scale-up of the community scorecard process in the...
TRANSCRIPT

1
Scale-up of the Community Scorecard Process in the Madagascar Health Sector
Discussion Draft November 20, 20081
This approach paper presents the ongoing Community Score Card (CSC) pilot in Madagascar, discussing how the program has evolved and presenting options for scale-up and institutionalization. The discussion is organized as follows:
• A discussion of the first two phases of the CSC, and lessons learned regarding the most cost efficient and effective organization of Community Score Cards in Madagascar
• A discussion of next steps for the CSC, in terms of methodological improvement, defining institutionalization for the Madagascar CSC, potential for scale-up, and discussion of how the CSC might be organized, in terms of institutional home, implementing partners, funding, and actual implementation.
The objective of this paper is to provide stakeholders with the information necessary to define a strategy on the above objectives. ���%DFNJURXQGCSCs are a tool used to solicit direct feedback from service users and to initiate dialogue between users and service providers. The CSC is meant to empower users with information (on norms of service, on the structure of the sector, and on how to advocate for improvements), to encourage communication between users and service providers outside of the health center, to mobilize communities and service providers to work together to improve services, and to improve health center management at multiple levels by dissemination of results at the local health center (Centre de Santé de Base, or CSB), district, and regional levels. Compared to some other social accountability tools, the CSC is relatively low tech and therefore can be replicated on a larger scale at a lower cost than some alternative methods (such as citizen report cards for example, which are useful for evaluating performance at the national or regional level). Unlike traditional administrative monitoring systems, the CSC (a) directly implicates civil society, (b) focuses on rapid local public disclosure of feedback versus more lengthy centralized analysis, (c) requires sharing information with users on norms of service and on what aspects of service they can work with service providers to improve (as well as where issues may be outside of the providers’ control), and (d) in some cases, may involve comparison or an element of competition in the performance of different service providers. In sum, CSCs are meant to shorten the accountability loop between service providers and clients and to ultimately lead to better service quality. In experiences such as those in Uganda, similar mechanisms have been shown to lead to improvements in health care quality and quantity; increases in local health center utilization, number of assisted deliveries, and use of family planning services; and decrease in visits to traditional healers and self-medication. (See Bjorkman, Reinikka, Svensson, 2006 on the Uganda case).
1 All exchange rates calculated at 1575 Ar/1USD, the Central Bank of Madagascar exchange rate of August 4, 2008.

2
CSCs in Madagascar began in 2006, following a World Bank-organized study tour in which several civil society and government representatives traveled to Bangalore, India, to learn more about Social Accountability and CSCs. With World Bank-funded training and technical assistance, a group of civil society representatives, financed by the Programme de Réformes pour l'Efficacité de l'Administration (PREA) and the Projet de Gouvernance et Developpement Institutionnel (PGDI), in close collaboration with the Ministry of Health, conducted the first non-training CSCs in 4 health centers across 2 regions of Madagascar in February-March 2007. Based on the success of these first activities (Phase 1), a second phase (Phase 2) has been undertaken in the health sector in the Anosy region in May 2008, under the leadership of PREA/PGDI and the Ministry of Health, and with the active involvement of a committee composed of the Poles Integrées de Croissance (PIC), the Projet de Gouvernance des Ressources Minerales (PGRM), the Bureau Independent Anti-Corruption (BIANCO) and the Region of Anosy. For this phase, the World Bank continues to provide international technical assistance, as well as funding and managing several national technical assistant positions. The first set of Phase 2 pilots have been completed (August 2008), and the follow-up phase, in which the exercise will be repeated to evaluate changes in user satisfaction and health outcomes, will begin in late October 2008. While Phase 1 of the CSC tested the applicability of the CSC methodology and adapted the tool to the Malgache context; Phase 2 tests certain methodological and implementation strategies to increase cost efficiency, improve results monitoring, and increase effectiveness of the tool. These adaptations are in response to questions posed by the Ministry of Health regarding the cost-benefit analysis of the CSC during the 2008 National Conference on Social Accountability. This approach paper presents the current analysis of Phases 1 and 2, and lays out key issues to be discussed in terms of whether and how the CSC should be institutionalized and scaled up as a permanent, sustainable tool in the health sector (Phase 3).
���'HWDLOHG�'LVFXVVLRQ�RI�3KDVHV���DQG��Phase 1: Following the study tour to Bangalore, a local civil society association, OPTA, was formed as the initial focal institution for social accountability in Madagascar. OPTA’s membership included representatives from academia, science, the youth community, a consumers’ association, and local mayors, all based in Antananarivo. In September 2006, OPTA members received a one-week training on CSC methodology from a World Bank-funded international technical assistant. In January, 2007, OPTA invited collaboration from other civil society groups, associations and NGOs, many of which represented national networks. A team of 22 facilitators, representing OPTA and the members of this new consortium (including SanteNet, Pact Madagascar, and FJKM) then received additional World Bank-funded theoretical and practical CSC training. In February-March 2007, this new group of CSC facilitators, self-named the “Core Team,” conducted pilot CSCs in the regions of Haute Matsiatra (central highlands) and Boeny (coastal). The team conducted two CSCs per region, including regional dissemination meetings, to which press was invited and results were published, as well as regional training activities to build local capacity among locally interested civil society representatives.

3
In June, 2007, the Core Team conducted follow-up activities in the two regions. In this Phase, results were measured in terms of user satisfaction. Results were promising, with improvements seen in each of the CSBs on almost all user-generated satisfaction indicators, by as much as 96%. Users in the target communities worked with service providers to improve transparency and accountability, by posting opening hours and drug prices, improving reliability of payments to dispensatrices and guardiens, and promoting community-level investment in health services. Some communities organized fundraisers to hire masons to improve facilities, other communities organized payments-in-kind to gather resources to build facilities communally. This process of improving dialogue, accountability, and transparency improved user satisfaction in terms of availability of drugs, human resources, CSB infrastructure, doctor/patient reception, and cost of drugs. See Annex 2 for a more detailed discussion of results. In each of the communities, volunteer monitoring groups were set up to take responsibility for following the implementation of the communities’ action plans. These volunteer committees included service providers, users and members of the commune administration, charged with holding regular consultations to ensure the action plan was being followed. However, at the national level, no resources were allocated for continued intervention, so following the CSC, responsibility for follow-up has been with the local committees. Phase 1 of the CSC cost approximately US$30,000, not including the cost of international technical assistants, i.e. US$7,903 per CSC. (See Annex 3 for more specific breakdown of costs) Phase 2: Phase 2 of the CSCs is currently underway in the Anosy region; the follow-up CSCs have recently been completed, but final results will be available in late December. The methodology for Phase 2 was designed by the World Bank, PGDI/PREA, and the implementing NGO, with the input of numerous World Bank and sectoral experts in Madagascar, and was validated by the national CSC steering committee (PREA/PGDI, the Ministry of Health, PIC, PGRM, and BIANCO) and the Region of Anosy. PREA/PGDI is funding the CSC direct costs, and contracted with Pact/MSIS, an international NGO, to implement the CSC in 20 CSBs in Anosy region. Phase 2 of the CSC pilot builds on the results and lessons learned from Phase 1, with certain key objectives for improvement: to refine the CSC methodology and implementation arrangements to make it more cost efficient, more rigorous and inclusive, and more practical for widespread implementation. Activity In Phase 2, Pact Madagascar/MSIS recruited 70 facilitator candidates. The team of technical assistants and PACT then provided training to these facilitator candidates the best 50 facilitators were selected from amongst these to work on the CSC. The facilitators were divided into two types: 10 Regional facilitators (RFs), possessing strong numeric, analytical, and organizational capacity, and 40 Communal facilitators (CFs), with strong facilitation

