sbg in cancer and oral mucositis - biotec.no · market cap of ~nok 520m per 20 august 2009 started...
TRANSCRIPT
Immunity for Life TM
Sven Rohmann
VP Business Development
SBG in Cancer and Oral Mucositis
Disclaimer
This Presentation includes and is based, inter alia, on forward-looking information and statements that aresubject to risks and uncertainties that could cause actual results to differ. These statements and thisPresentation are based on current expectations, estimates and projections, which generally are identifiable bystatements containing words such as ”expects”, ”believes”, ”estimates” or similar expressions. Important factorsthat could cause actual results to differ materially from those expectations include, among others, generaleconomic and industry conditions in markets which are expected to be major markets for Biotec PharmaconASA’s products, as well as risks and uncertainties related to product development, regulatory approvals,commercial partnerships, the outcome of intellectual property rights litigation and the competitive situation.
Although Biotec Pharmacon ASA believes that its expectations and the Presentation are based upon reasonableassumptions, it can give no assurance that those expectations will be achieved or that the actual results will beas set out in the Presentation. Biotec Pharmacon ASA is making no representation or warranty, expressed orimplied, as to the accuracy, reliability or completeness of the Presentation, and neither Biotec Pharmacon ASAnor any of its directors, officers or employees will have any liability to you or any other persons resulting fromyour use of the information contained herein.
This presentation was prepared for the European Cancer Cluster Partnering Meeting in Toulouse, on September3rd and 4th 2009, and the information contained within will not be updated in this presentation. The followingslides should be read and considered in connection with other information provided by the company.
