safety training potential reducing children's · swimming lessons may increase the risk of...
TRANSCRIPT

Injury Prevention 1995; 1: 228-233
Water safety training as a potential means ofreducing risk of young children's drowning
Kenneth N Asher, Frederick P Rivara, Deborah Felix, Linley Vance, Rosemary Dunne
AbstractObjectives-To determine the effects oftraining in swimming and water safety onyoung preschool children's ability torecover safely from a simulated episodeof falling into a swimming pool.Design-Randomized trial of 12 or eightweeks' duration water safety and swimm-ing lessons for children 24 to 42 monthsold.
Outcome measures-Swimming ability,deck behavior, water recovery, and swim-ming to side after jumping into pool weremeasured before, during, and after thetraining program.
Results-109 children completed thestudy (61 in the 12 week group, 48 in theeight week group). The average age was34-2 months, 54% were male. Swimmingability, deck behavior, water recovery,and jump and swim skills improved overbaseline levels in both groups. By the endof training, the 12 week group improvedmore than the eight week group only inswimming ability. Improvements inwater recovery and jump and swim skillswere associated positively with changes inswimming ability.Conclusions-Swimming ability andsafety skills of young preschool childrencan be improved through training. Suchprograms may offer some protection forchildren at risk ofdrowning and there wasno indication that this program increasedthe risk of drowning. However, pool fenc-ing, other barriers around water, andparental supervision still remain themost important prevention strategies toreduce drowning in young children.(Injury Prevention 1995; 1: 228-233)
Keywords: water safety training, drowning.
Each year 700 children under 5 years old diefrom drowning in the United States, makingdrowning the third leading cause of death inthis age range.'2 Of these, children between 2and 3 years are at greatest risk.'6 Near drown-ing carries a high risk of serious neurologicalsequelae in survivors, with nearly all whorequire cardiopulmonary resuscitation dyingor being left with severe brain injury. Thus,primary prevention remains the most effectivetactic to significantly reduce the risk of mor-tality and serious morbidity from drowning.To address this problem, passive approaches
such as four sided fencing with self latching
gates have received attention.5 Despite theirproven effectiveness and their attractiveness aspassive prevention strategies, these have notbeen widely adopted in the United States.'Another popular but unproved preventionstrategy is teaching swimming and water safetyskills to young children. This has beenvigorously promoted by the Red Cross, theYMCA, and other organizations, and widelypublicized by the mass media. Nevertheless, itseffectiveness in reducing mortality or mor-bidity has not been adequately evaluated.78Some experts have even raised concerns thatswimming lessons may increase the risk ofdrowning by lessening toddlers' fear of thewater and creating a false sense of security inparents.9 Adverse effects of swimming oninfants and toddlers have been reported, in-cluding water intoxication'0 and various infec-tious diseases." For these reasons, manyorganizations (including the AmericanAcademy of Pediatrics) have hesitated to sup-port water safety and swimming lessons foryoung children.The purpose of this study is to begin to
investigate the possibility of reducing pre-school children's risk ofdrowning by providingtraining in swimming skills and water safety. Itis not feasible to conduct a prospective trialwith decreased drowning episodes as an out-come. The annual rate of drowning in this agegroup is approximately six per 100 000.6 Thus,over one million children would have to bestudied to observe a 50% risk reduction. Anincrease in water safety skills, and recoveryfrom a simulated episode of falling into a poolare, therefore, used as a proxy for decreaseddrowning risk.The study was based upon the following
hypotheses. First, swimming ability would bepositively related to the degree of participationin the training program. Second, children withwater safety training would exhibit saferbehavior at the poolside than children with lesstraining. Third, children with more trainingwould act more competently in simulated highrisk situations than children with less training.Fourth, children's swimming ability would bepositively related to their water safety behavior.Fifth, children's developmental and behavioralcharacteristics would have independent effectson water safety behavior before training, andon changes due to instruction.
Subjects and methodsSUBJECTSThis study population consisted of childrenbetween 24 and 42 months of age at entry intothe study. Children and families were recruited
Harborview InjuryPrevention andResearch Center,Departments ofPediatrics andEpidemiology,University ofWashington andChildren's HospitalMedical Center,Seattle, Washington,USAKN AsherFP RivaraD FelixL VanceR Dunne
Correspondence and requestsfor reprints to:Dr KN Asher, HarborviewInjury Prevention andResearch Center, 325 NinthAvenue, ZX-IO, Seattle, WA98104, USA.