4
skills. Each team of 2 CFs were assigned to one CSB, where they conducted a CSC; in half of these groups, both CFs had prior experience in the commune; in half, neither did. The RFs, in groups of 2, were assigned 3 communes each, circulating and assisting the CFs in their respective communes. Including 3 CSCs conducted as part of the training activity, 20 CSCs were conducted in communes across the region. The initial implementation of this activity was completed in early August, 2008 and follow-up interventions were completed in late November 2008. A regional dissemination activity was held on September 16th, and a second meeting to publicize results of the follow-up will be held in mid-December, 2008. Results of Phase 2 Results of Phase 2 of the CSC – meaning quantifiable changes in user satisfaction or health outcomes – will only be available once the process is completed, towards the end of December, 2008. However, preliminary reports from the target communes point to similar patterns as in Phase 1. During the initial field work of Phase 2, facilitators reported that the CSC created unprecedented opportunities for communities and service providers to come together to discuss norms and service delivery in an open forum. Discussion allowed users to better understand the services offered by CSBs, to ask questions about prices and services, and to express any dissatisfactions with service quality. For service providers, the CSC allowed them to explain their own constraints to service, to dispel certain health myths, to explain the importance of coming to the CSB, and to explain certain often misunderstood topics, such as the Equity Fund, and the difference between brand name and generic drugs. Initial CSC action plans from the 20 target communes included community plans to raise funds or supplies for improving infrastructure, community plans to increase user understanding of certain health issues and treatment, publication of drug pricing lists and opening hours, mobilization of village CoSan and CoGe, and community campaigns to petition the ministry for additional personnel in keeping with CSB norms. While results were measured primarily through changes in user satisfaction in Phase 1, in Phase 2, results will also include data on certain health indicators (as agreed upon by SanteNet, the World Bank, and the Ministry of Health), which will allow for measuring changes in service use and health outcomes, in addition to user satisfaction. While user satisfaction is an important indicator of service quality, some studies have illustrated how the poorest sometimes rate services more positively than wealthier counterparts due to differences in expectation rather than to differences in actual service – those accustomed to better services have higher standards for service, and are therefore more critical than those who are accustomed to very little. The introduction of more quantitative indicators in Phase 2 will attempt to provide a more balanced view of use and performance of the health services at the community level.2
While quantitative results for Phase 2 are not yet available, similar scorecard and report card exercises, which involved publication of user evaluations, have produced significant results in other countries. In Uganda, a citizen report card at health centers led to a 16% increase in utilization rates over the first year of the project and a 68% jump in the number of deliveries.
2 However, because no control group was used, results will not be fully attributable to the CSC.

5
Rates of patients seeking antenatal care rose by 20% and by 63% for those seeking family planning over the first year of the intervention.3 A number of similar health indicators – including rate of utilization, numbers of deliveries at the CSB, and use of family planning – are being tracked and results should be available with the final results in early December 2008.
Methodological Analysis Phase 2 was designed based on Phase 1, with key modifications to reduce per-CSC costs, to explore ways to scale-up the CSC, to strengthen results monitoring, and to make the tool more effective. As a part of these methodological improvements, Phase 2 explored the feasibility of using facilitators with various degrees on connection to the target communes. For instance, what is the benefit to having facilitators who know local dialect, and how does this compare with the costs of having facilitators working so close to their own communities? Are facilitators with personal or professional links to a community objective? Do they feel confident facilitating a critical discussion? Do they possess the necessary technical skills - including good analytical and numeric skills - to conduct the CSC with limited technical assistance? Use of commune-level facilitators may have cost-saving implications, so this phase tested combinations of facilitators to maximize the benefits from these trade offs and reduce the costs. While it proved logistically difficult to recruit facilitators living permanently in the target communes in Phase 2, it was possible to explore some of the above questions by using facilitators with prior experience in the communes. CFs were selected such that in half of the CF teams, both CFs had prior personal or professional connections to the target communes. In the other half, neither did. Facilitators were evaluated in terms of their skills as a facilitator, as well as their dynamic with and ability to mobilize the particular commune to which they were assigned, all in relation to the strength of their prior connection to the commune (on a scale from 1 to 5). While this arrangement does not answer all of the above questions because facilitators do not continue living in the target communes, it does allow for analysis of some key factors. 4
The CSC is nearing completion (more definitive results will be available when facilitator evaluations can be compared to levels of improvement at the CSBs), but preliminary evaluations of the different facilitators reveal that facilitators with more experience in a given commune performed more strongly than those without experience in the target commune, in terms of facilitation skills, as well as in their ability to mobilize a community to participate, and to communicate effectively with the community. One key factor in this increased efficacy, however, is simply mastery of the local dialect. Dialects vary throughout the country, and vary from village to village in Anosy. In some of the target communes, the
3 Martina Bjorkman, Ritva Reinikka, Jakob Svensson, “Seminar Paper No. 749: Local Accountability,” Institute for International Economic Studies, Stockholm University, 2006: 1,19 4 Regional facilitators completed evaluations of each communal facilitor; the national technical assistant and implementing NGO coordinator also provided analysis of facilitator strengths and weaknesses.

6
doctors themselves did not speak the local dialect, so having facilitators who could was crucial to effective facilitation. Facilitators with knowledge of the commune were also evaluated as more effective facilitators due to a deeper understanding of local customs and traditions, and a more immediate understanding of the health, governance, and logistical concerns facing the commune; they were also able to act as guides in navigating the physical and political landscape. However, these facilitators were not deemed to be biased in any way that interfered with their ability to conduct the CSC. As noted above, the methodology for Phase 2 also differed from Phase 1 in that it included improved impact evaluation and results monitoring. In addition to the inclusion of quantitative indicators, a database is being designed by an international technical assistant, who will train the implementing NGO on how to use the database to enhance comprehensive analysis of results, including comparison of performance of CSBs and factors responsible. The sustainability of the CSC was also improved in Phase 2. In Phase 1, Tana-based facilitators conducted the initial CSCs, and returned three months later to conduct the follow-up CSC. There were no structured intermediate interventions, nor any follow-up, nor were facilitators from the target regions, nor continuing to live there. In Phase 2, all facilitators are from the Anosy region, and the communal facilitators have met with the target communities each month since the initial CSCs, to keep the local follow-up committees on track with the communities’ agreed action plans.
Cost Benefit Analysis of Phase 2 Phase 2 was designed to aid in determining how to reduce per-CSC costs. The total projected cost of Phase 2 (not including international technical assistant) was US$121,010.5This is approximately US$6,050 per CSC. However, it is important to note that based on current actual disbursements, while the total CSC could cost as much as US$121,000, it is more likely to be nearer to US$81,000, including the implementing NGO and training, or US$4,050 per CSB. Based on an analysis of projected costs alone, costs in Phase 2 are already significantly lower than in Phase 1 (US$7,903 per CSC). One of the main cost elements (approximately $25,000) of Phase 2 was the administrative costs of the implementing NGO. Phase 2 is the first regional pilot for the CSC in Madagascar, so there were many logistical issues, and it included intense reporting requirements that required significant administrative support. Having successfully completed this Phase, with a successful methodology in place, subsequent Phases in subsequent regions should require moderately less intensive support, less intensive reporting, and/or may be conducted with regional NGOs (rather than national or international), which may help in keeping costs down. Specific suggestions on these arrangements are addressed in section 3 of this report.
5 In Ariary: 190,590,339 Ar total, or 9,528,750 Ar per CSB. Total cost includes National Technical assistant funded by World Bank), 4 trainers (funded by WB), and the cost of all Pact activities and fees.
7
Within the activity costs for this Phase (i.e. not administrative, training, or technical assistance costs), per diems and transportation were by far the largest cost areas for Phase 2. This was in part due to the fact that, although it was intended that CFs would come from target communes, thereby reducing per diem and transport costs, this was not ultimately feasible. So, sending facilitators to work in communes required payment of per diem and transportation. Furthermore, to monitor the activity, weekly feedback meetings were held with all facilitators in Ft. Dauphin, which provided an important monitoring opportunity, but further drove up transport costs.
In summary, while the costs of Phase 2 have been high, factors that drove up costs were largely due to the fact that this was a pilot activity at this scale, and have been identified and will be modified in subsequent phases, to bring costs down. (See section 3.1 for specific cost reduction estimates for subsequent CSCs). 3. 1H[W�6WHSV�LQ�WKH�&RPPXQLW\�6FRUH�&DUGIn considering next steps for the community score cards in the health sector in Madagascar, several key elements for consideration include:
3.1 Lessons Learned for Methodological Improvements and Implications for Future Interventions (Changes to the detailed methodology of a single CSC)
3.2 Structure of Scale-Up (Determining the depth and breadth of each CSC intervention) 3.3 Institutional Structure and Institutionalization of Future CSCs (Determining how CSCs will be
organized and implemented) 3.4 Funding for Future CSCs (How CSCs will be funded)
����/HVVRQV�/HDUQHG�DQG�.H\�0HWKRGRORJLFDO�$PHQGPHQWV�� While still in progress, the experiences of Phase 2, and insight and inputs from the Ministry of Health, SanteNet, USAID, and the PGDI project have all provided lessons on how to continue refining the CSC methodology in Madagascar.
Communal Facilitators v. Communal Mobilisers In Phase 2, it was noted that community facilitators with strong links to target communes are effective in terms of organization and facilitation of focus groups, and generating community ownership and participation. In the Anosy region, though, they lacked the capacity to be effective, independent facilitators; they had difficulty writing reports, carrying out calculations, and reporting on key data. Anosy is one of the lowest ranked regions in Madagascar in terms of educational attainment, and this may be a factor in the difficulty finding commune-level facilitators capable of independently facilitating a CSC. However, the strength of these local facilitators in mobilization and facilitation, and the importance of local ownership of the tool indicates that commune-based facilitators should be included wherever possible, but in a way that responds to capacity concerns. Therefore, in order to respond to this capacity issue during scale-up in similar regions, two models are proposed for future interventions, one model for regions with higher literacy and educational attainment at the commune level, and a separate model for those with lower

