®
FOR HEALTHY LIVING
FOR SOCIAL RESPONSIBILITY
JOPLIN FAMILY YMCA
FINANCIAL AGREEMENT &
AUTHORIZATION FOR
AUTOPAYMENT
Child's Name Date of Birth ------------------------------- --------
Responsible Party's Information
Name ----------�F-irs_t ___________ M_I ___________ La_s_t -------------
Address -----�S-tr -ee-1-----------�Ap_t_#------�C�it_y ______ �S-tate
Home Phone # Cell Phone # Work# Zip
----------- ----------- ------------
Socia I Security# __________ Relationship to child _________ Email ____________ _
• Automatic bank and credit card drafts for the enrolled child's tuition are processed at 9am on Monday mornings,regardless of bank holidays, unless the Joplin Family YMCA billing office is closed.
• Weekly tuition is billed at a flat weekly rate. No other discounts will be provided based on closures or absences forholidays, illness, weather or any other unforeseeable events. I understand I will be charged the same rate every weekwhether the enrolled child attends the program or not.
• I understand I am only allowed ONE excused week of absences per calendar year.• A wrjtten notjce must be submjtted to Childcare Billing Office a week prior or no later than the Friday prior to
any additions/changes to the enrolled child's record/account. Add/Change Forms are available at the site oronline for me to use as written notice for cancellation out of the program and for additions/changes. If I do notprovide advance written notice, I will be charged the regular weekly rate.
• If the child is enrolled into the activity days or drop program, my payments are due in advance and must be receivedbefore the child attends the program. Proof of payment will be required at drop off. If payment is not made .b.e.fo.re. theenrolled child attends, I will incur a $10 late fee. If I do not make my payment in full by close of business Friday, mybalance will be automatically deducted from my bank account or charged to my credit card the following Monday.
• A ONE JIME and PERMANENT switch from the weekly program to the daily drop program (and vice versa) is allowed.Written notice of the switch must be submitted by a week or Friday prior to the planned week of change.
• I am fully responsible for updatjnq changes to my credjt/debjt card number expjratjon and securjty code or my bank
checkjnq/sayjnqs jnformatjon a week or the frjday prjor to my next bank draft date• If my payment for my tuition or balance is returned or declined, I will be notified immediately and will be assessed a $25
return-payment fee, and my payment will be due immediately.• If I do not make my payment in full by close of business Friday, the enrolled child will not be allowed to attend the
program until payment is made.• If I receive assistance through a third party agency, I am fully responsible for the remaining balance the third party
does not pay.• If the enrolled child is not allowed to attend the program due to non-payment and I do not make payment, I will be
referred to a third-party collection aqency.
BANK DRAFT (Attach a voided check to this form) CREDIT CARD DRAFT
Name on Bank Account Name on Card
Name of Bank Card Tv□e
Boutin□# #
Account# Exoiration Pate
D Checking D Savings Securitv Code
I have given authority to the above bank or credit card company to honor all preauthorized ACH drafts on my account for childcare payment and/or outstanding balance due for the current program my child is enrolled.
I understand that by signing this form I assume all financial responsibility for this child and agree to abide by all policies in the parent handbook (included with the enrollment packet).
Parent/Guardian Signature: _____________________________ Date: ____ _For confidentiality purposes, this document is only accepted by fax (417-625-2503), in person, or through the upload link on our After School Program webpage.

Revised 4/13/2021
School Age Services (Ages 5 to 12)
JOPLIN FAMILY YMCA School Plus After School Services
Out of School Activity Days
Summer School After School Extension
Summer Day Camp
School Plus Available at these area schools:
Carl Junction Elementary
Joplin School District
Cecil Floyd
Eastmorland
Irving
Kelsey Norman
McKinley
Royal Heights
Soaring Heights
Stapleton
West Central (Jefferson/Columbia)
Webb City School District
Madge T. James (Webster)
Mark Twain (Eugene Fields/Middle)
Carterville
Harry S. Truman
The Y’s mission: To promote a positive, nurturing
environment while protecting youth from any form of
abuse. Our staff have been trained in child abuse prevention.