228
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from
Water safety training as a potential means of reducing risk ofyoung children's drowning
by letters at the child care centers and follow uptelephone calls over an 18 month period frommiddle income Seattle area child care centersnear public pools chosen for the study. We feltthat families with more limited resourceswould have difficulty coming to all the trainingand testing sessions. Children were onlyaccepted if they had no prior swimming train-ing and no chronic medical or developmentaldisability, based on parents' completion of therevised Denver Prescreening DevelopmentalQuestionnaire.'2 Participants received $50upon completion of the last measures. Thisstudy was approved by the human subjectsreview committees of Children's Hospital andMedical Center and the University ofWashington.
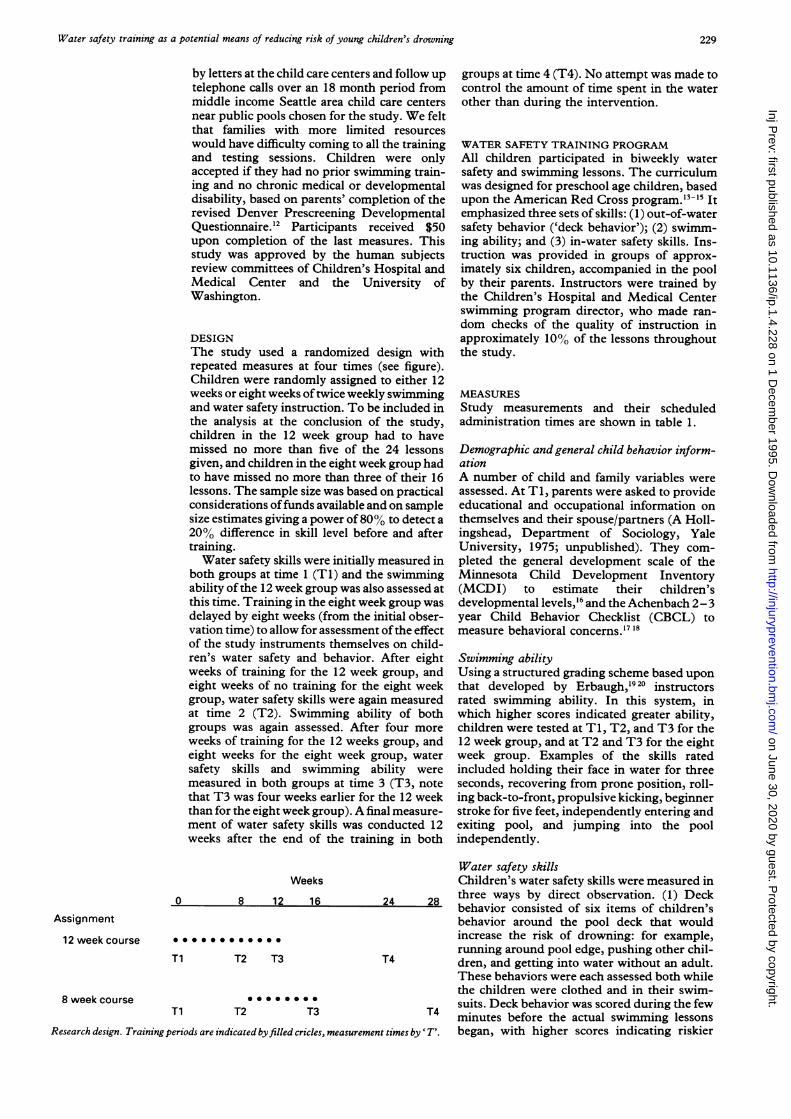
DESIGNThe study used a randomized design withrepeated measures at four times (see figure).Children were randomly assigned to either 12weeks or eight weeks oftwice weekly swimmingand water safety instruction. To be included inthe analysis at the conclusion of the study,children in the 12 week group had to havemissed no more than five of the 24 lessonsgiven, and children in the eight week group hadto have missed no more than three of their 16lessons. The sample size was based on practicalconsiderations offunds available and on samplesize estimates giving a power of80% to detect a20% difference in skill level before and aftertraining.Water safety skills were initially measured in
both groups at time 1 (T1) and the swimmingability of the 12 week group was also assessed atthis time. Training in the eight week group wasdelayed by eight weeks (from the initial obser-vation time) to allow for assessment ofthe effectof the study instruments themselves on child-ren's water safety and behavior. After eightweeks of training for the 12 week group, andeight weeks of no training for the eight weekgroup, water safety skills were again measuredat time 2 (T2). Swimming ability of bothgroups was again assessed. After four moreweeks of training for the 12 weeks group, andeight weeks for the eight week group, watersafety skills and swimming ability weremeasured in both groups at time 3 (T3, notethat T3 was four weeks earlier for the 12 weekthan for the eight week group). A final measure-ment of water safety skills was conducted 12weeks after the end of the training in both
Weeks
8 12 16
Assignment
12 week course
Ti T2 T3
Ti T2 T3
groups at time 4 (T4). No attempt was made tocontrol the amount of time spent in the waterother than during the intervention.
