screening for neuroborreliosis patients with stroke fileelitis with symptomslike paraparesis,...
TRANSCRIPT
1393
Screening for Neuroborreliosis inPatients With Stroke
Susanne Hammers-Berggren, MD; Ann Grondahl, MD; Mats Karlsson, MD, PhD;Magnus von Arbin, MD, PhD; Anders Carlsson, MD; Goran Stiernstedt, MD, PhD
Background and Purpose: Borrelia burgdorferi, the etiologic agent of Lyme disease, can cause differentneurological manifestations. We studied the prevalence of Lyme neuroborreliosis in patients with stroke.
Methods: During a 1-year period, sera from patients with cerebral thrombosis or transient ischemicattack without cardioembolism were investigated for antibodies against B burgdorferi.
Results: One of 281 patients had a positive serum immunoglobulin M titer and 23 of 281 (8%) hadpositive serum immunoglobulin G titers against B burgdorferi. One of the 24 seropositive patients, with a
diagnosis of transient ischemic attack due to dysphasia, had a lymphocytic pleocytosis and intrathecalantibody production against B burgdorferi. The medical history revealed a 9-month period of general andneurological symptoms compatible with Lyme neuroborreliosis before the strokelike incidents.
Conclusions: We conclude that Lyme neuroborreliosis may imitate stroke, but screening for antibodiesagainst B burgdorferi seems to be of little value and may be replaced by a careful medical history. (Stroke.1993;24:1393-1396.)KEY WORDs * cerebral ischemia, transient * cerebral thrombosis * Lyme disease
L yme disease was first recognized in 1975 becauseof an epidemic of arthritis in the city of Lyme,Conn.1 The etiologic agent, Borrelia burgdorferi
discovered in 1982,2 is spread to humans by ticks of thegenus Ixodes. The most common clinical pictures of thedisease have been characterized. The spirochete maycause symptoms in the skin, nervous system, joints, andheart.",3-6The clinical manifestations of Lyme neuroborreliosis
are usually meningitis, meningoradiculitis, or cranialneuritis.5-8 The frequency of recovery from neuroborre-liosis is high even in patients not treated with antibiot-ics.9 In rare instances, however, neurological symptomsmay progress in untreated cases, causing encephalomy-elitis with symptoms like paraparesis, hemiparesis, dys-phasia, and ataxia.78'10-12 Strokelike manifestations ofLyme neuroborreliosis have been reported in a fewpublications.13-20 The clinical presentation in the pub-lished case reports of strokelike manifestations in neu-roborreliosis are characterized as transient ischemicattack (TIA) or cerebral infarction without cardioem-bolic source. The pathogenesis can be explained by avasculopathy with a localized vasculitis that may causefocal neurological symptoms from the central nervoussystem (CNS) with a sudden onset.'3-16,18,20 Angio-graphic changes of cerebral vessels compatible with
Received November 20, 1992; final revision received March 10,1993; accepted April 5, 1993.From the Departments of Infectious Diseases (S.H.-B., M.K.)
and Internal Medicine (A.G., M. von A., A.C.), Danderyd Hospi-tal, Danderyd, and the Department of Infectious Diseases (G.S.),Huddinge Hospital, Huddinge, Sweden.
Reprint requests to Susanne Hammers-Berggren, MD, Depart-ment of Infectious Diseases, Danderyd Hospital, 182 88 Dan-deryd, Sweden.
vasculitis have been demonstrated in a few cases ofLyme neuroborreliosis with strokelike symptoms.13-15The aim of the present study was to investigate the
prevalence of neuroborreliosis in patients with a diag-nosis of cerebral thrombosis or TIA without cardioem-bolism who lived in a B burgdorferi-endemic area.