No shares of Biotec Pharmacon are being offered in connection with this presentation and no such shares havebeen registered under the U.S. Securities Act of 1933, as amended (the "Act"), and such shares may not beoffered or sold in the United States absent registration or an applicable exemption from the registrationrequirements of the Act.
2

Biotec Pharmacon – Company facts
Market Cap of ~NOK 520m per
20 August 2009
Started in animal health in
1990, with particulate beta
glucans against infectious
diseases in fish
Established pharmaceutical
operation in 2000, with the
development of soluble beta
glucan (SBG)
Consumer Health and Marine
Biochemicals Businesses are
further assets.3
8
10
12
14
16
18
20
22
24
01/1
2/0
8
01/0
1/0
9
01/0
2/0
9
01/0
3/0
9
01/0
4/0
9
01/0
5/0
9
01/0
6/0
9
01/0
7/0
9
01/0
8/0
9
Biotec Pharmacon(OSE ticker "Biotec")
Biotec Pharmacon Oslo Børs, Pharma&Biotech

Pharmaceutical conceptSBG regulates the innate immune system
SBG (Soluble Beta Glucan)
a unique/proprietary, highly
bioactive, soluble beta-1,3/1,6-
glucan
from cell walls of yeast
alien to the human body
How it works:
SBG has regulating and
normalizing effect on
macrophages and other
immune-competent cells.
enhances the efficacy of the
adaptive immune system4

Mechanisms of action: CellsSBG simultaneously branches into receptors
on e.g. macrophages
5
CR3 (CD11b/CD18)-receptor SBG
Toll like receptor 2/6
AB
C
Dectin-1
“Human b-glucan receptor”

Mechanism of actionb-Glucan binding of Dectin-1 receptor results in activation of
macrophages
6
Naive macrophage
CR
Target cell
=Tumor antigen
mAb C3b
LIMITED ACTION
C3b
Target cell
mAb
(1-n)= beta-glucan
ACTION
Cytokine
production
Acute inflam.
Phagocytosis
Expression of
co-factors
FcR
MacrophageDectin-1
FcR
CR
SBG

Mechanism of actionb-Glucan binding of complement receptor 3 results in iC3b-
mediated activation of granulocytes
7
granulocyte
CD11bCD18
granulocyte
Target cell
=Tumor antigen
mAb iC3b
NO ACTION
iC3b
Target cell
mAb
(1-n)= beta-glucan
ACTION