WATER SAFETY TRAINING PROGRAMAll children participated in biweekly watersafety and swimming lessons. The curriculumwas designed for preschool age children, basedupon the American Red Cross program.'3-'5 Itemphasized three sets of skills: (1) out-of-watersafety behavior ('deck behavior'); (2) swimm-ing ability; and (3) in-water safety skills. Ins-truction was provided in groups of approx-imately six children, accompanied in the poolby their parents. Instructors were trained bythe Children's Hospital and Medical Centerswimming program director, who made ran-dom checks of the quality of instruction inapproximately 10% of the lessons throughoutthe study.
MEASURESStudy measurements and their scheduledadministration times are shown in table 1.
Demographic and general child behavior inform-ationA number of child and family variables wereassessed. At TI, parents were asked to provideeducational and occupational information onthemselves and their spouse/partners (A Holl-ingshead, Department of Sociology, YaleUniversity, 1975; unpublished). They com-pleted the general development scale of theMinnesota Child Development Inventory(MCDI) to estimate their children'sdevelopmental levels,'6 and the Achenbach 2-3year Child Behavior Checklist (CBCL) tomeasure behavioral concerns.'7 18
Swimming abilityUsing a structured grading scheme based uponthat developed by Erbaugh,'9 20 instructorsrated swimming ability. In this system, inwhich higher scores indicated greater ability,children were tested at T1, T2, and T3 for the12 week group, and at T2 and T3 for the eightweek group. Examples of the skills ratedincluded holding their face in water for threeseconds, recovering from prone position, roll-ing back-to-front, propulsive kicking, beginnerstroke for five feet, independently entering andexiting pool, and jumping into the poolindependently.
Water safety skillsChildren's water safety skills were measured inthree ways by direct observation. (1) Deck
24 28 behavior consisted of six items of children'sbehavior around the pool deck that wouldincrease the risk of drowning: for example,running around pool edge, pushing other chil-
T4 dren, and getting into water without an adult.These behaviors were each assessed both whilethe children were clothed and in their swim-suits. Deck behavior was scored during the few
T4 minutes before the actual swimming lessons!ttimes by 'Tr. began, with higher scores indicating riskier
0
8 week course
Research design. Training periods are indicated byfilled cricles, measuremen
229
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from

Asher, Rivara, Felix, Vance, Dunne
Table 1 Data collected and measurement times
Measurement timeMeasure Ti T2 T3 T4Demographic and general childbehavior information
Parents' education and occupation xMCDI xCBCL x
Swimming ability in each group12 week x x x8 week x x
Water safety skillsDeck behavior x x x xWater recovery x x x xJump and swimn x x x x
behavior. (2) Water recovery, that is the abilityto recover and stand up when dropped fromtwo feet above the water (which was at theshallow end of the pool two feet deep), wasassessed, first, with the instructor releasing thechild, and if the child resisted, with the parentreleasing the child. If the child resisted releasefrom two feet above the water, the adult wouldattempt release from the water's surface. (3)Jump and swim, that is the ability to jump fromedge of pool into the pool and swim back to theside. The child was initially asked to do this bythe observer, if the child refused the observer,the child was then asked to jump by the parent.If the child resisted jumping from the side, sheor he was released by the adult in the pool toswim to the side. The child was not required toclimb out ofthe pool. Water recovery and jumpand swim were ordinally rated from the lessdifficult challenges to the more difficult asdescribed above, with higher scores indicatinggreater skill. Independent observers blind tochildren's group assignments conducted allobservations and ratings, with frequent ran-dom reliability checks by the research coor-dinator. All were assessed at Ti, T2, T3, andT4.
