safety first: the use of restraints - lms.rn.com · • the type or technique of restraint or...
TRANSCRIPT
Material protected by Copyright
Safety First: The Use of Restraints
This course has been awarded Two (2.0) contact hours.
Copyright © 2010 by RN.com. All Rights Reserved. Reproduction and distribution
of these materials are prohibited without the express written authorization of RN.com.
First Published: May 20, 2010
Updated: July 18, 2013 Updated: January 19, 2018 Expires: January 31, 2021

Material protected by Copyright
Acknowledgements RN.com acknowledges the valuable contributions of… … Suzan R. Miller-Hoover DNP, RN, CCNS, CCRN-K Conflict of Interest and Commercial Support RN.com strives to present content in a fair and unbiased manner at all times, and has a full and fair disclosure policy that requires course faculty to declare any real or apparent commercial affiliation related to the content of this presentation. Note: Conflict of Interest is defined by ANCC as a situation in which an individual has an opportunity to affect educational content about products or services of a commercial interest with which he/she has a financial relationship. The author of this course does not have any conflict of interest to declare. The planners of the educational activity have no conflicts of interest to disclose. There is no commercial support being used for this course.

Material protected by Copyright
Purpose The purpose of this course is to provide healthcare workers with the skills and knowledge to care for patients requiring the use of restraints. Restraint use is very regulated by national and state regulations; therefore, this course will explore the regulations and how they affect healthcare workers and institutions. Because restraint regulations are different for psychiatric and long-term care facilities, this module will concentrate on restraint use in acute-care facilities. Objectives After successful completion of this course, you will be able to: 1. Define physical restraints, chemical restraints, non-violent/non-self-harm restraints, and
violent/self-harm restraints 2. Discuss when to use restraints 3. Discuss less restrictive measures and how they affect restraint use 4. Identify risk factors associated with restraint use 5. Delineate order set requirements for the different types of restraints 6. Delineate nursing care standards for caring for and documentation of restraints

Material protected by Copyright
Introduction All healthcare institutions must consider restraint use of any kind as a last resort for managing patients with therapeutic devices that need protecting or patients who have the potential to hurt themselves or others. Restraint use is not without associated risks. Therefore, the Joint Commission (TJC) and the Centers for Medicare and Medicaid Services (CMS) along with state and local regulatory agencies have enacted special programs to safe guard patients, families, visitors, and healthcare workers. Important Note: Each of the governing agencies’ expectations are similar; however, there are distinct differences which may make a specific agency’s rules more prescriptive. It is up to the healthcare facility to determine which agency’s regulations to follow. CMS standards were written to guide healthcare facilities who care for patients utilizing Medicare and Medicare. TJC standards were written for healthcare facilities operating under TJC accreditation. CMS and TJC standards apply to:
• All hospitals (acute care, long-term care, psychiatric, children's, and cancer) that use TJC accreditation for deemed status purposes
• All locations within the hospital (including medical/surgical units, critical care units, forensic units, emergency department, psychiatric units, etc.)
• All hospital patients, regardless of age, who are restrained or secluded (including both inpatients and outpatients) (CMS, 2015 & TJC, 2017)
As you can see, healthcare facilities which have JC accreditation, care for Medicare/Medicaid patients, and exist in a state with restraint regulations will have to review and develop policies which contain elements from all three agencies. This module will discuss the regulations and how to put them into action. Each facility will have policies, procedures, and documentation requirements; be sure to read, know, and follow these policies in your organization. Regulatory Requisites Centers for Medicare and Medicaid Services (CMS): Conditions of Participation (CoP) This document ensures that hospitals and other institutions caring for patients covered by Medicare and Medicaid receive a high standard of care based on patient outcomes. Restraints are covered under the CoP §482.13 Condition of Participation: Patient’s Rights.
• §482.13(e) Standard: Restraint or Seclusion • §482.13(f) Standard: Restraint or Seclusion: Staff Training Requirements • §482.13(g) Standard: Death Reporting Requirements
(Centers for Medicare and Medicaid (CMS), 2015) Each of these standards have multiple criterions to further delineate the standards. The Joint Commission (TJC): Provision of Care, Treatment, and Services (PC) This document reveals what a facility with JC accreditation must do to ensure continued high standards of care with positive outcomes. Restraints are covered in the following chapters:
• PC.03.05.01: The hospital uses restraint or seclusion only when it can be clinically justified or when warranted by patient behavior that threatens the physical safety of the patient, staff, or

Material protected by Copyright
others. • PC.03.05.03: The hospital uses restraint or seclusion safely • PC.03.05.05: The hospital initiates restraint or seclusion based on an individual order • PC.03.05.07: The hospital monitors patients who are restrained or secluded. • PC.03.05.09: The hospital has written policies and procedures that guide the use of restraint or
seclusion. • PC.03.05.11: The hospital evaluates and reevaluates the patient who is restrained or
secluded. o A physician, clinical psychologist, or other licensed independent practitioner responsible
• PC.03.05.13: The hospital continually monitors patients who are simultaneously restrained and secluded.
• PC.03.05.15: The hospital documents the use of restraint or seclusion. • PC.03.05.17: The hospital trains staff to safely implement the use of restraint or seclusion • PC.03.05.19: The hospital reports deaths associated with the use of restraint and seclusion.
(The Joint Commission (TJC), 2017) Each of these chapters have multiple criterions to further delineate the standards. This module will refer to the standards of CMS and TJC chapters and criterions. To see each document in its entirety, refer to Appendices A & B. Definitions These restraint definitions are used by CMS and TJC.
• Physical Restraint: 42 CFR 482.13(e)(1) (i)(A): Any manual method, physical or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient to move his or her arms, legs, body, or head freely
• Chemical Restraint: 42 CFR 482.13 (e)(1)(i)(B): A drug or medication when it is used as a restriction to manage the patient’s behavior or restrict the patient’s freedom of movement and is not a standard treatment or dosage for the patient’s condition
• 42 CFR 482.13(e)(1)(i)(C): A restraint does not include devices, such as orthopedically prescribed devices, surgical dressings or bandages, protective helmets, or other methods that involve the physical holding of a patient for the purpose of conducting routine physical examinations or tests, or to protect the patient from falling out of bed, or to permit the patient to participate in activities without the risk of physical harm (this does not include a physical escort)
• Seclusion: 42 CFR 482.13(e)(1)(ii): the involuntary confinement of a patient alone in a room or area from which the patient is physically prevented from leaving. Seclusion may only be used for the management of violent or self-destructive behavior
• Non-violent/Non-Self-Destructive Restraints: Protection from the removal of medical devices before medically indicated
• Violent/Self-Destructive Restraints: Protection from behaviors that jeopardizes the immediate safety of patients and staff
(CMS, 2015 & TJC, 2017) Restraints: The Last Resort Did you read appendices A & B and are you now an expert on restraints? Probably not, more than likely you are overwhelmed by the amount of regulations guiding the use of restraints! Not to worry, this module will simplify the amount of information and help guide your practice to help ensure that safe restraint use and good patient outcomes.

