_section 4 - oklahomanurses.org · web viewthe nurse planner guarantees that ancc coa and tna...
TRANSCRIPT

September 2014
Oklahoma Nurses Association6414 N. Santa Fe, Suite A
Oklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
APPROVED PROVIDER ACTIVITY DOCUMENTATION TOOLTITLE PAGE
Throughout this tool you will find items highlighted—these are to be removed, or changed to represent your organization name. DO NOT leave any highlighted items unattended.Organization Name:
Organization Address:
Street address
City State Zip Code
DEMOGRAPHIC DATA:
Date of first presentation: __________________
Location(s) of activity (if applicable)-City and State:
This activity is: (Please check one.)
Provider-Directed______ (live – in person or webinar) or Learner-Paced _____ (enduring material)
Start Date: ___________________ Expiration Date: ___________________
Number of Contact Hours Awarded: ________
How often will this activity be offered? _______ One-time _________ Multiple times
Is this continuing nursing education? Does the content of this education activity enable the Registered Nurse learner to acquire or improve knowledge, skills, or practice that promote the professional development or performance of the Registered Nurse while enhancing his/her contribution to quality healthcare? Is the content generalizable regardless of the employer? Does the content meet the definition of and criteria for continuing nursing education as outlined in chapter 216 of the Texas Board of Nursing’s rules and regulations?
Yes ___ Please continue to the next question. No ___ STOP! – You may not provide this activity for CNE.
Is a currently licensed Registered Nurse with a baccalaureate degree or higher in nursing is actively involved, as the Nurse Planner, in the planning, implementing and evaluation process of this continuing nursing education activity? Yes ____ Please continue.
No ____ STOP! You may not provide this activity for CNE.Please list the name and credentials and other necessary information of the Approved Provider Unit Nurse Planner involved with/responsible for this education activity:Nurse Planner: (Name and degrees/credentials)
Telephone: ______/ _______________ Extension: ________ FAX: ________/______________
E-mail: Alternate E-mail:
Will this activity offer other types of continuing education credit? Yes No
Form11092014 Page ___________
Title of activity:

September, 2014
If yes, what? Continuing Medical Education
Pharmacy
Social Worker
Others:
Have you read the “Approved Provider Activity Guidelines and Criteria”?Yes ___ Please continue to the next question. No ___ STOP! Go back and read the information in the “Approved Provider Activity Guidelines and
Criteria”. If you have questions, contact your Approved Provider Unit’s Primary Nurse Planner.
Have you read the ANCC “Content Integrity Standards”?Yes ___ Please continue to the next section. No ___ STOP! Go back and read the information in the “Content Integrity Standards.” If you have
questions, contact your Approved Provider Unit’s Primary Nurse Planner.
A. Assessment of Learner Needs
1. What needs assessment method(s) was/were used to identify the need for this activity? (Check all that apply.)
___ Written needs assessment or survey
___ Specifically requested by Registered Nurses/management
___ Quality studies/performance improvement activities
___ Evaluations from previous education activities
___ Trends in literature, law, and healthcare
___ Trends in treatments and technology
___ Other: ___________________________________________________
2. Indicate source(s) of supporting evidence for the needs assessment data. (Check all that apply.)
___ Annual survey/needs assessment ___ Literature review
___ Outcome/quality data ___ Research findings
___ Requests (phone, in-person, email) ___ Activity evaluation summary
___ Content Expert ___ Other: __________________________
___________Nurse Planner initials (required): Supporting evidence/documentation for the above selection(s) is on file and available upon request.
3. Findings of the needs assessment: Executive summary of data gathered that validates the need for this activity. Address: The “problem in practice” (difference between current state and devised state or opportunity for
improvement) How this activity will be used to evaluate the applicant’s impact on nursing professional
development and/or patient outcomes.
Form111092014 Page ___________

September, 2014
B. Description of Target Audience
Identify the Registered Nurse target audience for which this continuing nursing education activity is being designed:
____ All Registered Nurses
____ Advanced Practice Registered Nurses
____ RNs in a specialty areaIdentify specialty:
C. Purpose Statement
1. Based on the needs assessment data in Section A above, identify the appropriate gap(s) in the intended Registered Nurse target audience that this education activity will address: (Check all that apply.)____ Gap in knowledge (knows)
_ ___ Gap in skills (knows how)
____ Gap in practice (shows/does)
Describe:
2. What is the desired/achievable state (outcome) for this activity?
3. Based on the needs assessment data and the gap analysis described in #1 above, what outcome measurement(s) will the planning committee use to measure the success/impact of this activity?
4. Develop a purpose statement for this activity. The purpose is a statement of intent that reflects the justification/rationale for the activity and describes how this activity will enrich the Registered Nurse’s contributions to quality health care and his or her pursuit of professional career goals by addressing identified gaps in knowledge, skills, or practice based on the needs assessment. NOTE: Consider HOW you expect the Registered Nurse to utilize the information presented once he/she is back in their workplace. (The measureable, desired outcome). Add #1, 2 & 3 together into a complete purpose statement below.
The purpose of this education activity is to enhance the _____________________________ (identified gaps)
of the _________________________ Registered Nurse in the area of ____________________(target audience) (justification/rationale)
by addressing _________________________________________________ in an effort to(information to be covered)
___________________ as evidenced by ______________________________________.(outcome) (measurement)
Form111092014 Page ___________
Describe:
Describe:

September, 2014
D. Qualified Planners (Planning Committee)
Submit a Biographical Data Form and a Conflict of Interest Disclosure form for each member serving on the Planning Committee listed below. Minimum planning committee membership is two. Resumes and curriculum vitas are NOT accepted.
Nurse Planner: Must have a current valid RN license and baccalaureate or higher degree in nursing. The Nurse Planner guarantees that ANCC COA and TNA criteria guide the development, implementation and evaluation of this activity. (Also responsible for and must actively participate in the assessing, planning, implementation and evaluation of activity.)
Name: ____________________________________
Credentials/Degrees: _________________________
**************************************************************************************************************
***
Content Expert: (Must have documented qualifications that demonstrate education, knowledge, and expertise in the subject matter.)
Name: ____________________________________
Credentials/Degrees: _________________________**************************************************************************************************************
*******
Others Participating on the Planning Committee:
Name: ____________________________________
Credentials/Degrees: _________________________Role:______________________________________
**************************************************************************************************************
*******
Name: ____________________________________
Credentials/Degrees: _________________________Role: _____________________________________
**************************************************************************************************************
*******
Name: ____________________________________
Credentials/Degrees: _________________________Role: ______________________________________
**************************************************************************************************************
*******
Duplicate page for additional planning committee members.
___________Nurse Planner initials (required): Needs assessment data was evaluated by the Nurse Planner and other members of the planning committee and was used to validate the need for this education activity.
Form111092014 Page ___________

Rev. September 2014
Oklahoma Nurses Association6414 N. Santa Fe, Suite A
Oklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
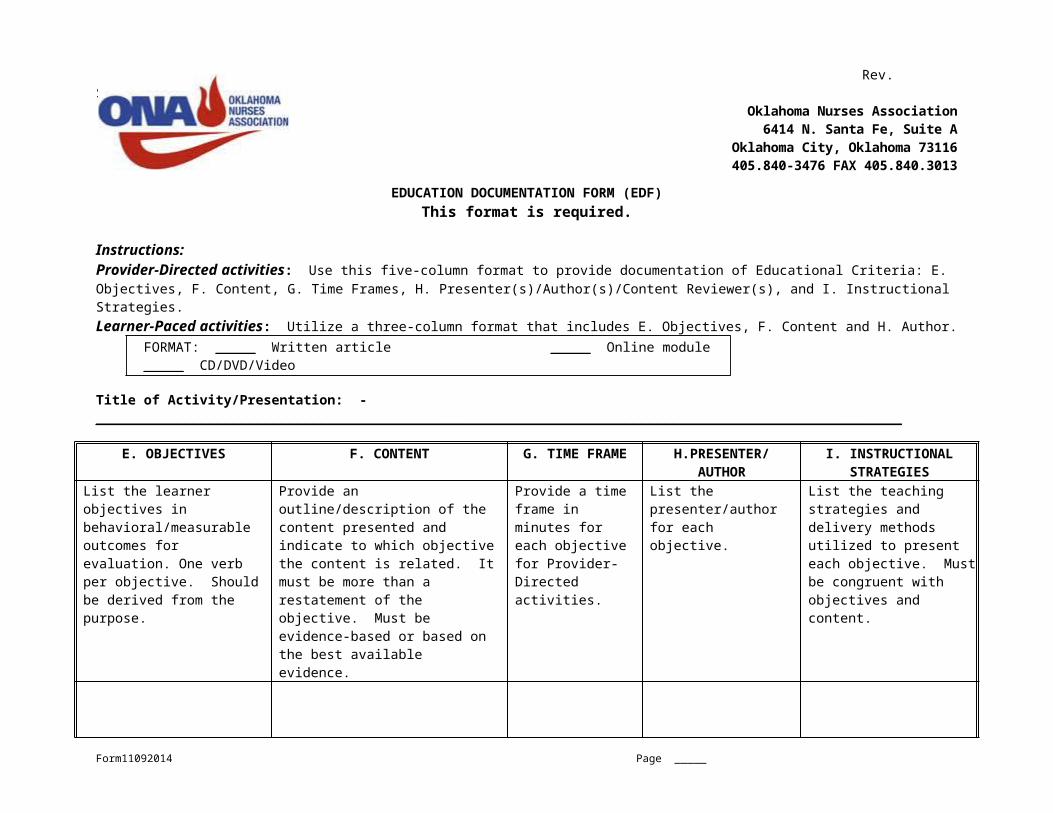
EDUCATION DOCUMENTATION FORM (EDF)This format is required.
Instructions:Provider-Directed activities: Use this five-column format to provide documentation of Educational Criteria: E. Objectives, F. Content, G. Time Frames, H. Presenter(s)/Author(s)/Content Reviewer(s), and I. Instructional Strategies. Learner-Paced activities: Utilize a three-column format that includes E. Objectives, F. Content and H. Author.
FORMAT: _____ Written article _____ Online module _____ CD/DVD/Video
Title of Activity/Presentation: _____________________________________________________________________________________________________
E. OBJECTIVES F. CONTENT G. TIME FRAME H.PRESENTER/ AUTHOR
I. INSTRUCTIONAL STRATEGIES
List the learner objectives in behavioral/measurable outcomes for evaluation. One verb per objective. Should be derived from the purpose.
Provide an outline/description of the content presented and indicate to which objective the content is related. It must be more than a restatement of the objective. Must be evidence-based or based on the best available evidence.
Provide a time frame in minutes for each objective for Provider-Directed activities.
List the presenter/author for each objective.
List the teaching strategies and delivery methods utilized to present each objective. Must be congruent with objectives and content.
Evaluation Method(s): ___ Minutes to complete evaluation method(s)___ Total minutes for this presentation
Form11092014 Page _____
I. (Continued) Reference List
When listing out references:1. Use an approved format (APA, MLA, etc).2. List starting with most recent to oldest.
Content for this education activity was chosen from:
____ Information available from the following organization/web site (organization must use current available evidence within past 5 years as resource for readers; may be published or unpublished content. EXAMPLES Agency for Healthcare Research and Quality, Center for Disease Control, National Institutes of Health):
List here:
____ Information available through peer-reviewed journal/resource (reference should be within past 5 years):
List here:
____ Clinical guidelines (EXAMPLE www.guidelines.gov):
List here:
____ Expert resource (individual, organization, educational institution) (book, article, web site):
List here:
____ Textbook reference:
List here:
____ Other:
List here:
Form11092014 Page _____