DATA ANALYSISRepeated measures analysis of variance wasused to assess the effects of the intervention, aswell as of duration of training. Ti measureswere compared with T4, and the differences
Table 2 Characteristics ofparticipating children andfamilies at beginning and end ofwater safety training
Group12 week 8 week Total
Baseline assessment (TI)No 91 71 162Male (%) 50 54 53Mean (SD) age in months 33 0 (5 6) 33-4 (5 6) 34-1 (5 6)SES (% at level)*
1 23 37 312 36 36 363 30 23 264 11 4 8
Final assessment (T4)No 61 48 109Male (%) 52 56 54
Mean (SD) age in months 34 6 (5 5) 33 6 (5-6) 34-2 (5-5)SES (% at level)*
1 21 42 302 39 33 373 33 23 284 7 2 5
SES = socioeconomic status.
between the eight week and 12 week groupswere compared at T1, T2, T3, T4.
ResultsSTUDY STAMPLEAt the beginning of the study (Ti), 162 child-ren were enrolled: 91 randomly assigned to the12 week group and 71 to the eight week group.Although equal numbers of children wereinitially assigned to the two groups, there wasdrop out before the study began at T1. Thisdifferential early drop out continued through-out the study, precluding equal group sizes,and was probably related to the extra measure-ment session in the eight week group beforeswimming lessons began. Even so, the twogroups did not differ significantly on age orgender. About 67% ofthe sample fell in the twohighest categories of socioeconomic status;although somewhat fewer families in the 12week group were in the highest category, thedifference in these proportions was notsignificant (see table 2).By the end of the study 109 children had met
all of the criteria for inclusion in the analyses.Their mean (SD) age was 34-2 (5 5) months,with boys comprising 54% of the sample. As atTi, the two groups did not differ significantlyin these characteristics. As before, despiteapparent under-representation of 12 weekgroup families in the highest category ofsocioeconomic status compared with the eightweek group, the difference did not reachsignificance. There were no differencesbetween the 109 children who completed thestudy and the 53 children who dropped out ongender, age distribution, socioeconomic status,or baseline skills in water safety, deck behavior,or water recovery. Reasons for drop out wereprimarily inability to come to training and/ortesting sessions.
WATER SAFETY OUTCOME MEASURESSwimming abilityBoth groups showed highly significant imp-rovements in swimming ability during theeight weeks after the beginning of training(T1-T2 for the 12 week group, T2-T3 for theeight week group) (Wilk's A multivariate F (1,49) = 141 00, p<0 0001). This improvementcontinued to week 12 (that is, T3) (Wilk's Amultivariate F (1,51) = 164-71, p< 0.0001).The eight week group was significantlysuperior to the 12 week group at the first lesson(T1 for the 12 week group, T2 for the eightweek), and at eight weeks (T2 for the 12 weekgroup, T3 for the eight week), but not whencompared with the 12 week group's finalability. However, the two groups' improve-ment over time did not differ significantly fromone another (table 3). These changes frombefore to after training represent improve-ments in skill from being able to only bob in thewater initially to being able to kick propulsivelyby the end of training.