Material protected by Copyright
Operationalizing the Regulations This section is based on Appendices A-CMS Conditions of Participation & B-TJC Provision of Care, please refer to the appendices for the actual regulatory verbiage. In some cases, either CMS or TJC may be more prescriptive than the other. The most prescriptive regulations will be discussed. CMS Standard: 482.13(e) and TJC PC.03.05.01 through PC.03.05.05 regulate when restraints can be used. Most important to note:
• The hospital uses restraint or seclusion only when it can be clinically justified or when warranted by patient behavior that threatens the physical safety of the patient, staff, or others.
• All patients have the right to be free from restraint or seclusion, of any form, imposed as a means of coercion, discipline, convenience, or retaliation by staff.
• The type or technique of restraint or seclusion used must be the least restrictive intervention that will be effective to protect the patient, a staff member, or others from harm.
• The hospital uses the least restrictive form of restraint or seclusion that protects the physical safety of the patient, staff, or others.
• The hospital discontinues restraint or seclusion at the earliest possible time, regardless of the scheduled expiration of the order.
• The hospital implements restraint or seclusion using safe techniques identified by the hospital’s policies and procedures in accordance with law and regulation.
• The use of restraint and seclusion is in accordance with a written modification to the patient’s plan of care.
• The hospital initiates restraint or seclusion based on an individual order Operationalization: Writing policies which are inclusive of the CMS and TJC standards.
• The hospital’s policies and procedures regarding restraint or seclusion include, but are not inclusive of, the following:
o Physician, clinical psychologist, and other authorized licensed independent practitioner training requirements
o Staff training requirements o The determination of who has authority to order restraint and seclusion o The determination of who has authority to discontinue the use of restraint or seclusion o The determination of who can initiate the use of restraint or seclusion o The circumstances under which restraint or seclusion is discontinued o The requirement that restraint or seclusion is discontinued as soon as is safely possible o A definition of restraint in accordance with 42 CFR 482.13(e)(1)(i) (A–C) o A definition of seclusion in accordance with 42 CFR 482.13(e)(1)(ii) o A definition or description of what constitutes the use of medications as a restraint in
accordance with 42 CFR 482.13(e)(1)(i)(B) o A determination of who can assess and monitor patients in restraint or seclusion o Time frames for assessing and monitoring patients in restraint or seclusion
Restraint: Orders Non-violent/non-self-destructive Restraints
• A physician, clinical psychologist, or other authorized licensed independent practitioner primarily responsible for the patient’s ongoing care orders the use of restraint or seclusion in
Material protected by Copyright
accordance with hospital policy and law and regulation • The hospital does not use standing orders or PRN (also known as “as needed”) orders for
restraint or seclusion. • The attending physician or clinical psychologist is consulted as soon as possible, in
accordance with hospital policy, if he or she did not order the restraint or seclusion. • Unless state law is more restrictive, every 24 hours, a physician, clinical psychologist, or other
authorized licensed independent practitioner primarily responsible for the patient’s ongoing care sees and evaluates the patient before writing a new order for restraint or seclusion used for the management of violent or self-destructive behavior that jeopardizes the immediate physical safety of the patient, staff, or others in accordance with hospital policy and law and regulation.
• Orders for restraint used to protect the physical safety of the nonviolent or non–self-destructive patient are renewed in accordance with hospital policy
Operationalization:
• The order for restraints, whenever possible, should be written by the trained healthcare provider prior to applying the restraints. The exception to this rule, is when the medical device is in eminent danger of being removed or otherwise damaged. In this circumstance, the nurse can apply the restraints and then call the physician for orders as soon as possible.
• The orders must be renewed every 24 hours. o If your facility states in the policy that the orders are renewed every day, that is
acceptable, but the statement must be in the policy about when the orders are renewed. Violent/Self-Destructive Restraints Orders
• Unless superseded by State law that is more restrictive: o Each order for restraint or seclusion used for the management of violent or self-
destructive behavior that jeopardizes the immediate physical safety of the patient, a staff member, or others may only be renewed in accordance with the following limits for up to a total of 24 hours: 4 hours for adults 18 years of age or older 2 hours for children and adolescents 9 to 17 years of age 1 hour for children under 9 years of age
o After 24 hours, before writing a new order for the use of restraint or seclusion for the management of violent or self-destructive behavior, a physician or other licensed independent practitioner who is responsible for the care of the patient as specified under §482.12(c) of this part and authorized to order restraint or seclusion by hospital policy in accordance with State law must see and assess the patient.
• When restraint or seclusion is used for the management of violent or self-destructive behavior that jeopardizes the immediate physical safety of the patient, a staff member, or others, the patient must be seen face-to-face within 1 hour after the initiation of the intervention by a:
o Physician or another licensed independent practitioner; or o Registered nurse or physician assistant who has been trained in accordance with the
requirements specified in paragraph (f) of this section.
Operationalization: Restraint use for violent or self-destructive behaviors is more highly regulated than non-violent behavior restraints. This is because the violent patient is at a higher risk for untoward events. Violent/Self-Harm Restraint orders are therefore stricter for both the nurse and healthcare providers. The most difficult portion of these orders to operationalize is the requirement that the healthcare

Material protected by Copyright
provider must come in and see the patient face-to-face within one hour of the restraint or seclusion being implemented. Additionally, if the patient discontinues the behavior within that hour, the provider MUST still have a face to face assessment within that first hour. This is because the patient’s behavior, no matter how short lived, indicates a serious medical or psychological need for prompt evaluation of the behavior that led to the intervention. To help alleviate the time constraints of this regulation, nurses or physician assistants can be trained to conduct this evaluation. Neither agency states what should be in a restraint order; however, restraint order contents must be outlined in policy.
• Restraint orders include: o Date and time of restraint order o Expiration date and time of order o What type of restraint o Circumstances under which a restraint is to be discontinued o What restraint device should be used
Restraint: Monitoring and Documentation TJC standard PC.03.05.13
• The patient who is restrained for non-violent behavior should be assessed every two hours • The patient who is restrained for violent behavior should be assessed every 15 minutes • The patient who is simultaneously restrained and secluded is continually monitored by trained
staff either in-person or through the use of both video and audio equipment that is in close proximity to the patient. Note: In this element of performance “continually” means ongoing without interruption
• Documentation of restraint and seclusion in the medical record includes the following: o Any in-person medical and behavioral evaluation for restraint or seclusion used to
manage violent or self-destructive behavior o A description of the patient’s behavior and the intervention used o Any alternatives or other less restrictive interventions attempted o The patient’s condition or symptom(s) that warranted the use of the restraint or
seclusion o The patient’s response to the intervention(s) used, including the rationale for continued
use of the intervention • Individual patient assessments and reassessments o The intervals for monitoring o Revisions to the plan of care o The patient’s behavior and staff concerns regarding safety risks to the patient, staff, and
others that necessitated the use of restraint or seclusion o Injuries to the patient • Death associated with the use of restraint or seclusion
Restraint: Training CMS standard §482.13(f) and TJC standards PC.03.05.15 & PC.03.05.17:
• The hospital documents the use of restraint or seclusion. o The hospital trains staff on the use of restraint and seclusion, and assesses their
competence, at the following intervals: At orientation Before participating in the use of restraint and seclusion On a periodic basis thereafter
• The hospital must require appropriate staff to have education, training, and demonstrated