8
literacy and educational attainment.6 These two models both feature local level facilitators, with varying levels of technical support.
- Model 1 “Facilitators”: In regions with higher educational attainment, continue to use the Facilitateur Communaux and Facilitateur Regionaux approach as used inPhase 2. However, while this model was less effective in the Anosy region, it may be more practical, and cost effective in other regions where commune-level capacity is more available. This model is based on successful implementation of a similar model in Uganda, and its strength is based on the fact that it allows for capacity building and use of facilitators at the commune level, while providing a moderate level of reinforcement at the regional level. Additionally, increased reliance on commune-based facilitators reduces cost, versus a strategy that requires bringing capacity to the target communes.
- Model 2 “Mobilisateurs”: In regions with lower educational attainment, CFs may be replaced with community mobilisers (CMs). These mobilisers should be based in the target communes, but in this model would be primarily responsible for mobilizing participants for CSC activities, rather than responsible for actual facilitation. These mobilisers will be given brief training in the CSC (informational, rather than highly technical), and be provided with a small stipend for their work. An increased number of RFs will be used to facilitate the CSCs, working in collaboration with the CMs, in order to maximize benefits of using local facilitators, but also to ensure technical capacity. A potential model for this approach would be to have 2 mobilisers from each target commune, and approximately 16 RFs (depending on how communes are spaced), who would be divided into groups of 4, covering 5 communes each over a 5 week period. Because this Mobilisateur model requires more intensive participation from the RFs, it is a slightly more expensive model.
Table 1: Costs of )DFLOLWDWHXU v. 0RELOLVDWHXU�Models
Model ‘)DFLOLWDWHXU’(including 2 follow-up activities, not integrated with KM)
Model ‘0RELOLVDWHXU’(including 2 follow-up activities, not integrated with KM)
Cost per CSC US$5,895 US$6,522 Cost per Region US$119,707 US$130,477 Cost per 22 Regions US$2,633,559 US$2,869,825
6 Regions of high educational attainment may be as regions where the Taux d’Achevement is higher than 14.0.

9
Based on concerns that the RF/CF/CM model may be too expensive and too cumbersome, a third model is possible, although not advised. In this model, the methodology would be simplified. There would be no Regional Facilitators, such that CFs would be responsible for all facilitation. This model could be implemented through existing programs like the Champion Communes program (as will be discussed in the next section), or through an independent contracted NGO. However, there are a number of risks with such a model. As noted, in the Anosy pilot, capacity was a major issue, even with the assistance of Regional Facilitators, and technical assistance. Reports were delayed and incomplete, and calculations were often incorrect; trainers, technical assistants, and the implementing NGO had to spend significant time rectifying these problems. Reducing technical assistance and supervision would increase the potential for such problems, which could compromise the efficacy of the entire intervention. Therefore, this model is not suggested. If desired, however, this model might be tested on a moderate scale, such as in one region, while the models above are tested in other regions. However, as this model relies on exceptionally strong capacity among communal facilitators, it is advised that it only be implemented in regions with the highest educational attainment, such as Analamanga. Pilot regions should also be sufficiently urban to allow easy supervision by the implementing NGO and technical assistants. Such a model could be conducted, with follow-up, for approximately $97,000 including supervision and follow-up activities. Regional Facilitators In Phase 2, per diems were one of the most significant expenses, particularly for the RFs, who had to travel to assist CFs in various communes. To reduce this cost, and to decentralize capacity so that technical expertise exists closer to the communes being targeted, RFs should be recruited by district in subsequent phases, in both facilitateur and mobilisateur models. These RFs would circulate to the target communes within their district, as in Phase 2, but would not have to travel as far or for as long, therefore reducing costs. Thus, in every district in which communes are being targeted, RFs would be recruited, 2 per region, for example. Communication Phase 2 demonstrated the importance of a strong communications strategy. Participation from commune-based facilitators could have been higher if there had been more time to publicize the tool and recruitment. Thus, to improve community level participation – investment in advertising well in advance of the intervention (through radio, visits to communes, and postering) should be greatly increased. Spending more time and resources to ensure thorough community awareness in all the target communes will increase community interest, demand, and mobilization, and increase the likelihood that strong candidates apply from each commune. Demand In planning subsequent phases, target communes should be selected, in part at least, based on demand at the commune level (perhaps from a larger pool of pre-selected communes or regions). To generate this demand, regional implementing partners should conduct district

10
level presentations on the CSC, to which all relevant communes (civil society, health center staff, and commune and Fokontany authorities) could be invited. The meeting should include a discussion of the objectives, methodology, and community obligations involved in a CSC, as well as an explanation and training on how to submit a request for assistance in conducting a CSC at the commune level. Participation of district authorities like the SDD would be encouraged. Applications would then be accepted from civil society, mayors, and CSB personnel to request a CSC in a particular commune. Demonstration that two or more of these stakeholder groups (local authorities, civil society, health center staff) support the activity would be encouraged.
����6WUXFWXUH�RI�6FDOH�8S� To date, completed and ongoing CSCs have been implemented as pilot projects to determine the applicability and cost effectiveness of the Community Score Card in Madagascar. Results have been reported to the Ministry of Health, and in ongoing and subsequent phases, methodology is being developed to monitor these results to promote continued improvement. If the CSCs are to be scaled-up, however, this scale-up needs to be considered either as 1) continuing, deepening interventions in selected communities, gradually expanding to cover most, if not all, of the country (Scale-Up Model 1) or as 2) ameans for quickly spreading the CSC methodology to all regions (Scale-Up Model 2). In Scale-Up Model 1, the CSC is conducted several times over a defined time interval (at 6 month intervals over 1.5-2 years, for example), in a given number of target regions and communes. The objective would be to reinforce local capacity, making it more likely that the community will continue with the CSC process in the health sector and/or use it in other sectors; to reinforce community understanding and participation in the idea that demanding accountability can bring results; and to create opportunities to track results over time, to examine how health outcomes and rates of satisfaction are changing. Scale-Up Model 2 is designed to more quickly reach all regions, by only conducting the CSC as one- or two-time interventions. However, without conducting multiple CSCs, results may be more limited if communities are hesitant at first, the impact may be more short-lived, and it will be difficult to monitor the impact of the tool. Table 2. Costs of Scale-Up Model 1 v. Model 2
Scale-Up Model 1 Scale-Up Model 2 )DFLOLWDWHXUV 0RELOLVDWHXUV )DFLOLWDWHXUV 0RELOLVDWHXUVInitial Implementation in 1 Region (20 CSCs, including National Trainers and TA; notincluding international TA, which would be required throughout)
US$93,007 US$95,865 US$93,007 US$95,865

