scientific article endoscopy in endodontics - …€¦ · of the oral cavity was somewhat delayed...
TRANSCRIPT

26 Alpha Omegan 104:1/2, 2011
ABSTRACTA successful outcome of endodontic treatmentdepends to a large extent on accurate intraoperativefindings. Conventionally, micromirrors and micro-probes have been used for this purpose. The dentaloperating microscope (DOM) has been implementedto enhance visibility during dental procedures.However, the microscope, a sizable tool, remainsbetween operating field and the dental practitioner,making his ability to manipulate more complicated.Also, the interference of the hands and the hand-piece with the visualization of the surgical field andinaccurate observation of the endodontic instrumentsduring the procedure. Endoscopy reportedly providesthe dentist with excellent vision and ease of use.It also provides a better intraoperative visualization incomparison with micromirrors. Further developmentof endoscopy made it possible to combine magnification,light, irrigation/suction and surgical microinstrumentsin one device. This combination could lead to anadvanced root canal treatment technique.
INTRODUCTIONQuite understandably, the development of the endoscopyof the oral cavity was somewhat delayed because the oralcavity can be well observed by a naked eye. However, itwas not long before high-frequency currents foundapplication in surgery in the form of light and heat.Instrument makers combined electrical illumination withoptic devices making possible diagnosis of internal condi-tions. Julius Bruck’s “stomatoscope” was the first instru-ment to include light and Max Nitze’s instruments couldbe passed through tubes thus facilitating actual treatment.These devices were in use in the 1900s.
Since the 1960s and 70s, further development ofstomatoscopy has helped to diagnose early stages ofbuccal carcinoma,1 changes in the mouth mucosa,2
keratopathies of the mouth,3 and some other lesions. Atthat stage, the main endoscopic concern in the field of theoral cavity was not to observe but to avoid damaging teethduring esophagoscopy or gastroscopy.4 However, alreadyin the 1970s, endoscope was used in the oral cavity itselfto observe cavity forming lesions of the mouth.5
At the very end of the 20th century, endoscopyinvolves using the OrascopeTM, a modified medicalendoscope, for treatment in the oral cavity. It uses fiberoptics, making the instrument lightweight and flexible.In the past, fiber-optic imaging provided superiorergonomics but suffered from poor image quality. At thesame time, distally, the bulb incorporates a leaflet valve toseal the endoscope’s entry point into the oral cavity.
As the population expands and ages, the demand forendodontic therapy can be expected to increase as patientsseek dental options to keep their teeth for alifetime. New materials, techniques and instruments areentering the marketplace to assist dentists in providingpatients with more predictable and reliable endodontictreatment. In addition, these new systems make thedelivery of endodontic services more efficient.
Pioneering works on the use of endoscope as an aidto endodontic diagnosis appeared in the 1970s.6 Enhancedmagnification and illumination systems have raised the“awareness level” of what practitioners can visualizeand perform only in the 1990s.7,8 These almost modernendoscopes provided improved visualization of root
J. Moshonov — Associate Professor andActing Chairman, Department ofEndodontics, the Hebrew University-Hadassah School of Dental Medicine,Jerusalem, Israel; Correspondence to:Dr. Joshua (Shuki) Moshonov, Dept. ofEndodontics, The Hebrew University-Hadassah, School of Dental Medicine, P.O.B.12272, Jerusalem 91120, Israel;E-mail: [email protected]
O. Nahlieli — Professor and Chairman Oraland Maxillofacial Surgery Department,Barzilai Medical Center Ashkelon, Israel.Affiliated to Faculty of Medicine, Ben GurionUniversity of the Negev, Beer Sheva, IsraelCorrespondence to: Dr. Oded Nahlieli,Department of Oral and Maxillofacial SurgeryBarzilai Medical, Center Ashkelon 78306,Israel
Endoscopy in Endodontics Joshua Moshonov, DMD; Oded Nahlieli, DMD
Scientific Article

Endoscopy in Endodontics — Moshonov, Nahlieli 27
apicies, especially those not in the line of direct vision.They were able to illuminate and identify roots in thesinus. By allowing a magnified view of the root-endpreparation before and after placement of the fillingmaterial, any fractures or extraneous material could beidentified. These instruments finally became quite smalland readily transportable from one operative room toanother. The cost of the endoscopes was a fraction of theprice of the surgical microscope.