Material protected by Copyright
knowledge based on the specific needs of the patient population in at least the following: o Techniques to identify staff and patient behaviors, events, and environmental factors
that may trigger circumstances that require the use of a restraint or seclusion. • Training content: Individuals providing staff training must be qualified as evidenced by
education, training, and experience in techniques used to address patients' behaviors • Training documentation: The hospital must document in the staff personnel records that the
training and demonstration of competency were successfully completed. Restraint: Death Reporting CMS standard §482.13(g) and TJC standard PC.03.05.19: The hospital reports the following information to the Centers for Medicare & Medicaid Services (CMS) regarding deaths related to restraint or seclusion.
• Each death that occurs while a patient is in restraint or seclusion • Each death that occurs within 24 hours after the patient has been removed from restraint or
seclusion • Each death known to the hospital that occurs within 1 week after restraint or seclusion where it
is reasonable to assume that use of restraint or placement in seclusion contributed directly or indirectly to a patient's death.
Restraint: Alternatives CMS and TJC recognize that there may be circumstances in which the use of restraint or seclusion may be necessary to prevent a patient situation from escalating, staff often skillfully intervene with alternative techniques to redirect a patient, engage the patient in constructive discussion or activity, or otherwise help the patient maintain self-control and avert escalation. The use of nonphysical intervention skills does not mean attempting a complex series of interventions or a lengthy checklist of steps to initiate before restraining or secluding a patient. Rather, a whole toolbox of possible interventions can be implemented during the course of a patient’s treatment based upon the assessment of an individual patient’s responses. What types of alternatives can you identify?
• Distraction o TV o Folding towels/wash cloths
• Family presence • Sitters • Placing the patient in a room closer to the nurse’s station • Placing a patient in or near the nurse’s station to interact with staff
Are there others? Think of what your hospital has available to use with patients to help keep them from pulling out medical devices? Restraint: Assessment Before restraints can be used, a thorough patient assessment should be performed. What are the behaviors the patient is exhibiting? Is there an underlying issue that needs to be attended to? Is the patient in pain? Is the patient bored? Does the patient need to use the restroom? Are there medical devices that are in danger of being pulled out? Is the patient in danger of harming him/her self or staff members?

Material protected by Copyright
These questions need to be answered before you make the decision to restrain the patient.
Material protected by Copyright
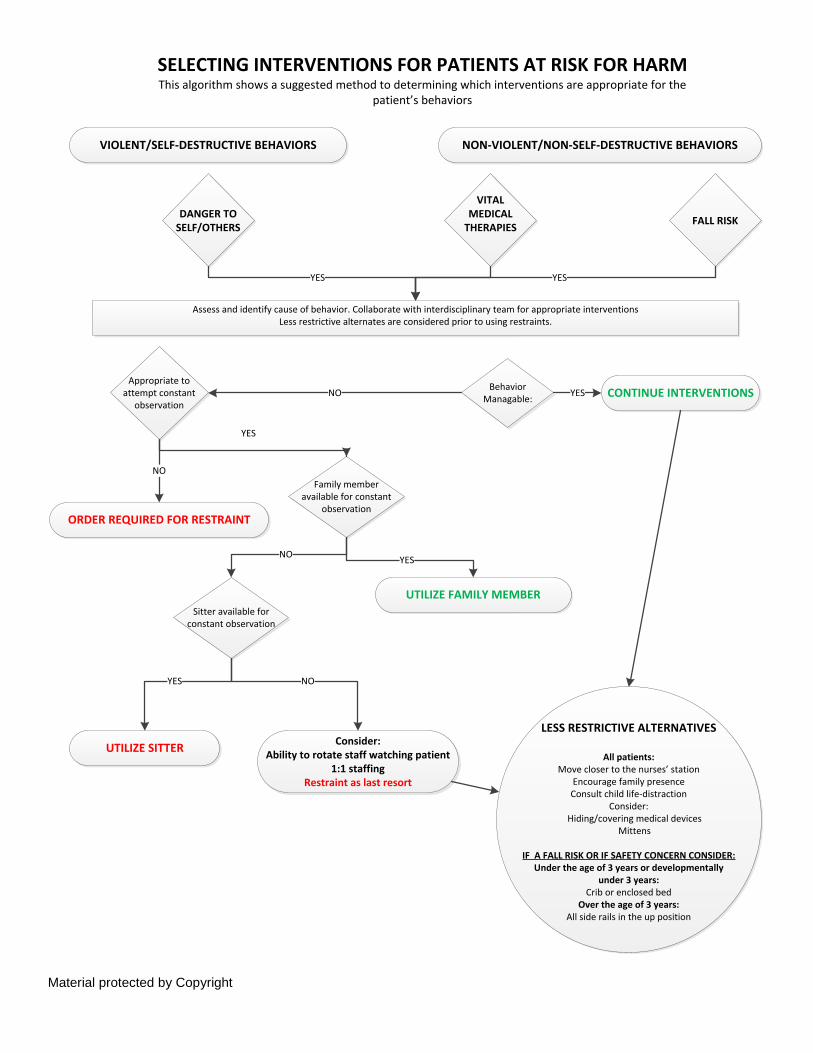
SELECTING INTERVENTIONS FOR PATIENTS AT RISK FOR HARMThis algorithm shows a suggested method to determining which interventions are appropriate for the
patient’s behaviors
VIOLENT/SELF-DESTRUCTIVE BEHAVIORS
Consider:Ability to rotate staff watching patient
1:1 staffingRestraint as last resort
UTILIZE SITTER
NON-VIOLENT/NON-SELF-DESTRUCTIVE BEHAVIORS
UTILIZE FAMILY MEMBER
ORDER REQUIRED FOR RESTRAINT
DANGER TO SELF/OTHERS
VITAL MEDICAL
THERAPIES FALL RISK
Assess and identify cause of behavior. Collaborate with interdisciplinary team for appropriate interventionsLess restrictive alternates are considered prior to using restraints.
Behavior Managable:
Family member available for constant
observation
Appropriate to attempt constant
observation
Sitter available for constant observation
YES YES
NO
YES
YESNO
YES NO
CONTINUE INTERVENTIONSYES
NO
LESS RESTRICTIVE ALTERNATIVES
All patients: Move closer to the nurses’ station
Encourage family presenceConsult child life-distraction
Consider: Hiding/covering medical devices
Mittens
IF A FALL RISK OR IF SAFETY CONCERN CONSIDER:Under the age of 3 years or developmentally
under 3 years:Crib or enclosed bed
Over the age of 3 years:All side rails in the up position
Material protected by Copyright
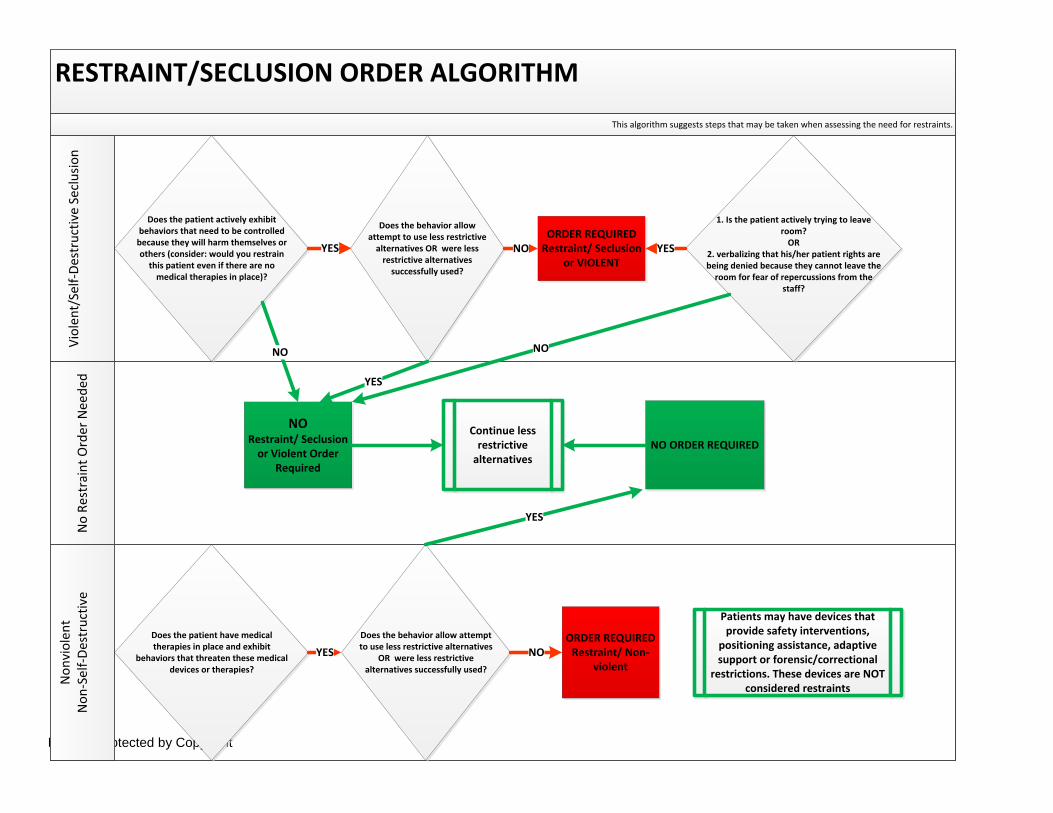
RESTRAINT/SECLUSION ORDER ALGORITHMN
o Re
stra
int O
rder
Nee
ded
Viol
ent/
Self-
Dest
ruct
ive
Secl
usio
nN
onvi
olen
t N
on-S
elf-D
estr
uctiv
e
This algorithm suggests steps that may be taken when assessing the need for restraints.
Does the patient actively exhibit behaviors that need to be controlled
because they will harm themselves or others (consider: would you restrain
this patient even if there are no medical therapies in place)?
Does the behavior allow attempt to use less restrictive
alternatives OR were less restrictive alternatives
successfully used?
ORDER REQUIREDRestraint/ Seclusion
or VIOLENT
1. Is the patient actively trying to leave room?
OR2. verbalizing that his/her patient rights are being denied because they cannot leave the
room for fear of repercussions from the staff?
NO ORDER REQUIREDContinue less
restrictive alternatives
NO Restraint/ Seclusion
or Violent Order Required
Does the patient have medical therapies in place and exhibit
behaviors that threaten these medical devices or therapies?
Does the behavior allow attempt to use less restrictive alternatives
OR were less restrictive alternatives successfully used?
ORDER REQUIREDRestraint/ Non-
violent
Patients may have devices that provide safety interventions,
positioning assistance, adaptive support or forensic/correctional
restrictions. These devices are NOT considered restraints
YES NO YES
NO
YES
NO
NOYES
YES