Revised 4/13/2021
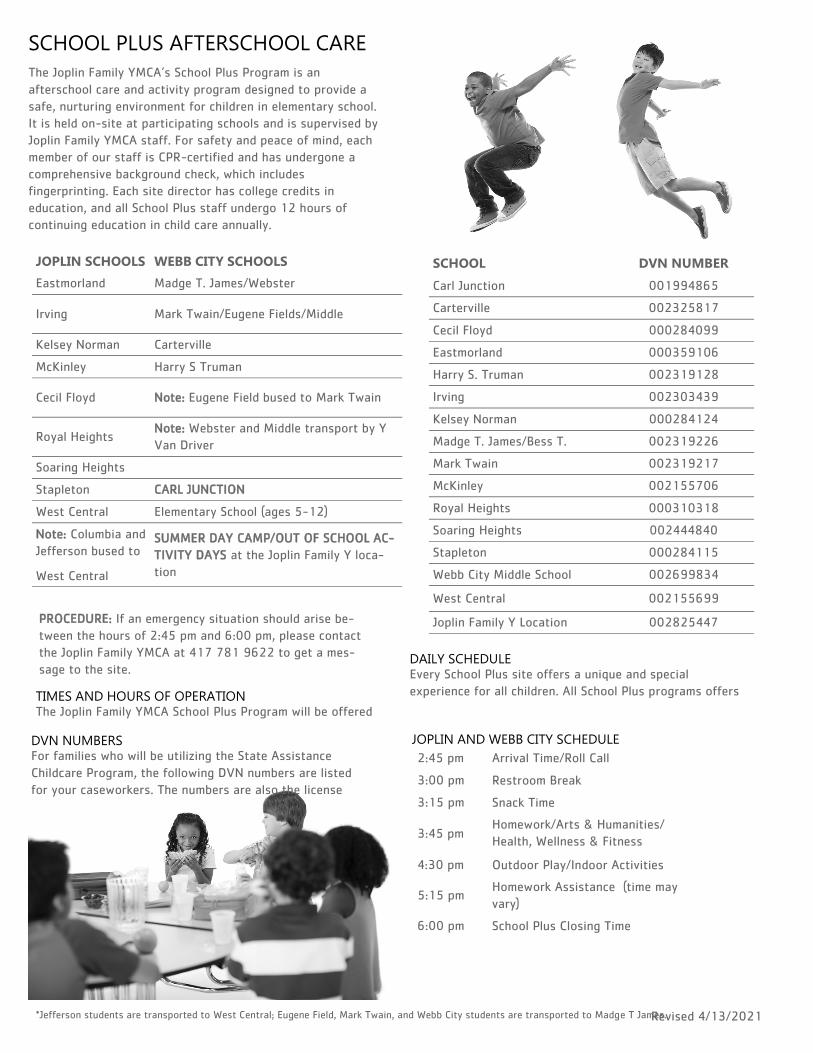
SCHOOL PLUS AFTERSCHOOL CARE
The Joplin Family YMCA’s School Plus Program is an
afterschool care and activity program designed to provide a
safe, nurturing environment for children in elementary school.
It is held on-site at participating schools and is supervised by
Joplin Family YMCA staff. For safety and peace of mind, each
member of our staff is CPR-certified and has undergone a
comprehensive background check, which includes
fingerprinting. Each site director has college credits in
education, and all School Plus staff undergo 12 hours of
continuing education in child care annually.
DAILY SCHEDULE Every School Plus site offers a unique and special
experience for all children. All School Plus programs offers
2:45 pm Arrival Time/Roll Call
3:00 pm Restroom Break
3:15 pm Snack Time
3:45 pm Homework/Arts & Humanities/
Health, Wellness & Fitness
4:30 pm Outdoor Play/Indoor Activities
5:15 pm Homework Assistance (time may
vary)
6:00 pm School Plus Closing Time
JOPLIN AND WEBB CITY SCHEDULE
*Jefferson students are transported to West Central; Eugene Field, Mark Twain, and Webb City students are transported to Madge T James.
