safety nets in cambodia - foodsecurity.gov.kh
TRANSCRIPT

Safety nets in Cambodia Concept note and inventory June 30, 2009 Council for Agriculture and Rural Development (CARD) World Food Programme (WFP) World Bank East Asia Human Development Unit (WB) This Note has been prepared by Jeanine Braithwaite, Lucilla Bruni, Tim Conway, Jennica Larrison, and Jamele Rigolini from the World Bank East Asia Unit, with inputs from the Council for Agriculture and Rural Development and the World Food Programme, and feedback from members of the Technical Working Group on Food Security and Nutrition. The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors, and do not necessarily represent the view of the institutions they are affiliated to.

2
Table of Contents 1. Introduction and Executive Summary ..................................................................... 3 2. Social protection and safety nets: concepts and definitions .................................. 7 3. Poverty and vulnerability profile ........................................................................... 13 4. Inventory of social protection and safety net interventions ................................ 17 5. Gaps and challenges of existing interventions ...................................................... 26 Annex 1: Inventory of Social Protection Interventions ................................................ 29 Annex 2: Additional Tables ............................................................................................. 40 Annex 3: List of Social Protection‐related projects ...................................................... 41 References ........................................................................................................................ 43 Acronyms ......................................................................................................................... 46 Tables Table 1: Poverty and inequality trends ......................................................................................... 14 Table 2: Estimated impact of extreme floods and droughts, 2000‐2005 ...................................... 14 Table 3: Risk management matrix ................................................................................................. 19 Table 4: WFP food distribution and beneficiaries in 2008 ............................................................ 22 Table 5: UNICEF safety nets budget, 2006‐2010 ........................................................................... 23 Table 6: Social Intervention Chapters by Ministries and other Government Agencies ................ 34 Table 7: Overseas Development Assistance – Ten major sectors in 2008 .................................... 40 Table 8: Summary Disbursement from Donors and NGOs, by province ....................................... 40 Table 9: Inventory of all ongoing donor funded projects related to Social Protection ................. 41
Figures Figure 1: Trends in overall social spending (% of GDP) ................................................................. 18
Boxes Box 1: The Identification of Poor Households Program ................................................................ 24 Box 2: Workfare: evidence from international best practice ........................................................ 25

3
1. Introduction and Executive Summary This note presents the main features, achievements, gaps, and challenges faced by safety net programs in Cambodia. The aim of the note is to provide a basis for discussion among Government and Development Partners, as a first step towards formulating a social protection strategy for Cambodia.
1 This note is an outcome of a process of initial review and concept development which is designed to support the establishment of a social safety net system in Cambodia. At the Cambodia Development Cooperation Forum (CDCF) in December 2008, the Government and its development partners discussed the heightened need for a coherent safety net system in the face of global price and financial crises and the effects of these shocks on Cambodia. As a result of this discussion, the Government assigned to the Council for Agriculture and Rural Development (CARD) the responsibility for managing a number of pieces of initial analysis, including clarification of terms and concepts with regard to safety net policy; a review of key sources of household vulnerability in Cambodia; an inventory (or “mapping”) of existing safety nets; and an initial outline of policy options to guide strategy development. Over the first half of 2009, CARD has convened meetings of a broad set of national stakeholders. This process has helped to build consensus on the meaning of key concepts and the broad direction for policy development. These findings and recommendations will be presented and discussed at a National Forum in June 2009. It is also hoped that they will help in the formulation of the government’s new medium‐term National Strategic Development Plan (NSDP) for the period 2010‐2013, and in the identification of policies for achieving the Cambodian Millennium Development Goals by 2015.
2 Social protection consists of a broad set of arrangements and instruments designed to assist
individuals, households, and communities to better manage risk, shocks, and extreme poverty. Social protection arrangements involve social groupings (practices of risk‐sharing and charity based on kinship or community principles); private sector actors (insurance markets); and the state, acting through public policies and programs and through the creation of a legal and regulatory environment that structures and facilitates civil society and private action.
3 Informal arrangements based in kinship and community practices and gifts from wealthy
urban groups to poorer rural communities provide households with some protection against risk. However, these arrangements cannot substitute for a functioning government‐provided safety net. While transfers from richer households to poorer households may play a valuable role in helping households deal with occasional household‐level (idiosyncratic) crises, they may fail in the face of widespread (covariant) shocks such as an extensive flood or a rapid economy‐wide increase in food prices. Inter‐household assistance may also exclude the very poorest (e.g. those living in villages where they have no relatives).
4 An effective social protection system goes beyond protecting the poor. To the extent that it
encourages prudent risk‐taking and enhances opportunities for the poor, it is beneficial for growth. Social protection can also help Governments embark on reforms that have long‐term benefits in economic efficiency but high short‐term social and political costs, by providing effective compensation to those negatively affected by the reform. Social protection should therefore be an integral part of countries’ growth and poverty reduction strategies.

4
5 Safety nets are a subset of social protection policy. State‐provided social protection—the focus
of this note–typically includes safety nets, social insurance, a legal and policy framework (e.g. on labor standards), and targeted social services. Safety nets usually consist of interventions that are (i) designed for the most poor and vulnerable poor and (ii) are non‐contributory (that is, are financed out of general revenue—taxation or official development assistance (ODA)—by contrast to social insurance schemes, which rely on prior contributions from the recipient). Examples of safety net interventions include workfare (i.e. food‐ and cash‐ for work),; unconditional and conditional transfers (in cash or kind); and, under some definitions, subsidies designed to ensure the poor have access to health, education, housing or public utilities such as water or electricity.
6 Safety nets can play at least three key roles in development policy. They act to assist
households in managing risks that could have negative impacts over both the short and long term; they enable households to invest better in their future, promoting an environment favorable to inclusive economic growth; and they facilitate necessary policy reforms, by providing transitional support to compensate groups negatively affected by (for example) trade liberalization, the removal of untargeted energy subsidies, or reform of state‐owned enterprises.
7 Cambodia has emerged from three decades of instability with an impressive record of
sustained growth and poverty reduction. Yet, Cambodians still face many serious forms of vulnerability. With the majority of the population engaged in single crop subsistence agriculture heavily dependent upon the weather, poor harvests and food insecurity (in particular during the lean season) are major sources of vulnerability. Illness and injury, and the high costs of treatment, are also critical factors in pushing non‐poor households into poverty. For many of Cambodia’s young and generally under‐educated population now entering the workforce, unemployment or underemployment is an endemic risk, while those who have obtained jobs in export‐oriented sectors of the economy (such as garment manufacture or tourism) are now vulnerable to job loss or drastically reduced earnings due to recession and falling demand in overseas markets.
8 These forms of vulnerability, which push people into poverty or keep them there, have serious
long‐term consequences for households and for national development. Poverty and periodic shocks result in child malnutrition and high child and maternal mortality rates; selling land or other household productive assets at low prices to raise cash for food or medical treatment; taking on debt; and taking children out of school to help out at home. While child nutrition, health and survival rates improved between 2000 and 2005, there is evidence that they have worsened again over the last 18 months due to high food prices and economic slowdown.
9 Given the extent of poverty in Cambodia, the priority should be to develop a sound safety net
system, as the first stage in building an effective and affordable social protection system. For this reason, this note shall focus mostly on safety nets, rather than looking at the whole social protection panorama. It is however important to remember that safety nets and social protection are part of a broader social protection system; and that social protection in turn is an element within an overall strategic framework for poverty reduction that also includes social insurance; health, education, and financial services; infrastructure and utilities; and other policies aimed at reducing risk and creating opportunity.

5
10 To date, safety net interventions have addressed some key sources of vulnerability in
Cambodia. With support from development partners, health fee waivers, scholarships and exemptions have helped households deal with health costs and keep their children in school. Other safety net interventions include food distribution, labor‐intensive public works, and targeted transfers.
11 Despite these efforts, many sources of vulnerability have not yet been tackled, as safety net
interventions do not reach some population groups and regions in need of assistance. The urban poor, those who have become poor recently and those who dip in and out of poverty over time (the transient poor) are often left out of current safety net interventions. Most existing programs have limited geographical coverage, and may not be covering regions and groups that most need them. Geographically disaggregated analysis that links program coverage to sources of vulnerability may be necessary, to allow better identification of coverage gaps and more targeted use of existing resources to reach the most vulnerable population groups.
12 The majority of interventions currently existing in Cambodia provide benefits in kind (food) rather than cash. Food‐ and cash‐based schemes each have different advantages and disadvantages; the relative merits of one compared to the other are largely context‐specific, depending on the operation of local food markets, household behavior, and institutional and logistical considerations. (In some circumstances, there may even be a case for combining food and cash transfers within one program.) In building a comprehensive national safety net system and addressing non‐food vulnerabilities, there may be potential for introducing cash‐based interventions to complement existing in‐kind assistance. To assess this potential, it would be important to develop and evaluate pilot schemes to assess their effectiveness in tackling key aspects of poverty and vulnerability (e.g. poor child nutrition, harvest failure, the costs of ill health) before deciding whether to take these approaches to scale.
13 Effective and affordable safety net interventions depend on good mechanisms for accurately targeting support to those who need it. Targeting has not yet been mainstreamed into safety net implementation, and many safety net programs still rely on ad hoc targeting procedures whose accuracy has not been tested. Targeting has costs: to ensure the optimum ratio of benefits for these costs, it is necessary to ensure that, where possible, different safety net programs draw on the same targeting system. The Government’s Identification of Poor Households Program (IDPoor) follows standardized procedures and criteria to compile lists of poor households: use of IDPoor as the main system for targeting would reduce overall targeting costs. There is a strong case for allocating additional resources for accelerating implementation of household identification as an underpinning to the development of national safety nets.
14 While there is a strong rationale for using ID Poor for all schemes targeted at poor households
(i.e., having only one rather than many systems for proxy means testing), other targeting methods can be used to complement this. Self‐targeting may be appropriate for some forms of safety net program, including in urban areas (which ID Poor does not yet cover, and where considerable work would be needed to adapt its current mix of proxy means testing and community verification). There may also be scope for geographical targeting. Fine‐grained maps of poverty and vulnerability may be generated either from administrative data (e.g. the commune / sangkat database) or from combining data from the 2008 census and household survey through small‐area estimation techniques. Such maps can help to prioritize areas for the

6
extension of ID Poor and household‐targeted schemes that it supports; or to identify poor areas for infrastructure investments that can be expected to have community‐wide benefits.
15 Institutionally, safety net implementation often reflects immediate priorities (such as the
need to respond to the food price crisis), rather than a longer‐term vision for safety net development. Frequent changes in priorities driven by events prevent the development of a longer‐term vision that would eventually allow not only reliable, standing arrangements to identify and protect the poor and vulnerable, but also more effective rapid responses. In many countries with a large number of development partners (DPs), safety net spending reflects priorities dictated by DPs’ interests and earmarked funding sources. This leads to relatively large sums available for safety net interventions in some sectors (e.g. workfare), while other equally if not more important areas (such as education and malnutrition) remain largely uncovered.
16 Government and development partners should thus seek better coordination in their safety
net efforts. In the absence of a comprehensive social protection and safety net strategy, a patchwork of programs currently exists. These programs now need to be adapted into a coherent safety net framework. For this to happen requires analysis of priorities in addressing sources of vulnerability, as a first step towards a longer‐term strategy for safety net implementation.
17 A major constraint for addressing these institutional challenges is the lack of a Government
body with a clear mandate to develop an overall strategy and monitor and coordinate its implementation. At present, safety net policies and programs are scattered across several ministries. The Ministry of Social Affairs, Veterans and Youth Rehabilitation (MOSVY), Ministry of Labor and Vocational Training (MOLVT) and the Ministry of Women’s Affairs (MOWA) are all mandated with managing state social services for the wider population, and helping to protect specific vulnerable groups against risks. However, no Government body has the mandate to coordinate safety net interventions across ministries and Development Partners, or to formulate cross‐sectoral interventions. The lack of a clear designated agency impedes the development of a comprehensive social protection and safety net strategy and of large‐scale, cross‐sectoral interventions.
18 An underlying challenge is the small size of the Government budget allocated for safety nets,
with the majority of funding provided by development partners. The lack of resources has considerably hindered the Government’s ability to develop an effective safety net system. In the process of developing a comprehensive safety net strategy, it will be important to explore how to incorporate programs led by Development Partners into the Government’s own development strategy and institutional capacity strengthening.
19 The design of a safety net system for Cambodia needs to reflect a realistic assessment of
implementation capacity. This assessment needs to address both central and sub‐national capacities, especially in the light of the ongoing process of decentralization and deconcentration (D&D), which is expected to transfer responsibilities and powers to Province, District and Commune levels. As part of a broader review of progress in public financial management reform, research in the second half of 2009 will assess the ability of sub‐national authorities to manage, monitor and account for safety net programs.

7
2. Social protection and safety nets: concepts and definitions
20 Social protection consists of a broad set of instruments designed to assist individuals, households, and communities to better manage risk, shocks, and extreme poverty. An efficient social protection system goes beyond protecting the poor. To the extent that it encourages prudent risk taking, and enhances opportunities for the poor, it is beneficial for growth. It can also help societies embark on reforms that are necessary for long‐term structural transformation and economic growth but which have high political costs in the short and medium term. Social protection should therefore be an integral part of countries’ growth and poverty reduction strategies.
21 While social protection helps society as a whole to manage risk, safety nets are designed for
the most poor and vulnerable. Social protection includes contributory schemes (health and unemployment insurance, contributory pension schemes) that are usually designed for formal sector workers and the middle class. By contrast, safety nets are non‐contributory interventions financed out of general revenue (taxation or ODA); targeted to the poor and those most at risk of poverty; to help them mitigate the effects of shocks and maintain a minimum socially‐accepted living standard (through income support and / or access to basic services). Safety nets usually include workfare (food‐ or cash for work), transfers (of cash or food, either unconditional or conditional), and, under some definitions, subsidies for basic goods and services for the poor.
22 Given high poverty rates and the emerging impact of the global economic crisis, the priority
now is for Cambodia to focus on developing a sound safety net system. This can then serve as a foundation on which to build up a more comprehensive and sophisticated social protection system over time. For this reason, this note shall focus mostly on the review, assessment and challenges faced by safety nets, rather than looking at the whole social protection panorama. It is however important to remember that safety nets fit within a larger social protection framework, which is in turn part of a broader poverty reduction strategy. As such, safety nets complement policies and programs for social insurance; health, education, and financial services; the provision of utilities and roads; and other policies aimed at reducing poverty and managing risk and vulnerability.
The role of safety nets in national development
23 Safety nets play multiple roles in development policy. Most societies hold strong convictions
that adequate provision for the poor is required (though they may differ in how this should be achieved): by transferring income to the poorest and most vulnerable, safety nets have an immediate impact on poverty and inequality. In addition to this direct and immediate function, safety nets also make three key contributions to long‐term national development policy: • Safety nets help households manage risk and vulnerability. At a minimum, safety net
programs help households facing hard times to avoid irreversible losses, allowing them to maintain the household and business assets on which their livelihoods are based, and to adequately nourish and school their children. Throughout the world, falling income among poor households leads to increased child malnutrition (with long‐lasting consequences on child growth, cognitive and learning ability, and schooling attainments: Alderman et al,

