scar revision & camouflage · scar revision & camouflage michael e. decherd, md ......
TRANSCRIPT

Scar Revision & Camouflage
Michael E. Decherd, MD
Faculty Advisor: Karen H. Calhoun, MD
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
April 24, 2002
2
Introduction
• Scarring
– Dorland’s: a “mark remaining after the healing of a wound or other
morbid process”
• Mechanism
– Trauma
– Surgical
• Location & orientation
– Cosmesis
– Function
Scarring is a result of the normal healing process. Many factors influence
the final appearance of this process including the mechanism of injury,
location of the injury, the initial management of the wound and any
complications that occur during the healing process.

3
Ideal Scar
• Flat
• Narrow
• Good color match
• Parallel to or within skin crease
The ideal scar is level with the surrounding tissues, has a favorable color match, is
narrow, parallel to or lying within a RSTL, and sinuous without long straight
unbroken lines. Not all scars are able to be improved by revision techniques and
those that are already optimal may be made much worse if a poorly thought out
attempt at revision is undertaken. Patients should be carefully counseled to assure
that their expectations are realistic – if they expect the scar to be completely gone -
I.e invisible – they need education or they are likely to be displeased with the
outcome.
4
Strategies • Prevention
– Incision planning
• Relaxed skin tension lines
• Facial subunits
– Careful surgical technique
– Postop
• Wound care
• Steroid injection
• Antitension taping
• Excision
– Irregularization
– Reorientation
• Camouflage
– Cosmetics
– Dermabrasion
We will discuss several strategies that assist the surgeon faced with treating a previously formed scar, treating a
wound that is likely to scar, or when contemplating inducing a wound on the face that is likely to scar. The most
basic of these principles is careful planning of surgical incisions to minimize the cosmetic impact. Secondly,
appropriate care of a traumatic wound or a post operative wound may lessen the scar formation. When a
cosmetically unpleasant scar results and is mature, several options are available to render the scar less noticeable.
While not elegant or involved, consultation with a cosmetics specialist may be all that is needed to achieve a
pleasing result, and should not be forgotten as an option in the camouflage of facial scars.

5
Timing
• Traditionally 6 to 12 months
• Perhaps earlier for those perpendicular to
tension lines
• Dermabrasion 6 to 9 weeks
– High fibroblast activity
The timing of scar revision has traditionally been after the scar has had a period of maturation of 6 to 12
months. This allows time for scar maturation and better defines what needs to be accomplished in the revision.
Patients often need to be counseled and reassured during this waiting period that the outcome is likely to be
improved if appropriate time is taken for the scar to mature and the proper treatment selected.
Many would argue that scars lying outside RSTLs and especially those perpendicular to RSTLs are likely to
have a poor cosmetic outcome and early revision and reorientation can be considered.
Dermabrasion is frequently performed at 6-9 weeks post injury utilizing the high fibroblastic activity in the
wound at that time to aid in favorable wound healing.
6
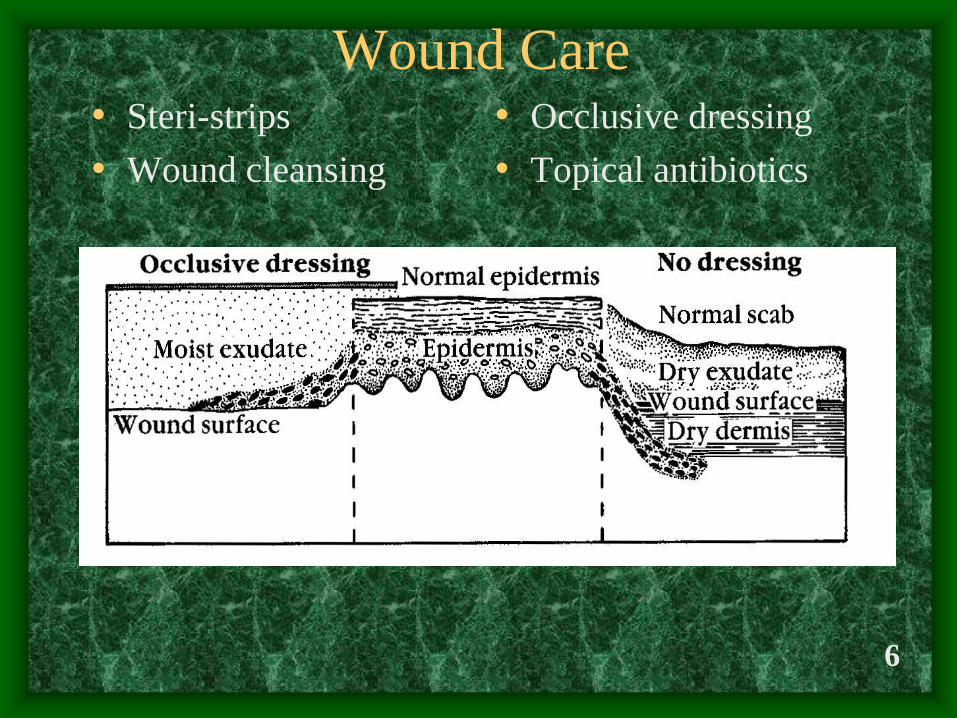
Wound Care • Steri-strips
• Wound cleansing
• Occlusive dressing
• Topical antibiotics