Material protected by Copyright
Case Study 1: Mrs. C is 89 years-old and hospitalized for a broken leg. The leg was repaired and casted late yesterday evening. Mrs. C’s family has gone home to get some much-needed rest after a very long and stressful day. Mrs. C is restless and trying to get out of bed. What is your assessment?
A. Restrain Mrs. C before she gets hurt B. Assess Mrs. C for pain and the need to use the bathroom C. Assess Mrs. C as a high risk for falls D. Assign a sitter to Mrs. C
If your assessment includes all but A, you are correct. There are underlying reasons why Mrs. C may be restless and trying to get out of bed. You are treating Mrs. C with less restrictive alternatives than restraints. You have given Mrs. C pain medications that were ordered for her postoperative rehabilitation. You have established and documented that Mrs. C is a high-risk for falls and have placed all four-side rails up to help protect her from getting out of bed. You are documenting your interventions, you document:
A. Mrs. C is a high-risk for fall due to pain medications, her age, and because she has a long-leg cast on. All four side-rails are placed up to help decrease her chance of falling.
B. Mrs. C. is being placed in non-violent/non-self-harm restraints due to the use of chemical restraints and physical restraints (side rails up).
C. Mrs. C. is being placed in violent/self-harm restraints due to her attempts to get out of bed D. Mrs. C is being placed in soft-restraints to remind her to stay in bed
Because you know the restraint requirements, you know that Mrs. C is not considered to be restrained. Your decision is based on:
• Mrs. C’s behavior is based on pain and a recent surgery. Making her a high-risk for falls, putting all four side-rails up, and documenting that, assures that you are keeping her safe.
• Mrs. C is prescribed pain medications, so the pain medications are not considered a chemical restraint
• While Mrs. C’s behavior is putting her at risk for self-harm, she is not being restrained by your interventions
• If you place Mrs. C in soft-restraints, you will be restraining her and will need an order One of your colleagues suggests that instead of placing all four side-rails in the raised position, you should consider only raising three side rails. You wonder if this is an effective way to keep Mrs. C safe from falling. Your colleague explains, that according the CMS interpretive guidelines and your hospital’s policy, there is a fine line between side-rails as a restraint and side-rails as a safety intervention. The CMS interpretive guides state, raising fewer than four side rails when the bed has segmented side rails would not necessarily immobilize or reduce the ability of a patient to move freely as defined in the regulation. For example, if the side rails are segmented and all but one segment are raised to allow the patient to freely exit the bed, the side rail is not acting as a restraint. In the elderly population, use of all four side rails is risky, especially for the disoriented, who may see the side-rail as a barrier to be climbed over, may crawl out the end of the bed, or may try to get

Material protected by Copyright
between the segmented rails. CMS interpretive guidelines state: the patient may have an increased risk for a fall or other injury by attempting to exit the bed with the side rails raised. The risk presented by side rail use should be weighed against the risk presented by the patient's behavior as ascertained through individualized assessment. Raising fewer than four side rails when the bed has segmented side rails would not necessarily immobilize or reduce the ability of a patient to move freely as defined in the regulation. For example, if the side rails are segmented and all but one segment are raised to allow the patient to freely exit the bed, the side rail is not acting as a restraint. As a result of this conversation, what do you consider?
A. Putting all four side-rails in the down position B. Angling the side-rail with one end down to allow a safer exit from the bed C. Doing nothing, you are within the guidelines The most prudent and easily defended solution is to put the side-rail in an angled down position (the same as putting one segmented side-rail down).
Case Study 2 Johnny B. is an 18-year-old admitted to the emergency department with a suspicion of drug intoxication. He appears to be cooperative and lethargic. An IV is placed for hydration and for medication administration. The drug screen indicates that Johnny has taken a drug with hallucinogenic properties. You are concerned that he may become violent and institute which of the following:
A. Place him in violent/self-harm restraints – he may become violent B. Place him in non-violent/non-self-harm restraints – he may pull out his IV C. Place him in seclusion – he may try to hurt the staff D. He requires no restraint at this time – his behavior doesn’t warrant restraints
Rationale: PC.03.05.01: The hospital uses restraint or seclusion only when it can be clinically justified or when warranted by patient behavior that threatens the physical safety of the patient, staff, or others. Restraints: Devices Restraints are NOT defined by the type of device used. There are many devices that may be restraints in specific circumstances and are not restraints in other circumstances. The assessment of the patient and situation will guide the healthcare worker to the right decision. Consider the developmentally delayed teenager who weighs 250 pounds. He is attempting to pull out his naso-gastric tube. Due to his size and strength, soft wrist restraints are ineffective. Can you place him in neoprene restraints (locking restraints)? If you do, is he in violent or non-violent restraints? The answer is: You can place him in neoprene restraints and still be able to document non-violent restraint use. Remember: CMS and TJC require that you use the least restrictive restraint. (CMS §482.13(e)(3) - The type or technique of restraint or seclusion used must be the least restrictive intervention that will be effective to protect the patient, a staff member, or others from harm)