J.Presenter/Author/Content Reviewer Qualifications
Submit a Biographical Data Form and a Conflict of Interest Disclosure form for each person listed below. Resumes and curriculum vitas are NOT accepted.Name: _________________________________Credentials/Degrees: ______________________Indicate the level of participation in the planning process.Planning_____ Attended planning committee meeting
_____ Individually contacted to discuss content and objectives
_____ Developed objectives
_____ Developed content
_____ Other, please describe____________________________________________________
Name: _________________________________
Credentials/Degrees: ______________________Indicate the level of participation in the planning process.Planning_____ Attended planning committee meeting
_____ Individually contacted to discuss content and objectives
_____ Developed objectives
_____ Developed content
_____ Other, please describe____________________________________________________
Duplicate this section as needed.
1. Indicate how the needed qualification(s) of presenter(s)/author(s) are/were identified. (Check all that apply.)_X__ Content expertise____ Demonstrated comfort with teaching methodology (e.g., web-based, etc.)____ Presentation skills____ Familiarity with target audience____ Other:
Describe:
2. Indicate how the planning committee assures the qualification(s) of presenter(s)/author(s) are/were appropriate and adequate. (Check all that apply.)____ Review of biographical data form of presenter/author____ Recommendation by colleagues/credible content expert____ Review of literature written by presenter/author____ Observation of previous presentation by presenter/author____ New presenter/author being mentored by: _________________________ ____ Other:
Describe:
Form11092014 Page _____
K. Verifying Participation and Successful Completion
1. Verifying Participation
The Approved Provider maintains verification of a Registered Nurse’s participation through use of a unique identifier. Note: The BON discourages the use of the RN license number. ANCC discourages the use of the SSN as a discriminator for those with similar names. A common alternative is the use of birth month and day.
___ Sign-In Sheets ___ Signed attestation statement by participant
___ Log-in/Computer Log ___ Registration Forms
___ Other: __X_ Unique Identifier: ____________________
Describe:
A COPY OF YOUR PROPOSED VERIFICATION DOCUMENT FOR THIS ACTIVITY – WITH A PLACE FOR THE UNIQUE IDENTIFIER – MUST BE INCLUDED WITH THIS ACTIVITY TOOL.
2. Successful Completion
Criteria for successful completion should be consistent with the activity’s purpose, objectives, and instructional strategies.
A. Criteria for successful completion: (Check all that apply.)____ Attendance at entire activity.____ Attendance for at least ___% of the activity.____ Attendance at one (1) or more sessions (partial credit).__X_ Completion/submission of evaluation form.____ Achieving a passing score on a post-test.
Passing score: ________% Test/key on page(s) _________.
____ Return skill demonstration/competency assessment.____ Completion of a Learner-Paced packet/module.____ Other:
Describe:
B. Rationale for method(s) selected above to determine successful completion. (Check all that apply.)____ Method of evaluation selected____ Importance of content knowledge____ Importance of content application____ Required by employer/organization____ Other:
Describe:
L. Awarding Contact Hours
Number of contact hours to be awarded:_ ______ (Up to the 1/100th as appropriate)
1. Provider-Directed:
Presentation time plus evaluation time divided by 60 minutes equals total number of contact hours.________________ divided by 60 minutes = _____. __ __ contact hoursTotal number of minutes Do not roundfrom column G of the Education Documentation Form
2. Learner-Paced:Form11092014 Page _____

____ Pilot Study____ Historical Data____ Word Count____ Other:
Describe:
Describe the method and rationale used in determining the number of contact hours to be awarded for successful completion of this Learner-Paced activity. Contact hours must be calculated in a logical, defensible manner. Show evidence (math calculation) of how contact hours were determined.
M. Activity Evaluation
Instructions: Place a check mark or “x” next to applicable statements or phrases. (Check all that apply.)1. Describe the method(s) of evaluation to be used:
Short-Term
____ Pre and/or Post-test
__X_ Evaluation form
____ Active participation during learning activity
____ Case study/case scenario analysis
____ Direct observation of skill performance (Return demonstration – attach a copy of the tool)PAGE NUMBER _____
____ Role playing
____ Other:
Describe:
AND/ORLong-Term
____ Longitudinal study of changes in practice
____ Data collection related to quality outcome measures
____ Observation of performance in practice
____ 3-6 months post-program survey/test
____ _ Other:
Describe:
2. Describe how evaluation data will be used:
____ Make revisions to this activity
____ Make revisions to future activities
_X _ Reviewed by the planning committee members and presenter/author/content reviewer
____ Future planning of education activities
____ Other:
Describe:
Form11092014 Page _____
3. Describe how the learners will be provided feedback:
____ Questions and answers during/at conclusion of activity
____ Self-Check questions
____ Return demonstration
____ Role play
____ Discussion/dialogue during activity
____ Return results of testing
__X_ Certificate of successful completion
_____ Follow-up communication:
Describe how:
_____ Other:
Describe:
4. ___________Nurse Planner initials (required): Upon completion of the activity, a summative evaluation will be generated and kept on file for six (6) years.
5. ___________Nurse Planner initials (required): The Nurse Planner in conjunction with the planning committee will review the Summative Evaluation(s) to assess the education activity’s effectiveness and to identify how results may be used to guide future education activities.
Provider-Directed evaluations must include the following seven criteria: 1. Learner’s achievement of EACH objective.2. Expertise of EACH individual presenter.3. Relationship of objectives to overall purpose of the activity.4. Effectiveness of teaching strategies.5. Perceived bias during a presentation.6. Outcomes measurement assessment.7. Confirmation of disclosure.
Learner-Paced evaluations must include the following seven criteria: 1. Learner’s achievement of EACH objective.2. Effectiveness of teaching/learning resource(s).3. Relationship of objectives to overall purpose of the activity.4. Time required of the learner to complete the activity.5. Perceived bias during a presentation.6. Outcomes measurement assessment.7. Confirmation of disclosure.
A COPY OF YOUR ACTIVITY EVALUATION TOOL MUST BE INCLUDED WITH THIS ACTIVITY TOOL.
N. Promotional Materials
1. Type of advertising to be used: (Check all that apply. Include a copy of each with this tool.)
____ Flyer (Page #: ______) _____ Brochure (Page #: ______)____ Memo/Letter (Page #: ______) _____ Meeting Notice (Page #: ______)____ Email (Page #: ______) _____ Website (Page #: ______)____ Calendar (Page #: ______) _____ Social Media (Page #: ______)____ Save the Date (Page #: ______)
____ Other:
Form11092014 Page _____
Describe: (Page #: ______)