Phagocytosis
Respiratory burst
Cytotoxicity
FcR
CD18
Cytokines
from activated MØ
FcRCD11b
+ SBG
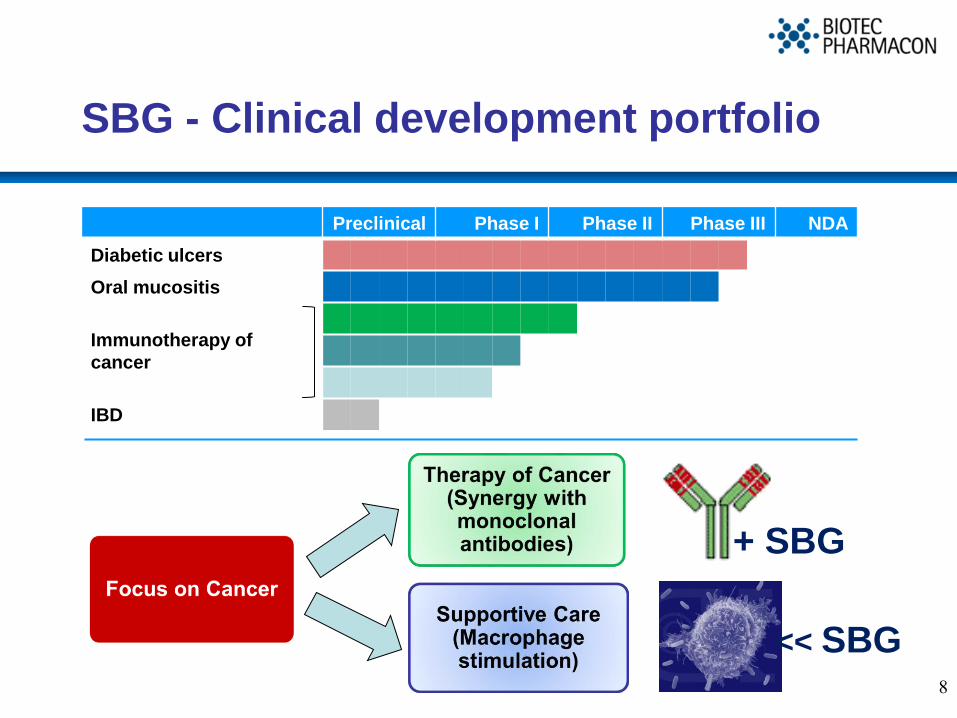
SBG - Clinical development portfolio
8
Preclinical Phase I Phase II Phase III NDA
Diabetic ulcers
Oral mucositis
Immunotherapy of
cancer
IBD
<< SBG
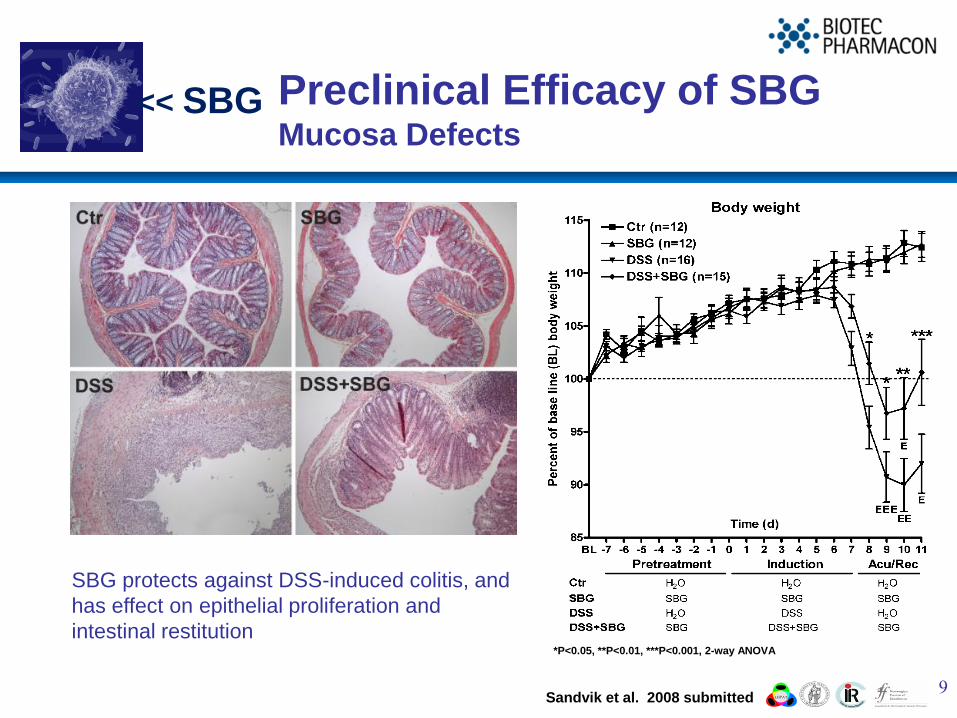
Preclinical Efficacy of SBG Mucosa Defects
9
*P<0.05, **P<0.01, ***P<0.001, 2-way ANOVA
SBG protects against DSS-induced colitis, and
has effect on epithelial proliferation and
intestinal restitution
Sandvik et al. 2008 submitted
<< SBG
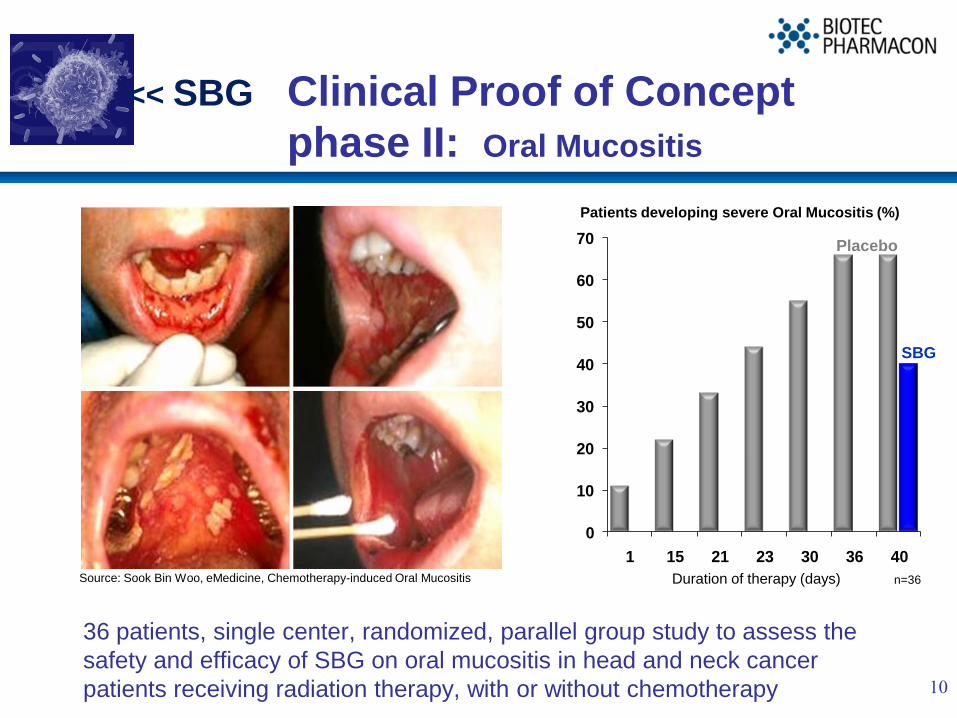
Clinical Proof of Concept
phase II: Oral Mucositis
36 patients, single center, randomized, parallel group study to assess the
safety and efficacy of SBG on oral mucositis in head and neck cancer
patients receiving radiation therapy, with or without chemotherapy 10
0
10
20
30
40
50
60
70
1 15 21 23 30 36 40
SBG
Placebo
Patients developing severe Oral Mucositis (%)
Duration of therapy (days) n=36Source: Sook Bin Woo, eMedicine, Chemotherapy-induced Oral Mucositis
<< SBG

Clinical phase 2008 2009 2010
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Phase III, Europe Phase III, Eastern Europe 2
nd study put on hold awaiting results from the 1
st study
Pivotal Trial - Phase IIIOral Mucositis
11
Patient population
• Number of patients; n=130
• 129 patients enrolled
• No changes made after sample size
reassessment
Primary endpoint
• Incidence of OM CTCgrade 3/4 at any time of
commencement of radiotherapy up to 5 days
after radiotherapy ceases.
Secondary endpoints
• Time from commencement of Radiotherapy to
onset of OM CTC grad 3/4 ;
• Duration of OM CTC grade 3/4
• Overall incidence of OM CTC grade 2, 3 and 4
Blue area = periods of patient inclusion, black areas = periods of study completion and reporting
Eligible for orphan drug designation in Europe.
<< SBG

MoA – Synergy with mAbsCancer
12
Synergy of p.o. barley beta-
glucan and antibodies against
tumor associated antigen in nude