Material protected by Copyright
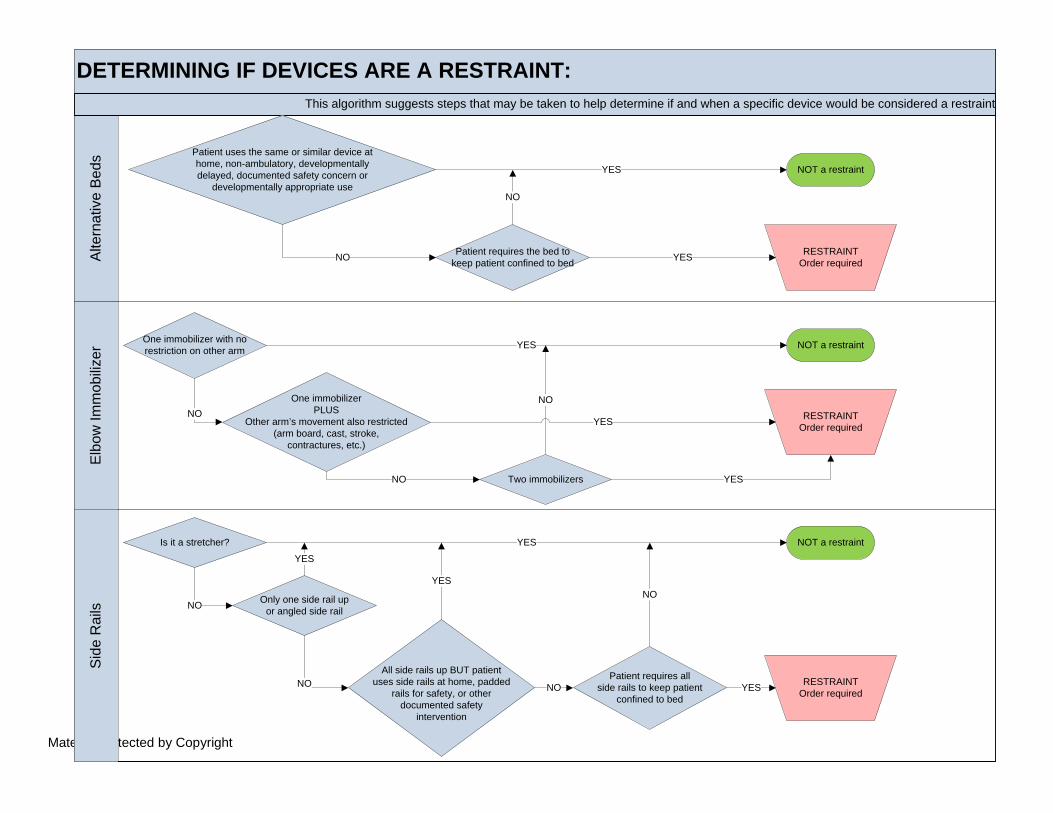
The following algorithm suggests way to determine if a device is being used as a restraint.
Material protected by Copyright
DETERMINING IF DEVICES ARE A RESTRAINT:Si
de R
ails
Elbo
w Im
mob
ilizer
Alte
rnat
ive
Beds
This algorithm suggests steps that may be taken to help determine if and when a specific device would be considered a restraint
Patient uses the same or similar device athome, non-ambulatory, developmentallydelayed, documented safety concern or
developmentally appropriate use
Patient requires the bed to keep patient confined to bed
One immobilizer with no restriction on other arm
One immobilizerPLUS
Other arm’s movement also restricted (arm board, cast, stroke,
contractures, etc.)
Only one side rail upor angled side rail
All side rails up BUT patientuses side rails at home, padded
rails for safety, or other documented safety
intervention
NOT a restraint
NOT a restraint
NOT a restraint
Two immobilizers
RESTRAINTOrder required
RESTRAINTOrder required
RESTRAINTOrder required
YES
YES
YES
YES
YES
YES
YES
NO
NO
NO
NO
Is it a stretcher? YES
NO
Patient requires allside rails to keep patient
confined to bed
NO
NO
NO
NO YES
Material protected by Copyright
What other devices might be considered restraints:
A. Mitts with thumb B. Mitts or gloves attached to the bed C. Sheets tucked in tightly D. Papooses
Rationale: Every device above except for mitts with a thumb would be considered restraints as you are restricting the patient’s ability to move. Restraint: Medications One of the hardest concepts to master is whether a medication is considered a chemical restraint. Psychiatric or sedative medications when used routinely as part of the patient’s treatment plan are NOT considered restraints. Can you determine if the situations below are using a medication as a chemical restraint? Fentanyl, Versed, and Rocuronium in the intensive care unit to help ventilate a patient Valium used to stop a seizure Haldol to treat “sundowner’s syndrome” Haldol to stop a psychiatric patient from acting out The first two examples are of medications used within a treatment plan to treat a medical condition. While the medication used to help ventilate a patient restricts movement, it is usually used within an ordered plan of care for a specific reason. From the information listed above, it is hard to tell for sure if the Haldol is being used as a restraint. Consider: Is the patient with “sun downer’s syndrome” a known patient? Does he require Haldol on a regular or PRN basis to control his syndrome?
• If the answer is yes, then the Haldol is NOT a chemical restraint. However, if the patient just started exhibiting the signs of sundowner’s and he is given a one-time dose of Haldol and it puts him to sleep; he Has Been chemically restrained.
• If the dose was meant to relax him and not put him to sleep to restrict his behavior, then he is NOT chemically restrained.
Again, with the use of Haldol with the psychiatric patient, if the drug is part of the treatment plan, it is NOT a restraint
• If it is used to diminish his movements, it is NOT a restraint • If it is used to completely restrict his movements, it IS a restraint
Medications that are prescheduled, routinely scheduled, and PRN medications are not considered chemical restraints. In most cases, chemical restraints are just-in-time medications used to de-escalate a violent patient’s harmful behavior. Restraint: Seclusion Which of the following scenarios indicates that the patient is in seclusion?
A. A suicidal patient voluntarily confined to his/her room with a sitter present B. A Suicidal patient involuntarily confined to his/her room with a sitter present

