screening for subclinical thyroid dysfunction in non-pregnant
TRANSCRIPT
Hyperthyroidism and hypothyroidism arecommon conditions that have lifelong effects onhealth.1,2 About 5% of U.S. adults report havingthyroid disease or taking thyroid medication.1,2
Consequences of untreated hyperthyroidisminclude atrial fibrillation, congestive heart failure,osteoporosis, and neuropsychiatric disorders.Hypothyroidism causes symptoms that reducefunctional status and quality of life.3
Subclinical thyroid dysfunction, which canbe diagnosed by thyroid function tests beforesymptoms and complications occur, is viewedas a risk factor for developing hyperthyroidismand hypothyroidism complications. The goalof screening is to identify and treat patientswith subclinical thyroid dysfunction beforethey develop these complications.4–6
The term subclinical hyperthyroidism describesconditions characterized by a low thyroid-stimulatinghormone (TSH) and normal levels of circulatingthyroid hormones (thyroxine and triiodothyronine).Subclinical hyperthyroidism has the same causes asovert hyperthyroidism. These include excessive doses
of levothyroxine, Graves’ disease, multinodulargoiter, and solitary thyroid nodule. Most studies ofthe course of subclinical hyperthyroidism concernpatients whose history, physical examination,ultrasound, or thyroid scan suggests one of thesecauses. There are relatively few studies of patientswho are found by screening to have an undetectableTSH, normal free thyroxine (FT4) and normal freetriiodothyronine (FT3) levels, and a negativethyroid evaluation, the largest group identified in ascreening program. The prevalence of subclinicalhyperthyroidism is about 1% (95% confidenceinterval [CI], 0.4%–1.7%) in men older than 60 and1.5% (CI, 0.8%–2.5%) in women older than 60.7
The terms subclinical hypothyroidism and mildthyroid failure refer to patients who have an elevatedTSH and a normal FT4 level (Table 1).6 Subclinicalhypothyroidism is common, especially in olderwomen.1,2,7–16 In an analysis of the Third NationalHealth and Nutrition Examination Survey(NHANES-III), a population-based survey of17,353 people aged 12 or older representing theU.S. population, the prevalence of subclinical
Screening for Subclinical ThyroidDysfunction in Non-Pregnant Adults:A Summary of the Evidence for theU.S. Preventive Services Task Force
Mark Helfand, MD, MPH
1
From the Oregon Health & Science University, Evidence-based Practice Center, Portland, Oregon.
The author of this article is responsible for its contents, including any clinical or treatment recommendations. No statementin this article should be construed as an official position of the U.S. Agency for Healthcare Research and Quality or theU.S. Department of Health and Human Services.
Address correspondence to Mark Helfand, MD, MPH, Oregon Health & Science University, Evidence-based Practice Center,Portland, OR 97239.
Reprints are available from the AHRQ Web site (www.preventiveservices.ahrq.gov) and through the National GuidelineClearinghouse™ (www. guideline.gov). Print copies of this article, along with other USPSTF evidence summaries andRecommendations and Rationale statements, are available by subscription to the Guide to Clinical Preventive Services, ThirdEdition, Periodic Updates. The cost of this subscription is $60 and is available through the AHRQ Publications Clearinghouse(call 1-800-358-9295 or e-mail [email protected]).
Reprinted with permission from Medicare Coverage of Routine Screening for Thyroid Dysfunction (2003) by the National Academyof Sciences, courtesy of the National Academies Press, Washington, D.C. Appendix B, 75–113, and published in Ann InternMed. 2004;140:128–141.
2
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
hypothyroidism was 5.8% among white,non-Hispanic females, 1.2% among black,non-Hispanic females, and 5.3% amongMexican-American females.1 The prevalence ofsubclinical hypothyroidism was 3.4% among whitemen, 1.8% among black men, and 2.4% amongMexican American men. In the Whickham survey,a large, good-quality, population-based study with20-year follow-up, prevalence was 4% to 5%among women aged 18 to 44, 8% to 10% amongwomen aged 45 to 74, and 17.4% among womenolder than age 75.17 The prevalence was 1% to 3%among men aged 18 to 65 and 6.2% among menover age 65.
In this paper, I address whether the primary carephysician should screen for thyroid function inpatients seen in general medical practice who haveno specific indication for thyroid testing and whocome to the physician for other reasons. I focus onwhether screening should be aimed at detection ofsubclinical thyroid dysfunction and whetherindividuals who have mildly abnormal TSH valuescan benefit.
Methods In consultation with members of the U.S.
Preventive Services Task Force (USPSTF) andan Institute of Medicine expert panel, I definedthe population, interventions, and outcomes ofinterest and developed key questions to guide theliterature review.18 The population of interest wasasymptomatic, non-pregnant adults who do not
have a goiter, nodule, proptosis, tremor, profoundphysical tiredness, or a past history of thyroiddisease.19 I also included elderly patients whocomplained of 1 or 2 nonspecific or mildsymptoms, such as cold intolerance, fatigue,weight gain, or constipation, because they areno more likely to have abnormal thyroid functiontests than those who have no complaints.20
Previous systematic reviews have established thatsubclinical thyroid function is common and can bediagnosed easily using a TSH test.7,8,21 In this article,I focus on the following questions:
1. What are the complications of subclinical thyroiddysfunction?
2. What are the benefits of earlier treatment ofsubclinical hypothyroidism and hyperthyroidism?
3. What are the adverse effects of treatment?
To find articles published before 1998, I searchedthe reference lists of previous reviews6,8,9,21–29 and ourown files of over 1,600 full-text articles from 1910to 1998.1 I then searched MEDLINE® andEMBASE from 1996 to February 2002,PreMEDLINE in March 2002, and the CochraneLibrary (2002, Issue 2) to identify recent articlesrelevant to each question.
For question 1, I searched for studies of thecausal relationship between subclinical thyroiddysfunction and any potential complication. Iincluded studies if they were conducted in thegeneral adult population, a demographic segment ofthe adult population, or among patients seen in the
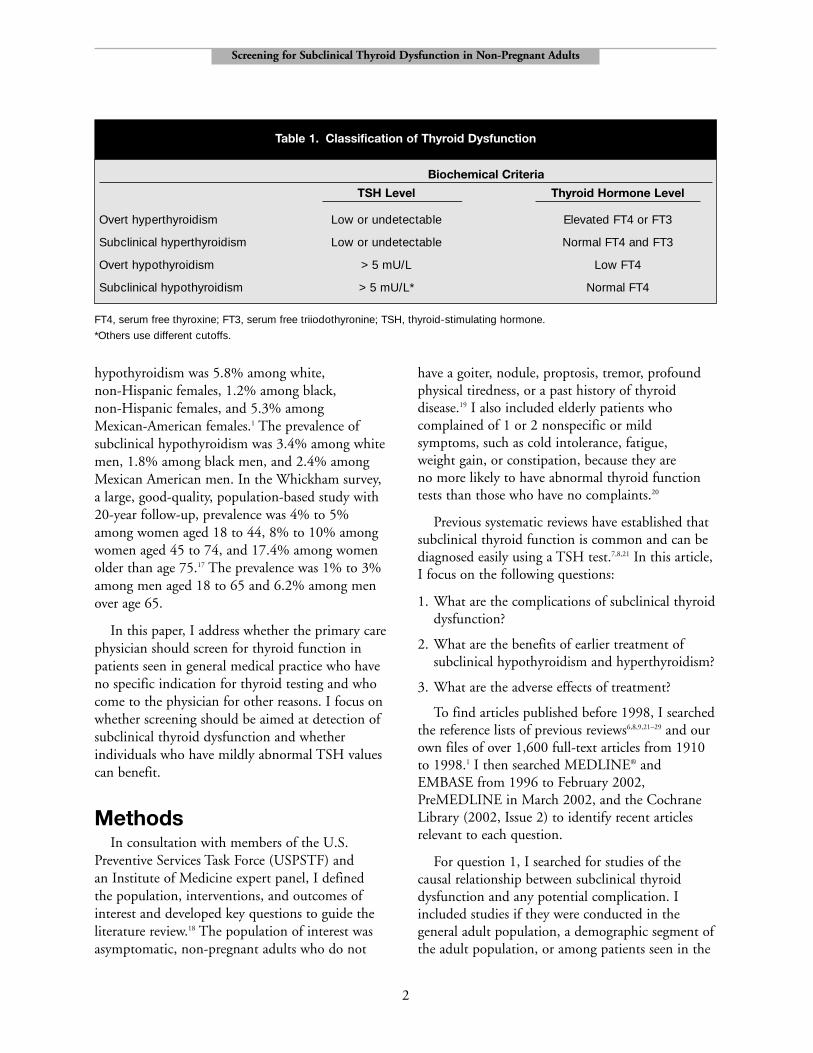
FT4, serum free thyroxine; FT3, serum free triiodothyronine; TSH, thyroid-stimulating hormone.
*Others use different cutoffs.
Biochemical Criteria
TSH Level Thyroid Hormone Level
Overt hyperthyroidism Low or undetectable Elevated FT4 or FT3
Subclinical hyperthyroidism Low or undetectable Normal FT4 and FT3
Overt hypothyroidism > 5 mU/L Low FT4
Subclinical hypothyroidism > 5 mU/L* Normal FT4
Table 1. Classification of Thyroid Dysfunction

3
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
general clinic setting. I excluded studies of screeningfor congenital or familial thyroid disorders andstudies of screening in pregnant women, inpatients,institutionalized patients, and series of patients seenin specialized referral clinics for depression or obesity.
To examine the benefits and harms of treatment(questions 2 and 3), I included any controlled trialof oral levothyroxine or triiodothyronine that usedTSH levels as a criterion for entry, in any population,including patients with known thyroid disease. Ialso included recent observational (pre/post treatmentand time series) studies that had not been includedin previous meta-analyses.7,9,21,30
I reviewed abstracts and articles to identifystudies that met the eligibility criteria and abstractedinformation about the setting, patients, interventions,and outcomes of each included trial using a standardtemplate. I used predefined criteria from the USPSTFto assess the internal validity of included studies18 andrated the applicability of each study to screening.
This article is based on a larger evidence report thatwas funded by the Agency for Healthcare Researchand Quality (AHRQ) and the Institute of Medicine(available at http://www.preventiveservices.ahrq.gov).Staff of both funding agencies, members of theUSPSTF, and members of an Institute of Medicineexpert panel reviewed the draft of the larger reportand made editing suggestions.
Results
Subclinical HyperthyroidismAdvocates of screening for subclinical
hyperthyroidism argue that early treatment mightprevent the later development of atrial fibrillation,osteoporotic fractures, and complicated overthyperthyroidism. Other potential benefits are earliertreatment of neuropsychiatric symptoms andprevention of the long-term consequences ofexposure of the heart muscle to excessive stimulationfrom thyroid hormones.
Evidence regarding potentialcomplications
Atrial fibrillation. A good-quality cohort study inthe Framingham population found that, in patientsolder than 60 who did not take levothyroxine andhad a serum TSH level of 0.1 mU/L or less, the riskof atrial fibrillation was 32% (CI, 14%–71%) over10 years.31 The risk for patients who had a normalTSH level was 8%. A more recent cross-sectionalstudy of atrial fibrillation in overt and subclinicalhyperthyroidism had serious flaws and was rated asbeing of poor quality.32 The clinical consequencesof atrial fibrillation in patients who have a low TSHhave not been studied. In general, chronic atrialfibrillation is associated with stroke and othercomplications and with a higher risk for death.33
Mortality. A population-based, 10-year cohortstudy of 1,191 people aged 60 or older found ahigher mortality rate among patients who had a lowTSH initially.34 The excess mortality was dueprimarily to cardiovascular diseases. In this study, therecruitment strategy and the statistical adjustmentfor potential confounders were inadequate; patientswho had a low TSH may have had a higherprevalence of other illnesses, but adjustment wasdone only for age and sex, not for comorbidity.Comorbidity adjustment would be critical becauseacutely ill and chronically ill elderly patients oftenhave falsely low TSH levels, presumably because oftheir illness.35 Thus, while it is possible that patientswho had a low initial TSH had higher mortalitybecause of their thyroid disease, it is also possiblethat patients who were ill to begin with had a lowTSH as a result of their illness.