micea) Melanoma xenografts in nude mice
b) Epidermoid carcinoma xenografts
c) Human breast carcinoma xenografts
c) Herceptin
b) anti-EGF-R
a) anti-GD3
Additional Finding:
Subcutaneous Daudi lymphoma was
significantly suppresses when rituximab
was administered with oral BG (not shown)
+ SBG
Cheung N-K et al. Cancer Immunol Immunother (2002) 51:557-564
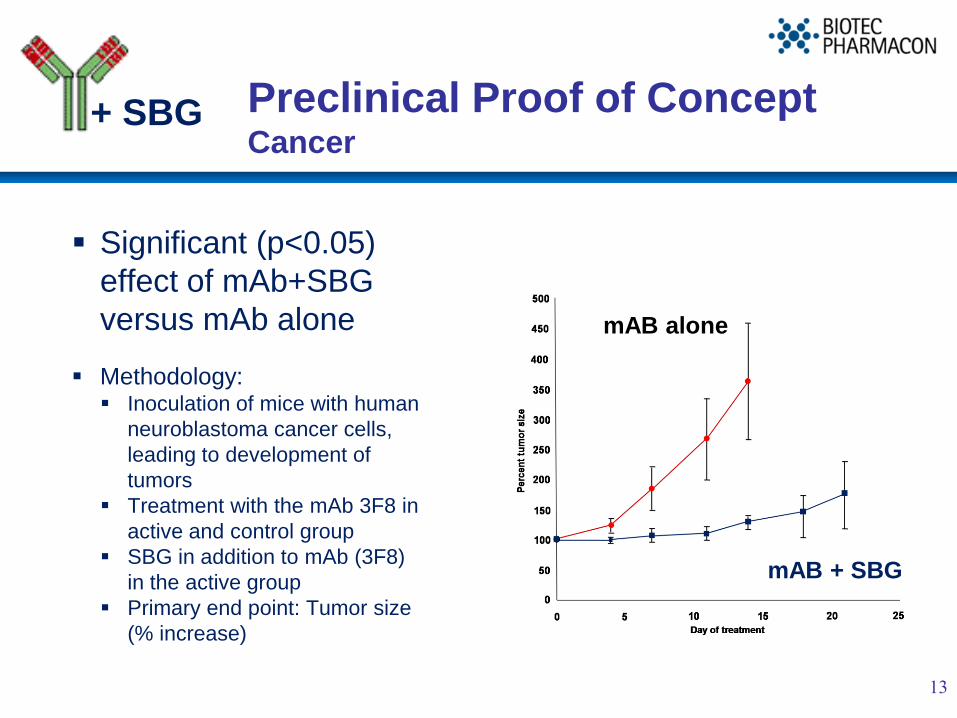
Preclinical Proof of ConceptCancer
Significant (p<0.05)
effect of mAb+SBG
versus mAb alone
Methodology: Inoculation of mice with human
neuroblastoma cancer cells,
leading to development of
tumors
Treatment with the mAb 3F8 in
active and control group
SBG in addition to mAb (3F8)
in the active group
Primary end point: Tumor size
(% increase)
13
mAB alone
mAB + SBG
+ SBG
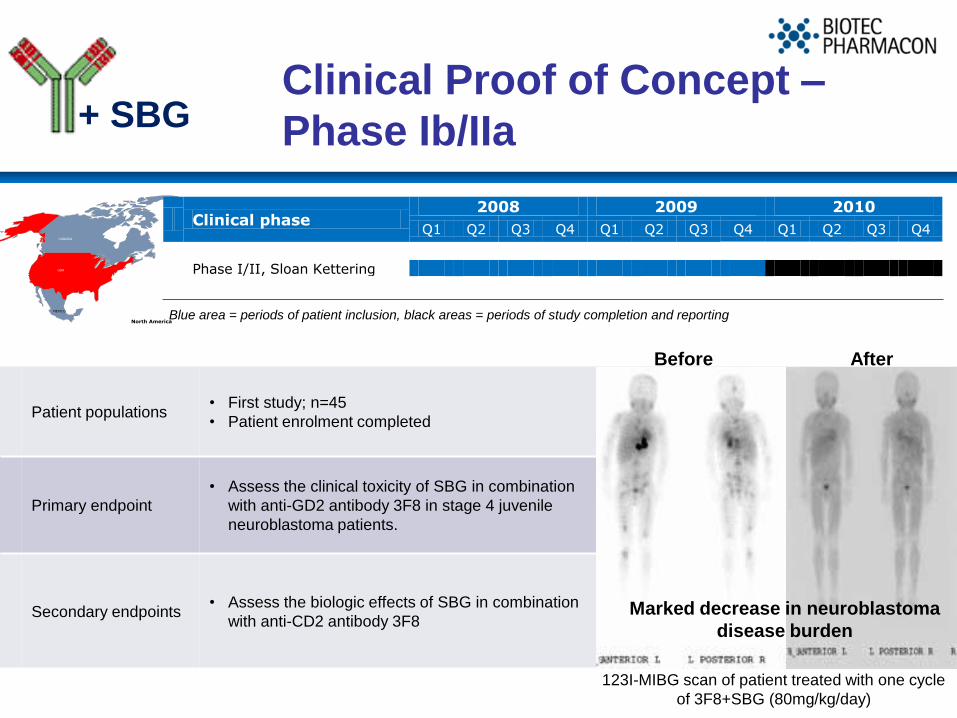
Clinical phase 2008 2009 2010
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Phase I/II, Sloan Kettering
Patient populations• First study; n=45
• Patient enrolment completed
Primary endpoint
• Assess the clinical toxicity of SBG in combination
with anti-GD2 antibody 3F8 in stage 4 juvenile
neuroblastoma patients.
Secondary endpoints• Assess the biologic effects of SBG in combination
with anti-CD2 antibody 3F8
Blue area = periods of patient inclusion, black areas = periods of study completion and reporting
Clinical Proof of Concept –
Phase Ib/IIa
Before After
123I-MIBG scan of patient treated with one cycle
of 3F8+SBG (80mg/kg/day)
Marked decrease in neuroblastoma
disease burden
+ SBG
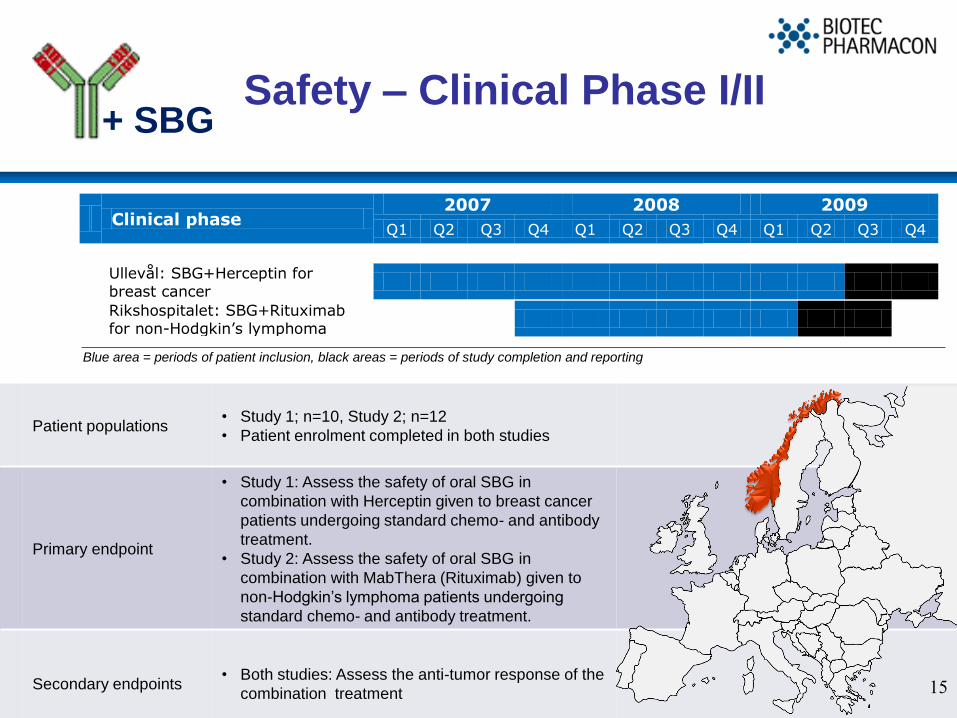
Clinical phase 2007 2008 2009
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Ullevål: SBG+Herceptin for breast cancer
Rikshospitalet: SBG+Rituximab for non-Hodgkin’s lymphoma
Patient populations• Study 1; n=10, Study 2; n=12
• Patient enrolment completed in both studies
Primary endpoint
• Study 1: Assess the safety of oral SBG in
combination with Herceptin given to breast cancer
patients undergoing standard chemo- and antibody
treatment.