8
2008; Ferreira and Schady, 2008); higher school drop‐out rates with long term consequences on the children’s labor market performance (Ferreira and Schady, 2008); and to the selling of productive assets such as land and livestock (which impedes households’ recovery from the crisis: Fafchamps et al., 1998; Carter et al., 2004). At best, safety nets can provide an insurance element that lets households make choices about livelihoods that yield higher earnings. Safety nets thus both protect households and promote their independence.
• Safety nets can enable households to make better investments in their future, promoting an environment favorable to equitable and sustainable economic growth. In this role, safety nets basically act to remedy credit market failures, allowing households to take up investment opportunities that they would otherwise miss — both in terms of investment in the human capital of their children and in the livelihoods of the earners.
• Safety nets can directly assist governments in making reforms. Short‐term safety net programs can compensate those who are negatively affected by reforms that are necessary for economic development, or who may oppose and stall these reforms (Grosh et al. 2008). For example, with safety nets in place energy sectors can price for efficiency, and trade policy can focus on growth rather than job protection.
Safety net instruments
24 While different international organizations adopt somewhat different definitions of safety
nets, a core set of interventions are common to all definitions (Grosh et al 2008). The kinds of programs typically included as common elements in a safety net are unconditional transfers in cash and kind, price subsidies, public works schemes, conditional transfers, and fee waivers:
• Unconditional cash and near‐cash transfers help the poor to maintain basic consumption levels. These may be in the form of cash, or vouchers or stamps for purchasing goods and services. Vouchers or stamps limit the choice beneficiaries have for the use of funds; cash transfers allow beneficiaries to use the funds on whatever they see fit to smooth household income and consumption, but may be less helpful in times of national crises when transfers do not have the same purchasing power due to higher prices. Programs include needs‐based social assistance, family allowances, non‐contributory pensions and disability transfers, and food stamps. Cambodia does not presently have large programs for cash and near‐cash transfers.
• Conditional transfers (in cash or kind) link (i) the provision of resources to poor households to maintain consumption levels over the short term with (ii) incentives for these households to invest in human capital (health and education), with long term, inter‐generational benefits. Poor households are given transfers in exchange for compliance with specific conditions (or “co‐responsibilities”) encouraging them to use education and health services and lowering the cost of accessing such services. School feeding is an example of a conditional in‐kind transfer with wide reach in Cambodia. Conditional cash transfers (CCTs) have proved very effective in improving lagging human development indicators in a number of countries (Fiszbein et al 2009; Farrington and Slater 2006; UNDP 2006). In Cambodia, the scholarship for the poor program under the Education Sector Support project has increased enrollment rates in the program area by 20 percent (Filmer and Schady, 2009). As with any instrument, it is important to remember that conditional transfers cannot serve as a

9
complete safety net, as households without access to health or education facilities or without children of school age are not eligible for these programs.
• Unconditional in‐kind transfers can help ensure access to critical basic goods. They are particularly useful where private markets do not work well enough to ensure that supply will respond to increased demand. Transfers of food (the most common form of in‐kind transfer) can be used to improve nutritional status as well as help maintain consumption levels, by addressing food security directly. Examples of in‐kind transfers include mother/child food supplement programs, take‐home food rations, school supplies and uniforms. The Rice Distribution program under the Emergency Food Assistance Project supervised by the Ministry of Economy and Finance (MEF), and the Mother and Child Health program supported by the World Food Programme (WFP) are examples of in‐kind transfers.
• Workfare schemes (food‐ and cash‐ for work) offer low‐skilled poor individuals jobs in improving, repairing, and building local infrastructure. The program provides those who are willing to work with some protection from under‐ and unemployment through the generation of income. Because they can self‐target (offering a wage rate lower than the market rate so that only the poorest will enroll), workfare programs can avoid the need for an administrative process for identifying the poor, and so decrease costs related to beneficiary selection. However, in many countries political considerations often prevent offering low wage rates: paying higher rates either dramatically increases the cost of these interventions or leads to severe rationing of assistance. As with all safety nets, there will be some people who need assistance for whom workfare is not a suitable intervention (i.e. those who are not able to work, such as the elderly; those who are ill or disabled); other programs will be needed to reach these groups. Among others, the Ministry of Rural Development (MRD), WFP, and the International Labor Organization (ILO) have implemented workfare programs in Cambodia.
• Fee waivers assist in providing the poor with access to essential services including health care, schooling, utilities, or transport. While other users would be charged a fee, the poor receive these services for free or at a reduced rate. However, if the institutions providing these services are not fully compensated for the loss of revenue, they may seek to avoid serving the poor, provide a lower quality of service, or face a financing gap which may ultimately reduce the quality of services more generally. In Cambodia, Health Equity Funds (HEFs) provide funds to compensate health facilities for operating exemption policies which allow the poor to obtain treatment without paying user fees. Of the safety net provisions currently existing in Cambodia, health fee exemptions backed by equity funds are probably the program with the most extensive coverage. More than most, this safety net is also reasonably thoroughly mainstreamed in Government sector policy (even if financing is still largely dependent upon development partners).
• Price subsidies for basic commodities also act as a transfer, ensuring that the poor maintain minimum consumption levels of basic goods and services such as food, energy, housing, and utilities. Subsidies are however generally seen as being a second‐best safety net intervention: when they are available equally to the poor and non‐poor, they dramatically increasing the cost of assistance. Differentiated tariffs can achieve greater targeting efficiency, but entail costs of their own.

10
25 Food‐ and cash‐based transfers each have different advantages and disadvantages (Grosh et al 2008 p. 272; Gentilini 2007; Devereaux and Gorman 2006). The most important issue in deciding between food and cash is the functioning of local food markets. Food transfers may be preferable when food markets do not work well (e.g. for remote communities): under these circumstances, cash transfers that are not managed well may push up the local price of food, resulting in limited net welfare gains for recipients (and welfare losses for poor households not receiving transfers: Aker 2009). By contrast, cash transfers may be preferable when food markets function reasonably well and can meet increased household demand: in these circumstances, the added flexibility of cash may help poor families meet needs which will include food but may also include other essential non‐food expenditures1.
26 The choice of form of transfer needs to reflect not only how the transfer will affect consumers
in the short term but also how it will affect food production in the medium term. An increase in local food prices as a result of cash transfers will have a negative effect on households that do not receive benefits and who need to buy food, but may have a positive impact on poor farmers who can sell a surplus: after some time higher prices will result in higher incomes for these households, and improved local food availability. Conversely, if not implemented carefully, food transfers in unconnected markets may undermine local agricultural production (by driving down farmgate prices for food), even as they ensure immediate food security (and can help drive back down prices inflated by hoarding and speculating).
27 Whether food‐ or cash‐based transfers work better in any particular situation will also depend on intra‐household behavior, the specifics of poverty and food security challenges, and logistical and institutional issues. Food‐based arrangements address food insecurity directly: the content of food transfers can be tailored to address specific nutritional problems (e.g. using fortified foods to tackle micronutrient deficiencies), with some evidence that food transfers have longer‐term impact of child growth than do unconditional cash transfers (Gentilini 2008). Small transfers of good quality food may be more effective than cash when there is a concern that a cash transfer might be diverted to non‐food consumption (e.g. alcohol or cigarettes). However, cash is logistically easier to manage, with considerably lower administrative costs (food entails costs and systems for procurement, storage, and distribution) and capacity for rapid response.
28 In practice, the relative benefits of cash or food transfers depends heavily on context and design. The value of transfers to beneficiaries and the effects of these transfers on markets (multipliers / distortions) in a given situation may reflect not so much the intrinsic advantages and disadvantages of food versus cash but specific program design choices to do with benefit levels, targeting, and delivery mechanisms (when and where benefits are distributed). Under some circumstances, there is also a case for combining food and cash transfers (Gentilini 2007).
1 From the recipient’s point of view, food may also be preferable to cash during periods of rapid
inflation. However, when food prices are rising rapidly and fiscal space is limited, the agency supplying the transfer will find it difficult to continue supplying the same quantity of food as the purchasing power of their procurement budget declines. In the absence of additional financial resources and / or large stockpiles, rising food prices may result in rationing food transfers (reducing the size of the transfer and / or the number of recipients) or stop‐start program implementation. In these circumstances, the difference between food and cash may ultimately be minor.

11
29 There are often fears that in a weak fiduciary environment, transfer schemes may be subject to large scale leakage, with a significant proportion of benefits going to the non‐poor. This may be why transfer schemes in Cambodia remain relatively small. The issue requires serious attention: however, successful schemes both in Cambodia and in other countries suggest there are ways of preventing diversion, which can and should be built into systems for targeting, enrolment, monitoring and auditing.
30 Education and health subsidies also relate to safety nets. Cambodia has recently made significant progress through the implementation of the Scholarships for the Poor program (under the Education Sector Support project) and the expansion of Health Equity Funds.
31 Globally, there is a wide variation in both the manner in which each of these types of program
is implemented, and the relative success that they enjoy. In other words, there are few universal lessons: the details of design and implementation matter a great deal, with the result that the same broad type of program (e.g. workfare) might be very successful in one country, and unsuccessful in another. Program objectives should match the needs of the target population; design and implementation choices need to reflect country context (including socio‐cultural issues) and a realistic assessment of institutional capacity.
Targeting
32 Good targeting is essential to the success of safety nets. Targeted assistance makes it possible
to provide a more generous package of benefits to a more restricted set of vulnerable people in need, often at lower overall costs. Targeting aims to include all who are intended to benefit (i.e. the poor) and exclude those who are not intended to benefit (the non‐poor). Targeting is particularly important with regard to safety nets, as non‐contributory transfers are primarily a private good and households are unlikely to possess an upper limit of what they would wish to receive (Grosh et al. 2008).
33 The choice of targeting mechanism will reflect administrative, social and political
considerations. Achieving good targeting requires both good design at the outset and fine‐tuning during operation in order to balance different considerations (e.g. minimizing exclusion of the poor versus minimizing inclusion of the non‐poor). An effort to target narrowly may not be helpful when there are only minor differences between poorer groups, and particularly when there is a high degree of “churning”, with people moving in and out of poverty over time (in which case the scheme would need to conduct require frequent re‐assessment of households’ circumstances to ensure accurate targeting). Those designing and implementing targeted schemes should also pay attention to the costs that the poor may have to incur to prove eligibility; the potential risk that targeted benefits may create perverse incentives (resulting in people changing their behavior to qualify); and the risk that targeting criteria may be subject to political manipulation. There are a number of ways to address each of these issues and so ensure that targeting does deliver its potential: these need to be considered carefully at the design stage and their effectiveness monitored during implementation.
34 A comprehensive safety net system can make use of various methods to balance responsiveness in case of emergencies with efficient medium‐ to long‐term targeting. Targeting can be geographic, if pockets of poverty exist; or can be household‐based if poverty is
12
widespread, with poor households mixed up with non‐poor households. Often, the most effective targeting systems combine two (or more) different targeting mechanisms. The most advanced systems use means‐tested or proxy‐means tested methods that ask detailed questions to households about their wealth, income, and assets to determine who is eligible. The Ministry of Planning’s Identification of Poor Households system is an example of proxy‐means tested targeting tailored to the rural Cambodian context, combined with community validation (see Box 1).
35 As proxy‐means targeting is relatively costly to maintain, it should be used to target various
social protection programs at the same time, since economies of scale can be reached by splitting costs across interventions. However, some programs should also adopt other targeting methods, both because proxy‐means testing tends to be less good at responding in the short term to changes in the need for assistance, and because proxy means testing, despite its sophistication, would still miss some vulnerable households (see Ravallion, 2003 and 2008). Other targeting methods include: • simpler categorical targeting (i.e. children, elderly, disabled pregnant women, etc.); • geographical targeting (universal coverage in areas with very high poverty incidence); and • self‐targeting, where limited assistance is offered to everybody but at some cost to
households, so that only the neediest ones would participate (the most common intervention of this type is public works, where work is offered to all people willing to work, but at low wages).

13
3. Poverty and vulnerability profile
36 Cambodia has emerged from three decades of instability with an impressive record of sustained growth and poverty reduction. While still living with the legacy of genocide, social upheaval, civil war, and political violence, Cambodia is now experiencing a period of peace and stability with an open economy and a fledgling democracy. The last decade has been characterized by high rates of sustained economic growth, averaging seven percent GDP growth per year between 1997 and 2007. Over the same period, per capita income doubled from US$285 to US$593 per year. Such growth pattern has raised living standards and reduced poverty, which fell from an estimated 45‐50 percent in 1994 to 35 percent in 2004 and 30 percent in 20072. Rising incomes and improved public services have contributed to improving human development indicators. Rapid growth and poverty reduction were accompanied by structural transformations—integration into the regional and global economy, a gradual shift of employment from agriculture to manufacturing, and migration from rural to urban areas.
37 Despite impressive poverty reduction, one out of three individuals continues to live below the
poverty line. Poverty incidence largely remains a rural phenomenon. While poverty rates decreased in both urban and rural areas, inequality and the urban‐rural divide increased between 1993‐94 and 2007. Less than one percent of the population in Phnom Penh was deemed to be poor in 2007, compared to more than twenty percent in other urban areas, and almost 35 percent in rural areas, where approximately 80 percent of the population lives (Table 1). While inequality in Phnom Penh has decreased, it has increased in other urban and rural areas – leading to an overall increase in inequality from a Gini coefficient of 0.39 to 0.43 in only three years3. A large proportion of the population also remains near‐poor and vulnerable to shocks that can push them into poverty.
38 An increasing number of rural households have also become landless since land redistribution
in the 1980s. A 2004 Oxfam study estimated that 20% of rural households were affected by landlessness, with those affected rising by 2 percent per year. Another 25 percent of households have less than 0.5 hectares, an insufficient amount of land to sustain them. The poor also lack or have few basic assets that ensure a flow of income and can act as collateral to gain credit: these include draft animals or adequate housing. Lack of assets also means that the poor have few instruments to cope with consumption or income shocks.
2 The baseline poverty estimate is less precise because the 1993/4 survey did not cover the full rural
population (due to security concerns relating to the ongoing civil conflict). As such, this figure is estimated by identifying the poverty trend within the directly comparable geographical area covering the sampling frame of the 1993/4 survey, and then extrapolating this trend to the whole country.
3 The Gini coefficient is a measure of overall inequality, in which a value of zero represents a theoretical maximum of absolute equality, and a value of one represents a theoretical maximum of absolute inequality.