Deck behaviorDeck behavior varied significantly from TIthrough T4, only because of a significant
230
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from
Water safety training as a potential means of reducing risk ofyoung children's drowning
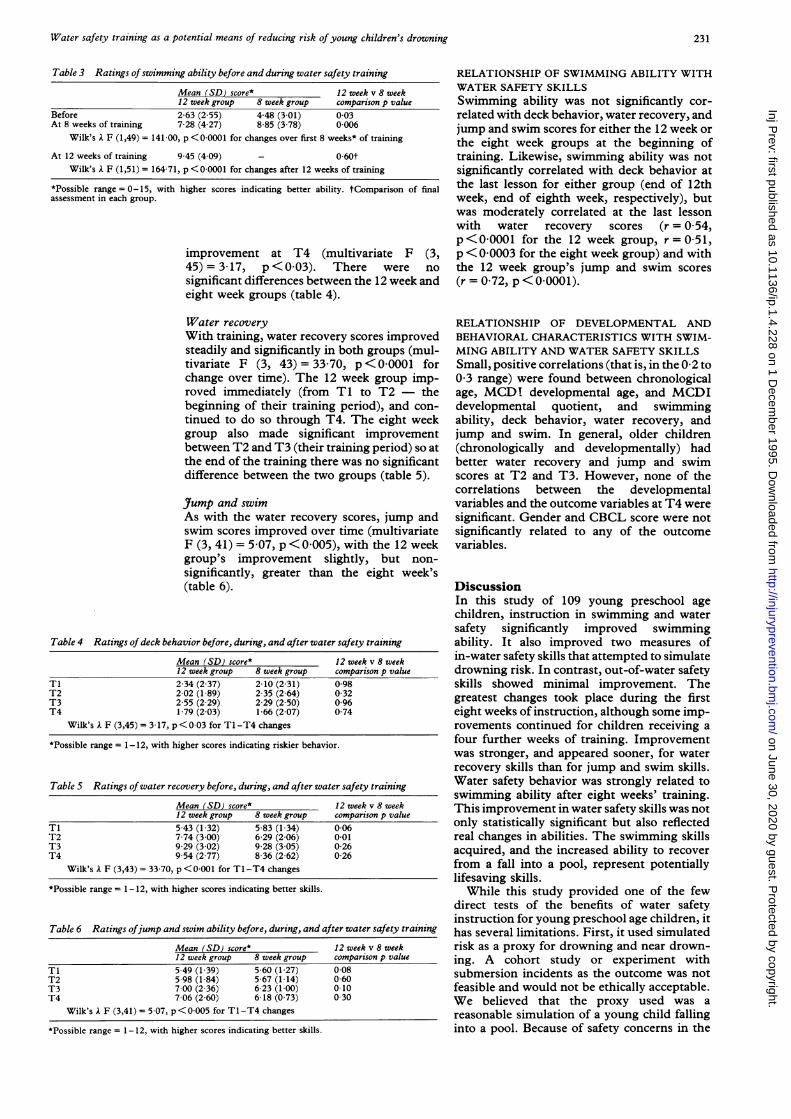
Table 3 Ratings ofswimming ability before and during water safety training
Mean (SD) score* 12 week v 8 week12 week group 8 week group comparison p value
Before 2-63 (2 55) 448 (3 01) 003At 8 weeks of training 7 28 (4 27) 8 85 (3 78) 0 006
Wilk's A F (1,49) = 141 00, p < 000001 for changes over first 8 weeks* of training
At 12 weeks of training 9-45 (4 09) - 060tWilk's A F (1,51) = 164 71, p<0 0001 for changes after 12 weeks of training
*Possible range= 0-15, with higher scores indicating better ability. tComparison of finalassessment in each group.
improvement at T4 (multivariate F (3,45) = 317, p <0 03). There were nosignificant differences between the 12 week andeight week groups (table 4).
Water recoveryWith training, water recovery scores improvedsteadily and significantly in both groups (mul-tivariate F (3, 43) = 33 70, p<00001 forchange over time). The 12 week group imp-roved immediately (from T1 to T2 - thebeginning of their training period), and con-tinued to do so through T4. The eight weekgroup also made significant improvementbetween T2 and T3 (their training period) so atthe end of the training there was no significantdifference between the two groups (table 5).
Jtump and swimAs with the water recovery scores, jump andswim scores improved over time (multivariateF (3, 41) = 5 07, p<0 005), with the 12 weekgroup's improvement slightly, but non-significantly, greater than the eight week's(table 6).
Table 4 Ratings ofdeck behavior before, during, and after water safety training
Mean (SD) score*12 week group 8 week group2 34 (2-37) 2-10 (2-31)2 02 (1 89) 2 35 (2-64)2-55 (2-29) 2-29 (2 50)1 79 (2 03) 1-66 (2 07)
Wilk's A F (3,45) = 3 17, p < 003 for T1-T4 changes
12 week v 8 weekcomparison p value0-98032096074
*Possible range = 1-12, with higher scores indicating riskier behavior.
Table 5 Ratings ofwater recovery before, during, and after water safety training
Mean (SD) score*12 week group 8 week group5-43 (1 32) 5-83 (1 34)7-74 (3-00) 6-29 (2 06)9 29 (3 02) 9 28 (3 05)9 54 (2 77) 8 36 (2-62)
Wilk's A F (3,43) = 33 70, p< 0O001 for T1-T4 changes
12 week v 8 weekcomparison p value0060-01026026
*Possible range = 1-12, with higher scores indicating better skills.