Osteoporosis and fracture. Most data about the riskfor osteoporosis and fracture come from women whotake thyroid hormones rather than from untreatedwomen found by screening to have a low TSH. Twometa-analyses of older studies36,37 suggest that womenwho have a low TSH because they take thyroidhormones are at higher risk for developingosteoporosis. However, a good-quality study from theStudy of Osteoporotic Fractures (SOF) cohort foundsimilar bone loss among women with undetectable,low, and normal TSH levels, but markers of boneturnover were higher in women with a low TSH.38
In a more recent nested sample of cases and controls
from SOF, the risk for hip fracture among womenwho had an undetectable TSH was elevated, but ofborderline statistical significance (adjusted hazardratio, 3.6; CI, 1.0–12.9).39 The risk for vertebralfracture among women who had an undetectableTSH was significantly elevated when compared with235 controls (odds ratio [OR], 4.5; CI, 1.3–15.6).Among women who had a borderline low serumTSH (0.1–0.5 mU/L), the risk for vertebral fracture(OR, 2.8; CI, 1.0–8.5), but not hip fracture, waselevated.
This analysis has limited relevance to screeningbecause the investigators were not able to obtainserum FT4 or FT3 tests, which could havedistinguished between overt and subclinicalhyperthyroidism. Also, among the 148 women withhip fractures, 22 had an undetectable serum TSH(< 0.1 mU/L), and of these, approximately 19 (86%) were taking thyroid hormones when theirinitial TSH measurement was obtained. Bauer andcolleagues stated that “thyroid hormone use was notassociated with increased risk for ... fracture,” butthere were not enough women with undetectableTSH levels not taking thyroid hormone to make a valid comparison.39 Finally, at baseline, the hipfracture cases were significantly older, weighed less, had lower bone density, were less healthy byself-report, and were twice as likely to have ahistory of hyperthyroidism than controls. Theanalysis could not exclude the possibility that some of the women with low TSH levels had several interacting risk factors and that other factorsconcomitant with age or socioeconomic status couldhave been confounders.
Other studies of the risk for osteoporosis amongpatients not taking levothyroxine concern smallnumbers of patients with nodular thyroid diseaseor Graves’ disease40–43 rather than patients who haveno obvious clinical signs of thyroid disease.
Complicated thyrotoxicosis and progression toovert hyperthyroidism. Overt thyrotoxicosis canbe complicated by severe cardiovascular orneuropsychiatric manifestations requiringhospitalization and urgent treatment. There areno data linking subclinical hyperthyroidism tothe later development of complicated thyrotoxicosis.
Such a link is unlikely to be made because1) complicated thyrotoxicosis is rare, 2) one-halfof cases occur in patients with knownhyperthyroidism, and 3) complications areassociated with social factors, including insurancestatus, that may also affect access to screening andfollow-up services.44
Progression from subclinical to overthyperthyroidism is well documented in patientswith known thyroid disease (goiter or nodule), butnot in patients found by screening to have a lowTSH and no thyroid signs. Based on the sparse datafrom screening studies, a previous meta-analysisestimated that each year, 1.5% of women and 0% ofmen who have a low TSH and normal FT4 andFT3 levels develop an elevated FT4 or FT3.7,45,46
Symptoms and cardiac effects. In the setting ofnodular thyroid disease, Graves’ disease, orlong-term use of suppressive doses of levothyroxine,subclinical hyperthyroidism has been associated withcognitive abnormalities, abnormalities in cardiaccontractility, and exercise intolerance.47–52 However,the frequency of symptoms or myocardialcontractility abnormalities in patients who havesubclinical hyperthyroidism found by screening hasnot been studied; no study has linked abnormalitiesin cardiac contractility or output to thedevelopment of clinically important heart disease.
Efficacy of Treatment forSubclinical Hyperthyroidism
No controlled trials of treatment for subclinicalhyperthyroidism have been done. Smallobservational studies in patients with nodularthyroid disease not detected by screening haveshown improvements in bone metabolism andhemodynamic measures after treatment.53–56
Subclinical Hypothyroidism
Evidence regarding potentialcomplications
Progression to overt hypothyroidism. There is goodevidence from well-conducted longitudinal studiesthat subclinical hypothyroidism is a strong risk factor
4
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults

for the later development of overt hypothyroidism.In addition to the TSH level, older age, antithyroidantibodies, and female sex are also strong risk factors.In the Whickham survey, for a 50-year-old womanwho has a serum TSH level of 6 mU/L and positiveantithyroid antibodies, the risk for developing overthypothyroidism over 20 years was 57%; for a50-year-old woman with a serum TSH level of 9mU/L, the risk was 71%.57 A 50-year-old womanwho had a normal TSH and negative antibody testhad a risk of only 4% over 20 years. The risk forprogression was not evenly distributed throughoutthe follow-up period. Nearly all women whodeveloped hypothyroidism within 5 years had aninitial serum TSH greater than 10 mU/L.
Symptoms, mood, and quality of life. In its 1998review and guideline, the American College ofPhysicians concluded that, in the generalpopulation, it was not clear that the prevalenceand severity of symptoms and the quality of lifediffers for individuals who have mildly elevatedTSH levels compared with those who do not.7,20,58
Since then, 2 cross-sectional studies in volunteershave addressed this question, with mixed results.An interview survey of 825 Medicare enrollees in New Mexico found no differences in theage-adjusted frequency of self-reported symptomsbetween participants with serum TSH elevationsfrom 4.7 to 10 mU/L and those with normalTSH concentrations.14 A larger survey fromColorado (n = 25,862) is less pertinent because it included patients who took levothyroxine inthe analysis of symptoms. It also found nodifference between euthyroid patients and thosewith subclinical hypothyroidism in currentsymptoms, but found a higher percentage of“changed symptoms” in the subclinicalhypothyroid group (13.4% vs 15.4%).2
Patients who have subclinical hypothyroidism, aTSH >10 mU/L, and a history of antithyroidtreatment for Graves’ disease or nodular thyroiddisease have a higher prevalence of symptoms thanhealthy controls.22,59 This observation is probablyvalid, but an important limitation of the evidenceshould be noted: the appropriate comparisongroup is not healthy volunteers, but patients whohave a normal TSH and a history of antithyroid
treatment. This is because euthyroid patients whohave a history of treatment for hyperthyroidismalso have a higher prevalence of anxiety,depression, and psychosocial dysfunction thanhealthy controls.60
Hyperlipidemia. Overt hypothyroidism has longbeen known to be associated with elevated levels ofcholesterol,61 but patients in the earliest studies hadsevere hypothyroidism. In more recent studies, thereis a clinically important increase in total cholesteroland low-density lipoprotein (LDL) cholesterolamong men62 and women63,64 with overthypothyroidism in those who have serum TSHlevels higher than 20 mU/L.
In women with subclinical hypothyroidism, therelation between TSH and total cholesterol or LDLcholesterol is inconsistent. In the Whickham survey,there was no relationship between subclinicalhypothyroidism and hyperlipidemia.17 In theRotterdam study16 (discussed in detail below), lipidlevels were significantly lower among women withsubclinical hypothyroidism than among euthyroidwomen. The New Mexico Elder Health Survey, afair-quality study of randomly selected Medicarerecipients, found no differences in levels of totalcholesterol, LDL cholesterol, high-densitylipoprotein (HDL) cholesterol, or triglyceridesbetween patients who had a serum TSH less than4.6 (n = 684) and those who had a serum TSHbetween 4.7 and 10 mU/L (n = 105). There werenon-significant increases in LDL cholesterol andHDL cholesterol among women who had a serumTSH greater than 10 mU/L (LDL cholesterol 3.7mmol/L [143 mg/dL] vs 3.3 mmol/L [128 mg/dL]in euthyroid women, P = 0.08; HDL cholesterol1.07 mmol/L [41.6 mg/dL] vs 1.23 mmol/L [47.5mg/dL], P = 0.053).14
Conversely, a recent cross-sectional study of 279women older than age 65 found a strong relationshipbetween hyperlipidemia and serum TSH levels.65 Ofthe 279 women, 19 (6.8%) had a serum TSH greaterthan 5.5 mU/L. After adjustment for age, weight,and estrogen use, women who had a serum TSHgreater than 5.5 mU/L had 13% higher LDLcholesterol (95% CI, 1%–25%) and 13% lowerHDL cholesterol (CI, –25% to 0%) than those with
5
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults

6
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
a normal serum TSH (0.1–5.5 mU/L). However,2 of the 19 women who had an elevated TSH usedlevothyroxine, suggesting they had inadequatelytreated overt hypothyroidism. Because FT4 and FT3levels were not measured, it is possible that others inthis group had overt hypothyroidism as well.
Men with a mildly elevated TSH generally do nothave an increased risk for hyperlipidemia, but dataon men are sparse. Men with hypercholesterolemiado not have a higher prevalence of subclinicalhypothyroidism than men with normal lipid levels.66
Atherosclerosis. The relationship between subclinicalhypothyroidism and the later development ofatherosclerosis is unclear.14,16,67 The Whickhamsurvey found no relationship between initial TSHlevels and the subsequent development of ischemicheart disease over 20 years of follow-up.67
A widely publicized population-based study of1,149 women aged 55 or older from Rotterdamcame to a different conclusion.16 The main analysisin the paper was cross-sectional. In that analysis,after adjustment for age, body mass index,cholesterol level, blood pressure, and smoking status,a serum TSH greater than 4.0 mU/L was associatedwith a history of myocardial infarction (OR, 2.3;CI, 1.3–4.2) and with atherosclerosis of theabdominal aorta, which was diagnosed by blindedreview of a lateral radiograph of the lumbar spine(OR, 1.9; CI, 1.2–3.1). An analysis of incidentmyocardial infarction over 3 to 6 years of follow-upfound a statistically non-significant increased risk inwomen with a serum TSH greater than 4.0 mU/L(adjusted relative risk, 2.5; CI, 0.7–9.1).
The strengths of the Rotterdam study are therelatively large sample size, adjustment for somepotential confounders, and validated, blindedassessment of outcomes. Because the study wasprimarily cross-sectional, however, the findingsdo not prove that an elevated TSH precedes thedevelopment of atherosclerosis. The prospectivepart of the study adds little because, at baseline, thewomen who had an elevated TSH had a higherprevalence of atherosclerotic disease; they would beexpected to have a higher incidence of myocardialinfarction over 3 to 6 years, in any case. Theprospective analysis would have been more
consequential if patients who had atherosclerosisat baseline had been excluded.