Subjects and MethodsDuring 1990, a serum sample was drawn from all of
the 495 patients admitted to the Department of InternalMedicine, Danderyd Hospital, Stockholm, Sweden,with a diagnosis of stroke according to the InternationalClassification of Diseases, Ninth Revision (ICD-9).21The study population of 281 patients comprised 143
men and 138 women. Their ages varied from 22 to 99(median, 74) years. Included were all cases with adiagnosis of cerebral thrombosis (n= 176) or TIA with-out cardioembolism (n= 105). Cerebral thrombosis wasdefined as an acute loss of focal cerebral function, withsymptoms lasting longer than 24 hours, for which acardioembolic source and cerebral hemorrhage wereexcluded. We defined TIA as an acute loss of focalcerebral or ocular function, with symptoms lasting lessthan 24 hours. Cardioembolism was defined as atrialfibrillation, organic heart defect, cardiac infarctionwithin 3 months, cardiomyopathy, valve prosthesis, orbradytachyarrhythmia. Cerebral hemorrhage was ex-cluded by computed tomography or lumbar puncture(LP).
Patients with a diagnosis of cerebral hemorrhage,cardioembolic stroke, or unspecified stroke were ex-cluded from the present study.The serum sample drawn at admission from the study
patients (serum I) and a second serum sample drawn 6weeks later (serum II) were analyzed with an indirect
by guest on April 13, 2017
http://stroke.ahajournals.org/D
ownloaded from
1394 Stroke Vol 24, No 9 September 1993
495 stroke
281 cerebral thrombosisTIA without cardioembolism
1 pos IgM (610)
16 lgG > 500< 990
|\ 2 LP
2no pleo-cytosisor intra-thecalB.b. a.b.
SERUM H 163 94 stationary 12 2seroneg missing 1gM titer stationary missing
values IgG titers values
23 pos IgG
7 lgG > 1000
3 no LP 4 LP/ \
1 2 3 1death anticoa- no pleo- pleo-
gulant cytosis cytosistherapy or Intra- + intra-
thecal thecalB.b a.b. B.b a.b.
repeatedserumsamplesstationarylgG titers
case report
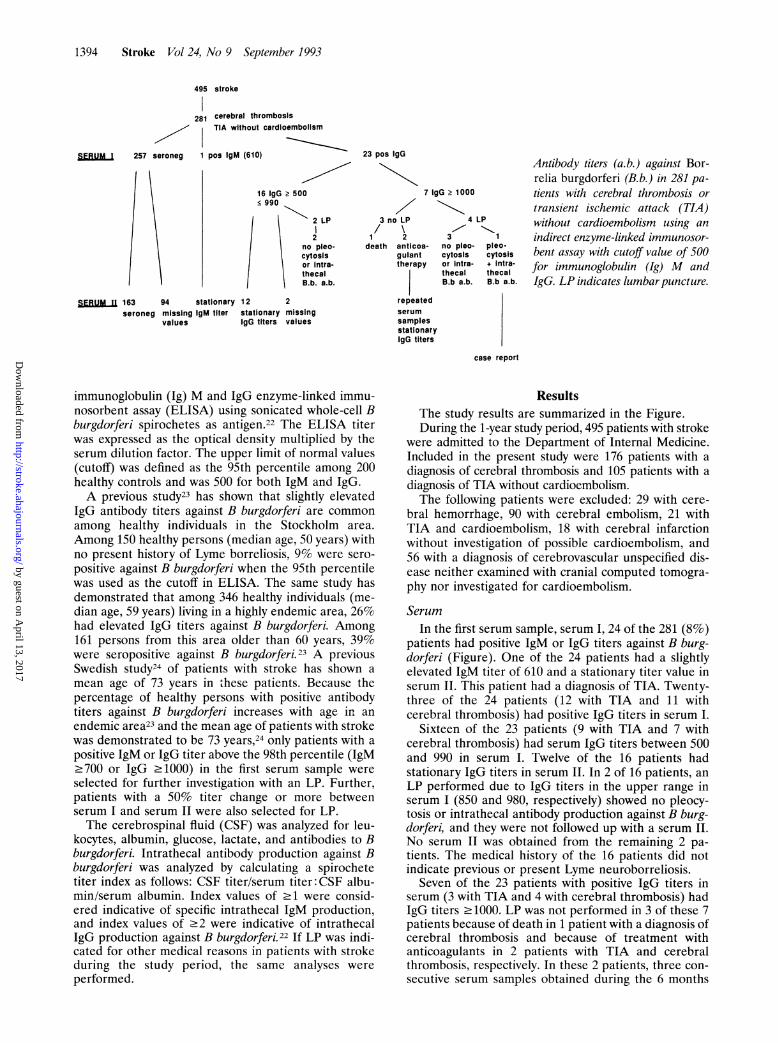
Antibody titers (a.b.) against Bor-relia burgdorferi (B.b.) in 281 pa-
tients with cerebral thrombosis or
transient ischemic attack (TIA)without cardioembolism using an
indirect enzyme-linked immunosor-bent assay with cutoff value of 500for immunoglobulin (Ig) M andIgG. LP indicates lumbarpuncture.