Table 6 Ratings ofjump and swim ability before, during, and after water safety trainingMean (SD) score*12 week group 8 week group5 49 (1 39) 5 60 (1 27)5-98 (1 84) 5 67 (1 14)7 00 (2-36) 6 23 (1 00)7 06 (2 60) 6 18 (0 73)
Wilk's A F (3,41) = 5 07, p< 0005 for T1-T4 changes
12 week v 8 weekcomparison p value0080600-100 30
*Possible range = 1-12, with higher scores indicating better skills.
RELATIONSHIP OF SWIMMING ABILITY WITHWATER SAFETY SKILLSSwimming ability was not significantly cor-related with deck behavior, water recovery, andjump and swim scores for either the 12 week orthe eight week groups at the beginning oftraining. Likewise, swimming ability was notsignificantly correlated with deck behavior atthe last lesson for either group (end of 12thweek, end of eighth week, respectively), butwas moderately correlated at the last lessonwith water recovery scores (r = 0 54,p<0 0001 for the 12 week group, r=051,p< 0 0003 for the eight week group) and withthe 12 week group's jump and swim scores(r = 0-72, p<0 0001).
RELATIONSHIP OF DEVELOPMENTAL ANDBEHAVIORAL CHARACTERISTICS WITH SWIM-MING ABILITY AND WATER SAFETY SKILLSSmall, positive correlations (that is, in the 0-2 to0 3 range) were found between chronologicalage, MCDI developmental age, and MCDIdevelopmental quotient, and swimmingability, deck behavior, water recovery, andjump and swim. In general, older children(chronologically and developmentally) hadbetter water recovery and jump and swimscores at T2 and T3. However, none of thecorrelations between the developmentalvariables and the outcome variables at T4 weresignificant. Gender and CBCL score were notsignificantly related to any of the outcomevariables.
DiscussionIn this study of 109 young preschool agechildren, instruction in swimming and watersafety significantly improved swimmingability. It also improved two measures ofin-water safety skills that attempted to simulatedrowning risk. In contrast, out-of-water safetyskills showed minimal improvement. Thegreatest changes took place during the firsteight weeks of instruction, although some imp-rovements continued for children receiving afour further weeks of training. Improvementwas stronger, and appeared sooner, for waterrecovery skills than for jump and swim skills.Water safety behavior was strongly related toswimming ability after eight weeks' training.This improvement in water safety skills was notonly statistically significant but also reflectedreal changes in abilities. The swimming skillsacquired, and the increased ability to recoverfrom a fall into a pool, represent potentiallylifesaving skills.While this study provided one of the few
direct tests of the benefits of water safetyinstruction for young preschool age children, ithas several limitations. First, it used simulatedrisk as a proxy for drowning and near drown-ing. A cohort study or experiment withsubmersion incidents as the outcome was notfeasible and would not be ethically acceptable.We believed that the proxy used was areasonable simulation of a young child fallinginto a pool. Because of safety concerns in the
TIT2T3T4
TIT2T3T4
TiT2T3T4
231
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from

Asher, Rivara, Felix, Vance, Dunne
study, we did not assess the impact of theintervention on more realistic drowningscenarios, for example, falling into and gettingout of a pool without an adult present. We alsodo not know how well our tests measured theability of a child to avoid or survive a realsubmersion episode. There was no way to'validate' these measures further.
Second, the comparison group (eight week)received training as well as the full treatmentgroup (12 week), diminishing the possibledifferences between the two conditions. Thiscomparison group allowed us to test the shortterm changes in swimming skills without anintervention, as well as any possible effect ofthetesting procedures themselves on skills. Inaddition, it would have been difficult to recruitsubjects without offering any training. The twogroups were similar demographically, althoughthe eight week group had a somewhat higher,but non-significant, proportion of families atthe highest socioeconomic level. The twogroups were similar at baseline in their deckbehavior, water recovery, and jump and swimscores - our major outcome measures. How-ever, the eight week group had higher swimm-ing ability at initial assessment than did the 12week group. The reasons for this are unknown,but as safety skills and swimming ability wereunrelated at baseline, the effect on the outcomeshould be small.