In the Rotterdam study, women with subclinicalhypothyroidism had lower lipid levels thaneuthyroid women; this might be an artifact ofhigher use of diet or other lipid-lowering therapy inwomen with known cardiovascular risk factors, butit also might suggest that atherosclerosis developedby another mechanism. One hypothesis is thatelevations in both homocysteine and cholesterolmay contribute to the elevated risk foratherosclerosis in overt hypothyroidism. Incross-sectional studies, including an analysis of theSecond National Health and Nutrition ExaminationSurvey (NHANES-II) sample, patients with overthypothyroidism had higher homocysteine levelsthan euthyroid patients.68,69 The association ofelevated homocysteine and overt hypothyroidismappears to persist after controlling for serum folatelevels, which are decreased in overthypothyroidism.68–72 However, in the only studyconcerning patients who had subclinicalhypothyroidism, there was no association.73
Efficacy of TreatmentI identified 14 randomized trials of levothyroxine
therapy, 8 of which met the inclusion criteria.58,59,74–79
Six concerned patients with elevated TSH levels,1 concerned hyperlipidemic patients withhigh-normal TSH levels,75 and the last trialconcerned patients with a normal TSH who hadsymptoms of hypothyroidism.77
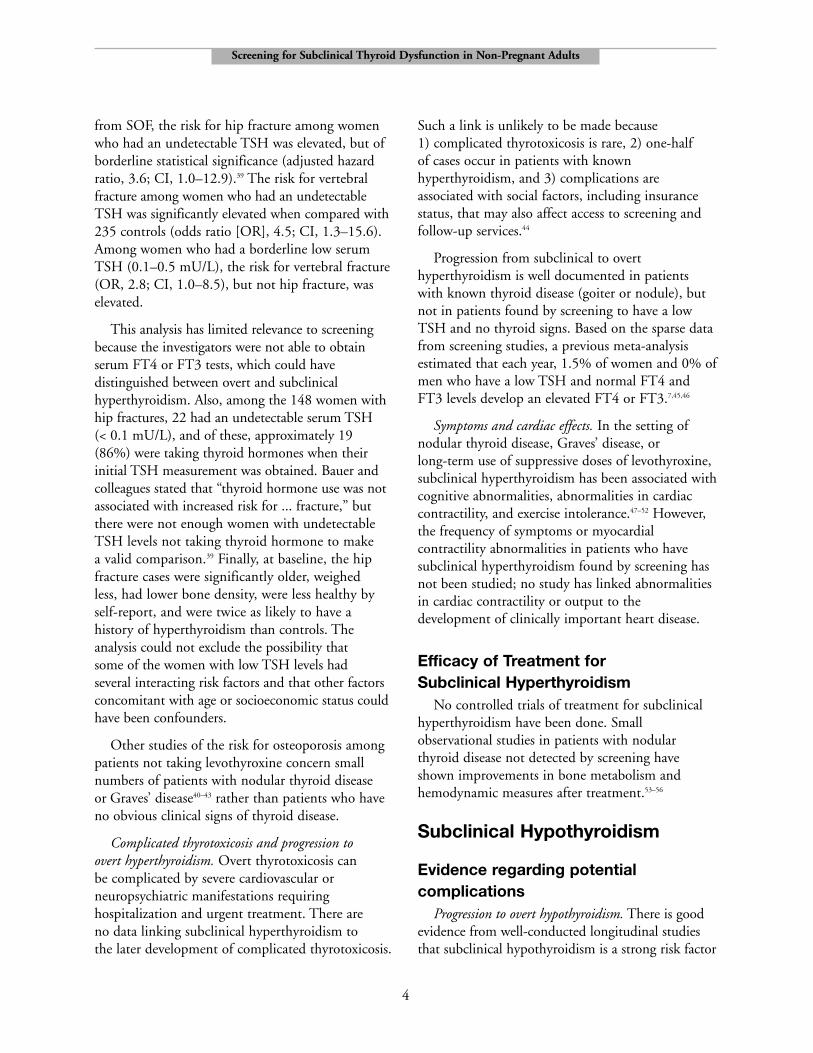
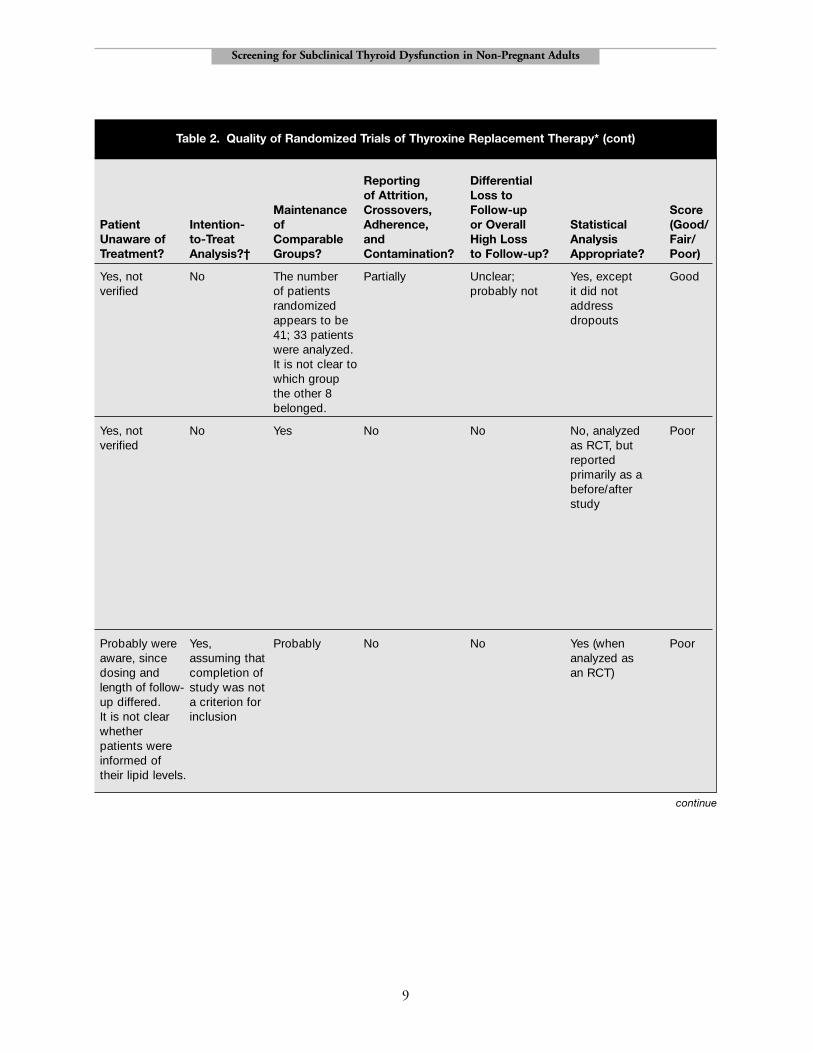
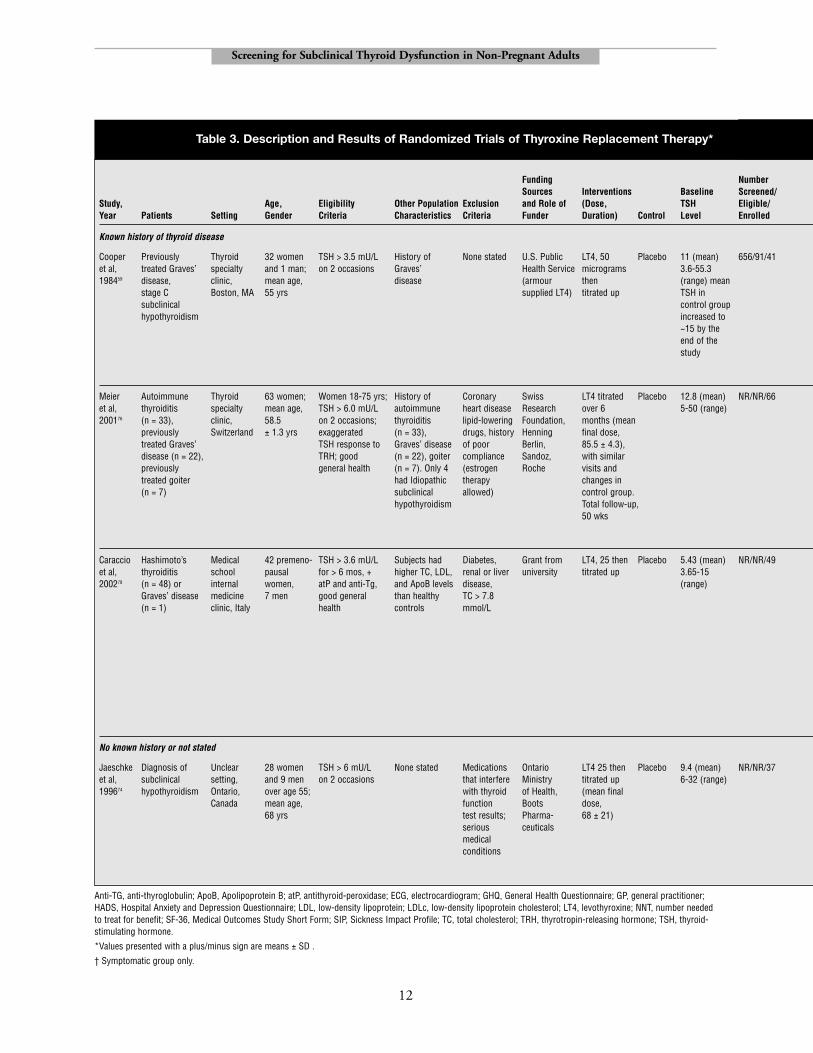
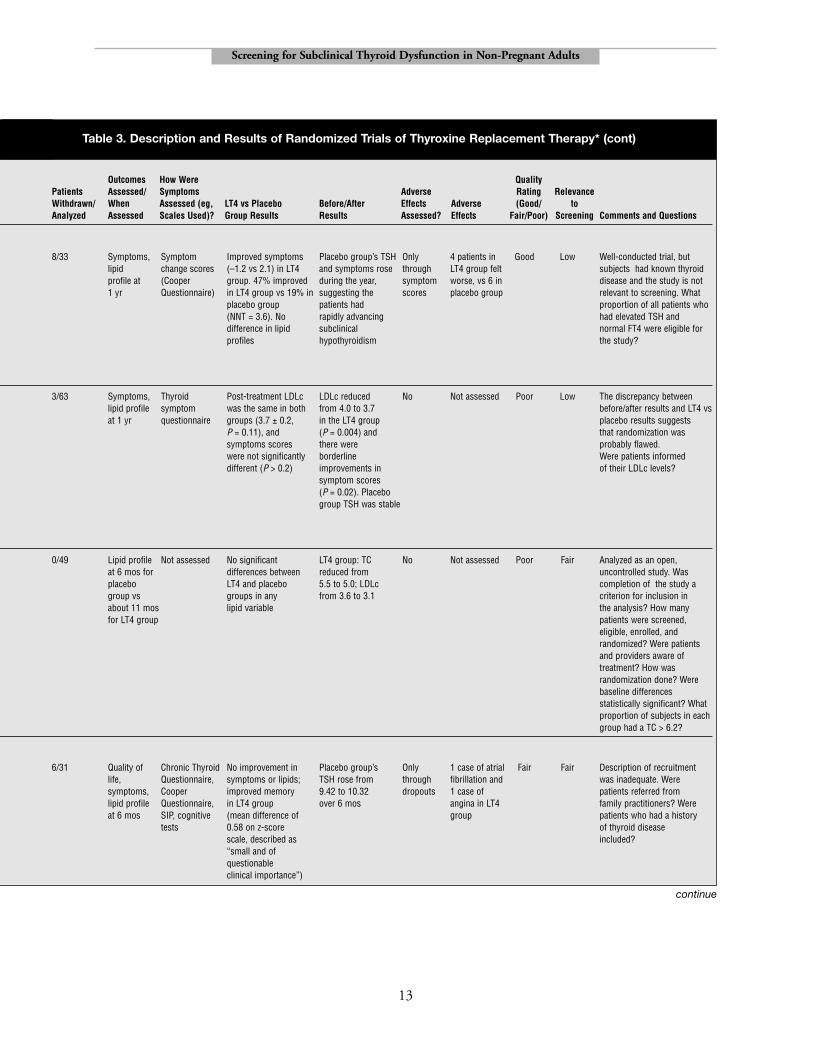
Randomized trials of levothyroxine treatment insubclinical hypothyroidism and in symptomaticpatients who have a normal TSH are described inTable 2 (quality ratings) and Table 3 (descriptionand results). The first 2 trials in the tablesconcerned patients followed in thyroid specialtyclinics. In both trials, patients had a mean serumTSH above 10 mU/L. The first trial (Cooper et al)concerned patients who had been treated for Graves’disease in whom TSH was increasing relativelyquickly.59 Symptoms were rated on the CooperQuestionnaire, a 24-point scale that records how 6symptoms of hypothyroidism change over time.After 1 year, patients taking levothyroxine improved

7
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
by 2.1 points, while patients taking placebodeteriorated by 1.2 points (P = 0.037). Thedifference (3.3 points) is roughly equivalent tocomplete relief of 1 symptom and partial relief of asecond symptom per patient. Eight (47%) of 17treated patients reported reduced or mildersymptoms, 4 felt worse, and 5 reported no changein symptoms. In the placebo group, 3 (19%) of 16patients felt better, 6 felt worse, and 7 reported nochange. The difference between the proportion ofpatients who felt better in each group was 0.28(CI, –0.09 to 0.65), indicating that the numberneeded to treat to benefit 1 patient was 3.5.59
Treatment had no effect on lipid levels. The internalvalidity of this trial was rated as good quality; it wasthe highest-quality trial of the group.