2. The following is the appropriate statement to use. It may not be combined with another statement. This statement MUST stand-alone.
Oklahoma Nurses Association is an approved provider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
O. Documentation of Completion
The certificate of successful completion given to the participant must include the following information:
a. Approved Provider name and address, including street, city, state, and zip code.b. Approved Provider ID Number. c. Name of participant.d. Title of the activity.e. Number of contact hours awarded.f. Day, month and year of the activity presentation, (or completion date if Learner-Paced).g. Correct TNA approval statement:
A COPY OF YOUR CERTIFICATE OF SUCCESSFUL COMPLETION MUST BE INCLUDED WITH THIS ACTIVITY TOOL WITH THE CORRECT STATEMENT.
P. Commercial Support and Sponsorship
1. Does this activity receive any commercial support/sponsorship? Yes ____ No ____
If “no”, proceed to Section Q.
If “yes”, complete the following grid and address #2 and #3 below.
Name of Organization Funding or In-Kind Donation Amount
Type of Organization (commercial interest or
sponsor)
2. Content integrity has been/will be maintained by: (Check all that apply.)
____ The commercial support/sponsorship policy/procedure has been discussed with those providing commercial support or sponsorship.
____ The commercial support/sponsorship policy/procedure has been shared in writing with those providing commercial support/sponsorship.
____ Presenters/Authors have been informed of the policy/procedure re: commercial support and sponsorship and agree to not promote the products or entity providing the financial or in-kind services.
____ In conjunction with the above, the session will be monitored and violators of the policy/ procedure will not be asked to present again.
____ Other:
Form11092014 Page _____
Oklahoma Nurses Association is an approved provider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation..
Describe:
3. The following precautions have been taken to prevent bias in the educational content: (Check all that apply.)
a.____ Our position on bias has been discussed with each presenter/author.b.____ Each presenter has agreed to present information fairly and without bias.c.____ Each presenter has agreed to not promote his/her books, services or products.d.____ The presenter(s)’s slides and handouts have been reviewed by a content expert/reviewer to
ensure lack of bias.e.____ In conjunction with a-b-c & d, the session will be monitored and violators of the policy/
procedure will not be asked to present again.f. ____ Other:
THE APPROVED PROVIDER UNIT HAS A WRITTEN POLICY/ PROCEDURE RELATED TO COMMERCIAL SUPPORT AND SPONSORSHIP THAT WAS REVIEWED WITH THOSE ENTITIES PROVIDING COMMERIAL SUPPORT AND SPONSORSHIP. ___________Nurse Planner initials: [REQUIRED IF ACTIVITY IS RECEIVING COMMERCIAL SUPPORT AND/OR SPONSORSHIP.]
IF THIS ACTIVITY RECEIVES COMMERCIAL SUPPORT OR SPONSORSHIP, A COPY OF THE SIGNED “COMMERCIAL SUPPORTER AGREEMENT” OR A “SPONSOR AGREEMENT” MUST BE INCLUDED WITH THIS TOOL. COMMERCIAL SUPPORTERS/ SPONSORS MUST BE LISTED ON THE PROMOTIONAL MATERIALS.
COMMERCIAL SUPPORT AGREEMENT(S): PAGE(S): ________________________________
SPONSORSHIP AGREEMENT(S): PAGE(S): _______________________________________
Q. Conflict of Interest Guidelines
1. Were any conflicts of interest identified? Yes ____ No ____
If “yes”, describe below how conflicts of interest were resolved.a)___ Conflict was discussed with the individual.b) ___ Revised the role of the individual with conflict of interest so that the relationship is no
longer relevant to the education activity.c)___ Review of the education activity by a content reviewer or the planning committee to
evaluate for potential bias, balance in presentation, evidence-based content or other indicators of integrity, an absence of bias, AND monitoring the education activity to evaluate for commercial bias in the presentation.
d) ___ Review of the education activity by a content reviewer or the planning committee for potential bias, balance in presentation, evidence-based content or other indicators of integrity, an absence of bias, AND reviewing participant feedback to evaluate for commercial bias in the activity.
e)___ Other
Describe:
2. In reviewing the Biographical Data Forms and Conflict of Interest Disclosure forms, did the Nurse Planner and/or planning committee suspect that there might be a conflict of interest and/or potential for bias that was not self-reported on the form? Yes ____ No ____ If “yes”, what was the concern?
What was done to resolve it?
Form11092014 Page _____
Describe:
R. Disclosures Provided to Activity Participants
Describe the METHOD (such as verbal, handout, flyer, brochure) used to notify participants at the beginning of the education activity of the following: (Multiple methods, or a single method are appropriate.) Check disclosure methods you will use.
Disclosures Promotional Material
Verbal Handout AV Slide
1. Requirements for Successful Completion
2. Absence or Presence of Conflicts of Interest
Disclosures required if applicable:
3. Commercial Support/ Sponsorship
Yes
N/A
Yes
N/A
Yes
N/A
Yes
N/A
4. Expiration Date for Awarding Contact Hours(Enduring Materials Only)
Yes
N/AFor PD activity
Yes
N/AFor PD activity
Yes
N/AFor PD activity
Yes
N/AFor PD activity
When this information is disclosed verbally at the activity, the Approved Provider must be able to supply TNA with written documentation that appropriate verbal disclosure occurred at the activity. An activity attendee must attest, in writing:
a. That disclosure did occur.
b. What information was disclosed?
A COPY OF THE DOCUMENTATION OF THE WRITTEN OR VERBAL DISCLOSURES THAT ADDRESSES ALL OF THE ABOVE COMPONENTS MUST BE INCLUDED WITH THIS TOOL.
S. Joint Providership (if applicable)
Will the activity be jointly provided? Yes _____ No _____
If yes, complete the following grid:
Name of joint providing organization(s) Joint Provider agreement Page #
Note: As the Approved Provider of this education activity, the following items are your responsibility:
Determining the educational objectives and content Selecting planners, presenters, authors and content reviewers Awarding of contact hours Recordkeeping procedures Developing evaluation methods Managing any sponsorship or commercial support Ensuring the Approved Provider is prominently displayed on all promotional materials and
certificate of successful completion.
For Learner-Paced online activities, include the following with your activity application:
Form11092014 Page _____
“Print Screen” of:
Disclosure to participants
Evaluation Tool
Certificate of Successful Completion
Form11092014 Page _____