Material protected by Copyright
The operative word that defines seclusion is “involuntarily” confined. In some states, there is a 3-day hold that a member of the psychiatric team can place on a patient who meets certain criteria. This 3-day hold is considered seclusion as the patient is not free to leave. A “time-out” is not considered seclusion or restraint. A time-out is usually considered part of the treatment plan and is for a predetermined amount of time for a predetermined behavior. Restraint: Other
A. Family member presence is considered a less-restrictive alternative to restraints. B. If the restraints are removed while the family is present and then placed back on after they
leave, this is considered discontinuing the restraint and a new order is required. C. If the restraints are removed while a healthcare worker is in the room for the purpose of caring
for the patient’s needs, and then replaced before the healthcare worker leaves the room, this is NOT an episode of restraint and no new order is required.
Conclusion: Safe patient care hinges on looking at the patient as an individual and assessing the patient’s condition, needs, strengths, weaknesses, and preferences. Such an approach relies on caregivers who are skilled in individualized assessment and in tailoring interventions to individual patient’s needs after weighing factors such as the patient’s condition, behaviors, history, and environmental factors. There will always be situations where restraints are necessary, but most of the time patient’s behaviors should be managed with alternative methods. Restraint regulations are highly prescriptive, and they should be, to protect the patient and the healthcare worker.
RESTRAINT SHOULD ALWAYS BE USED AS A LAST RESORT!!

Material protected by Copyright
References Centers for Medicare & Medicaid (CMS). (2015). The CMS Interpretive Guidelines for the Hospital Conditions of Participation. Retrieved from: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R37SOMA.pdf §482.13(e) Standard: Restraint or Seclusion §482.13(f) Standard: Restraint or Seclusion: Staff Training Requirements §482.13(g) Standard: Death Reporting Requirements The Joint Commission. Comprehensive Accreditation Manual for Hospitals, Oak Brook, IL: Joint Commission Resources, 2017. Longo, M.A. & Miller-Hoover, S. (2016). Effective decision making in the use of pediatric restraints. Journal of Pediatric Nursing.31:2, 217-221.
Material protected by Copyright
Disclaimer This publication is intended solely for the educational use of healthcare professionals taking this course, for credit, from RN.com, in accordance with RN.com terms of use. It is designed to assist healthcare professionals, including nurses, in addressing many issues associated with healthcare. The guidance provided in this publication is general in nature, and is not designed to address any specific situation. As always, in assessing and responding to specific patient care situations, healthcare professionals must use their judgment, as well as follow the policies of their organization and any applicable law. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Healthcare organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Healthcare providers, hospitals and facilities that use this publication agree to defend and indemnify, and shall hold RN.com, including its parent(s), subsidiaries, affiliates, officers/directors, and employees from liability resulting from the use of this publication. The contents of this publication may not be reproduced without written permission from RN.com. Participants are advised that the accredited status of RN.com does not imply endorsement by the provider or ANCC of any products/therapeutics mentioned in this course. The information in the course is for educational purposes only. There is no “off label” usage of drugs or products discussed in this course. You may find that both generic and trade names are used in courses produced by RN.com. The use of trade names does not indicate any preference of one trade named agent or company over another. Trade names are provided to enhance recognition of agents described in the course. Note: All dosages given are for adults unless otherwise stated. The information on medications contained in this course is not meant to be prescriptive or all-encompassing. You are encouraged to consult with physicians and pharmacists about all medication issues for your patients.

Material protected by Copyright
Appendix B: Centers for Medicare and Medicaid Services (CMS)
Conditions of Participation (CoP) This document ensures that hospitals and other institutions caring for patients covered by Medicare and Medicaid receive a high standard of care based on patient outcomes. §482.13 Condition of Participation: Patient’s Rights This CoP delineates what a patient should know about his/her rights while hospitalized. Included in this section are three standards that refer to restraint and seclusion. These standards are:
• §482.13(e) Standard: Restraint or Seclusion o All patients have the right to be free from physical or mental abuse, and corporal
punishment. All patients have the right to be free from restraint or seclusion, of any form, imposed as a means of coercion, discipline, convenience, or retaliation by staff. Restraint or seclusion may only be imposed to ensure the immediate physical safety of the patient, a staff member, or others and must be discontinued at the earliest possible time.
o Restraint or seclusion may only be used when less restrictive interventions have been determined to be ineffective to protect the patient, a staff member, or others from harm.
o The type or technique of restraint or seclusion used must be the least restrictive intervention that will be effective to protect the patient, a staff member, or others from harm.
o The use of restraint or seclusion must be in accordance with a written modification to the patient's plan of care Implemented in accordance with safe and appropriate restraint and seclusion
techniques as determined by hospital policy in accordance with State law o The use of restraint or seclusion must be in accordance with the order of a physician or
other licensed independent practitioner who is responsible for the care of the patient as specified under §481.12(c) and authorized to order restraint or seclusion by hospital policy in accordance with State law.
o Orders for the use of restraint or seclusion must never be written as a standing order or on an as needed basis (PRN).
o The attending physician must be consulted as soon as possible if the attending physician did not order the restraint or seclusion.
o Unless superseded by State law that is more restrictive: Each order for restraint or seclusion used for the management of violent or self-
destructive behavior that jeopardizes the immediate physical safety of the patient, a staff member, or others may only be renewed in accordance with the following limits for up to a total of 24 hours:
• 4 hours for adults 18 years of age or older • 2 hours for children and adolescents 9 to 17 years of age • 1 hour for children under 9 years of age
After 24 hours, before writing a new order for the use of restraint or seclusion for the management of violent or self-destructive behavior, a physician or other licensed independent practitioner who is responsible for the care of the patient as specified under §482.12(c) of this part and authorized to order restraint or seclusion by hospital policy in accordance with State law must see and assess the patient.
o Each order for restraint used to ensure the physical safety of the non-violent or non-self-destructive patient may be renewed as authorized by hospital policy.
o The condition of the patient who is restrained or secluded must be monitored by a
Material protected by Copyright
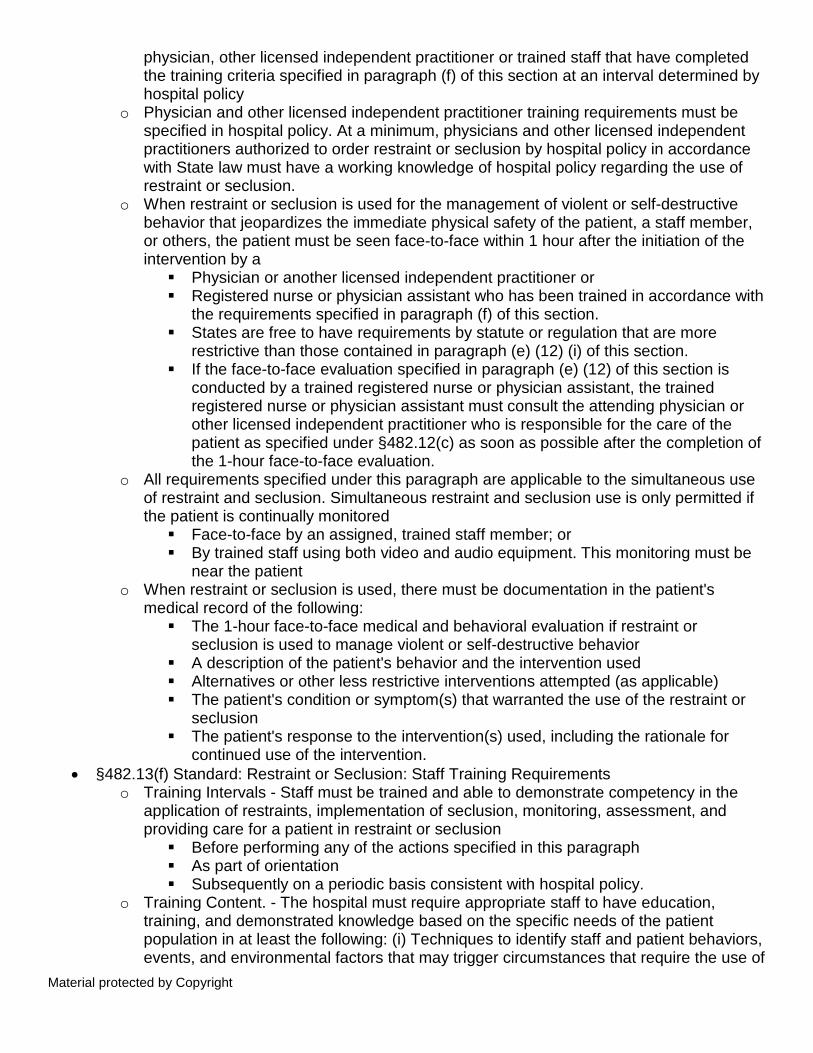
physician, other licensed independent practitioner or trained staff that have completed the training criteria specified in paragraph (f) of this section at an interval determined by hospital policy
o Physician and other licensed independent practitioner training requirements must be specified in hospital policy. At a minimum, physicians and other licensed independent practitioners authorized to order restraint or seclusion by hospital policy in accordance with State law must have a working knowledge of hospital policy regarding the use of restraint or seclusion.
o When restraint or seclusion is used for the management of violent or self-destructive behavior that jeopardizes the immediate physical safety of the patient, a staff member, or others, the patient must be seen face-to-face within 1 hour after the initiation of the intervention by a Physician or another licensed independent practitioner or Registered nurse or physician assistant who has been trained in accordance with
the requirements specified in paragraph (f) of this section. States are free to have requirements by statute or regulation that are more
restrictive than those contained in paragraph (e) (12) (i) of this section. If the face-to-face evaluation specified in paragraph (e) (12) of this section is
conducted by a trained registered nurse or physician assistant, the trained registered nurse or physician assistant must consult the attending physician or other licensed independent practitioner who is responsible for the care of the patient as specified under §482.12(c) as soon as possible after the completion of the 1-hour face-to-face evaluation.
o All requirements specified under this paragraph are applicable to the simultaneous use of restraint and seclusion. Simultaneous restraint and seclusion use is only permitted if the patient is continually monitored Face-to-face by an assigned, trained staff member; or By trained staff using both video and audio equipment. This monitoring must be
near the patient o When restraint or seclusion is used, there must be documentation in the patient's
medical record of the following: The 1-hour face-to-face medical and behavioral evaluation if restraint or
seclusion is used to manage violent or self-destructive behavior A description of the patient's behavior and the intervention used Alternatives or other less restrictive interventions attempted (as applicable) The patient's condition or symptom(s) that warranted the use of the restraint or
seclusion The patient's response to the intervention(s) used, including the rationale for
continued use of the intervention. • §482.13(f) Standard: Restraint or Seclusion: Staff Training Requirements
o Training Intervals - Staff must be trained and able to demonstrate competency in the application of restraints, implementation of seclusion, monitoring, assessment, and providing care for a patient in restraint or seclusion Before performing any of the actions specified in this paragraph As part of orientation Subsequently on a periodic basis consistent with hospital policy.
o Training Content. - The hospital must require appropriate staff to have education, training, and demonstrated knowledge based on the specific needs of the patient population in at least the following: (i) Techniques to identify staff and patient behaviors, events, and environmental factors that may trigger circumstances that require the use of