Conditions that were once almost impossible tomanage and had unpredictable results can now bepredictably managed simply because one has the abilityto see clear enough. The advent of endodontic microscopy9,10
and endoscopy has opened up a whole new world ofexploration. In the 1990s, only a few clinicians believed inits utility; now graduates of advanced education programsin endodontics are required to be competent inmicroscopy. With magnifications of x10 and beyond, theclinician can look for fractures or cracks and can evenevaluate the quality of a restorative procedure.
With respect to nonsurgical endodontic therapy,the microscope can facilitate the location of a hidden orcalcified canal. Subsequent to the rise of microscopycame microinstruments armamentaria. Instruments
such as micromirrors and ultrasonic tips for cleaningand removing broken instruments, micropluggersand micropaddles for repairing stripping perforations, andspecial ultrasonic tips for preparing root-end cavity arenow in the marketplace.
The introduction of endoscopy11 at the turn of themillennium involves using a fiberoptic probe to exploreinternal and external components of the root canal. Imagestaken via the probe are projected on a video monitorfor evaluation purposes. Besides aiding the clinician indiagnosis and technique, the ability to communicate to apatient what is being viewed educates the patient andthereby enhances the doctor-patient interrelationship.
The advent of orascopy as a cutting edge techniquehas changed the way endodontists visualize as well asthink about endodontics. The very beginning of the 21stcentury brought a revolution to endodontics.12 Aspractitioners begin to see and understand endodonticetiology, it will enable oral physicians to providetreatment based on visual confirmation rather thanradiographic estimates. In the future, conventionalendoscopic endodontics will be done very much likephysicians provide treatment. It will be more qualitativerather than quantitative. Dentists will use endoscopy toinstrument, irrigate, and obturate while viewing the rootcanal system in real time.13-16
EQUIPMENT DEVELOPMENTThere are rigid, flexible and semi-flexible endoscopes.The rigid endoscopes have less value in endodonticsbut can be used during apical root-end resection.17 Theflexible and semi-flexible endoscopes can be veryvaluable addition to the armamentarium.
Many microendoscopic applications in medicaltechnology and for industrial applications require smallworking diameters starting at 0.15 up to about 1 mm.These working diameters permit only about 3000 pixelsfor the image guide due to space requirements; however,the applications demand higher resolutions with morethan at least 10,000 pixels (e.g., 20,000, 30,000, 50,000).In addition, the handle of the microendoscopic probe andthe probe feed line should be configured as lightweight aspossible, which requires the image-transmitting system tohave a flexible image-guiding system to the endoscopiccamera (for video observation). Image guides with pixelcounts greater than 3000 do not allow distal probe tipswith working diameters of less than 0.5 mm.18-20
The semi-rigid endoscope combines the advantagesof flexible and rigid miniendoscopes: it has a clear view,a small diameter, stiffness and good “pushability”; henceit may be the best instrument available. Being successfullyused in salivary gland surgery,21-23 they soon found theirplace in the dental armamentarium.
Miniature endoscope for root canal treatment includes:a handpiece basically consists of three segments:
Fig. 1 A complete towerof the endoscopic system

28 Alpha Omegan 104:1/2, 2011
• A semi-flexible examination probe, to beinserted into the root canal, including anergonomic handle;
• Flexible optical fiber connections for lighttransmission (toward distal) and image trans-mission (toward proximal);
• Rigid eyepiece with a cold light source connectionand coupler for a high-quality CCD camera.
For illumination, a bundle of randomly arrangedoptical fibers is employed, which transmits the lightfrom the external cold light source to the distal tip of theendoscope, thereby utilizing the principle of total opticalreflection at the boundary with an optically thinnermedium (i.e., with a thinner index of refraction). Due tosuch small diameters, only spatially aligned optical fiberscan be used. These relay the image fiber by fiber, spot by
spot, also by way of total reflection. Thus the lightintensity and color characteristics are transmitted via eachoptical fiber.24
A correct optical image is ensured by a lens at thedistal end, and by an ocular telescope at the proximal end.Image quality is determined by the quality of the opticalfibers and by the number of pixels. In practice, thenumber of pixels possible is limited by the outer diameterof the endoscope, and by the fact that each fiber cannotbe smaller than a few micrometers, due to opticalconsiderations. The extraordinary quality of the high-purity glass used, combined with sophisticated productiontechnology, is what makes imaging using the smallest ofcross sections possible.13,14,17,25
The endodontic endoscope permits to visualize,irrigate, and clean and shape the root canal at the sametime.26,27 Optical cavity creation is crucial in every
Fig. 2 All-in-one endoscopic mobile system with camera, video, monitor,a light source, and an archive system
Fig. 3 Intraoperative view during the endoscopic root canal treatment
Fig. 4 0.9 mm diameter, 10000 pixels endoscope with wide angle lens(1200), note the flexibility due to the nitinol coating
Fig. 5 A close up magnification of the 0.9 mm endoscope tip

Endoscopy in Endodontics — Moshonov, Nahlieli 29
endoscopy procedure. In endodontic endoscopy, the bestmedium is suction formation with low pressure vacuumvia the channel and intermittent irrigation with isotonicsaline. Another option of working with the endoscope isparallel working, in this option the endoscope is in thechannel together with the instrument.
