sdacep march 6, 2015 abigail polzin, md sanford usd medical center emergency medicine
TRANSCRIPT

Delayed Sequence IntubationSDACEPMarch 6, 2015Abigail Polzin, MDSanford USD Medical CenterEmergency Medicine

Objectives
• Define Delayed Sequence Intubation• Discuss the Published Literature• Case Review and Video Review of DSI• Applications in Community EDs
Delayed Sequence Intubation
• Hot Topic in EM• Scott Weingart of EM Crit

Emergency Medicine
• Expertise in airway management•RSI•Difficult Airways
• Expertise in Sedation•Local Anesthesia•Anxiolysis•Procedural Sedation

Rapid Sequence Intubation• Combined administration of sedative and paralytic
for rapid endotracheal intubation.• On room air patients will have 45-60 seconds
before desaturation. • Studies as far back as the 1960’s found that
providing pre-oxygenation with high FiO2 can increase this time.
• Preoxygenation is recommended for every ED intubation.
Preoxygenation• Non-rebreather set at 15L/min + (+/- nasal
cannula in addition)• 8 Vital Capacity Breaths or 3 minutes of pre-
oxygenation• Goal is oxygenation of 100%• Adding positive pressure (BiPAP, CPAP, PEEP
Valves) can increase oxygenation and decrease desaturations during intubation.
Weingart, Preoxygenation and Prevention of Desaturation…
Preoxygenation• Co-Morbidities that can impact preoxygenation• Obesity• CHF• COPD• Anemia• Volume Depletion• Increased Metabolic Demand (trauma, sepsis, agitation,
AMS)
• Impossible to predict the amount of time before desaturation, especially in our ED patient population.

So…… What if you
can’t preoxygenate
?

Delayed Sequence Intubation
“A procedural sedation, where the
procedure is pre-oxygenation”

The Data


Patient
• A patient requiring emergent intubation but resistant to pre-intubation preparations because of altered mental status.
Dissociation
• Administer a dissociative dose of Ketamine by slow IV-Push; administer additional doses as needed.
Preoxygenat
e
• Use NRB Mask + Nasal Cannula. If Sats <95% use NIPPV.
Paralyze
• Administer Succinylcholine or Rocuronium.
Apneic Oxygenation
• Perform apneic oxygenation with nasal cannula.
Intubate
• Use difficult airway techniques as indicated

Patient
• A patient requiring emergent intubation but resistant to pre-intubation preparations because of altered mental status.
• Good lungs but agitated/altered• Trauma patient• Ingestions• Sepsis
• Bad lungs• COPD• CHF• Pulmonary Edema
• Bad lungs AND agitated/altered

Dissociation
• Administer a dissociative dose of Ketamine by slow IV-Push; administer additional doses as needed.
• Why is ketamine ideal for this?• Keeps the patient breathing• Keeps airway reflexes intact
• 1 mg/kg (less than our typical dose for procedural sedation)
• Repeat as needed (0.5 mg/kg) until dissociation achieved
• Other medications?• Propofol, Etomidate, Dexmetatomodine, Droperidol

Ketamine
• Classified as a dissociative anesthetic that has potent analgesic and sedative effects• Unlike most sedative agents – a typical dose
response curve is not observed (once dissociated, giving larger doses likely won’t increase level of sedation)
• Can be given via the IV or IM route• IV - onset ~30 seconds• IM - onset ~3-4 minutes

Ketamine• Complications/side effects
• Respiratory depression when given via RAPID push • Emergence reactions• Post sedation emesis• Excessive salivary secretions• Laryngospasm • Arrythmias
• Contraindications• Allergy to ketamine• Elevated ICP or TBI patients (historical contraindication)• January 2015 Annals of Emergency Medicine• “According to the available literature, the use of ketamine in
critically ill patients does not appear to adversely affect patient outcomes.”
• Cautions• Severe coronary artery disease

Preoxygenatio
n
• Use NRB Mask + Nasal Cannula. If Sats <95% use NIPPV.
• Now patient will be able to tolerate mask, nasal cannula.• DSI ≠ NIPPV for preoxygenation