14
Table 1: Poverty and inequality trends % Population
1993/94 2004 2007 2004 2007
Phnom Penh 9.9 11.4 4.6 0.83 0.37 0.34Other Urban 10.2 - 24.7 21.8 0.44 0.47Rural 79.8 - 39.2 34.7 0.34 0.36Cambodia 100 47* 34.7 30.1 0.40 0.43
Poverty Headcount (%) Gini Coefficient
Source: Knowles (2008) for the 2004 and 2007 data; and World Bank Cambodia Poverty Assessment (2006) for 1993/94 data. Due to limited coverage of the 1993/94 survey, poverty data for Cambodia in 1993/94 have been extrapolated.
39 The non‐diversification of household economies exacerbates the vulnerability of rural
Cambodians. Most rural households rely heavily on subsistence agriculture for their livelihood, with rice cultivation accounting for 90 percent of total cultivated area and 80 percent of agricultural labor input. Cambodia’s unique hydrological regime and very low levels of coverage by water control infrastructure means that agricultural production (and thus household food security) is heavily dependent upon the weather and can fluctuate significantly from year to year. In the first half of this decade, unusual floods and droughts severely affected large parts of the countryside (Table 2), resulting in three years with negative rates of agricultural growth. Table 2: Estimated impact of extreme floods and droughts, 2000‐2005
Year Flood / drought
Population affected (millions)
Provinces affected
Estimated deaths
Estimated damage ($m)
ha. of crop Growth in agricultural
GDP Damaged Destroyed
2000/01 flood 3.4 19 347 157 374,174 ‐ 0.4%
2001/02 flood 2.1 62
36 250,000
3.6% drought c. 0.5 6
2002/03 drought 2
all (8 acutely)
22 134,926 ‐ 2.5%
flood 1.5 29 12 40,027
2004/05 drought 2 14 21 62,702 ‐0.9% Source: ADI (2007), compiled from various sources; agricultural GDP from NIS.
40 Rice yields remain among the lowest in the region due to limited and poor use of improved
seed, fertilizer, tillage, and water management. Because productive off‐farm opportunities are limited, rural households lack alternatives that would allow them to maintain stable incomes or cope in times of poor harvest.
41 Recent global economic shocks threaten to have considerable negative impact on economic
growth and poverty reduction. As of February 2009, rice prices remained about 60 percent higher than in January 2008. With food accounting for 60‐70 percent of rural household expenditures, and rice alone comprising 40‐50 percent, the high cost of food has had a significant impact on rural households, who represent roughly 90% of all poor in the country.
42 More recently, the global financial crisis is affecting Cambodia through dramatic declines in
external demand within Cambodia’s key manufacturing and service sectors. Recession in the US and Europe in particular are affected Cambodia’s garment exports and tourism revenues; recession is also affecting FDI flows, particularly into real estate. The result is significant job losses and reduced earnings for Cambodians working in garment factories, tourism or the construction industry (Kang et al 2009; CDRI 2009 forthcoming). In the absence of safety nets system to provide them with subsistence income, these laid off workers are at high risk of falling

15
into poverty. These recent job losses exacerbate a more long‐standing problem of pronounced youth underemployment: more than 200,000 young Cambodians currently enter the workforce every year, with many struggling to find adequate jobs.
43 Overwhelmingly, poverty in Cambodia reflects the presence of young and many children in
the household. Nearly one‐third of the population lives in households with seven or more members which have a poverty rate of 42 percent, against an average of 30 percent. Accordingly, 2007 data show that the poverty rate for children aged 0‐5 is 37.7 percent (that is, 37.7 percent of children live in a poor household), while the poverty rate of people aged 65 and over is 25 percent (World Bank, 2009). Less than 4 percent of the population lives in single‐person or two‐person households: their poverty rate is less than 8 percent (World Bank 2009). There are too few child‐ and teen‐headed households to generate a statistically significant measurement of their poverty level, but anecdotal evidence (World Bank 2006b) and reporting by NGOs suggest that such households constitute part of the extreme poor. In urban areas, extremely poor groups include homeless people and garbage scavengers.
44 With the majority of the population engaged in subsistence agriculture, food insecurity is a
dominant feature of poverty and vulnerability in Cambodia. In the 2001 Participatory Poverty Assessment (PPA), respondents cited “being hungry” as their primary concern. Although overall food and rice availability has improved in recent years, chronic food insecurity is faced by many subsistence farmers, landless or marginal land holders, the urban poor, and other vulnerable groups. An estimated one in five rural inhabitants is unable to secure enough food to meet the nutritional norm of 2,100 calories per day.
45 The immediate outcomes of food insecurity include child malnutrition and high child and
maternal mortality rates. Child malnutrition is widespread. The 2005 Cambodian Demographic Health Survey found despite significant improvement since 2000, 43% of children aged 0 to 5 were still chronically malnourished (stunted), 28% were underweight, and 8% were acutely malnourished (wasted). Poor dietary diversity, with 76% of calories provided by rice and other cereals, results in severe micronutrient deficiencies among the most vulnerable: according to the WFP, Cambodia is among 36 countries with the highest burden of child under‐nutrition in the world, and one of 33 “alarming or extremely alarming” countries in terms of hunger and under‐nutrition. Cambodian rates for child and maternal mortality rates are also amongst the highest in the region.
46 Emerging evidence suggests that recent global economic shocks are starting to reverse
progress made in previous years. Estimates up to and including 2007 suggest that child nutrition and survival rates, while poor, were improving over time. However, the Cambodia Anthropometric Survey (CAS) in late 2008 suggests that the decline in child malnutrition and ill health has now stagnated and possibly started to reverse (National MCH Centre et al 2008). It also draws attention to the differentiated effect of the crisis on child development, with widening disparities emerging between different groups in Cambodian society.
47 With youth and rural residents comprising the majority of the vulnerable in Cambodia, safety
net programs are an important asset for improving human development indicators and reducing inequality. Common and serious vulnerabilities include poor nutrition, lack of effective access to education, and risks of unemployment, underemployment and low wages faced by the working poor. To address malnutrition and dropouts, some incentive‐based safety nets may

16
help the poor while addressing the root causes of vulnerability: for example, drawing on the successful experience of Cambodia’s scholarship program under the Education Sector Support project, cash transfers based on the conditionality of mothers and children attending health checks and courses on nutrition could assist in improving malnutrition rates. Workfare programs could also act as a solution for the working poor in rural areas, providing a flow of income during the lean season. Such programs could also be applied to urban areas to address specific issues faced by the poor and vulnerable where pockets of poverty are present.
48 Disabled people are also a vulnerable group. Those with a pronounced disability constitute
around 1‐2 percent of the population (World Bank 2006c), but if disability is defined as people with functional limitations that preclude them from full participation in economic and social life the percentage in Cambodia would rise much higher— up to 10‐12 percent of the population according to some estimates (Mont 2007). If the extra costs of disability were taken into account, households with disabled members would be significantly poorer than households without disabled members (Braithwaite and Mont, 2008 and 2009).
17
4. Inventory of social protection and safety net interventions
49 The social risk management framework, which links a vulnerability profile to existing interventions, is a useful instrument to identify gaps in coverage. The risk management framework (Holzmann and Jorgensen, 2000) analyzes social protection issues by type of risk and the three strategies available to deal with risk (prevention and mitigation actions taken in advance of a shock, and coping strategies adopted after a shock has occurred). The framework reviews three levels of formality of risk management (informal household or community‐based arrangements; market‐based arrangements such as private insurance; and public sector arrangements managed by the state); and the many actors involved (individuals, households, communities, NGOs, governments at various levels and international organizations), all against a background of asymmetric information and different types of risk. This expanded view of social protection focuses specifically on the poor (as they are the most vulnerable to risk and typically lack appropriate risk management instruments) and emphasizes the double role of risk management instruments in (i) protecting basic livelihood as well as (ii) promoting risk taking.
50 In Cambodia as in all societies (especially societies without an extensive government safety
net), social practices provide an element of informal social protection. Individuals and households may be able to draw on help from relatives, neighbors or other social contacts to manage risk; smooth out highs and lows in household income and consumption; and obtain help in times of crisis (McAndrew 1998; Kim 2001). Public safety net strategy should reflect understanding of these informal social protection practices of households and communities: policies and programs should seek to complement the positive effects of these practices, or at least avoid undermining them (Norton et al 2001; Morduch and Sharma 2002). Flows of gifts from wealthier individuals (generally in urban areas) to poorer communities (generally in rural areas) may also play an informal social protection function under some circumstances.
51 However, policy‐makers need to be realistic about the limits as well as the potential of
informal social protection practices, which evolve over time in response to broader economic and social change. In Cambodia, traditional practices, rooted in trust that existed within small, stable rural communities, have been eroded over time by the effects of civil war, revolution and displacement in the 1970s and 1980s. It seems that they have also been transformed by the spread of market economics since the early 1990s (Krishnamurthy 1999), which has improved living standards, but has also increased population mobility, intra‐community inequalities, and commodification of inter‐household exchanges previously conducted upon the basis of reciprocity (e.g. allowing others to cultivate a portion of one’s land, but now for a fee).
52 Logic and comparative research suggests that informal safety net practices start to fail in the
face of an economy‐wide crisis. When everyone’s incomes and living standards fall at the same time, it becomes harder for households to help each other out. Ongoing research by CDRI finds evidence of this process in Cambodia. The price and financial crises are compounding a rise in vulnerability driven by more long‐term processes of increasing land concentration and decreasing access to common property resources. In this context, households are finding it more difficult to extend assistance to one another, and are rationing this assistance. Rural households report that while some forms of inter‐household assistance remain common (e.g. looking after another family’s children, sharing information on opportunities, pooling resources for funerals), others (providing small loans of cash or food at no interest) are increasingly

18
extended only to close relatives, or may be fully or partially commodified. Those surveyed also report that pagoda associations are increasingly forced to target more narrowly, restricting their support only to the elderly without families (CDRI, 2009 forthcoming).
53 Similarly, there are limits to the safety net functions that can be played by gifts from wealthier
individuals in urban business or government positions to rural communities. These may provide useful short‐term assistance: but the size of these flows and their effectiveness in helping households to manage risks and crises is likely to vary greatly over time and from one community to the next. This lack of predictability limits their value in helping households make long‐term decisions (such as whether to keep children in school or sell assets to deal with a protracted crisis): being able to depend on availability of benefits when needed is (or should be) a key advantage of a formal, government‐provided safety net system.
54 Thus, there is a clear need for an expanded and coherent government safety net system to
complement informal arrangements. The social risk matrix in Table 3 helps to classify broad categories of risk and vulnerability facing Cambodians, and to then identify what existing public sector social protection instruments currently exist to help individuals and households manage each of these risks. (A more comprehensive classification could provide details on coverage or benefit levels for each of these interventions. However, this level of detailed information is not available currently for many of these programs.) As discussed later below, a review of this matrix reveals that in relation to the critical risks faced by Cambodian households, the ongoing set of social protection interventions tends to fall short of needs, in terms of typology of programs, their coverage, and the overall spending.
55 Despite upward trends, the social sector spending remains low by East Asian standards. The
RGC budget for social ministries increased by one‐half of a percentage point between 2004 and 2009, from 2.6 percent to 3.1 percent of GDP.4 This is still lower than the regional level: in East Asia, average public spending on education alone was 4.3 percent in 2004 (Figure 1).
Figure 1: Trends in overall social spending (% of GDP)
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
2004 2005 2006 2007 2008 (Est.) 2009 (Est.)
Health Education Social AffairsLabor Total Womens Affairs
Source: MEF and World Development Indicators.
4 The Royal Government of Cambodia includes in the classification of social Ministries the Ministries for
Information, Culture and Fine Arts, Environment, and Cults and Religion. However, for the purpose of this review, a more conventional definition of social sectors is adopted, limited to the Ministries of Education, Youth and Sports (MOEYS); Health (MoH); Social Affairs and Veterans and Youth Rehabilitation (MOSVY); Labor and Vocational Training (MOLVT); and Women Affairs (MOWA).

Table 3: Risk management matrix
Risk Reduction Measures
Formal sector/Contributory systems General subsidies Safety nets
Lifecycle
Hunger/Children’s development - Social Cash Cards (MoSVY) - School feeding programs, take home rations, FFW programs (RGC,WFP)
- Child Survival (UNICEF)
Illness/Injury/Disease
- Cambodia National Insurance Company (CAMINCO)
- NSSF: Workmen compensation (MoLVT) - NSSF: Health Insurance (planned) (MoLVT)
- Exemptions at Health Facilities for poor patients (MoH) - Health Equity Funds (MOH, USAID, BTC, WB, ADB) - Maternal and Child Health Service in Rural Area (MoH with support from various donors inc. Japan, EU/EC)
- Hospital policy and micro‐insurance (e.g. France) - Community primary health services programs (RGC with support from e.g. Belgium, Netherlands, UK, EU/EC)
- Community‐based Health Insurance by private non‐profit organizations( GRET, CAAFW, BFH, RACHA, CHHRA/Malteser)
Death - Orphans and widow allowances (MoSVY)
Disability - Invalidity Pensions (MoSVY)
Old Age
- Civil Servants and Veterans Retirement pensions (MoSVY)
- Old People’s Associations (MoSVY) - NSSF: Employer based pension schemes (planned) (MoLVT)
- NCSSF: Health Insurance(planned) - (MOSVY)
Economic
End of source of livelihood (i.e. crop failure, cattle disease)
Unemployment
- Labor intensive public works programs (WFP food for work program, ILO labor intensive infrastructure programs.)
- Vocational training (WFP)
Low income/Pro poor programs
- Subsidizing rice in Phnom Penh and Siem Reap through the release of 300MT of rice. (RGC)
- Eliminate Suspension of rice exports (RGC)
- Suspension of duties and VAT to reduce price of agricultural inputs (RGC)
- Expanded, subsidized distribution of seed and fertilizer to smallholder farmers and assessment (RGC)
- Food distributions (MEF/ADB, WFP/Spain)
- Scholarship for the poor program (MOEYS, WB)
- Basic Education Programs (MOEYS, ADB, Belgium, EU/EC, Finland, Netherlands, Sweden, UNICEF, WB)
Social/ Governance
Exclusion, losing social status/capital Extortion, corruption
Crime, domestic violence - National Action to Combat Violence Against Women (RGC)
- Child Protection Program (UNICEF)
20
56 Given the current budget structure, it is hard to determine the level of Government spending on social protection and safety nets. The new budget structure, in use since 2007, has two chapters (64 and 65) in which there are items labeled as social interventions. 5 (The detailed budget allocation for these two chapters across all government agencies is presented in the separate inventory document). Government expenditure on these items amounted to a total of US$181 million across all Government agencies in 2008, showing a 55% increase since 2007. Nevertheless, given the level of aggregation in the budget, it is not possible to determine how much of this amount goes to social protection and safety net activities, and how much to other types of social interventions. Furthermore, nearly all existing Government agencies report spending on these chapters, though not all are actually mandated with a social agenda.6
57 Unconditional cash and near cash transfers appear to target mostly public employees and
formal sector workers, rather than the rural poor. The Ministry of Social Affairs, Veterans and Youth Rehabilitation (MoSVY), responsible for social security programs for public sector employees, and the Ministry of Labor and Vocational Training (MoLVT), responsible for private sector workers, spent roughly US$35.7 million on social interventions in 2008, 98 percent of which was spent by the MoSVY (US$35.0). The majority of funds are spent on unconditional cash and near cash transfers for the civil service and veterans, which relate more to social protection than safety nets. All retired and disabled civil servants and veterans, as well as their widows and orphans, are entitled to benefits in the form of a pension and compensation. The MoLVT on the other hand, is responsible for the National Social Security Fund (NSSF), established in 2008, which is set to provide by 2012 all private sector employees of firms with more than eight employees with: (i) employment injury coverage; (ii) health insurance; and (iii) pension coverage. With the introduction of the NSSF, social spending of the MoLVT increased by over 300% since 2007, to roughly US$668,000 in 2008. As of February 2009, the NSSF had enrolled roughly 400 firms in the Employment injury scheme, about 250 of which are garment factories, covering a total of roughly 300,000 workers.7
5 Chapter 64.5 is called “Allowances and Social Transfers”, and includes: 1. Family 2. Health and birth
giving 3. Death 4. Retirement 5. Demission 6. Work accidents and Invalidity 7. Orphans of personnel 8. Other 9. Return Attenuation. Chapter 65.7 refers to “Social Assistance”, which includes 1. Assistance for hospitalization 2. Medicaments 3. Food and supplies 4. Natural Disaster 5. Research Stipends 6. Local scholarships and research 7. Scholarships and research for abroad 8. Others. Chapter 65.8 refers to “Subsidies to cultural and social entities”, including subsidies to 1. Communities 2. To orphan centers 3. For travel scholarships 4. For the Red Cross 5. For sport and culture community 6. To rehabilitation centers 7. King affairs (King’s charity programs).
6 To a large extent, the observed increase in social spending between 2007 and 2008 is due to increases in spending by non‐social ministries, such as Ministry of Water Resources and Meteorology, the Constitutional Council, the Ministry of Industry, Mine and Energy, and the Ministry of Agriculture, Forestry and Fishery. As a consequence, it is hard to assess whether the observed increase corresponds to an actual increase in spending on social programs (in particular safety nets).
7 Data and the description of the NSSF coverage and workings were collected through personal interviews with NSSF representatives.
21
Safety net spending and implementation
58 Safety nets in Cambodia comprise scholarships, fee waivers, and exemptions. The Ministry of Education, Youth and Sports (MoEYS) initiated implementation of a Scholarship for the Poor program in 2006. As of October 2008, the program covered 21,459 secondary school children across all provinces with the exception of Phnom Penh. Eligible children are selected through an ad hoc mechanism: school management committees distribute a form for students to fill in, collecting information on their living standards. The school then collects all forms and compiles a database, which is sent to the MoEYS. The latter contracts a private firm to calculate an index based on the collected information, and the MoEYS awards scholarships to the 50% of students with the highest poverty index. The poorest half of that 50% is labeled ‘very poor’ and the other half ‘medium poor’. An evaluation of the Scholarship for the Poor program has shown that it has increased enrollment by 20 percent (Filmer and Schady, 2009): building on this success, a pilot is currently underway aiming to expand the program in primary schools.
59 User fee exemption policies backed by Health Equity Funds (HEFs) are used to improve access
to health care for the poor (UNICEF 2008). HEFs reimburse health providers for caring for patients who are classified as poor: this protects poor patients against out‐of‐pocket user fee payments which might otherwise prevent or deter them from obtaining treatment, while ensuring that facilities still receive income (without which an exemption policy might create an incentive to deny or ration treatment to poor patients). HEFs work closely with the MOP Identification of Poor Households Program (see Box 1). Poor individuals, whether identified through the Identification of Poor Households process or through an in situ assessment of poverty level by medical staff, are covered for all costs of hospitalization and other medical services, as well as expenses for transportation and food during their stay in the hospital.
60 As of March 2009, there were 50 HEFs in place in Cambodia, covering about 3,168,883 people or about 68% of the poor population in Cambodia. HEFs are managed through cooperative arrangements between Government, Development Partners and local NGOs and financed by a combination of a regular government budget and additional support from development partners (for a total of US$1.4 million in 2008). Health equity funds serve as an important complement to existing supply‐side subsidies, which are aimed at lowering the cost of health care but generally do not reach the poor because of barriers to access such as unofficial demands for payment.
61 One drawback of Health Equity Funds is that they do not protect people who are above the
poverty line but at risk of falling into poverty due to health care costs. One way to address this is the implementation of community‐based health insurance (CBHI) schemes which target the near‐poor who can afford to pay a minimal amount for premium contribution in exchange for a defined health care benefit package. There are currently 12 schemes in the country covering about 73, 828 members. As a way to broaden coverage, increased sustainability, efficiency and purchasing power, a pilot project linking health equity funds and CBHI was implemented. Equity fund pilots in other countries address this issue by covering health care costs above an annual or episode maximum for the non‐poor. This is an option which could be explored for Cambodia to increase the risk reduction impact of equity funds.
62 Apart from education and health interventions, safety net programs in Cambodia consist
mainly of food distribution, food for work, and labor intensive public works programs. In