Further improvement of the endoscopic techniquethat leads to combination of several functions in onedevice permits to minimize removal of the hard tissue ofa tooth. Such minimal invasive approach is an importantelement in making the treated tooth less fragile in thefuture.27
Currently, there are four types of magnificationdevices and systems to be used in dentistry: loupes, DOM(Dental Operating Microscope), Orascopes, and modularendoscope system (microendoscopes). The range ofmagnification of the dental loupes varies from x2 to x6.The DOMs provide magnification from x4 to x25. WhileDOM is different, orascope and endoscope have somesimilarities. Orascope (Jedmed, St. Louis, MO, USA) is
used to visualize within a root canal system, and the rigidendoscope which can be connected to the computerizedsystem (of the Orascope system) is used to visualize canalaccess in conventional endodontic therapy and in surgicalendodontic treatment. Diameters of orascopes withflexible fiber optic probe tips vary from 0.7 to 1.8 mm.The Modular endoscope system (Sialotechnology Ltd.,Ashkelon, Israel) being based on modern technology ofmicroendoscopes is used in small channel organs (salivarygland ductal system, tear canals) and is designed to enablethe practitioner to work inside the root canal withmagnification and instrument access. The system includesthree parts: endoscopic compact system, optical part thatincludes ocular part and the endoscope, and handpiecewith a disposable part.
MODULAR ENDOSCOPE SYSTEMFOR ENDODONTIC TREATMENTThe Modular endoscope system (Sialotechnology Ltd.,Ashkelon, Israel) is designed and manufactured basedon the experienced gained from other surgical fields ofsmall channels, especially from salivary ductal system.It also based on modern endoscopic technology ofmagnification, blood and condensation removal, compactdigital endoscopic unit and modern sterilizationprinciples. The modular endoscope system includes all inone endoscopic compact system, optical system hand-piece with disposable cannulae and accessories.
One of the main problems when dealing withendoscopic digital illumination and archive system in den-tal clinics is the diameter and the volume of theequipment. Until few years ago such system occupied atower (Fig. 1) that included all these equipment. A rapiddevelopment in endoscopic digital and illuminationminiaturization led to compact system that fits in a dental
Fig. 6 The 2.2 mm modular endoscope with the endoscope projectionoutside the handpiece
Fig. 7 The complete handpiece with the endoscope inside – the suctionpipe is connected (the black arrow).
Fig. 8 The transillumination effect

30 Alpha Omegan 104:1/2, 2011
operatory.29 It consists of a camera, a video, a monitor, alight source, and an archive system. All the equipmentneeded for the endoscopic procedure is combined in onelaptop being a system compatible to the dental clinic. Thesystem contains all the required digital processing, themonitor and the light source which is essential for themicro-endoscopy (Figs. 2, 3). The camera features a highresolution SONY sensor or similar. The most importantoperating skill for the camera is a zooming technique.30,31
Another unique feature of the all in one system is theoption to store pictures and video clip onto a USB flashdisk. Data from the USB disk can be easily transferred tothe computer via a standard USB port.
The endoscope is flexible due to special nitinolcoating (Fig. 4). The optical part which is 0.9 mm ofdiameter, is a piece of equipment that enables the
practitioner a magnification of up to 20 with clear picturewith wide angle (Fig. 5). An additional 0.5 mm endoscopeis also available. It is unique due to its diameter whichenables a practitioner to insert the endoscope to smalldiameter canals and to observe them in detail.31
Sterilization of both endoscopes can be achieved withliquid solutions, plasma sterilization, and gas. The 0.5 mmendoscope is fully autoclavable.