11
Two Unassisted Follow Ups, i.e. every 6 months following the Initial Implementation for a total of 2 years
US$11,070 US$34,582 N/A N/A
Additional Follow-Up Supervision
US$15,000 US$20,000 N/A N/A
Cost per CSC US$5,895 US$6,522 US$4,650 US$4,793 Cost per Region US$119,707 US$130,447 US$93,007 US$95,865 Cost over 22 Regions US$2,633,559 US$2,869,825 US$2,046,160 US$2,109,026
Of the two designs, Model 1 would create more local level capacity, would give participants a greater exposure to the CSC tool and encourage more sustained results, would allow for a longer period over which to develop and locally track an action plan, and would allow for more informed monitoring of the changes created by the CSC. Sustained interventions would address one of the primary issues encountered in the Phase 1 and Phase 2 CSC pilots – namely, community hesitation. Communities’ incentives to raise issues and hold their service providers accountable are diminished when they see the intervention as short-term. Community members have expressed fear that they will face retribution from service providers after facilitators leave. An on-going intervention demonstrates to users that there are greater incentives to participation, and rewards and grants associated with participation would enable them to set goals and targets as a community. As such, Model 1 is the recommended option, although with the objective of expanding to cover the entire country in 4-5 years.
����'HWHUPLQLQJ�DQ�,QVWLWXWLRQDO�6WUXFWXUH�IRU�WKH�&6&���For the sustainable scale up of the Community Score Card and definition of a national CSC strategy, an institutional structure – including technical, organizational, strategic and financial aspects - must be defined. While the CSC is one of the simpler Social Accountability tools, to be conducted effectively, the CSC nonetheless requires a significant amount of organization, funding, and technical expertise. While Phase 1 of the CSC was coordinated by the Ministry of Health, PGDI/PREA, and the World Bank, with just 2 international technical assistants recruited, scaling up to 20 communes, in one region in Phase 2 required recruitment of an Anosy-based NGO to implement, with the support of a team of trainers and national and international technical assistants. Managing this process at the national level, for multiple regions, will be best achieved through a clear institutional structure, with clear responsibility for each of the four following dimensions:
A. Technical Coordinators: To provide technical assistance and training on the CSCs, and be responsible for assuring quality control of all CSC activities. Technical coordinators will also be responsible for managing some funding aspects of the CSC (those not handled by the Ministry of Health or the implementing partner).

12
B. Implementing Partner: To organize, manage, and administer the implementation of the CSC, with the support from technical coordinators.
C. Strategic Coordinating Committee: To provide strategic guidance on CSC activities – what regions, on what timeline, etc.
3.A. Technical Coordinators While the CSCs are a relatively simple tool, to conduct a CSC accurately, high level technical capacity is required to train trainers, train facilitators, and monitor and analyze results. If the tool is not conducted correctly (i.e. focus groups not convened in a representative manner, tool not presented correctly, data not recorded correctly and in a timely manner, calculations not done correctly), results will not be useful at the community level for improving service delivery, nor will they be useful at the regional or national level for tracking how well service delivery is improving. To assure that the tool is done efficiently, technical support – in the form of technical assistants and qualified trainers - is required. To conduct the CSC nationally, i.e. in multiple regions at a time, it is advisable to have a technical committee – a base for this technical expertise – that is comprised of technical experts, with a roster of qualified trainers and technical assistants that can be contracted for various projects. As custodians of such a roster, this technical committee would be responsible for validating CSC trainers, as well as assuring the quality of the technical support on CSCs. Under the PGDI 2 project, a Social Accountability Secretariat is being created that will include national and international technical assistants on the Community Score Card, as well as regional focal points. This Secretariat will report to a tri-partite committee composed of PREA/Government, Bank/partners, and civil society.7 For future phases of the CSC in the health sector, this Secretariat could be designated as this technical ‘home’ for the Community Score Cards, responsible for providing technical assistance on the organization of the interventions, training of trainers, and training of facilitators. In CSC interventions, the Secretariat would be contracted (by the Ministry of Health, or by other ministries in other interventions) to train facilitators and assure the technical quality of the intervention, as well as providing guidance on the organization and structure of interventions. The Secretariat would be responsible for contracting all required CSC trainers and technical assistants. As the ‘home’ for technical capacity and organizational experience (i.e. technical assistants with experience conducting CSCs in Madagascar), the Secretariat would also be the home for management of funding for the CSC, and would be responsible for all procurement and contracts not handled through the contracting Ministry or designated to the implementing partner. There are several advantages to using the Secretariat as the technical home for the CSC:
7 The final structure is still being finalized, but will include: a national coach responsible for managing the secretariat and oversight of PGDI’s social accountability agenda; regional focal points on social accountability to implement ongoing programs in strategic areas; a national expert on community scorecards; a national expert on participatory budgeting (who may work closely with MDAT and FDL initially).

13
- The technical leadership of the CSC should be independent of the Ministry of Health. While the involvement of the Ministry of Health is crucial to the success of CSCs in the health sector, CSCs are based on the principle of independent third party monitoring. So while the support and endorsement of the Ministry of Health are crucial to the success of the tool in the health sector, there needs to be a layer of independence in the implementation of the process.8 Under this arrangement, the Ministry could commission the Secretariat to provide technical assistance on the CSC, and the Secretariat would report to the Ministry, but having the Secretariat as an independent control on financing would create a level of independence from the Ministry. The Ministry would appoint its own internal focal points, who would work with the secretariat and national and international technical assistants recruited by PGDI to organize and monitor CSC activities.
- An additional advantage to the secretariat arrangement: while Ministry focal points could provide sectoral knowledge, the Secretariat would represent a centralized technical knowledge bank on the CSC that can also be used for other sectors in future.
The SAc Secretariat will include 6 regional focal points. However, to reduce costs and increase local ownership and management of the CSC, it may be advisable that the SAc secretariat recruit additional regional CSC coaches for regions to be targeted that have not already been assigned a SAc focal point. This would reduce per diems and transport costs of sending technical assistants from Tana to assist with CSC, would allow more CSCs to be conducted simultaneously, and would decentralize CSC capacity. These regional CSC coaches could be recruited by the SAc secretariat and provided with CSC training. They would then be responsible for assisting the implementing partner in the organization and management of the CSC. For regions without a SAc focal point, a CSC ‘coach’ for 100 days (initial implementation), plus 50 days for follow-up work, plus training in Tana, would cost approximately US$9,000. Using a national level Coach in this position would cost significantly more (approximately US$12000), making the selection of regional coaches more cost and time efficient. This regional coach approach is integrated into subsequent costings as part of the technical assistance budget.
3.B. Implementing Partner
The second major dimension of the scale up of the CSCs is how they are actually implemented. The Secretariat will provide technical guidance on implementation, but the ‘implementing partner’ is the partner that will be contracted to manage the implementation.
8 Although the CSC is meant to provide independent, third party monitoring, the support of the Ministry of Health is essential to ensuring enthusiastic participation of service providers and users alike. Service providers have expressed that they need authorization from their superiors to participate, and users have similarly expressed concerns that without a written notification from the district or regional authorities, stating that service providers can and should participate, and users fear reprisals from service providers after the activity ends. To users, the Ministry’s involvement is insurance that local service providers will listen to their critiques. Additionally, the Ministry’s participation is important in defining health indicators to measure the impact of the CSC. However, the CSC must be independent enough that users, providers, and facilitators feel they can express and elicit constructive criticism of the health service.