immunoglobulin (Ig) M and IgG enzyme-linked immu-nosorbent assay (ELISA) using sonicated whole-cell Bburgdorferi spirochetes as antigen.22 The ELISA titerwas expressed as the optical density multiplied by theserum dilution factor. The upper limit of normal values(cutoff) was defined as the 95th percentile among 200healthy controls and was 500 for both IgM and IgG.A previous study23 has shown that slightly elevated
IgG antibody titers against B burgdorferi are common
among healthy individuals in the Stockholm area.
Among 150 healthy persons (median age, 50 years) withno present history of Lyme borreliosis, 9% were sero-
positive against B burgdorferi when the 95th percentilewas used as the cutoff in ELISA. The same study hasdemonstrated that among 346 healthy individuals (me-dian age, 59 years) living in a highly endemic area, 26%had elevated IgG titers against B burgdorferi. Among161 persons from this area older than 60 years, 39%were seropositive against B burgdorferi.23 A previousSwedish study24 of patients with stroke has shown a
mean age of 73 years in these patients. Because thepercentage of healthy persons with positive antibodytiters against B burgdorferi increases with age in an
endemic area23 and the mean age of patients with strokewas demonstrated to be 73 years,24 only patients with a
positive IgM or IgG titer above the 98th percentile (IgM.700 or IgG .1000) in the first serum sample were
selected for further investigation with an LP. Further,patients with a 50% titer change or more betweenserum I and serum II were also selected for LP.The cerebrospinal fluid (CSF) was analyzed for leu-
kocytes, albumin, glucose, lactate, and antibodies to Bburgdorferi. Intrathecal antibody production against Bburgdorferi was analyzed by calculating a spirochetetiter index as follows: CSF titer/serum titer: CSF albu-min/serum albumin. Index values of .1 were consid-ered indicative of specific intrathecal IgM production,and index values of .2 were indicative of intrathecalIgG production against B burgdorferi.22 If LP was indi-cated for other medical reasons in patients with strokeduring the study period, the same analyses were
performed.
ResultsThe study results are summarized in the Figure.During the 1-year study period, 495 patients with stroke
were admitted to the Department of Internal Medicine.Included in the present study were 176 patients with a
diagnosis of cerebral thrombosis and 105 patients with a
diagnosis of TIA without cardioembolism.The following patients were excluded: 29 with cere-
bral hemorrhage, 90 with cerebral embolism, 21 withTIA and cardioembolism, 18 with cerebral infarctionwithout investigation of possible cardioembolism, and56 with a diagnosis of cerebrovascular unspecified dis-ease neither examined with cranial computed tomogra-phy nor investigated for cardioembolism.