Paralyze
• Administer Rocuronium or Succynilcholine
Apneic Oxygenation
• Passive oxygenation following paralysis with nasal cannula
Intubation
• Using difficult airway resources as needed

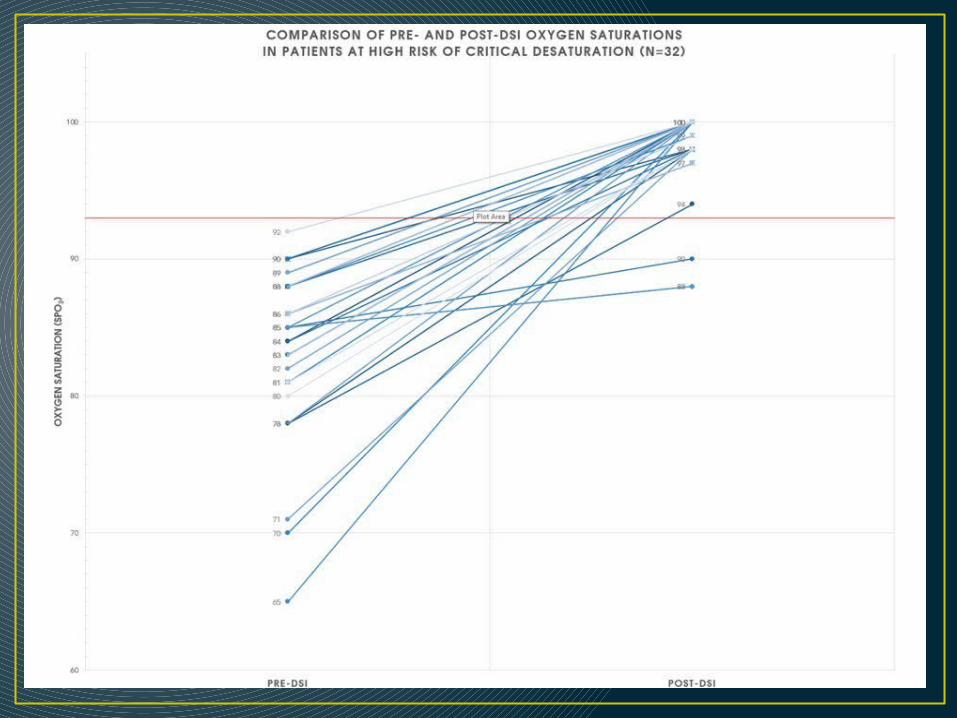
Annals of Emergency Medicine• 62 Patients• “Self controlled”• Primary outcome – best saturation without DSI compared
to post-DSI SpO2.
• PNA, Asthma, Pulmonary Edema• Oxygenation Failure• Ventilatory Failure• Airway Protection

EligibleN=64
Patients
Received DSIN= 62
Patients
NRB Preoxygenat
ion N=23 Patients
IntubatedN=23
Patients
NIPPV Preoxygenat
ion N=39 Patients
IntubatedN=37
Patients
Admitted on NIPPV
N=2 Patients
Excluded2 Patients (could not
record post-DSI SpO2)

Reason for DSI
•31% couldn’t tolerate NRB•60% couldn’t tolerate NIPPV

Limitations
• Not RCT• Selection bias• Missed patients• Small study

Intubation• In the study, 2 patients had such improvement in
oxygenation and air movement that they did not require intubation following ketamine administration.
Case• 44 y/o F with PMH Fibromyalgia, Obesity, presented
to OSH on 2/3/15 with cough, pharyngitis. No PMH other than +tobacco/marijuana use. Started on Z-pack, discharged home.
• Returned to OSH on 2/4/15 in AM. CXR was obtained, worsening respiratory complaints, pleuritic R side chest pain. Admitted and started on antibiotics. +Blood cultures with gram+ cocci in chains.
• 17:15 called to arrange transfer. Has had worsening respiratory distress for >2 hours. O2 sats in 80’s on NRB.
• Advised to start BiPAP – pt was unable to tolerate. Transported by ground EMS.

CXR

Case
• Vital Signs 20:25• 124/53• HR 105• T 97.3• 83% on 15L
• Pt arrived in ED.• Agitated, leaning
forward, diaphoretic, NRB on.
• Able to speak 1-2 words.
• Still awake but altered.