Third, the study sample was self selected(that is, parents volunteered their children),and thus were more likely to have some interestin water safety. The effects of this on thechildren's performance is unknown. The child-ren participating in the study were mostly frommiddle and upper income families. The res-ponse of children from poorer and lesseducated families to the intervention is un-known, limiting generalizability of the results.There were somewhat more families in thehighest socioeconomic strata in the eight weekgroup. However, there were no differences inthe proportion of children in the two loweststrata, in which one might expect to see someeffect on the intervention. The duration of theswimming lessons ofeight to 12 weeks may alsolimit the generalizability of the study results, assuch lessons may not be available to somefamilies. Future studies should examine theeffectiveness of fewer lessons and shorterintervention on swimming skills and watersafety.
Fourth, the artificiality of the study setting(that is, participating in a research and trainingstudy, and receiving payment) may haveaffected the behavior of the children and theirparents, although the children's age wouldlessen this effect.
Fifth, the relatively short duration of child-ren's involvement in the study limited ourability to assess how long the effect persists,especially if it is not reinforced.
Finally, the study did not attempt to measureany potential negative effects of the interven-tion, such as an over confidence on the part ofchildren and/or their parents after the training.Some injury prevention strategies have provedpotentially harmful, such as the effect of
drivers' education which lowered driving ageand increased the number of motor vehiclecrashes in young drivers.2' These potentialnegative effects are important to evaluate andshould be examined in future, larger studies ofwater safety training.
This study should be viewed as an exp-loratory effort to provide information on theeffectiveness of water safety training. Theability to fully test the intervention with a largescale experiment using submersion or drown-ing as an outcome is limited, given the relativerarity of these events. Such an evaluation willrequire quasiexperimental methods, such as acase-control study in which the exposure ofinterest is prior water safety training.
Despite the above limitations, the results ofthis study offer several implications for parentsand others interested in the safety of youngchildren around water. First, water safety is nota simple entity. Different aspects are affectedby training in different ways, for example, deckbehavior did not improve significantly, despitethe improvement in in-w4ter safety skills.While water safety training for young pre-school age children may reduce their risk ofdrowning, it does not have a similar effect ontheir poolside behavior, and thus their risk offalling in. Finally, while there was no supportfor the concern that water safety instructionincreases young children's risk of drowning,their improved skills do not reduce the need foradult monitoring, supervision, and safetyawareness. The potential impact of such aprogram on decreasing parental vigilance mustbe further assessed, because vigilance is acrucial element in any drowning preventionprogram.
IMPLICATIONS FOR PREVENTIONWe believe that the results of this study showthat there are potential benefits for youngpreschool age children in learning swimmingand water safety skills. This study should berepeated by others; if the results are replicated,swimming and water safety training should bepromoted as part of a drowning preventionprogram for this age range. However, a comp-rehensive approach would incorporate passiveprotection, such as water barriers and personalflotation devices, active measures such as watersafety and swimming instruction, and parentalawareness and supervision. All such elementsshould be advocated strongly to optimize watersafety and enjoyment for young children.
This work was supported by Maternal and Child HealthResearch Grant No MCJ-530607, from the Maternal and ChildHealth Bureau of the United States Department of Health andHuman Services.
Great appreciation is expressed to the children and theirparents who participated in this study, the swimming instruc-tors from Seattle Children's Hospital and Medical Center, andRobert Soderberg, who provided analytic assistance with amaximum of energy and minimum of exasperation.
1 Baker SP, O'Neill B, Ginsburg MJ, Li G. The injury factbook. 2nd Ed. New York: Oxford University Press, 1992.
2 O'Carroll PW, Alkon E, Weiss B. Drowning mortality inLos Angeles County, 1976 to 1984. JAMA 1988; 260:380-3.
232
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from

Water safety training as a potential means of reducing risk ofyoung children's drowning
3 Quan L, Gore EJ, Wentz K, Allen J, Novack AH. Ten-yearstudy ofpediatric drownings and near-drownings in KingCounty, Washington: lessons in injury prevention.Pediatrics 1989; 83: 1035-40.
4 Washington State Injury Prevention Program. Drowning inWashington State. Olympia, WA: Washington StateDepartment of Health, 1991.