SerumIn the first serum sample, serum I, 24 of the 281 (8%)
patients had positive IgM or IgG titers against B burg-dorferi (Figure). One of the 24 patients had a slightlyelevated IgM titer of 610 and a stationary titer value inserum II. This patient had a diagnosis of TIA. Twenty-three of the 24 patients (12 with TIA and 11 withcerebral thrombosis) had positive IgG titers in serum I.
Sixteen of the 23 patients (9 with TIA and 7 withcerebral thrombosis) had serum IgG titers between 500and 990 in serum I. Twelve of the 16 patients hadstationary IgG titers in serum II. In 2 of 16 patients, an
LP performed due to IgG titers in the upper range inserum I (850 and 980, respectively) showed no pleocy-tosis or intrathecal antibody production against B burg-dorferi, and they were not followed up with a serum II.
No serum II was obtained from the remaining 2 pa-
tients. The medical history of the 16 patients did notindicate previous or present Lyme neuroborreliosis.
Seven of the 23 patients with positive IgG titers inserum (3 with TIA and 4 with cerebral thrombosis) hadIgG titers .1000. LP was not performed in 3 of these 7patients because of death in 1 patient with a diagnosis ofcerebral thrombosis and because of treatment withanticoagulants in 2 patients with TIA and cerebralthrombosis, respectively. In these 2 patients, three con-secutive serum samples obtained during the 6 months
S U.M..IL 257 seroneg
by guest on April 13, 2017
http://stroke.ahajournals.org/D
ownloaded from

Hammrs-Brggen e alBorrelia Serology in Cerebral Thrombosis and TIA 1395
after the stroke incidents showed stationary IgG titers,and no symptoms of Lyme borreliosis appeared duringfollow-up.Serum II was obtained from 163 of the 257 patients
who were negative in serum I. No seroconversion wasseen in these samples. Serum II was not obtained fromthe remaining 94 seronegative patients, 15 ofwhom diedduring the 6-week follow-up period.
Cerebrospinal FluidIn 2 of 16 patients with IgG titers between 500 and
990 and in 4 of 7 patients with IgG titers .1000, LP wasperformed. In S of these 6 patients (1 with TIA and 4with cerebral thrombosis), LP showed no pleocytosisand the spirochete titer index did not indicate intra-thecal antibody production against B burgdorferi. TheLP from the sixth patient showed pleocytosis withlymphocytic predominance and intrathecally producedantibodies against B burgdorferi. The initial diagnosiswas TIA (see the following Case Report).LP was performed in another 3 of the 281 patients in
the study. In one, LP was performed to differentiatebetween hemorrhage and infarction. This patient wasseronegative but had an elevated IgG titer against Bburgdorferi in CSF without pleocytosis. A second LPperformed 4 weeks later verified the results of the first LP,showing intrathecally produced IgG antibodies against Bburgdorferi without pleocytosis. The serum sample fromthis patient remained negative for antibodies against Bburgdorferi. Her medical history revealed no clinical symp-toms of active or earlier neuroborreliosis, and the finaldiagnosis was that of hemorrhagic cerebral infarctionwithout cardioembolism. In a second patient, LP wasperformed because of findings of polyneuropathy simulta-neously with the hemiparesis, and in a third patient LPwas done because of high fever and hemiparesis at admis-sion. These two patients were seronegative, and the CSFshowed no pleocytosis or signs of intrathecal antibodyproduction against B burgdorferi.Case ReportA previously healthy 66-year-old woman started to
suffer from headache and pain in her neck and shoul-ders and mandibular and lumbar regions in the spring of1989. She consulted her dentist, who did not find anyexplanation for the mandibular pain. In the summer shedeveloped vertigo, balance disturbances, intense pain inher arms, and tiredness. Examination at the local hos-pital and follow-up by her general practitioner showednormal clinical status, electrocardiogram, and routineblood tests.From the end of August and during the following