14
Rather than a ‘home’ this group may be seen as a coordinating partner, linking technical capacity in the secretariat with local participants in the target regions and communes, whom they will be training. However, this role alone requires significant organizational capacity. As such, this partner must have excellent organization, strong regional contacts, and experience rolling out programs in multiple regions. Tasks in the implementation of a CSC in any single region involve advertisement of the CSC activity; recruitment of potential facilitators (RFs, CFs/CMs); organization of a facilitator training; organization of the logistics for all CSCs (transportation, lodging and per diems for facilitators); all supplies for the CSCs; and monitoring of results reporting. Implementation of the CSC requires significant preparation in the field, and is most efficient if it is done through existing networks, building on existing relationships with communes. It is also most easily organized by an organization with an established office, staff, computers, and vehicles. Performing these functions simultaneously in multiple regions will require excellent organization and administrative capacity, as well as strong technical capacity. In Phase 2, the implementing partner was an international NGO with regional presence. While the NGO performed well for a first pilot of this size, the administration/supervisions costs for the NGO alone were approximately US$25,000. For subsequent phases, objectives should be to reduce costs, and establish an implementation arrangement that provides a necessary level of independence from the Ministry, while also allowing the Ministry to benefit from the information generated through the CSC. The Ministry of Health has made a commitment to increasing citizen participation and accountability in health centers across the country; this is currently being implemented through the Champion Communes (KM) program, working through the SanteNet project. This program is planned for roll out in 500 communes in 16 regions, over the next several years. The Ministry has expressed interest in building the CSC into the KM program, as one of the tools used in KM-participating communes. Adding the CSC into the KM program would have benefits both for the implementation of the CSC, as well as for the outcomes of the KM program itself. In terms of the CSC, integrating the CSC into the KM program would streamline implementation, reduce costs, and provide a simple mechanism for monitoring improvements in service delivery. For the KM program, integration would also strengthen results of the KM program by strengthening the community participation element, increasing community involvement in the health sector, and could have spill over benefits to other sectors.
Integration of the CSC into the KM program would streamline recruitment of facilitators, (since this is already a part of the KM program), reduce training costs (since training is also already an element of the KM program) and would dramatically reduce the supervision budget. CSCs would become an additional tool in the KM program but, under Scale-Up Model 1, would be repeated every 6 months, approximately, for a period of 1.5-2 years. Results of the CSCs would be disseminated at the local level, as well as passed on to the Ministry of Health for tracking results. Table 3: Costs of Integration with KM Model

15
KM Integrated Model (Scale-Up Model 1)
Non KM Integrated model (Scale-Up Model 1) )DFLOLWDWHXUV 0RELOLVDWHXUV )DFLOLWDWHXUV 0RELOLVDWHXUV
Initial Implementation in 1 Region (20 CSCs, including National Trainers and TA; not including international TA, which would be required throughout)
US$54,738 US$57,326 US$93,007 US$95,865
Two Unassisted Follow Ups, i.e. every 6 months following the Initial Implementation for a total of 2 years
US$10,836 US$16,859 US$11,070 US$34,582
Cost per CSC US$3,279 US$4,552 US$5,895 US$6,522 Cost per Region US$65,574 US$91,044 US$119,707 US$130,447 Cost over 22 Regions US$1,442,638 US$2,002,968 US$2,633,559 US$2,869,825
The KM program will be rolled out in 500 communes in 16 regions, with sustained support over the 5 year program. Integration with the KM tool could be undertaken initially in 4 regions, over 8 months, with existing technical assistance and training capacity. With existing capacity, 12 regions could be covered in approximately 40 months, including all follow-up activities, meaning that the entire country could be reached in just under 80 months. With the training of an additional 20 trainers and 4 technical assistants, for approximately US$15,000, 6 regions could be undertaken at a time, with 22 Regions covered in approximately 40 months. In a given KM region, the regional implementing NGO, contracted by SanteNet, would be responsible for managing the selection of communes (based on demand), recruiting community facilitators or mobilisers (depending on the model), as well as regional facilitators. A technical assistant, contracted by the Secretariat, would provide organizational and technical guidance to the NGO, and trainers (also contracted by the Secretariat) would provide training in the CSC to all facilitators. Three months after the initial implementation of the CSC, trainers and TA would return to assist in training and implementation of the follow-up phase. After this, regional and communal facilitators would be responsible for conducting follow-up activities at the commune level, as well as district and regional dissemination meetings. Depending on the capacity model used (Facilitateur or Mobilisateur),regional facilitators would have a more or less central role in the follow-up activities. Ideally, in the CSC as in the KM itself, sustained CSC interventions would provide the community with sufficient training and motivation that following the 2 year CSC intervention, communities would continue using the tool in the health sector, or might start applying it in other sectors.
3.C Strategic Coordinating Committee A third essential element of the institutionalization and scale up of the CSCs is the designation of a strategic coordinating committee that will be responsible for the strategic

16
direction of the CSCs. Topics addressed by this committee would include (but would not be limited to) regions to be covered (from amongst those being targeted by KM), and in what order. This committee would be specifically for the CSCs in the health sector, and would be comprised of representatives from the Ministry of Health, the SAc Secretariat, civil society, SanteNet, PGDI, the World Bank, and other funding partners.
��'���)XQGLQJ�RI�&6&V��As noted, in Phase 2 of the CSCs, the projected cost per CSC was approximately US$6,050, not including international technical assistance.�Based on lessons learned in Phase 2, it is estimated that CSCs in subsequent phases can be conducted for between approximately US$3,279 and US$4,552 per CSC, if integrated with the KM model, using Facilitateur and Mobilisateur models, respectively, with Scale-Up Model 1. For the ongoing pilots, funding has been secured under the PGDI 2 project, however, for substantial scale-up, additional funding will be required. This funding is not yet secured. SanteNet has indicated that supervision costs for communes already under the KM program can be absorbed into the SanteNet program. The remaining cost for each region is approximately, using Scale-Up Model 1, is US$65,574 or US$91,004, for Facilitateur or Mobilisateur regions, respectively, not including international technical assistance.
It would be the responsibility of the SAc secretariat to manage (although not fully raise or provide) the funding. Potential categories of funding are as follows, for one region (Scale Up Model 1, integrated with KM, Facilitateur and Mobilisateur models, including a training activity to build training and TA capacity): �Table 5: Potential breakdown of costs by activity, including training of trainers � 1 Region Scale Up Model 1,
KM22 Region Scale Up Model 1, KM
Facilitateur Mobilisateur Facilitateur Mobilisateur Preparation, Training activities, Trainers and TA (PGDI?)
$43,475 US$30,295 US$956,450 US$666,490
Training of Trainers (National capacity building) (PGDI?)
US$14,625 US$14,625 US$14,625 US$14,625
Activities (Other source of funding)
US$22,099 US$60,749 US$486,178 US$1,336,478
Supervision (SanteNet)
SanteNet SanteNet SanteNet SanteNet
Total for 1 US$80,199 US$105,669 US$1,457,253 US$2,017,593

17
region
����3URSRVHG�$FWLRQ�3ODQPhase 1: Train initial capacity and begin pilots of Community Score Cards in 2 regions of Madagascar to determine feasibility and applicability of the Community Score Card in the Malagache context. In this phase, 22 facilitators were trained in Antananarivo, who then conducted 4 CSCs in 2 regions, and over 140 additional civil society representatives were given introductory trainings in the CSC. (Completed)
Phase 2: Test different means for improving cost effectiveness, improving the impact of the tool, and improving results monitoring, through a 20 commune pilot in the Anosy region. (In Progress) Discussion Phase (In Progress): This phase is on ongoing discussion and planning phase. Key topics to be determined in this phase include:
- Structure for the scale-up of the CSCs, i.e., deepened interventions in many regions, gradually expanding, or less intensive interventions in all regions.
- Technical, organizational, and strategic coordination for future phase of the CSC - Funding of the CSC
The approach discussed in this paper is the result of consultations with the Ministry of Health, USAID, SanteNet, PGDI, and the World Bank, and will be discussed in a videoconference with these and other partners on November 25. The objective of that meeting is to define a strategy for next steps in the scaling up and institutionalization of the CSC. This discussion will be organized by the World Bank and PREA/PGDI. Phase 3: Based on the outcome of the Discussion Phase, Phase 3 would be the institutionalization and scaling up of the Community Score Card to a given number of regions.
Following agreement on integration of the CSC into the KM program, proposed next steps would include: ¾ A technical meeting between the Social Accountability Secretariat and the Ministry of
Health and SanteNet project to determine a detailed time line and implementation plan for the integration of the two tools.
¾ Integration of the CSC into the KM toolkit in 4 initial regions (simultaneous deployment in 2 regions, followed by deployment in another 2 regions simultaneously, plus 3 month follow-up in each of these regions). For each region, either a high or low capacity strategy (Facilitateur or Mobilisateur) would be adopted. Based on SanteNet’s timing, more regions might be added to the initial pilots, although this would require an additional training of trainers to ensure adequate training capacity, given that each region requires 4-5 qualified trainers.
¾ Under the existing KM model, in each region, the SanteNet program contracts with an NGO responsible for regional implementation. Communes would be selected based on expressed demand from communes, following district level presentation meetings by the contracted NGOs. In the KM program, community animators are trained to support the

18
KM approach at the commune level. For the CSC-targeted communes, CSC instruction would be added to the animators’ training. In additional, Regional facilitators would also be would be recruited to provide higher level support. This model would be adapted for higher or lower capacity regions, using either commune level facilitators or mobilisers
¾ Trainers and technical assistance would be contracted and funded by the SAc Secretariat.