For treatment procedures, the endoscope is insertedinto a special handpiece which gives the dentist optionsfor observation and treatment (Fig. 6).
The handpiece has three channels. The centralchannel contains the endoscope (0.9 mm endoscope10,000 pixels 120° lens).
The other two channels are for suction and forinstruments32 (Fig. 7). There is one type of handpiece andthere are three types of cannulae.
The connection of a suction device to the hand-piece is an important factor. The suction activity createsthe optical cavity in the endodontic endoscopy. Thehandpieces are supplied with disposable cannulae.The handpiece is fully autoclavable.
OPTICAL CAVITY IN ENDODONTIC ENDOSCOPYIn endodontic endoscopy, the best medium is suctionformation with low-pressure vacuum via the channel andintermittent irrigation with isotonic saline. The suctionpipe is connected to one of the side channels of the hand-piece. It avoids condensation, remove debris and fluidsby irrigation. When immersed in a bleeding site, theendoscope window is cleaned by continuous laminarirrigation flow to allow observation of the cavity wallsunder variable magnification. Cortical and cancellousbone structures can be differentiated in situ and pathologiesdetected during capillary bleeding.33 It permits thepractitioner to use one hand to operate the endoscopeand to suction the irrigation materials during the rootcanal procedures.
Fig. 9 (A, B) An intraoperative endoscopic view during apical surgery of the lower 1st and 2nd premolars (arrows).
Fig. 10 An endoscopic view during removal of pulpal tissue
A B
Endoscopy in Endodontics — Moshonov, Nahlieli 31
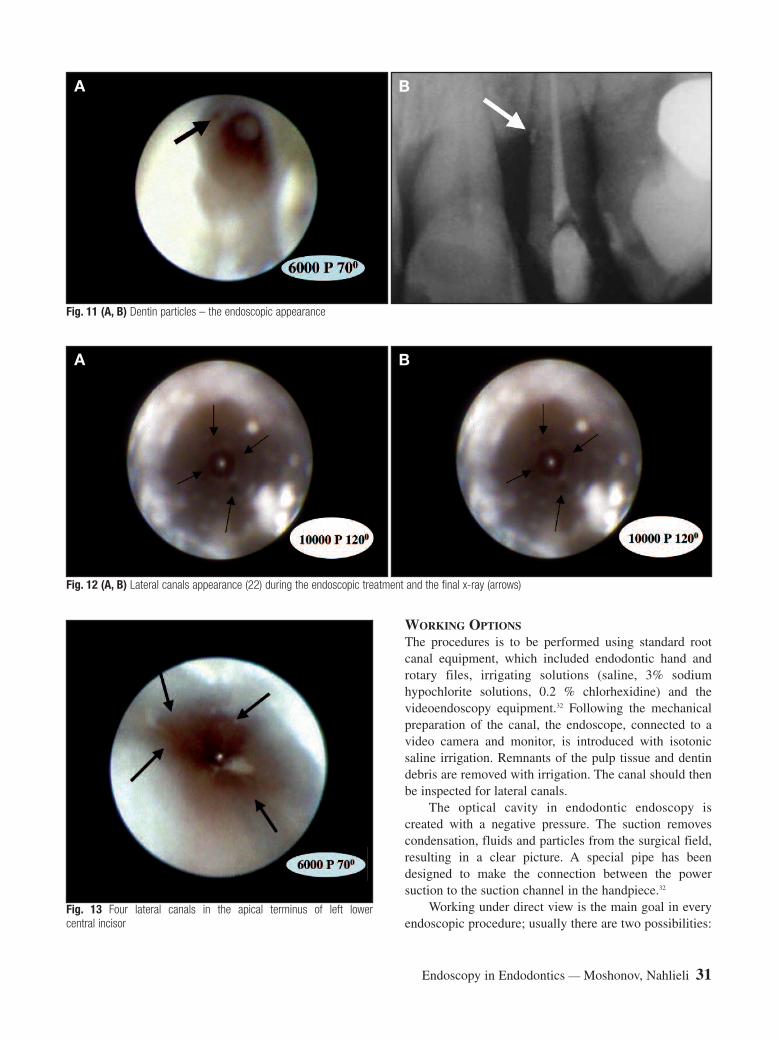
WORKING OPTIONSThe procedures is to be performed using standard rootcanal equipment, which included endodontic hand androtary files, irrigating solutions (saline, 3% sodiumhypochlorite solutions, 0.2 % chlorhexidine) and thevideoendoscopy equipment.32 Following the mechanicalpreparation of the canal, the endoscope, connected to avideo camera and monitor, is introduced with isotonicsaline irrigation. Remnants of the pulp tissue and dentindebris are removed with irrigation. The canal should thenbe inspected for lateral canals.