22
October 2008, the Ministry of Economy and Finance implemented and co‐financed a US$40.08 million ADB‐supported food emergency operation to mitigate the effects of the increase in food prices on poor households. The emergency package consisted of a US$17.5 million grant and an additional US$17.5 million loan at concessional rates from the ADB. Approximately US$19 million is intended for social protection measures, with the remaining allocated to measures aimed at increasing food productivity and government capacity in implementing food security operations. In the first phase (October‐November 2008), roughly 342,000 beneficiaries in 200 communes received in‐kind assistance (35Kg rice rations) in seven provinces surrounding the Tonle Sap Lake. The MEF Project Management Unit (PMU) is now considering food‐for‐work assistance to help poor households in food insecure areas coping with the lean season for the next two years, as well as cash for work interventions in urban and other non food insecure areas.
63 The World Food Program (WFP) remains the largest implementer of safety net programs. in
2008 the WFP distributed 28,133 metric tons of rice to 886,929 beneficiaries, for a total value of US$23.2 million (Table 4). Through its Food for Work (FFW) program, in 2008 the WFP, working with the Ministry of Rural Development, provided roughly 3,795 metric tons of rice to 113,808 vulnerable beneficiaries in identified food‐insecure communes from the 12 most food‐insecure provinces, in exchange for work on public infrastructure projects, helping to mitigate critical food shortages among vulnerable households in Cambodia. The WFP also implements a nutritional program‐‐the Mother and Child Health (MCH) program—which distributes monthly food rations (consisting of rice, vegetable oil, fortified corn soy blend and sugar) to pregnant and lactating mothers living in poor households in food vulnerable communities. In 2008 the MCH distributed a total of 2,777 metric tons of food. The WFP works in partnership with local NGOs, who handle the food distribution, as well as health centers, which provide basic health education during the distribution. Other joint RGC‐WFP programs include school feeding, and food distribution to tuberculosis and HIV/AIDS patients (see Table 4). Table 4: WFP food distribution and beneficiaries in 2008
Activity
No. of Beneficiaries
Food Distribution (mt) Value (USD)
Total Female Rice Fish Veg. Oil Salt Bean CSB Sugar Total
Basic Education School 470,709 225,873 5,861.99 1,002.77 532.24 145.05 1,437.20 ‐ ‐ 8,979.26 Take‐home 114,063 57,033 2,492.50 0.04 167.21 ‐ 344.60 ‐ ‐ 3,004.35 Vocation 1,099 648 14.60 0.28 1.05 0.29 ‐ ‐ ‐ 16.22 Sub‐total 585,871 283,554 8,369.09 1,003.09 700.50 145.34 1,781.80 ‐ ‐ 11,999.83 9,900,000
Health & Nutrition TB 38,547 19,493 4,135.52 ‐ 102.86 68.79 ‐ ‐ ‐ 4,307.17 HIV/AIDS 89,870 46,289 4,971.19 ‐ 166.83 82.56 ‐ ‐ ‐ 5,220.58 MCH 57,306 41,609 1,107.81 ‐ 73.48 ‐ ‐ 1,428.12 167.41 2,776.82 Sub‐total 185,723 107,391 10,214.52 ‐ 343.17 151.35 ‐ 1,428.12 167.41 12,304.57 10,100,00
Disaster Risk Reduction FFW 113,808 56,903 3,795.23 ‐ ‐ ‐ ‐ ‐ ‐ 3,795.23 FFT 1,527 1,104 33.75 ‐ ‐ ‐ ‐ ‐ ‐ 33.75 Sub‐total 115,335 58,007 3,828.98 ‐ ‐ ‐ ‐ ‐ ‐ 3,828.98 3,200,000 Grand Total: 886,929 448,952 22,412.59 1,003.09 1,043.68 296.70 1,781.80 1,428.12 167.41 28,133.38 23,200,00Source: World Food Program.

23
64 UNICEF is among the most active Development Partners in supporting the Government in implementing safety net programs across various lines of social protection, ranging across education, health (including HEFs) and nutrition, and child protection. Since 2006, UNICEF has invested roughly US$16 million per year on strengthening basic social service provision, and plans to invest an additional US$13 million in each of 2009 and 2010 (see Table 5). UNICEF supports the Government by providing funds and developing Government capacity to define and implement its agenda. It works closely with Government at both national and sub‐national levels, including support to provincial, district and commune structures in six priority provinces (Kampong Speu, Prey Veng, Svay Rieng, Kampong Thom, Stung Treng and Otdar Meanchey).
Table 5: UNICEF safety nets budget, 2006‐2010 2006 2007 2008 2009 2010 Total
Child Survival 3,624 3,624 3,624 3,624 3,624 18,120 Seth Koma 3,260 3,260 3,260 3,260 3,260 16,300 Expanded Basic Education 6,100 6,700 5,450 4,000 3,450 25,700 Child Protecion 3,380 3,230 3,030 3,030 2,930 15,600 Total 16,364 16,814 15,364 13,914 13,264 75,720 Figures are in Thousands of US$. Source: UNICEF‐ Government Country Program Action Plan.
65 The Government also relies on Development Partners, mainly WHO, UNICEF, WFP and FAO, for support to nutrition. WHO and UNICEF provide significant technical assistance to the Ministry of Health, and more specifically the National Maternal and Child Health Center and the National Nutrition Programme in the area of nutrition‐specific policies and guidelines, integrated nutrition monitoring system, and capacity building of health staff at various levels in the area of infant and child feeding (i.e. early and exclusive breastfeeding, appropriate complementary feeding), micronutrient supplementation and management of malnutrition. Additionally, UNICEF works to support establishment of national community‐based systems for delivery of nutrition‐specific messages, services and food commodities and for development of improved practices in relation to nutrition practices at the community, family and individual level. WFP implements the Support for Mother and Child Health (MCH) Project in cooperation with the National Maternal Child Health Centre and NGO cooperating partners, such as RACHA and World Vision. Targeted to food insecure areas, the MCH Project seeks to reduce under‐nutrition among pregnant and lactating women and children 0‐24 months of age by integrating micronutrient fortified food, nutrition education and other health interventions provided through local health clinics. Despite these efforts and the progress already achieved, malnutrition levels in Cambodia remain high, and much work remains to be done in this area (National MCH Centre et al 2008).
66 Government and Development Partners are also making efforts to develop targeting
mechanisms to channel safety net assistance in a more cost‐effective manner. The most important targeting system is the Identification of Poor Households(IDPoor) program of the Ministry of Planning (MoP), supported by German Technical Cooperation (GTZ), which creates lists of poor households in all villages covered, compiles a Database of Poor Households, and issues Equity Cards to identified poor households (see Box 1). Currently, Health Equity Funds are the largest users of IDPoor data, for provision of free or subsidized health care assistance to the poor. However, there are many other current and potential users of the data. To further consolidate the IDPoor Program as the national targeting system, a Sub‐Decree has been drafted and submitted to the Council of Ministers, mandating the use of (i) IDPoor procedures for

24
identification of poor households and (ii) the data generated by these procedures for appropriate targeted assistance programs.
Box 1: The Identification of Poor Households Program
Government and Development Partners are developing interventions to better target assistance to the poor. The Government’s officially mandated targeting program in rural areas is the Identification of Poor Households (IDPoor) Program of the Ministry of Planning (MoP), which has received support by the German Government through German Technical Cooperation (GTZ). The IDPoor identification procedures are consultative and participatory, with village representatives themselves conducting interviews using a standard questionnaire with objective criteria based mainly on assets, combined with community consultation and validation. The MoP coordinates and monitors the entire process, distributes data on poor households to decision‐makers and service providers, and issues Equity Cards to poor households. During 2007 and 2008, the IDPoor program conducted identification of poor households in five provinces and a total of around 2100 villages and in 2009 extended its coverage to around 3000 more villages in seven provinces. All areas covered by the IDPoor system during that period have been areas in which Health Equity Funds (HEFs) operate, and poor households identified are entitled to receive free or subsidized medical assistance at public health centers. In addition to the 11 provinces partially or fully covered between 2007 and 2009 by the MoP, in the same period Health Equity Fund Implementers and their partners have been using the IDPoor procedures for identification of poor households in many other provinces and districts around the country, covering around 2,200 villages. Other organisations have carried out pre‐identification procedures in other areas of the country, but their methodologies differ among each other and from the official MoP procedures, and their results are not comparable.
While the IDPoor system is currently mostly used by Health Equity Funds for provision of services, many other programs and projects targeting the poor already use it or have the potential to use it (e.g. scholarships for the poor). The IDPoor system has also proven to be an effective targeting tool for emergency assistance: in covered areas, it has been used for instance to target emergency rice distribution by the ADB‐financed Emergency Food Assistance project, where in October and November 2008 about 68,000 households around the Tonle Sap lake (20% of poor families in 200 communes) received 35kg rice rations. An evaluation of IDPoor in 2008 showed a good degree of satisfaction among communities involved in the process, in particular regarding its accuracy (i.e. limited inclusion and exclusion errors), fairness and level of community participation. The IDPoor Program therefore has great potential to become a national targeting system that will improve the effectiveness, objectivity, and transparency of targeting of assistance to poor households in such fields as education, health, social protection, as well as in emergency operations. To further consolidate the IDPoor Program as the national targeting system, a Sub‐Decree has been drafted and submitted to the Council of Ministers mandating the use of the IDPoor procedures for identification of poor households and the data generated for appropriate targeted assistance programs. At the moment, the IDPoor Program only covers households living in rural areas, and no alternative targeting system has been developed to identify poor individuals living in urban areas.
67 Some workfare programs have also been put in place to assist the poor with under‐ and
unemployment and improve local infrastructure. In addition to WFP’s Food for Work program, the Government has endorsed labor‐based appropriate technologies (LBAT) to generate employment through improvement and maintenance of essential rural infrastructure. The ILO and the ADB have been the main Development Partners to provide assistance to the
25
Government in implementing the Mainstreaming Labor‐Based Road Maintenance to the National Road Network program. Between 2006 and 2008, the ILO channeled nearly US$4.8m, roughly half from the Government and half from the Japanese Fund for Poverty Reduction, to this project. Between 2007 and 2008 ADB also provided US$690,398 to implement a Mainstreaming Labor‐Based Road Maintenance to the National Road Network program. The Government implemented this project through two agencies and coordinated its efforts though the Technical Working Groups.
68 If well implemented, workfare is an effective safety net intervention to combat under‐ and
unemployment (del Ninno et al 2008). Workfare can be an effective safety net for the economically active poor, as it provides employment while at the same time contributing to development of local and national infrastructure. A key advantage of workfare is that it “self‐targets” by offering a low wage rate: it could be therefore a viable safety net intervention in urban areas, where other targeting methods have proven difficult to implement, but also in rural areas to help households cope with natural disasters and the lean season. However, international experience shows that political considerations have often threatened the long‐term sustainability of workfare programs: often, Governments have sought to win favor by setting the offered wage rate excessively high, attracting the near‐ and non‐poor in addition to the poor, and leading to unsustainable program costs or to the severe rationing of assistance excluding many households in need. Box 2: Workfare: evidence from international best practice
Current public works programs in Cambodia undoubtedly have helped provide employment to rural unskilled labor in Cambodia, and when food‐based, these programs have contributed to mitigating critical food shortages among vulnerable households. In planning future workfare interventions, some improvements to the current interventions based on international best practice could be considered:
• First and foremost, a credible Government monitoring system would need to be developed, along the lines of systems implemented in other countries;
• Information on the prevailing market wage rate for unskilled labor would need to be collected by province, in order to compare and adjust the public works wage accordingly, to that the public works wage is maintained at a level slightly lower than the prevailing market wage;
• It is very important to go beyond mere earth‐moving activity, and towards other tasks that are critical for improving labor productivity, and general rural development. To achieve this, it would be essential to provide for critical minimum non‐labor cost (at least 10%) and put in place technical supervision;
• At present there is no assessment of the quality of outputs. It is important to pay attention to the quality of outputs generated to ensure sustainability of the products: if outputs are not of reasonable quality, public works programs can become very expensive and inefficient programs;
• In order to attract women to worksites and render the program gender sensitive, it is best if work opportunities are provided as close as possible to households, to minimize time spent to get to the site. Over the medium term, public works activities could also include crèches, where women could leave their children and engage in community work activities;
• Lastly, it could make sense to move gradually from Food for Work to Cash for Work in the interest of reducing logistical costs, promoting a cash economy and ensuring vibrancy of grain and non‐grain markets.