The second trial (Meier et al) concerned patientswith thyroiditis or a history of Graves’ disease.76
Treatment with levothyroxine had no effect onsymptoms. In reporting results, the authorsemphasized that there was a significant reductionin LDL cholesterol in the levothyroxine-treatedgroup, from 4.0 to 3.7 mmol/L (P = 0.004), andno significant reduction in the placebo group.The difference appears to be related to an imbalancein the groups at baseline: pre-treatment LDLcholesterol was 4.0 mmol/L (154 mg/dL) in thetreatment group versus 3.7 mmol/L (143 mg/dL)in the placebo group. In fact, post-treatment LDLcholesterol was the same in both groups (3.7 ± 0.2mmol/L [143 ± 7 mg/dL, P = 0.11]). When theresults were analyzed as a randomized trial, thedifference between the treatment and control groups’lipid levels was not significant. The discrepancysuggests that randomization may have been flawed.
The rated relevance of these 2 studies to screeningis low. The Cooper et al study supports treatmentin patients with a history of treated Graves’ disease,especially if the serum TSH is above 10 mU/L.However, it has little relevance to screening becausethe natural history of treated Graves’ diseasediffers from the natural history of spontaneoushypothyroidism in the general population.59
The third trial recruited patients known to haveHashimoto’s thyroiditis, positive antithyroidantibodies, and mildly elevated TSH levels.78 When
analyzed as a randomized trial, there were nosignificant differences between levothyroxine-treatedand placebo groups on any lipid variable. Whenanalyzed as a pre-/post-treatment study, there was astatistically significant reduction in LDL cholesterollevels (3.6 mmol/L [139 mg/dL] to 3.1 mmol/L[120 mg/dL]) in the levothyroxine-treated group,but not in the control group. The study appeared tobe unblinded, which is a major flaw becausedifferential attention to lipid levels in the treatmentand control groups could lead to different behavioralapproaches to reducing lipid levels. If the results arevalid, they would be relevant to screening; the meanTSH was only slightly elevated, and patients whohave antithyroid antibodies and a modestly elevatedTSH are found commonly in screening programs.
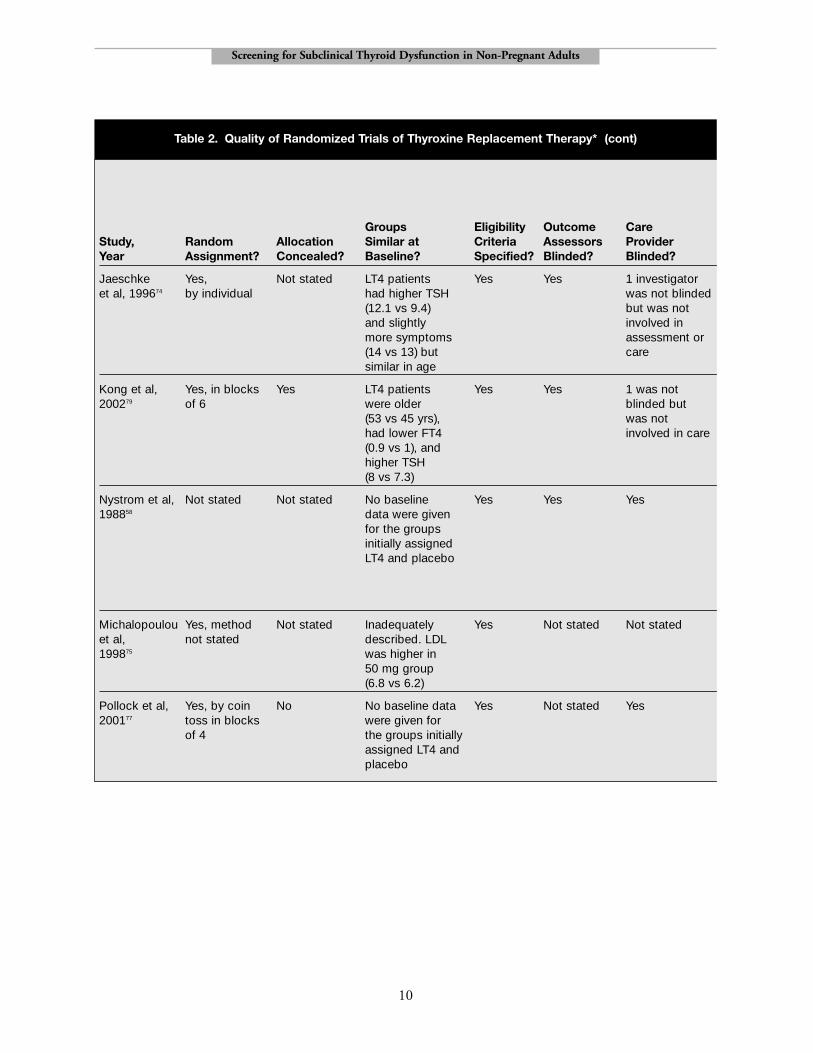
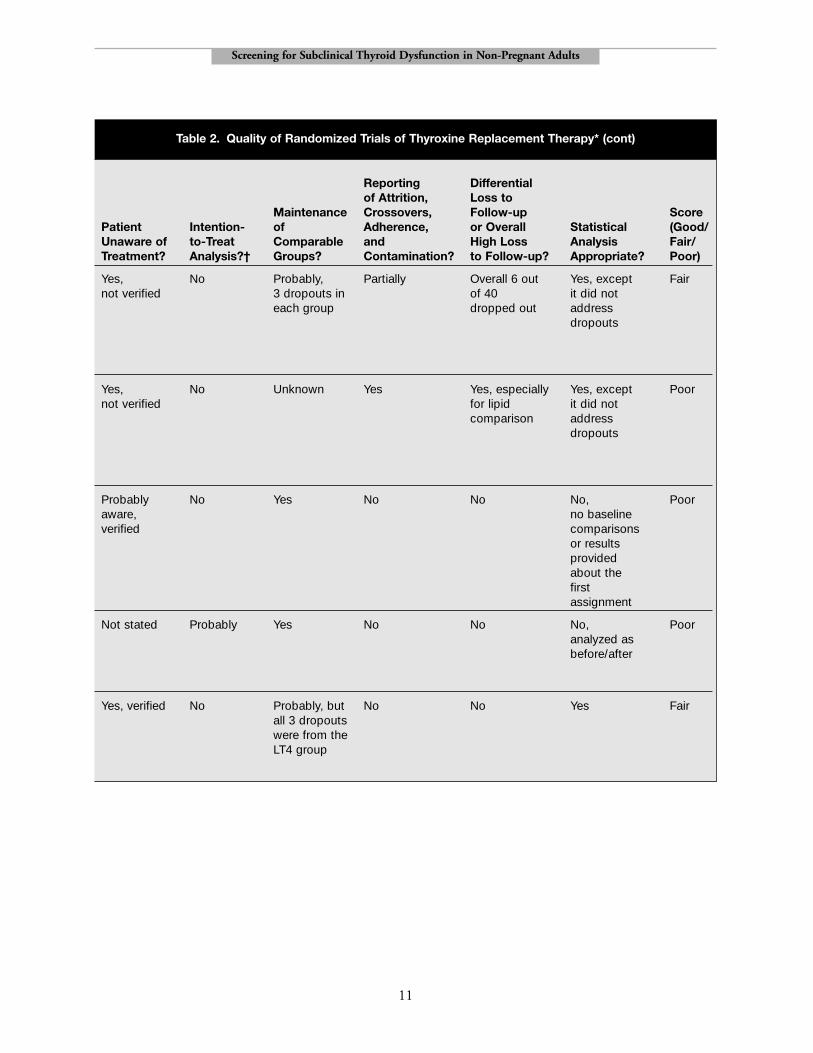
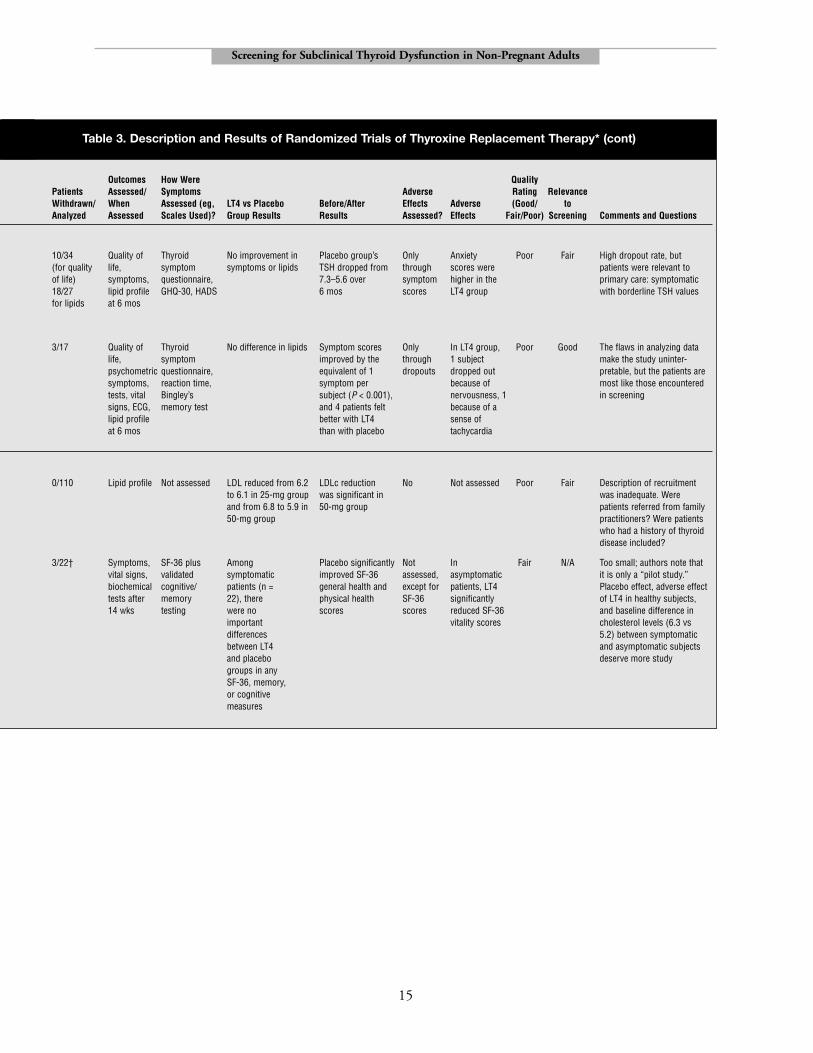
The next 3 studies may have had more relevanceto screening or primary care: they generallyconcerned patients, mostly women, with subclinicalhypothyroidism who were not previously treated forGraves’ disease or nodular thyroid disease. However,2 of the 3 studies had poor internal validity. In thefair-quality trial by Jaeschke and colleagues, 37patients with subclinical hypothyroidism wererecruited from the outpatient clinics of acommunity hospital and randomized tolevothyroxine treatment or placebo.74 Patients givenplacebo did as well or better than those givenlevothyroxine. After 6 months, in the levothyroxinegroup, 8 patients improved, 3 worsened, and 5remained the same, according to the CooperQuestionnaire. In the placebo group, 11 patientsimproved, 1 worsened, and 4 remained the same.After 11 months, patients treated with levothyroxinehad a small but statistically significant improvementin short-term memory, but treatment did notimprove general health status as measured by astandardized questionnaire, the Sickness ImpactProfile (SIP). The other negative trial was too smallto achieve balance in the compared groups and hada high rate of loss to follow-up.79
A small crossover trial58 concerned womenidentified by screening in the general population.The 20 patients were women older than age 50 whohad an initial serum TSH between 4 and 15 mU/L.After 6 months of treatment, the mean symptomscore improved by 1.81 units, equivalent to complete
8
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
FT4, serum free thyroxine; LDLc, low-density lipoprotein cholesterol; LT4, levothryroxine; RCT, randomized controlled trial; TSH,thyroid-stimulating hormone.