Material protected by Copyright
a restraint or seclusion. The use of nonphysical intervention skills Choosing the least restrictive intervention based on an individualized assessment
of the patient's medical, or behavioral status or condition The safe application and use of all types of restraint or seclusion used in the
hospital, including training in how to recognize and respond to signs of physical and psychological distress (for example, positional asphyxia)
Clinical identification of specific behavioral changes that indicate that restraint or seclusion is no longer necessary
Staff must be trained and demonstrate competency in monitoring the physical and psychological well-being of a patient who is restrained or secluded, including but not limited to, respiratory and circulatory status, skin integrity, vital signs, and as well as any special requirements specified by hospital policy associated with the 1-hour face-to-face evaluation
The use of first aid techniques and certification in the use of cardiopulmonary resuscitation, including required periodic recertification
o Trainer Requirements. - Individuals providing staff training must be qualified as evidenced by education, training, and experience in techniques used to address patients' behaviors
o Training Documentation. - The hospital must document in the staff personnel records that the training and demonstration of competency were successfully completed.
• §482.13(g) Standard: Death Reporting Requirements Hospitals must report deaths associated with the use of seclusion or restraint.
o The hospital must report the following information to CMS: Each death that occurs while a patient is in restraint or seclusion Each death that occurs within 24 hours after the patient has been removed from
restraint or seclusion Each death known to the hospital that occurs within 1 week after restraint or
seclusion where it is reasonable to assume that use of restraint or placement in seclusion contributed directly or indirectly to a patient's death.
• “Reasonable to assume” in this context includes, but is not limited to, deaths related to restrictions of movement for prolonged periods of time, or death related to chest compression, restriction of breathing or asphyxiation
• Each death referenced in this paragraph must be reported to CMS by telephone no later than the close of business the next business day following knowledge of the patient's death
• Staff must document in the patient's medical record the date and time the death was reported to CMS.
(Centers for Medicare and Medicaid (CMS), 2015)

Material protected by Copyright
Appendix B: The Joint Commission (TJC) Provision of Care, Treatment, and Services (PC) This document reveals what a facility with JC accreditation must do to ensure continued high standards of care with positive outcomes. Within this Provision of Care, Treatment, and Services Chapter, TJC discusses what the facility must do to ensure patient safety with the use of restraints and seclusion. Within this chapter, there are ten standards that refer to the use of restraints and seclusion. These standards are:
• PC.03.05.01: The hospital uses restraint or seclusion only when it can be clinically justified or when warranted by patient behavior that threatens the physical safety of the patient, staff, or others.
o The hospital uses restraint or seclusion only to protect the immediate physical safety of the patient, staff, or others.
o The hospital does not use restraint or seclusion as a means of coercion, discipline, convenience, or staff retaliation.
o The hospital uses restraint or seclusion only when less restrictive interventions are ineffective.
o The hospital uses the least restrictive form of restraint or seclusion that protects the physical safety of the patient, staff, or others.
o The hospital discontinues restraint or seclusion at the earliest possible time, regardless of the scheduled expiration of the order.
• PC.03.05.03: The hospital uses restraint or seclusion safely. o The hospital implements restraint or seclusion using safe techniques identified by the
hospital’s policies and procedures in accordance with law and regulation. o The use of restraint and seclusion is in accordance with a written modification to the
patient’s plan of care. • PC.03.05.05: The hospital initiates restraint or seclusion based on an individual order
o A physician, clinical psychologist, or other authorized licensed independent practitioner primarily responsible for the patient’s ongoing care orders the use of restraint or seclusion in accordance with hospital policy and law and regulation
o The hospital does not use standing orders or PRN (also known as “as needed”) orders for restraint or seclusion.
o The attending physician or clinical psychologist is consulted as soon as possible, in accordance with hospital policy, if he or she did not order the restraint or seclusion.
o Unless state law is more restrictive, orders for the use of restraint or seclusion used for the management of violent or self-destructive behavior that jeopardizes the immediate physical safety of the patient, staff, or others may be renewed with the following limits: 4 hours for adults 18 years of age or older 2 hours for children and adolescents 9 to 17 years of age 1 hour for children under 9 years of age Orders may be renewed according to the time limits for a maximum of 24
consecutive hours. o Unless state law is more restrictive, every 24 hours, a physician, clinical psychologist, or
other authorized licensed independent practitioner primarily responsible for the patient’s ongoing care sees and evaluates the patient before writing a new order for restraint or seclusion used for the management of violet or self-destructive behavior that jeopardizes the immediate physical safety of the patient, staff, or others in accordance