26
5. Gaps and challenges of existing interventions
69 Safety net interventions in Cambodia face several challenges related to implementation, institutional, and financing issues. Given the many sources of vulnerability faced by the poor in the country, safety nets ought to be a key component of social protection development. Many challenges however remain in terms of: the instruments used to address vulnerability; the ability of programs to focus on the impoverished by accurately targeting communities and households; the institutional organization in place to implement programs and facilitate coordination among government agencies and donors; and the amount of resources allocated to safety net interventions.
Challenges in the implementation of existing interventions
70 Existing safety net interventions exclude some important vulnerable groups. Urban areas are often left out of current safety net interventions: while these are significantly less poor than rural ones, pockets of extreme poverty exist in urban settings. Existing interventions also often fall short of providing assistance to those who recently fell into poverty, or are poor for a transient period, such as farmers during the lean season or victims of natural disasters. In order to address these gaps, assistance could be provided by expanding and improving existing workfare programs in selected areas. Malnutrition also remains one of the most severe challenges in Cambodia, but instruments adequate to the magnitude of the challenge remain to be developed.
71 Cambodia has not yet made significant use of some types of safety net programs that have
proved successful in other countries. Over the last decade, a growing number of countries have achieved considerable success with conditional cash transfers (programs which provide households with cash payments so long as they make use of public services). Cambodia has achieved good outcomes through the Scholarship for the Poor program, but only on a small scale. Learning from this success, it may be worth piloting incentive‐based cash transfer schemes to address the problems of widespread stunting and wasting, by offering compensation that is conditional on bringing infants and children to health clinics for checkups and attending training on nutritional practices.
72 Existing interventions are largely food‐based. These arrangements have the advantage of
directly addressing shortages and providing households with a stable flow of food. However, in building a more comprehensive safety net system there may be potential for complementing this in‐kind assistance with cash‐based interventions which would help to address the whole range of vulnerabilities faced by households (such as cash strapping or inability to satisfy non food needs). In particular, it is worth exploring the potential for cash transfers, with or without conditions, to address the challenge of food insecurity and resulting child malnutrition. The fact that few cash‐based interventions have been piloted to date may reflect the strong fiduciary challenges faced by the country. Nonetheless, as the success of Health Equity Funds shows, solutions to these challenges exist; and the Scholarship for the Poor program, which has raised enrolment by providing poor families with cash transfers for keeping their children in school, suggests that there is unmet potential for cash‐based solutions.

27
73 Targeting has not yet been mainstreamed into safety net implementation, and even among safety net programs that make use of targeting, many still rely on ad hoc targeting procedures whose accuracy has not been investigated. Targeting of safety net interventions should be further promoted. Given the relatively high cost of targeting, it would be important to limit the number of targeting programs from which several safety net programs could draw. A strong candidate for further development is the Government’s Identification of Poor Households targeting system. Nonetheless, while initial analyses have shown a good degree of satisfaction with IDPoor’s accuracy, transparency, fairness and level of participation, a thorough study on the implementation procedures, the system’s robustness in terms of governance risks, and the accuracy of the results obtained would be helpful to further assess strengths and identify opportunities for improvement, taking into account international best practice. Poverty / vulnerability maps could be developed at relatively low cost and used to target certain forms of safety net support; and self‐targeted workfare may be necessary where ID Poor has not yet identified poor households, or in circumstances of rapid change when a significant number of people may have moved into poverty since the ID Poor exercise was last conducted.
74 Most programs in place have also limited geographical coverage. Few programs have national
coverage, and therefore neglect a considerable number of vulnerable poor. Furthermore, existing programs may not actually be covering regions that most need them. A geographically disaggregated analysis linking sources of vulnerability to program coverage may be useful, since it would allow better identification of coverage gaps and targeting of existing resources towards the most vulnerable regions.
75 Finally, there is a need for better monitoring and more rigorous evaluations of existing
interventions to increase their effectiveness, by rapidly addressing implementation challenges and drawing from international best practices. Few interventions or institutions are actually collecting critical monitoring information, which makes it difficult to assess the effectiveness of ongoing programs. Moreover, there are few rigorous and thorough evaluations of existing safety net interventions, making it difficult to assess how well they perform by international standards, and where there would be areas for improvement.
Institutional challenges
76 Safety net implementation often reflects immediate priorities (such as the need to respond to the food crisis) rather than a shared longer‐term vision for safety net development. Frequent changes in priorities dictated by unexpected events such as the food and financial crises hinder the establishment of a longer‐term strategy for safety net development, which would eventually allow not only long‐term protection of the poor and vulnerable, but also more effective rapid responses. Moreover, safety net spending sometimes reflects priorities dictated by Development Partners’ interests and earmarked funding sources. This leads to relatively large sums available for safety net interventions in some sectors (such as workfare), while other equally if not more important areas (such as malnutrition) remain largely uncovered.
77 Government and Development Partners should seek better coordination across interventions.
In the absence of a coherent social protection strategy, a patchwork of programs currently exists, which now needs to be adapted into a coherent safety net framework. For this to happen, an analysis of priorities in addressing sources of vulnerability should be performed as a
28
first step. Thereafter, a strategy for safety net implementation should be developed (for instance under the umbrella of the Technical Working Group for Food Security and Nutrition), and both Government and Development Partners should coordinate safety net implementation along the lines of the developed strategy.
78 As with all public policy, the design of a safety net system for Cambodia needs to be adapted
to the capacity of the public sector institutions that must then implement this policy. Different policies and programs will have different requirements in terms of financial and human resources and the kinds of institutional arrangements needed for successful implementation. Where the capacity for implementation is currently lacking, it needs to be built over time, with resources and time allowed for this process.
79 A major constraint for addressing these institutional challenges is the lack of a Government
body with a clear mandate to coordinate interventions across ministries and Development Partners, and to facilitate and monitor implementation of cross‐sectoral interventions. As in many countries, safety net interventions are scattered across several ministries. The MoSVY, MOLVT and the Ministry of Women’s Affairs (MOWA) are all mandated with managing state social services for the wider population, and helping to protect specific vulnerable groups against risks. However, no Government body has the mandate to coordinate safety net interventions across ministries and Development Partners, as well as to implement cross‐sectoral interventions. The lack of a clearly designated agency with responsibility for defining an overall strategy significantly impedes the development of a comprehensive social protection and safety net system and of large‐scale cross‐sectoral interventions.
80 Both central and sub‐national capacities matter for the successful implementation of safety
net policies and programs. Sub‐national authorities already have important roles to play in managing the targeting process under the Identification of Poor Household program. The ongoing process of decentralization and deconcentration (D&D) is expected gradually to transfer functions to Province, District and Commune levels: this D&D process needs to be taken into consideration when allocating responsibilities and powers for different aspects of safety net implementation between national and sub‐national authorities. In the second half of 2009, research undertaken as part of a broader review of progress in public financial management reform will assess the ability of sub‐national authorities to manage, monitor and account for safety net programs.
81 As an underlying challenge, the budget for safety net implementation remains low, with the
majority of funding provided by Development Partners and earmarked for interventions that are often implemented in parallel to the Government system. Government budget for safety nets remains low. Moreover, most programs are implemented by Development Partners, thus leaving concerns regarding the long‐term sustainability of such programs. Ways to incorporate programs led by Development Partners into the Government’s own agenda should be explored as part of the process of developing a comprehensive safety net strategy.

29
Annex 1: Inventory of Social Protection Interventions
The current framework for social protection in Cambodia
Policy framework for social protection
82 The Government reiterated its commitment to alleviating poverty through social protection. In the Second Phase of the Rectangular Strategy for Growth, Employment, Equity and Efficiency, announced in September 2008 by HE the Prime Minister of Cambodia, the Royal Government sets out to:
i. Give priority to improving working conditions for workers and employees,
ii. Enforce of Social Security Law,
iii. Implement benefit and pension schemes for people with disabilities and their dependents;
iv. Ensure protection of those covered by the Labor Law; and
v. Make available to all employees insurance coverage against workplace accidents.
83 The Royal Government also intends to continue to strengthen support to people with disabilities and families of veterans, as well as retired civil servants and veterans. This will be achieved by implementing a comprehensive pension system under the National Social Security Fund (see Section II). In this context, the government intends to promulgate a "Law on the Comprehensive National Social Security Fund" and a "Law on the Establishment of National Pension for Veterans".
84 The Second Phase of the Rectangular Strategy will continue to be operationalized in the National Strategic Development Plan (NSDP), which will be extended to 2013. In the NSDP 2006‐2010 Midterm Review, the RGC explicitly recognizes as a challenge for the next years to provide safety nets to the poor during times of inflationary stress, particularly shortage of the staple rice, through targeted subsidies and tax relief on essential commodities. The RGC also identifies the urgent need to implement measures to ensure safety nets for the most vulnerable through subsidies and targeted labor intensive work like food for work programs, as means to reduce poverty.
85 The NSDP Midterm review explicitly addresses the issue of increasing inequality. It recognizes that this trend, evident in increasing disparities in income, consumption and economic opportunities between urban and rural areas and high and low income groups, can be addressed by more and focused attention to rural areas and agricultural production; and by ensuring that adequate safety nets exist to stop low income groups sliding back into poverty.
86 The NSDP Midterm Review also reaffirms that a proper nutritional status of all Cambodians, particularly the vulnerable is an important element of national development. Food security and nutrition is recognized in the NSDP as a cross‐cutting issue: achieving progress here depends on the synergy of growth and output from many sectoral activities as outlined in the Strategic Framework for Food Security and Nutrition. The NSDP envisages that targeted efforts in various sectors will ensure that “poor and food‐insecure Cambodians, by 2010, have substantially

30
improved physical and economic access to sufficient, safe and nutritious food at all times to meet their dietary needs and food preferences to an active and healthy life”. Overall food security outcomes (improved nutritional status) have been improving steadily since 2000, thanks to the fast growing economy; agricultural growth; increasing availability and affordability of food; and healthier food intake, supported by health and nutrition education, micronutrient supplementation and fortification programs (iron, vitamin A) and continued enforcement of universal iodisation and food safety standards. It is important that progress so far is sustained in the future: rapid increases in food prices threaten food security and nutrition for the very poor and vulnerable (see box 2.1), which needs to be monitored closely. Of particular importance is to track periodic progress or changes in stunting and underweight status among children (as sub‐indicators).
87 The need for a Government safety net strategy was discussed at the Second Cambodia Development Cooperation Forum (CDCF) in December 2008. At the CDCF, HE the Deputy Prime Minister Keat Chhon assigned to the Food Security and Nutrition Technical Working Group (TWG FSN), co‐chaired by the Council for Agricultural and Rural Development (CARD) and the World Food Program (WFP), the responsibility to undertake a review of safety net interventions and elaborate options for a safety net strategy. At the Third Cambodian Economic Forum (organized by SNEC on 5 February 2009 in Phnom Penh), development partners welcomed and supported the RGC’s recent commitment to implement a coordinated social safety net system as an important initiative and essential element in protecting the poorest and most vulnerable from possible economic shocks.
Legal framework of social protection in Cambodia
88 The fundamental commitments to provide social protection for Cambodians lie in the Constitution, which contains articles on the rights of citizens and responsibilities of Government related to social protection. For example8:
i. Article 36: “Every Khmer citizen shall have the right to obtain social security and other social benefits as determined by law. Khmer citizens of either sex shall have the right to form and to be member of trade unions. The organization and conduct of trade unions shall be determined by law.”
ii. Article 46: “The commerce of human beings, exploitation by prostitution and obscenity which affect the reputation of women shall be prohibited…The state and society shall provide opportunities to women, especially to those living in rural areas without adequate social support, so they can get employment, medical care, and send their children to school, and to have decent living conditions.”
iii. Article 72: “The health of the people shall be guaranteed….Poor citizens shall receive free medical consultation in public hospitals, infirmaries and maternities. The State shall establish infirmaries and maternities in rural areas.”
iv. Article 75: “The State shall establish a social security system for workers and employees.”
89 Several organic laws have been passed to codify some of the social protection related tenets of the Constitution. The most relevant laws which have been adopted or are currently under consideration include: 8 From World Bank (2006), p. 35

31
i. The Labor Law passed in October 1998. This law provides for a standard legal workweek of 48 hours, not to exceed eight hours per day. It also stipulates time‐and a‐ half for overtime, and double time if overtime occurs at night, on Sunday, or on a holiday. The minimum allowable age for a salaried position is set at 15 years, or at 18 years for anyone engaged in work which may be hazardous, unhealthy, or unsafe. The Labor Law embodies most of the ILO conventions on core labor standards, all of which Cambodia has ratified. The application and enforcement of labor standards in Cambodia is discussed in greater detail below.
ii. The Insurance Law passed in June 2000. The insurance law provides a legal framework for better regulation of insurance market activities. To help develop the insurance sector, the RGC envisages an expansion of the activities of the state‐owned Cambodian National Insurance Company (CAMINCO) to include life insurance, pensions, credit, and natural disaster insurance. However, these insurance schemes will benefit only a small proportion of the population in the initial stages and most likely will not be accessible to the poor, who lack the surplus funds necessary to insure their risks.
iii. The Law on Social Security Schemes for Persons Defined by the Provisions of the Labor Law passed in September 2002. This law entitles workers and employees in the private sector to old age, invalid, and survivors’ benefits as well as workmen’s compensation. The law has been promulgated but not implemented since it requires a sub‐decree on the National Social Security Fund (NSSF), which will cover employment injury insurance (EII), the pension scheme, and a short‐term benefit system. Notably, the EII would cover the formal sector as well as the self‐employed based on voluntary participation. However, as in the case of the Insurance Law, only a very small segment of the population is expected to benefit from the Law on Social Security Schemes given the small size of Cambodia’s formal sector.
iv. A National Action Plan to Combat Violence Against Women has been developed, and is being implemented in accordance with the Law on the Prevention of Domestic Violence and Protection of Victims adopted in 2005.
v. The Law on Suppression of Trafficking in Humans and Sexual Exploitation, adopted in late 2007, consistent with the UN Palermo Protocol. The draft law provides for heavier punishment if victims are below 15 years of age and gives police more power to investigate and arrest suspected traffickers
Historical background on social protection in Cambodia
90 Prior to the war in 1970, Cambodian social practices of sharing, extended families and neighbor networks, and general community self‐help activities provided aspects of informal social protection. The monks and the pagoda played an important role in offering meals and temporary shelter to poor and vulnerable people within the community; in times of family shortage, young men could enter the monastery. The most important source of protection was through extended family structures, which provided assistance (generally in kind) to people in need9.
9 This section draws on Ngy (2009). Only a few research studies were carried out before the war and as a result we
have relatively little knowledge of how people traditionally coped in times of difficulties. Some insights can be obtained from Ebihara (1968); Delvert (1961); and personal accounts such as Meas (1995). See also discussion of pre‐war social organization in Kiernan (1982).
32
91 The dramatic socio‐economic and political changes of the past two decades have had significant impact on the social fabric of Cambodia. The structure of Cambodian society has changed and its culture has been dislocated. None are more vulnerable to these upheavals than children and women. Families, which provide the first safety net for the survival, protection and healthy development of children, have been fragmented and weakened by death and separation. Communities or villages, once composed of extended family networks established for generations, have been shattered and reformed by forced population movements, displacement, and repatriation (UNICEF 1995). This tradition is still playing a role as an informal social safety net in the modern history of Cambodia, where wealthy families, high ranking officials, business people and communities extended their own private means to assist and offer help to others.
92 The Paris Peace Agreement was signed in 1991, ending more than two decades of conflict, social dislocation and the destruction of infrastructure and facilities in Cambodia. The first democratic election was organized and a new Royal Government was established in 1993. This marked the beginning of a transition from a phase of war towards peace, from a culture of continued conflict to a culture of greater compromise, dialogue and reconciliation. In response to the challenges, the strategy for the National Program for Rehabilitation and Development of Cambodia (NPRDC) was developed, adopted and implemented. The broad aims of the RGC were set out in the NPRDC in February 1994, and elaborated in the objective of the NPRDC in February 1995 ("striving to achieve a sustainable growth with equity and justice").
93 The NPRDC declared war on poverty, and the development of the rural areas is seen as critical to raising the living standards for the majority (85%) of the Cambodian population. Rural development was also seen as an important contribution toward national integration, reconciliation and security10. Since 1993, rural development has played an important role in implementing and achieving the goals and targets set by the RGC’s various policy documents such as the NPRDC, the first (1996‐2000) and second (2001‐2005) Socio‐Economic Development Plans (SEDP I and II) and the 2003‐2005 National Poverty Reduction Strategy (NPRS). Work in the rural development sector has contributed toward the reduction of poverty in rural areas through decentralized and participatory approaches to improving access and to creating opportunities. The vision of “Returning to the Villages” was and continues to be the theme for activities that seek to alleviate poverty through the implementation of projects and programs that will improve rural access to socio‐economic services and strengthen and empower grass‐roots organizations at the village level to achieve sustainable development and self‐reliance.
94 In response to the needs in rural areas, external assistance has been provided to rural development projects and programs. ADB, World Bank, KfW, GTZ, JICA, EU, DFID, Sida, UN agencies (i.e. UNHCR, UNDP, WFP, UNICEF, WHO, ILO) and other donors have provided financial (grant and loan) and technical assistance to improve rural access and opportunities. Rural development activities included, but were not limited to, rehabilitation of the rural infrastructure such as roads, market, water supply and sanitation; expanding rural credit
10 Source: H.E. Mr. Keat Chhon, Senior Minister of State in Charge of Rehabilitation and Development of Cambodia
as cited in Cambodia Times January 16‐22, 1994. “There are many ways to ensure security and rural development, although it is a long process, is the best way to ensure security. Rural development does not only mean agriculture. This includes the improvement of agricultural output, health facilities, education and change of behavior, which is very important. Overall, the quality of life must be improved and this is what rural development involves”.