September 2014 Oklahoma Nurses Association
6414 N. Santa Fe, Suite AOklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
ACTIVITY BIOGRAPHICAL DATA FORM FOR:Activity Title:Activity Date:
Instructions: Use this format to provide documentation of an individual’s expertise as a planning committee member or as presenter/author/content reviewer for this activity. Submitted information must not be more than 2 pages and must be typed. Do not attach any additional material.
Check which role(s) you are fulfilling:Nurse Planner Content Reviewer
Content Expert Other
Presenter/Author
Full Name:
Degrees:Credentials: (please spell out)Preferred Contact Address:Number and Street:City, State and Zip Code:Preferred Contact Telephone:E-mail Address:Present Position: (Employer, job title)
Biographical Data Use the space below to briefly describe your professional experience as it relates to your role, as indicated above, in this continuing nursing education activity. Based on the role(s) checked above, complete the appropriate following statement:
As Nurse Planner, I have education, experience or knowledge related to ANCC/TNA criteria through (check all that apply):
___ Years of experience with ANCC/TNA criteriaAttendance at a recent TNA “Individual Activity Workshop” Date attended:____ Number of CNE activities the Nurse Planner has had approvedGraduate education that included ANCC/TNA criteria as a curriculum elementReviewed FAQs and the “Approved Provider Activity Guidelines and Criteria” on the TNA websiteMentored by the Approved Provider’s Primary Nurse Planner
Additional Information:
As Content Expert, I have content expertise in this topic by:
As Presenter/Author, I have content expertise specific to this education activity by:
As Content Reviewer, I have content expertise specific to this education activity by:
Other : As ________________________, my professional experience as it relates to this continuing nursing education activity is:
Form11092014 Page _____

Form11092014 Page _____

September 2014 Oklahoma Nurses Association
6414 N. Santa Fe, Suite AOklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
CONFLICT OF INTEREST DISCLOSURE FORM
The potential for conflicts of interest exists when an individual has the ability to control or influence the content of an education activity and has a financial relationship with a commercial interest, the products or services of which are pertinent to the content of the education activity.
A commercial interest, as defined by the American Nurses Credentialing Center (ANCC) and the Texas Nurses Association (TNA), is an entity producing, marketing, reselling, or distributing healthcare goods or services consumed by or used on patients, or an entity that is owned or controlled by an entity that produces, markets, resells, or distributes healthcare goods or services consumed by or used on patients.
All individuals who have the ability to control or influence the content of an education activity must disclose all relevant relationships** with any commercial interest, including but not limited to members of the planning committee, presenters, authors, and/or content reviewers. Relevant relationships must be disclosed to the learners during the time when the relationship is in effect and for 12 months afterward. All information disclosed must be shared with the participants/learners prior to the start of the education activity.
**Relevant relationships, as defined by ANCC/TNA, are relationships with a commercial interest if the products or services of the commercial interest are related to the content of the education activity.
Relationships with any commercial interest of the individual’s spouse/partner may be relevant relationships and must be reported, evaluated, and resolved.
Evidence of a relevant relationship with a commercial interest may include but is not limited to receiving a salary, royalty, intellectual property rights, consulting fee, honoraria, ownership interest (stock and stock options, excluding diversified mutual funds), grants, contracts, or other financial benefit directly or indirectly from the commercial interest.
Financial benefits may be associated with employment, management positions, independent contractor relationships, other contractual relationships, consulting, speaking, teaching, membership on an advisory committee or review panel, board membership, and other activities from which remuneration is received or expected from the commercial interest.
As an Approved Provider of continuing nursing education by the Texas Nurses Association, it is the policy of Oklahoma Nurses Association to ensure balance, independence, objectivity and scientific rigor in all of its continuing nursing education activities. All planning committee members and presenter(s) /author(s) /content reviewer(s) participating in a Oklahoma Nurses Association activity must disclose to Oklahoma Nurses Association any financial relationships that they or an immediate family member may have with any commercial interest in any amount occurring within the past 12 months that create a conflict of interest. An “immediate family member” is defined as someone with whom you have a relationship involving the sharing of income or assets.
The intent of this disclosure is not to prevent an individual with commercial interest affiliations from participating, but rather to inform Oklahoma Nurses Association of any financial relationships so that conflicts can be resolved prior to the activity.
Form11092014 Page _____