*Values reported with plus/minus signs are means ± SD.
† Symptomatic group only.
Groups Eligibility Outcome CareStudy, Random Allocation Similar at Criteria Assessors ProviderYear Assignment? Concealed? Baseline? Specified? Blinded? Blinded?
Cooper et al, Yes, by Not stated LT4 patients Yes Yes Probably (1 of198459 individual were older 2 investigators
(58.2 vs 50.2) is said to beand had fewer blinded)symptoms (2.1 vs 2.4) but otherwise similar
Meier et al, Sequential No LT4 patients Yes Not stated Yes200176 assignment had higher TSH
using a (14.4 ± 1.7 vs predefined list; 11.3 ± 1.0) and randomized by LDLc (4.1 vs 3.7) matched pairs but were
otherwise similar for the whole groups (n = 66); comparisons were not presented for the analyzed group(n = 63)
Caraccio Yes, Not stated Generally yes, Yes No Noet al, 200278 by individual but mean TSH
(6 vs 4.9) and LDLc (3.6 vs 3.3) were higher in LT4 group
Table 2. Quality of Randomized Trials of Thyroxine Replacement Therapy*
9
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Reporting Differential of Attrition, Loss to
Maintenance Crossovers, Follow-up ScorePatient Intention- of Adherence, or Overall Statistical (Good/ Unaware of to-Treat Comparable and High Loss Analysis Fair/ Treatment? Analysis?† Groups? Contamination? to Follow-up? Appropriate? Poor)
Yes, not No The number Partially Unclear; Yes, except Goodverified of patients probably not it did not
randomized address appears to be dropouts41; 33 patientswere analyzed. It is not clear to which group the other 8 belonged.
Yes, not No Yes No No No, analyzed Poorverified as RCT, but
reported primarily as a before/afterstudy
Probably were Yes, Probably No No Yes (when Pooraware, since assuming that analyzed as dosing and completion of an RCT)length of follow- study was not up differed. a criterion forIt is not clear inclusionwhether patients wereinformed of their lipid levels.
Table 2. Quality of Randomized Trials of Thyroxine Replacement Therapy* (cont)
continue
10
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Groups Eligibility Outcome CareStudy, Random Allocation Similar at Criteria Assessors ProviderYear Assignment? Concealed? Baseline? Specified? Blinded? Blinded?
Jaeschke Yes, Not stated LT4 patients Yes Yes 1 investigator et al, 199674 by individual had higher TSH was not blinded
(12.1 vs 9.4) but was not and slightly involved in more symptoms assessment or (14 vs 13) but caresimilar in age
Kong et al, Yes, in blocks Yes LT4 patients Yes Yes 1 was not 200279 of 6 were older blinded but
(53 vs 45 yrs), was not had lower FT4 involved in care(0.9 vs 1), and higher TSH (8 vs 7.3)
Nystrom et al, Not stated Not stated No baseline Yes Yes Yes198858 data were given
for the groupsinitially assigned LT4 and placebo
Michalopoulou Yes, method Not stated Inadequately Yes Not stated Not statedet al, not stated described. LDL 199875 was higher in
50 mg group (6.8 vs 6.2)
Pollock et al, Yes, by coin No No baseline data Yes Not stated Yes200177 toss in blocks were given for
of 4 the groups initially assigned LT4 and placebo
Table 2. Quality of Randomized Trials of Thyroxine Replacement Therapy* (cont)
11
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Reporting Differential of Attrition, Loss to
Maintenance Crossovers, Follow-up ScorePatient Intention- of Adherence, or Overall Statistical (Good/ Unaware of to-Treat Comparable and High Loss Analysis Fair/ Treatment? Analysis?† Groups? Contamination? to Follow-up? Appropriate? Poor)
Yes, No Probably, Partially Overall 6 out Yes, except Fairnot verified 3 dropouts in of 40 it did not
each group dropped out address dropouts
Yes, No Unknown Yes Yes, especially Yes, except Poornot verified for lipid it did not
comparison address dropouts
Probably No Yes No No No, Pooraware, no baseline verified comparisons
or results provided about the first assignment
Not stated Probably Yes No No No, Pooranalyzed asbefore/after
Yes, verified No Probably, but No No Yes Fairall 3 dropouts were from the LT4 group
Table 2. Quality of Randomized Trials of Thyroxine Replacement Therapy* (cont)
12
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Funding NumberSources Interventions Baseline Screened/
Study, Age, Eligibility Other Population Exclusion and Role of (Dose, TSH Eligible/ Year Patients Setting Gender Criteria Characteristics Criteria Funder Duration) Control Level Enrolled
Known history of thyroid disease
Cooper Previously Thyroid 32 women TSH > 3.5 mU/L History of None stated U.S. Public LT4, 50 Placebo 11 (mean) 656/91/41et al, treated Graves’ specialty and 1 man; on 2 occasions Graves’ Health Service micrograms 3.6-55.3 198459 disease, clinic, mean age, disease (armour then (range) mean
stage C Boston, MA 55 yrs supplied LT4) titrated up TSH in subclinical control group hypothyroidism increased to
~15 by the end of the study
Meier Autoimmune Thyroid 63 women; Women 18-75 yrs; History of Coronary Swiss LT4 titrated Placebo 12.8 (mean) NR/NR/66et al, thyroiditis specialty mean age, TSH > 6.0 mU/L autoimmune heart disease Research over 6 5-50 (range)200176 (n = 33), clinic, 58.5 on 2 occasions; thyroiditis lipid-lowering Foundation, months (mean
previously Switzerland ± 1.3 yrs exaggerated (n = 33), drugs, history Henning final dose, treated Graves’ TSH response to Graves’ disease of poor Berlin, 85.5 ± 4.3), disease (n = 22), TRH; good (n = 22), goiter compliance Sandoz, with similar previously general health (n = 7). Only 4 (estrogen Roche visits and treated goiter had Idiopathic therapy changes in (n = 7) subclinical allowed) control group.
hypothyroidism Total follow-up,50 wks
Caraccio Hashimoto’s Medical 42 premeno- TSH > 3.6 mU/L Subjects had Diabetes, Grant from LT4, 25 then Placebo 5.43 (mean) NR/NR/49et al, thyroiditis school pausal for > 6 mos, + higher TC, LDL, renal or liver university titrated up 3.65-15 200278 (n = 48) or internal women, atP and anti-Tg, and ApoB levels disease, (range)
Graves’ disease medicine 7 men good general than healthy TC > 7.8 (n = 1) clinic, Italy health controls mmol/L
No known history or not stated
Jaeschke Diagnosis of Unclear 28 women TSH > 6 mU/L None stated Medications Ontario LT4 25 then Placebo 9.4 (mean) NR/NR/37et al, subclinical setting, and 9 men on 2 occasions that interfere Ministry titrated up 6-32 (range)199674 hypothyroidism Ontario, over age 55; with thyroid of Health, (mean final
Canada mean age, function Boots dose, 68 yrs test results; Pharma- 68 ± 21)
serious ceuticalsmedical conditions
Table 3. Description and Results of Randomized Trials of Thyroxine Replacement Therapy*
Anti-TG, anti-thyroglobulin; ApoB, Apolipoprotein B; atP, antithyroid-peroxidase; ECG, electrocardiogram; GHQ, General Health Questionnaire; GP, general practitioner;HADS, Hospital Anxiety and Depression Questionnaire; LDL, low-density lipoprotein; LDLc, low-density lipoprotein cholesterol; LT4, levothyroxine; NNT, number neededto treat for benefit; SF-36, Medical Outcomes Study Short Form; SIP, Sickness Impact Profile; TC, total cholesterol; TRH, thyrotropin-releasing hormone; TSH, thyroid-stimulating hormone.
*Values presented with a plus/minus sign are means ± SD .
† Symptomatic group only.
13
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Outcomes How Were QualityPatients Assessed/ Symptoms Adverse Rating Relevance Withdrawn/ When Assessed (eg, LT4 vs Placebo Before/After Effects Adverse (Good/ to Analyzed Assessed Scales Used)? Group Results Results Assessed? Effects Fair/Poor) Screening Comments and Questions
8/33 Symptoms, Symptom Improved symptoms Placebo group’s TSH Only 4 patients in Good Low Well-conducted trial, but lipid change scores (–1.2 vs 2.1) in LT4 and symptoms rose through LT4 group felt subjects had known thyroidprofile at (Cooper group. 47% improved during the year, symptom worse, vs 6 in disease and the study is not 1 yr Questionnaire) in LT4 group vs 19% in suggesting the scores placebo group relevant to screening. What
placebo group patients had proportion of all patients who (NNT = 3.6). No rapidly advancing had elevated TSH and difference in lipid subclinical normal FT4 were eligible for profiles hypothyroidism the study?
3/63 Symptoms, Thyroid Post-treatment LDLc LDLc reduced No Not assessed Poor Low The discrepancy between lipid profile symptom was the same in both from 4.0 to 3.7 before/after results and LT4 vs at 1 yr questionnaire groups (3.7 ± 0.2, in the LT4 group placebo results suggests
P = 0.11), and (P = 0.004) and that randomization was symptoms scores there were probably flawed.were not significantly borderline Were patients informed different (P > 0.2) improvements in of their LDLc levels?
symptom scores (P = 0.02). Placebogroup TSH was stable
0/49 Lipid profile Not assessed No significant LT4 group: TC No Not assessed Poor Fair Analyzed as an open, at 6 mos for differences between reduced from uncontrolled study. Was placebo LT4 and placebo 5.5 to 5.0; LDLc completion of the study a group vs groups in any from 3.6 to 3.1 criterion for inclusion inabout 11 mos lipid variable the analysis? How many for LT4 group patients were screened,
eligible, enrolled, and randomized? Were patients and providers aware of treatment? How was randomization done? Were baseline differences statistically significant? What proportion of subjects in each group had a TC > 6.2?