autumn, the patient suffered from headache, fatigue,weight loss of 10 kg, balance disturbances, and handtremor. During December she developed blurred vision,and in January 1990 she consulted an ophthalmologist.Nothing pathological was found.On January 27 she developed acute dysphasia that
disappeared within a few hours, and no further symp-toms appeared during 2 days of observation at theDepartment of Internal Medicine of Danderyd Hospi-tal. Computed tomography of the brain, electrocardio-gram, routine blood samples, and clinical status includ-ing blood pressure were normal. The patient did notsmoke or have any other known risk factors for cardio-
vascular diseases. She was discharged with a diagnosisof TIA and included in the present study. Medicationwith 75 mg/d aspirin was initiated. Her medical historyof general and neurological symptoms since 9 monthswas not found out during the 2 days in the hospital.After discharge, serology against B burgdorferi showedan elevated IgG titer of 1075 in serum I. An LP showed74x 106 leukocytes/L (reference, .5 X 10/L); 97% lym-phocytes; protein, 1.9 (reference, .0.5 g/L); glucoseratio, 0.3 (reference, >0.5); and lactate, 3.4 mmolIL(reference, <3.0 mmol/L). The IgG titer against Bburgdorferi in CSF was 66. and the albumin ratio was0.028. Specific intrathecal IgG production against Bburgdorferi was found in CSF. Syphilis serology wasnegative.The patient was treated with 200 mg/d oral doxycy-
dline for 14 days. The headache, neck pain, handtremor, fatigue, and balance disturbances graduallydisappeared. No further symptoms of dysphasia ap-peared, and she had a complete clinical recovery atfollow-up after 1 year. The LP at follow-up was normalconcerning cells, protein, glucose ratio, and lactate. Shewas then seronegative but had persistent intrathecalantibody production against B burgdorferi.
DiscussionEarlier publications have shown that Lyme neurobor-
reliosis can cause strokelike manifestations.13 20 Thisscreening study performed during 1 year also demon-strates the possibility of neuroborreliosis imitatingstroke, but the frequency seems to be low. Among 281patients with a diagnosis of cerebral thrombosis or TIAwithout cardioembolism, only one had strokelike symp-toms due to chronic neuroborreliosis.
In the present study, we chose the 98th percentile asthe cutoff in ELISA for IgM and IgG in serum I or a50% titer change between serum I and serum II as acriterion to perform an LP. Neuroborreliosis cannot becompletely excluded in the 18 seropositive patients inwhom an LP was not performed. However, none ofthese patients had rising or declining antibody titers atfollow-up. Also, none of the patients had any clinicalsymptoms compatible with neuroborreliosis before thediagnosis of stroke. The elevated antibody titers in thesepatients were probably caused by earlier exposure to Bburgdorferi.
Previous studies have shown that patients with earlyneuroborreliosis may be seronegative (usually thosewith a disease duration of 6 weeks or less).22'25'26 Be-cause serum II was negative at the 6-week follow-up ofall patients with a negative serum I, it is unlikely thatany of these patients had an undiagnosed active neu-roborreliosis. Most case reports concerning patientswith strokelike symptoms due to neuroborreliosis havedescribed patients with disease durations of months,'3-16,19,20 as in our case report. It therefore seems unlikelythat patients with focal neurological symptoms fromCNS and a negative serology against B burgdorferi sufferfrom neuroborreliosis.The patient with a sudden onset of dysphasia and
CSF findings with pleocytosis and intrathecal antibodyproduction against B burgdorferi had a typical medicalhistory of a chronic Lyme neuroborreliosis with symp-toms of radicular pain, headache, weight loss, and soforth. Thus, we emphasize the importance of obtaining