TIMES AND HOURS OF OPERATION The Joplin Family YMCA School Plus Program will be offered
DVN NUMBERS For families who will be utilizing the State Assistance
Childcare Program, the following DVN numbers are listed
for your caseworkers. The numbers are also the license
SCHOOL DVN NUMBER
Carl Junction 001994865
Carterville 002325817
Cecil Floyd 000284099
Eastmorland 000359106
Harry S. Truman 002319128
Irving 002303439
Kelsey Norman 000284124
Madge T. James/Bess T. 002319226
Mark Twain 002319217
McKinley 002155706
Royal Heights 000310318
Soaring Heights 002444840
Stapleton 000284115
Webb City Middle School 002699834
West Central 002155699
Joplin Family Y Location 002825447
JOPLIN SCHOOLS WEBB CITY SCHOOLS
Eastmorland Madge T. James/Webster
Irving Mark Twain/Eugene Fields/Middle
Kelsey Norman Carterville
McKinley Harry S Truman
Cecil Floyd Note: Eugene Field bused to Mark Twain
Royal Heights Note: Webster and Middle transport by Y
Van Driver
Soaring Heights
Stapleton CARL JUNCTION
West Central Elementary School (ages 5-12)
Note: Columbia and
Jefferson bused to
West Central
SUMMER DAY CAMP/OUT OF SCHOOL AC-
TIVITY DAYS at the Joplin Family Y loca-
tion
PROCEDURE: If an emergency situation should arise be-
tween the hours of 2:45 pm and 6:00 pm, please contact
the Joplin Family YMCA at 417 781 9622 to get a mes-
sage to the site.

Revised 4/13/2021
WINTER/SPRING BREAK CAMPS
The Joplin Family YMCA’s Winter and Spring Break camps are
care and activity programs designed to provide a safe and
nurturing environment for children in elementary school on
winter and spring break respectively. Camps are held at the
Joplin Family Y and are supervised by Joplin Family Y staff. For
safety and peace of mind, all members of our staff are CPR
certified and have undergone background checks.
PROCEDURES Children must be dropped off at the Joplin Family Y between
7 am – 8 am and picked up between 3 pm – 6 pm. (Not this is
subject to change. Updates will be available on the
Joplinfamilyy.org website.
TIMES AND HOURS OF OPERATION The Winter and Spring Break camps are held Monday –
Friday; their start and end dates are based on the Joplin
School District’s calendar. Care is provided 7 am – 6 pm for
both camps.
DAILY SCHEDULE Each day’s activities, lunch, and snacks are determined prior
to each camp’s start.
DVN NUMBERS Winter/Spring Break camps do not qualify for the State
Assistance Childcare Program.
SUMMER DAY CAMP
The Joplin Family Y’s Summer Day Camp is a care and
activity program designed to provide a safe and nurturing
environment for children in elementary school on summer
break. Camp is held at the Joplin Family Y and includes daily
off-site activities. Camp is supervised by Joplin Family Y
staff. For safety and peace of mind, all members of our staff
are CPR certified and have undergone background checks.
Note: programming activities are subject to change.
PROCEDURES Children must be dropped off at the east door of Joplin
Family Y between 7 am – 7:30 am and picked up between 3
pm – 6 pm. Note: visit joplinfamiilyy.org website for any
changes/updates.
TIMES AND HOURS OF OPERATION Summer Break Camp is held Monday – Friday; its start and
end dates are based on the Joplin School District’s calendar.
DAILY SCHEDULE Each day’s activities and meals are determined prior to the
camp’s start.
Breakfast, lunch, and a “Fuel Up, Stay Fit” afternoon snack
are provided to all campers.
Kids will participate in daily enrichment and structured
physical activities.
3:20 pm Arrival Time
3:30 pm Combine Groups/Roll Call
4:00 pm Snack Time
4:30 pm Homework/Arts & Humanities/
Health, Wellness & Fitness
5:00 pm Outdoor Play/Indoor Activities
5:30 pm Homework assistance (time may
vary)
6:00 pm School Plus Closing Time
CARL JUNCTION SCHEDULE*
*Start time on Fridays accommodates the early dismissal time.
SUMMER SCHOOL PLUS EXTENSION
For children enrolled in summer school in Joplin, Carl Junction,
and Webb City, we provide an extension on our School Plus
program. Joplin students are bused to the Joplin Family Y for
care, Carl Junction students are cared for on-site, and Webb
City students are transported to Carterville Elementary School
for care. NOTE: This is subject to change, if transportation is
not offered by the school.