The optical cavity in endodontic endoscopy iscreated with a negative pressure. The suction removescondensation, fluids and particles from the surgical field,resulting in a clear picture. A special pipe has beendesigned to make the connection between the powersuction to the suction channel in the handpiece.32
Working under direct view is the main goal in everyendoscopic procedure; usually there are two possibilities:
Fig. 11 (A, B) Dentin particles – the endoscopic appearance
Fig. 12 (A, B) Lateral canals appearance (22) during the endoscopic treatment and the final x-ray (arrows)
Fig. 13 Four lateral canals in the apical terminus of left lowercentral incisor
A B
A B
32 Alpha Omegan 104:1/2, 2011
1) Working via 1 port: the optical system and thesurgical instruments operate and function fromthe device.
2) Working via 2 ports: the optical system functionfrom one device and the surgical instrumentsoperate from another side.
The same principles are implemented in endodonticendoscopy.
OTHER USES OF THE ENDOSCOPEIN ENDODONTICS PROCEDURES
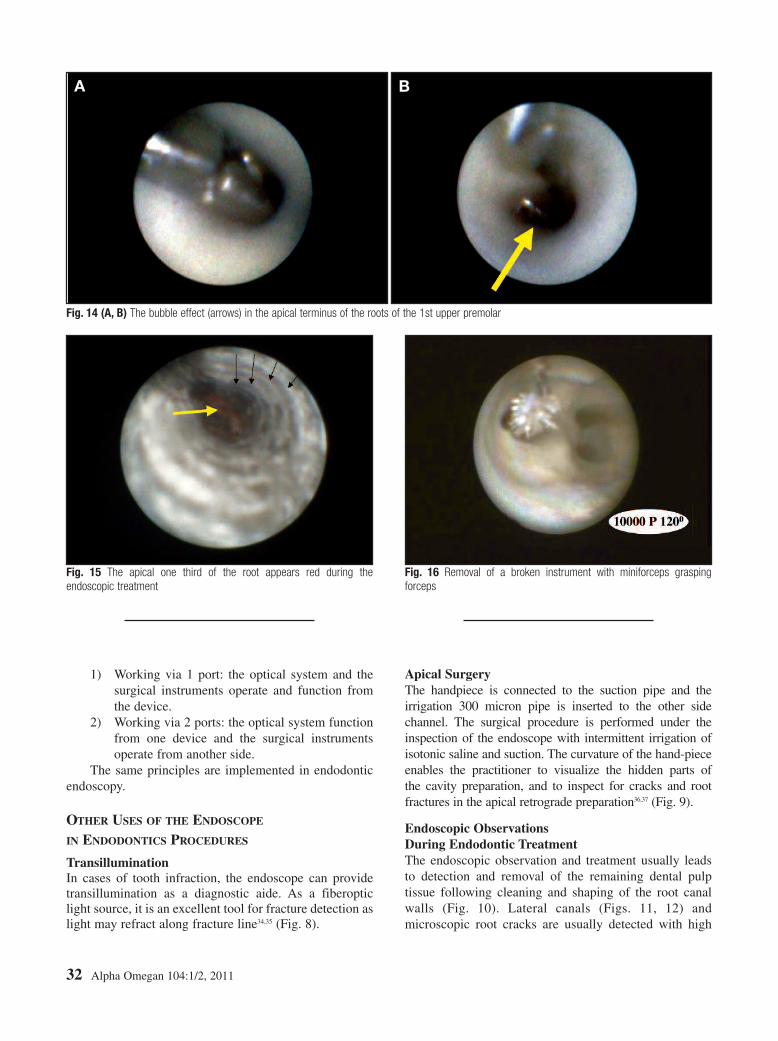
TransilluminationIn cases of tooth infraction, the endoscope can providetransillumination as a diagnostic aide. As a fiberopticlight source, it is an excellent tool for fracture detection aslight may refract along fracture line34,35 (Fig. 8).