Physical Exam• Constitutional:
Obese, diaphoretic, severe distress • HENT: • Head: Normocephalic and atraumatic.
Mallampati 4• Eyes: EOM are normal. Pupils are equal, round,
and reactive to light. • Neck: Normal range of motion. • Cardiovascular:
Tachycardic with 2+ peripheral pulses. No significant edema.
• Pulmonary/Chest: Patient in severe respiratory distress. She has increased work of breathing.
She has diffuse inspiratory rales in all lung fields and overall diminished.
• Abdominal: Soft. Bowel sounds are normal. She exhibits no distension. There is no tenderness. Neurological:
Waxing and waning alertness.Moving all extremities
• Skin: No rash noted. Diaphoretic

Case• How long will you have to RSI her before she
desats?• Will she be an easy or a difficult airway?• Even with video laryngoscopy this airway is likely
to be difficult, and 1 attempt taking longer than 15 seconds is likely to result in hypoxia.
• You are starting behind the 8 Ball.

Case• Patient weight = 124 kg (estimated at the time)• 100 mg Ketamine given• BiPAP placed for 10 minutes – O2 sats improved to
100%.• Pt did require repeat Ketamine to total of 200 mg.• Following this further sedation with etomidate (pt
was waking) and paralysis with succinylcholine.• Intubation took 1 attempt and 15 seconds.
Hypoxia to 73%.• Positive pressure ventilation slowly improved
oxygenation to 90%.

VIDEO
Case
• Hospital Course• Intubated until 2/13/15•Required PS 23, prone positioning, low tidal volumes•Antibiotics course•AKI requiring dialysis•Severe deconditioning and generalized weakness•Anticipated discharge to a skilled nursing facility

Delayed Sequence Intubation• What if DSI hadn’t been performed?• Oxygen-Hemoglobin dissociation curve• Anticipate even worse hypoxia and inability to ventilate
• Where’s the data?
Preoxygenation, Reoxygenation, and Delayed Sequence Intubation in the ED
Applications• “I’ve tried BiPAP but I’m claustrophobic”• The 95 year old DNR with pneumonia• Agitated trauma patients• Smaller facilities where intubation is not always
available/comfortable• Pre-hospital care?

Summary• Delayed sequence intubation is a viable
alternative to RSI in patients who are not able to pre-oxygenate well.
• It is a utilization of 2 key skills in Emergency Medicine (airway management and conscious sedation)
• Currently there is a small amount of published data available.
Special Thanks• Husband and Colleagues• Sanford USD Medical Center• Joel VanHuekelom, Pharm D• Misty Brendan• Patient from the case for giving her consent that
her story and video be shared for learning purposes

Questions & Comments
References• Weingart, Scott. "Preoxygenation, Reoxygenation, and Delayed Sequence
Intubation in the Emergency Department." The Journal of Emergency Medicine 40.6 (2010): 661-67. Print.
• Weingart, Scott, and Richard Levitan. "Preoxygenation and Prevention of Desaturation During Emergency Airway Management." Annals of Emergency Medicine 59.3 (2012): 165-75. Print.
• Weingart, Scott, and Seth Trueger. “Delayed Sequence Intubation: A Prospective Observational Study.” Annals of Emergency Medicine October 22, 2014. Online.
• Baillard, Cristophe. “Noninvasive Ventilation Improves Preoxygenation before Intubation of Hypoxic Patients.”American Journal of Respiratory and Critical Care Medicine 174 (2006): 171-177. Print.
• Weingart, Scott, and Darren Braude. "Airway Corner - Delayed Sequence Intubation." Interview. Audio blog post. EM:RAP. N.p., June 2014. Web. 4 Feb. 2015. <www.emrap.org>.
• Cohen, Lindsay. “The Effect of Ketamine on Intracranial and Cerebral Perfusion Pressure and Health Outcomes: A Systematic Review.” Annals of Emergency Medicine 65.1(2015): 43-51. Print.
• “Podcast UPDATE on Delayed Sequence Intubation (DSI).” EMCrit. N.p., 17 Nov. 2014. Web. 01 Mar. 2015.