• Study 2: Assess the safety of oral SBG in
combination with MabThera (Rituximab) given to
non-Hodgkin’s lymphoma patients undergoing
standard chemo- and antibody treatment.
Secondary endpoints• Both studies: Assess the anti-tumor response of the
combination treatment
Safety – Clinical Phase I/II
15
Blue area = periods of patient inclusion, black areas = periods of study completion and reporting
+ SBG

Partnering opportunities
In partnering discussions with both global and
regional partners
Presently all partnering possibilities open,
including:
Commercial partnering opportunities for
SBG for Oral mucositis
R&D Collaborations on the use of SBG
together with mAbs
R&D Collaborations on the use of SBG
together with cancer vaccines
16
+ SBG
<< SBG
Summary
SBG works
Established Proof of Concept on the beneficial effects of SBG
in supportive care in cancer (OM);
Established clinical data suggesting a potentially important
role of SBG in cancer treatment when combined with
antibodies.
Advanced clinical program in Europe and USA
Ongoing partnering discussions
Open to commercial and R&D partnerships on treatment of
oral mucositis and cancer.
17

18
Contact:
Sven Rohmann, MD, PhD
Mobile: +41 79 577 8895
E-mail: [email protected]
Biotec Pharmacon ASA,
Strandgata 3
N-9008 Tromso, Norway,
or
Biotec Pharmacon ASA,
Drammensveien 149
N-0277 Oslo, Norway
www.biotec.no
Appendix
Financials and Management

21
Financial Highlights
Q2 09 Q2 08 H1 09 H1 08 2008 Q1 09
Revenue 11.4 14.3 23.7 26.2 51.7 12.3
EBITDA, non-pharma 0.2 -1.1 -0.6 -3.8 -5.6 -0.8
EBITDA, pharma R&D -20.1 -10.0 -36.0 -21.0 -72.0 -15.9
EBITDA, unallocated -0.9 -3.5 -1.1 -5.1 -10.3 -0.2
EBITDA, total -20.8 -14.6 -37.7 -29.9 -87.9 -16.9
EBIT -21.6 -15.4 -39.2 -31.5 -91.3 -17.6
Net financials 1.0 2.0 2.5 3.9 8.3 1.5
Profit before tax, continued operations -20.6 -13.4 -37.8 -27.7 -83.0 -16.1
Net profit, continued operations -20.6 -13.4 -36.8 -27.7 -78.8 -16.1
Net profit, discontinued operations - 1.0 - 0.7 26.6 -
Net result for the period -20.6 -12.3 -36.8 -26.9 -52.2 -16.1
22
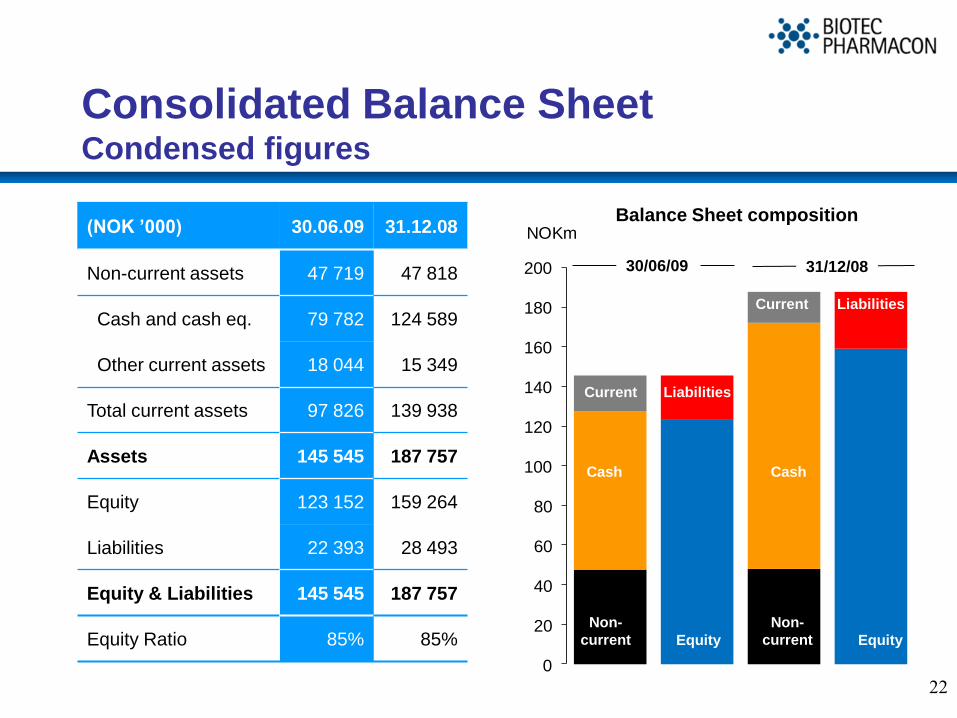
Consolidated Balance Sheet Condensed figures
(NOK ’000) 30.06.09 31.12.08
Non-current assets 47 719 47 818
Cash and cash eq. 79 782 124 589
Other current assets 18 044 15 349
Total current assets 97 826 139 938
Assets 145 545 187 757
Equity 123 152 159 264
Liabilities 22 393 28 493
Equity & Liabilities 145 545 187 757
Equity Ratio 85% 85%
0
20
40
60
80
100
120
140
160
180
200
NOKm
Equity
Liabilities
Non-
current
Current
31/12/0830/06/09
Balance Sheet composition
Cash
Current
Cash
Non-
current Equity
Liabilities
Management and Board of Directors
Management
Lars Viksmoen - CEO
Jørn Lunde - CFO
Rolf Engstad – CSO
Sven Rohmann – VP Business Development
Britt Olaussen – VP Clinical Development
Kari Skinnemoen – VP Regulatory Affairs
Steinar Børresen – VP Manufacturing
Arvid Vangen – VP Finance & Adm
Arvid Lindberg – Managing Director
Immunocorp Consumer Health
Board of Directors
Svein Mathisen (Chairman)
Jan Gunnar Hartvig
Ingrid Alfheim
Kari Stenersen
Ingrid Wiik
Arne Handeland
Morten Eide (Employee rep.)