19
¾ ANNEX 1: The Standard CSC Methodology: 7 basic steps
8 Standard Steps of a Community Score Card Preparatory Groundwork: 1. Preparatory Groundwork
a. Training of facilitators b. Briefing and obtaining permission from national level authorities at Ministry
of Health and Family Planning (i.e. MinSan, DDDS) c. Briefing and obtaining permission from regional authorities (i.e. DRSPF,
SSD) d. Contacting CSB II staff e. Facilitators obtain norms for CSB II from national MinSan authorities, to be
used and discussed in focus group and interface meetings. 2. Organization of the Community Gathering
a. Facilitators meet with community leaders (chef de Fokontany, traditional leaders, elders, religious leaders, civil society leaders) in CSB II catchment areas to discuss project, fix date, time, location of community meetings
3. Provider Focus Groups
a. Developing an Input Tracking Matrix o Facilitators meet with service providers from the CSB to compare
service norms to the actual situation b. Self-Evaluation by CSB staff (doctors, nurses, midwives, dispensatrices,
guardian) o Facilitators meet with service providers and guide service providers
through determining their indicators for service provision, ranking themselves on these norms and national norms, discuss justification for these scores and how to improve these scores
4. Community/Service users Scoring of Performance
a. Facilitators conduct focus groups with community members, trying to mobilize a cross-section of the community, and also emphasizing broad community mobilization. The number of focus groups depends on the commune, based on commune layout and distance of Fokontany.
b. A representative group is selected with guidance from the facilitators c. Facilitators meet with community members and guide them through
determining their indicators for service provision, ranking themselves on these norms and national norms, discuss justification for these scores and how to improve these scores
5. Interface Meeting between Community, Service Providers and other stakeholders a. Facilitators lead a discussion at the commune level ideally with at least the
CSB personnel and community members who were involved in Fokontany level discussions, but the meeting is open, and invitees include the commune, CoSan, CoGe, district, and local associations and NGOs.

20
b. Facilitators are responsible for compiling all user group discussion results into a composite table reflecting all results; on a volunteer basis, representatives from the user community present the different indicators, scores, reasoning, and suggestions for improvement to the assembled community members and CSB staff.
c. A representative from the CSB service providers presents results from service provider meetings to the assembled community members.
d. Facilitators guide discussion to determine an action plan for the following three months, including specific activities, timeline, and delegating responsibilities.
e. Facilitators work with participants to form a voluntary monitoring and implementation group, fixing their responsibilities for monitoring the action plan.
f. Facilitators work with the CSB staff and the communities to establish a representative, voluntary regional implementation committee in charge of convening once per month to monitor the action plan and determine any adjustments or activities that need to be undertaken to realize the objectives.
6. Regional Dissemination Meeting
a. Facilitators invite regional stakeholders (Chef de Region, regional ministry authorities (i.e. DRSPF for a health CSC), NGO representatives, civil society, and the media, community participants (users and CSB staff) for a presentation of CSC proceedings, results, and action plans. A segment of volunteers is selected from the Fokontany/commune level, with guidance from the facilitators to include both Chefs de Fokontany and CoSan representatives, but also to be gender and age balanced, to attend the regional dissemination meeting. This meeting serves to publicize differences between norms and reality, to alert the Ministry to perceptions of the CSB II, and to publicize the contract made in the action plan. In some instances, these presentations highlight certain shortcomings and responsibilities of the Ministry – such as lack of staffing, lack of infrastructure, lack of equipment, and where commitments have been made for improvement. �
7. Three to six months later, the evaluation process is repeated (as outlined above) to see whether any improvements have been registered.�

21
ANNEX 2 Results of Phase 1 CSC
The Phase 1 CSC had measurable results in a variety of aspects, including improved user satisfaction in terms of availability of drugs, human resources, CSB infrastructure, doctor/patient reception, cost of drugs, and overall levels of satisfaction. Levels of satisfaction were determined through focus group discussions with groups of users and service providers. In each CSB, one focus group was held with all service providers, but in each CSB catchment area multiple focus groups were held for service users, trying to target a selection of users in each of the accessible Fokontany served by a given CSB. In the first round of the CSC process, a total of seven focus groups were conducted in the communities served by the two CSBs in Haute Matsiatra and six in the communities served by the two CSBs in Boeny. These were then re-held during the follow up phase, meaning that a total of 26 focus groups were conducted in total. a. Overall Indicator Improvements After only three months, there were almost universal improvements in the level of user satisfaction in almost all of the indicators measured, in improved understanding and dialogue between service providers and service users, improved resource flow, and concrete improvements in CSB infrastructure. Overall levels of satisfaction are based on a number of standard indicators and indicators that users themselves developed, specific to their facilities. Therefore, as different CSB communities came up with different indicators, a dash in the tables above indicates an indicator not used by that particular CSB.

22
Table 6: Improvements in Health Care Users Level of Satisfaction of Most Common Indicators, February-June 2007 9
Region Haute Matsiatra Region Boeny Region
Indicators CSB IIMahaditra
%Change
CSB IIVohiposa
%Change
CSB IIAnkazaomborona
%Change
CSB IIAndranofasika
%Change
Availability of drugs 60% 78% 30% 44% 57% 30% 48% 61% 27% 37% 59% 59%
HumanResources/Staffing 62% 78% 26% 38% 40% 5% 40% 47% 18% 45% 50% 11%
Infrastructure 56% 78% 39% 46% 58% 26% 52% 60% 15% 24% 47% 96%
Reception 60% 81% 35% 72% 70% -3% 56% 71% 27% 52% 73% 40%
Cost of drugs - - - 42% 46% 10% 60% 66% 10% 42% 45% 7%
Availability ofmedical equipment 62% 74% 19% 40% 50% 25% 48% 58% 21% 37% 55% 49%
Overall Satisfaction 72% 85% 18% - 58% - 64% - 63%
N 31 55 100 53 152 67 67 73
9 In order to compile one indicator of degree of satisfaction, users ranked each indicator on a scale of 1 to 5. These rankings were then weighted to reflect thenumber of participants. A level of 100% meant that all users ranked the service at the highest level (5 = very satisfied). A level of 0% means that all usersranked the indicator at the lowest level (1=very dissatisfied).

23
An ‘overall satisfaction’ indicator was only examined in one of the four CSBs during the initial CSC and so changes could not be determined across all CSBs. This indicator will be more uniformly sampled in subsequent iterations of the CSC project; however, albeit not indicative across all the CSBs, the positive increase in user satisfaction from 72% to 85% percent - an 18% increase in how users rated satisfaction - is substantial. The following sections discuss specific improvements in some of the most commonly used indicators. b. Reception As is consistent with some other similar feedback mechanisms, one of the areas in which there was the most improvement was the perception of the reception that medical personnel extended to patients. This is likely because this was one of the indicators most immediately within the control of those involved in the CSC discussions. Some changes in perception were evident during even the first interface meetings. In many of the health centers, both doctors and patients initially felt frustrated with the way that doctors and health centers are overloaded; doctors felt they had too little time to give proper consultations, while patients felt that the waiting time was too long and at the end they received overly rushed consultations. In Vohiposa for example, the doctor complained that he had so many other related things to attend to in addition to attending to patients, while the patients complained that he was frequently not available and that there was not adequate care at night or on weekends. There was therefore need for dialogue between the community and the doctor in charge of the CSB to resolve these issues. Through the CSC process, users and service providers were able to discuss their concerns, and better understand the other’s constraints. CSBs have fixed times of operation but it was discovered during the CSC that most users were not aware of these opening hours. Users became less critical of the doctor and were more understanding of the pressure they were under when they better understood the constraints that the service providers face in the execution of their duties, including lack of adequate staff. As a result of dialogue, and resulting commitments (both sides better observing the hours of operation, for example) the follow-up stage saw markedly improved perception of how patients were received. c. Staffing Focus group discussions on human resource issues such as inadequate staff and non-payment of support staff by the commune, for instance, led, in some cases, to renewed community appeal to the Ministry of Health. In Mahaditra, for instance, when staffing issues were presented to the Ministry’s regional representatives at the regional dissemination meeting, the Ministry responded immediately; stating that they had not been aware of the concerns and immediately starting the process of reassigning a mid-wife to that CSB. In all CSBs, level of satisfaction with respect to staffing increased during the three month period. Also, as mentioned regarding the ‘acceuil’ indicator, the CSC process helped communities to become more aware of the hours of operation of CSBs; both in order to hold the doctor more accountable for being present during those hours, as well as to reduce demand on the