33
services and income generating activities; and strengthening human resources and institutional capacity at the national, provincial and local levels.
Review of interventions on social sectors
95 Despite improving trends, the budget for social sectors remains low by East Asian standards. The RGC budget for social ministries increased by one‐half of a percentage points between 2004 and 2009, to 3.1% of GDP.11 This proportion remains lower than the regional level: in East Asia, average public spending in education alone was 4.3 percent in 2004 (see Figure 1 in the main text).12
96 Given the current budget structure, it is hard to determine the level of Government spending on social protection and safety nets. The new budget structure, in use since 2007, has two chapters (64 and 65) in which there are items labeled as social interventions, namely items 64.5, 65.7 and 65.8.13 Government expenditure on these items amounted to a total of US$181million across all Government agencies in 2008, showing a 55% increase since 2007 (Table 6). Given the level of aggregation in the budget, it is not possible however to determine how much of this amount goes to social protection and safety net activities, and how much to other types of social interventions. Furthermore, nearly all existing Government agencies report spending on these chapters, though not all are actually mandated with a social agenda. The large observed increase in social spending between 2007 and 2008 is in fact due to a large extent to increases in spending by non social ministries, such as Ministry of Water Resources and Meteorology, the Constitutional Council, the Ministry of Industry, Mines and Energy, and the Ministry of Agriculture, Forestry and Fishery. As a consequence, it is hard to assess whether the observed increase corresponds to an actual increase in spending on social programs (in particular safety nets).
11 The Royal Government of Cambodia includes in the classification of social Ministries the Ministries for
Information, Culture and Fine Arts, Environment, Cults and Religious Affairs. However, for the purpose of this review, a more conventional definition of social sectors is adopted, limited to the Ministries of Education, Youth and Sports (MOEYS); Health (MoH); Social Affairs, Veterans and Youth Rehabilitation (MOSVY); Labor and Vocational Training (MOLVT); and Women’s Affairs (MOWA).
12 Here defined as Education, Youth and Sports; Health; Social Affairs, Veterans, and Youth Rehabilitation; Labor and Vocational Training; and Women’s Affairs. The RGC also classifies as social Ministries: Information, Culture and Fine Arts, Environment, Public Worship and Religion (see Table 6). However, for the purpose of this review, a more conventional definition of social sectors is adopted.
13 Chapter 64.5 is called “Allowances and Social Transfers”, and includes: .1 Family; 2. Health and birth giving; 3. Death; 4. Retirement; 5. Demission; 6. Work accidents and Invalidity; 7. Orphans of personnel; 8. Other; 9. Return Attenuation. Chapter 65.7 refers to “Social Assistance”, which includes 1. Assistance for hospitalization; 2. Medicaments; 3. Food and supplies; 4. Natural Disaster; 5. Research Stipends; 6. Local scholarships and research; 7. Scholarships and research for abroad; 8. Others. Chapter 65.8 refers to “Subsidies to cultural and social entities”, including subsidies to: 1. Communities; 2. To orphan centers; 3. For travel scholarships; 4 For the Red Cross; 5. For sport and culture community; 6. To rehabilitation centers; 7. King’s affairs (King’s charity programs).
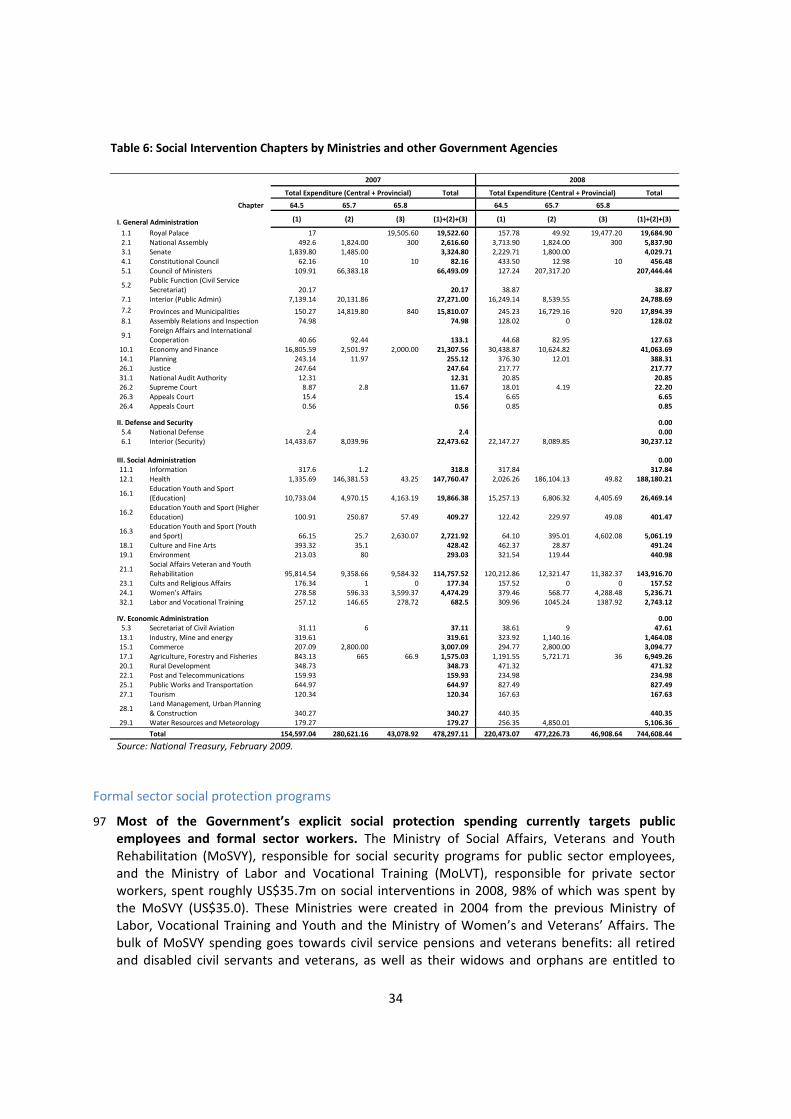
34
Table 6: Social Intervention Chapters by Ministries and other Government Agencies
2007 2008
Total Expenditure (Central + Provincial) Total Total Expenditure (Central + Provincial) Total
Chapter 64.5 65.7 65.8 64.5 65.7 65.8
I. General Administration (1) (2) (3) (1)+(2)+(3) (1) (2) (3) (1)+(2)+(3)
1.1 Royal Palace 17 19,505.60 19,522.60 157.78 49.92 19,477.20 19,684.902.1 National Assembly 492.6 1,824.00 300 2,616.60 3,713.90 1,824.00 300 5,837.903.1 Senate 1,839.80 1,485.00 3,324.80 2,229.71 1,800.00 4,029.71 4.1 Constitutional Council 62.16 10 10 82.16 433.50 12.98 10 456.485.1 Council of Ministers 109.91 66,383.18 66,493.09 127.24 207,317.20 207,444.44
5.2 Public Function (Civil Service Secretariat) 20.17 20.17 38.87 38.87
7.1 Interior (Public Admin) 7,139.14 20,131.86 27,271.00 16,249.14 8,539.55 24,788.697.2 Provinces and Municipalities 150.27 14,819.80 840 15,810.07 245.23 16,729.16 920 17,894.39 8.1 Assembly Relations and Inspection 74.98 74.98 128.02 0 128.02
9.1 Foreign Affairs and International Cooperation 40.66 92.44 133.1 44.68 82.95 127.63
10.1 Economy and Finance 16,805.59 2,501.97 2,000.00 21,307.56 30,438.87 10,624.82 41,063.6914.1 Planning 243.14 11.97 255.12 376.30 12.01 388.3126.1 Justice 247.64 247.64 217.77 217.7731.1 National Audit Authority 12.31 12.31 20.85 20.8526.2 Supreme Court 8.87 2.8 11.67 18.01 4.19 22.20 26.3 Appeals Court 15.4 15.4 6.65 6.6526.4 Appeals Court 0.56 0.56 0.85 0.85
II. Defense and Security 0.005.4 National Defense 2.4 2.4 0.006.1 Interior (Security) 14,433.67 8,039.96 22,473.62 22,147.27 8,089.85 30,237.12
III. Social Administration 0.0011.1 Information 317.6 1.2 318.8 317.84 317.84 12.1 Health 1,335.69 146,381.53 43.25 147,760.47 2,026.26 186,104.13 49.82 188,180.21
16.1 Education Youth and Sport (Education) 10,733.04 4,970.15 4,163.19 19,866.38 15,257.13 6,806.32 4,405.69 26,469.14
16.2 Education Youth and Sport (Higher Education) 100.91 250.87 57.49 409.27 122.42 229.97 49.08 401.47
16.3 Education Youth and Sport (Youth and Sport) 66.15 25.7 2,630.07 2,721.92 64.10 395.01 4,602.08 5,061.19
18.1 Culture and Fine Arts 393.32 35.1 428.42 462.37 28.87 491.24 19.1 Environment 213.03 80 293.03 321.54 119.44 440.98
21.1 Social Affairs Veteran and Youth Rehabilitation 95,814.54 9,358.66 9,584.32 114,757.52 120,212.86 12,321.47 11,382.37 143,916.70
23.1 Cults and Religious Affairs 176.34 1 0 177.34 157.52 0 0 157.5224.1 Women’s Affairs 278.58 596.33 3,599.37 4,474.29 379.46 568.77 4,288.48 5,236.7132.1 Labor and Vocational Training 257.12 146.65 278.72 682.5 309.96 1045.24 1387.92 2,743.12
IV. Economic Administration 0.005.3 Secretariat of Civil Aviation 31.11 6 37.11 38.61 9 47.61 13.1 Industry, Mine and energy 319.61 319.61 323.92 1,140.16 1,464.0815.1 Commerce 207.09 2,800.00 3,007.09 294.77 2,800.00 3,094.77 17.1 Agriculture, Forestry and Fisheries 843.13 665 66.9 1,575.03 1,191.55 5,721.71 36 6,949.2620.1 Rural Development 348.73 348.73 471.32 471.3222.1 Post and Telecommunications 159.93 159.93 234.98 234.98 25.1 Public Works and Transportation 644.97 644.97 827.49 827.4927.1 Tourism 120.34 120.34 167.63 167.63
28.1 Land Management, Urban Planning & Construction 340.27 340.27 440.35 440.35
29.1 Water Resources and Meteorology 179.27 179.27 256.35 4,850.01 5,106.36
Total 154,597.04 280,621.16 43,078.92 478,297.11 220,473.07 477,226.73 46,908.64 744,608.44
Source: National Treasury, February 2009.
Formal sector social protection programs
97 Most of the Government’s explicit social protection spending currently targets public employees and formal sector workers. The Ministry of Social Affairs, Veterans and Youth Rehabilitation (MoSVY), responsible for social security programs for public sector employees, and the Ministry of Labor and Vocational Training (MoLVT), responsible for private sector workers, spent roughly US$35.7m on social interventions in 2008, 98% of which was spent by the MoSVY (US$35.0). These Ministries were created in 2004 from the previous Ministry of Labor, Vocational Training and Youth and the Ministry of Women’s and Veterans’ Affairs. The bulk of MoSVY spending goes towards civil service pensions and veterans benefits: all retired and disabled civil servants and veterans, as well as their widows and orphans are entitled to

35
benefits in the form of pension and compensation. The MoLVT on the other hand, is responsible for the National Social Safety Fund (NSSF), established in 2008, which is set to provide by 2012 all private sector employees of firms with more than eight employees with: i) Employment injury coverage, ii) Health insurance, and iii) Pension coverage. With the introduction of the NSSF, social spending of the MoLVT increased by over 300% since 2007, to roughly US$668 thousand in 2008. As of February 2009, the NSSF had enrolled roughly 400 firms in the Employment injury scheme, about 250 of which are garment factories, covering a total of roughly 300,000 workers.14
98 The Ministry of Labor and Vocational Training (MoLVT) runs the National Social Safety Fund, established in 2008. This aims at providing private sector employees with: i) employment Injury coverage (workmen’s compensation), ii) health insurance, and iii) pension coverage. The MoLVT plans to phase in the implementation of these three components; the Employment Injury scheme already started in December 2008, while the Health Insurance and Pension Scheme are scheduled to start in 2010 and 2012, respectively. All firms having more than eight employees will be required to enroll in these schemes at the due time of the implementation phase. As of February 2009, the NSSF had enrolled roughly 400 firms in the Employment Injury scheme, about 250 of which are garment factories, covering a total of roughly 300,000 workers (interviews with NSSF representatives). The employer has to make a monthly contribution equals to 0.8% of the employee’s salary. The benefit is part in kind, part cash: the employee receives full medical assistance, plus receives 70% of the salary in order to compensate the forgone income during treatment.
99 The Ministry of Social Affairs, Veterans, and Youth Rehabilitation (MoSVY) provides assistance to retired civil servants, veterans and their dependents. The bulk of the Government’s social protection‐related expenditures goes towards this type of assistance. All retired and disabled civil servants and veterans, as well as their widows and orphans are entitled to benefits in the form of pension and compensation. Support for civil service pensions and veterans’ benefits receive the largest allocations of this budget. Beyond these priority areas, budget constraints have made it difficult for the Government to support even minimal direct interventions for the poor and vulnerable, and the Government relies on donors and NGOs to fill the gaps in reaching these groups.
100 Although allocations for civil service pensions account for a relatively large share of the total social protection budget, the payments are insufficient to meet the basic livelihood needs of beneficiaries. Most of MoSVY’s 2003 expenditures went toward pensions for over 22,000 retired civil servants. While the total amount of funding for pensions may seem substantial relative to the RGC’s overall expenditures, the actual amount received by beneficiaries in per capita terms as of 2003 was negligible. On average, retired civil servants received 70,000 Riels (US$17.50) per person per month in pensions, although some received as little as 27,000 Riels (US$7).
14 Data and the description of the NSSF coverage and workings were collected through personal interviews with
NSSF representatives.