Activity Title:Activity Date:
Name of person disclosing:«FIRST» «LAST», «DEGREE»
For all disclosures, complete each section, sign and date the last page. Please spell out all acronyms.
Is there an actual, potential or perceived conflict of interest for yourself or spouse/partner? Yes ____ No ____
If yes, complete the table below for all actual, potential or perceived conflicts of interest*:
Check all that apply Category Description
Salary/EmploymentRoyaltyStockSpeakers BureauConsultantOther
* All conflicts of interest, including potential ones, must be resolved prior to the planning, implementation, or evaluation of the continuing nursing education activity.
The signature of the individual completing this conflict of interest form attests to the accuracy of the information above.
Signature of Person Disclosing: __________________________________________Date: ______________
Procedures used to resolve conflict of interest or potential bias if applicable for this activity:
_____ Not applicable since no conflict of interest._____ Conflict was discussed with individual._____ Revised the role of the individual with conflict of interest so that the relationship is no longer relevant to
the education activity._____ Review of the education activity by a content reviewer or the planning committee to evaluate for
potential bias, balance in presentation, evidence-based content or other indicators of integrity, an absence of bias, AND monitoring the education activity to evaluate for commercial bias in the presentation.
_____ Review of the education activity by a content reviewer or the planning committee to evaluate for potential bias, balance in presentation, evidence-based content or other indicators of integrity, an absence of bias, AND reviewing participant feedback to evaluate for commercial bias in the activity.
_____ OtherDescribe:
Notes:
Signature of Nurse Planner: ______________________________________ Date: ____________________________As a member of the planning committee, I have reviewed the “Conflict of Interest Disclosure” for the Nurse Planner and verify that he/she has no relevant relationship(s) to resolve.
Notes:
Signature: ____________________________________________________ Date: ____________________________
Form11092014 Page _____

Sample Provider–Directed Evaluation Tool Format
Oklahoma Nurses AssociationTitle of Educational Activity
LocationDate
Purpose of Activity: insert purpose statement
We want to know! Please complete this evaluation tool and return your survey to the representative to receive your Certificate of Completion. Your anonymous responses will be used to revise this activity and to plan future activities.
Are you a Registered Nurse? Yes No1. Rate your achievement of the objectives listed below?
Using a scale of 1 to 5 with 1=not at all and 5=completely1 2 3 4 5
a. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
b. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
c. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
Repeat for all objectives
2. Rate the expertise/effectiveness of each individual presenter?Using a scale of 1 to 5 with 1=not at all and 5=completely
1 2 3 4 5
State Name of PresenterState Name of Presenter
Repeat for all presenters
3. Were the teaching methods/strategies effective? 1 2 3 4 54. Were the objectives relevant to the overall purpose? 1 2 3 4 55. As a result of this activity do you intend to make any changes to your practice/performance?
Please circle your answer: Yes No If no, why not? If yes, Identify changes you intend to make:
ooo
6. Were the following disclosed prior to the beginning of this activity either in writing or verbally?
Yes No
a. Requirements for Successful Completionb. Conflicts of interestc. Commercial support or Sponsorship N/A
7. Did you, as a participant notice any bias that was not previously disclosed in this presentation Yes NoIf yes, please describe who was biased and how.
Comments & Suggestions: Please use back of form for comments or suggestions.
You may ask additional questions, i.e., more information on speakers or facilities, to identify future topics, as you desire.
Form11092014 Page _____

Sample Learner–Paced Evaluation Tool Format
Oklahoma Nurses AssociationTitle of Educational Activity
Purpose of Activity: insert purpose statement
We want to know! Please complete this evaluation tool. Your anonymous responses will be used to revise this activity and to plan future activities. Circle the number that best fits your evaluation of this activity.
Are you a Registered Nurse? Yes No
1. Rate your achievement of the objectives listed below? Using a scale of 1 to 5 with 1=not at all and 5=completely
1 2 3 4 5a. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
b. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
c. OBJECTIVE AS IT APPEARS ON THE ED DESIGN FORM
Repeat for all objectives
2. How effective was the teaching/learning resource(s)? 1 2 3 4 53. Were the objectives relevant to the overall purpose? 1 2 3 4 54. How long in minutes did it take you, the learner, to complete this activity?
5. As a result of this activity do you intend to make any changes to your practice/performance?Please circle your answer: Yes No If no, why not? If yes, Identify changes you intend to make:
ooo
6. Were the following disclosed prior to the beginning of this activity either in writing?a. Requirements for Successful Completion Yes Nob. Conflicts of interest Yes Noc. Commercial support or Sponsorship N/A Yes Nod. Expiration Date
7. Did you, as a participant notice any bias that was not previously disclosed in this presentation Yes NoIf yes, please describe who was biased and how.
Comments & Suggestions:
Date Completed:
You may ask additional questions, i.e., more information to identify future topics, as you desire.
Form11092014 Page _____

CERTIFICATE OF SUCCESSFUL COMPLETION
This certifies completion of the educational activity entitled
Name of ActivityPresented on (Date/Year and Location)
For XX Contact Hours of Continuing Nursing Education
__________________________________________________________Name of Participant
Oklahoma Nurses Association is an approved provider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
Oklahoma Nurses Association6414 N. Santa Fe Ave., Suite. AOklahoma City, OK 73116www.oklahomanurses.org Provider # 11-285890-B Activity # ___________
Form11092014 Page _____