24
doctor outside of those hours. This may have also led to a rise in rates of satisfaction with the human resources of the CSBs. d. Availability of Drugs In all targeted CSBs, positive changes in perceptions of availability of drugs were recorded over the three month period. Strategies in the action plans included displaying lists of available drugs, improving management of drugs at the community level, and a 15 percent top-up of drug requests. In the case of Andranofasika, for instance, users reported that drugs were more available “through efforts deployed by the health personnel.” e. Infrastructure The CSCs empowered and assisted communities to take responsibility for some infrastructural and supply issues at the CSBs. For instance, following the initial CSC in Vohiposa, the mayor spearheaded a fundraising operation, code-named Operation Soupe,which raised 10,500 Ariary, as well as 570kg of paddi and 11 kg of white rice, which were then sold to raise an additional 381,300Ar (approximately US$160). This money raised was used to buy bricks and pay a mason to construct a shower. In addition, the community mobilized to build a toilet for the CSB. In Andranofasika, one of the problems identified was the lack of an enclosure around the CSBs. The community and their leaders; the mayor and Chefs de Fokontany and Fokonolona planted succulents around the perimeter of the CSB and as a result the level of satisfaction for infrastructure increased noticeably. Unfortunately, the tree planting was not done at the appropriate planting season and so many of the plants died.
Also in Andranofasika, in response to lack of accommodation - a commonly cited complaint at many of the CSBs - the head doctor helped to organize temporary accommodation for those that accompany patients to the CSB. Previously, lack of accommodation for family members made it very difficult for patients who could not travel on their own to visit the health center. f. Resource Flow In addition to increasing overall satisfaction with the functioning of health services, the CSCs also showed potential for improving the flow of municipal resources in some communities. In the CSB of Vohiposa, for instance, community members also discussed at the interface meeting that the indemnités paid to the guardian and the pharmacy dispenser were not sufficient, which jeopardized their ability to work at the CSB. The commune agreed to increase these amounts slightly. While this represented progress, the pharmacy dispenser and the guardian were still not fully paid staff, and the indemnités were still seen as insufficient. A request was made to the Ministry of Decentralization for assistance; the results of this are still pending.
25
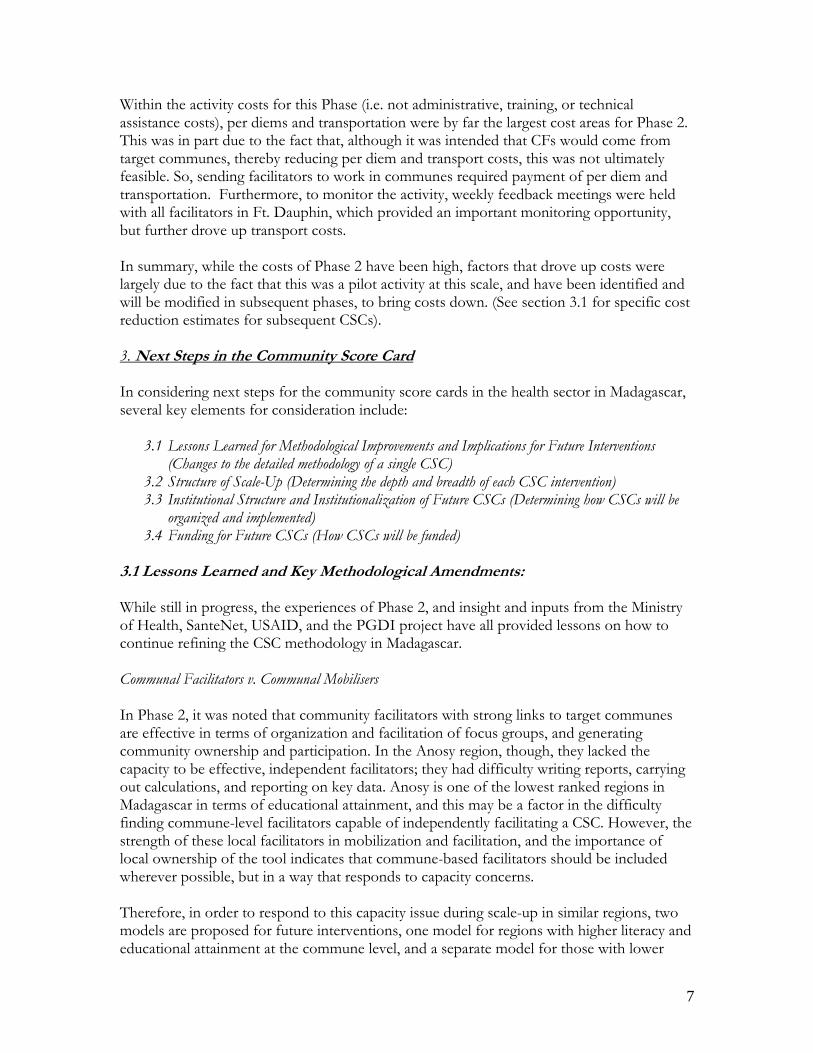
ANNEX 3 Scale-Up Model Monthly and Regional Plans
Scale-Up Model 1 with existing technical Capacity: The model below demonstrates a potential timeline using existing technical capacity (10 trainers, 2 TAs) RN = Region N II = Initial Implementation FU = Follow-Up LF = Local Follow-Up (i.e. without assistance of Trainers or TA, but with the assistance of RFs)
Table 7: Scale Up Model 1, with Existing Capacity Month R1 R2 R3 R4 R5 R6 R7 R8 R9 R10 R11 R12 1, 2 II II 3, 4 II II5,6 FU FU 7,8 FU FU 9,10 II II11, 12 II II13, 14 LF LF FU FU 15,16 LF LF FU FU 17,18 II II 19,20 II II 21,22 LF LF LF LF FU FU 23,24 LF LF LF LF FU FU 25,26 27,28 29,30 LF. LF. LF LF 31,32 LF LF LF LF 33,34 35,36 37,38 LF LF 39,40 LF LF
26
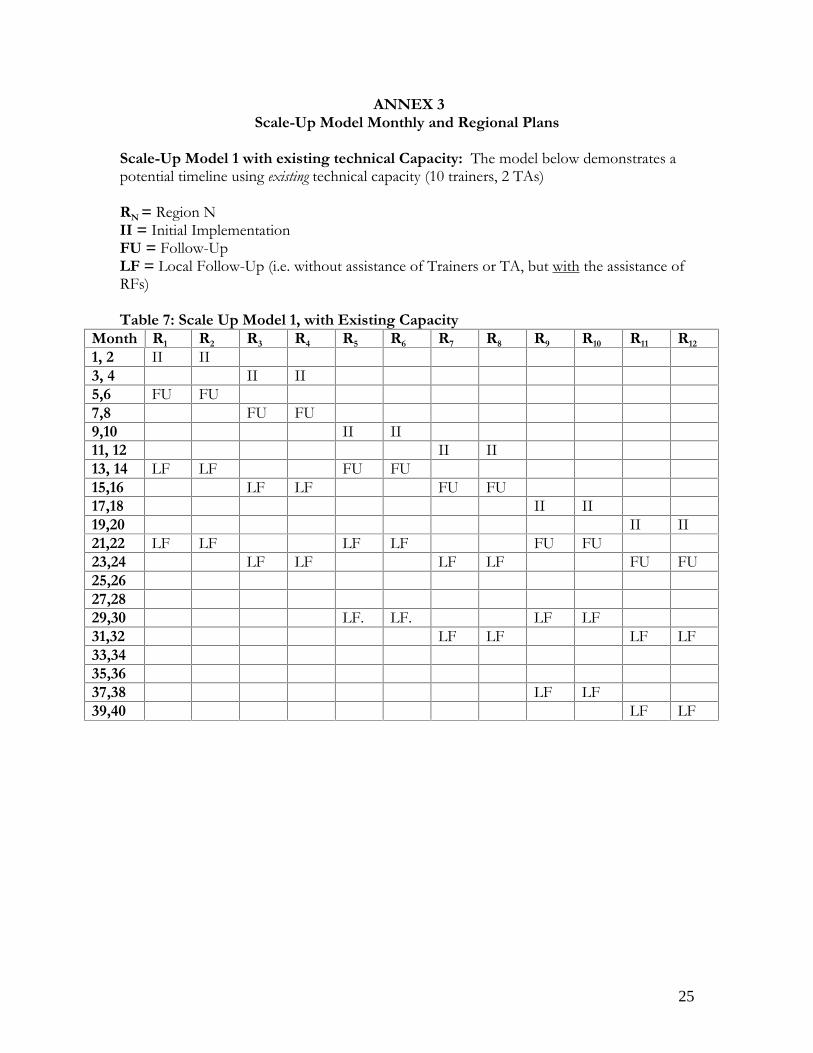
ANNEX 3 (cont’d)Scale-Up Model Monthly and Regional Plans
Scale-Up Model 1 with additional technical Capacity: The model below demonstrates a potential timeline using potential additionalcapacity, following a national training sessions (total of 30 trainers, 6 TAs)RN = Region NII = Initial ImplementationFU = Follow-UpLF = Local Follow-Up (i.e. without assistance of Trainers or TA, but with the assistance of RFs)