Hammers-Berggren et al
by guest on April 13, 2017
http://stroke.ahajournals.org/D
ownloaded from

1396 Stroke Vol 24, No 9 September 1993
a careful medical history for patients with stroke, espe-cially those without a history of or risk factors forcardiovascular diseases.The possibility that our patient with dysphasia suf-
fered from two different diseases, Lyme neuroborrelio-sis and TIA due to arteriosclerosis, is unlikely becauseshe had a typical medical history of ongoing chronicLyme neuroborreliosis and CSF findings of chronicmeningitis soon after developing strokelike symptoms.She also responded promptly to antibiotic therapy anddeveloped no further symptoms of stroke posttreat-ment. Previously published case reports of neuroborre-liosis imitating stroke have also concerned youngerpatients in whom strokelike symptoms due to arterio-sclerosis would be unusual.13,15'17'18,20One patient in the present study with a diagnosis of
cerebral thrombosis had an intrathecal antibody pro-duction against B burgdorferi but no signs of CSFinflammation or clinical picture of ongoing neuroborre-liosis. A previous study12 has shown that intrathecalantibody production against B burgdorferi can persistseveral years after clinical recovery from neuroborreli-osis, and we believe that this patient had an earlierundiagnosed neuroborreliosis with a spontaneousrecovery.Computed tomography is one of the routine diagnos-
tic methods used in evaluating stroke; LP is seldomperformed. This study demonstrates the importance ofperforming LP in patients with a medical history ofdiffuse neurological and general symptoms before theonset of strokelike symptoms.Lyme neuroborreliosis may sometimes progress to a
chronic disease, with a symptom duration of months oreven years. At this stage of the disease, strokelikemanifestations may occur. However, the prevalence ofneuroborreliosis among patients with a diagnosis ofstroke seems to be low. We found only one patient withstrokelike symptoms due to neuroborreliosis among the281 patients with a diagnosis of cerebral thrombosis orTIA without cardioembolism; thus, we conclude thatscreening with serology against B burgdorferi seems tobe of little value in these patients and may be replacedby a carefully gathered medical history.
References1. Steere AC, Malawista SE, Snydman DR, Shope RE, AndimanWA, Ross MR, Seele FM. Lyme arthritis: an epidemic of oligoar-ticular arthritis in children and adults in three Connecticut com-munities. Arthritis Rheum. 1977;20:7-17.
2. Burgdorfer W, Barbour AG, Hayes SF, Benach JL, Grunwald E,Davis JP. Lyme disease: a tick borne spirochetosis? Science. 1982;216:1317-1319.
3. Steere AC, Batsford WP, Weinberg M, Alexander J, Berger HJ,Wolfson S, Malawista SE. Lyme carditis: cardiac abnormalities inLyme disease. Ann Intern Med. 1980;93:8-16.
4. Steere AC, Bartenhagen NH, Craft JE, Hutchinson GJ, NewmanJH, Rahn DW, Sigal LH, Spieler PN, Stenn KS, Malawista SE. Theearly clinical manifestations of Lyme disease. Ann Intern Med.1983;99:76-82.
5. Pachner AR, Steere AC. The triad of neurological manifestationsof Lyme disease: meningitis, cranial neuritis and radiculoneuritis.Neurology. 1985;35:47-55.
6. Stiernstedt G. Tick borne Borrelia infection in Sweden. Scand JInfect Dis. (suppl) 1985;45:1-70.
7. Stiernstedt G, Gustavsson R, Karlsson M, Svenungsson B, Skol-denberg B. Clinical manifestations and diagnosis of neuroborre-liosis. Ann N YAcad Sci. 1988;539:46-55.
8. Hansen K, Lebech A-M. The clinical and epidemiological profileof Lyme neuroborreliosis in Denmark 1985-1990: a prospectivestudy of 187 patients with B. burgdorferi specific intrathecalantibody production. Brain. 1992;115:399-423.
9. Kriger H, Reuss K, Pulz M, Rohrbach E, Pflughaupt K-W, MartinR, Mertens HG. Meningoradiculitis and encephalomyelitis due toBorrelia burgdorferi: a follow-up study of 72 patients over 27 years.J Neurol. 1989;236:322-328.