Please refer to www.biotec.no for
more information
23

Further Pharmaceutical
concept Data
25
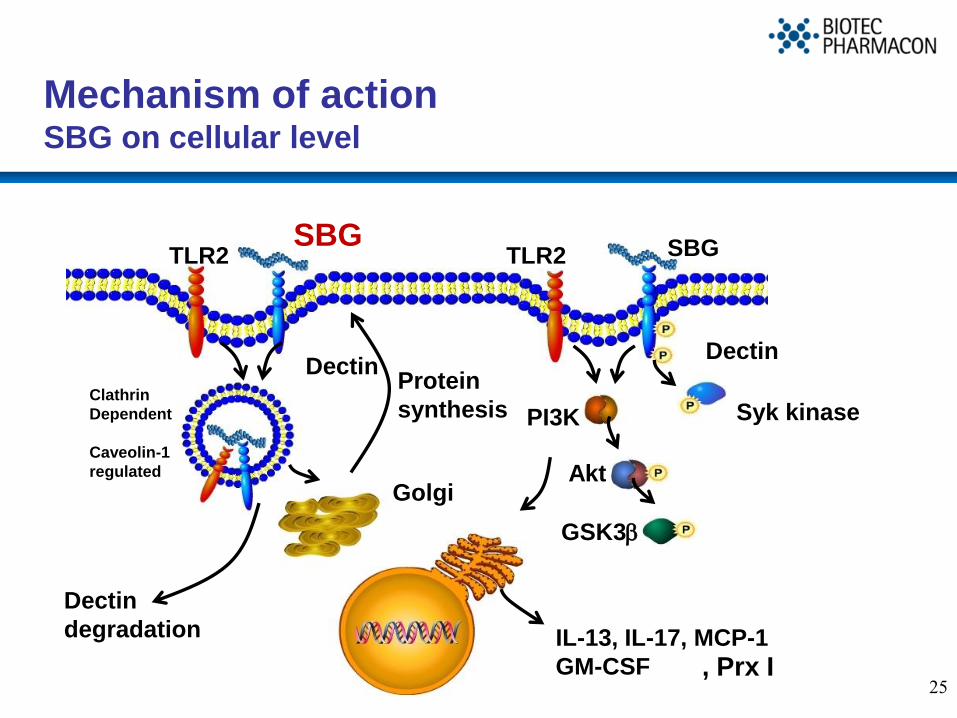
Mechanism of actionSBG on cellular level
TLR2
Dectin
SBG
Clathrin
Dependent
Caveolin-1
regulated
Golgi
Syk kinasePI3K
Akt
GSK3b
Dectin
degradation IL-13, IL-17, MCP-1
GM-CSF
TLR2 SBG
Dectin
Protein
synthesis
, Prx I
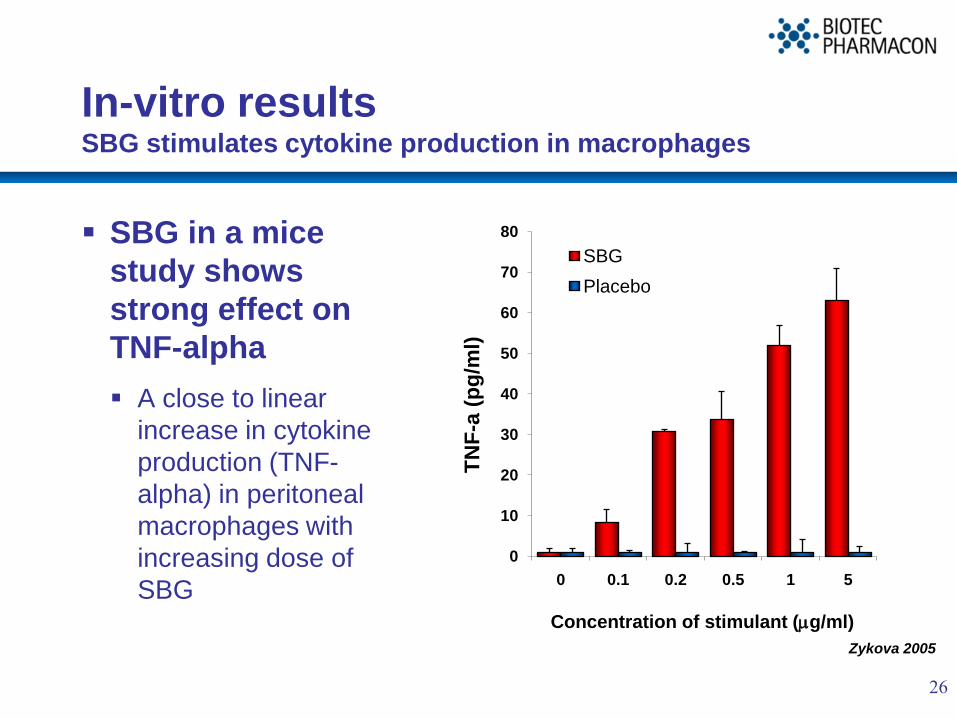
In-vitro resultsSBG stimulates cytokine production in macrophages
SBG in a mice
study shows
strong effect on