Apical SurgeryThe handpiece is connected to the suction pipe and theirrigation 300 micron pipe is inserted to the other sidechannel. The surgical procedure is performed under theinspection of the endoscope with intermittent irrigation ofisotonic saline and suction. The curvature of the hand-pieceenables the practitioner to visualize the hidden parts ofthe cavity preparation, and to inspect for cracks and rootfractures in the apical retrograde preparation36,37 (Fig. 9).
Endoscopic ObservationsDuring Endodontic TreatmentThe endoscopic observation and treatment usually leadsto detection and removal of the remaining dental pulptissue following cleaning and shaping of the root canalwalls (Fig. 10). Lateral canals (Figs. 11, 12) andmicroscopic root cracks are usually detected with high
Fig. 14 (A, B) The bubble effect (arrows) in the apical terminus of the roots of the 1st upper premolar
Fig. 15 The apical one third of the root appears red during theendoscopic treatment
Fig. 16 Removal of a broken instrument with miniforceps graspingforceps
A B

Endoscopy in Endodontics — Moshonov, Nahlieli 33
accuracy, providing better intraoperative judgment andfacilitating adequate treatment.38 Another observationduring treatment might be a color change in the canal. Theapical one third of the root appears red, probably becauseof the presence of the vascularized tissue (periodontalligament) and the transillumination effect (Fig. 13). Thefiles (hand and engine driven) and microinstruments helpto remove debris, an old obturation material, and brokeninstruments and posts (Figs. 14, 15). Irrigation andsuction are carried out via the working channels underdirect vision and improves the cleaning of the root canal32
(Figs. 16, 17, 18).
FUTURE DEVELOPMENTSIn the 21st century, as long as basic principles ofendodontic therapy are followed, the equipment and toolsavailable to clinicians increase the chances for a highersuccess rate. New materials, techniques and instrumentsare entering the marketplace to assist dentists in providingpatients with more predictable and reliable endodontictreatment.32,39 In addition, these new systems make thedelivery of endodontic services more efficient. Theintroduction of microsurgical principles in endodonticsinvolving techniques used for canal treatment hastremendously improved visualization of the operatingfield. At the same time, the advent of microsurgicalinstruments and dental operating microscope has broughtabout advantages in root canal instrumentation and theapplication of root canal filling materials. This developmenthas facilitated the use of cleaning and shapinginstruments, as well as root canal filling techniques.
This is not implying that endodontic treatment hasbecome easier; however, better tools and technology havemade it more predictable and challenge us to take on awider variety of complex cases. Diagnosis, in fact, hasbecome more challenging. Overall, case management ismore complex as geriatric patients and those who aremedically compromised are more inclined to seektreatment to save their teeth.
Further improvement of the endoscopic techniqueinvolving a combination of several functions in one devicepermits removal of minimal tooth structure. Such aminimally invasive approach is an important element inmaking the treated tooth less fragile in the future. �
REFERENCES1. Popescu V, Sturza M. Stomatoscopy in the diagnosis of early stages of buccal
carcinoma. Stomatologia (Bucur) 1969; 16(2): 153-164.2. Morgenroth K, Morgenroth K Jr. Comparative stomatoscopic and electron
microscopic scanning studies of changes in the mouth mucosa. Dtsch ZahnarztlZ 1970; 25(2): 199-207.
3. Popescu V, Sturza M. Value of stomatoscopy in the study of keratopathies ofthe mouth. Rev Stomatol Chir Maxillofac 1971; 72(2): 238-242.
4. Jones RF. Summary of hazards of endoscopy. Proc R Soc Med 1976; 69(9):670-672.
5. Onishi M. Endoscopic observation of cavity forming lesions of the mouth.Kokubyo Gakkai Zasshi 1977; 44(1): 72-73.
6. Detsch SG, Cunningham WT, Langloss JM. Endoscopy as an aid toendodontic diagnosis. J Endod 1979; 5(2): 60-62.
7. Held SA, Kao YH, Wells DW. Endoscope: an endodontic application. J Endod1996; 22(6): 327-329.
8. Bahcall JK, DiFiore PM, Poulakidas TK. An endoscopic technique forendodontic surgery. J Endod 1999; 25(2): 132-135.
9. Bahcall JK, Barss JT. Orascopy: a vision for the new millennium, Part 2. DentToday 1999; 18(9): 82-85.
10. Mines P, Loushine RJ, West LA, Liewehr FR, Zadinsky JR. Use of themicroscope in endodontics: a report based on a questionnaire. J Endod 1999;25:755-758.