• Steri-strips add strength to the wound during the critical time of deposition of collagen by fibroblasts in the first several days after wounding. Initially there is no inherent
strength to the wound due to the absence of collagen extending across the wound. Suture material provides some apposition of the wound edges, but only at the site of each
suture. Between sutures, there may be microscopic dehiscences of the wounds edges, thereby delaying healing and predisposing to a wide scar. Steri-strips applied to the
wound serve to minimize this. Appropriately applied Steri-strips remove tension from the wound by sticking and pulling the skin distal to the wound margins. In general, they
rarely last longer than 3-4 days at which point they should be removed and re-applied. When removing the strip, the two ends should be grasped and both sides removed
toward the wound to avoid distracting the edges.
• The wound should be cleansed in order to prevent the formation of crusts. The formation of crusts allows the colonization of accumulated serum or blood with bacteria thereby
putting the wound at risk for infection. Antiseptics have not been shown to have any therapeutic benefit on the treatment of either clean or contaminated wounds. Anti-septics
were designed to be used on intact skin and their effectiveness in this regard cannot be translated into effectiveness when used on open wounds. In fact, many are quite
detrimental in the wound healing process causing an increase in the intensity and duration of the inflammatory response, gross and histologic evidence of tissue necrosis, and
endothelial damage and thrombosis in an animal model. Special mention should be made of H2O2, a cleanser commonly used on wounds to reduce crusting and espoused
by many authors. It is falsely believed that the effervescent bubbling of the solution is evidence of its antibacterial activity. It has been shown however, that its antibacterial
potency is minimal at best. In addition, it can cause disruption of re-epithelialization by producing bullae under the new epithelium. It is also interesting that even a dilute 1:100
solution of H2O2 may be toxic to fibroblasts and impairs the microcirculation of wounds. It has been shown to delay wound healing in both humans and animals. ( Branemark
etal, J Bone Joint Surg, 49A:48, 1967). Given these adverse effects, it is perhaps most prudent to have the patient cleanse the wound with either sterile saline for plain tap
water to remove any crusts that form.
• The plane of migration of epithelial cells from the wound margin is determined in part by the water content of the wound bed. The epithelium seeks a plane of migration with a
critical humidity. Open, dessicated wounds epithelialize much more slowly than moist, occluded or semi-occluded wounds. As demonstrated in this figure, migrating
epidermal cells in air-exposed wounds moved beneath the crust scab and devitalized dermis to seek a plane with a critical moisture level. This route was a circuitous one
taken with significant metabolic expenditure by the keratinocyte and consequently delayed wound re-epithelialization. In constrast, wounds that were kept moist had a level of
adequate tissue humidity essentially at the wound base, thereby allowing for a more direct and speedier route of epithelialization. The practical message is that occlusive or
semi-occlusive dressings optimally promote re-epithelialization.
• The application of an occlusive dressing is useful, but may be difficult with many wounds of the head or neck. In addition, the dressing is only able to stay in place for several
days due to the need for wound care. In our warm climate, where one cannot help but perspire approximately 11.5 months out of the year, these bodily secretions may
accumulate under the dressing and along the wound edges to become an ideal environment for skin flora. Even if invasive infection is not the result, an increase in wound
inflammation may result.
• A good alternative is the “open” technique of wound care. The wound is covered with a generous amount of antibiotic ointment. This provides not only a moist wound
environment, but also a barrier to dust and dirt contamination, as well as protecting the wound from contamination with skin oils and bacteria. The antibiotic ointment also
provides some effect at the point at which the suture material pierces the skin, reducing the likelihood of the formation of stitch abscesses. For best effect, the antibiotic
ointment should be replaced every 3-4 hours after a gentle cleansing and crust removal using sterile saline or tap water.
• It may be difficult to employ both Steri-strips and antibiotic dressings. Many authors favor the open antibiotic dressing for fresh, primary wounds and steri-strips for scar
revision or reconstructive wounds. 7