36
Education
101 There have been significant improvements in the education sector in Cambodia over the past five years. This is seen particularly in terms of primary net enrollment gains, the introduction of program based‐budgeting and the development of a sound pro‐poor policy framework. Over the last decade, the RGC has steadily pursued its policy of reallocating public finances away from defense and security in favor of priority sectors; as a consequence, significant progress has been made in securing increasing and predictable resource for education. In 2009, RGC plans to increase the education budget from 1.60% to 2.09% of GDP. The total budget provided by donors to education in Cambodia during the school year 2006 2007 was in excess of $56m.
102 Since 2006 the Ministry of Education has implemented an education‐based pro‐poor intervention in the form of the Scholarship for the poor program. With support from various donors, as of October 2008 the program covered 21,459 children across all provinces except Phnom Penh. Eligible children are selected through a poverty assessment mechanism. School management committees collect information on students’ living standards through a survey: this information is consolidated in a database, on the basis of which a poverty index is calculated for each child. Scholarships are awarded to the 50% of all students with the highest poverty index. The poorest half of that 50% is labeled ‘very poor’ and the other half ‘medium poor’. The level of scholarship varies depending on (i) the level of poverty (medium or very) and (ii) school grade. At the lower secondary level, very poor children receive US$60 per year, while medium poor ones get US$45. At the primary level, all eligible children (very and medium poor) receive US$30 per year. Payments are made in three installments throughout the year. An evaluation of the Scholarship for the Poor Program has shown that it contributed to increasing enrolment by 20 percent (Filmer and Schady, 2009): building on this success, a pilot is currently underway aiming to expand the program in primary schools.
Health
103 In the health sector, the most notable effort to increase coverage of the poor and provide a form of insurance against health risks is that of Health Equity Funds. These are used to improve access to health care by the poor, as they were introduced to reimburse health providers for services to patients who are below the poverty line, thereby protecting poor patients against out‐of‐pocket payments while still allowing facilities to receive income. Equity funds serve as an important complement to existing supply‐side subsidies, which are aimed at lowering the cost of health care but generally do not reach the poor because of barriers to access such as unofficial demands for payment. As of March 2009, there were 50 HEFs in place in Cambodia, covering about 3,168,883 people or about 68% of the poor population in Cambodia. The Funds are managed in cooperation by government, donors and local NGOs.
104 HEF work closely with the Identification of the Poor project (ID Poor). Poor individuals, whether pre‐identified through the ID Poor process (see Box 1) or through an in situ assessment by medical staff (“post identification”), are covered for all costs of hospitalization and other medical services, as well as expenses for transportation and food during their stay in the medical facility. One drawback of Health Equity Funds is that they do not protect people who are above the poverty line and at risk of falling into poverty due to health care costs. Equity fund pilots in other countries address this issue by covering health care costs above an annual or episode maximum for the non‐poor, an option which could be explored for Cambodia to increase the risk reduction impact of equity funds.

37
Safety nets and pro‐poor programs
105 Safety nets programs in Cambodia consist mainly of food distribution and food‐for‐work / labor‐intensive public works programs. In October 2008 the Ministry of Economy and Finance implemented and co‐financed with US$5.08 million a US$40.08 million ADB‐financed food emergency operation to mitigate the effects of the increase in food prices on poor households. The emergency package consisted of a US$17.5 million grant and an additional US$17.5 million loan at concessional rates from the ADB, as well as the additional US$5.08 million from the Government of Cambodia, for a total of roughly US$40 million. Of these, approximately US$19 million will be allocated to social protection measures, with the remaining amount being allocated to measures aimed at increasing food productivity and government capacity in implementing food security operations. In the first phase, roughly 342,000 beneficiaries in 200 communes received in‐kind assistance (35Kg rice ratios) in the seven provinces surrounding the Tonle Sap Lake. The MEF Project Management Unit (PMU) is now considering food‐for‐work assistance to help poor households in food insecure areas coping with the lean season for the next two years.
106 The largest implementer of safety net programs remains the World Food Program (WFP), which in 2008 distributed 28,133 metric tons of rice to 886,929 beneficiaries, for a total value of US23.2m (see Table 4 in the main text for details on volume, value and number of beneficiaries of WFP programs in 2008). Through its Food for Work (FFW) program, in 2008 the WFP provided roughly 3,795.23mt of rice to 113,808 vulnerable beneficiaries in identified food insecure communes from the 12 most food insecure provinces, in exchange for work in public infrastructure projects. The WFP also implements a nutritional program, the Mother and Child Health (MCH) program, which distributes monthly food ratios (consisting of rice, vegetable oil, fortified corn soy blend and sugar) to pregnant and lactating mothers, living in poor households in food vulnerable communities. In 2008 the MCH distributed a total of 2,776.82 metric tons of food. The WFP works in partnership with local NGOs, who handle the food distribution, as well as health centers, which provide basic health education during the distribution.
107 UNICEF is one of the most active donors in supporting the RGC in implementing safety net programs. Its country program spans across various lines of social protection, ranging across education, child rights and nutrition (see Box 3 for a description of UNICEF programs). Since 2006, UNICEF has invested roughly USD16m per year on social protection intervention, and plans to invest an additional USD13m for 2009 and 2010, respectively (see Table 5 in the main text for details on UNICEF’s budget for social protection between 2006 and 2010). UNICEF’s strategy is to provide support to the RGC, by providing funds and helping in the implementation of its agenda. UNICEF focuses its attention to six priority provinces: Kampong Speu, Prey Veng, Svay Rieng, Kampong Thom, Stung Treng and Otdar Meanchey.
108 The Government also relies on donors, mainly WFP and UNICEF, for support to nutritional assistance. The WFP channels its nutrition interventions through the Mother and Child Health program, described above. UNICEF supports the RCG in its National Nutrition Program through the Child Survival Program (see Box 3), by providing nutritional assistance to mothers and children in the form of micronutrients, and providing nutritional education (i.e. training mothers on breastfeeding and feeding practices). Despite these efforts and the progress already achieved, malnutrition levels in Cambodia remain high, and much work remains to be done in this area.

38
109 Some workfare programs have also been put in place to assist the poor with under‐ and unemployment and improve local infrastructure. In addition to WFP’s Food for Work program, the Government has endorsed labor‐based appropriate technologies (LBAT) to generate employment through improvement and maintenance of essential rural infrastructure. The ILO and the ADB have been the main Development Partners to provide assistance to the
Box 3: UNICEF Social Protection programs
The Child Survival Program helps national counterparts achieve universal coverage of low‐cost and high‐impact life‐saving interventions to enhance child survival. The program consists of three projects: i) The Promoting Child Survival Project, that contributes to the nationwide expansion of immunization, control of diarrhoeal diseases and pneumonia, and malaria prevention; ii) The Improving Maternal Health and Newborn Care Project promotes access to antenatal care by skilled health personnel; iron supplementation; immunization with tetanus toxoid; promotion of clean delivery and referral for emergency obstetric care; knowledge and skills for exclusive breastfeeding; and vitamin A supplementation for lactating women; iii) The Health Behaviour Change Communication Project promotes key health and nutrition practices for child survival and development by strengthening the capacity of national, provincial and district health staff and other relevant actors to induce positive behaviour changes through a range of communication efforts.
The Expanded Basic Education Program supports the RGC to independently manage the Sector‐wide Approach (SWAp) for education and achieve the goals of Universal Primary Education. The program consists of three projects. i) The Capacity Building for Sector‐wide Education Reform and Decentralization Project assists national and provincial counterparts to effectively manage the SWAp with decreased reliance on external technical assistance; ii) The Improving Equitable Access and Quality of Basic Education Project provides support to primary teacher training colleges in promoting child friendly teaching and learning methods and supporting skills‐based health and hygiene promotion; iii) The Expanded Learning Opportunities for Disadvantaged Children and Youth Project addresses the specific needs of disadvantaged children without access to formal pre‐schools or basic education by supporting community or home‐based pre‐schools; a school readiness programme at the beginning of Grade 1; life skills education for in‐ and out‐of‐school youth; multi‐grade teaching and bilingual education for hard‐to‐reach and ethnic minority areas; accelerated learning for over‐aged children; and development and implementation of an inclusive education policy for children with disabilities.
The Child Protection Programme helps develop laws, policies and standards and raise national awareness, understanding and capacity to protect children at particular risk. The programme consists of three projects. The Social Protection Project will support the strengthening of systems to protect, care and reintegrate children without primary caregivers and children subjected to violence, abuse, trafficking and sexual exploitation. The Legal Protection Project will strengthen legislation to protect the rights of children in need of protection and will enhance government capacity and systems to develop and enforce legislation, particularly with regard to trafficking, sexual exploitation and abuse; alternative care including inter‐country adoption as a last resort; children in conflict with the law; and birth registration. The Accidents, Injuries and Disabilities Project will support actions to prevent, care for and rehabilitate children affected by landmines and UXO as well as by other accidents, injuries and disabilities.
The Local Governance for Child Rights Project (part of the Seth Koma Programme) facilitates collaboration among local government institutions, Commune Council members and local social service providers to promote positive behavior changes in communities and improve the delivery and utilization of basic social services for children and women.
Source: UNICEF –Royal Government of Cambodia (2006) Country Programme Action Plan

39
Government in implementing the Mainstreaming Labor‐Based Road Maintenance to the National Road Network program. Between 2006 and 2008, the ILO channeled nearly US$4.8m, roughly half from the Government and half from the Japanese Fund for Poverty Reduction, to this project. Between 2007 and 2008 ADB also provided US$690,398 to implement a Mainstreaming Labor‐Based Road Maintenance to the National Road Network program. The Government implemented this project through two agencies and coordinated its efforts though the Technical Working Groups.
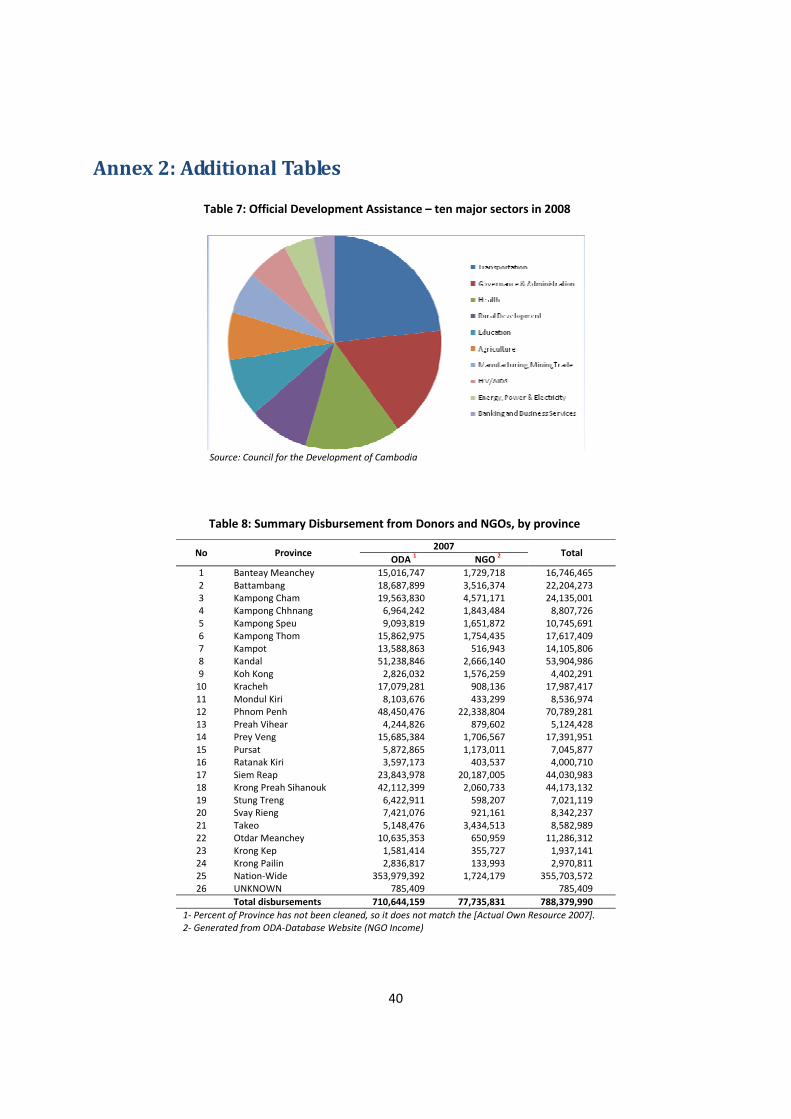
40
Annex 2: Additional Tables
Table 7: Official Development Assistance – ten major sectors in 2008
Source: Council for the Development of Cambodia
Table 8: Summary Disbursement from Donors and NGOs, by province
No Province 2007
Total ODA 1 NGO 2
1 Banteay Meanchey 15,016,747 1,729,718 16,746,465 2 Battambang 18,687,899 3,516,374 22,204,273 3 Kampong Cham 19,563,830 4,571,171 24,135,001 4 Kampong Chhnang 6,964,242 1,843,484 8,807,726 5 Kampong Speu 9,093,819 1,651,872 10,745,691 6 Kampong Thom 15,862,975 1,754,435 17,617,409 7 Kampot 13,588,863 516,943 14,105,806 8 Kandal 51,238,846 2,666,140 53,904,986 9 Koh Kong 2,826,032 1,576,259 4,402,291 10 Kracheh 17,079,281 908,136 17,987,417 11 Mondul Kiri 8,103,676 433,299 8,536,974 12 Phnom Penh 48,450,476 22,338,804 70,789,281 13 Preah Vihear 4,244,826 879,602 5,124,428 14 Prey Veng 15,685,384 1,706,567 17,391,951 15 Pursat 5,872,865 1,173,011 7,045,877 16 Ratanak Kiri 3,597,173 403,537 4,000,710 17 Siem Reap 23,843,978 20,187,005 44,030,983 18 Krong Preah Sihanouk 42,112,399 2,060,733 44,173,132 19 Stung Treng 6,422,911 598,207 7,021,119 20 Svay Rieng 7,421,076 921,161 8,342,237 21 Takeo 5,148,476 3,434,513 8,582,989 22 Otdar Meanchey 10,635,353 650,959 11,286,312 23 Krong Kep 1,581,414 355,727 1,937,141 24 Krong Pailin 2,836,817 133,993 2,970,811 25 Nation‐Wide 353,979,392 1,724,179 355,703,572 26 UNKNOWN 785,409 785,409 Total disbursements 710,644,159 77,735,831 788,379,990
1‐ Percent of Province has not been cleaned, so it does not match the [Actual Own Resource 2007]. 2‐ Generated from ODA‐Database Website (NGO Income)

41
Annex 3: List of social protectionrelated projects Table 9: Inventory of all ongoing donor funded projects related to Social Protection Donor Official Project Title
Health (40)
Hospitals1 Belgium Provision of Basic Health Services in the Province of Kampong Cham2 Belgium Provision of Basic Health Services in the Provinces of Siem Reap and Otdar Meanchey3 Japan The Project for Improving Maternal and Child Health Services in Prey Veng Operational District
2 Japan The Project for Installing Medical Equipment for Refferal Hospitals and Constructing of Kubal Damrey Health Post in Kratie Province
4 Republic of Korea
Strengthening the Refferal Hospitals in Cambodia or The Establishment of the Korea‐Cambodia Friendship Hospital in Kampong Chhnang
5 Switzerland Kantha Bopha Hospitals Primary Health
6 ADB JF9057 Health Care Financing for the Poor7 ADB LN1940 Health Sector Support Project8 Canada ADRA Canada 5 year Program 2006 ‐ 20119 EU/EC Community Based Health and Development Project
10 EU/EC Improving the Situation for Disadvantaged Groups in Rural Cambodia: A Capacity Building Approach to Community Mental Health Care
11 France Hospital policy and micro‐insurance12 Japan The Project for Improving Maternal and Child Health Service in Rural Area
13 UK Action Research to Advocacy (ARA): Empowering indigenous women to realise their health maternal rights in difficult environments of Cambodia
14 UK Health Sector Support (HSSP) ‐ Maternal Mortality Reduction (MMR)15 UNICEF Country Programme Action Plan 2006‐2010, Child Survival Programme16 USA Improved Health Services in HIV/AIDS and Infectious Diseases as well as in Maternal, Child and Reproductive Health 17 WFP Support for Mother‐and‐Child Health
Reproductive Health
18 EU/EC A Project to Address Unmet Need for Comprehensive Reproductive Health Information and Services Amongst Vulnerable Groups and the General Population in Four Key Locations in Cambodia
19 EU/EC Addressing the Reproductive Health, HIV and Primary Health Care Needs of Cambodian Women and Influencing Related National Policies
20 EU/EC Boosting Locally Based Health Education and Reproductive Health Services in Kompong Chhanang Province, Cambodia
21 EU/EC Improving the enabling environment to provide community led family planning and reproductive health to poor and vulnerable communities across 9 provinces ‐ CAMBODIA
22 EU/EC Rural Cambodian Youth Sexual Reproductive Health (RCYSRH)23 Germany Reproductive Health II 24 Germany Sector Related Program for Health25 Germany Support for Cambodia MDG 5: Improve Maternal Health (UNFPA)26 UK Health Sector Support (HSSP) ‐ Maternal Mortality Reduction (MMR)27 WFP Assisting People in Crisis
SWiM28 World Bank Health ‐ DFID Grant TF051053 Health Sector Support Project29 World Bank Health ‐ IDA Grant H0150: Health Sector Support Project30 World Bank Health ‐ IDA Grant H0160: Health Sector Support Project31 World Bank Health‐Main ‐ IDA 3728 Health Sector Support Project32 World Bank Health ‐Main ‐ IDA 44700 Cambodia Second Health Sector Support Program33 UK Health Sector Support (HSSP) 34 UK Health Sector Support Programme II (HSSP II)
Other35 Belgium Community primary health services in the province of Battambang36 Belgium Primary health services to mothers and children in Kompong Speu37 EU/EC Building the Capacity of Disability Rights Movements in Cambodia38 EU/EC Community Based Health Insurance (CBHI) for the Rural Poor39 EU/EC Towards the local ownership of the rehabilitation sector for People with Physical Disabilities (PWPD)‐ CAMBODIA 40 Netherlands Community‐based Rehabilitation for the Disabled