11. Bahcall JK, DiFiore PM, Poulakidas TK. An endoscopic technique forendodontic surgery. J Endod 1999; 25: 132-135.
12. Bahcall JK, Barss JT. Orascopic endodontics: changing the way we “think”about endodontics in the 21st century. Dent Today 2000; 19(5): 50-55.
Fig. 17 An endoscopic view following post removal for root canalretreatment (upper 1st bicuspid). Note the spiral imprint (black arrow) dueto the post configuration and the remain of the gutta percha (yellowarrow) in the apical part
Fig. 18 An endoscopic view of the micro-brush inside the distal rootof the tooth 36

About the Authors
Prof. Joshua Moshonov is a Clinical Associate Professor and Acting Chairman of the Department of Endodontics at the HebrewUniversity – Hadassah Faculty of Dental Medicine, Jerusalem, Israel. He received his DMD degree in 1979 and completed theEndodontic specialty program in 1989 both at the Hebrew University – Hadassah Faculty of Dental Medicine. He is Past Presidentof the Israel Endodontic Society. He is a member of the national board of Endodontics and was a member of the nationalexaminer committee in dentistry of the ministry of health of the state of Israel. Prof. Moshonov was also the Chairman of theJerusalem Branch of the Israel Dental Association, Chairman of the Israel Specialty Board of Endodontics, and now he is amember of the Scientific Council of the Israel Dental Association.
As a faculty member of the Hebrew University – Hadassah Faculty of Dental Medicine since 1988, Prof. Moshonov was formany years the director of the undergraduate endodontic program. He is also a member of the editorial board of “Refuat HapeVehashinaim,” the Journal of the Israel Dental Association and member of the editorial board of the British journal “EndodonticPractice.”
Prof. Moshonov has authored and co-authored many scientific articles and is invited to lectures both nationally and internationally.His current research focuses on the application of new technologies in dentistry in general and endodontics in particular and
laser applications in dentistry. Recently, together with Prof. Oded Nahlieli from Barzilai Hospital, Prof. Moshonov has developed anendoscope for dental treatment that is used especially for implant dentistry and endodontics.
He maintains a private practice limited to endodontics in Tel Aviv, Israel.
Prof. Oded Nahlieli graduated the Hebrew University Hadassah School of Dental medicine in Jerusalem. He completed his Oraland Maxillofacial Surgery residency in Israel; residency during 1988-1989, in the Oral and Maxillofacial Surgery Department inMassachusetts General Hospital Boston USA.
Prof. Nahlieli is the chairman of the Department of Oral and Maxillofacial Surgery at the Barzilai Medical Center Ashkelon, Israel.Since 1993 Dr. Nahlieli began developing the practice of Endoscopy of the salivary glands (Sialoendoscopy) and was one of the
pioneers in the field. He has extensive experience in salivary gland endoscopy having performed more than 2500 sialoendoscopies. He developed a series of endoscopes techniques and specific equipments for minimal invasive procedures in dentistry and
|medicine. He has lectured extensively on his specialty in Europe, Middle East and North America. Prof Oded Nahlieli has written more than 100 articles, 10 chapters, one book and obtained 25 patents, published in the
international literature. His articles on Sialoendoscopy are considered keystones in the modern management of salivary glandsinflammatory disorders.
34 Alpha Omegan 104:1/2, 2011
13. von Arx T, Hunenbart S, Buser D. Endoscope- and video-assisted endodonticsurgery. Quintessence Int 2002; 33(4): 255-259.
14. von Arx T, Hunenbart S, Buser D. Endoscopy in endodontic surgery. SchweizMonatsschr Zahnmed 2001; 111(11): 1302-1310.
15. Bahcall JK, Barss JT. Endodontic therapy using orascopic visualization. Anupdate. Dent Today 2003; 22(11): 95-98.
16. Nasseh AA. Technology in the endodontic office. Compend Contin Educ Dent2005; 26(5): 350, 352, 354-355.
17. von Arx T. Frequency and type of canal isthmuses in first molars detected byendoscopic inspection during periradicular surgery. Int Endod J 2005; 38(3):160-168.
18. Kautzky M, Susani M, Franz P, Zrunek M. Flexible fiberoptic endoscopy andlaser surgery in obliterated cochleas: human temporal bone studies. Lasers SurgMed 1996; 18(3): 271-277.