8
Wound Healing
• Inflammatory phase – hours
• Proliferative phase – days
• Remodeling phase – months

9
Wound Healing

10
It is generally agreed that there are at least 3 phases of wound healing: inflammatory or exudative phase,
proliferative or granulation phase and wound contraction or remodeling phase.
Inflammatory or Exudative Phase – 0-3 days (begins immediately upon injury) disruption of blood vessels -
influx of blood, serum proteins, platelets and clotting factors as well as collagen platelets initiate coagulation and
release substances such as growth factors,fibrinogen, and fibronectin, all of which promote cell migration into the
wound. 5-6 hours – neutrophils – fight bacterial contamination 24-48 hours – monocytes or macrophages –
phagocytose bacteria and neutrophils releasing platelet derived growth factor and transforming growth factor beta
needed to initiate granulation tissue formation
Proliferative or Granulation Phase – 3-4 days to 30 days post injury rapid increase in fibroblast and epithelial
cell mitoses, and increase in synthesis of extracellular collagen and proteoglycans re-epithelialization begins
within hours but intensifies with rapid mitosis and new epithelial cells migrate along a bridge of fibrin when cells
contact one another, migration ceases due to contact inhibition and keratinization begins most sutured wounds
have epithelial coverage by 4 days post-injury angiogenesis follows fibroblast proliferation (begins at about 48
hours post injury) granulation tissue made up of fibroblasts, macrophages and new capillaries is the result
collagen synthesis extremely active at 5-7 days
Wound Contraction (Matrix Formation) or Remodeling Phase – begins approx 4 weeks and continues for 6-
18 months
characterized by reduction in fibroblasts, macrophages and wound vascularity Fibronectin eliminated as type I
collagen accumulates later type III collagen forms with fibronectin myofibroblasts cause wound contraction (0.6
to 0.75mm per day) scar size is a function of wound tension, patient age, O2 supply to the area –mechanical stress
promotes collagen synthesis and deposition leading to hypertrophic scarring hypoxia stimulates collagen
deposition as well Contracts 0.6-0.75 mm/day

11
Cellular Activity in Wound
Healing

12
Wound Healing

13
Hypertrophic Scar / Keloid
Hypertrophic scar Keloid
Can regress Does not regress
Oriented collagen Random eosinophilic
collagen
Confined to wound Not confined
Scant mucin Mucinous stroma
No myofibroblasts Myofibroblasts

14
Hypertrophic Scarring

15
Keloid
• Pressure can lead to resolution

16
Keloids

17
Keloids
• Described 1700 BC
• Chele – Greek for crablike
• More common in darker-skinned persons
• Most common age 10-30
• Usually after trauma
• Usually within a year

18
Keloids – Treatment
• Steroids
• Excision – Laser vs. cold
• Pressure
• Interferon
• Low-dose radiation
• Silicone Gel sheeting (hydrocolloid dressing)
• Combination

19
Patient Encounter
• Common reaction to scar is ANGER
• Counseling regarding expectations
• Counseling regarding timecourse
– Cannot rush healing
– Possible touch-ups later
• Photodocumentation
– Consistent exposure and lighting

20
Scar Photography
Flat Lighting Side Lighting

21
Scar Revision?

22
Good Candidate Scars
• Longer than 20 mm
• Wider than 1-2 mm
• Disturbing function
• Poor match to surrounding tissue
– Color
– Depth
• Against RSTLs

23
Hidden Incisions
• Hide incision in orifice
– Transconjunctival, sublabial, intranasal, etc.
• Hide incision in hair
– Bevel edges, be aware of future balding
• Hide behind anatomic prominence
– Ex: retroauricular, submental
• Hide in junction of aesthetic subunits
• Hide in Relaxed Skin Tension Lines (RSTLs)