6/31 Quality of Chronic Thyroid No improvement in Placebo group’s Only 1 case of atrial Fair Fair Description of recruitment life, Questionnaire, symptoms or lipids; TSH rose from through fibrillation and was inadequate. Were symptoms, Cooper improved memory 9.42 to 10.32 dropouts 1 case of patients referred from lipid profile Questionnaire, in LT4 group over 6 mos angina in LT4 family practitioners? Were at 6 mos SIP, cognitive (mean difference of group patients who had a history
tests 0.58 on z-score of thyroid disease scale, described as included?“small and of questionable clinical importance”)
Table 3. Description and Results of Randomized Trials of Thyroxine Replacement Therapy* (cont)
continue
14
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Funding NumberSources Interventions Baseline Screened/
Study, Age, Eligibility Other Population Exclusion and Role of (Dose, TSH Eligible/ Year Patients Setting Gender Criteria Characteristics Criteria Funder Duration) Control Level Enrolled
No known history or not stated, continued
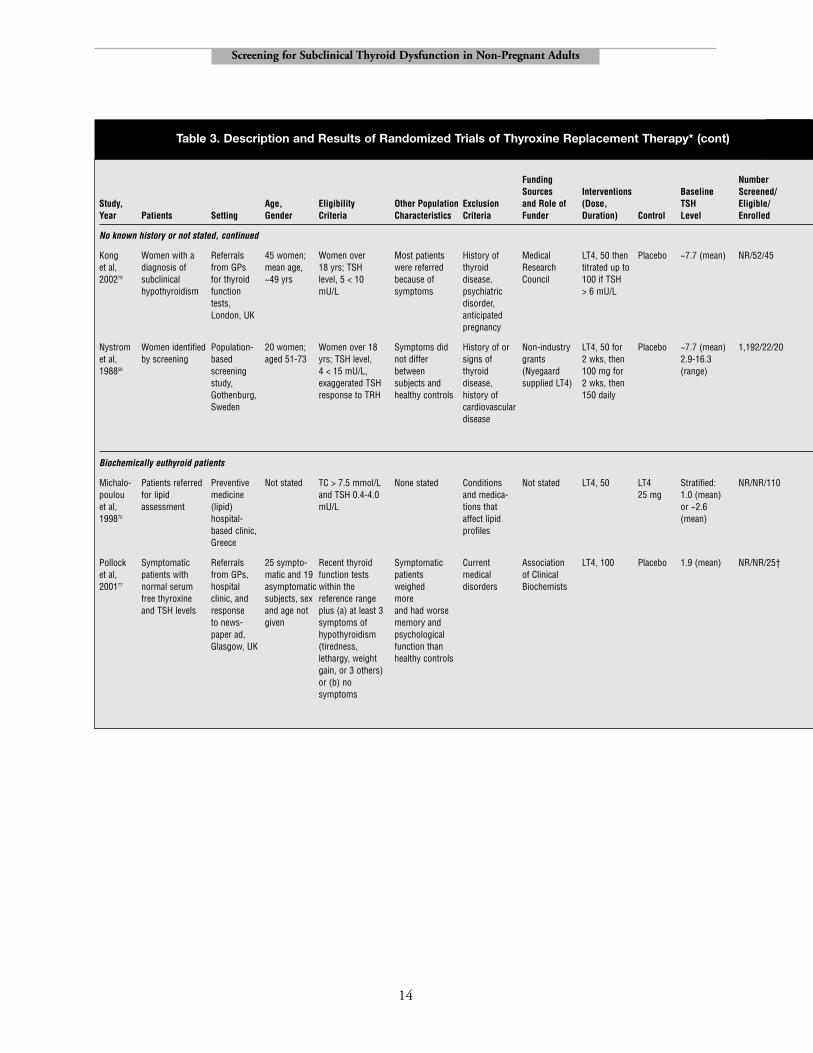
Kong Women with a Referrals 45 women; Women over Most patients History of Medical LT4, 50 then Placebo ~7.7 (mean) NR/52/45et al, diagnosis of from GPs mean age, 18 yrs; TSH were referred thyroid Research titrated up to 200279 subclinical for thyroid ~49 yrs level, 5 < 10 because of disease, Council 100 if TSH
hypothyroidism function mU/L symptoms psychiatric > 6 mU/Ltests, disorder, London, UK anticipated
pregnancy
Nystrom Women identified Population- 20 women; Women over 18 Symptoms did History of or Non-industry LT4, 50 for Placebo ~7.7 (mean) 1,192/22/20et al, by screening based aged 51-73 yrs; TSH level, not differ signs of grants 2 wks, then 2.9-16.3198858 screening 4 < 15 mU/L, between thyroid (Nyegaard 100 mg for (range)
study, exaggerated TSH subjects and disease, supplied LT4) 2 wks, then Gothenburg, response to TRH healthy controls history of 150 dailySweden cardiovascular
disease
Biochemically euthyroid patients
Michalo- Patients referred Preventive Not stated TC > 7.5 mmol/L None stated Conditions Not stated LT4, 50 LT4 Stratified: NR/NR/110poulou for lipid medicine and TSH 0.4-4.0 and medica- 25 mg 1.0 (mean)et al, assessment (lipid) mU/L tions that or ~2.6 199875 hospital- affect lipid (mean)
based clinic, profilesGreece
Pollock Symptomatic Referrals 25 sympto- Recent thyroid Symptomatic Current Association LT4, 100 Placebo 1.9 (mean) NR/NR/25†et al, patients with from GPs, matic and 19 function tests patients medical of Clinical 200177 normal serum hospital asymptomatic within the weighed disorders Biochemists
free thyroxine clinic, and subjects, sex reference range more and TSH levels response and age not plus (a) at least 3 and had worse
to news- given symptoms of memory and paper ad, hypothyroidism psychological Glasgow, UK (tiredness, function than
lethargy, weight healthy controlsgain, or 3 others)or (b) no symptoms
Table 3. Description and Results of Randomized Trials of Thyroxine Replacement Therapy* (cont)
15
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
Outcomes How Were QualityPatients Assessed/ Symptoms Adverse Rating Relevance Withdrawn/ When Assessed (eg, LT4 vs Placebo Before/After Effects Adverse (Good/ to Analyzed Assessed Scales Used)? Group Results Results Assessed? Effects Fair/Poor) Screening Comments and Questions
10/34 Quality of Thyroid No improvement in Placebo group’s Only Anxiety Poor Fair High dropout rate, but (for quality life, symptom symptoms or lipids TSH dropped from through scores were patients were relevant toof life) symptoms, questionnaire, 7.3–5.6 over symptom higher in the primary care: symptomatic18/27 lipid profile GHQ-30, HADS 6 mos scores LT4 group with borderline TSH valuesfor lipids at 6 mos
3/17 Quality of Thyroid No difference in lipids Symptom scores Only In LT4 group, Poor Good The flaws in analyzing data life, symptom improved by the through 1 subject make the study uninter-psychometric questionnaire, equivalent of 1 dropouts dropped out pretable, but the patients are symptoms, reaction time, symptom per because of most like those encountered tests, vital Bingley’s subject (P < 0.001), nervousness, 1 in screeningsigns, ECG, memory test and 4 patients felt because of a lipid profile better with LT4 sense of at 6 mos than with placebo tachycardia
0/110 Lipid profile Not assessed LDL reduced from 6.2 LDLc reduction No Not assessed Poor Fair Description of recruitment to 6.1 in 25-mg group was significant in was inadequate. Were and from 6.8 to 5.9 in 50-mg group patients referred from family 50-mg group practitioners? Were patients
who had a history of thyroid disease included?
3/22† Symptoms, SF-36 plus Among Placebo significantly Not In Fair N/A Too small; authors note that vital signs, validated symptomatic improved SF-36 assessed, asymptomatic it is only a “pilot study.” biochemical cognitive/ patients (n = general health and except for patients, LT4 Placebo effect, adverse effect tests after memory 22), there physical health SF-36 significantly of LT4 in healthy subjects, 14 wks testing were no scores scores reduced SF-36 and baseline difference in
important vitality scores cholesterol levels (6.3 vs differences 5.2) between symptomatic between LT4 and asymptomatic subjects and placebo deserve more studygroups in any SF-36, memory, or cognitive measures
Table 3. Description and Results of Randomized Trials of Thyroxine Replacement Therapy* (cont)

16
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
relief of 1 symptom per patient. As judged bysubjective improvement and cognitive measures, 4(24%) of the 19 patients who received levothyroxineimproved, while 2 (12%) felt worse with treatment.
The last 2 studies listed in Table 3 (Michalopoulouet al and Pollock et al) concern patients who haveTSH levels in the normal range. In the study byMichalopoulou and colleagues, 50 micrograms oflevothyroxine therapy reduced LDL cholesterol levelsfrom 6.8 to 5.9 mmol/L (262–228 mg/dL) inpatients with elevated total cholesterol levels (> 7.5mmol/L [> 290 mg/dL]) and normal TSH levels.75 Inthe study by Pollock and colleagues, levothyroxinewas ineffective in patients who had symptoms ofhypothyroidism but normal TSH and FT4 levels.77
The latter study, designed as a crossover study, foundthat levothyroxine significantly reduced the ShortForm-36 (SF-36) vitality score in healthy patientsand also documented a clinically important andstatistically significant effect of placebo.
Many observational studies have examined theeffects of treatment in patients with subclinicalhypothyroidism. A recent meta-analysis of bothobservational and randomized studies found that,in previously untreated patients, total cholesterolwas reduced by 0.14 mmol/L (5.6 mg/dL).80
Another review concluded that levothyroxinetreatment might reduce serum cholesterol by 8%in selected patients who have both a serum TSH of10 mU/L or greater and an elevated total cholesterolof 6.2 mmol/L or greater (240 mg/dL).7 About7% of individuals with subclinical hypothyroidismmeet these criteria.
The studies on which these analyses are basedhave important limitations.21 Many were before/afterstudies in which reductions in serum lipids couldhave been due to regression toward the mean.Samples were small, selection of patients was poorlydescribed, clinicians and patients were aware of thetreatment and of the need to lower lipid levels, andoutcome assessment may have been biased. That is,the problem is not that these studies are observational,but that many of them are poor quality.
The hazards of relying on observational studiesof the effect of drug therapy is illustrated by a large(n = 139) open study of levothyroxine to treat
symptoms of hypothyroidism in patients who hadnormal thyroid function tests. This study foundthat the mean number of signs and symptoms ofhypothyroidism decreased from 13 to 3 following6 months or more of treatment; 76% of patients hadimprovement or resolution of over 12 findings.81
Whether or not these effects are real (a subsequentrandomized trial had negative results [Table 3] butwas too small to exclude a clinically significanteffect), they illustrate that only well-controlled trialscan determine the effects of thyroxine therapy inpatients with subclinical hypothyroidism.