42
Donor Official Project Title
Education (16)
Primary/Basic41 ADB Improving Primary School Access in Disadvantaged Commune42 EU/EC EC Sector Budget Support to Basic Education 2008‐201043 EU/EC Improving Access to Quality Primary Education for Cambodian Street and Out‐of‐School Children, Cambodge
44 EU/EC Improving Livelihoods of Young Cambodians in Difficult Circumstances through Prevention and Sustainable Social Reintegration
45 EU/EC Mainstreaming Inclusive Primary Education, Cambodia46 EU/EC Targeted EC Support to Pro‐poor Education Reform in Cambodia ‐ Sector Budget Support47 Finland Assisting Children to School, ACTS48 World Bank Education ‐ TF92097 ‐ EDUCATION FOR ALL FAST TRACK INITIATIVE CATALYTIC TRUST FUND49 Sweden Expanded Basic Education Programme, Phase II 2006‐201050 UNICEF Country Programme Action Plan 2006‐2010, Expanded Basic Education Programme51 USA Increased Relevance, Quality and Access in Education52 WFP Assisting People in Crisis
Sector Policy53 EU/EC Targeted EC Support to Pro‐poor Education Reform in Cambodia ‐ Sector Budget Support54 World Bank Education ‐ JPN TF054868 Grant for Mainstreaming Inclusive Education Project
SWAp / sector budget support55 World Bank Education ‐ IDA Grant H0161: Education Sector Support Project56 World Bank Education‐ Main‐ IDA 40550 Education Sector Support Project
Community and Social Welfare (15)
57 ADB JF9017 Community‐Based Livelihood Enhancement for the Rural Poor in Northwestern Cambodia
58 ADB JF9064 Improving the Access of Poor Floating Communities on the Tonle Sap to Social Infrastructure and Livelihood Activities
59 ADB JF9114 Building Community Capacity for Poverty Reduction Initiatives in the Tonle Sap Basin60 Australia Asia Regional Trafficking in Persons Project61 Belgium Improvement of the working conditions of Cambodian workers62 EU/EC Community‐led poverty reduction in former conflict zones in North‐West Cambodia63 EU/EC Integrated approach to health promotion in highly vulnerable communities within Siem Reap Province, Cambodia. 64 FAO Off farm income generation with the National Programme for household Food Security and Poverty Reduction 65 Finland Prevention of trafficking in women and children66 ILO Better Factories Cambodia 67 ILO Support to Cambidan National Plan of Action on the Elinmination of the Worst Forms of Child Labour 68 Spain Integration of disabilities in the Development Policies in Cambodia69 Spain Social and Economic Development of the most vulnerable families of Phnom Penh70 Australia SCA Child Protection Implementation ‐ NGO Cooperation Agreements71 Japan The Project for Transporting Walkers for Disabilities
Emergency & Food Aid (5)
72 ADB TA7145 Strenthening Institutional Capacity for Emergency Response to Food Crisis and Improving Food Security 73 EU/EC Disaster Preparedness Programme 5th Action Plan for South East Asia ‐ Cambodia projects74 EU/EC Programme 6th Action Plan for South East Asia ‐ Cambodia projects75 Spain Humanitarian AID to WFP 'Assisting People in Crisis'76 WFP Assisting People in Crisis Source: own elaboration on the basis of information from the Council for Development of Cambodia, retrieved on June 10, 2009 from http://cdc.khmer.biz/

43
References
Aker, Jenny (2009) Cash (or food?) for thought: the debate on cash versus food isn’t over (yet). Center for Global Development http://blogs.cgdev.org/globaldevelopment/2009/03/cash‐or‐food‐for‐thought‐the‐d.php
Alderman, Harold, John Hoddinott and Bill Kinsey (2006), “Long Term Consequences on Early Childhood Malnutrition,” Oxford Economic Papers, 58(3), 450‐74.
ADI (2007) Understanding social capital in response to floods and droughts: a study of five villages in two ecological zones of Kompong Thom Province. CCC, Phnom Penh, August 2007. English: http://www.ccc‐cambodia.org/ADI%20Project/ADI%20Reports/Flood_and_Drought_Rp‐Eng.pdf Khmer: http://www.ccc‐cambodia.org/ADI%20Project/ADI%20Reports/Flood_and_Drought_Rp‐Kh.pdf
Braithwaite, Jeanine and Daniel Mont. (2008), “Disability and Poverty: A Survey of World Bank Poverty Assessments and Implications.” World Bank: SP Discussion Papers, No. 0805. February.
Carter, Michael R., Peter D. Little, Trevodaj Morgues and Workneh Negatu (2004) “Shocks, sensitivity and resilience: tracking the economic impacts of environmental disasters on assets in Ethiopia and Honduras.” BASIS Research Program on Poverty, Inequality, and Development, USAID, Washington, DC. CDRI (2009, forthcoming) Rapid assessment of the impacts of the economic crisis on Cambodian households: component 2 – informal risk management and safety net practices (working title). Cambodia Development Resource Institute: Phnom Penh. Chea Chantum and Hildegard Lingnau (2008) “Social security and social policies in Cambodia.” pp. 11‐16 in Cambodia Development Review Vol. 12 Issue 4 December 2008. http://www.cdri.org.kh/ Del Ninno, Carlo; Subbarao, Kalanidhi and Milazzo, Annamaria (2009) How to make public works work: a review of the experiences. World Bank Social Protection Discussion Paper No. 0905 Delvert, Jean (1961) Le Paysan Cambodgien. Paris, The Hague: Mouton and Co. Chapters 7, 14, 16 and 17 translated into English in 1997 by Ms. Sonal Shah. Devereaux, Stephen and Clare Gorman (2006) Unconditional cash transfers in Africa. IDS in Focus Issue 1: social protection. May 2006. Ebihara, May (1968) Svay, a Khmer village in Cambodia. PhD dissertation: Columbia University: 1968 / Ann Arbor Michigan: University Microfilms: 1971. Fafchamps, Marcel, Christopher Udry and Katherine Czukas (1998), “Drought and Saving in West Africa: Are Livestock a Buffer Stock?,” Journal of Development Economics, 55(2), 273‐305. Farrington, John and Rachel Slater (2006) “Cash transfers: panacea for poverty reduction or money down the drain?” Editors’ introduction to special cash transfers theme issue of Development Policy Review Vol. 24 No. 5 (September 2006)
Ferreira, Francisco and Norbert Schady (2008), “Aggregate Economic Shocks, Child Schooling, and Child Health,” World Bank Policy Research Working Paper, No. 4701.
Filmer, Deon, and Norbert Schady (2006) Getting girls into school: evidence from a scholarship program in Cambodia. World Bank Policy Research Working Paper No. 3910 http://www‐

44
wds.worldbank.org/servlet/WDSContentServer/WDSP/IB/2007/11/28/000158349_20071128084228/Rendered/PDF/wps3910.pdf Filmer, Deon, and Norbert Schady (2009) Promoting schooling through scholarships in Cambodia: evidence from the Education Sector Support Project. Impact Evaluation Brief: World Bank.
Fiszbein, Ariel and Norbert Schady with Francisco H.G. Ferreira, Margaret Grosh, Nial Kelleher, Pedro Olinto and Emmanuel Skoufias (2009) Conditional cash transfers: reducing present and future poverty. World Bank Policy Research Report: Washington DC. http://go.worldbank.org/H9PAWAIX70
Gentilini, Ugo (2007) Cash and food transfers: a primer. WFP Occasional Paper No. 18; 2007. http://wfp.org/policies/Introduction/other/Documents/pdf/OP18_Cash_and_Food_Transfers_Eng%2007.pdf
Gentilini, Ugo (2008) “Cash transfers, vouchers and food transfers: an overview of the key issues.” Rural 21: May 2008. www.rural21.com/uploads/media/rural_eng_19‐21_03.pdf
Grosh, Margaret, Carlo del Ninno, Emil Tesliuc, and Azedine Ouerghi (2008) For protection and promotion: the design and implementation of effective safety nets. World Bank http://go.worldbank.org/K0Z8SB4VJ0
Kang Chandararot, Sok Sina, Kim Sedara and Liv Dannet (2009) Rapid assessment on the impact f the financial crisis in Cambodia. CIDS with support from ILO; Phnom Penh; January 2009. Kiernan, Ben (1982) “Introductory note” pp. 31‐3 in Ben Kiernan and Chanthou Boua (eds.) (1982) Peasants and politics in Kampuchea, 1942‐81. London: Zed Press / Armonk, NY: M.E. Sharpe Inc.: 1982. Kim Sedara (2001) Reciprocity: informal patterns of social interactions in a Cambodian village near Angkor park. MA thesis; Department of Anthropology, Northern Illinois University.
Krishnamurthy, Veena with Huon Sathea, Koy Pharin, Pho Seng Ban, Prak Somonea and Ros Pheak (1999) The impact of armed conflict on social capital: a study of two villages in Cambodia. Social Services of Cambodia for World Bank: March 1999.
McAndrew, John (1998) Interdependence in household livelihood strategies in two Cambodian villages. CDRI Working Paper No. 7. CDRI in association with UNRISD. www.cdri.org.kh
Meas Nee (with Joan Healy) (1995) Towards restoring life: Cambodian villages. Phnom Penh: JSRC. Mont, Daniel. (2007), “Measuring Disability Prevalence.” World Bank: SP Discussion Papers, No. 0706. March.
Morduch, Jonathan and Manohar Sharma (2002) “Strengthening public safety nets from the bottom up.” Development Policy Review Volume 20 Number 5: 569‐588. http://www3.interscience.wiley.com/cgi‐bin/fulltext/118955799/PDFSTART
National MCH Centre, WVI and NIPH (2008) Cambodia Anthropometrics Survey 2008: initial findings of national survey. Presentation of key findings from a survey organized by National MCH Center, World Vision Cambodia and National Institute of Public Health.
Ngy Chanphal (2009) Developing Effective and Affordable Social Safety Nets for Cambodia. Discussion Paper. February 10.
Norton, Andy, Tim Conway and Mick Foster (2001) Social protection concepts and approaches: implications for policy and practice in international development. ODI Working Paper 143; London; February 2001. http://www.odi.org.uk/resources/download/2178.pdf

45
Prom Tola (2007) Cambodia country report – final (Volume 6 in Scaling up of the Social Protection Index for committed poverty reduction) Halcrow China Ltd. For ADB, November 2007.
Ravallion, Martin (2003), “Targeted Transfers in Poor Countries: Revisiting the Trade‐Offs and Policy Options,” World Bank Social Protection Discussion Paper, No. 0314.
Ravallion, Martin (2008), “Bailing out the world’s poorest,” World Bank Policy Research Working Paper, No. 4763.
Subbarao, Kalanidhi and Bruni, Lucilla Maria (2009) “A short policy note on Food and Cash for Work Programs in Cambodia,” draft document.
UNDP (2006) “Social protection: the role of cash transfers.” Poverty in Focus June 2006; UNDP International Poverty Centre.
UNICEF (1995‐6) Towards a better future: an analysis of the situation of children and women in Cambodia. Phnom Penh.
UNICEF (2008) Evaluation of UNICEF‐supported health equity fund in Svay Rieng province. Sophie Biacabe for UNICEF; May 2008.
World Bank. (2006a) Cambodia: Halving Poverty by 2015?. Poverty Assessment 2006. Report No. 35213‐KH. February. http://go.worldbank.org/0VEL0T5SZ0
World Bank (2006b), Making the New Indonesia Work for the Poor. http://indopov.org/newindonesia.pdf
World Bank. (2006c), Managing Risk and Vulnerability in Cambodia: An Assessment and Strategy for Social Protection. June. http://go.worldbank.org/TBUMQRBO32
World Bank (2009) Poverty profile and trends in Cambodia, 2007. June 2007.

46
Acronyms ADB Asian Development Bank ADI Analysis of Development Initiatives BTC Belgian Technical CooperationCAMINCO Cambodia National Insurance Company CARD Council for Agricultural and Rural Development CAS Cambodia Anthropometric Surveys CBHI Community‐Based Health Insurance CCC Cooperation Committee for Cambodia CCT conditional cash transfer CDCF Cambodia Development Cooperation Forum CDRI Cambodia Development Resource Institute CHHRA Cambodia Health and Human Rights Alliance CIDS Cambodia Institute for Development Studies DFID Department for International Development (UK) DP Development Partner EU European Union FFT food‐for‐training FFW food‐for‐work GDP Gross Domestic Product GRET Group de Recerche et d’Echanges Technolgiques GTZ Gesellschaft für Technische Zussamenarbeit (German technical cooperation) HEF Health Equity Fund IDS Institute for Development Studies (Brighton) ILO International Labour Organisation LBAT Labour‐Based Appropriate Technology m million MAFF Ministry of Agriculture, Forestry and Fishery MCH Mother and Child Health MEF Ministry of Economy and FinanceMOEYS Ministry of Education, Youth and Sports MOH Ministry of Health MOLVT Ministry of Labour and Vocational Training MoP Ministry of Planning MoSVY Ministry of Social Affairs, Veterans and Youth Rehabilitation MoWA Ministry of Women's Affairs MRD Ministry of Rural Development mt metric tonnes NGO Non‐Governmental Organization NIPH National Institute for Public Health NPRS National Poverty Reduction Strategy (2003‐5) NPRDC National Programme for the Rehabilitation and Development of CambodiaNSDP National Strategic Development Plan NSFC National Social Security Fund for Civil Servants NSSF National Social Safety Fund ODA Official Development Assistance ODI Overseas Development Institute (London) PPA participatory poverty assessment

47
RACHA Reproductive and Child Health Alliance RGC Royal Government of Cambodia SEDP Socio‐Economic Development Plans (1996‐2000 and 2001‐2005) Sida Swedish International Development Agency SNEC Supreme National Economic Council TB tuberculosis TWG‐FSN Technical Working Group for Food Security and Nutrition UNDP United Nations Development Programme UNICEF United Nations Children's Fund USAID United States Agency for International Development WB World Bank WFP World Food Progamme WHO World Health Organisation WVI World Vision International