19. Hill DL, Langsaeter LA, Poynter-Smith PN, Emery CL et al. Feasibility studyof magnetic resonance imaging-guided intranasal flexible microendoscopy.Comput Aided Surg 1997; 2(5): 264-275.
20. Thiberville L, Salaün M, Lachkar S, Dominique S, et al. Confocalfluorescence endomicroscopy of the human airways. Proc Am Thorac Soc2009; 6(5): 444-449.
21. Nahlieli O, Neder A, Baruchin AM. Salivary gland endoscopy: a new techniquefor diagnosis and treatment of sialolithiasis. J Oral Maxillofac Surg 1994;52(12): 1240-1242.
22. Nahlieli O, Baruchin AM. Sialoendoscopy: three years’ experience as adiagnostic and treatment modality. J Oral Maxillofac Surg 1997; 55(9):912-918.
23. Marchal F, Becker M, Dulguerov P, Lehmann W. Interventional sialendoscopy:a targeted problem and its solution. Laryngoscope 2000; 110(2 Pt 1): 318.
24. Erokhin V, Kumar Ram M, Yavuz O. The new frontiers of organic andcomposite nanotechnology. Oxford: Elsevier, 2008: 3-18, 121.
25. Ailor JE Jr. Managing incomplete tooth fractures. J Am Dent Assoc 2000;131(8): 1168-1174.
26. Taschieri S, Del Fabbro M. Endoscopic endodontic microsurgery: 2-yearevaluation of healing and functionality. Braz Oral Res 2009; 23(1): 23-30.
27. Del Fabbro M, Taschieri S, Lodi G, Banfi G, Weinstein RL. Magnificationdevices for endodontic therapy. Cochrane Database Syst Rev 2009; 8(3):CD005969. 28. Pitiot A, Delingette H, Thompson PM. Automated imagesegmentation: issues and applications. In: Leondes CT, ed. Medical imagingsystems technology: methods in general anatomy (Medical Imaging SystemsTechnology) (v. 3). Singapore – London: World Scientific PublishingCompany, 2005; 195-244.
29. Nogueira JF Jr, Stamm AC, Lyra M. Novel compact laptop-based image-guidance system: preliminary study. Laryngoscope 2009; 119(3): 576-579.
30. Yang L, Peng C, Wu H, Zhao D, Zhang J. Development of a video imagesystem for wireless capsule endoscopes based on DSP. Sheng Wu Yi Xue GongCheng Xue Za Zhi 2008; 25(1): 7-11.
31. Nishikawa A, Nakagoe H, Taniguchi K, Yamada Y, et al. How does the cameraassistant decide the zooming ratio of laparoscopic images? Analysis andimplementation. Med Image Comput Comput Assist Interv Int Conf MedImage Comput Comput Assist Interv 2008; 11(Pt 2): 611-618.
32. Moshonov J, Michaeli E, Nahlieli O. Endoscopic root canal treatment.Quintessence Int 2009; 40:739-744.
33. Engelke WG. In situ examination of implant sites with support immersionendoscopy. Int J Oral Maxillofac Implants 2002; 17(5): 703-706.
34. Brynjulfsen A, Fristad I, Grevstad T, Hals-Kvinnsland I. Incompletely fracturedteeth associated with diffuse longstanding orofacial pain: diagnosis andtreatment outcome. Int Endod J 2002; 35(5): 461-466.
35. Filippi A, Meier ML, Lambrecht JT. Periradicular surgery with endoscopy: aclinical prospective study. Schweiz Monatsschr Zahnmed 2006; 116(1): 12-17.
36. Taschieri S, Rosano G, Weinstein T, Del Fabbro M. Endoscopic managementof a lateral root lesion. A case report. Minerva Stomatol 2008; 57(11-12):587-595.
37. Taschieri S, Rosano G, Francetti L, Agliardi E, Del Fabbro M. A modifiedtechnique for using the endoscope in periradicular surgery. A case report.Minerva Stomatol 2008; 57(7-8): 359-367.
38. Walton R, Rivera E. Cleaning and shaping 206-238. In: Walton R, TorabinejadM, eds. Principles and practice of endodontics. 3rd ed. 2002.
39. Keiser K. Magnification options in endodontics: a comparison of the operatingmicroscope and the endoscope. Tex Dent J 2007; 124(2): 208-216.