Adverse Effects ofLevothyroxine Treatment
Adverse effects of replacement doses oflevothyroxine include nervousness, palpitations,atrial fibrillation, and exacerbation of anginapectoris. Adverse effects were not assessed carefullyin the randomized trials listed in Table 3, althoughsome reported them incidentally. In 1 of the trials,2 of 20 (10%) patients taking levothyroxine quitthe protocol because of nervousness and a senseof palpitations.58 In another, 2 of the 18 (11%)patients assigned to levothyroxine withdrew becauseof complications, 1 because of an increase in angina, and the second because of new-onset atrialfibrillation.74 In a third, anxiety scores were higherin the levothyroxine group.79
A systematic review of observational studiespublished from 1966 to 1997 found thatreplacement doses of levothyroxine (restoring TSHto normal levels) have not been associated withosteoporosis or with any other serious long-termadverse effects.82 A short-term randomized trial oflevothyroxine for subclinical hypothyroidismconfirms this view.83
The harms of overtreatment with levothyroxine,indicated by an undetectable TSH, are uncertain.About one-fourth of patients receiving levothyroxinefor primary hypothyroidism are maintainedunintentionally on doses sufficient to cause the TSHto be undetectable.2,31 Data from the Framinghamcohort suggest that 1 excess case of atrial fibrillationmight occur for every 114 patients treated withdoses of levothyroxine sufficient to suppress the

17
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
TSH.31 As mentioned above, some informationsuggests that, in patients taking levothyroxine, anundetectable TSH is associated with an increasedrisk for osteoporosis36,37 and fractures,39 but otherstudies have found no difference in bone density38 orhip fracture rates.84 Suppressive doses oflevothyroxine can temporarily increase heart rateand left ventricular mass,85 but there is no evidencethat this causes long-term complications.
Another potential harm is treatment of healthypatients based on false-positive test results. Inscreening programs and in the primary care clinic,many patients found to have an abnormal TSHrevert to normal over time. In 1 randomized trial,for example, mildly elevated TSH level reverted tonormal in 8 of 19 patients given placebo.74 In olderpatients, only 59% (range, 14%–87%) of patientswith an undetectable TSH on initial screening hadan undetectable TSH level when the TSH wasrepeated.45,86 In the Framingham cohort, screeningidentified 41 people with an undetectable serumTSH (≤ 0.1 mU/L) and a normal serum FT4 level(< 129 nmol/L).87 After 4 years of follow-up, when33 of these people were retested, 29 had higherserum TSH levels (> 0.1 mU/L).
DiscussionThe ability of screening programs to detect
subclinical thyroid dysfunction has beendemonstrated in good-quality cohort studies.There is also good evidence that, in the generalpopulation, an undetectable TSH level is arisk factor for the later development of atrialfibrillation, but there have not been any studiesof early treatment to prevent this complication.
An elevated TSH level—even a mildly elevatedone—is a risk factor for the later development ofovert hypothyroidism. Early treatment wouldprevent this progression, but the balance of benefitsand harms is unclear. The key uncertainties are:
1. Without screening or prophylaxis, how longwould overt hypothyroidism be undetected?
2. How much morbidity would undiagnosed overthypothyroidism cause while undetected?
3. What are the harms of treatment in those whodo not progress?
Data showing that progression to overt disease isassociated with significant burden of illness wouldstrengthen the case for preemptive treatment.
Other potential harms of subclinical thyroiddysfunction are not well established. Data regardingosteoporosis, fracture, hyperlipidemia, andatherosclerotic disease are inconsistent, and mostdata come from patients who take levothyroxine orhave clinically evident thyroid disease.
Not surprisingly, experts give conflictingadvice about the treatment of subclinicalhypothyroidism.6,21,26,28 There is good evidencethat levothyroxine reduces symptoms (but not lipidlevels) in patients who have a markedly elevatedTSH level (> 10 mU/L) following surgery orradioiodine treatment. However, in apparentlyhealthy patients who have mildly elevated TSH levels(4–7 mU/L), the largest group identified byscreening, the frequency of hyperlipidemia andsymptoms may be no different from that ofeuthyroid individuals. The main gap in the evidenceis the lack of convincing data from controlled trialsthat early treatment reduces lipid levels, symptoms,or the risk for cardiovascular disease for patients withmild thyroid dysfunction detected by screening.
AcknowledgmentsThe author thanks Robert Utiger, Marc Stone,
Doug Bauer, Steven Teutsch, and David Atkins fortheir comments on the report on which this articleis based.
References1. Hollowell JG, Staehling NW, Flanders WD, et al.
Serum TSH, T(4), and thyroid antibodies inthe United States population (1988 to 1994):National Health and Nutrition ExaminationSurvey (NHANES III). J Clin Endocrinol Metab.2002;87(2):489–499.
2. Canaris GJ, Manowitz NR, Mayor G, Ridgway EC.The Colorado thyroid disease prevalence study.Arch Intern Med. 2000;160(4):526–534.
18
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
3. Billewicz WZ, Chapman RS, Crooks J, et al.Statistical methods applied to the diagnosis ofhypothyroidism. Q J Med. 1969;38(150):255–266.
4. Danese MD, Powe NR, Sawin CT, Ladenson PW.Screening for mild thyroid failure at the periodichealth examination: a decision and cost-effectivenessanalysis. JAMA. 1996;276(4):285–292.
5. Ladenson PW, Singer PA, Ain KB, et al. AmericanThyroid Association guidelines for detection ofthyroid dysfunction. Arch Intern Med.2000;160:1573–1575.
6. McDermott MT, Ridgway EC. Subclinicalhypothyroidism is mild thyroid failure and shouldbe treated. J Clin Endocrinol Metab.2001;86:4585–4590.
7. Helfand M, Redfern CC. Clinical guideline, part 2.Screening for thyroid disease: an update. AmericanCollege of Physicians. Ann Intern Med.1998;129(2):144–158.
8. Wang C, Crapo LM. The epidemiology of thyroiddisease and implications for screening. EndocrinolMetab Clin N Am. 1997;26(1):189–218.
9. Helfand M, Crapo LM. Screening for thyroiddisease. Ann Intern Med. 1990;112(11):840–849.
10. Kung AW, Janus ED. Thyroid dysfunction inambulatory elderly Chinese subjects in an area ofborderline iodine intake. Thyroid.1996;6(2):111–114.
11. Danese D. Subclinical hypothyroidism in flightpersonnel: evaluation for suitability to fly. Rev IntServ Forces Armees. 1997;70(1–3):32–36.
12. Chuang CC, Wang ST, Wang PW, Yu ML.Prevalence study of thyroid dysfunction in theelderly of Taiwan. Gerontology.1998;44(3):162–167.
13. Knudsen N, Jorgensen T, Rasmussen S,Christiansen E, Perrild H. The prevalence of thyroiddysfunction in a population with borderline iodinedeficiency. Clin Endocrinol. 1999;51(3):361–367.
14. Lindeman RD, Schade DS, LaRue A, et al.Subclinical hypothyroidism in a biethnic, urbancommunity. J Am Geriatr Soc. 1999;47(6):703–709.
15. Rivolta G, Cerutti R, Colombo R, Miano G,Dionisio P, Grossi E. Prevalence of subclinicalhypothyroidism in a population living in the Milan
metropolitan area. J Endocrinol Invest.1999;22(9):693–697.
16. Hak AE, Pols HA, Visser TJ, Drexhage HA,Hofman A, Witteman JC. Subclinicalhypothyroidism is an independent risk factor foratherosclerosis and myocardial infarction in elderlywomen: the Rotterdam Study. Ann Intern Med.2000;132(4):270–278.
17. Tunbridge WMG, Evered DC, Hall R, et al.The spectrum of thyroid disease in a community:the Whickham survey. Clin Endocrinol (Oxf ).1977;7:481–493.
18. Harris RP, Helfand M, Woolf SH, et al. Currentmethods of the U.S. Preventive Services Task Force:a review of the process. Am J Prev Med2001;20(3S):21–35(http://www.elsevier.com/locate/ajpmonline).
19. Crooks J, Murray IP, Wayne EJ. Statistical methodsapplied to the clinical diagnosis of thyrotoxicosis. QJ Med. 1959;110:211–234.
20. Eden S, Sundbeck G, Lindstedt G, et al.Screening for thyroid disease in the elderly.Serum concentrations of thyrotropin and3,5,3’-triiodothyronine in a representativepopulation of 79-year-old women and men.Compr Gerontol. 1988;2(1):40–45.
21. Chu JW, Crapo LM. The treatment of subclinicalhypothyroidism is seldom necessary. J ClinEndocrinol Metab. 2001;86(10):4591–4599.
22. Cooper DS. Clinical practice. Subclinicalhypothyroidism. N Engl J Med.2001;345(4):260–265.
23. Osman F, Gammage MD, Sheppard MC, FranklynJA. Clinical review 142: cardiac dysrhythmias andthyroid dysfunction: the hidden menace? J ClinEndocrinol Metab. 2002;87:963–967.
24. Klein I, Ojamaa K. Mechanisms of disease: thyroidhormones and the cardiovascular system. N Engl JMed. 2001;344:501–509.
25. O’Reilly DS. Thyroid function tests—time for areassessment. BMJ. 2000;320:1332–1334.
26. Stockigt JR. Case finding and screening strategiesfor thyroid dysfunction. Clin Chim Acta.2002;315(1–2):111–124.
19
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
27. Toft AD. Clinical practice. Subclinicalhyperthyroidism. N Engl J Med.2001;345(7):512–516.
28. Tunbridge WM, Vanderpump MP. Populationscreening for autoimmune thyroid disease. EndocrinolMetab Clin N Am. 2000;29(2):239–253, v.
29. Weetman AP. Hypothyroidism: screening andsubclinical disease. BMJ.1997;314(7088):1175–1178.
30. Tanis BC, Westendorp GJ, Smelt HM. Effectof thyroid substitution on hypercholesterolaemiain patients with subclinical hypothyroidism:a reanalysis of intervention studies. Clin Endocrinol.1996;44(6):643–649.
31. Sawin C, Geller A, Wolf P, et al. Low serumthyrotropin concentrations as a risk factor foratrial fibrillation in older persons. N Engl J Med.1994;331:1249–1252.
32. Auer J, Scheibner P, Mische T, Langsteger W, EberO, Eber B. Subclinical hyperthyroidism as a riskfactor for atrial fibrillation. Am Heart J.2001;142(5):838–842.
33. Benjamin EJ, Wolf PA, D’Agostino RB, SilbershatzH, Kannel WB, Levy D. Impact of atrial fibrillationon the risk of death: the Framingham Heart Study.Circulation. 1998;98(10):946–952.
34. Parle JV, Maisonneuve P, Sheppard MC, Boyle P,Franklyn JA. Prediction of all-cause andcardiovascular mortality in elderly people from onelow serum thyrotropin result: a 10-year cohortstudy. Lancet. 2001;358:861–865.
35. Attia J, Margetts P, Guyatt G. Diagnosis of thyroiddisease in hospitalized patients. A systematic review.Arch Intern Med. 1999;159:658–665.
36. Uzzan B, Campos J, Cucherat M, Nony P, BoisselJP, Perret GY. Effects on bone mass of long termtreatment with thyroid hormones: a meta-analysis.J Clin Endocrinol Metab. 1996;81:4278–4289.
37. Faber J, Galloe AM. Changes in bone mass duringprolonged subclinical hyperthyroidism due toL-thyroxine treatment: a meta-analysis. Eur JEndocrinol. 1994;130(4):350–356.
38. Bauer DC, Nevitt MC, Ettinger B, Stone K. Lowthyrotropin levels are not associated with bone lossin older women: a prospective study. J ClinEndocrinol Metab. 1997;82(9):2931–2936.
39. Bauer DC, Ettinger B, Nevitt MC, Stone KL. Riskfor fracture in women with low serum levels ofthyroid-stimulating hormone. Ann Intern Med.2001;134:561–568.