DVN NUMBERS
SCHOOL DVN NUMBER
Carl Junction 001994865
Carterville 002325817
Joplin Family Y 002825447
Revised 4/13/2021
SCHOOL AGE SERVICES POLICIES
All policies are final and without exception.
PAYMENT INFORMATION Each child is considered to have his/her own account, and
tuition is due IN ADVANCE for each child. If a parent has not
paid the fee, the child’s account will be considered unpaid,
resulting in the child not being able to attend. Services will be
suspended for accounts that become seven days past due.
We will not become involved in disputes with divorced or
separated parents as to who will pay the fee.
FEES
•No discounts will be given for partial weeks attended unless
we do not offer a full week of service.
•Every participant must also pay a non-refundable enrollment
fee due at the time of enrollment.
DRAFTED PAYMENTS Program payments for School Plus and Summer Day Camp are
made through weekly auto bank draft with credit or debit
card or through a checking or savings account. Auto-bank
drafts are processed at 9:00 am on Monday mornings,
regardless of bank holidays, unless the Joplin Family YMCA is
closed.
RETURNED-PAYMENT FEE If a bank or credit/debit card draft is returned or declined,
you will be notified immediately and will be assessed a $25
returned-payment fee, and your payment will be due
immediately. If you do not make your payment in full by close
of business on Friday, your child will be suspended from the
program until payment is made. If your child is suspended
from the program due to non-payment and you do not make
payment, you will be referred to a third-party collection
agency.
FINANCIAL ASSISTANCE
Financial Aid assistance is available. Please visit our
joplinfamilyy.org website for additional information. Families
who have received assistance previously must re-apply each
year. Parents are responsible for the balance owed after third
-party payments.
TAX STATEMENTS
End-of-year tax statements may be requested from the
Child Care Billing Office the last week of January. We
distribute tax information for the School Plus and Day
Camp Programs only. Your request can be made by
emailing [email protected].
ORIENTATION You will be oriented with the specific School Age Services
program when you register at the Joplin Family YMCA. You
will be asked to read through and sign the policies and fill out
an enrollment form. In addition to completing the
enrollment information, you will also need to supply us
with a copy of your child’s current immunization record.
LATE PICKUP FEE If a child is not picked up by 6:10 pm, a late fee will be
incurred. Additional late fees will be assessed every 10
minute increment thereafter. You will be emailed a late
pickup form along with the late fee amount via email.
ABANDONMENT After all attempts to contact parents and emergency contacts
have failed, a child who is not picked up by 7:00 pm will be
considered abandoned. The police department and the
Division of Family Services will be called.
SIGNING IN/OUT PROCEDURE It is mandatory that you or someone approved on your child’s
enrollment form sign your child out of the program each day.
A child may only be released to persons listed on the
enrollment form. Persons who do not regularly pick up your
child will be asked to show a picture ID. You also may be
asked for ID on occasion. Only individuals 16 years of age or
older may pick up a child from the program.
MEALS AND SNACKS Depending on the program, children may be provided a daily
breakfast, lunch, and/or a snack. Notify staff of any food
allergies. If your child does have food allergies, we will need a
doctor’s letter on file.
PARENT/GUARDIAN VISITATION Parents/guardians are welcome to visit School Age Services
programs at any time. We would love to have you share your
job skills or hobbies with us. Please contact the Joplin Family
Y if you wish to share your skills/hobbies during the program.
If at any time your visitation disrupts the program, you will
be asked to leave. Note: this is subject to change. Visit our
website at joplinfamilyy.org for any updates/changes.

Revised 4/13/2021
ILL CHILDREN
A child may NOT attend a School Age Services program if he/
she is experiencing any of the symptoms below:
•Fever of 100.4 degrees Fahrenheit or higher
•A rash that may be considered contagious
•Vomiting or diarrhea twice or more on the same day of the program
HEAD LICE (INCLUDING NITS OR EGGS) Children with head lice may not return until treated and upon our staff finding no evidence of eggs or lice. •Any other illness that is deemed contagious
Children who are suspected of having a contagious illness
SHALL NOT BE ACCEPTED INTO CARE. If a child becomes ill
while attending a School Age Services program, parents/
guardians are requested to come for their child at once.