5 Wintemute GJ. Childhood drowning and near-drowning inthe United States. Am J Dis Child 1990; 144: 663-9.
6 Wintemute GJ, Kraus JF, Teret SP, Wright M. Drowningin childhood and adolescence: a population-based study.Am J Public Health 1987; 77: 830-2.
7 Rivara FP. Traumatic deaths of children in the UnitedStates: currently available prevention strategies. Pediat-rics 1985; 75: 456-62.
8 Diamond EF. Swimming instruction for preschool children.Sports Med 1975; 3: 58-60.
9 Committee on Pediatric Aspects ofPhysical Fitness, Recrea-tion, and Sports. Swimming instructions for infants.Pediatrics 1980; 65: 847.
10 Wright M, deSilva P, Sinha S. Hyponatraemia in children.BMY 1992; 305: 51-2.
11 Mahoney FJ, Farley TA, Kelso KY, Wilson SA, Horan JM,McFarland LM. An outbreak of hepatitis A associatedwith swimming in a public pool. J Infect Dis 1992; 165:613-8.
12 Frankenburg WK, Fandal AW, Thornton SM. Revision ofthe Denver Prescreening Developmental Questionnaire.
Pediatr 1987; 110: 653-7.13 The American National Red Cross. Swimming and aquatics
safety. Washington, DC: American National Red Cross,1981.
14 The American National Red Cross. American Red Crosswater safety instructor's manual. St Louis, MO: Mosby -Year Book, 1992.
15 American National Red Cross. Swimming and diving. StLouis, MO: Mosby - Year Book, 1992.
16 Ireton J, Thwing E. The Minnesota Child DevelopmentInventory. Minneapolis, MN: Behavioral ScienceSystems, 1974.
17 Achenbach TM, Edelbrock C, Howell CT. Empirically-based assessment of the behavioral/emotional problems of2-3-year-old children. J Abnorm Child Psychol 1987; 15:629-50.
18 McConaughy SH, Achenbach TM. Practical guide for theChild Behavior Checklist and related materials. Burling-ton, VT: University of Vermont, 1988.
19 Erbaugh SJ. Assessment of swimming performance ofpreschool children. Percept Mot Skills 1978; 47: 1179-82.
20 Erbaugh SJ. Effects of aquatic training on swimming skilldevelopment of preschool children. Percept Mot Skills1986; 62: 439-46.
21 Robertson LS. Crash involvement ofteenaged drivers whendriver education is eliminated from high school. Am JPublic Health 1980; 70: 599-603.
* * * * *
'Transport minister needs head examined over helmetuse'This was the headline used for a letter I wrote to our local papercomplaining about the transport minister's reasons for notwishing to introduce helmet legislation. His explanation was theold chestnut: you can't pass a law (or enforce one) until somemythical proportion of the population is already, in effect, incompliance. (I wish I knew where this came from). Although Ithink my letter was a good one, it was greatly enhanced by onethat appeared below it from a parent describing how her 10 yearold was rendered unconscious after colliding with a car. Thehelmet was 'smashed in on one side from the impact. . .'- ampletestimony to the force absorbed. Interestingly, she concluded bystating her belief in how important it is for parents to set a goodexample, and asserting that she always wears a helmet.
More on bike helmetsA columnist in the Globe and Mail (which describes itself asCanada's national newspaper) wrote a piece with the title 'Whyhelmet laws treat adults like children'. His arguments weresimply incredible (literally so). Apart from a raft ofirrelevant andmisleading statistics, he agued that 'The costs of mandatoryhelmets is measured not only in dollars but in lives. The addednuisance of finding and wearing a helmet will cause a certainnumber ofbike trips to be replaced with car trips; ... That meansmoe chance of auto accidents, and fewer health benefits fromcycling'. I am simply unable to follow this logic. Can anyonehelp? (Globe and Mail, June 21, 1995.)
Tales of an inept bikeriding editorAfter finally deciding to replace my old and beloved bike helmetwith a lighter, more jazzy one, I find myself quite unable to figureout how to adjust the straps to ensure a proper fit. Does anyonehave any SIMPLE advice that an aging bicyclist is likely tounderstand?
233
on June 30, 2020 by guest. Protected by copyright.
http://injuryprevention.bmj.com
/Inj P
rev: first published as 10.1136/ip.1.4.228 on 1 Decem
ber 1995. Dow
nloaded from