24
Relaxed Skin Tension Lines

25
Lines of Maximum Extensibility
• Lines of Maximum
Extensibility (LMEs)
are perpendicular to
RSTLs

26
Relaxed Skin Tension Lines
• Somewhat mirrored by lines of aging

27
Relaxed Skin Tension Lines

28
Facial Subunits
Incisions may be camouflaged
primarily by placing them at
the junction of aesthetic
subunits of the face. These
occur where there is a contour
change on the face or at the
junction of non-hair bearing
and hair-bearing skin. The
shadows that are cast from the
changes in contour tend to
hide the scars well.

29
Facial Subunits – Example

30
Surgical Technique
• Adequate anesthesia
• Proper instruments
• Suture materials
• Closure of dead space
• Careful handling of tissue
• Precise closure of dermal layer

31
Technique
• Perpendicular
incision – unless
in hair-bearing
area

32
Technique
Improper Proper – everts

33
Depressed Scars
• Excision
• Injection
– Fat
– Collagen
• Bovine
• Human
Collagen allergy

34
Surgical Options • Simple excision (fusiform)
– Best for small scars that are wide or depressed
– Ex: trach scar
– Angle needs to be less than 30 degrees
• Serial excision
– Based upon ability of skin to stretch over time
– Can move scar to better anatomic location
– Also good for reducing grafted areas
– Alternatively, tissue expansion
• Shave – best for small raised scars

35
Serial Excision
• Scar could be moved
via serial excision to
hairline

36
Intramarginal Excision
• Hypertrophic scars
– Incisions within scar may heal better
– May be better than total excision

37
Intramarginal Excision

38
Z-Plasty
• Lengthens
• Reorients The well-known Z-plasty technique of scar manipulation both lengthens
and reorients the scar. It is especially useful in dealing with scars that
cross important RSTLs, distort anatomic features, or create webs or bands
across cncavities. By spreading the forces acting on a given point over
several directions, the Z-plasty helps to minimize distortions created by the
strong contractile forces during wound healing. Thus, the Z-plasty may
perform a cosmetic role by effacing a scar and may effect a functional
improvement by the lengthening it provides.
The classic Z-plasty represented in this diagram has two 60 degree angles
and three limbs of equal length. Undermining the two flaps created by
incising these limbs and transposing them theoretically increases the
length of the scar by 75%. The actual amount of lengthening is critically
dependent on the elasticity and availability of the surrounding skin. In
addition, increases in length from the rotated Z-plasty triangles vary
depending on the angle between the central and peripheral limbs. Angles
of less than 30 degrees may result in flap tip necrosis, those greater than 75
degrees in redundant standing-cutaneous cones.
Every Z-plasty has four different possible designs for the lateral limbs.
The correctly designed Z-plasty uses lateral limbs that parallel the
RSTL of interest. In addition, the ends of the lateral limbs must lie
precisely in the line where the new central limb will be placed. The angles
can be varied and made unequal to ensure that the limbs will fall in the
desired position. Multiple Z-plasties may be used in tandem around the
curve of a trapdoor deformity, allowing interdigitation of flap and
surrounding skin and thus effecting excellent scar camouflage. Less lateral
distortion is obtained by using multiple Z-plasties instead of a single,
larger Z-plasty centered about the same scar. This is important around
critical areas such as the medial canthus, where millimeter changes can
have significant functional and cosmetic implications.
The surgeon must be ever aware and weigh the versatility and benefits of
the Z-plasty against the fact that it requires two extra incisions, and
subsequent scars, to correct a single scar.

39
Z-Plasty
• Keep angle > 30 degrees to avoid tip necrosis

40
Z-Plasty

41
Z-Plasty
• Angles greater
than 60 degrees
can be broken
into multiple
flaps

42
Z-Plasty

43
Z-Plasty

44
Z-Plasty
• Angle should be no less than 30 degrees
• Optimally between 45 and 60 degrees
• Long scars can do with a series of Z-plasties
• Careful technique to avoid tip necrosis

45
M-plasty
• With a large standing cone, reduces amount
of healthy skin excised
– Ex: Lip, forehead flap

46
M-plasty

47
M-Plasty
• Can advance
tip with
closure

48
W-Plasty
• Eye is drawn to straight lines
• Straight scars more likely to cause
contracture
• W-plasty is regularly irregular
• Maximum segment length 6mm
• No. 11 blade helpful