Material protected by Copyright
with hospital policy and law and regulation. o Orders for restraint used to protect the physical safety of the nonviolent or non–self-
destructive patient are renewed in accordance with hospital policy • PC.03.05.07: The hospital monitors patients who are restrained or secluded.
o Physicians, clinical psychologists, or other licensed independent practitioners or staff who have been trained in accordance with 42 CFR 482.13(f) monitor the condition of patients in restraint or seclusion.
• PC.03.05.09: The hospital has written policies and procedures that guide the use of restraint or seclusion.
o The hospital’s policies and procedures regarding restraint or seclusion include the following: Physician, clinical psychologist, and other authorized licensed independent
practitioner training requirements Staff training requirements • The determination of who has authority to order
restraint and seclusion The determination of who has authority to discontinue the use of restraint or
seclusion The determination of who can initiate the use of restraint or seclusion The circumstances under which restraint or seclusion is discontinued • The
requirement that restraint or seclusion is discontinued as soon as is safely possible
A definition of restraint in accordance with 42 CFR 482.13(e)(1)(i) (A–C) A definition of seclusion in accordance with 42 CFR 482.13(e)(1)(ii) • A definition
or description of what constitutes the use of medications as a restraint in accordance with 42 CFR 482.13(e)(1)(i)(B)
A determination of who can assess and monitor patients in restraint or seclusion Time frames for assessing and monitoring patients in restraint or seclusion
o Physicians, clinical psychologists, and other licensed independent practitioners authorized to order restraint or seclusion (through hospital policy in accordance with law and regulation) have a working knowledge of the hospital policy regarding the use of restraint and seclusion.
• PC.03.05.11: The hospital evaluates and reevaluates the patient who is restrained or secluded.
o A physician, clinical psychologist, or other licensed independent practitioner responsible for the care of the patient evaluates the patient in-person within one hour of the initiation of restraint or seclusion used for the management of violent or self-destructive behavior that jeopardizes the physical safety of the patient, staff, or others. A registered nurse or a physician assistant may conduct the in-person evaluation within one hour of the initiation of restraint or seclusion; this individual is trained in accordance with the requirements in PC.03.05.17, EP 3.
o When the in-person evaluation (performed within one hour of the initiation of restraint or seclusion) is done by a trained registered nurse or trained physician assistant, he or she consults with the attending physician, clinical psychologist, or other licensed independent practitioner responsible for the care of the patient as soon as possible after the evaluation, as determined by hospital policy.
o The in-person evaluation, conducted within one hour of the initiation of restraint or seclusion for the management of violent or self-destructive behavior that jeopardizes the physical safety of the patient, staff, or others, includes the following: An evaluation of the patient’s immediate situation The patient’s reaction to the intervention

Material protected by Copyright
The patient’s medical and behavioral condition The need to continue or terminate the restraint or seclusion
• PC.03.05.13: The hospital continually monitors patients who are simultaneously restrained and secluded.
o The patient who is simultaneously restrained and secluded is continually monitored by trained staff either in-person or through the use of both video and audio equipment that is in close proximity to the patient. Note: In this element of performance “continually” means ongoing without interruption
o Documentation of restraint and seclusion in the medical record includes the following: Any in-person medical and behavioral evaluation for restraint or seclusion used
to manage violent or self-destructive behavior A description of the patient’s behavior and the intervention used Any alternatives or other less restrictive interventions attempted The patient’s condition or symptom(s) that warranted the use of the restraint or
seclusion The patient’s response to the intervention(s) used, including the rationale for
continues use of the intervention • Individual patient assessments and reassessments
The intervals for monitoring Revisions to the plan of care The patient’s behavior and staff concerns regarding safety risks to the patient,
staff, and others that necessitated the use of restraint or seclusion Injuries to the patient • Death associated with the use of restraint or seclusion The identity of the physician, clinical psychologist, or other licensed independent
practitioner who ordered the restraint or seclusion Orders for restraint or seclusion Notification of the use of restraint or seclusion to the attending physician Consultations
• PC.03.05.15: The hospital documents the use of restraint or seclusion. o The hospital trains staff on the use of restraint and seclusion, and assesses their
competence, at the following intervals: At orientation Before participating in the use of restraint and seclusion On a periodic basis thereafter
• PC.03.05.17: The hospital trains staff to safely implement the use of restraint or seclusion o Based on the population served, staff education, training, and demonstrated knowledge
focus on the following: Strategies to identify staff and patient behaviors, events, and environmental
factors that may trigger circumstances that require the use of restraint or seclusion.
Use of nonphysical intervention skills Methods for choosing the least restrictive intervention based on an assessment
of the patient’s medical or behavioral status or condition Safe application and use of all types of restraint or seclusion used in the hospital,
including training in how to recognize and respond to signs of physical and psychological distress (for example, positional asphyxia)
Clinical identification of specific behavioral changes that indicate that restraint or seclusion is no longer necessary
Monitoring the physical and psychological well-being of the patient who is restrained or secluded, including, but not limited to, respiratory and circulatory

Material protected by Copyright
status, skin integrity, vital signs, and any special requirements specified by hospital policy associated with the in-person evaluation conducted within one hour of initiation of restraint or seclusion
Use of first-aid techniques and certification in the use of cardiopulmonary resuscitation, including required periodic recertification
o Individuals providing staff training in restraint or seclusion have education, training, and experience in the techniques used to address patient behaviors that necessitate the use of restraint or seclusion.
o The hospital documents in staff records that restraint and seclusion training and demonstration of competence were completed.
• PC.03.05.19: The hospital reports deaths associated with the use of restraint and seclusion. o The hospital reports the following information to the Centers for Medicare & Medicaid
Services (CMS) regarding deaths related to restraint or seclusion (this requirement does not apply to deaths related to the use of soft wrist restraints; for more information, refer to EP 3 in this standard): Each death that occurs while a patient is in restraint or seclusion Each death that occurs within 24 hours after the patient has been removed from
restraint or seclusion Each death known to the hospital that occurs within one week after restraint or
seclusion was used when it is reasonable to assume that the use of the restraint or seclusion contributed directly or indirectly to the patient’s death. The types of restraints included in this reporting requirement are all restraints except soft wrist restraints.
(The Joint Commission (TJC), 2017).