TNF-alpha
A close to linear
increase in cytokine
production (TNF-
alpha) in peritoneal
macrophages with
increasing dose of
SBG
26
Zykova 2005
0
10
20
30
40
50
60
70
80
0 0.1 0.2 0.5 1 5
TN
F-a
(p
g/m
l)
Concentration of stimulant (mg/ml)
SBG
Placebo
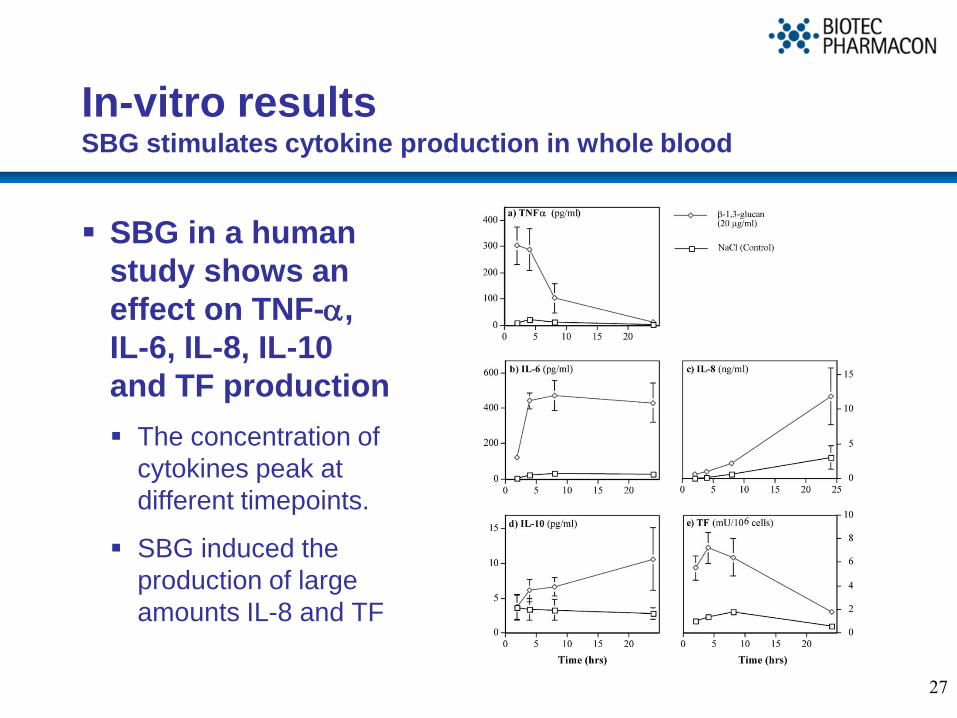
In-vitro resultsSBG stimulates cytokine production in whole blood
SBG in a human
study shows an
effect on TNF-a,
IL-6, IL-8, IL-10
and TF production
The concentration of
cytokines peak at
different timepoints.