September 2014 Oklahoma Nurses Association
6414 N. Santa Fe, Suite AOklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
Commercial Support AgreementOklahoma Nurses Association is committed to presenting Continuing Education activities that promote improvements or quality in healthcare and are independent of the control of commercial interests. As part of this commitment, the Oklahoma Nurses Association has outlined in this written agreement the terms, conditions, and purposes of commercial support for its CE activities
A commercial interest, as defined by the American Nurse's Credentialing Center (ANCC) and the Texas Nurses Association (TNA), is any entity producing, marketing, reselling, or distributing healthcare goods or services consumed by or used on patients, or an entity that is owned or controlled by an entity that produces, markets, resells, or distributes healthcare goods or services consumed by or used on patients. Nonprofit or government organizations, non-healthcare-related companies, and healthcare facilities are not considered commercial interests.
Commercial support is financial or in-kind contributions given by a commercial interest that are used to pay for all or part of the costs of a CNE activity.
Note: Organizations providing commercial support may not provide or joint provide an education activity.
Title of Education Activity:Activity Location (if live): Activity Date (if live):Name of Commercial Interest Organization:Name of Approved Provider:Total amount of commercial support:
Area(s) of activity Commercial Interest organization would like to support: Unrestricted Restricted*
o Speaker honorariao Speaker expenseso Mealo Other (please list):
* Commercial interest may request that funds be used to support a specific part of an education activity. The Approved Provider may choose to accept the restriction or not accept the commercial support. The Approved Provider maintains responsibility for all decisions related to the activity as described below.
Terms and Conditions1. All organizations must comply with the ANCC Content Integrity Standards for Industry Support in Continuing Education
Activities, which is available on the TNA web page.2. This activity is for educational purposes only and will not promote any proprietary interest of a
Commercial Interest Organization providing financial or in-kind support.3. The Approved Provider is responsible for all decisions related to the education activity. The Commercial Interest
Organization providing financial or in-kind support may not participate in any component of the planning process of an education activity, including:
Assessment of learning needs Determination of objectives Selection or development of content Selection of planners, presenters, authors and/or content reviewers Selection of teaching/learning strategies Evaluation methods
Form11092014 Page _____

4. The Approved Provider will make all decisions regarding the disposition and disbursement of commercial support in accordance with ANCC/TNA criteria.
5. All commercial support associated with this activity will be given with the full knowledge and consent of the Approved Provider. No other payments shall be given to any individuals involved with the supported education activity.
6. Commercial support will be disclosed to the participants of the education activity.7. Commercial Interest Organizations may not exhibit, promote or sell products or services during the introduction of an
education activity, while the education activity takes place or at the conclusion of an education activity, regardless of the format of the education activity.
Statement of Understanding:
Signatures below of the representatives duly authorized to enter into agreements on behalf of the organizations listed indicates agreement of the terms and conditions listed in the Commercial Support Agreement above.
Approved Provider Name: Oklahoma Nurses AssociationAddress: 6414 N. Santa Fe, Suite A
Oklahoma City, Oklahoma 73116Name of Representative: Jane NelsonEmail Address: [email protected] Number: 405.840.3476Fax Number: 405.840.3013
Signature: _________________________________________________ Date: ____________________
Joint Provider Organization Name:Address:
Name of Representative:Email Address:Phone Number:Fax Number:
Signature: _________________________________________________ Date: ____________________
Commercial Interest Organization Name:Address:
Name of Representative:Email Address:Phone Number:Fax Number:
Signature: _________________________________________________ Date: ____________________
Form11092014 Page _____

September 2014 Oklahoma Nurses Association
6414 N. Santa Fe, Suite AOklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
Sponsorship Agreement
Oklahoma Nurses Association is committed to presenting Continuing Education activities that promote improvements or quality in healthcare and are independent of the control of commercial interests. As part of this commitment, the Oklahoma Nurses Association has outlined in this written agreement the terms, conditions, and purposes of sponsorship for its CE activities
Sponsorship is financial or in-kind contributions from an organization that does not fit the category of a commercial interest and that are used to pay for all or part of the costs of a CNE activity.
A commercial interest, as defined by the American Nurse's Credentialing Center (ANCC)/Texas Nurses Association (TNA), is any entity producing, marketing, reselling, or distributing healthcare goods or services consumed by or used on patients, or an entity that is owned or controlled by an entity that produces, markets, resells, or distributes healthcare goods or services consumed by or used on patients. Nonprofit or government organizations, non-healthcare-related companies, and healthcare facilities are not considered commercial interests.
Note: Organizations providing sponsorship may not provide or joint provide an education activity.
Title of Education Activity:Activity Location (if live): Activity Date (if live):Name of Sponsorship Organization:Name of Approved Provider:Total amount of sponsorship:Area(s) of activity organization providing sponsorship would like to support:
Unrestricted Restricted*
o Speaker honorariao Speaker expenseso Mealo Other (please list):
* The organization providing sponsorship may request that funds be used to support a specific part of an education activity. The Approved Provider may choose to accept the restriction or not accept the sponsorship. The Approved Provider maintains responsibility for all decisions related to the activity as described below.
Terms and Conditions1. This activity is for educational purposes only and will not promote any proprietary interest of an organization
providing sponsorship.2. The Approved Provider is responsible for all decisions related to the education activity. The sponsorship organization
may not participate in any component of the planning process of an education activity, including: Assessment of learning needs Determination of objectives Selection or development of content Selection of planners, presenters, authors and/or content reviewers Selection of teaching/learning strategies Evaluation methods
3. The Approved Provider will make all decisions regarding the disposition and disbursement of sponsorship in accordance with ANCC/TNA criteria.
Form11092014 Page _____

4. All sponsorship associated with this activity will be given with the full knowledge and consent of the Approved Provider. No other payments shall be given to any individuals involved with the supported education activity.
5. Sponsorship will be disclosed to the participants of the education activity.6. The sponsorship organization may not exhibit, promote or sell products or services during the introduction of an
education activity, while the education activity takes place or at the conclusion of an education activity, regardless of the format of the education activity.
Statement of Understanding:
Signatures below of the representatives duly authorized to enter into agreements on behalf of the organizations listed indicates agreement of the terms and conditions listed in the Sponsorship Agreement above.
Approved Provider Name: Oklahoma Nurses AssociationAddress: 6414 N. Santa Fe, Suite A
Oklahoma City, Oklahoma 73116Name of Representative: Jane NelsonEmail Address: [email protected] Number: 405.840.3476Fax Number: 405.840.3013
Signature: _________________________________________________ Date: ____________________
Joint Provider Organization Name:Address:
Name of Representative:Email Address:Phone Number:Fax Number:
Signature: _________________________________________________ Date: ____________________
Sponsorship Organization Name:Address:
Name of Representative:Email Address:Phone Number:Fax Number:
Signature: _________________________________________________ Date: ____________________
Form11092014 Page _____