Table 8: Scale-Up Model 1, with Additional CapacityMonth R1 R2 R3 R4 R5 R6 R7 R8 R9 R10 R11 R12 R13 R14 R15 R16 R18 R19 R20 R21 R22
1, 2 II II II II II II3, 45,6 FU FU FU FU FU FU7,8 II II II II II II9,1011, 12 FU FU FU FU FU FU13, 14 LF LF LF LF LF LF II II II II II II15,1617,18 FU FU FU FU FU FU19,20 LF LF LF LF LF LF II II II21,22 LF LF LF LF LF LF23,24 FU FU FU25,26 LF LF LF LF LF LF27,28 LF LF LF LF LF LF29,3031,32 LF LF LF33,34 LF LF LF LF LF LF35,3637,3839,40 LF LF LF
27
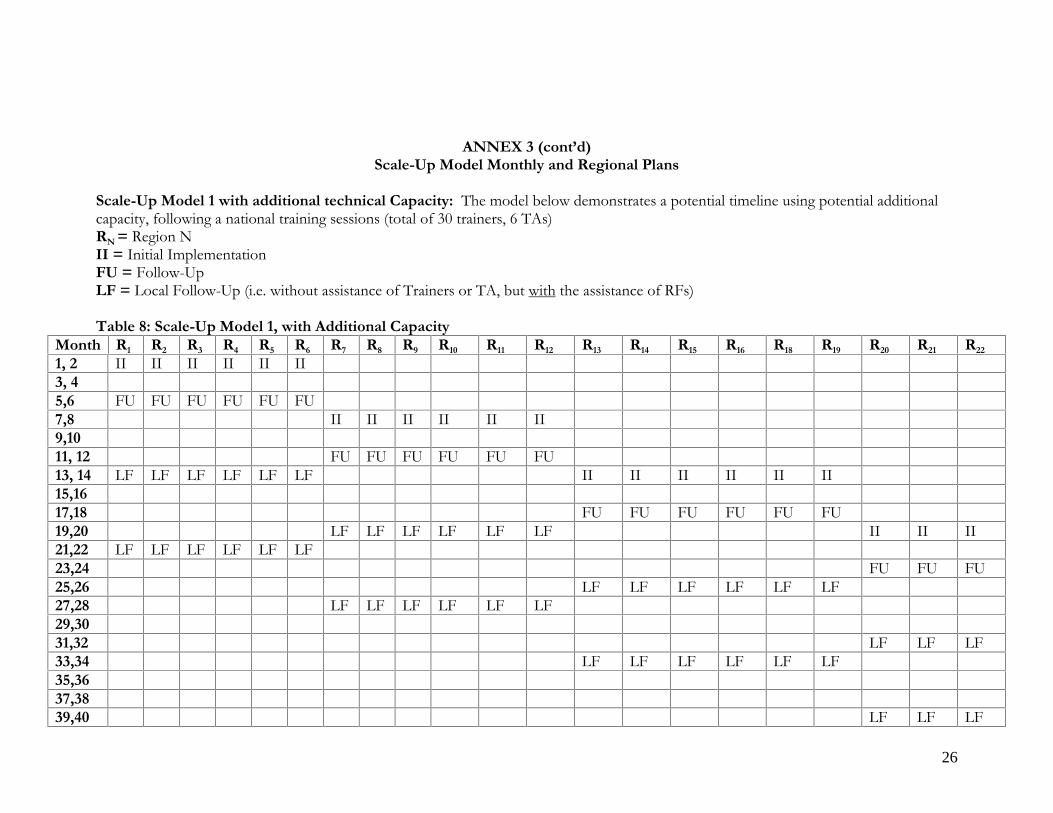
ANNEX 4 The CSC Process, Roles and Responsibilities for Regional Roll-out in Madagascar
1. Preparatory Groundwork:
a. National Preparation: National implementing partner obtains norms for CSB II from national MinSan authorities, to be used and discussed in focus group and interface meetings.
b. Regional NGO/government partner obtains letter of intent from Ministry of Health ensuring support for the program.
c. Decision reached with Ministry of Health which indicators and objective health criteria will be monitored.
d. Regional Preparation: e. CSC regional coach works with KM coordinating NGO on organization of
regional CSC. f. CSC regional coach with regional NGO conducts district-level presentation
meetings to civil society, mayors, health center staff, and other local authorities to solicit demand for CSCs.
g. Following expressions of demand, animators are recruited from target communes (or already selected KM animators are identified for further CSC training). Regional facilitators are recruited, with representation from the district level.
2. Training of CSC Regional and Communal Facilitators. a. Facilitators/mobilizers, depending on capacity model being used, are provided
with up to 10 days of CSC training, including theoretical and field-based training. 3. Implementation of the CSC:
a. Communal Facilitators/mobilizers return to communes and begin widespread sensitization on the CSC, to mobilize maximum diversity of participants in CSCs. Regional Facilitators, circulate between defined number of communes simultaneously, conducting CSCs – evaluation by users, design of input tracking matrix and auto-evaluation by prestataires, interface meeting. Follow-up committees are put in place in the communities, with Communal Facilitators responsible for reporting, and transmission of reports to the Ministry of Health.
4. Regional dissemination meeting, including users and service providers from all targeted communes, regional and district level authorities, civil society, media.
5. Every month, communal facilitators facilitate meeting of the commune-level follow-up committee.
6. Follow-up: Three months later, a brief training is conducted for all regional and communal facilitators and follow-up of the CSC is conducted, with communal and regional participation. Results from this phase are sent to the district and regional health authorities for M&E.
7. For Scale-Up Model 1: CSCs are repeated twice – once 6 months after the initial follow-up, and again 6 months later.

28
ANNEX 5 Models for scaling up CSC Capacity (Phase 3)
ANNEX 5.A.: Sample Weekly Schedule for First 20 CSCs in Region X Table 9: Weekly Calendar for Regional CSC Activity M T W Th F Sa Su M T W Th F Sa Su M T W Th F Regional Facilitators
Trav
el
CSC Communes 1-5
Trav
el
CSC Communes 6-10 Tr
avel
Off
CSCs Communes 11-15 Tr
avel
Community Mobilisers CSCs 1-5
Mobilisation of participants, authorities
CSC Communes 1-5
Community Mobilisers 6-10
Mobilization of participants, authorities
CSC Communes 6-10
Community Mobilisers 11-15
Mobilization of participants, authorities
CSCs Communes 11-15
Community Mobilisers 16-20
Mobilization of participants, authorities