SBG induced the
production of large
amounts IL-8 and TF
27

Toxicology/safety in animalsSBG in in-vitro and in-vivo animal studies
Very favourable toxicity
No potential clinical hazard identified for proposed
human use, for either topical or oral administration
28
No potential found for mutagenicity or genotoxicity
Minimal lethal dose could not be found in toxicity studies in
rodents or non-rodents
NOEL dose of 200 mg/kg/day after oral administration for 28
days in rats, 300mg/kg/day in dogs
Demonstrated good local tolerance after topical application
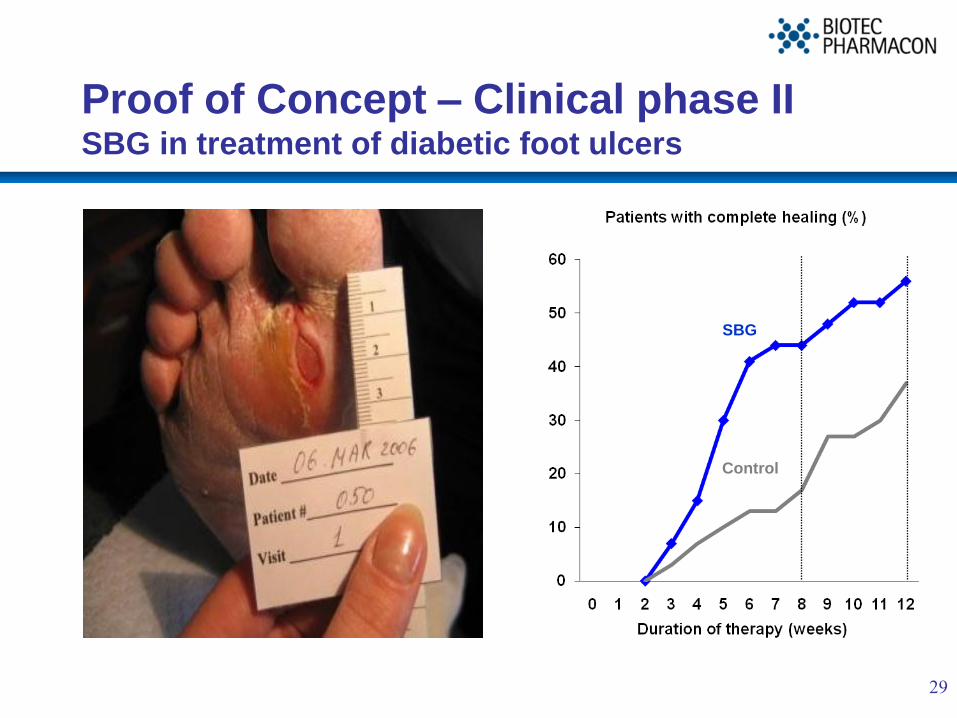
Proof of Concept – Clinical phase IISBG in treatment of diabetic foot ulcers
29
SBG
Control
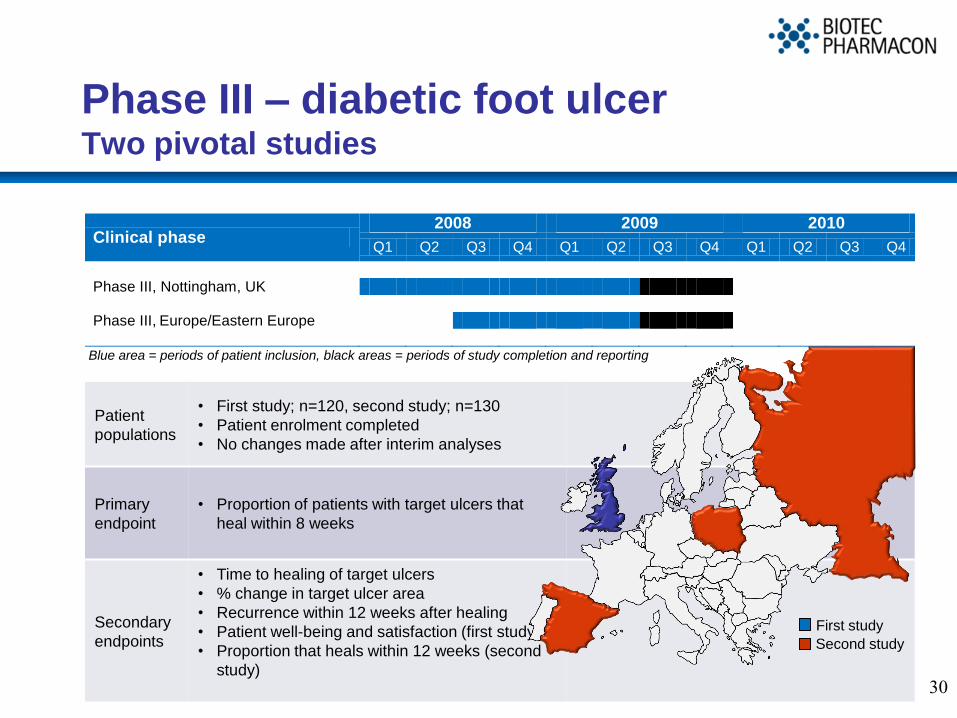
Patient
populations
• First study; n=120, second study; n=130
• Patient enrolment completed
• No changes made after interim analyses
Primary
endpoint
• Proportion of patients with target ulcers that
heal within 8 weeks
Secondary
endpoints
• Time to healing of target ulcers
• % change in target ulcer area
• Recurrence within 12 weeks after healing
• Patient well-being and satisfaction (first study)
• Proportion that heals within 12 weeks (second
study)
Phase III – diabetic foot ulcerTwo pivotal studies
30
Clinical phase 2008 2009 2010
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Phase III, Nottingham, UK Phase III, Europe/Eastern Europe
Blue area = periods of patient inclusion, black areas = periods of study completion and reporting
First study
Second study

Diabetic foot ulcers Milestone schedule
31
YTD
• Completed patient inclusion in 1st phase III study
• Performed interim study in 2nd phase III study
• Completed patient inclusion in 2nd phase III study
Q3 2009• Completion of treatment and follow-up programs
• Data collection and analysis
Q4 2009 • Final results expected to be ready from both studies
July-2010• Filing for market approval in Europe, in a decentralized
process with UK as reference member state