Oklahoma Nurses Association
Disclosure to Participants Sample Tool Format
Approval Statement:Oklahoma Nurses Association is an approved provider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
(Title of education activity)
Requirements for Successful Completion:
The purpose of this education activity is:
AND/OR
The objectives of this education activity are: (add as many lines as necessary)
1.
2.
3.
4.
To receive contact hours for this continuing education activity, the participant must:
Once successful completion has been verified, a “Certificate of Successful Completion” will be awarded for __________ contact hours.
Conflicts of Interest:
Explanation: A conflict of interest occurs when an individual has an opportunity to affect or impact educational content with which he or she may have a commercial interest or a potentially biasing relationship of a financial nature. All planners and presenters/authors/content reviewers must disclose the presence or absence of a conflict of interest relative to this activity. All potential conflicts are resolved prior to the planning, implementation, or evaluation of the continuing nursing education activity. All activity planning committee members and presenters/authors/content reviewers have submitted Conflict of Interest Disclosure forms.
[The planning committee members and presenters/authors/content reviewers of this CNE activity have disclosed no relevant financial relationships related to the planning or implementation of this CNE activity.]
OR[The planning committee members and presenters/authors/content reviewers of this CNE activity have disclosed the following relevant financial relationships related to the planning or implementation of this CNE activity.]
__________________________________ ________________________________(Person’s name) (Name of Commercial Interest)_______________________________________________________________________(Nature of relationship)
__________________________________ ________________________________(Person’s name) (Name of Commercial Interest)_______________________________________________________________________(Nature of relationship)
Form11092014 Page _____
Disclosures required if applicable:
Commercial Support or Sponsorship:This CNE activity has received the following commercial support and/or sponsorship(s):
_____________________________ _______________________________(Company) (Type of Support)
_____________________________ _______________________________(Company) (Type of Support)
Expiration Date for Awarding Contact Hours: (Include only if this education activity is a learner-paced activity). This activity expires _________________________________.
Reporting of Perceived Bias:Bias is defined by the American Nurses Credentialing Center’s Commission on Accreditation (ANCC COA) as preferential influence that causes a distortion of opinion or of facts. Commercial bias may occur when a CNE activity promotes one or more product(s) (drugs, devices, services, software, hardware, etc.). This definition is not all inclusive and participants may use their own interpretation in deciding if a presentation is biased.
The ANCC COA is interested in the opinions and perceptions of participants at approved CNE activities, especially in the presence of actual or perceived bias in continuing education. Therefore, ANCC invites participants to access their “ANCC Accreditation Feedback Line” to report any noted bias or conflict of interest in the education activity. The toll free number is 1(866) 262-9730.
Attestation:If any or all of the above information was disclosed verbally to participants, the Approved Provider must attest that the disclosure did occur. This section may be removed if the document is being used as a handout to participants.
I, ____________________________, attest that the above information was disclosed to the continuing nursing education activity participants.
______________________________________________ ___________________Signature – Activity Attendee Date
Form11092014 Page _____
September 2014 Oklahoma Nurses Association
6414 N. Santa Fe, Suite AOklahoma City, Oklahoma 73116405.840-3476 FAX 405.840.3013
AGREEMENT FOR JOINT PROVIDING A CONTINUING NURSING EDUCATION ACTIVITY
This education activity is being jointly provided by Oklahoma Nurses Association and (Name of Joint Provider).
Title of Activity:
Date(s) if live presentation:
Date to begin if enduring material:
Total number of contact hours:
Approved Provider Nurse Planner’s Name: Patti Muller-Smith, BSN, MA, Ed.D, RN
Each item must be checked to reflect the appropriate responsibility. Items indicated as “Required” are the responsibility of the Approved Provider and are not negotiable. Joint providing an education activity is a collaborative venture that requires the direct involvement of the Primary Nurse Planner and the Nurse Planner. The Oklahoma Nurses Association and (Name of Joint-Provider) will both agree on the selection of topics and speakers for jointly offered CE programs.
Responsibilities Approved Provider (Joint Provider Name)
Determining educational objectives and content Required
Selecting planners, presenters, authors and/or content reviewers
Required
Determining appropriate number and awarding of contact hours
Required
Recordkeeping procedures Required
Developing evaluation methods Required
Managing any commercial support or sponsorship Required
Ensuring the Approved Provider is prominently displayed on all promotional materials and certificates of successful completion.
Required
Other items (suggestions only): These items listed below are typically the responsibility of the joint provider if they are required for the activity
Publicity/Marketing
Activity planning and implementation
Printing:
Registration:
Supplies: (list)
Physical location:
AV Supplies:
Food:
Other:
Form11092014 Page _____
FINANCIAL AGREEMENT
The Oklahoma Nurses Association and (Name of Joint-Provider) agree that ONA will provide this service to the (Name of Joint-Provider) for an administrative fee of $150 for up to 8 contact hours. Contact Hours may not be purchased.
Oklahoma Nurses Association is an approved provider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
Approved Provider Representative:
_________________________________________________________________________Signature of representative:
Jane Nelson, CAEExecutive DirectorOklahoma Nurses Association6414 N. Santa Fe, Suite AOklahoma City, OK [email protected]
Joint Provider Representative:
_________________________________________________________________________Typed name and official title:
_________________________________________________________________________Signature of representative:
_________________________________________________________________________Name of Co-Provider Organization/Agency:
_________________________________________________________________________Street Address: City: State Zip Code
_________________________________________________________________________Phone: Email address:
Form11092014 Page _____