Should the ill child have a fever of 100.4 degrees Fahrenheit
or above, or visible symptoms of an illness, the child will be
isolated from the other children and will be monitored by a
staff person until the parent/guardian arrives. Any neglect of
this policy may result in your child being permanently
released from the program.
MEDICATION POLICY Please list on your child’s enrollment form all medications
taken regularly. If an accident occurs, we will refer to their
enrollment form for taken medications and doses. As a
general rule, the School Age Services staff will not administer
medications unless absolutely necessary and required by the
doctor to be given during programming.
The medication must be in its original container, with the
pharmacist’s label marked with the prescription name, date,
child’s name, and physician’s name. (Your pharmacist will
provide an additional container for this purpose.)
At the end of the medication period, parents should take
home any unused medication. The School Plus Program is
separate from the school. We cannot accept or assume
instructions from the school concerning medication, ONLY
FROM YOU. The School Age Services department reserves
the right to refuse to administer medication to children in
our program; it is ultimately the parents’ responsibility to
ensure children receive their medication.
MEDIIA RELEASE
Child in our program may have opportunities to be
involved in media cover and/or photos demonstrating their
social skills and team building in the community.
RELEASE AND WAIVER OF LIBILITY HEREBY RELEASES WAIVES, DISCHARGES AND COVENANTS
NOT TO SUE the YMCA, its directors, officers, employees, and
agents; releases from all liability to the undersigned, his
personal representative, assigns, heirs, and next of kin for
any loss or damage, and any claim or demands thereof on
account of illness/injury to the person or property or
resulting in death of the undersigned, whether caused by the
negligence of the releases or otherwise.
ACCIDENTS The Joplin Family YMCA is not responsible for any injury
incurred while children are at any School Age Services
program. Parents/guardians will assume responsibility for all
medical costs while their children are attending Joplin Family
YMCA programs.
SPECIAL CARE PLANS If your child has special needs as defined by the Missouri
Department of Health and Senior Services, you will be required
to complete a Specialized Care Plan. All YMCA child care
programs try to accommodate children’s needs as much as
possible; unfortunately, there are times our programs cannot
meet the needs of all children. In such cases we will be glad to
offer suggestions for appropriate care through other
providers.
CHILD CUSTODY CASES, FOSTER CARE In a situation where one or both parents are prohibited by law
from having contact with their child, the custodial parent/court
-appointed guardian must present legal documents (e.g.
custodial order, ex parte order, etc.) informing us of the
situation. The Joplin Family Y cannot refuse a parent the right
to pick his/her child up if that parent is listed on the
enrollment form unless we have received legal documents
prohibiting that parent from having contact with the child.
BEHAVIOR MANAGEMENT AND DISCHARGE POLICY A write-up will be used any time a situation has occurred with
a child in which behavior has disrupted the program, harmed or
potentially harmed any child involved, or has caused concern
from staff that the behavior could serve to diminish the
program. The first write-up will serve as a warning to the
student and will be discussed with the parent/guardian. A
second write-up may result in a 1- to 5-day suspension from
the program. A third write-up may result in discharge from the
program until the following school year. Parents are not
allowed to employee Y staff for babysitting while their child is
in the program. IF A SEVERE BEHAVIOR INCIDENT OCCURS,
YOUR CHILD MAY BE SUSPENDED OR DISCHARGED
IMMEDIATELY.
ANTI-VIOLENCE The Joplin Family YMCA makes every effort to ensure the
safety of all children. That is why we will not tolerate any
violent or aggressive behavior. Bringing any potentially
dangerous objects to the program (knives, smoke bombs,
firecrackers, guns, etc.) is strictly prohibited.
You may schedule an appointment with the Director of School
Age Services at any time to discuss any issue relevant to your
child’s progress in the program.
PERSONAL PROPERTY The Joplin Family YMCA is not responsible for any personal
property brought to our programs. Please label your child’s
belongings. If any property is brought to a program site that
may cause a disruption, you will be asked to remove the
property.