49
W-plasty

50
W-Plasty
• Try to place segments in RSTLs

51
W-Plasty
• Helpful in
curved scars

52
W-Plasty
• Can use small VY segment to gain length

53
W-Plasty
• Correcting a design error
54
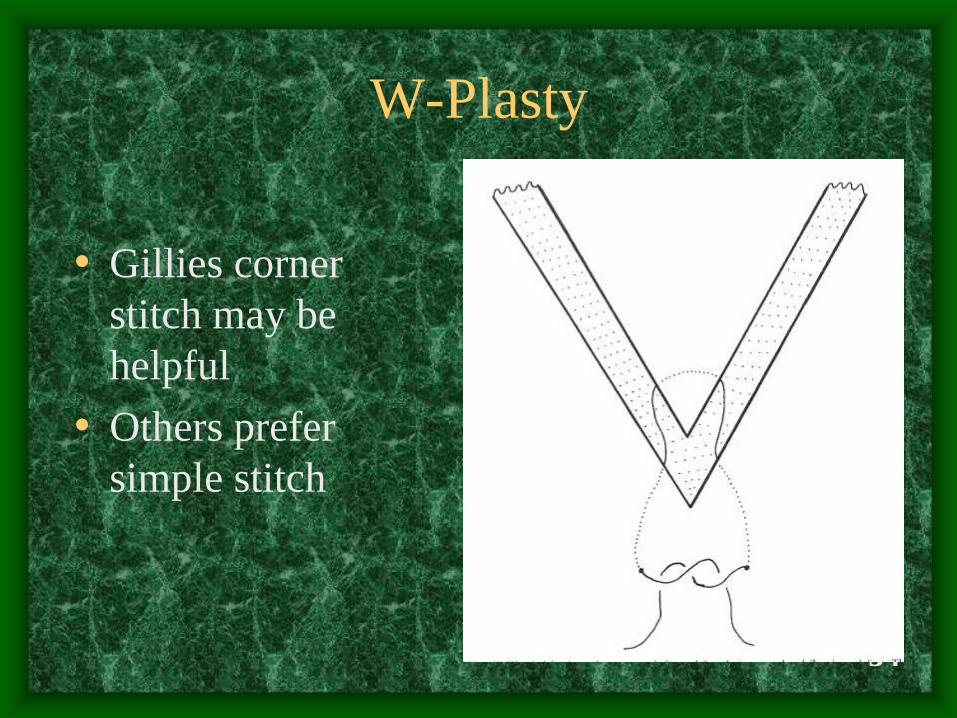
W-Plasty
• Gillies corner
stitch may be
helpful
• Others prefer
simple stitch

55
W-plasty
• Note
exposure on
photos

56
Geometric Broken Line Closure
• Irregularly irregular

57
Geometric Broken Line Closure

58
Geometric Broken Line Closure
• After closing dermis can run with Fast-Sorb

59
Geometric Broken Line Closure

60
Adjunctive Measures
• Dermabrasion
• Laser
• Cosmetic camouflage

61
Dermabrasion
• Reduces surrounding
skin to level of scar
• Blends color/texture
• Laser resurfacing now
popular
• Best done around 6
weeks

62
Dermabrasion

63
Dermabrasion

64
Laser
• More control
• Good for pigment
• Minimizes particulate matter
• Optimum laser/combination under
investigation

65
Laser

66
Cosmetics
• Very safe
• Allows sooner return to function
• May instead of or in addition to surgery

67
Cosmetics

68
Cosmetics

69

70
Treatment Algorithm

71
Conclusion
• “an ounce of prevention”
– Surgical planning and technique
– Wound care
• Counseling
• Timing
• Careful analysis
• Appropriate technique