40. Gurlek A, Gedik O. Effect of endogenoussubclinical hyperthyroidism on bone metabolismand bone mineral density in premenopausal women.Thyroid. 1999;9(6):539–543.
41. Mudde AH, Reijnders FJ, Kruseman AC. Peripheralbone density in women with untreated multinodulargoitre. Clin Endocrinol. 1992;37(1):35–39.
42. Foldes J, Tarjan G, Szathmari M, Varga F, KrasznaiI, Horvath C. Bone mineral density in patients withendogenous subclinical hyperthyroidism: is thisthyroid status a risk factor for osteoporosis? ClinEndocrinol. 1993;39(5):521–527.
43. Kumeda Y, Inaba M, Tahara H, et al. Persistentincrease in bone turnover in Graves’ patients withsubclinical hyperthyroidism. J Clin EndocrinolMetab. 2000;85(11):4157–4161.
44. Sherman SI, Simons L, Ladenson PW. Clinical andsocioeconomic predispositions to complicatedthyrotoxicosis: a predictable and preventablesyndrome? Am J Med. 1996;101:192–198.
45. Parle J, Franklyn J, Cross K, Jones S, Sheppard M.Prevalence and follow-up of abnormal thyrotropin(TSH) concentrations in the elderly in the UnitedKingdom. Clin Endocrinol (Oxf ). 1991;34:77–83.
46. Sundbeck G, Eden S, Jagenburg R, Lindstedt G.Thyroid dysfunction in 85-year-old men andwomen. Influence of non-thyroidal illness and drugtreatment. Acta Endocrinol. 1991;125(5):475–486.
47. Schlote B, Schaaf L, Schmidt R, et al. Mental andphysical state in subclinical hyperthyroidism:investigations in a normal working population.Biol Psychiatry. 1992;32(1):48–56.
48. Schlote B, Nowotny B, Schaaf L, et al. Subclinicalhyperthyroidism: physical and mental state ofpatients. Eur Arch Psychiatry Clin Neurosci.1992;241(6):357–364.
49. Figge J, Leinung M, Goodman AD, et al. Theclinical evaluation of patients with subclinicalhyperthyroidism and free triiodothyronine (free T3)toxicosis. Am J Med. 1994;96(3):229–234.
50. Biondi B, Fazio S, Cuocolo A, et al. Impairedcardiac reserve and exercise capacity in patients

20
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults
receiving long-term thyrotropin suppressive therapywith levothyroxine. J Clin Endocrinol Metab.1996;81(12):4224–4228.
51. Biondi B, Fazio S, Palmieri EA, et al. Leftventricular diastolic dysfunction in patients withsubclinical hypothyroidism. J Clin EndocrinolMetab. 1999;84(6):2064–2067.
52. Biondi B, Palmieri EA, Fazio S, et al. Endogenoussubclinical hyperthyroidism affects quality of lifeand cardiac morphology and function in youngand middle-aged patients. J Clin Endocrinol Metab.2000;85(12):4701–4705.
53. Mudde AH, Houben AJ, NieuwenhuijzenKruseman AC. Bone metabolism duringanti-thyroid drug treatment of endogenoussubclinical hyperthyroidism. Clini Endocrinol.1994;41(4):421–424.
54. Faber J, Jensen IW, Petersen L, Nygaard B, HegedusL, Siersbaek-Nielsen K. Normalization of serumthyrotrophin by means of radioiodine treatment insubclinical hyperthyroidism: effect on bone loss inpostmenopausal women. Clin Endocrinol.1998;48(3):285–290.
55. Gonzalez Vilchez F, Castillo L, Pi J, Ruiz E. Cardiacmanifestations of primary hypothyroidism.Determinant factors and treatment response.[Spanish]. Rev Esp Cardiol. 1998;51(11):893–900.
56. Sgarbi, JA, Villaca F, Garbeline B, Villar HE,Romaldini JH. The effects of early antithyroidtherapy for endogenous subclinical hyperthyroidismin clinical and heart abnormalities. J Clin EndocrinolMetab. 2003;88(4):1672–1677.
57. Vanderpump MP, Tunbridge WMG, French JM,et al. The incidence of thyroid disorders in thecommunity: a twenty-year follow-up of theWhickham Survey. Clin Endocrinol (Oxf ).1995;43:55–68.
58. Nystrom E, Caidahl K, Fager G, Wikkelso C,Lundberg PA, Lindstedt G. A double-blindcross-over 12-month study of L-thyroxine treatmentof women with ‘subclinical’ hypothyroidism.Clin Endocrinol. 1988;29(1):63–75.
59. Cooper DS, Halpern R, Wood LC, Levin AA,Ridgway EC. L-Thyroxine therapy in subclinicalhypothyroidism. A double-blind, placebo-controlledtrial. Ann Intern Med. 1984;101(1):18–24.
60. Fahrenfort JJ, Wilterdink AM, van der Veen EA.Long-term residual complaints and psychosocialsequelae after remission of hyperthyroidism.Psychoneuroendocrinology. 2000;25(2):201–211.
61. Mason RL, Hunt HM, Hurxthal L. Bloodcholesterol values in hyperthyroidism andhypothyroidism. N Engl J Med.1930;203:1273–1278.
62. Johnston J, McLelland A, O’Reilly DS. Therelationship between serum cholesterol andserum thyroid hormones in male patients withsuspected hypothyroidism. Ann Clin Biochem.1993;30(Pt 3):256–259.
63. Valdemarsson S, Hansson P, Hedner P, Nilsson-EhleP. Relations between thyroid function, hepatic andlipoprotein lipase activities, and plasma lipoproteinconcentrations. Acta Endocrinol.1983;104(1):50–56.
64. Elder J, McLelland A, O’Reilly DS, Packard CJ,Series JJ, Shepherd J. The relationship betweenserum cholesterol and serum thyrotropin, thyroxine,and triiodothyronine concentrations in suspectedhypothyroidism. Ann Clin Biochem.1990;27:110–113.
65. Bauer DC, Ettinger B, Browner WS. Thyroidfunctions and serum lipids in older women: apopulation-based study. Am J Med.1998;104(6):546–551.
66. Bindels AJ, Westendorp RG, Frolich M, Seidell JC,Blokstra A, Smelt AH. The prevalence of subclinicalhypothyroidism at different total plasma cholesterollevels in middle aged men and women: a need forcase-finding? Clin Endocrinol. 1999;50(2):217–220.
67. Vanderpump MP, Tunbridge WM, French JM, et al.The development of ischemic heart disease inrelation to autoimmune thyroid disease in a 20-yearfollow-up study of an English community. Thyroid.1996;6(3):155–160.
68. Nedrebo BG, Ericsson UB, Nygard O, et al.Plasma total homocysteine levels in hyperthyroid andhypothyroid patients. Metabolism. 1998;47(1):89–93.
69. Morris MS, Bostom AG, Jacques PF, Selhub J,Rosenberg IH. Hyperhomocysteinemia andhypercholesterolemia associated with hypothyroidismin the third US National Health and NutritionExamination Survey. Atherosclerosis.2001;155(1):195–200.

70. Diekman MJ, van der Put NM, Blom HJ, TijssenJG, Wiersinga WM. Determinants of changes inplasma homocysteine in hyperthyroidism andhypothyroidism. Clin Endocrinol.2001;54(2):197–204.
71. Lien EA, Nedrebo BG, Varhaug JE, Nygard O,Aakvaag A, Ueland PM. Plasma total homocysteinelevels during short-term iatrogenic hypothyroidism. JClin Endocrinol Metab. 2000;85(3):1049–1053.
72. Catargi B, Parrot-Roulaud F, Cochet C, Ducassou D,Roger P, Tabarin A. Homocysteine, hypothyroidism,and effect of thyroid hormone replacement. Thyroid.1999;9(12):1163–1166.
73. Lindeman RD, Romero LJ, Schade DS, Wayne S,Baumgartner RN, Garry PJ. Impact of subclinicalhypothyroidism on serum total homocysteineconcentrations, the prevalence of coronary heartdisease (CHD), and CHD risk factors in theNew Mexico Elder Health Survey. Thyroid.2003;13(6):595–600.
74. Jaeschke R, Guyatt G, Gerstein H, et al. Doestreatment with L-thyroxine influence health statusin middle-aged and older adults with subclinicalhypothyroidism? J Gen Intern Med.1996;11(12):744–749.
75. Michalopoulou G, Alevizaki M, Piperingos G, et al.High serum cholesterol levels in persons with‘high-normal’ TSH levels: should one extend thedefinition of subclinical hypothyroidism? Eur JEndocrinol. 1998;138(2):141–145.
76. Meier C, Staub JJ, Roth CB, et al. TSH-controlledL-thyroxine therapy reduces cholesterol levels andclinical symptoms in subclinical hypothyroidism:a double blind, placebo-controlled trial (BaselThyroid Study). J Clin Endocrinol Metab.2001;86(10):4860–4866.
77. Pollock MA, Sturrock A, Marshall K, et al.Thyroxine treatment in patients with symptomsof hypothyroidism but thyroid function testswithin the reference range: randomised doubleblind placebo controlled crossover trial. BMJ.2001;323(7318):891–895.
78. Caraccio N, Ferrannini E, Monzani F. Lipoproteinprofile in subclinical hypothyroidism: response tolevothyroxine replacement, a randomizedplacebo-controlled trial. J Clin Endocrinol Metab.2002;87:1533–1538.
79. Kong WM, Sheikh MH, Lumb PJ, et al. A 6-monthrandomized trial of thyroxine treatment in womenwith mild subclinical hypothyroidism. Am J Med.2002;112:348–354.
80. Danese MD, Ladenson PW, Meinert CL, Powe NR.Clinical review 115: effect of thyroxine therapy onserum lipoproteins in patients with mild thyroidfailure: a quantitative review of the literature. J ClinEndocrinol Metab. 2000;85(9):2993–3001.
81. Skinner GR, Holmes D, Ahmad A, Davies A,Benitez J. Clinical response to thyroxine sodium inclinically hypothyroid but biochemically euthyroidpatients. J Nutr Environ Med. 2000;10:115–124.
82. Greenspan SL, Greenspan FS. The effect of thyroidhormone on skeletal integrity. Ann Intern Med.1999;130(9):750–758.
83. Ross DS. Bone density is not reduced duringthe short-term administration of levothyroxineto postmenopausal women with subclinicalhypothyroidism: a randomized, prospective study.Am J Med. 1993;95(4):385–388.
84. Leese GP, Jung RT, Guthrie C, Waugh N, BrowningMC. Morbidity in patients on L-thyroxine: acomparison of those with a normal TSH to thosewith a suppressed TSH. Clin Endocrinol.1992;37(6):500–503.
85. Biondi B, Palmieri EA, Lombardi G, Fazio S.Effects of subclinical thyroid dysfunction on theheart. Ann Intern Med. 2002;137:904–914.
86. Sundbeck G, Jagenburg R, Johansson P-M, Eden S,Lindstedt G. Clinical significance of a low serumthyrotropin concentration by chemiluminometricassay in 85-year-old women and men. Arch InternMed. 1991;151:549–556.
87. Sawin CT, Geller A, Kaplan MM, Bacharach P,Wilson PWF, Hershman JM. Low serum thyrotropin(thyroid-stimulating hormone) in older personswithout hyperthyroidism. Arch Intern Med.1991;151:165–168.
AHRQ Pub. No. 04-0530BJanuary 2004
21
Screening for Subclinical Thyroid Dysfunction in Non-Pregnant Adults