10. Ackerman R, Rehse-Kupper B, Gollmer E, Schmidt R. Chronicneurologic manifestations of erythema migrans borreliosis. AnnN YAcad Sci. 1988;539:16-23.
11. Halperin JJ, Luft BJ, Anand AK, Roque CT, Alvarez 0, VolkmanDJ, Dattwyler RJ. Lyme neuroborreliosis: central nervous systemmanifestations. Neurology. 1989;39:753-759.
12. Hammers-Berggren S, Hansen K, Lebech A-M, Karlsson M.Borrelia burgdorferi specific intrathecal antibody production inneuroborreliosis: a follow up study. Neurology. 1993;43:169-175.
13. Uldry PA, Regli F, Bogousslavsky J. Cerebral angiopathy andrecurrent strokes following Borrelia burgdorferi infection. J NeurolNeurosurg Psychiatry. 1987;50:1703-1704.
14. Midgard R, Hofstad H. Unusual manifestations of nervous systemBorrelia burgdorferi infection. Arch Neurol. 1987;44:781-783.
15. Veenendaal-Hilbers JA, Perquin WVM, Hoogland PH, DoornbosL. Basal meningovasculitis and occlusion of the basilar artery intwo cases of Borrelia burgdorferi infection. Neurology. 1988;38:1317-1319.
16. Hanny PE, Hauselmann HJ. Die Lyme-Krankenheit aus der Sichtdes Neurologen. Schweiz Med Wochenschr. 1987;117:901-915.
17. Schmutzhard E, Pohl P, Stockhammer G, Kleedorfer B, Stanek G.Unusual neurological manifestations of second-stage Lyme borre-liosis. Ann N YAcad Sci. 1988;539:495-496.
18. Kohler J, Kern U, Kasper J, Rhese-Kupper B, Thoden U. Chroniccentral nervous system involvement in Lyme borreliosis. Neurology.1988;38:863-867.
19. Olsson J-E, Zbornikova V. Neuroborreliosis simulating a pro-gressive stroke. Acta Neurol Scand. 1990;81:471-474.
20. May EF, Jabbari B. Stroke in neuroborreliosis. Stroke. 1990;21:1232-1235.
21. World Health Organization. International Classification ofDiseases,1975 Revision. Geneva, Switzerland: WHO; 1977.
22. Stiernstedt G, Granstrom M, Hederstedt B, Skoldenberg B.Diagnosis of spirochetal meningitis by enzyme-linked immuno-sorbent assay and indirect immunofluorescence assay in serum andcerebrospinal fluid. J Clin Microbiol. 1985;21:819-825.
23. Gustavsson R, Svenungsson B, Gardulf A, Stiernstedt G, ForsgrenM. Prevalence of tick-borne encephalitis and Lyme borreliosis in adefined Swedish population. Scand J Infect Dis. 1990;22:297-306.
24. von Arbin M, Britton M, de Faire U. Mortality and recurrencesduring eight years following stroke. J Intern Med. 1992;231:43-48.
25. Karlsson M, Mollegfard I, Stiernstedt G, Henriksson AM, WretlindB. Characterization of antibody response in patients with Borreliameningitis. Serodiagn Immunother Infect Dis. 1988;2:375-386.
26. Hansen K, Hindersson P, Strandberg-Pedersen N. Measurementof antibodies to the Borrelia burgdorferi flagellum improves serodi-agnosis in Lyme disease. J Clin Microbiol. 1988;26:338-346.
by guest on April 13, 2017
http://stroke.ahajournals.org/D
ownloaded from

S Hammers-Berggren, A Gröndahl, M Karlsson, M von Arbin, A Carlsson and G StiernstedtScreening for neuroborreliosis in patients with stroke.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1993 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.24.9.1393
1993;24:1393-1396Stroke.
http://stroke.ahajournals.org/content/24/9/1393World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 13, 2017
http://stroke.ahajournals.org/D
ownloaded from