72
Bibliography
• Alster TS, Lewis AB, Rosenbach A. Laser scar revision: comparison of CO2 laser vaporization with and without simultaneous pulsed dye laser treatment. Dermatol Surg 24:1299-1302, 1998.
• Berlinger NT. Wound healing. Otolaryngol Clin North Am 15(1):29-34, 1982 Feb.
• Bernstein L. Z-plasty in head and neck surgery. Arch Otolaryn 89:574-84, 1969 Apr.
• Borges AF. Principles of scar camouflage. Facial Plast Surg 1(3):181-90, 1984.
• Borges AF. Timing of scar revision techniques. . Clinics in Plastic Surgery 17(1)71-6, 1990 Jan.
• Borges AF. Relaxed skin tension lines. Derm Clin 7(1):169-77, 1989 Jan.
• Brown LA, Pierce HE. Keloids: scar revision. J Dermatol Surg Oncol 12(1):51-6, 1986 Jan.
• Cantrell RW. Iatrogenic scar camouflage. Facial Plast Surg 1(3):191-208, 1984.
• Davidson TM. Scar Revision. Self-Instruction Package (SIPac). American Academy of Otolaryngology - Head and Neck Surgery Foundation, Inc: Alexandria, 1998.
• Farrior RT. Dermabrasion in facial surgery. Laryngoscope 95:534-45, May 1985.
• Harmon CB, Zelickson BD, Roenigk RK, et al. Dermabrasive scar revision: immunohistochemical and ultrastructural evaluation. Dermatol Surg 21:503-8, 1995.
• Kaplan B, Potter T, Moy RL. Scar revision. Dermatol Surg 23:435-42, 1997.
• Koopman CF. Cutaneous wound healing: an overview. Otolaryngol Clin North Am 28(5):835-45, 1995 Oct.
• McGillis ST, Lucas AR. Scar revision. Dermatologic Clinics 16(1):165-80, 1998 Jan.
• Moran ML. Scar revision. Otolaryngol Clin North Am 34(4):767-80, 2001 Aug.
• Nicolai JP, Bos MY, Smale CE. A protocol for the treatment of hypertrophic scars and keloids. Aesthetic Plastic Surgery 11:29-32, 1987.

73
Bibliography
• Orentreich D, Orentreich N. Acne scar revision update. Derm Clin 5(2):359-68, 1987 Apr.
• Pazienza LE. Cosmetology: an adjunct to aesthetic facial surgery -- a reconstructive aethetician's
perspective. In Aesthetic Facial Plastic Surgery. Romo T, Millman Al, (eds.) Thieme: New York,
2000.
• Porter JP. Treatment of the keloid: what is new?. Otolaryngol Clin North Am 35(1):207-20, 2002
Feb.
• Preuss S, Breuing KH, Eriksson E. Plastic surgery techniques. In Plastic Surgery: Indications,
Operations, and Outcomes. Achauer BM, et al, (eds). Mosby: St. Louis, 2000.
• Roenigk HH. Scar camouflage using dermabrasion. Facial Plast Surg 1(3):249-57, 1984.
• Rudolph R. Wide spread scars, hypertrophic scars, and keloids. Clinics in Plastic Surgery
14(2)253-60, 1987 Apr.
• Sherris DA, Larrabee WF, Murikami CS. Management of scar contractures, hypertrophic scars, and
keloids. Otolaryngol Clin North Am 28(5):1057-67, 1995 Oct.
• Stal S, Hamilton S, Spira M. Surgical treatment of acne scars. Clinics in Plastic Surgery 14(2)261-
76, 1987 Apr.
• Tardy ME, Denneny J. Surgical alternatives in scar camouflage. Facial Plast Surg 1(3):209-25,
1984.

74
Bibliography
• Tardy ME, Thomas JR, Pashcow MS. The camouflage of cutaneous scars. Ear, Nose,
& Throat Journal 60:61-70, 1981 Feb.
• Thomas JR, Ehlert TK. Scar revision and camouflage. Otolaryngol Clin North Am
23(5):963-73, 1990.
• Thomas JR, Frost TW. Scar revision and camouflage. In Local Flaps in Facial
Reconstruction, Baker SR and Swanson NA, (eds.) Mosby: St Louis, 1995.
• Thomas JR, Holt GR. Facial Scars: Incision, Revision, & Camouflage. Mosby: St.
Louis, 1989.
• Webster RC, Smith RC. Scar revision and camouflaging. Otolaryngol Clin North Am
15(1):55-68, 1982 Feb.
• Wolfe D, Davidson TM. Scar revision. Arch Otolaryngol Head Neck Surg 117:200-4,
1991 Feb.
• Yang JY. Intrascar excision for persistent perioral hypertrophic scar. Plast Recon Surg
98(7):1200-7 1996 Dec.